melkersson-rosenthal syndrome: a possible association with psoriasis
TRANSCRIPT

J AM ACAD DERMATOL
VOLUME 67, NUMBER 4Letters 795
lower incidence of complications. All of the patientswho did develop dry sockets postoperatively, how-ever, healedwithout further complication. The resultsobtained from this preliminary examination of theeffects of isotretinoin on wisdom teeth removal sug-gest that patients do not need to defer third molarsurgery during treatment with isotretinoin.
Jyoti Sharma, BS,a Diane M. Thiboutot, MD,b andAndrea L. Zaenglein, MDb,c
Penn State College of Medicinea; Department ofDermatology, Penn State Hershey MedicalCenterb; and Department of Pediatrics, PennState Children’s Hospital, Hersheyc
Funding sources: None.
Conflicts of interest: None declared.
Correspondence to: Andrea L. Zaenglein, MD, De-partment of Dermatology, HU14, Penn StateHershey Medical Center, 500 University Dr,Hershey, PA 17033
E-mail: [email protected]
REFERENCES
1. Zachariae H. Delayed wound healing and keloid formation
following argon laser treatment or dermabrasion during iso-
tretinoin treatment. Br J Dermatol 1988;118:703-6.
2. Roenigk HH Jr, Pinski JB, Robinson JK, Hanke CW. Acne,
retinoids, and dermabrasion. J Dermatol Surg Oncol
1985;11:396-8.
3. Khatri K. Diode laser hair removal in patients undergoing
isotretinoin therapy. Dermatol Surg 2004;30:1205-7.
4. Bui CH, Seldin EB, Dodson TB. Types, frequencies, and risk
factors for complications after third molar extraction. J Oral
Maxillofac Surg 2003;61:1379-89.
5. Bouloux GF, Steed MB, Perciaccante VJ. Complications of third
molar surgery. Oral Maxillofac Surg Clin North Am
2007;19:117-28.
http://dx.doi.org/10.1016/j.jaad.2011.02.001
Melkersson-Rosenthal syndrome: A possibleassociation with psoriasis
To the Editor: Fissured tongue (FT) and geographictongue were reported to occur with greater preva-lence in psoriatic patients compared with controlpatients. The prevalence of FT in psoriatic patientsranged from 22.6% to 47.5%.1 However, whereasgeographic tongue and psoriasis were associatedwith HLA-C*06, no association was found betweenFT and HLA-C*06.2
Melkersson-Rosenthal syndrome (MRS) is a rareneuromucocutaneous disorder characterized by atriad of symptoms consisting of recurrent orofacialswelling, FT, and recurrent facial nerve paralysis.Only 25% of patients with MRS manifest all 3
symptoms, and most patients have an oligosymp-tomatic or monosymptomatic form of MRS.3 Itsmost consistent finding is recurrent orofacial or lipswelling, with the classic histologic finding ofepithelioid noncaseating granulomas. However,the histologic findings may be nonspecific and theabsence of granulomas does not exclude the diag-nosis of MRS.3 MRS is more common in youngadults. The origin is unknown, although contactsensitivity, infection, and genetic factors have beenproposed.
A retrospective analysis was conducted in aseries of 12 Israeli patients with the diagnosis ofMRS (Table I). All presented with orofacial swelling(recurrent or constant) involving mainly the lips,and granulomas were recorded in 4 (33%). Fivecases (42%) manifested the full triad of symptoms, 2(17%) were oligosymptomatic, 2 (17%) were mon-osymptomatic, and 3 (25%) manifested orofacialswelling without granulomas. The mean age at theonset of symptoms was 34 years. Medical historyand physical examination revealed the presence ofpsoriasis in 5 cases (42%) and psoriasiform lesionson the palms in 1 case (8%). Psoriatic arthritis wasassociated with 1 case and skin biopsy specimens in2 cases confirmed the diagnosis of psoriasis. Afamily history of psoriasis was obtained in 3 cases.The full triad of symptoms was observed in 4 ofthese 6 cases with psoriasis (67%), FT was recordedin 5 (83%) cases, and granulomas were recorded in2 (33%) cases. The overall prevalence of psoriasis inthe current series of MRS was 50% (95% confidenceinterval 21.7-78.3).
The overall prevalence of psoriasis in the worldis estimated to be 1% to 2%, with geographicvariations ranging from 0.2% to 1.5% in China,2.2% to 4.6% in the United States, 4.7% in Canada,to 6.5% in Germany.4 Accordingly, the occurrenceof psoriasis in the current series of MRS, which is arare disorder, is higher than that expected in thegeneral population. This may imply an associationthat has not been reported to date between psori-asis and MRS.
Psoriasis has already been associated with gran-ulomatous diseases such as Crohn’s disease5 andsarcoidosis. In the current series of MRS no evi-dence for either Crohn’s disease or sarcoidosis wasfound. The high prevalence of psoriasis observed inthe current series of MRS (50%) may be related tothe presence of FT. The presence of granulomas inMRS (33%) may imply linkage among psoriasis, FT,and granulomatous diseases. In view of the limita-tions of the retrospective study design furtherinvestigations are needed. Moreover, the possiblerole of genetic links and immune factors (T helper
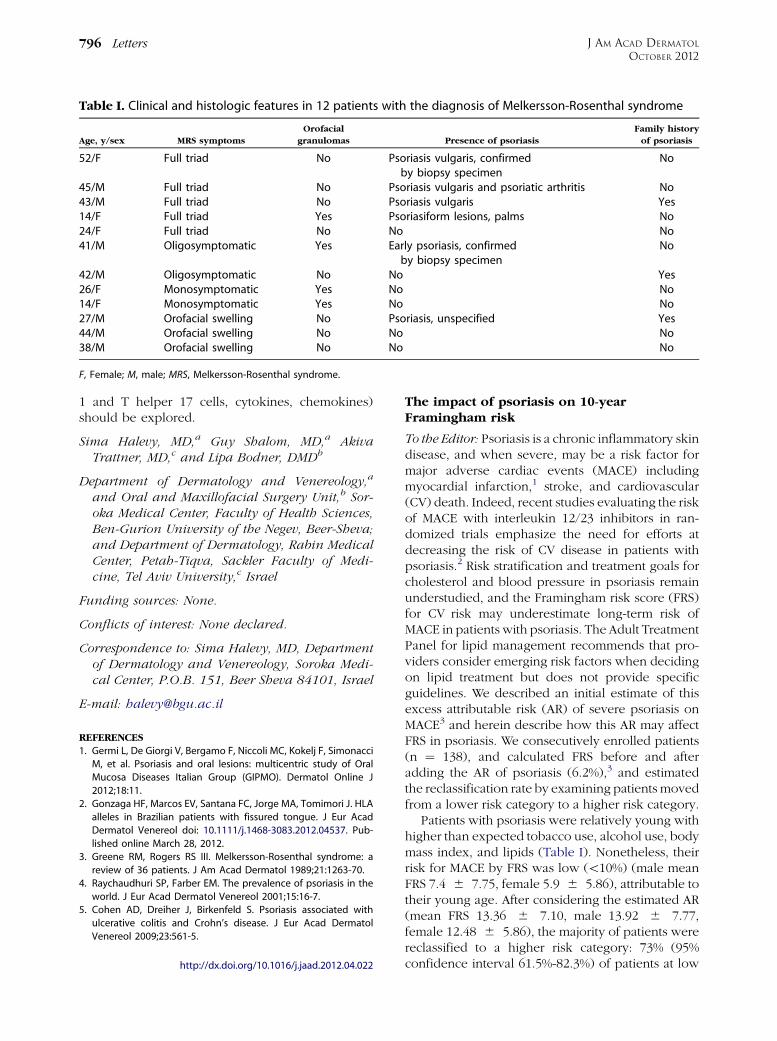
Table I. Clinical and histologic features in 12 patients with the diagnosis of Melkersson-Rosenthal syndrome
Age, y/sex MRS symptoms
Orofacial
granulomas Presence of psoriasis
Family history
of psoriasis
52/F Full triad No Psoriasis vulgaris, confirmedby biopsy specimen
No
45/M Full triad No Psoriasis vulgaris and psoriatic arthritis No43/M Full triad No Psoriasis vulgaris Yes14/F Full triad Yes Psoriasiform lesions, palms No24/F Full triad No No No41/M Oligosymptomatic Yes Early psoriasis, confirmed
by biopsy specimenNo
42/M Oligosymptomatic No No Yes26/F Monosymptomatic Yes No No14/F Monosymptomatic Yes No No27/M Orofacial swelling No Psoriasis, unspecified Yes44/M Orofacial swelling No No No38/M Orofacial swelling No No No
F, Female; M, male; MRS, Melkersson-Rosenthal syndrome.
J AM ACAD DERMATOL
OCTOBER 2012796 Letters
1 and T helper 17 cells, cytokines, chemokines)should be explored.
Sima Halevy, MD,a Guy Shalom, MD,a AkivaTrattner, MD,c and Lipa Bodner, DMDb
Department of Dermatology and Venereology,a
and Oral and Maxillofacial Surgery Unit,b Sor-oka Medical Center, Faculty of Health Sciences,Ben-Gurion University of the Negev, Beer-Sheva;and Department of Dermatology, Rabin MedicalCenter, Petah-Tiqva, Sackler Faculty of Medi-cine, Tel Aviv University,c Israel
Funding sources: None.
Conflicts of interest: None declared.
Correspondence to: Sima Halevy, MD, Departmentof Dermatology and Venereology, Soroka Medi-cal Center, P.O.B. 151, Beer Sheva 84101, Israel
E-mail: [email protected]
REFERENCES
1. Germi L, De Giorgi V, Bergamo F, Niccoli MC, Kokelj F, Simonacci
M, et al. Psoriasis and oral lesions: multicentric study of Oral
Mucosa Diseases Italian Group (GIPMO). Dermatol Online J
2012;18:11.
2. Gonzaga HF, Marcos EV, Santana FC, Jorge MA, Tomimori J. HLA
alleles in Brazilian patients with fissured tongue. J Eur Acad
Dermatol Venereol doi: 10.1111/j.1468-3083.2012.04537. Pub-
lished online March 28, 2012.
3. Greene RM, Rogers RS III. Melkersson-Rosenthal syndrome: a
review of 36 patients. J Am Acad Dermatol 1989;21:1263-70.
4. Raychaudhuri SP, Farber EM. The prevalence of psoriasis in the
world. J Eur Acad Dermatol Venereol 2001;15:16-7.
5. Cohen AD, Dreiher J, Birkenfeld S. Psoriasis associated with
ulcerative colitis and Crohn’s disease. J Eur Acad Dermatol
Venereol 2009;23:561-5.
http://dx.doi.org/10.1016/j.jaad.2012.04.022
The impact of psoriasis on 10-yearFramingham risk
To the Editor: Psoriasis is a chronic inflammatory skindisease, and when severe, may be a risk factor formajor adverse cardiac events (MACE) includingmyocardial infarction,1 stroke, and cardiovascular(CV) death. Indeed, recent studies evaluating the riskof MACE with interleukin 12/23 inhibitors in ran-domized trials emphasize the need for efforts atdecreasing the risk of CV disease in patients withpsoriasis.2 Risk stratification and treatment goals forcholesterol and blood pressure in psoriasis remainunderstudied, and the Framingham risk score (FRS)for CV risk may underestimate long-term risk ofMACE in patients with psoriasis. The Adult TreatmentPanel for lipid management recommends that pro-viders consider emerging risk factors when decidingon lipid treatment but does not provide specificguidelines. We described an initial estimate of thisexcess attributable risk (AR) of severe psoriasis onMACE3 and herein describe how this AR may affectFRS in psoriasis. We consecutively enrolled patients(n ¼ 138), and calculated FRS before and afteradding the AR of psoriasis (6.2%),3 and estimatedthe reclassification rate by examining patients movedfrom a lower risk category to a higher risk category.
Patients with psoriasis were relatively young withhigher than expected tobacco use, alcohol use, bodymass index, and lipids (Table I). Nonetheless, theirrisk for MACE by FRS was low (\10%) (male meanFRS 7.4 6 7.75, female 5.9 6 5.86), attributable totheir young age. After considering the estimated AR(mean FRS 13.36 6 7.10, male 13.92 6 7.77,female 12.48 6 5.86), the majority of patients werereclassified to a higher risk category: 73% (95%confidence interval 61.5%-82.3%) of patients at low