metastasising pilar tumour ofscalp - jcp.bmj.com · it is concluded that the pilar tumouris a...
TRANSCRIPT
J Clin Pathol 1986;39:757-760
Metastasising pilar tumour of scalpPA BATMAN,* HJR EVANSt
From the Departments of *Histopathology, and tSurgery, St George's Hospital Medical School, London
SUMMARY A case of pilar tumour of the scalp, treated by local excision and radiotherapy, latermetastasised to the neck. The variable histological growth patterns of the primary tumour and itsmetastases are described. It is concluded that the pilar tumour is a genuine neoplasm of the hairfollicle that is occasionally capable of malignant behaviour.
Mann et al described two cases of pilar tumours show-ing histological evidence of invasion.' Both thesecases showed a non-invasive and an invasive com-ponent, but neither had metastasised at the time ofreporting. Follow up on one of the patients, case 3 inthe report ofMann et al, is now available': Metastasesof the primary scalp tumour were excised from theposterior triangle of the neck. Paradoxically, themetastases displayed a growth pattern similar to thatinterpreted as a non-invasive component in the pri-mary tumour.
Controversy reigns as to whether the pilar tumourrepresents a hyperplastic or a neoplastic process; thisreport shows that the lesion is capable of metasta-sising, albeit only to local sites. With the possibleexception of the metastasising tumour of the scalprecorded in 1916,2 visceral metastases of pilar tumourhave not been observed.
Case history
The patient, an English woman born in 1906, had hada cyst underlying the skin of the occipital scalp formany years. For two years before its excision thelesion had slowly increased in size and had becomeinflamed. When the lesion was removed, together withsurrounding skin and subcutaneous tissue in Novem-ber 1977 it measured 1 8 x 1-3 cm and had ulceratedthe overlying epidermis. No regional lymph-adenopathy was detected at that time. Local surgerywas followed by a course of radiotherapy to the area.
In July 1981 a nodule, which had been present forthree months and which measured 1-5 cm in diameter,was excised from the subcutis of the left posteriortriangle of the neck, at least 12cm from the site of theoriginal scalp lesion. In January 1984 three furtherrecurrent nodules, the largest 2cm in diameter, wereexcised from the same area of the neck. The patient
Accepted for publication 5 March 1986
remained well and free of recurrence two years afterthis third operation.
Pathology
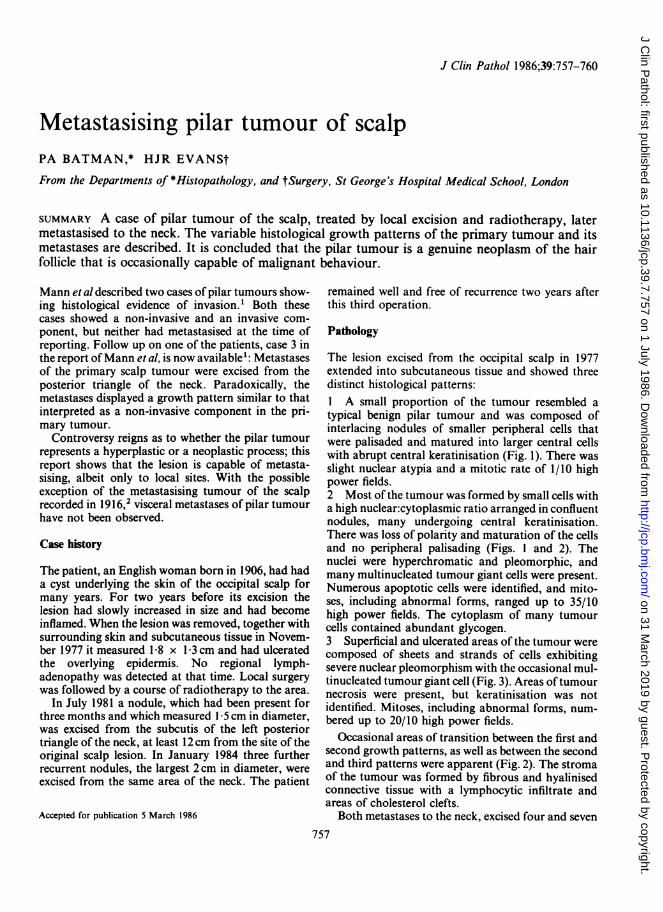
The lesion excised from the occipital scalp in 1977extended into subcutaneous tissue and showed threedistinct histological patterns:1 A small proportion of the tumour resembled atypical benign pilar tumour and was composed ofinterlacing nodules of smaller peripheral cells thatwere palisaded and matured into larger central cellswith abrupt central keratinisation (Fig. 1). There wasslight nuclear atypia and a mitotic rate of 1/10 highpower fields.2 Most of the tumour was formed by small cells witha high nuclear:cytoplasmic ratio arranged in confluentnodules, many undergoing central keratinisation.There was loss of polarity and maturation of the cellsand no peripheral palisading (Figs. 1 and 2). Thenuclei were hyperchromatic and pleomorphic, andmany multinucleated tumour giant cells were present.Numerous apoptotic cells were identified, and mito-ses, including abnormal forms, ranged up to 35/10high power fields. The cytoplasm of many tumourcells contained abundant glycogen.3 Superficial and ulcerated areas of the tumour werecomposed of sheets and strands of cells exhibitingsevere nuclear pleomorphism with the occasional mul-tinucleated tumour giant cell (Fig. 3). Areas oftumournecrosis were present, but keratinisation was notidentified. Mitoses, including abnormal forms, num-bered up to 20/10 high power fields.
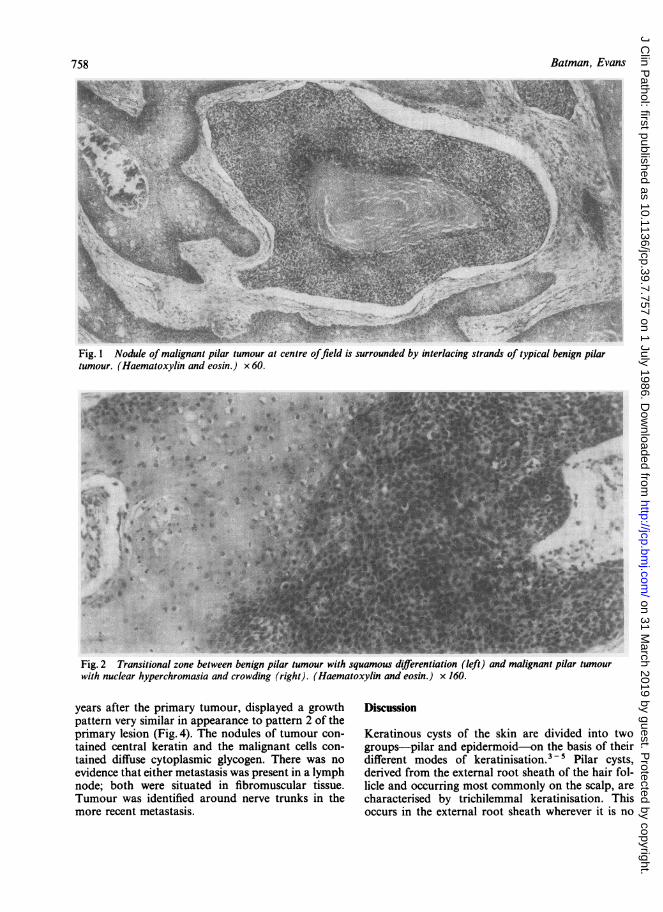
Occasional areas of transition between the first andsecond growth patterns, as well as between the secondand third patterns were apparent (Fig. 2). The stromaof the tumour was formed by fibrous and hyalinisedconnective tissue with a lymphocytic infiltrate andareas of cholesterol clefts.
Both metastases to the neck, excised four and seven757
on 31 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.7.757 on 1 July 1986. Dow
nloaded from
Batman, Evans
Fig. 1 Nodule ofmalignant pilar tumour at centre offield is surrounded by interlacing strands of typical benign pilartumour. (Haematoxylin and eosin.) x 60.
Fig. 2 Transitional zone between benign pilar tumour with squamous differentiation (left) and malignant pilar tumourwith nuclear hyperchromasia and crowding (right). (Haematoxylin and eosin.) x 160.
years after the primary tumour, displayed a growth Discussionpattern very similar in appearance to pattern 2 of theprimary lesion (Fig. 4). The nodules of tumour con- Keratinous cysts of the skin are divided into twotained central keratin and the malignant cells con- groups-pilar and epidermoid-on the basis of theirtained diffuse cytoplasmic glycogen. There was no different modes of keratinisation.3 5 Pilar cysts,evidence that either metastasis was present in a lymph derived from the external root sheath of the hair fol-node; both were situated in fibromuscular tissue. licle and occurring most commonly on the scalp, areTumour was identified around nerve trunks in the characterised by trichilemmal keratinisation. Thismore recent metastasis. occurs in the external root sheath wherever it is no
758
on 31 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.7.757 on 1 July 1986. Dow
nloaded from

Metastasising pilar tumour of scalp
'.K:A.+p VX
*41W
:. wf
il.,"WtX F
Fig. 3 Undifferentiated pilar tumour showing markednuclear pleomorphism. (Haematoxylin and eosin) x 400.
AA
Fig. 4 Metastatic pilar tumour similar in appearance tomalignant areas of pilar tumour in Fig 1 (Haematoxylinand eosin) x SO.
longer covered by the internal root sheath and differsfrom epidermal keratinisation by increase in size ofthe keratinocytes, with loss of their nuclei and abrupttransition into dense keratin without an intermediatekeratohyaline layer.`8
Small foci of intraluminal budding are observed
759
quite commonly in the wall of pilar cysts. Sometimesproliferating epithelium replaces most if not all of thepre-existing wall of the cysts.9 The stimulusresponsible for this process and its biological naturehave been disputed. Factors that may induce prolif-eration are thought to include trauma,'0 infection,and irritation from the contents of the cyst.3 11 12 Forthis reason the pilar tumour is usually regarded as apseudoepitheliomatous hyperplasia rather than as aneoplasm. Mann etal' argued that it represented agenuine neoplasm.The histological features of a pilar tumour are dis-
tinctive. The lesion is composed of interlacing nodulesof squamous epithelium that are sharply separatedfrom the surrounding tissue and undergo abrupt tri-chilemmal keratinisation into amorphous and focallycalcified keratin in their centre.' The usual lack ofcytological atypia and stromal invasion distinguishthe tumour from a squamous cell carcinoma9 forwhich it is often mistaken clinically. ° Many pilartumours contain epithelial pearls and isolated dys-keratotic cells, findings that may arouse suspicion ofan erroneous diagnosis of malignancy.6 Areas of epi-dermal keratinisation, forming laminated keratin withan intermediate keratohyaline layer, suggestdifferentiation of the tumour towards epithelium ofthe follicular infundibulum. Other areas of thetumour may resemble the lower part of the follicularouter root sheath, forming glycogenated clear cells,squamous eddies, a palisaded arrangement of basalcells at the periphery of nodules, and an investingthick hyalinised zone of collagen.9
It is accepted that pilar tumours, which show nocytological atypia, are capable of eroding bone and ofrecurring after inadequate excision.' 12 -15 Exam-ination of the earlier reports describing cases of squa-mous cell carcinoma arising in so called "sebaceouscysts" reported before Wilson-Jones's recognition ofthe proliferating pilar cyst as a separate entity,'2shows a poorly documented assortment of cysticlesions.i6 Many of these lesions may have been pilartumours, as judged by their benign course, includingrare occurrence of metastases. l7 - 1 9More recent descriptions of malignant change in
pilar tumours conform to two patterns-namely, cir-cumscribed nodules of cytologically malignant squa-mous epithelium, suggesting dedifferentiation withinnodules of the pilar tumour (growth pattern 2 in ourcase), and diffuse spindle cell growth of malignantcells adjacent to tumour nodules and infiltrating sur-rounding stroma (growth pattern 3 in ourcase).i 13 14 16 20 Regional metastases from pilartumours have been documented pathologically inthree patients to date, including the present case.'4 21Metastases of spindle cell squamous carcinomas aris-ing in other organs of the body may contain only the
i.I *I 1.1"
iO, ,4..,..I
i
on 31 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.7.757 on 1 July 1986. Dow
nloaded from

760
squamoid component of the tumour.2022 An analogymay be made between the behaviour of these tumoursand maligant pilar tumours of the scalp, in that thereported metastases of the latter have all seemed toreproduce the histological appearance of the nodularprimary lesion, while metastases resembling theapparently less differentiated infiltrative componenthave not so far been described.The case reported here documents unequivocal
regional metastases from a clearly malignant tri-chilemmal tumour. The possibility of such malignantbehaviour has not met with general acceptance.Therefore, the much more common benign analogueshould be regarded as a trichilemmoma, and thereseems little point in retaining the term "proliferatingtrichilemmal cyst" for this entity. Distant metastasisor death attributable to these tumours have not yetbeen confirmed.
We thank Professor E Wilson-Jones for his advice, MrJA Gillespie for permission to publish this case report,Mrs P McKinnon for secretarial help, and Mr D Haw-tin for photographic help.
References
Mann B, Salm R, Azzopardi JG. Pilar tumour: a distinctive type oftrichilemmoma. Diagn Histopathol 1982;5:157-67.
2Seff I, Berkowitz S. Carcinomatous degeneration of sebaceouscysts. Surg Gynecol Obstet 1916;33:469-73.
3Pinkus H, Mehregan AH. A guide to dermatohistopathology. 3rdEd. New York: Appleton-Century-Crofts, 1981.
4Kligman AM. The myth of the sebaceous cyst. Arch Dermatol1964;89:253-6.
5McGavran MH, Binnington B. Keratinous cysts of the skin. ArchDermatol 1966;94:499-508.
Batman, Evans
6Lever WF, Schaumburg-Lever G. Histopathology of the skin. 6thEd. JB Lippincott Company, 1983.
7Pinkus H. "Sebaceous cysts" are trichilemmal cysts. Arch Dermatol1969;99:544-55.
8Kimura S. Trichilemmal cysts: ultrastructural similarities to thetrichilemmal sac. Dermatologica 1978;157:164-70.
9Brownstein MH, Arluk DJ. Proliferating trichilemmal cyst: a simu-lant of squamous cell carcinoma. Cancer 1981;48:1207-14.
'°Headington JT. Tumors of the hair follicle: a review. Am J Pathol1976;85:480-505.
lLeppard BJ, Sanderson KV. The natural history of trichilemmalcysts. Br J Dermatol 1976;94:379-90.
Wilson-Jones E. Proliferating epidermoid cysts. Arch Dermatol1966;94:1 1-19.
13Baptista AP, Silva LGE, Born MC. Proliferating trichilemmal cyst.J Cutan Pathol 1983;10:178-87.
14 Holmes EJ. Tumours of lower hair sheath: common histogenesis ofcertain so-called "sebaceous cysts", acanthomas and "sebaceouscarcinomas". Cancer 1968;21:234-48.
Dabska M. Giant hair matrix tumour. Cancer 1971;28:701-6.Reed RJ, Lamar LM. Invasive hair matrix tumors of the scalp.Arch Dermatol 1966;94:310-16.
'7Peden JC. Carcinoma developing in sebaceous cysts. Ann Surg1948;128:1 136-47.
Collins DC. Carcinoma originating in sebaceous cysts. Can MedAssoc J 1936;35:370-2.
"Bishop EL. Epidermoid carcinoma in sebaceous cysts. Ann Surg1931;93:109-12.
20 Wamer TFCS. Proliferating pilar cyst with spindle cell component.J Cutan Pathol 1979;6:310-16.
21Saida T, Oohara K, Hori Y, Tsuchiya S. Development of a malig-nant proliferating trichilemmal cyst in a patient with multipletrichilemmal cysts. Dermatologica 1983;166:203-8.
22Martin MR, Kahn LB. So-called pseudosarcoma of the esophagus.Arch Pathol Lab Med 1977;101:604-9.
Requests for reprints to: Dr PA Batman, Department ofHistopathology, St George's Hospital Medical School,Cranmer Terrace, Tooting, London SW17 ORE, England.
on 31 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.7.757 on 1 July 1986. Dow
nloaded from