metabolism in surgery
TRANSCRIPT

7/28/2019 Metabolism in Surgery
http://slidepdf.com/reader/full/metabolism-in-surgery 1/5
Energy Metabolism and Normal Nutritional Requirements
FERNANDO L. LOPEZ, MD, FPCS
Professor of Surgery
UST Department of Surgery
Compiled and edited by Arvin 09-01-08
OBJECTIVES
To review normal protein, carbohydrate and lipid
metabolism
To understand the mechanisms that regulatesubstrate utilization and energy production
To demonstrate methods for calculating nutritional
requirements
NUTRIENTS
Protein 4 kcal / g
Carbohydrates
o enteral 4 kcal / g
o parenteral 3.4 kcal / g
Lipids 9 kcal / g
Water
Vitaminso Water soluble
o Fat soluble
Minerals
o Electrolytes
o Trace elements and ultra trace minerals
Amino Acids
• NON-ESSENTIAL
− Isoleucine − Alanine
− Phenylalanine
− Methionine− Histidine
− Tryptophan
− Tyrosine
− Aspartic Acid
− Glutamic Acid
− Cysteine
− Glycine
− Serine
− Proline
• CONDITIONALLY
ESSENTIAL
− Glutamine
− Arginine
• ESSENTIAL
− Leucine
− Lysine
− Valine
− Threonine
Chemical Structure of an Amino Acid
NITROGEN BALANCE
NB = IN – (UN + RNL)
NB: Nitrogen Balance
IN: Ingested Nitrogen
UN: 24-Hour Urine Nitrogen
RNL: Remaining Nitrogen Loss (3.1 g/d)
Respiratory Quotient (RQ)
RQ: Respiratory Quotient
VCO2: CO2 Produced
VO2: Oxygen Consumed
RQ
• Glucose oxidation
1 glucose + 6 O2 = 6 CO2 + 6 H20
6/6 = 1.0
• Fat oxidation
1 palmitate + 23 O2 = 16 CO2 + 16 H2O
16/23 = 0.7
• Protein oxidation
1 amino acid + 5.1 O2 = 4.1 O2 + 2.8 H2O
4.1/5.1 = 0.8
• Lipogenesis > 1.0 – 8.0
Nutrient Utilization
• Regulation
– Nutrient availability
– Hormonal environment
– Inflammatory state

7/28/2019 Metabolism in Surgery
http://slidepdf.com/reader/full/metabolism-in-surgery 2/5
Energy Substrate Utilization
Fasting state:
o Depends on nutrient availability
In stress:
o Depends on hormonal environment and
inflammatory response
Body Composition
Weight (kg) 70 60 Weight (kg) 70 60
Total Water (L) 42 31 Fat (kg) 12.5 17
Intracellular 28 19 BCM
Extracellular 14 12 Protein (kg) 12.5 9
Total Solids (kg) 28 28.8 Minerals (kg) 3 3
MALNUTRITION
In malnutrition, energy expenditure must be calculated
based on actual body weight.
OBESITY
In obesity, energy expenditure must be calculated on ideal
weight.
Calculating Basal Energy Expenditure
Harris-Benedict Equation
o Variables
gender, weight (kg), height (cm),
age (years)
Men:
66.47 + (13.75 x weight) + (5 x height) – (6.76 x age)Women:
655.1 + (9.56 x weight) + (1.85 x height) – (4.67 x age)
Calorie requirement = BEE x activity factor x stress factor
Calorie Calculation
“Rule of Thumb”
Calorie requirement = 25 to 30 kcal/kg/day
METABOLIC RESPONSE TO STARVATION AND TRAUMA:
NUTRITIONAL REQUIREMENTS
Objectives
Explain the differences between metabolic
responses to starvation and trauma
Explain the effect of trauma on metabolic rate and
substrate utilization
Determine calorie and protein requirements during
metabolic stress
Metabolic Reaction to Starvation
Hormone Source Change in
Secretion
Norepinephrine Sympathetic Nervous
System
↓ ↓ ↓
Norepinephrine Adrenal Gland ↑
Epinephrine Adrenal Gland ↑
Thyroid Hormone
T4
Thyroid Gland
(changes to
T3 peripherally)
↓ ↓ ↓
Energy Expenditure in Starvation
Metabolic Response to Trauma
METABOLIC RESPONSE TO TRAUMA: EBB PHASE
Characterized by hypovolemic shock
Priority is to maintain life/homeostasis
o ↓ Cardiac output
o ↓Oxygen consumption
o ↓ Blood pressure
o ↓ Tissue perfusion
o ↓ Body temperature
o ↓ Metabolic rate
METABOLIC RESPONSE TO TRAUMA: FLOW PHASE
↑ Catecholamines ↑ Glucocorticoids
↑ Glucagon
Release of cytokines, lipid mediators
Acute phase protein production
Metabolic Response to Trauma
7/28/2019 Metabolism in Surgery
http://slidepdf.com/reader/full/metabolism-in-surgery 3/5
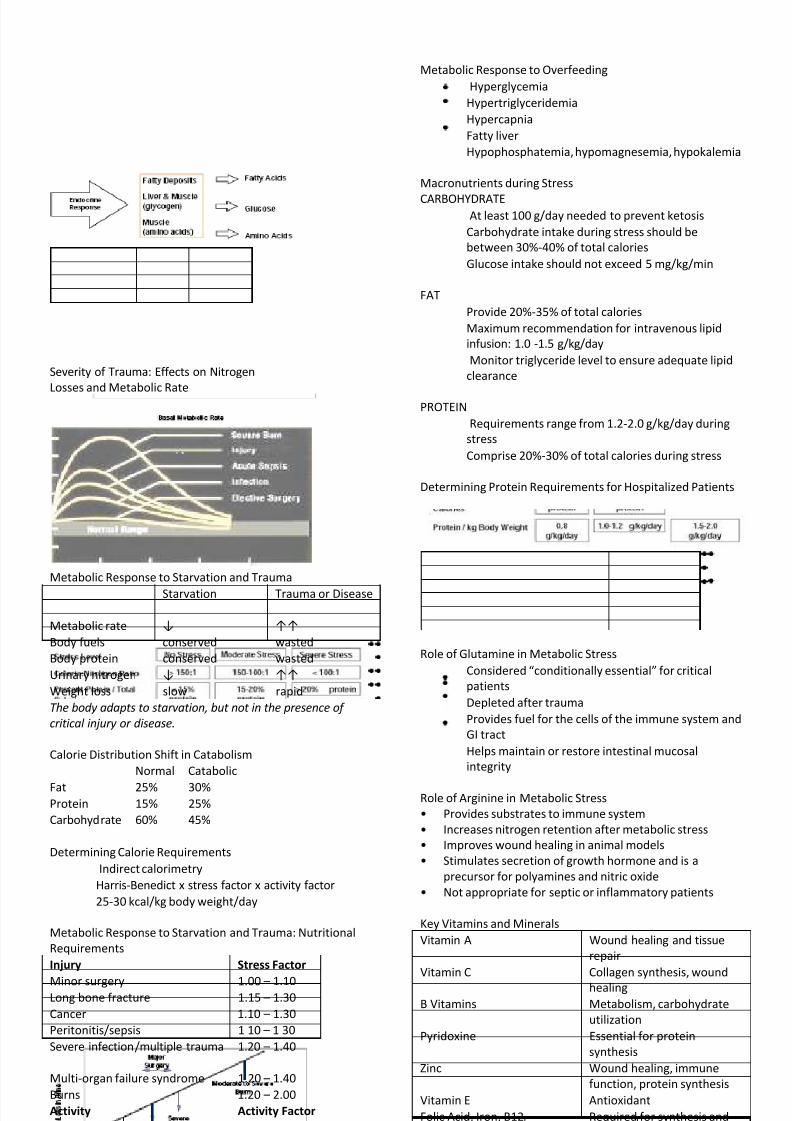
Severity of Trauma: Effects on Nitrogen
Losses and Metabolic Rate
Metabolic Response to Starvation and Trauma
Starvation Trauma or Disease
Metabolic rate ↓ ↑↑
Body fuels conserved wasted
Body protein conserved wasted
Urinary nitrogen ↓ ↑↑
Weight loss slow rapid
The body adapts to starvation, but not in the presence of
critical injury or disease.
Calorie Distribution Shift in Catabolism
Normal Catabolic
Fat 25% 30%Protein 15% 25%
Carbohydrate 60% 45%
Determining Calorie Requirements
Indirect calorimetry
Harris-Benedict x stress factor x activity factor
25-30 kcal/kg body weight/day
Metabolic Response to Starvation and Trauma: Nutritional
Requirements
Injury Stress Factor
Minor surgery 1.00 – 1.10Long bone fracture 1.15 – 1.30
Cancer 1.10 – 1.30
Peritonitis/sepsis 1 10 – 1 30
Severe infection/multiple trauma 1.20 – 1.40
Multi-organ failure syndrome 1.20 – 1.40
Burns 1.20 – 2.00
Activity Activity Factor
Confined to bed 1.2
Out of bed 1.3
Metabolic Response to Overfeeding
Hyperglycemia
Hypertriglyceridemia
Hypercapnia
Fatty liver
Hypophosphatemia, hypomagnesemia, hypokalemia
Macronutrients during Stress
CARBOHYDRATEAt least 100 g/day needed to prevent ketosis
Carbohydrate intake during stress should be
between 30%-40% of total calories
Glucose intake should not exceed 5 mg/kg/min
FAT
Provide 20%-35% of total calories
Maximum recommendation for intravenous lipid
infusion: 1.0 -1.5 g/kg/day
Monitor triglyceride level to ensure adequate lipid
clearance
PROTEIN
Requirements range from 1.2-2.0 g/kg/day during
stress
Comprise 20%-30% of total calories during stress
Determining Protein Requirements for Hospitalized Patients
Role of Glutamine in Metabolic Stress
Considered “conditionally essential” for critical
patients
Depleted after trauma
Provides fuel for the cells of the immune system and
GI tract
Helps maintain or restore intestinal mucosal
integrity
Role of Arginine in Metabolic Stress
• Provides substrates to immune system
• Increases nitrogen retention after metabolic stress
• Improves wound healing in animal models
• Stimulates secretion of growth hormone and is a
precursor for polyamines and nitric oxide
• Not appropriate for septic or inflammatory patients
Key Vitamins and Minerals
Vitamin A Wound healing and tissue
repair
Vitamin C Collagen synthesis, wound
healing
B Vitamins Metabolism, carbohydrate
utilization
Pyridoxine Essential for protein
synthesis
Zinc Wound healing, immune
function, protein synthesis
Vitamin E Antioxidant
Folic Acid, Iron, B12 Required for synthesis and
replacement of red blood
cells
7/28/2019 Metabolism in Surgery
http://slidepdf.com/reader/full/metabolism-in-surgery 4/5
Nutritional Assessment
Medical history
Physical examination
Biochemical markers
Anthropometric measures
Tools for Nutritional Evaluation
Malnutrition Screening Tool (MST)1
Malnutrition Universal Screening Tool (MUST)2
DETERMINE for screening and assessment3
Subjective Global Assessment (SGA)4
Patient-Generated SGA (PG-SGA)5
Mini Nutritional Assessment (MNA)6
Nutritional Risk Index (NRI)7
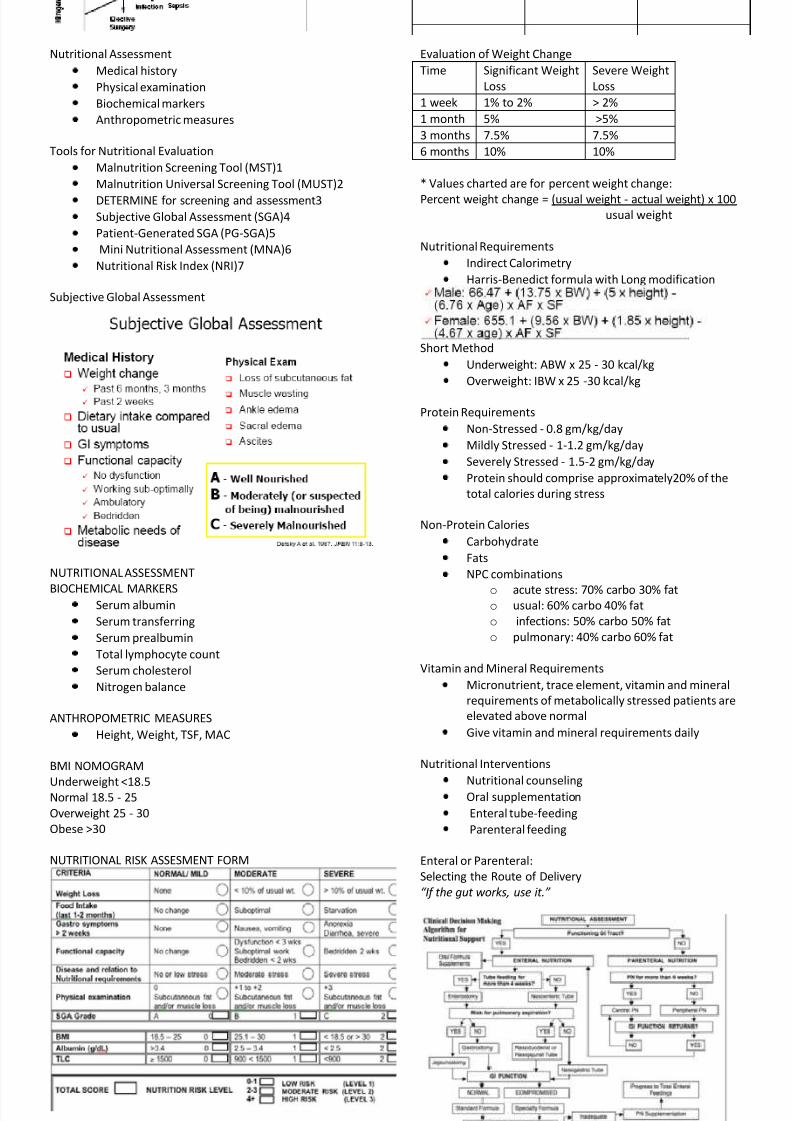
Subjective Global Assessment
NUTRITIONAL ASSESSMENT
BIOCHEMICAL MARKERSSerum albumin
Serum transferring
Serum prealbumin
Total lymphocyte count
Serum cholesterol
Nitrogen balance
ANTHROPOMETRIC MEASURES
Height, Weight, TSF, MAC
BMI NOMOGRAM
Underweight <18.5Normal 18.5 - 25
Overweight 25 - 30
Obese >30
NUTRITIONAL RISK ASSESMENT FORM
Evaluation of Weight Change
Time Significant Weight
Loss
Severe Weight
Loss
1 week 1% to 2% > 2%
1 month 5% >5%
3 months 7.5% 7.5%
6 months 10% 10%
* Values charted are for percent weight change:
Percent weight change = (usual weight - actual weight) x 100usual weight
Nutritional Requirements
Indirect Calorimetry
Harris-Benedict formula with Long modification
Short Method
Underweight: ABW x 25 - 30 kcal/kg
Overweight: IBW x 25 -30 kcal/kg
Protein Requirements
Non-Stressed - 0.8 gm/kg/day
Mildly Stressed - 1-1.2 gm/kg/day
Severely Stressed - 1.5-2 gm/kg/day
Protein should comprise approximately20% of the
total calories during stress
Non-Protein Calories
Carbohydrate
Fats
NPC combinations
o acute stress: 70% carbo 30% fato usual: 60% carbo 40% fat
o infections: 50% carbo 50% fat
o pulmonary: 40% carbo 60% fat
Vitamin and Mineral Requirements
Micronutrient, trace element, vitamin and mineral
requirements of metabolically stressed patients are
elevated above normal
Give vitamin and mineral requirements daily
Nutritional Interventions
Nutritional counselingOral supplementation
Enteral tube-feeding
Parenteral feeding
Enteral or Parenteral:
Selecting the Route of Delivery
“If the gut works, use it.”

7/28/2019 Metabolism in Surgery
http://slidepdf.com/reader/full/metabolism-in-surgery 5/5
The rationale for early EN
Use of the gut stimulates GALT & MALT resulting in
enhanced immune response
Early feeding can trigger gut immunity and thereby
improve outcomes
Delay or failure may promote a proinflammatory
state with disease severity & morbidity
Enteral Formulas: Categories
Polymeric formulaso Commercial
o Blenderized
Oligomeric formulas
Disease-specific formulas
Modular formulas (concentrated protein and
carbohydrate preparations)
Polymeric Formulas
Contain intact macronutrients and require digestion:
o Intact proteins
o Polysaccharides
o Disaccharideso Polyunsaturated fatty acids (PUFA)
o Medium-chain triglycerides (MCT)
o Vitamins and minerals
Oligomeric Formulas
Hydrolyzed macronutrients facilitate digestion and
absorption
Components Glucose polymers
Amino acids
– Glutamine
– Arginine
Peptides
Monosaccharides
Disaccharides
Polyunsaturated fatty acids
Medium-chain triglycerides
Vitamins and minerals
Also called “elemental,” “semi-elemental,”
“All in One” Parenteral Formulas
Optimal utilisation of calories
Minimizes metabolic complications
o reduced volume load
o reduced CO2 production
o avoidance of hyperglycaemia
o less fat synthesis
Permits peripheral administration
Access for Parenteral Nutrition
Central PN
Percutaneous
Subclavian / Jugular
Femoral
PIC line
Cutdown
Basilic vein
External jugular
Aseptic technique required at
all times
Peripheral PN
Any peripheral vein
Aseptic technique
required at all times
Best removed after 48 –
72 hrs
Take home message (1)
ROUTINE SCREENING
Assessment of risk for nutrition related
complications
High index of suspicion
Consider nature of illness and over-all condition of
patient in the context of a second insult
ACCURATE ASSESSMENT
Accurate calculation of calorie & protein
requirements
Strict monitoring of actual feed delivery is more
effective than overestimation of patient
requirements
Overfeeding may be more harmful than
underfeeding !
ROUTE OF DELIVERY
Early & preferential use of EN, combined with PN
whenever necessaryMONITORING IMPLEMENTATION
Pre-op: Monitor actual intake as an index of success
Post-op: Monitor clinical parameters
DOCUMENT THE ENTIRE PROCESS !
What is our measure of success?
Surgical nutrition will become an established routine
in patient care
Surgical nutrition will become systematic and
organized w/ multidisciplinary participation
Patient outcomes will improve
The objective proof will be DOCUMENTATION
-arvin 09-01-08