megaprosthetic replacement of knee in a young boy of 14 years
TRANSCRIPT

Megaprosthetic replacement of knee in a young boy of 14 years

Case Report
Megaprosthetic replacement of knee in a young boyof 14 years
Raju Vaishya b,*, Md. Zamil Zaidur Rahim a, Vivek Kumar Shrivastava c
aClinical Fellow, Arthroscopy and Arthroplasty, Department of Orthopaedics & Joint Replacement Surgery,
Indraprastha Apollo Hospitals, New Delhi, Indiab Prof., Sr Consultant, Department of Orthopaedics & Joint Replacement Surgery, Indraprastha Apollo Hospitals,
New Delhi, IndiacDNB Student, Department of Orthopaedics & Joint Replacement Surgery, Indraprastha Apollo Hospitals,
New Delhi, India
a r t i c l e i n f o
Article history:
Received 25 April 2013
Accepted 5 July 2013
Available online 15 August 2013
Keywords:
Osteosarcoma
Limb salvage
Tibia
Megaprosthesis
a b s t r a c t
Now a days, Total Knee Replacement (TKR) is a common for elderly patients but is an
uncommon procedure in young individuals. Recently, limb conservation surgery for ma-
lignant bone tumours like osteosarcoma around the knee has become a common indica-
tion for TKR in young. We report, here a histologically confirmed osteosarcoma in right
proximal tibia of a 14-year-old boy who was managed successfully by limb salvage surgery
using Global Modular Replacement System (GMRS, Stryker).
Copyright ª 2013, Indraprastha Medical Corporation Ltd. All rights reserved.
1. Introduction
Osteosarcomaisanaggressivemalignantneoplasmarising from
primitive transformed cells of mesenchymal origin.1 It is the
most common histological form of primary bone cancer. This is
largely a disease of youthwithmore than 75%of cases occurring
in those less than 25 years of age.2 The management of osteo-
sarcoma in young patients remains a challenging problem and
the treatment optionmayvary fromnon-operative treatment to
operative treatments like amputation and limb conservation.
Wereport a caseof 14-year-oldmale,withgrade IIBdisease,who
was successfully treated by limb conservative surgery. After
three cycles neoadjuvant chemotherapy, the tumour was
excised in toto and replacement was done by Global Modular
Replacement System (GMRS Stryker).
2. Case report
A 14-year boy (NT) reported to us with a history of progressive
increasing painful swelling in right proximal tibia of six
months. It has been associated with restricted knee move-
ment. The swelling was 6 cm � 4 cm in size, oval in shape
(Fig. 1). It was moderately tender, stony hard and fixed to the
bone but overlying skin was free. There was no distal neuro-
vascular deficit. He was investigated with X-ray and MRI
* Corresponding author.E-mail address: [email protected] (R. Vaishya).
Available online at www.sciencedirect.com
journal homepage: www.elsevier .com/locate/apme
a p o l l o m e d i c i n e 1 0 ( 2 0 1 3 ) 2 9 3e2 9 6
0976-0016/$ e see front matter Copyright ª 2013, Indraprastha Medical Corporation Ltd. All rights reserved.http://dx.doi.org/10.1016/j.apme.2013.07.001
whichwere suggestive of lytic mass in upper end of tibia (Figs.
2 and 3). Core biopsy confirmed the diagnosis of osteosar-
coma. Haematological profile revealed anaemia with mild
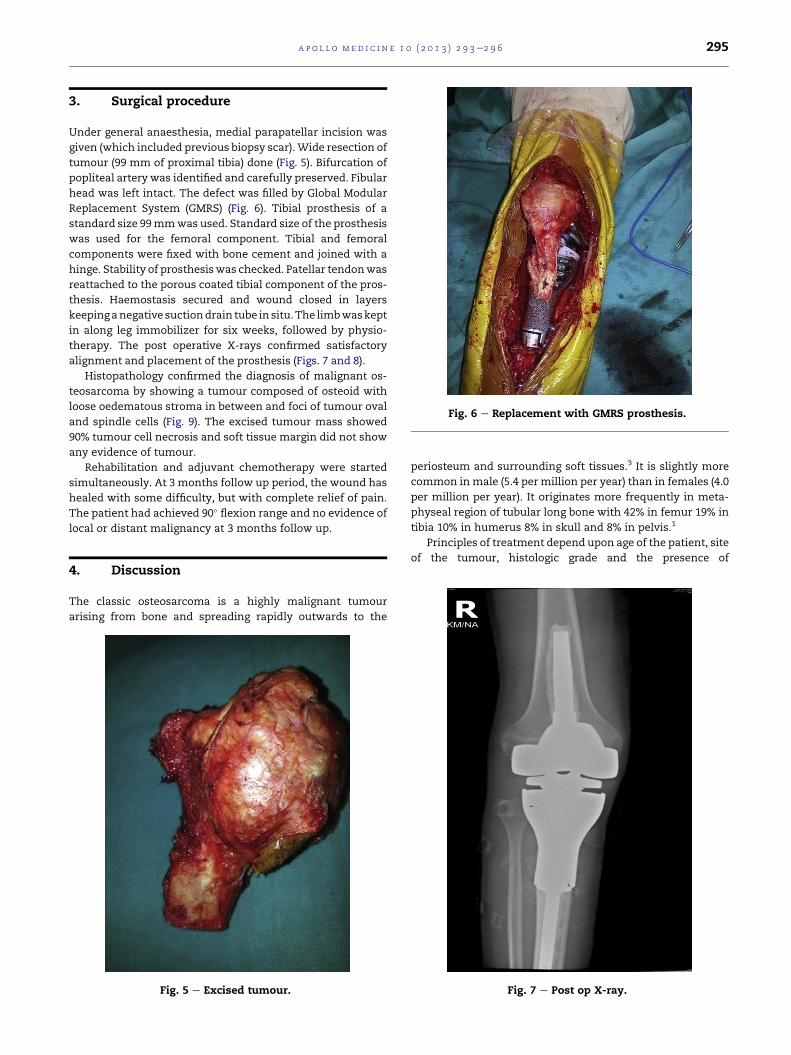
elevation of ESR. PET CT scan revealed FDG avid lytic sclerotic
destruction in upper tibia with FDG avid soft tissue compo-
nent and areas of punctuate calcification anteromedially in
right upper leg e likely malignant primary bone tumour
(Fig. 4). No evidence of FDG avid distant metastases seen.
This boy was treated, pre operatively, by three cycles
neoadjuvant chemotherapy with Cisplatin and Adriamycin
followed by tumour excision and replacement done by Global
Modular Replacement System (GMRS). Post operative period
was uneventful and he was discharged on 5th post operative
day.
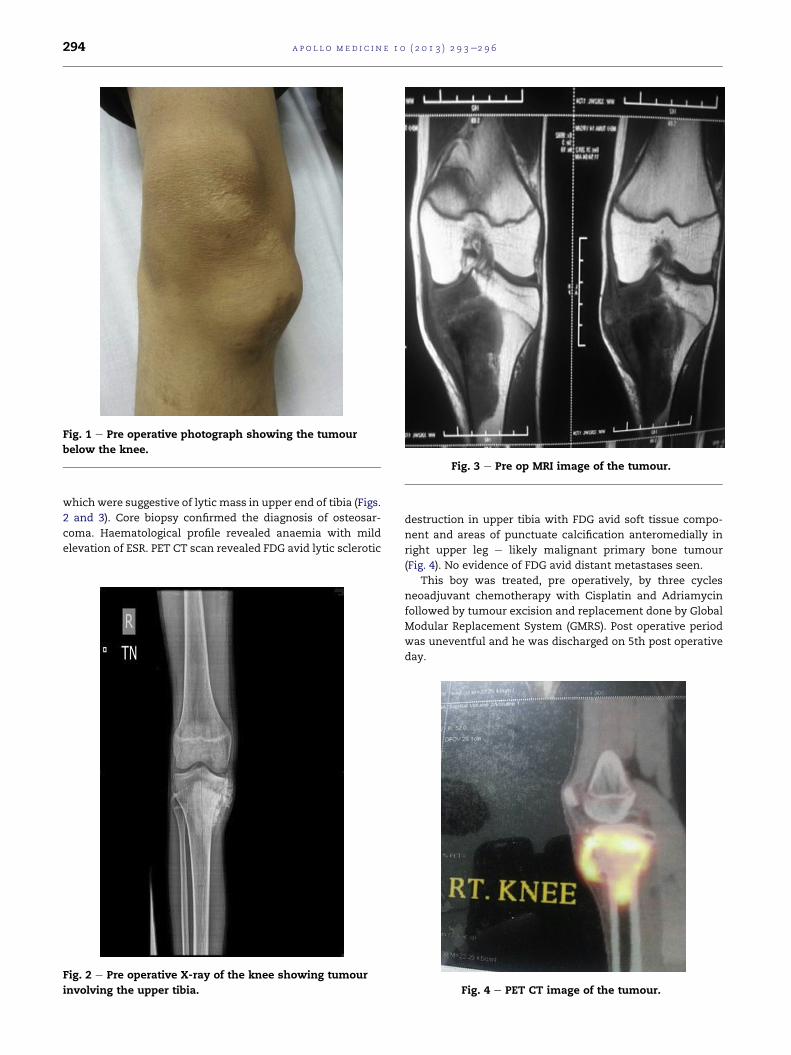
Fig. 1 e Pre operative photograph showing the tumour
below the knee.
Fig. 2 e Pre operative X-ray of the knee showing tumour
involving the upper tibia.
Fig. 3 e Pre op MRI image of the tumour.
Fig. 4 e PET CT image of the tumour.
a p o l l o m e d i c i n e 1 0 ( 2 0 1 3 ) 2 9 3e2 9 6294
3. Surgical procedure
Under general anaesthesia, medial parapatellar incision was
given (which included previous biopsy scar).Wide resection of
tumour (99 mm of proximal tibia) done (Fig. 5). Bifurcation of
popliteal artery was identified and carefully preserved. Fibular
head was left intact. The defect was filled by Global Modular
Replacement System (GMRS) (Fig. 6). Tibial prosthesis of a
standard size 99mmwas used. Standard size of the prosthesis
was used for the femoral component. Tibial and femoral
components were fixed with bone cement and joined with a
hinge. Stability of prosthesiswas checked. Patellar tendonwas
reattached to the porous coated tibial component of the pros-
thesis. Haemostasis secured and wound closed in layers
keepinganegative suctiondrain tube in situ.The limbwaskept
in along leg immobilizer for six weeks, followed by physio-
therapy. The post operative X-rays confirmed satisfactory
alignment and placement of the prosthesis (Figs. 7 and 8).
Histopathology confirmed the diagnosis of malignant os-
teosarcoma by showing a tumour composed of osteoid with
loose oedematous stroma in between and foci of tumour oval
and spindle cells (Fig. 9). The excised tumour mass showed
90% tumour cell necrosis and soft tissue margin did not show
any evidence of tumour.
Rehabilitation and adjuvant chemotherapy were started
simultaneously. At 3 months follow up period, the wound has
healed with some difficulty, but with complete relief of pain.
The patient had achieved 90� flexion range and no evidence of
local or distant malignancy at 3 months follow up.
4. Discussion
The classic osteosarcoma is a highly malignant tumour
arising from bone and spreading rapidly outwards to the
periosteum and surrounding soft tissues.3 It is slightly more
common in male (5.4 per million per year) than in females (4.0
per million per year). It originates more frequently in meta-
physeal region of tubular long bone with 42% in femur 19% in
tibia 10% in humerus 8% in skull and 8% in pelvis.1
Principles of treatment depend upon age of the patient, site
of the tumour, histologic grade and the presence of
Fig. 5 e Excised tumour.
Fig. 6 e Replacement with GMRS prosthesis.
Fig. 7 e Post op X-ray.
a p o l l o m e d i c i n e 1 0 ( 2 0 1 3 ) 2 9 3e2 9 6 295

metastasis. Most patients with osteosarcoma around the knee
are treated with one of three surgical proceduresdwide
resection with prosthetic knee replacement, wide resection
with allograft arthrodesis, or a transfemoral amputation.4
Over the past 30 years, limb-sparing procedures have
become the standard, mainly due to concomitant advances in
chemotherapy and sophisticated imaging techniques. Such
advances have made limb salvage possible even after patho-
logic fracture, previouslywhichwas considered as an absolute
indication for amputation.5
Endoprosthetic reconstruction has gained wide popularity
for limb-sparing surgery. This involves replacing the removed
bone with a metal implant. This obviates the need for bone to
bone healing as is necessary with allografts.
Megaprosthetic reconstruction has many advantages. It
provides immediate stability which allows earlier rehabilita-
tion with immediate full weigh bearing. Most endoprostheses
are modular, thus allowing incremental prosthetic replace-
ment in response to the length of resected bone. In addition,
improvement in implant materials has greatly increased the
durability ofmodern endoprostheses. They are able to achieve
their primary aim of providing long-term function for some
patients with relatively low physical demands.6
Patients who had undergone resection and prosthetic knee
replacement showed higher self-selected walking velocities
and a more efficient gait with regard to oxygen consumption
than patients with transfemoral amputations.7
In a study, over 43 patient between 1993 and 2002 malig-
nant tumour around knee region evaluating life quality, it was
found that all patients rated the therapy excellent or good,
regardless of the type of prosthesis, length or type of resection
or tumour site, surgical intervention did not limit their every-
day life activities.8
While differences between amputation and limb-sparing
procedures do exist, long-term outcomes with regards to pa-
tient function and satisfaction appear to be similar.
Conflicts of interest
All authors have none to declare.
r e f e r e n c e s
1. Ottaviani G, Jaffe N. The epidemiology of osteosarcoma. In:Jaffe N, et al., eds. Pediatric and Adolescent Osteosarcoma. NewYork: Springer; 2009.
2. Mirra JM. Bone Tumors: Clinical, Radiologic, and PathologicCorrelations. Philadelphia: Lea and Febiger; 1989.
3. Solomon Louis, Warwick David J, Nayagam Selvadurai.Tumour. In: Apley’s System of Orthopaedics and Fractures. 8th ed.Arnold; 2001:185e190, 4.
4. Terry Canale S, Daugherty Kay, Jones Linda. Campbell’sOperative Orthopaedics. 11th ed. 566 [chapter 9].
5. Scully SP, Ghert MA, Zurakowski D, et al. Pathologic fracture inosteosarcoma: prognostic importance and treatmentimplications. J Bone Joint Surg. 2002;84A:49.
6. Peh Khee T, Mann Hong T. Functional outcome study of mega-endoprosthetic reconstruction in limbs with bone tumoursurgery. Ann Acad Med Singap. 2009;38:192e196.
7. Otis JC, Lane JM, Kroll MA. Energy cost during gait inosteosarcoma patients after resection and knee replacementand after above-the-knee amputation. J Bone Joint Surg.1985;67A:606.
8. Skaliczki G, Antal I, Kiss J, Szalay K, Skaliczki J, SzendrTi M.Functional outcome and life quality after endoprostheticreconstruction following malignant tumours around the knee.Int Orthop (SICOT). 2005;29:174e178.
Fig. 8 e Post op X-ray.
Fig. 9 e Histology appearance.
a p o l l o m e d i c i n e 1 0 ( 2 0 1 3 ) 2 9 3e2 9 6296

Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/