methamphetamine: who really gets burned nathan kemalyan, md facs medical director, oregon burn...
TRANSCRIPT

Methamphetamine:Who Really Gets Burned
Nathan Kemalyan, MD FACS
Medical Director, Oregon Burn Center
Credits:
Kelli Salter, M.D.
Surgical Resident, OHSU

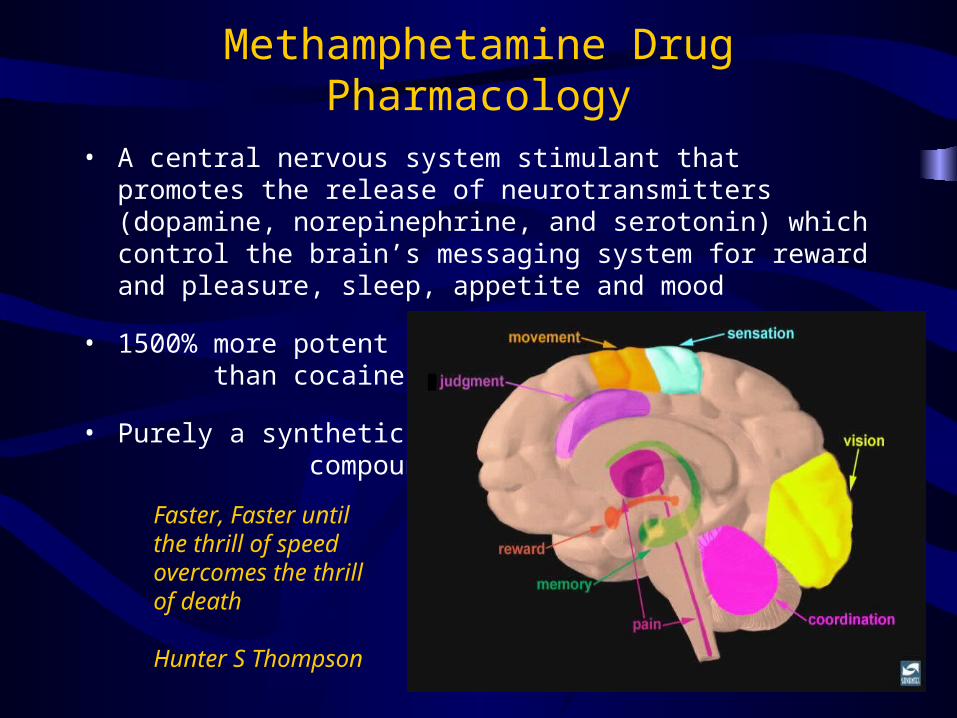
Methamphetamine Drug Pharmacology
• A central nervous system stimulant that promotes the release of neurotransmitters (dopamine, norepinephrine, and serotonin) which control the brain’s messaging system for reward and pleasure, sleep, appetite and mood
• 1500% more potentthan cocaine
• Purely a syntheticcompound
Faster, Faster untilthe thrill of speedovercomes the thrillof death
Hunter S Thompson

"Appalachian Methamphetamine Lab"Pieter Boggle VIII
Methamphetamine: Historical Aspects
Adolf Hitler
JF Kennedy

Methamphetamine: Historical Aspects
• 1887: Amphetamine synthesized in Germany
• 1919: Methamphetamine synthesized in Japan
• 1930-40: Performance enhancer in WWII
• 1930s: Treatment for nasal passage inflammation, narcolepsy,attention deficit disorder, obesity and fatigue
• 1960s: First recreational use
• 1970s: Legal production > 10 billion tablets ( ~1000X legitimatemedical use)
• 1970: Amphetamine/Methamphetamine classified as aSchedule II drug
• 1980s: Illegal street forms popularized(injected, inhaled or taken orally)

Methamphetamine Historical Aspects
• 1988: Smokable form (ice or glass) introduced from Hawaii
• Prior to 1990s: Manufacture controlled by the “White MotorcycleGangs” using phenyl-2-propanone (P2P)
• 1998: Federal Chemical Diversion and Trafficking Act placedP2P under federal control
• 2003: Ephedrine (precursor) banned in its pure form in US(increased restriction on
pseudoephedrine)
• 2004: Identification required (in many states) to purchaseover-the-counter cold medications that
contain pseudoephedrine
• Today: 90% of the Methamphetamine available in United Statestransported from Mexico

Current Methamphetamine Statistics
• The second most common illicit drug used worldwide• 35 million regular users
• 12 million Americans have tried Methamphetamine• 40% from 2000; 156% from 1996• 1.5 million regular users
• 2003 National Survey: 5% of 8th graders and 15% of 12th graders have tried Methamphetamine once in their lifetime
• > 17000 clandestine labs seized in United States in 2004 (100% from 2002 and ~ 600% from previous decade)
• Over 50 recipes extracted from Internet Search


Oregon Statistics
• Number of Methamphetamine lab seizures in Oregon increased from 67 in 1995 to 591 in 2001
• Oregon was third in the nation for number of children (241) found at Methamphetamine labs during 2001-2002
• 2001: 2750 children (> half of all foster cases) were taken from parents using or making Methamphetamine
• Between 4300 and 5350 children retrieved from Methamphetamine homes have circulated in foster homes since 2001
• 2005: 472 labs and ~ 35 Kg Methamphetamine seized in state of Oregon (7,000,000 dosage units)


Methamphetamine Addiction Statistics
• 100 people: alcoholic drink/day X 3 weeks = 8/100 addicted
• 100 people: oral or snort Methamphetamine or Cocaine daily X 3 weeks = 14/100 addicted
• 100 people: smoke or inject Methamphetamine twice = 90/100 addicted
• Methamphetamine addict that wants to quit: After 11 months of not using, 100% of recovering addicts will use Methamphetamine if offered

Methamphetamine AssociatedHospital Admissions (2002)


General Impact on Burn Centers
• Need for decontamination (treat chemical and thermal burns)
• Clandestine production (“cooking”) of Methamphetamine involves > 30 different chemicals
• Increased incidence of trauma from explosions/projectiles• Emergency medical personnel injury• Withdrawal (higher sedation/narcotic use)• Majority of patients uneducated and uninsured• Extended length of stay• Greater excision and graft failure• Increased cost of treatment
Users and Cooks
• Cooks– Adult Male– Undernourished– Paranoid ideation– Agitated, impulsive– Vague, Implausible history of injury– Big burns, lots of critical care

Legitimate Organic Chemistry Production
• Highly Educated, Sober Operator
• Safety-Designed Facility
• Personal Protective Equipment
• Process Control
• Safety Practice
• Decontamination Facility and Emergency Response Plan

Methamphetamine Production Facility
• Hotel Room, Rental Apartment, Trailer, Tent• High School Dropout• Judgment is Impaired-High on Methamphetamine,
Cannabis, etc.• Agitated, impulsive, impatient• Smoking a Cigarette• Garbage Cans, Dry Ice and Kitchen Utensils• No Ventilation, No Plexiglas Shield, No PPE

Users and Cooks
• Cooks– Adult Male– Undernourished, poor dentition– Paranoid ideation– Agitated, impulsive– Vague, Implausible history of injury– Big burns, lots of critical care

• Users– All ages– Males and Females– Uneducated– Poly-substance users– Poor social/family resources– Difficult to discharge– Erratic follow-up, rehabilitation

Burn Center behavior patterns
• Recreational User– Goes to sleep, awakens 2-3 days later
• Hard Core User/Cook– Tachycardia, Hypertension, Agitation– Weeks in duration


Methamphetamine Associated Solvents
• Absorbed after ingestion, inhalation or dermal contact
• Associated Pathologies:• Pneumonitis; Respiratory depression
• CNS depression
• Hepatotoxicity
• Renal toxicity (pyuria, hematuria, acute renal failure)
• Ventricular arrhythmias

Methamphetamine Associated Caustics (Acids and Alkalis)
• Chemical Burns: Direct contact, ingestion, inhalation
• Associated Pathologies:• Pneumonitis; Respiratory depression• CNS depression• Hepatotoxicity• Renal toxicity (pyuria, hematuria, acute renal failure)• Ventricular arrhythmias

Methamphetamine AssociatedMetals and Salts
• Multiorgan toxicity• Skin burns
• Eye and Respiratory tract irritations
• Nervous system: Headache and seizures
• Gastrointestinal irritations (nausea, vomiting, diarrhea)
• Renal
• Hematological
Methamphetamine-Associated Burn Injuries:A Retrospective Analysis
• Retrospective review of medical records (507 burn patients)• 34 patients (6.7%) identified
• Mean Age: 31.9 7.65 years; 92% male• 41% tested positive for other illicit drugs (excluding alcohol)• Mean % TBSA: 18.9 % 20.72 % (range: 1.5-90%)
70.6% flame injury; 20.6% chemical injury• Drug withdrawal: 44.1% (agitation and hypersomnolence)• Average length of stay: 15.9 19.2 days (range 0-72)• Mean cost/patient: $77,580 (range: $112-$426,386)
• 69.6% unemployed• 11.8% with third-party insurance• 44.1% uninsured without government assistance• 44.1% supplemented with Medicaid or Medicare• 96.8% of cost related to length of stay, %TBSA and total days
on ventilator
Danks, R. R., Wibbenmeyer, L.S., Faucher, L.D., et al. J Burn Care Rehabil 2004; 25: 425-429

The Methamphetamine Burn Patient
• Retrospective study• 15 (2%) Age-matched and TBSA-matched patients
• Mean Age: 30 6 years• 10 male; 5 female
• Results:• Methamphetamine patients required at least 2-3X the
calculated volume of resuscitation, irrespective of burn size• All Methamphetamine patients with 40% TBSA burn died
(estimated 60% survival without Methamphetamine)
Warner, P., Connelly, J.P., Gibran, N.S., et al. J Burn Care Rehabil 2003; 24: 275-278

Methamphetamine Laboratory Explosions: A New and Emerging Burn Injury
• Retrospective study• 15 (4%) patients: Age-matched and TBSA-matched
patients to 45 patients• Mean Age: 35.5 years (range 21-48)• Mean burn size 36% TBSA

Methamphetamine Laboratory Explosions: A New and Emerging Burn Injury
• 87% Men• 93% Caucasian• 73% unemployed• 73% uninsured• 87% no college education
Methamphetamine Laboratory Explosions: A New and Emerging Burn Injury
• Tox Screen• 100% Methamphetamine• 66% two or more drugs (opiates,
benzodiazapines, cannabis)

Methamphetamine Laboratory Explosions: A New and Emerging Burn Injury
• Results:• Methamphetamine patients required at least 1.5-2X the
calculated volume of resuscitation, irrespective of burn %• 73% with inhalation injury: Mean 33 days on ventilator (17
days for control) • Skin graft loss 33% (12.5% for control)• Higher predicted need for sedation/pain control• Longer hospital stay: Mean 30 days (21 for control)• Higher mean cost/patient: $228,732 ($74,799 for control)
Santos, A.P., Wilson, A.K. Hornung, C.A., et al. J Burn Care Rehabil 2005; 26: 228-232

The Faces of Methamphetamine

“Meth Mouth”Source: New York Times, June 11, 2005

3 years, 5 months later


“Methamphetamine: You wished it would have
killed you the first time”- unknown author