memorialcare: health system-level accountability for...
TRANSCRIPT
MemorialCare: Health System-Level Accountability for the Triple AimRegina Berman, VP, Population Health & Accountable Care
Helen Macfie, Chief Transformation Officer
C17, IHI Forum, December, 2017

Session GoalsPresenters have no conflicts to disclose
Focus: Creating a portfolio of population health initiatives across multiple payors and settings to pursue Triple Aim results.
Keys:• Macro and micro systems to successfully
deliver on ACOs and Bundled Payment• Drivers and learnings from five ACOs+
1. Galvanizing leadership2. Creating a strategic roadmap – & case study3. Advancing our overall “system of care”4. Innovating to improve care, quality & safety5. Governance6. Outcomes & 360 ROI thinking7. Where to next and questions

1 Galvanizing Leadership

About MemorialCare
Total Assets $3.3 billion– Annual Revenues $2.3 billion– Bond Rating AA- stable
Hospitals– Patient Discharges 67,000– Patient Days 317,000– ER Visits 214,000– Babies delivered 10,500– Surgeries – IP/OP 31,700
Ambulatory Access– “At Risk” Lives/ACOs 260,000– Seaside Health Plan 40,300– Medical Group Visits 600,000– Ambulatory Surgeries 57,000
Workforce– Employees 11,000– Affiliated Physicians 2,600– Employed Physicians 230

What made us go down this path?
STRATEGIC AIMRight thing to do
Shifting from Hospital-Based to Integrated System of Care
Strategic differentiator
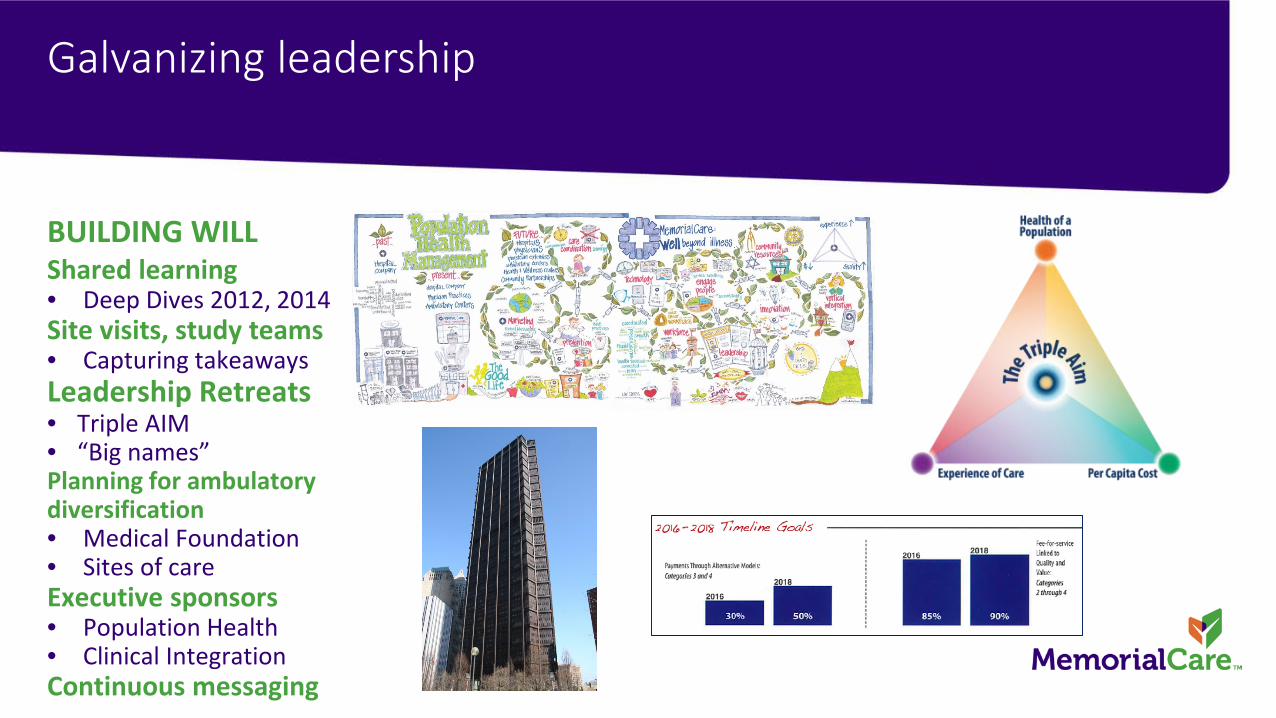
Galvanizing leadership
BUILDING WILLShared learning• Deep Dives 2012, 2014Site visits, study teams• Capturing takeawaysLeadership Retreats• Triple AIM• “Big names”Planning for ambulatory diversification• Medical Foundation• Sites of careExecutive sponsors• Population Health• Clinical IntegrationContinuous messaging

2 Creating a Strategic Roadmap
Artistically speaking…

Strategic focus and evolution

Changing the mixPortfolio diversification
INTEGRATING DELIVERYMedical Group and IPA• 25 years of successful HMO experience• Now 914,000 active patients• Primary care chassis and specialist network• Partnerships – UC Irvine Health, Cedars Sinai, ACO partners
Ambulatory Services• Revenue diversification & strategic partnerships• Joint venture (ASCs, Imaging, Dialysis)And…ACOs R Us• 92,150 ACO lives• 260,000 total “at risk lives”, plus 50K in Health Plan and Vivity• Bold Goal 500K by 2021

Committing to risk-taking and the Triple Aim
ACO or At Risk Attribution and Key Descriptors
CMMINext Gen ACO

Boeing

What Employers Want
“If providers can’t give us lower cost, better outcomes and better quality, we don’t want to waste our time; we can get the current value anywhere.”
David Lansky, CEOPacific Business Group on Health
$VALUE = QUALITY
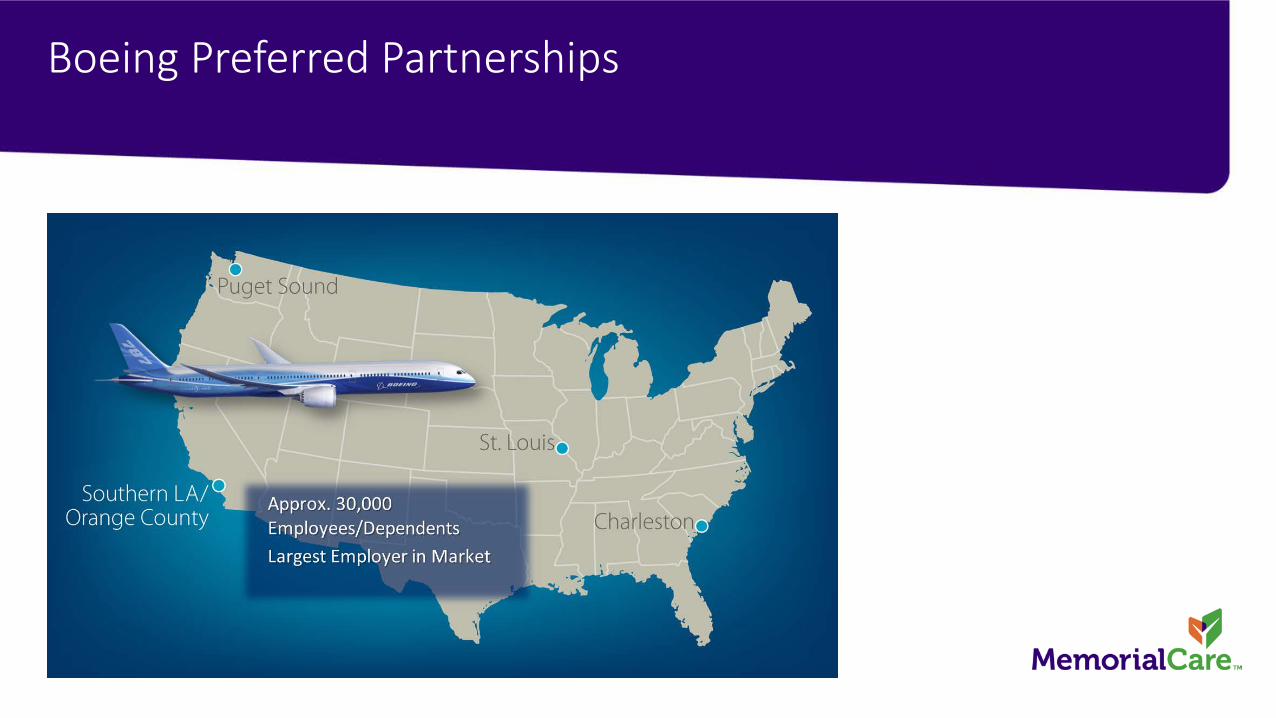
Boeing Preferred Partnerships

Rigorous RFP Process
ALL HANDS ON DECKDriven by MercerShort time frameRequirements

Boeing Selection CriteriaExquisite care and service
Network• Quality• Access Culture• Physician leadership• Readiness for change, collaborativeFinancial• Willingness to invest, take riskInfrastructure• Ability to support transformation• Strong provider management• Technology, systems

PROGRAM DESIGN• Mixed PPO Model
• Designated – Employee elects program during annual enrollment• Attributed – majority of care is delivered at ACO partner
• ACO network is ‘In-Network’• PCP encouraged, not required
Financial Incentives for Employees• Lower employee premiums• Higher company funded HSA• No cost PCP office visit• No cost generic drugs
HDHP
PPO
HMOs
HDHP
PPO
HDHP
PPO
HMO
ACO
2016 2017
Boeing ACO Plan Structure

Network Development & Partnerships

Overview
BOEING’s EXPECTATIONSCost Reduction• Key levers: care coordination, setting of care - freestanding, pharmacy spend
Population Health• Key levers: 3D care model, intensive outpatient & clinics, key quality measures
Patient Experience• Ease and access to EHR, appointments, triage, referrals (24/7 Nurse Advice and Rx
Refills, home visit, telemedicine)
• Dedicated microsite

Financial Terms
KEYS TO MODEL• Providers paid at existing PPO rates by Blue Cross Blue Shield of Illinois• ACO guarantees a reduction in Total Cost of Care for each Performance Year• Savings (or losses) are shared• Savings (or losses) are adjusted for hitting Quality, Patient Experience, and
Access benchmarks
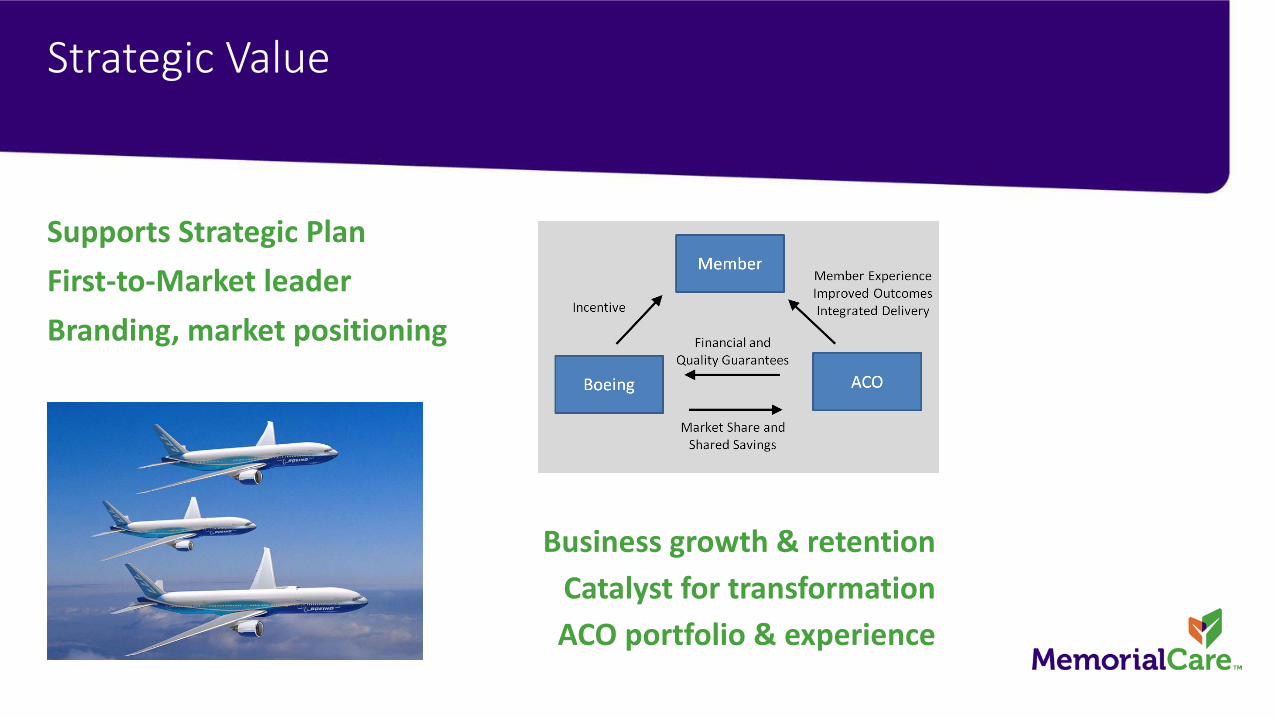
Strategic Value
Supports Strategic PlanFirst-to-Market leaderBranding, market positioning
Business growth & retentionCatalyst for transformationACO portfolio & experience
3 Advancing our Overall System of Care

The larger opportunity
Source: RTI/Cain Brothers Analysis, “Integrating Acute and Post-Acute Care”, 2012
LTCH
IRF
SNF
HHA
OPT Th.

• Patient centered primary and specialty care
• Access based on patient needs (i.e. telehealth; same-day visits; e-visits)
• Special care coordination and chronic care management programs
• Patient Activation assessment
Seco
ndar
ydr
iver
sPrimary drivers
Objectives MemorialCare ACODriver Diagram
Beneficiary Experience and
Engagement
Provider Support and Engagement
InformationTechnology and Analytics
Care Delivery and Management
Act
iviti
es a
nd e
lem
ents
• Provider and Staff Education
• Reminders at the point of care in chart
• Incentives based on achievement of quality metrics
• Disease Registries• Beneficiary
Identification at the point of care
• Identification of Gaps in Care
• Data and Analytics Capability
• Effective Cost Analysis
• Predictive Modeling and Risk Stratification
• Physician/ Provider Care Teams
• Care Coordination• Transitions of Care• Discharge Planning • Medication
Reconciliation• Advanced Care
Planning• Advanced Care
Planning & Palliative Care
Improve the health of beneficiariesImprove their experience of care – quality, access,
and service; and reduce per capita costs
Ensure members receive the right care, at the right time, through advanced care
coordination and patient support services
Support providers to ensure quality; positive health outcomes; and efficient resource use through advanced technology and tools

Evolving the “3D Care Model”Resourcing the plan
Meet the ACO Team
Building a Core TeamManagement TeamProject ManagersCommunity Based TeamAnalystMid-Levels (home visits)Case ManagersCare CoordinatorsSocial Work Services
Leveraging the InfrastructureNetwork Management
ContractingQualityPharmacy
Imbedded Hospital Case Manager
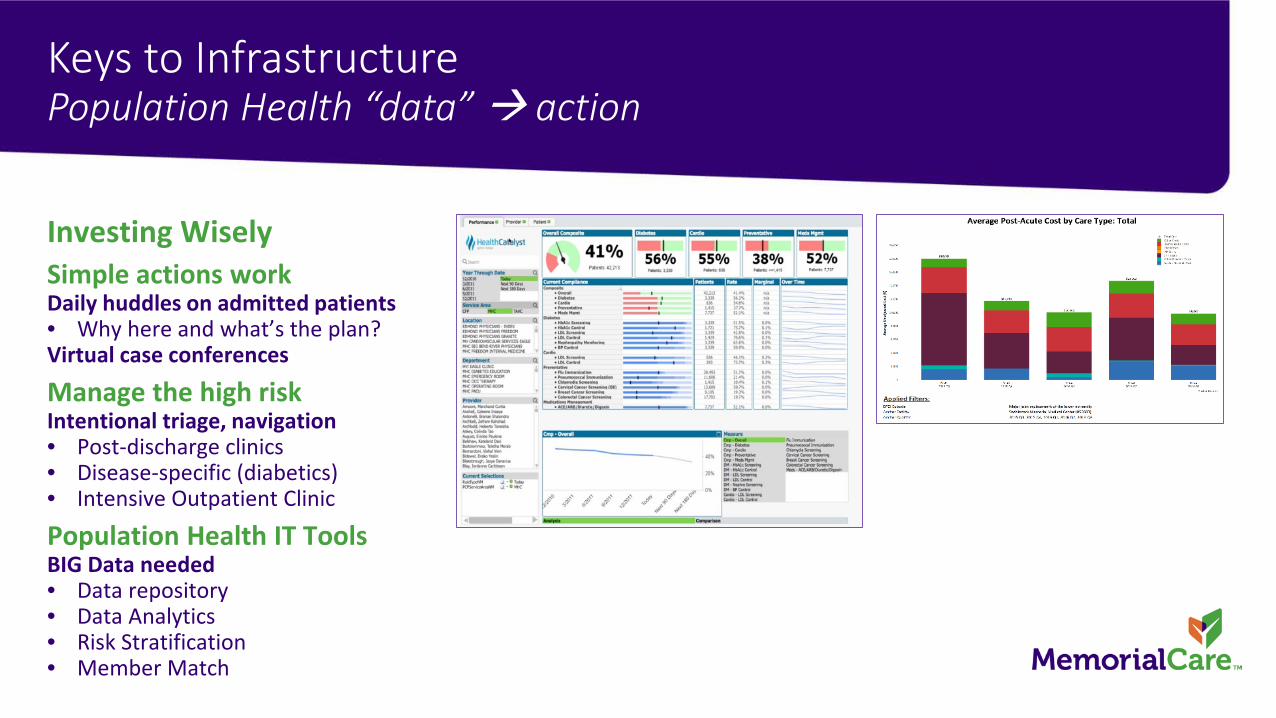
Keys to InfrastructurePopulation Health “data” action
Investing WiselySimple actions workDaily huddles on admitted patients• Why here and what’s the plan?Virtual case conferences
Manage the high riskIntentional triage, navigation• Post-discharge clinics• Disease-specific (diabetics)• Intensive Outpatient Clinic
Population Health IT Tools BIG Data needed• Data repository• Data Analytics• Risk Stratification• Member Match

Ex: Risk Stratification
**No PHI used—not a real patient

Ex: Enhancing Point of Service Visibility across the continuum
4 Innovating to improve Care, Quality & Safety –Filling in the Cracks
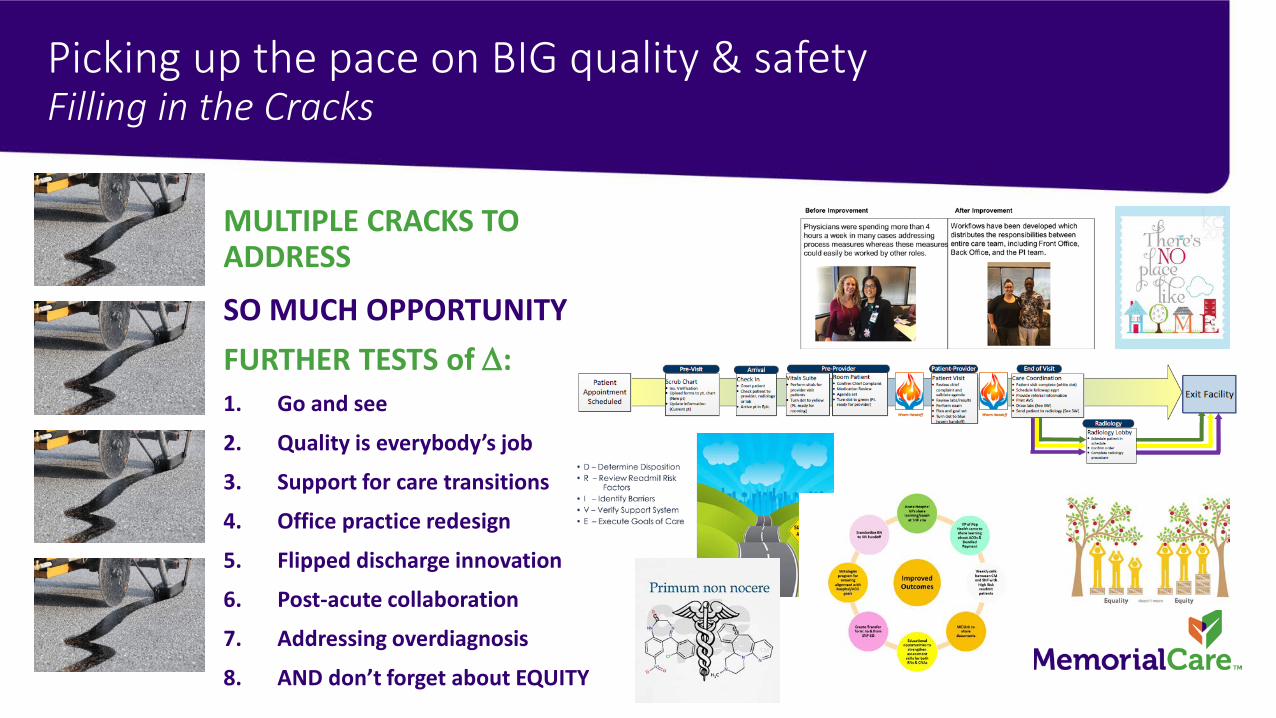
Picking up the pace on BIG quality & safetyFilling in the Cracks
MULTIPLE CRACKS TO ADDRESS
SO MUCH OPPORTUNITYFURTHER TESTS of ∆:1. Go and see
2. Quality is everybody’s job
3. Support for care transitions
4. Office practice redesign
5. Flipped discharge innovation
6. Post-acute collaboration
7. Addressing overdiagnosis
8. AND don’t forget about EQUITY

PDSA #1: Before data, “go and see”
Go to GembaEngage Lean Thinking – horizontal and vertical at point of serviceBPCI Case Study: 9 pools, 9 ways, 4 phases• Preadmit/admit phase
• Operative/recovery phase
• Post-operative phase
• Discharge & transitional care
Care and flow redesign opportunities abound everywhere!• With opportunity to prioritize…
Sponsor check-in points
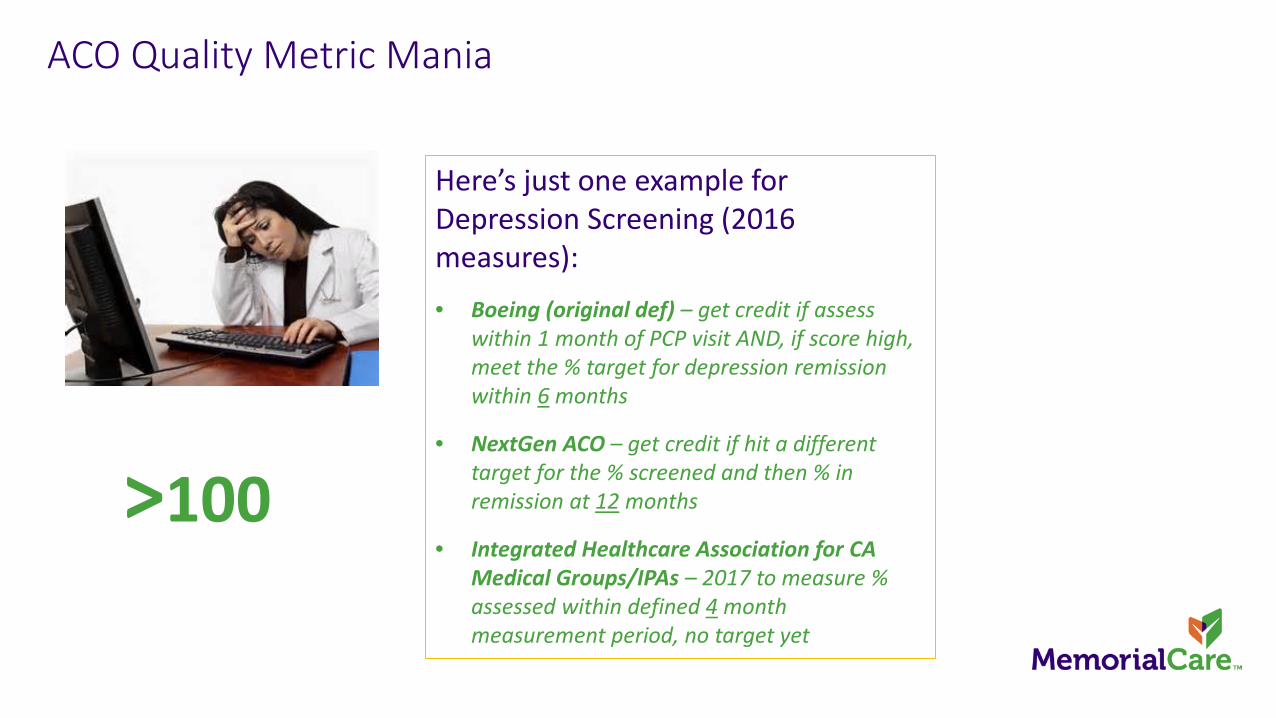
ACO Quality Metric Mania
Here’s just one example for Depression Screening (2016 measures):• Boeing (original def) – get credit if assess
within 1 month of PCP visit AND, if score high, meet the % target for depression remission within 6 months
• NextGen ACO – get credit if hit a different target for the % screened and then % in remission at 12 months
• Integrated Healthcare Association for CA Medical Groups/IPAs – 2017 to measure % assessed within defined 4 month measurement period, no target yet
>100

PDSA #2: Quality, Its Everyone’s JobEvolving the care team – addressing quality metric mania
LEVERAGING LEAN & ADVOCACYGoing offline to make a difference, needs supportNon-value-added “waste”Building in safetyHarnessing best ideasTests of change by MondayCreating standard workTools and tip sheetsRedesigning roles• Doctors, nurses, MAs, front officeBuilding into visibilityHuddles and dataChanging cultureAdvocacy for harmonizationIt’s working!

PDSA #3: Model of Care TransitionsFostering the accountable in ACO
SAFER TRANSITIONSColeman model• Use of a transition coach• Teaching skills, knowledge and attitude to empower and
manage to remain healthy & functionalThe 4 Pillars1. Medication self-management2. Patient-centered health record3. Timely follow-up with primary and specialty care4. Knowledge of red flagsDischarge PharmacistPatient contacts 30/60/90/180 days• Hospital/SNF Visit• Home Visit• Telephone Calls
The issue:• Inadequate preparation
for the next setting of care
• Patients/family act as default care coordinators
• Which leads to med errors, postponed follow-up care and re-hospitalization
• Re-hospitalization reduces value – Q/C

PDSA #4: Office Practice RedesignInnovating in a Value Stream
INNOVATING PRIMARY CAREInnovation Value StreamMultiple tests & spread• Office flow redesign• Ease & access• Communication throughout• Increased time with patient• Group visit redesign – chronic disease management• Roles team-based care
Patients love it!

PDSA #5: Flipped DischargeEnsuring safe transitions
DISCHARGE IN THE HOMEInnovation Testing• CWF/IHI global sourcing• Segmentation• D.R.I.V.E. team• LACE scoring• Ongoing PDSAs

PDSA #6: Post Acute Care FacilitiesBuilding coalitions, solving together
KEYS TO PARTNERSHIPCreate a VisionShared commitments• Share best practices/knowledge• Mentor partners & providers• Share data & support analyses• Promote implementation of evidence-based
interventions• Regular meetings, decision makers have to be present
The Community Coalition to Enhance Care Transitions (CCECT) is a leader in
establishing and initiating best practices to ensure safe and effective care transitions
for patients across the health care continuum
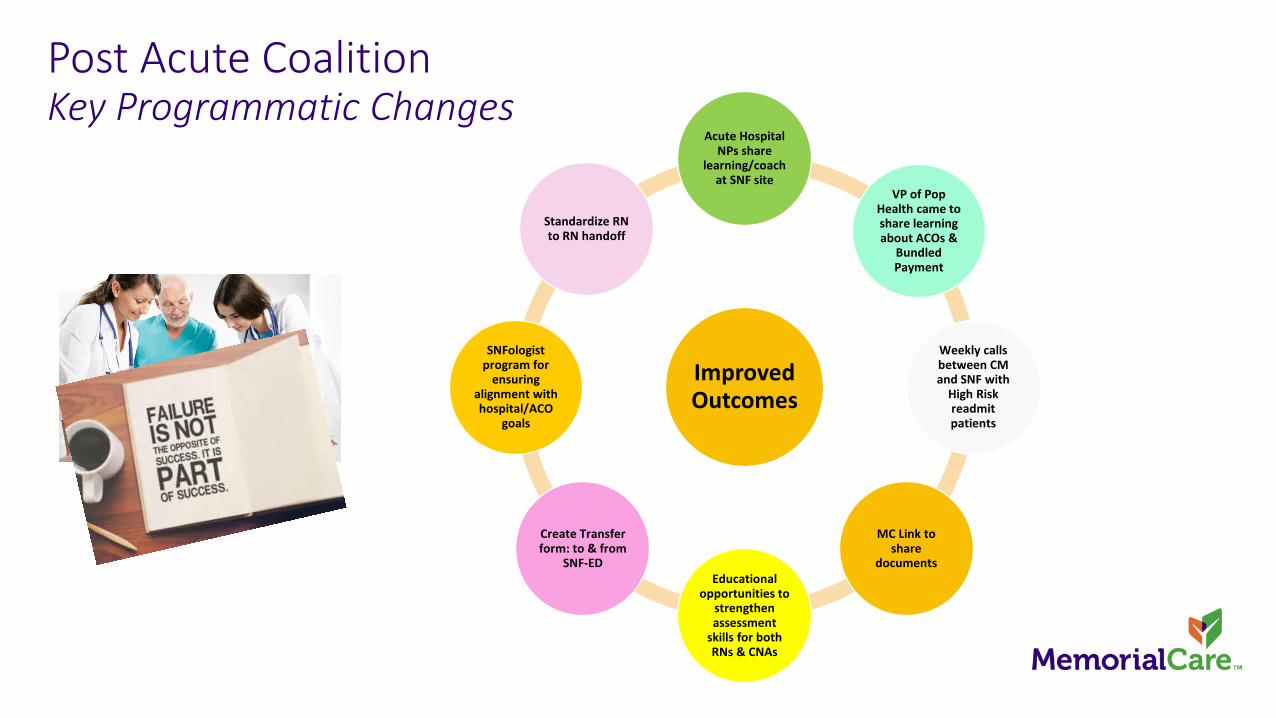
Post Acute Coalition Key Programmatic Changes
Improved Outcomes
Acute Hospital NPs share
learning/coach at SNF site
VP of Pop Health came to share learning about ACOs &
Bundled Payment
Weekly calls between CM and SNF with
High Risk readmit patients
MC Link to share
documentsEducational
opportunities to strengthen assessment
skills for both RNs & CNAs
Create Transfer form: to & from
SNF-ED
SNFologistprogram for
ensuring alignment with hospital/ACO
goals
Standardize RN to RN handoff

PDSA #7: Addressing Overdiagnosis head-onWe are stewards of precious resources
OVERDIAGNOSIS & OVERTREATMENTThe diagnosis of a condition or abnormality which will, if left alone, never cause symptoms, complications, or shortened life
The Prescription:• Make it strategic, hosting broad discussions• Understanding NNTB/NNTH and POEMS• Smart alerts – wisely choosing wisely• Shared decision-making – TheNNT.com• Advocacy – P4P measures that promote overtreatment• Addressing publication bias – publicizing ALL research
Opportunity to override per indication (evidence-links). Active learning over time greater impact than % followed

How to Overdiagnose1. First, change the rules
2. Improve technologies to see more3. Look harder4. Stumble onto incidental findings
Condition/Threshold
Old Definition
New Definition
New Cases Resulting
% Number Needed to Treat to Benefit
Number Needed to Treat to Harm
Diabetes – Fasting BG 140 126
11,697,000 13,378,000 1,681,000 14% ∞ (Death, MI, CVA, RF)250 (Prevent limb loss)
6 (hypoglycemia w/ hospitalization (1)
HypertensionSBP 160 140DBP 100 90
38,690,000 52,180,000 13,490,000 33% ∞ 12 (2)
HyperlipidemiaCholesterol 240 200
49,480,000 92,197,000 42,647,000 86% 50 (MI); death 244 5-20 (myalgia, weakness, cognition, DM) (3)
Osteoporosis in WomenT Score 2.52.0
8,010,000 14,791,000 6,781,000 85% ∞ ~500? (4)
Prediabetes 0 52,000,000 52,000,000 ∞ 4-8 Lifestyle change14 (metformin) (5)
2.4 (6)
1. www.TheNNT.com2. Redberg R, JAMA Int Med 11.13.20163. www.TheNNT.comn4. Gruber A et al., Int J Clin Pract 2006;60(5):5905. Drug Facts and Comparisons Oct. 2004

PDSA #8: EquityBuilding a Community focus
Social Determinants of Health and Life
Focus on equity2017 Physician Academy project teamCollaboration with Long Beach Health & Human ServicesInconvenient truths
• Household wealth• Social status• Support networks• Education• Employment• Social environments• Physical environments• Personal health
practices & coping skills
• Healthy child development
• Gender• Culture

Inconvenient truthsSDOH Impact in Long Beach, California

6 Governance

Our organization today

ACO requirements for oversight
Not one size fits all• Each ACO requires its own structure
• Ex: NextGen – Board of Managers, 80% practicing providers from roster, beneficiary and advocate
• Partner relationships and representation
Executive Steering teamStrategic Plan, annual review

Driver Diagram Metrics - customizable
Secondary Driver Metric (Data Source)
Member Experience and Engagement
• Increased In-Network Utilization (claims)• Patient Activation Assessment• Satisfaction Survey (CG-CAHPS)• Reduced ER utilization (claims)
Care Delivery and Coordination
• Reduction in ambulatory-sensitive admissions; reduced readmissions (claims)• Percent of discharged patients with medication reconciliation (quality data)• Percent of beneficiaries with evidence of Advanced Care Planning• Reduced SNF days per 1,000 (claims)• Increased generic prescribing rate (claims and chart)
Provider Support and Engagement
• Quality Metrics achievement (quality data)• Increased utilization of efficient providers or services (claims)• Provider satisfaction (survey)• Increased ASC utilization (claims)
Information Technology and Analytics
• Deploy analytics solution to include risk stratification; targeted interventions; integration with EMR; and ability to identify beneficiaries at point of care (in-house measurement)

7 Outcomes & ROI Thinking

Achieving Triple Aim ImpactStories matter – high touch care, building trust
BackgroundDW is a 69 y/o Latina female who had 21 ER visits in the last year, 17 resulting in admission
Major diagnoses: Diabetes Mellitus (DM), newly Dx Liver CA, cirrhosis, GERD, and depression
Social history: widow, with 3 minimally involved sons
ACO Case Management Intervention• Outreach to PCP and creation of a comprehensive plan of care• Mid Sept initiated daily calls which helped her safely manage at home• Social Work helped move her to an Extended Stay with her cherished
pet • Purchased and delivered a holiday meal using Memorial Care "Simply
Better" funds as she knew DW would be alone for the holiday• ACO Services: Care Coordinator, Case Manager, NP for home visit and
Social Worker
Ongoing Progress & Outcomes• Facilitated move to assisted living facility
(with cherished pet) in Dec which reduced her living expenses by $800 per month, improved dietary options and DM management with facility administering medications
• Enhanced social interaction resulting in lifted spirits and improved desire to self manage care
• Reduced ED visits and admissions• Reduced the cost of care and significantly
improved the patient’s social supports and quality
UNDERSTANDING WHAT MATTERS TO HER

NGACO PerformanceThe deferred ROI, and actuarials really matter
2016 Performance year 1• 24,764 initial alignment• 18,988 year end = 7% change• Over 1000 providers, many specialists
2017 Performance year 2• 17,177 initial alignment• 13,749 estimated year end• 374 providers mostly PCP – 67 % reduction
Actual Raw Claims Costs (does not include risk or stop loss factors)
$1,032 $1,026
$870
$600
$700
$800
$900
$1,000
$1,100
CY 2015 CY 2016 CY 2017 TD
ACO Expenditure PBPM - AD
AD Linear (AD)
$8,466
$7,801 $7,716
$6,000
$7,000
$8,000
$9,000
CY 2015 CY 2016 CY 2017 TD
ACO Expenditure PBPM - ESRD
ESRD Linear (ESRD)
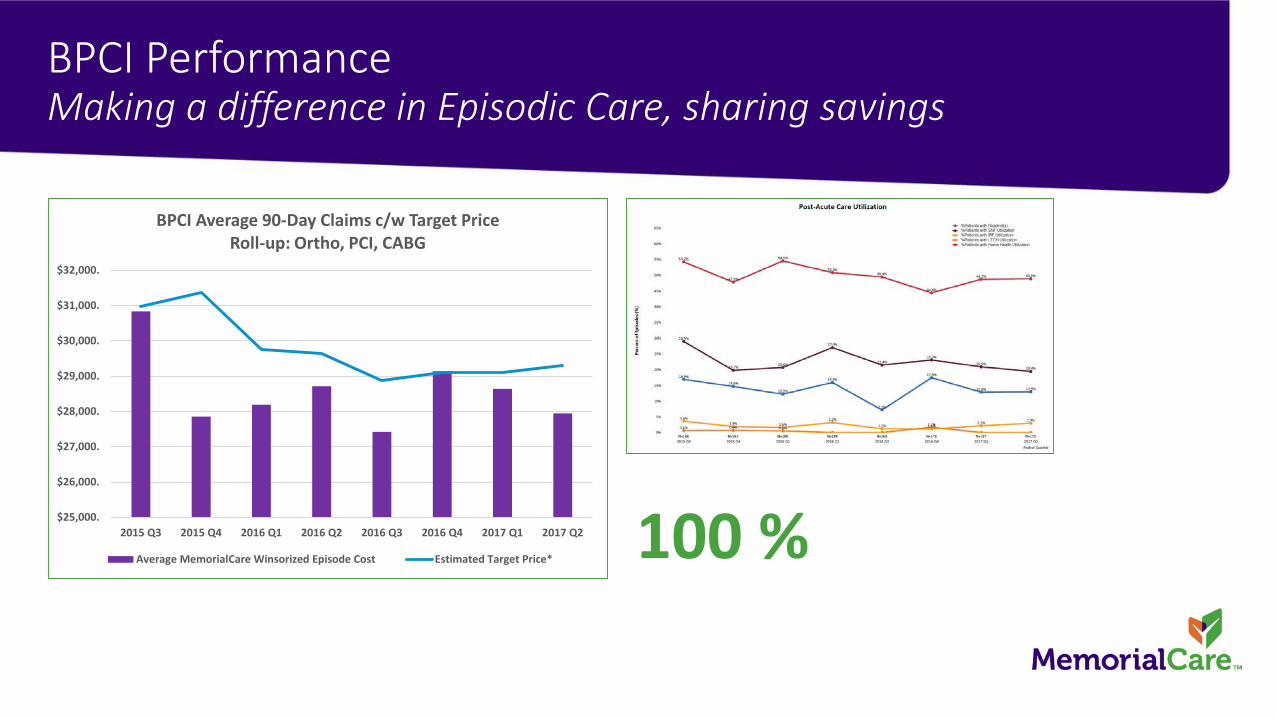
BPCI PerformanceMaking a difference in Episodic Care, sharing savings
100 %$25,000.
$26,000.
$27,000.
$28,000.
$29,000.
$30,000.
$31,000.
$32,000.
2015 Q3 2015 Q4 2016 Q1 2016 Q2 2016 Q3 2016 Q4 2017 Q1 2017 Q2
BPCI Average 90-Day Claims c/w Target PriceRoll-up: Ortho, PCI, CABG
Average MemorialCare Winsorized Episode Cost Estimated Target Price*
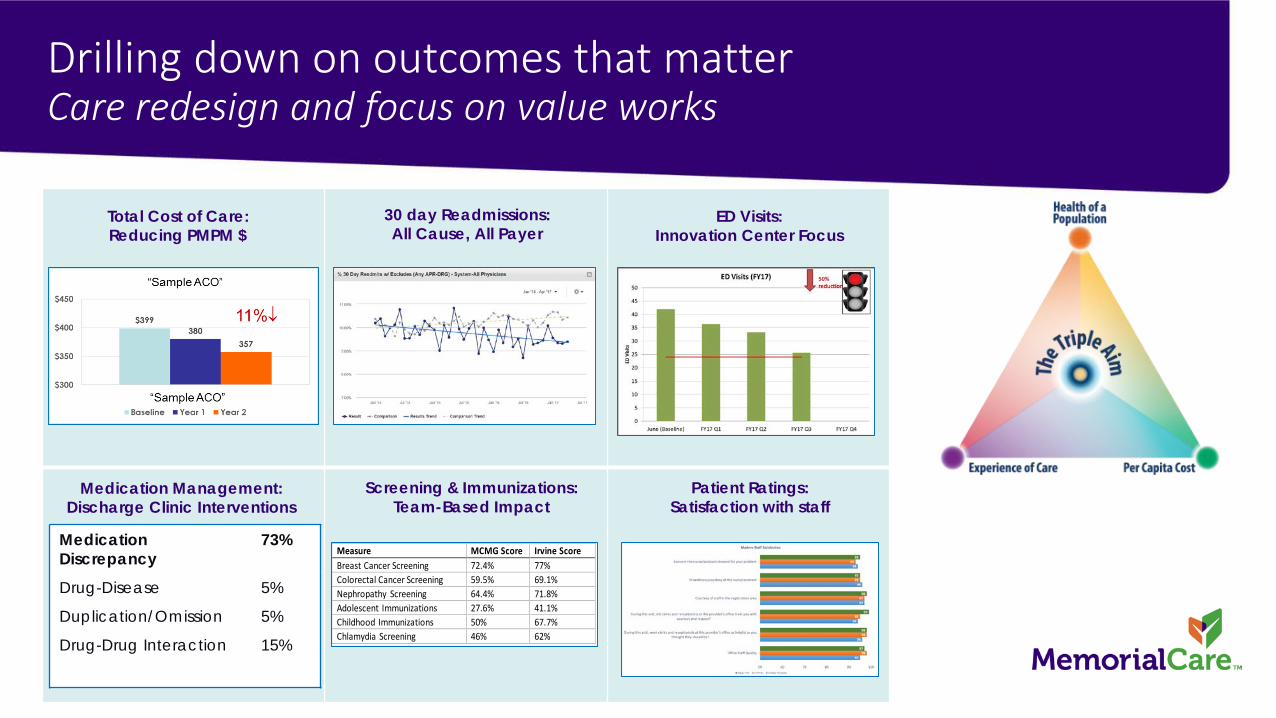
Drilling down on outcomes that matterCare redesign and focus on value works
30 day Readmissions:All Cause, All Payer
Total Cost of Care:Reducing PMPM $
ED Visits:Innovation Center Focus
Screening & Immunizations:Team-Based Impact
Medication Management:Discharge Clinic Interventions
Patient Ratings:Satisfaction with staff
Measure MCMG Score Irvine Score Breast Cancer Screening 72.4% 77% Colorectal Cancer Screening 59.5% 69.1% Nephropathy Screening 64.4% 71.8% Adolescent Immunizations 27.6% 41.1% Childhood Immunizations 50% 67.7% Chlamydia Screening 46% 62%
MedicationDiscrepancy
73%
Drug-Disease 5%
Duplication/Omission 5%
Drug-Drug Interaction 15%

More employers choosing usIf you build it, they will come…
Aetna Whole Health New for January 2018
Vivity – January 2015
Boeing – January 2017
Adventist – January 2017, 2018
Aetna Whole Health – September 2016MemorialCare-GNP network differentiation and growing reputation as the provider committed to value resulted in additional sold cases for 1-1-2018 go-live
Employers in the Queue
8 Where to Next and Questions

Barriers & Lessons Learned
KEY LESSONS LEARNED1. It is a strategic investment2. Engage actuarial assistance3. Partnering with others4. Outreach, explain, make it easy5. Patient centric support, involve6. Don’t budget return in year 1!7. Narrow networks Designated8. Engage expert resources, early9. Building & improving new tools10. It takes a village (IT, HR)11. Advocate for Q harmonization12. Focus on social determinants13. Leverage interest, collaboratives14. Education on # needed to treat15. Visibility, streamline, celebrate
Find the halo
POTENTIAL BARRIERS1. Leadership and vision2. Predicting risk and price of entry3. Geography4. Physician participation5. Patient engagement6. Focus on a performance year7. Attribution modeling8. Delayed / incomplete claims9. Data, data, data10. Adding (and finding) expertise11. Varying quality metrics12. Population segmentation13. Post-Acute alignment14. Overtreatment, overdiagnosis15. Equal opportunity burnout
Focusing only on ROI

Thank you.