meeting agenda · phtls eligibility participants must pass the course to be eligible for...
TRANSCRIPT
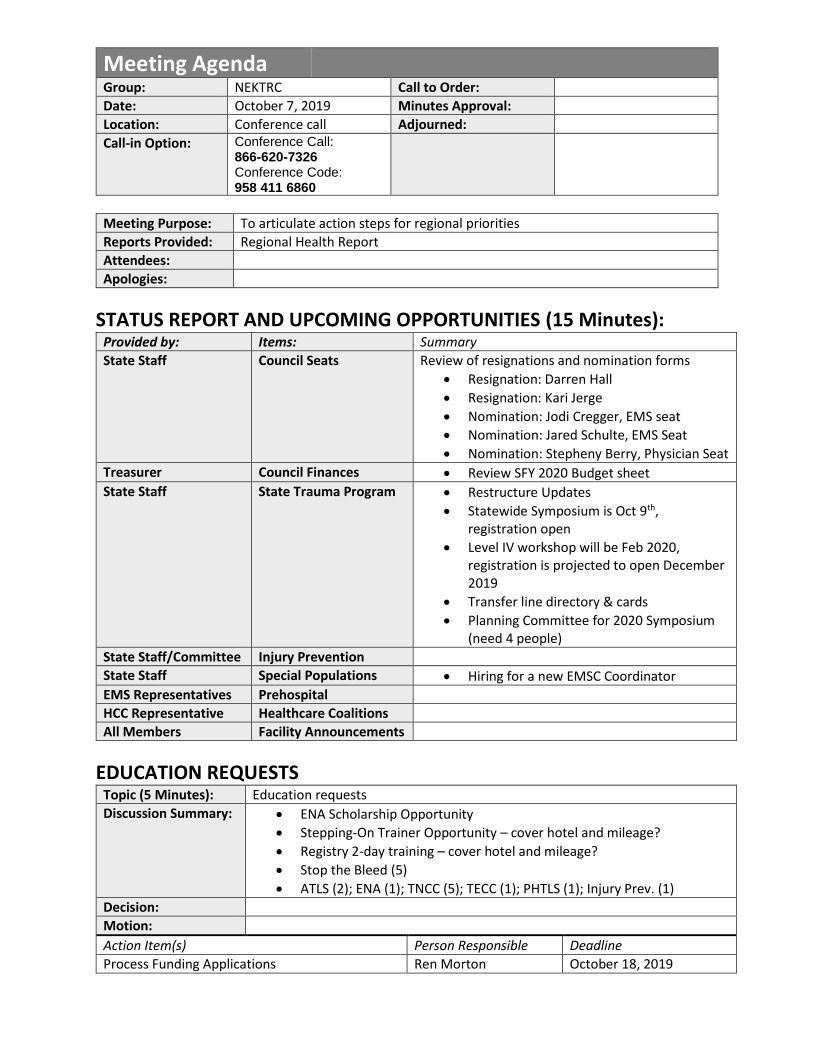
Meeting Agenda
Group: NEKTRC Call to Order:
Date: October 7, 2019 Minutes Approval:
Location: Conference call Adjourned:
Call-in Option: Conference Call: 866-620-7326 Conference Code: 958 411 6860
Meeting Purpose: To articulate action steps for regional priorities
Reports Provided: Regional Health Report
Attendees:
Apologies:
STATUS REPORT AND UPCOMING OPPORTUNITIES (15 Minutes): Provided by: Items: Summary
State Staff Council Seats Review of resignations and nomination forms
• Resignation: Darren Hall
• Resignation: Kari Jerge
• Nomination: Jodi Cregger, EMS seat
• Nomination: Jared Schulte, EMS Seat
• Nomination: Stepheny Berry, Physician Seat
Treasurer Council Finances • Review SFY 2020 Budget sheet
State Staff State Trauma Program • Restructure Updates
• Statewide Symposium is Oct 9th, registration open
• Level IV workshop will be Feb 2020, registration is projected to open December 2019
• Transfer line directory & cards
• Planning Committee for 2020 Symposium (need 4 people)
State Staff/Committee Injury Prevention
State Staff Special Populations • Hiring for a new EMSC Coordinator
EMS Representatives Prehospital
HCC Representative Healthcare Coalitions
All Members Facility Announcements
EDUCATION REQUESTS Topic (5 Minutes): Education requests
Discussion Summary: • ENA Scholarship Opportunity
• Stepping-On Trainer Opportunity – cover hotel and mileage?
• Registry 2-day training – cover hotel and mileage?
• Stop the Bleed (5)
• ATLS (2); ENA (1); TNCC (5); TECC (1); PHTLS (1); Injury Prev. (1)
Decision:
Motion:
Action Item(s) Person Responsible Deadline
Process Funding Applications Ren Morton October 18, 2019

WORKING AGENDA: Topic (20 Minutes): 2020 Priorities
Discussion Summary: • Regional Health Report
Decision:
Motion:
Action Item(s) Person Responsible Deadline
OTHER TOPICS RAISED/OPEN COMMENT Issue Raised By Summary To Be Discussed At
NEXT MEETING Date: November 26, 2019
Time: 1:00pm
Location: Children’s Mercy South
Objective: 2020 Priority Task articulation

Final Minutes 4/8/19 2019 Kansas Trauma Program | 1
Agenda Minutes Follow up In Attendance Executive Committee: Don Fishman, Lois Towster, David
Seastrom, Darren Hall, Dan Hudson, William Sachs, General Membership: Wael Khreiss, Baker, Tammy Newberry, Dorothy Rice, Darlene Whitlock, Angie Welsh, Shawna Beck, Staff: Ren Morton
Conference Call: 866-620-7326 Conference Code: 958 411 6860
Call to Order Call to order at 3:00pm 1st motion: David Seastrom 2nd motion: Lois Towster Motion carries, minutes approved
Don Fishman, MD
System Finance Treasurer’s Report See attached Spreadsheet. Discussion: Budget Priorities for SFY 2020 (Beginning July 1)
Tracy McDonald
Trauma Program Update
The ACT would like each region to claim a priority on the Bis Assessment to tackle for SFY 2020. See attached priorities. BIS Assessment Priority Claimed: 302.6
Ren Morton
Education New SFY 2020 Trauma Funding Application 1st Motion: Dave Seastrom 2nd Motion: Darren Hall Motion: Passes with changes NEKRTC Funding Reimbursement Policy Updates: Request PHTLS/TNCC Cards in a similar manner as ATLS card requirement TNCC Costs have increased. Increase cap to 170 per person. Wages will not be reimbursed Motion Lois Towster Motion David Seastrom Motion: Passes Stop the Bleed Distribution Policy: 3 kits per application cap. Motion to approve ATLS, PHTLS, TNCC: 1st Motion: Lois Towster 2nd Motion: David Seastrom Motion: Motion Passes
Executive Committee
Northeast Kansas Regional Trauma Council
Executive Committee Meeting Agenda
NEKRTC Regional Symposium
April 08, 2019

Final Minutes 4/8/19 2019 Kansas Trauma Program | 2
Agenda Minutes Follow up Motion to approve mini Grants at the following amounts:
Organization Topic Awarded Amt
Nemaha Valley Community Hospital Fire Safety $2,000.00
Hiawatha Community Hospital Bike Helmets $1,991.21
Riley County Health Department Home Safety $960.00
SafeKids Prairie Band Pottawatomi Home Safety $1,600.00
Pottawatomi County Driving Safety $848.00
Community Memorial Healthcare Fall Prev $520.00
Children's Mercy South HomeSafety $660.00
Ransom Memorial Health TBI $1,600.00
Sabetha Community Hospital CarSeatSafety $552.00
Wabaunsee Co Health Dept CarSeatSafety $360.00
Doniphan Co Health Dept BabyShower $0.00
1st Motion: Lois Towster 2nd Motion: Darren Hall Motion: Motion Passes
Injury Prevention HWY 75 initiative People interested in the Farmer’s Bill for suicide prevention.
Tracy McDonald Darlene Whitlock
Special Populations
Pediatrics: Interfacility transfer guidelines books and CT cards. Geriatrics: At the February ACT meeting, Danielle Sass presented Falls data to the Committee. The committee agreed to endorse the following measures:
• Expansion of fall prevention programs
• Expansion of access to evidence-based exercise programs
• Expansion of transportation access to attend programs. See attached infographic.
Tracy Cleary Ren Morton
Prehospital No Report Dan Hudson Darren Hall
Healthcare Coalitions
No Report Steve Hoeger Danielle Marten
Old Business
Don Fishman, MD
New Business Vote on SFY 2020 Executive Committee Officer Positions: Chairperson: Dr. Fishman Vice-Chairperson: Dr. Jerge Treasurer: Tracy McDonald Secretary: David Seastrom ACT Representative Candidates: Dr. Khreis Tammy Newberry Dr. McCullough
Don Fishman, MD

Final Minutes 4/8/19 2019 Kansas Trauma Program | 3
Agenda Minutes Follow up Stephany Berry 1st Motion: David Seastrom 2nd Motion: Darren Hall Motion Passes
Announcements / Each Facility / Agency
All Regional Partners
Adjournment . 4:20pm
Don Fishman, MD
NEXT UP
Meeting Date Time Location Form 2019 ACT Meeting May 1 10:00am – 3:00pm Kansas Medical
Society, Topeka In-person
2019 Executive Committee Meeting Jun 10 1:00pm Conference Call
2019 Executive Committee Meeting Aug 12 1:00pm Children’s Mercy In-person
2019 ACT Meeting Aug 21 10:00am – 3:00pm Kansas Medical Society, Topeka
In-Person
Kansas Statewide Symposium Oct 9 All-Day Ascension – Via Christi Hospitals Wichita
In-Person
2019 Executive Committee Meeting Oct 14 1:00pm Conference Call
2019 ACT Meeting Nov 6 10:00am – 3:00pm Kansas Medical Society, Topeka
In-Person
2019 Executive Committee Meeting Dec 9 1:00pm TBD In - person

1
Ren Morton [KDHE]
From: Hall, Darren <[email protected]>Sent: Friday, September 13, 2019 2:42 PMTo: Ren Morton [KDHE]; [email protected]; Lois Towster
([email protected])Subject: Resignation from NERTC
Follow Up Flag: Follow upFlag Status: Flagged
Categories: RTC
EXTERNAL: This email originated from outside of the organization. Do not click any links or open any attachments unless you trust the sender and know the content is safe.
Good afternoon all, After careful consideration, I have decided to retire from EMS. I will be relocating to Colorado to follow other interests. Mainly as a fly fishing guide in the Breckenridge, Co. area. It has been a honor to serve and attend the NERTC over the past several years and I know this committee will strive to improve trauma services in Kansas. Sincerely,
WtÜÜxÇ [tÄÄ Assistant EMS Chief Franklin County EMS 219 E 14th Ottawa, Kansas 66067 Office 785-229-7302 Fax 785-229-7310
“Get your facts first, then you can distort them as you please.” Mark Twain

THE REGIONAL TRAUMA COUNCIL
The regional trauma council members are chosen as leaders from each region’s trauma practitioners. The regional trauma council sets the direction of the conversation on trauma in each region by:
• Offering continuing education opportunities and funding
• Financially supporting initiatives to improve the regional system
• Collaborating on performance improvement.
By so doing, each region increases its capacity to provide quality patient care, increases the well-being of their communities through injury prevention, and prepares their communities for the worst-case trauma scenarios.
Leadership. Capacity Building. Community Well-Being
By-Laws Voting Privileges: Article 2 Section 2B “The Regional Trauma Councils encourage attendance and input at regular and special meetings from all interested parties. For the purposes of voting, however, the following rule shall pertain: All members, who fill the membership categories listed in Article 2 Section 1 of membership, shall be entitled to one vote. A proxy may be designated in writing and presented before or at any regular or special meeting.”
NOMINATORS INFMORATION (if applicable)
NAME
TITLE
FACILITY
NOMINEE INFORMATION
THE NOMINEE’S DISCIPLINE:
☐ Physician ☐ Hospital Administrator
☐ Nurse ☐ Health Dept. Representative
☐ EMS
NAME
TITLE
FACILITY ADDRESS
CITY, STATE, ZIP
PHONE
PROVIDE A BRIEF SUMMARY OF THE EDUCATION AND BACKGROUND THAT THE NOMINEE WOULD BRING TO THE REGIONAL TRAUMA COUNCIL LEADERSHIP:
*Complete one form per nomination
Return form to Ren Morton at [email protected]


THE REGIONAL TRAUMA COUNCIL The regional trauma council members are chosen as leaders from each region’s trauma practitioners. The regional trauma council sets the direction of the conversation on trauma in each regionby:
� Offering continuing education opportunities and funding
� Financially supporting initiativesto improve the regional system
� Collaborating on performance improvement.
By so doing, each region increases its capacity to provide quality patient care,increases the well-being of theircommunities through injury prevention, and prepares their communities for the worst-case trauma scenarios. Leadership. Capacity Building. Community Well-Being By-Laws Voting Privileges: Article 2 Section 2B “The Regional Trauma Councils encourage attendance and input at regular and special meetings from all interested parties. For the purposes of voting, however, the following rule shallpertain: All members, who fill the membership categories listed in Article 2 Section 1 of membership, shall be entitled to one vote. A proxy may be designated in writing and presented before or at any regular or special meeting.”
NOMINATORS INFMORATION (if applicable) NAME
TITLE
FACILITY
NOMINEE INFORMATION THE NOMINEE’S DISCIPLINE: ☐ Physician ☐ Hospital Administrator ☐ Nurse ☐ Health Dept. Representative ☐ EMS NAME
TITLE
FACILITY ADDRESS
CITY, STATE, ZIP
PHONE
PROVIDE A BRIEF SUMMARY OF THE EDUCATION AND BACKGROUND THAT THE NOMINEE WOULD BRING TO THE REGIONAL TRAUMA COUNCIL LEADERSHIP:
*Complete one form per nomination
Return form to Ren Morton at [email protected]
Jered SchulteEMS DirectorCoffey County EMS
Jered SchulteEMS Director
801 N. 4th StBurlington, KS. 66839620)[email protected]
28 years working in rural EMS @ Coffey County EMS, withthe last 24 years as a paramedic. Director of EMS since9-2018. Active in bringing in training and sending employeesto outside training.

2019 Carryover Balance $102.32
2020 RTC funds $18,000.00
2020 Beginning Balance $18,102.32
Date Expense/Description Check Payable To Budget Actuals Remaining Invoiced
$800.00 $0.00 $800.00
$3,300.00 $0.00 $3,300.00
$0.00
$0.00 $0.00 $0.00
Fiscal Agent Fee Stormont Vail Health $1,358.00 $0.00
$1,358.00 $1,358.00 $0.00
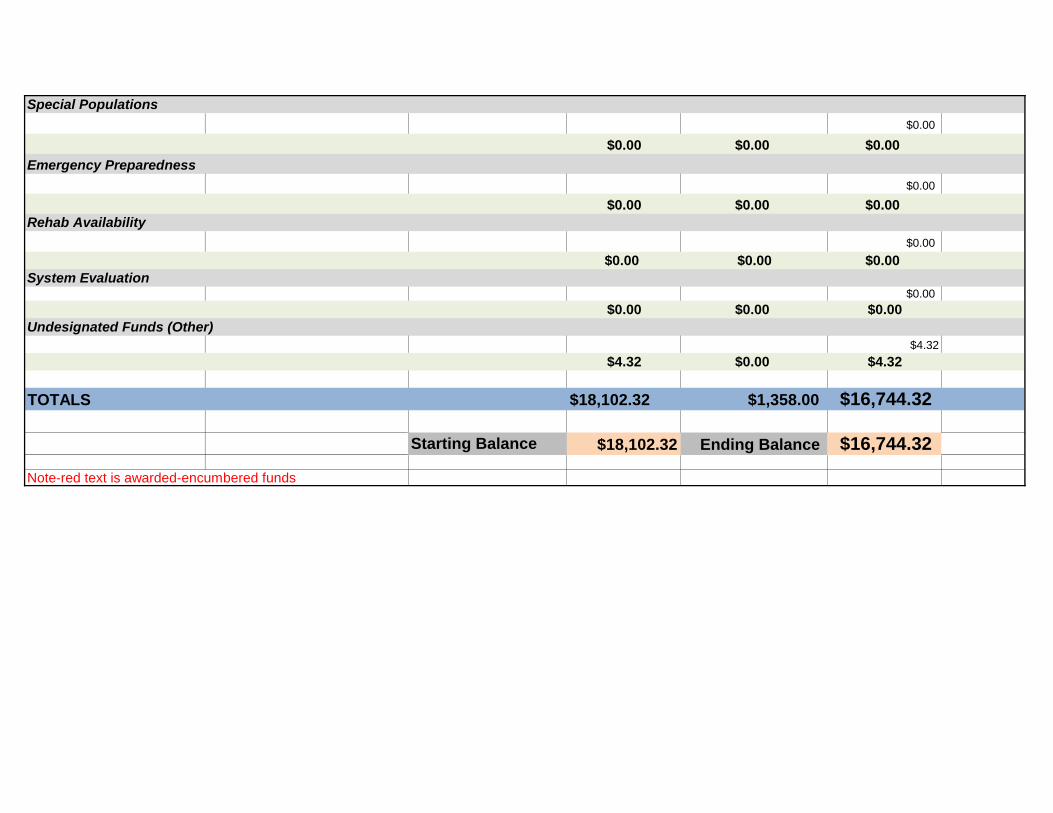
SFY 2020 NEKRTC Expenditure Spreadsheet July 1, 2019-June 30, 2020
I. Administrative Components
System Leadership
System Development
Public Information and Education
System Finance

$5,300.00 $0.00 $5,300.00
$2,000.00 $0.00 $2,000.00
$5,340.00 $0.00 $5,340.00
II.Clinical ComponentsInjury Prevention & Control
Prehospital
Acute Hospital
$0.00
$0.00 $0.00 $0.00
Emergency Preparedness
$0.00
$0.00 $0.00 $0.00
$0.00
$0.00 $0.00 $0.00
$0.00
$0.00 $0.00 $0.00
$4.32
$4.32 $0.00 $4.32
TOTALS $18,102.32 $1,358.00 $16,744.32
Starting Balance $18,102.32 Ending Balance $16,744.32
Note-red text is awarded-encumbered funds
System Evaluation
Undesignated Funds (Other)
Special Populations
Rehab Availability

2019 Kansas Trauma Program
Northeast Kansas Regional Trauma Council Trauma Funding Reimbursement Policy
Original: 21 Feb 2017 Updated: 08 Apr 2019 Effective: 01 Jul 2019
The Northeast Kansas Regional Trauma Council (NEKRTC) provides funding for trauma education and training events in the region. Below are reimbursement guidelines for the most common trauma training courses. To apply for funding for these courses or an innovative trauma education course/event, complete an application to submit to the council.
PHTLS
Eligibility Participants must pass the course to be eligible for reimbursement
Participation Goal Class of 12-16 participants or individual practitioner
Individual Award $100.00 per participant
Award Max Not to exceed $1,500.00
TNCC
Eligibility Participants must pass the course to be eligible for reimbursement
Participation Goal Class of 12 participants or individual practitioner
Individual Award $170.00 per participant
Award Max Not to exceed $2,040.00
ATLS
Eligibility Participants must pass the course to be eligible for reimbursement
Participation Goal Individual Practitioner
Individual Award Dependent upon employer CME contribution
Award Max Not to exceed $650.00
RTTDC
Eligibility A facility is eligible for funding for one RTTDC class per state fiscal year (Jul 1 – Jun 30).
Participation Goal Class of 16-20 participants
Award Max Reimbursement based on approved application budget and affidavit of expenditures. Not to exceed $1,500.00.
INJURY PREVENTION:
Eligibility Course/Event must occur within state fiscal year (July 1 – June 30).
Award Reimbursement based on approved application budget and affidavit of expenditures
Limitation Will not reimburse for staff wages
STOP THE BLEED (STB)
Eligibility Must be a stop the bleed trainer to apply for stop the bleed kits*
Award Max Up to 3 kits per application *To apply for stop the bleed kits, submit an application to the regional council. FUNDING:
• ATLS providers or individual practitioners attending courses outside of their facility must submit a copy of their credentialing card within 30 days of course completion.
• Course/event coordinators must submit class rosters (including city, zip, initial/renewal certification status) and a final affidavit of expenditures within 45 days of course completion
• Submit documentation to the Regional Trauma Coordinator
• Reimbursements will be made to the facility listed on the application once documentation is received. If documentation is not received within the appropriate timeframe, the funding application will be cancelled and the facility will not receive reimbursement.

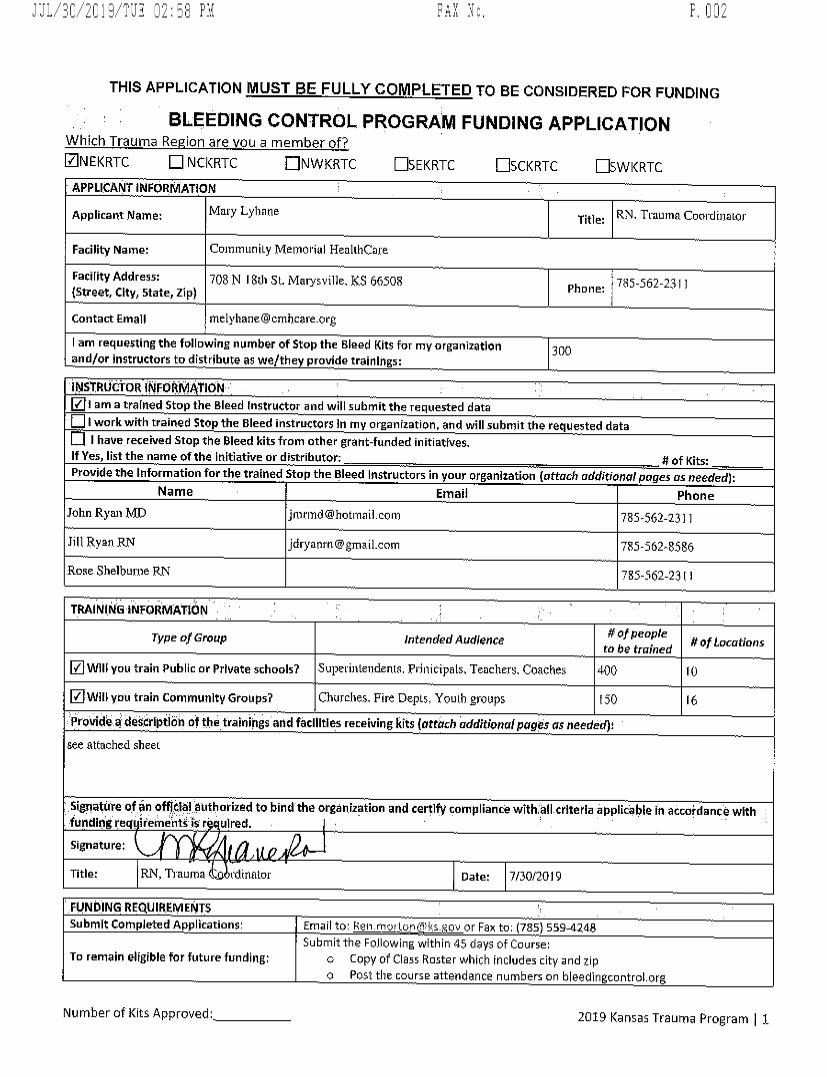
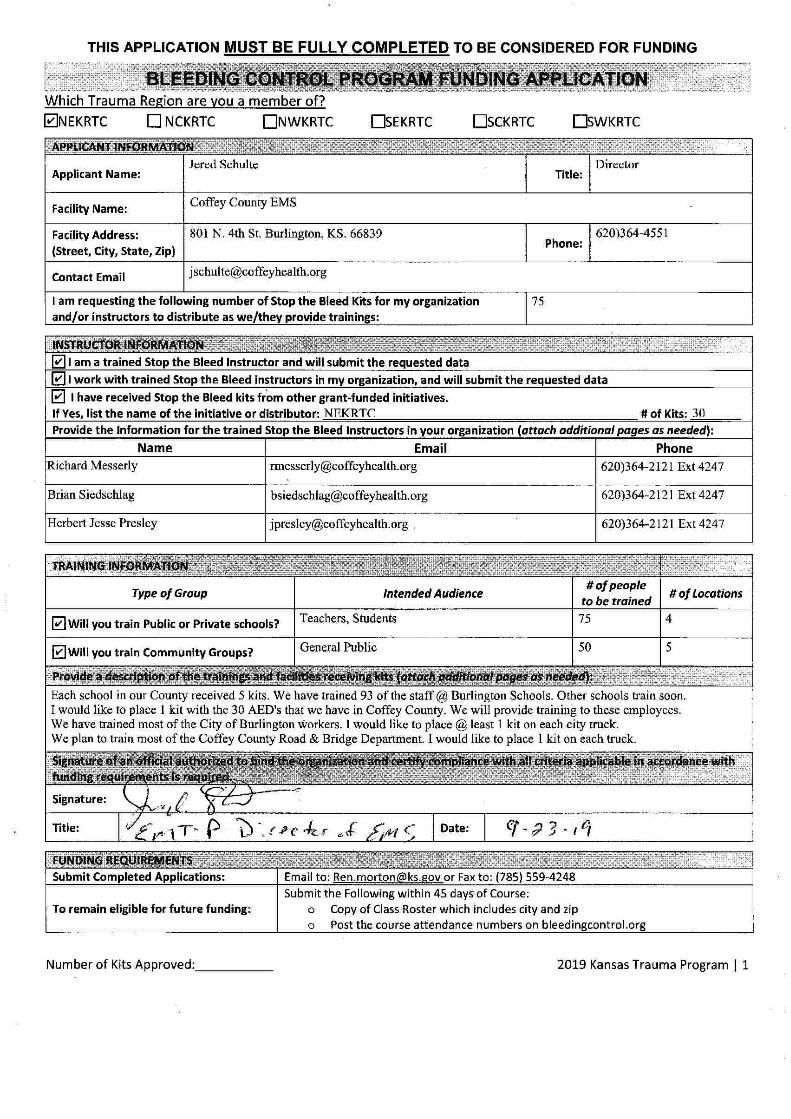
THIS APPLICATION MUST BE FULLY COMPLETED TO BE CONSIDERED FOR FUNDING
Number of Kits Approved:___________ 2019 Kansas Trauma Program | 1
Which Trauma Region are you a member of? ☐NEKRTC ☐ NCKRTC ☐NWKRTC ☐SEKRTC ☐SCKRTC ☐SWKRTC
APPLICANT INFORMATION
Applicant Name:
Title:
Facility Name:
Facility Address: (Street, City, State, Zip)
Phone:
Contact Email
I am requesting the following number of Stop the Bleed Kits for my organization and/or instructors to distribute as we/they provide trainings:
INSTRUCTOR INFORMATION I am a trained Stop the Bleed Instructor and will submit the requested data I work with trained Stop the Bleed instructors in my organization, and will submit the requested data I have received Stop the Bleed kits from other grant-funded initiatives.
If Yes, list the name of the initiative or distributor: _________________________________________________ # of Kits: ________ Provide the Information for the trained Stop the Bleed Instructors in your organization (attach additional pages as needed):
Name Email Phone
TRAINING INFORMATION
Type of Group Intended Audience # of people to be trained # of Locations
Will you train Public or Private schools?
Will you train Community Groups?
Provide a description of the trainings and facilities receiving kits (attach additional pages as needed):
Signature of an official authorized to bind the organization and certify compliance with all criteria applicable in accordance with funding requirements is required.
Signature:
Title: Date:
FUNDING REQUIREMENTS Submit Completed Applications: Email to: [email protected] or Fax to: (785) 559-4248
To remain eligible for future funding: Submit the Following within 45 days of Course:
o Copy of Class Roster which includes city and zip o Post the course attendance numbers on bleedingcontrol.org
BLEEDING CONTROL PROGRAM FUNDING APPLICATION
✔
✔
✔
✔
Teresa Taylor
Stormont Vail Health
1500 SW 10th Ave 785.354.5428
Trauma Prevention/Education
140
please see attached list
Staff/Faculty of USD 501 (Topeka Public Schools)
Topeka Public Schools is the largest district in Shawnee Co, serving approximately 14,000 students. There are over 1,300 teachers and1,100 support staff serving 6 high schools, 6 middle schools, and 15 elementary schools. We are requesting one bleeding control kitper 100 students. Our goal is to train 20%, or 480, of the School District's faculty and staff by June of 2020.
Trauma Prevention Coordinator and Outreach Educator 8/19/2019
Teresa D. Taylor Digitally signed by Teresa D. Taylor Date: 2019.08.19 14:23:01 -05'00'
JïL/3g/2g1T/TïE ?X
THIS APPLICATION MUST BE FULLY COMPLETED T0 BE CONSIDERED FOR FUNDING
BLEEDING CONTROL PROGRAM FUNDING APPLICATIONW hich Traurna ReRion are vou a member of?ZNEKRTC EEI NCKRTC U NWKRTC FA EKRTC F-ISCKRTC O WKRTCAPPLICANT INFORMATION
Mary Lybane RN. Trauma Coel'dllqakorApplican: Name: Title:
Facility Name: ColnmuniLy Memoriitl Healthcare
Façillty Address: 70s h! j 8th st, Marysville, K8 66508 785-562-23 1 IPhone:(Street, Clty, state, z1p)
contact Emall 1Mtlylàa!1e@ c)nlAcah'e.o$'g
I am requesting the following npmber of Stop the Bleed Klts for my organizatlon 30()and/or instructors to distrjbuîe as we/the provide 4rajnlngs:
INSTRUZtDR CNFORNI YION1-1e I am a tralned Stop the Bleed lnstruttor and will submit 1he requested data(Zl 4 workwith traineu Stop the Bleed instruuors In trly organization, anu will submit 1he requested data
I have received stop the Bleed kits from other grant-funded initiatives.If Yes, Iist the name of 'he Inltiative or distribnsor; # of Itits:Provide the Irlformation for tbe lralned Stop the Bleed Instructors in yoklr organlzatiorl futtach addiçionulpuges (J
.ç neededtjName Email Phone
John Ryan MD [email protected] 785-562-23 l 1
Jill Ryan RN jdïyamm@zmail,com 785-562-8536
Rose 8helburne RN 785-562-23 I 1
TRAINING INFORMATION 1
# ofpeopleType o.f Group Intended Audlence # o.f Locutîonsto be trp3nerl
IZ WIII you train Public or Prlvate schools? Superintendents. Prinlcipalsq Teachers. Coaches 400 1 0
r7/ WiII you train communlty Groups? Chklrches. Fil'e Depts, Yeuth groups 1 50 I 6
ptevidb a' degeflptlon of the trainings aad facllltles receiving kits fatttch ctfétfopclpggè.ç us neetfetfllszqt attached sheet
signatilre of hn offlûlàl âttthoeizêd to bind the orgàqizatio: and certlfy tofnpliance wîthfall crlterla applicable in atcoidance wlthf litllng re4 ifemilnt: ls r ulr:cl. 'usignature:
Title: RN, Trauma N rdintttor Date: 7/30/20 l 9
FONDING REQUIREMENTS ''submlt Completed Applicatiops! Email to: Relh mo! ton tillls Qtbt or Fa: to; (785) 559-4248
Submitthe Fojsowing within 45 (lays of Course:To remain eligible for future funding: o Copy of Class Roster which incltldes city arld zip
o Post tlle course attendance numbers on bjeedingcontrol.org
Number clf Kitî Approved: 2019 Kansas Trauma Progral'n I 1

JïL/3g/2g1T/TïE ?X
INSTRUW OR INFORMATIONCurrent Stop the Bleed Instructors (continuedl:Sandra Keller/ RNKay Richardson, RN
stop the Bleed Instructors To Be Added bv Fall 2019:Randall Brown? MDJohn l-laefele, MDPhll Caswell, RTM ike Stech, CRNABecky Heuer, APRNAshley Swearingen, RNM aria îeematter, RN
TRAINING INFORM ATIONSchools:
Community Memorial rlealthcare (CMH), Iocated in Marysville, KS, is the sole hospital in Marshall County. Over9,000 people call this rural area home and depend on CMH for their health care needs. The county boasts manyfamily farming operations expanding over several generations as well as several industrial and agriculturalindustries.
Marysville USD 354 has one public elementary school and two parochfal elementary schools as well as a publicJr./5r. High School. Our aim is to teach stop the Bleed classes for staff members at each school to includeprincipals, teachers, para-professionals, coaches, bus drivers, janitors, and office staff. Approximately 150individuals will receive training in USD 364. Classes w'Il be offered in Fall/winter 2019.
Valley Heights USD 498: sewing the communities of Blue Rapdds and Waterville, has one elementary school andone Jr./Sr. High school. Stop the Bleed classes will also be provided jn this dtstrict for principals, teachers, para-professionals, coaches, bus drivers, janitors, and office staff. Approximately 100 individuals will receive trainingin USD 498. Classes will be offered in Fall/Winter 2019.
UsD l13 and USD 380 have education centers spanning both Marshall and Nemaha counties in Kansas. W e may
expand our training classes to include these districts in 2020 but at this time our focus is primarily to get trainingout to those education facilities located speclfically in Marshall County. If added, this would encompass trainingof approximately 150-200 individuals,
communitv Groups:As in most rtlral communities, churches and volunteer organizations play a Iarge role in helping a community tothrive. Our area has several church denominations who, in addition to regular weekly sewices
, also open theirdoors for a variety of community events. A1I of the communities in the county also depend on volunteers fortheir local fire departments. W e plan to o'ffer Stop the Bleed classes to these community groups in Fall/Winter2019 and anticipate a minimum of 75-100 individuals to receive training.
We also have several industrial and agricultural industries within the county who would greatly benefit fromStop the Bleed training. Our goyl is to offer training for approximately 200 employees of these businesses in2020.


2019-07-26 08:59 Sabetha Fospitat 7852841595 >> KDFE P 1/1
THIS APPLICATION MUST BE FULLY COMPLETED TO BE CONSIDERED FOR FUNDING
1. BLEEDING CONTROL PROGRAM FUNDING APPLICATION hW hlch Trauma Recion are vou a membes of'?C;d NEKRTC F3 NCKRTC CIN V/KRTC CXEKRTC FRSCKRTC EXV/KRTCAPPUCANT INFORMATION
lenna Mcclain xtle: Director o NursingApplicant Name:
Faclllty Name: Sabetha Cemmunity Hpspital
Façlllty Addfessl 14th a oregon Sabetha, KS 66534 jjone: 785-224-1626P(street/ citw State, zlp)
contact Email jmcclain@sabeth:tospital.comI am reqvesting tHe followlng number of stop the Bleed Kits f@r my organlzatlon zjand/or Instrslctors to distrlbute as we/the provlde trainlngs;
IINSTRUW OR INFORMATION . 'IZ 1 af!l a trained stop &he Bleed Iestfudor and will submlt 1he reqpested data Ir-l I work with trained stop the Bleed Instrklcto/s irl my ofganlzatlon. and w1l1 submit the requested data I
I-''Z l have recelved Mop the Bleeu kits from other grant-fun:e: Tnitsative?. jf Yes 11st the name of the initiative or dlstrlbutor: Northczst Healttlcare Loalltlon f xits; 2QI : # t)Provide rhe Informatlon for the trained Stop the Bleed Instrudors In wur organization fottach tpdd/t//a//p/ge,i JJ neededt,
Name Email I Phone
Llnnae Coktr [email protected] 725-224-1512KAtq Goodman kgoodmAn@sabttl:alAospîtal.com 785-2:41623
ITRAINING INFORMATION
# o/geople jType ofGroup IntendedAudlencn # oliqcvtlonstp be tzlgaed
I'Z wlll you train Peblic o/ Prlvate schools? A1I Dlstrlct Staff 250 5
I'Z Will you train Communlty Groqps? Al1 Manufacturing Plants and Church Groups '? 8provide'a desçrlptlon of ttïe tralnlngs and facllltles reçelvlng kits tgtt/cà qddltlonulpuge.% J.$ neededtt
.
School Distrsct Classified staffto be trained $/14/19, teacllers to be trained at a later date.Manufacturing Plant stafftrainings being scheduled currenlly, Approxîmately 7 plants with multiple Iogaîions.The largest church is creating a rapld response team and will be dolng training in tht near future.
slgnatufe of an offlçlal avthorized to'bind 9he organlzaylon and certif'y compllance wlth a11 çrlterla applicable in aetofdance w1thfundin re ulrements ls required. ' ' ' .
:
slgnature: c e (Mtle: 'p ob.l Datel 7-J #-/j
IFUNDING REQUIREMENTSSubmit completed Ap Ileatlons: Emall t0: Ren.rnorton ks, ov or Fax to: 785 559..4246 I
Submlt the rollowing wlthln 4S days of Course:To remain eligible forfuture funuing: (J copy of Class Roster whicb lncludes clty and zip
o Post thc coklrse attendance numbers on bleedln contrtll.or
Number of Klys Approved: 2019 Kansas Traklma Program 1 l

Ju1/22/2019 10.39.27 AM St Francis HeaIth - ER 785-295-5505
TBIS APPLICATIQN MUST BE FULLY COMPLETED TO Be CQNSIDERED F5R FUNDING
PROGRAM FUNDING APPLICATIONW hich Trauma Reqion are vokl a member of?NEKRTC E1 N CKRTC EINV/KRTC ZDEKRTC EJSCKRTC CYV/KRTCAPPLICANT INFORMATION
Appllcent Namel ( Tltle:$ &IIJ: û bl:aaltyxame, - gitwt (.kFaclllty Address:
tstreet cpty, state, zlp) ' o 'V -1-9 O Pbtme; --$()(7.;-j.d(?-@x 1eontact Emall ywuft . (; . (,i am requestlng the followlng number ef Stop the Ieed Kits for my organizationand/or Instructots to distrlbute as we/the rovlde 'trainings: 1INSTRUW OR INFORMATIONI am * trained Stop y'he Bleed Instructnr and wlll submlt the requested dataI work wlth ttained 5top tbe bleed Instrncto/s in m or anlzation: and wlll submit the re uested data1 bave recelved stop the Bleed kits from other gfant-funded Inltlatîves.
tf Yew tist tha namq of the irûtlMive er dlstrtbutort #: of KhslProvlde ttye Irlformatlon fof the trelned stop the Bleed Insttuctors In our otganizatlon Lqttqch J##/t/oncl J el G
.ç needed :Name Emall PhQne
pqhh t . t a c, . q - -
TRAINING INFORMANON
# ofpeoplerype ojGroup lnfetlded Audfençe # vf tec/tlon:to be trlfrle/
wlll you ttain Publlc or Private schools? ():$4:p UZL.URwlll you train commtlnitycroups; jemds ljcl g. UM.L
-
Provide a descrlption of the traïnings and facllises regalvlng klts (cttlc?l uddltlontl plge.ç as needed):
r$ :4(4 ,1p klô Al.ts -? &, 4: * z, 4.'qî vs wtbu zyb.t- be cuçi<ta' P>-.e ï?h '/' .
sîgnature of a il utherlzed to hirld the organlzpsion and certlfy compliance wlth aII criterla appllcable in accordence withfundin re ei em s r ' ed
S Ign a t u r e t azzc'r's'-
q #'TITIe; V ,,.,. Datel .. .,.Z/'-' z
FUNDING REQUIREMENTSSubmit Com leted Appllcatlons: Email te: en.morto , ov or Fax to: 785) 559-4248
Submlt th: Foltowing wlthln 45 uays of Coursek'ro remaln allglble for future fgndîng: o Copy of Cless Roster whlch lncludes city and zIp
(z Pôst the course attendance numbers ön bleedln contfolvorg
BLEEDING CONTROL
Number of Kits Approved: 2019 Kensas Trauma Progrnrth j 1

FE2/2#/2g1J/Tïr )X
THIS APPLICATION M UST BE FULLY COMPLETED TO BE CONSIDERED FOR FUNDINGc'A?16
Traum a Educptibn Funding R equest Application
Which Reqional Trauma Counci I are you a member of'?
ZNEKRTC Z NCKRTC ZNWKRTC ZSEKRTC HSCKRTC ZSWKRTCAPPLICANT INFOXM ATION
Rebecca Heuer APRNApplicant Name: Title:
Faciliiy Name: Comluuaity MelRRc)l'îa.l llealtllcare
Facility Address: 708 N , 8th Marysville, Ks 66508 jj 785-562-23 l 1P one:
(street, cit'y, state, zip)Contact Email [email protected]
r-1/' Y e s - L e v e l IVYour Facilitr's Trauma Designation: U-l Workillg Toward Designation Level
No; not traulma desi nated at th is tilme.
'CHOOSE COURSE 'Fybu lpa only fldfclzfe ()tle caurse er qp Ikccfffpn,/' Advanced Trauma Life Support (ATLS)ATLS Provider: Rebecca Hetler Cfedentials: U-I MD I--I DO IW APRN U1 PAxd * ç/-Lèllqt ()/%z# 7-1:15' l'Lïizij'tl't'ti (?;? l'Lï6l l/d/'d! r?l ilïcliçïcltîllfï n7-!2-!//'12(? 6h(7.ç/.Registration Cost: $ 695 . 'j6lit /: :7 ltobcïtik,l:Does ANY employer rovide CME support? I-lYes 1--17 Nô
Prehospital Trauma Life Su @rt (PHTLS)Trauma Nursing Core Course TNCC)Rura) Trauma Team Develo ment Course (RTTDC
COURSX INFORM ATIONCourse Dates: From 7- 1 j -201 9 To 7- 1 1-201 9Course Location: Bryan Health, Lincoln. Ne
Have yOu received funding for this eourse in the past? F7 Yes IZ NoW ill this course be OPEN to others in tlle re ion? IZ Yes r-I NoWill this course be made AVAILABLE to others in the re ion? IZ Yes r7I NoPléase rtlvjde a statemeat on tlte RBACI for tlte itlaàs or lltlw it bellefit.s ottr re ioq's traqm? gystem:Rrbecca Heuer APRN works it'l the Emcrgency Department more than any other provjder. She cares for the majority of thc trauma's thRt
' ' 1 IV 'entel 01.1l Leve .
Signature of an official authorized tt) bind thû organization and certify compliance with aII criteriaa lieable ih accordance with ftlndjng reqtlirelaeats is' re uired.Slgnatur '
Title: EDfl-raulta Coordinator Date: 02/24/2019
Approved by Region (Date/lllitials): 20 1 8 Kallsas Tratllpa Progralm r l
FE2/2#/2g1J/Tïr )X
THIS APPLICATION MUST BE FULLY COMPLETED TO BE CONSSDERED FOR FUNDING
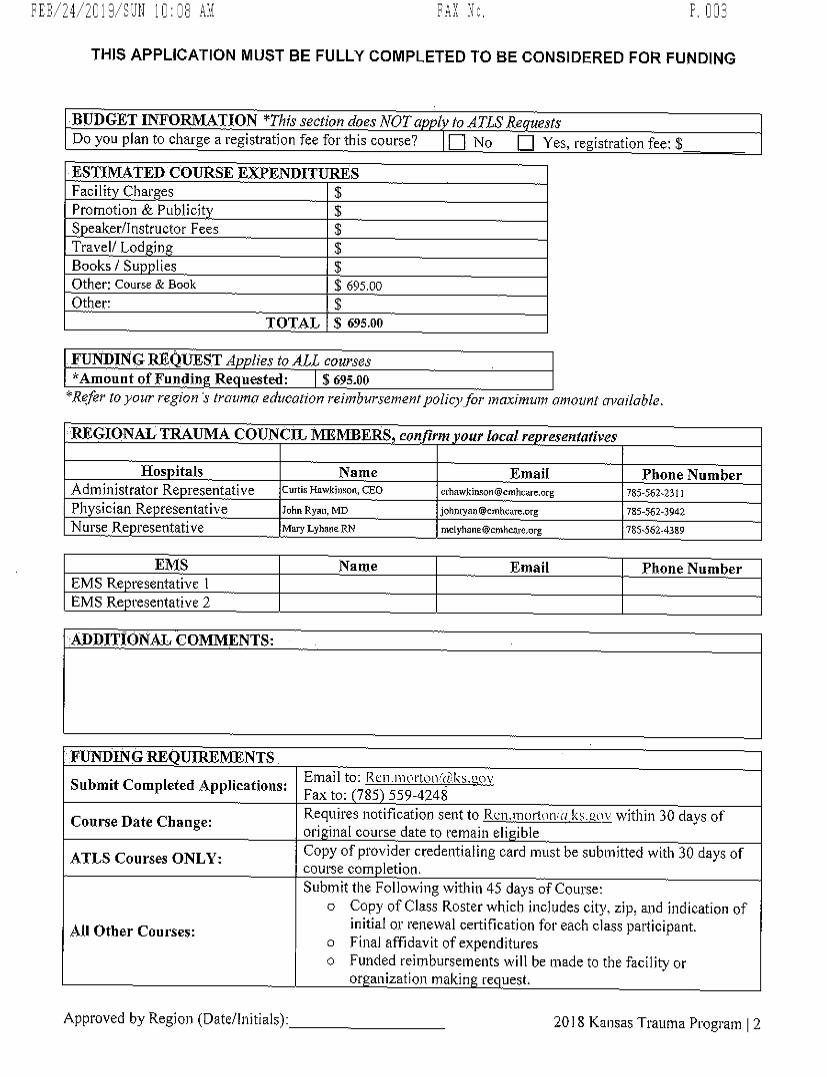
BUDGET INFO TION Bl-his section does NO1'a I to ATLS Ac uestsDo you plan to charge a registration fee for this course? U1 No 1-1 Yes, registration fee: $
ESTIM ATED COURSE EXPENIIITURESFaci lit Char es $Prolmotion & Publsokt $S eaker/lnstructor Fees $Travel/ Lod in $Books / Su lies $Other: Course & Book $ 695,00Other: $
TOTAL $ 695.00
FIJNI/NG REQU/ST -4 lies to ALL cx rwVrAmount of Fundin Re uested: $ 695.00''Rqfèr to ywzfr regipn b' trauma ddl/ct-/rjt)?z reimbursemçmt
.ptlfjclz for ?plzfzpz/p anlounf cl?c/?'flé/lt?.
REGIONAL TM UM A COUNCIL IVIEM BERS con lrm our Incal rg reszntatives
Hos ltals Name Email rhone NumberAdmînistrator Re resentative Curtis Hawkicsoq, cEo crbawkipwn@cohcare,or: 785-56:-231 lPh sician Re resentative 7vhn Ryan, MD johne,n@cmhctuxsorg 7:5-:62-3942Nurse Re resentative Mary Lyh,ne RN mclyhaqe@cmhcare,vrg 785-562-4389
EM S Name Email Phone NumberEM S Re resentativr 1EM S Re resentative 2
ADbITIONAL COMMENTS:
R INIO GREQIJIREMENTSElmai l to : 1.1 f.:r 1.1 . I 11 e rtoll '-.(? k s . u ovSubmit Completed Applieations:Fax to: 78$ 559-4248Requires notiGcatson sent to IleIn.1:l()dt1l'1.'tp.!1s.k)t% within 30 days ot-Course Date Change:ori inal course date to rtlmain eli ibleCopy of provider credential ing cal-d 1>1.1st be subm itted with 30 days ofATLS Courses ONLY:
.coulse com letion,Submit the Following within 45 days of Course!
Copy of Class Roster which iaoludes citys zip, and indication ofinitial or renewal certitscatjon for each class participallt.All Other Coarses:Final affidavit of expendituresFunded reimbursements wi l I be nqade to the faci l ity oror anization maltin re uest.
Approved by Region (Date/lnitials): - 20 I 8 Kallsas Trauma Progl'am l 2



THIS APPLICATION MUST BE FULLY COMPLETED TO BE CONSIDERED FOR FUNDING
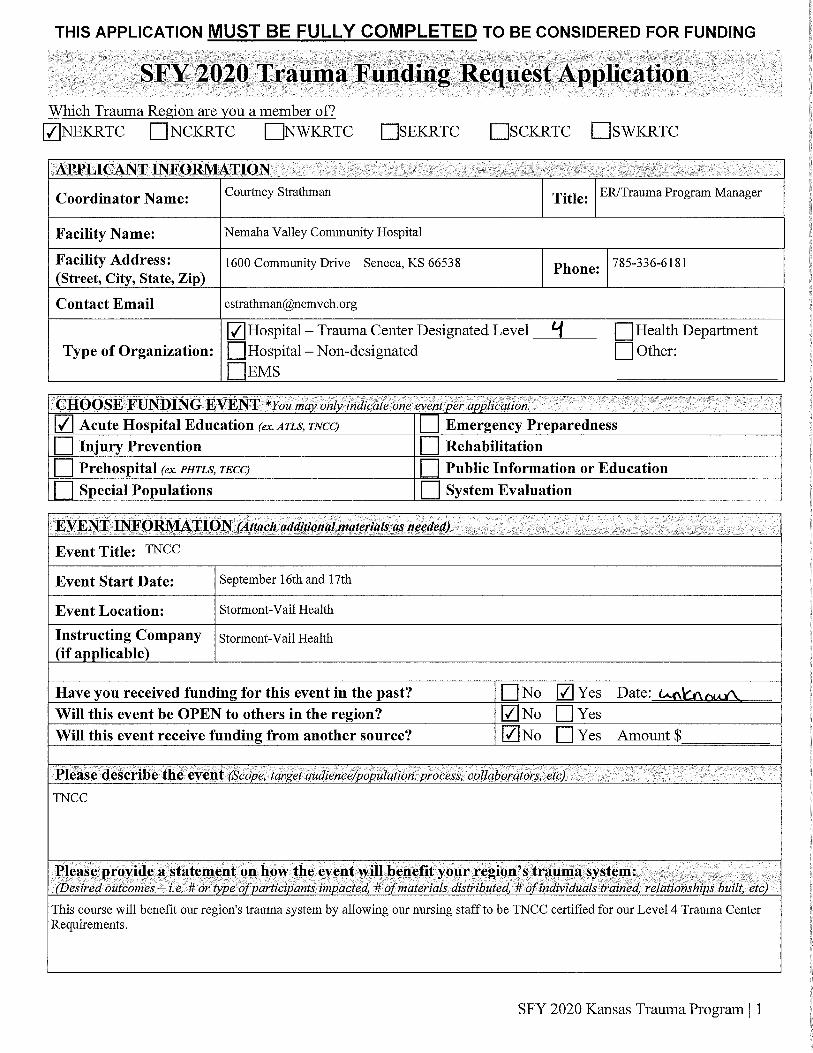
SFY 2020 Kansas Trauma Program | 1
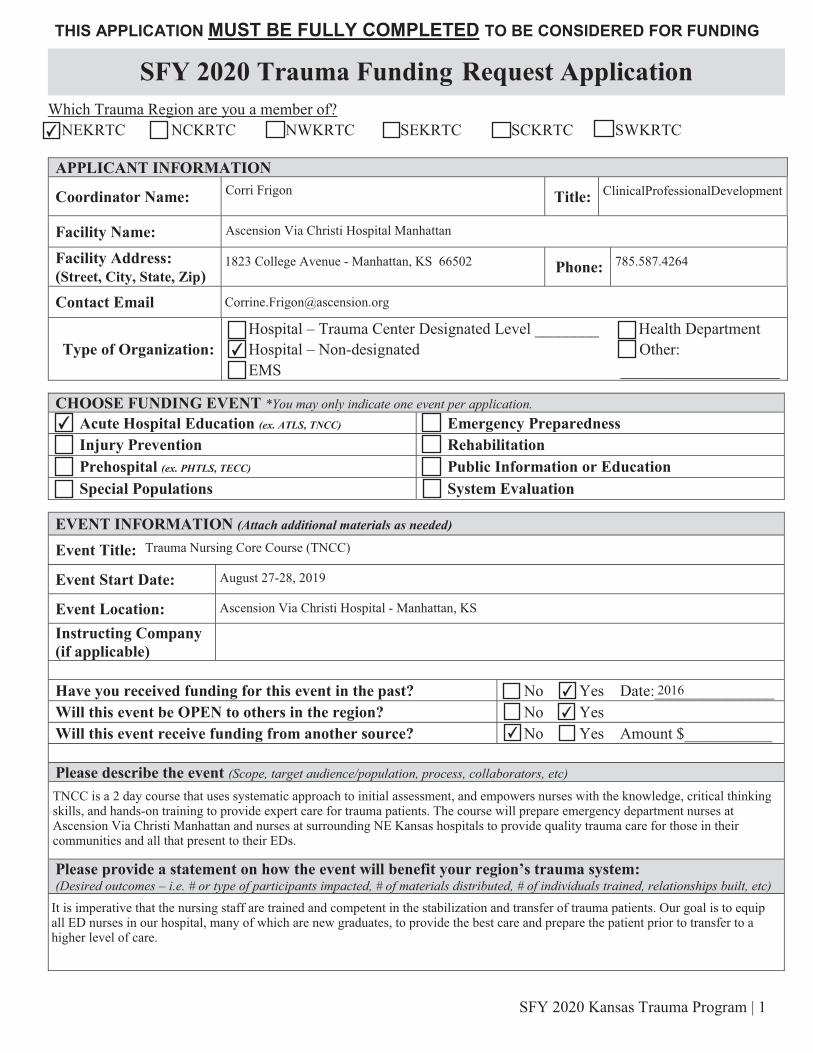
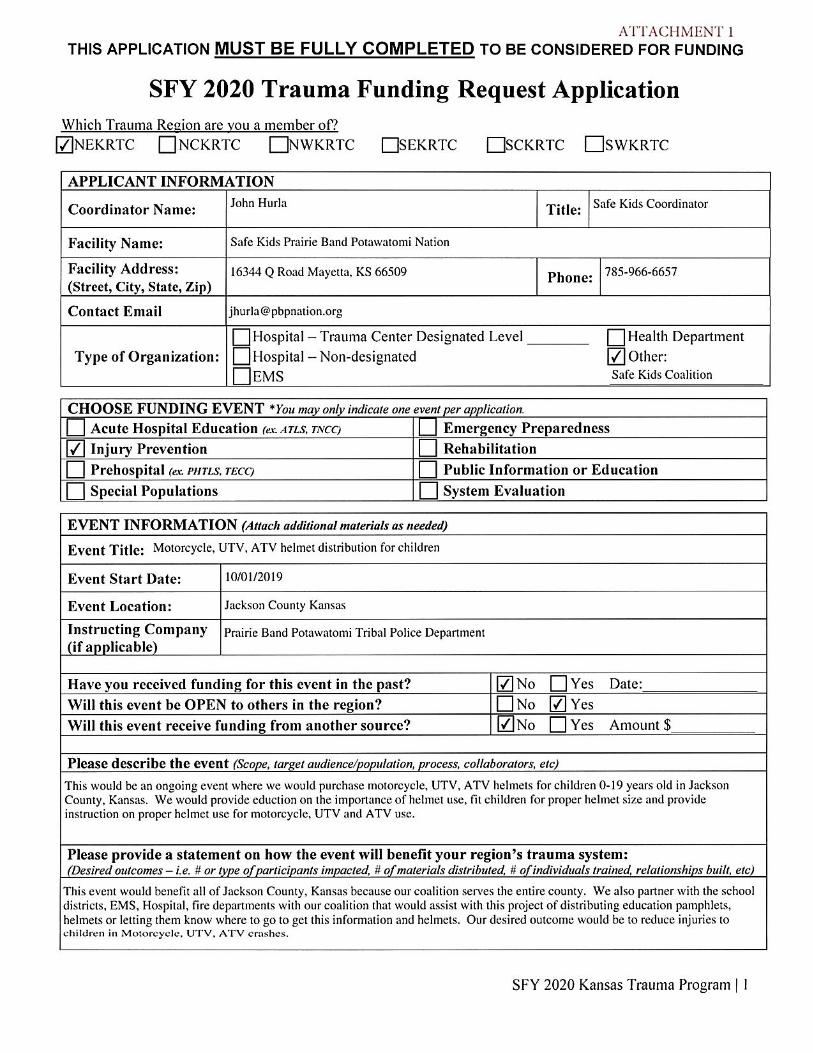
Which Trauma Region are you a member of? ☐NEKRTC ☐ NCKRTC ☐NWKRTC ☐SEKRTC ☐SCKRTC ☐SWKRTC APPLICANT INFORMATION
Coordinator Name: Title:
Facility Name:
Facility Address: (Street, City, State, Zip)
Phone:
Contact Email
Type of Organization: Hospital – Trauma Center Designated Level ________ Health Department Hospital – Non-designated Other: EMS ____________________
CHOOSE FUNDING EVENT *You may only indicate one event per application. Acute Hospital Education (ex. ATLS, TNCC) Emergency Preparedness Injury Prevention Rehabilitation Prehospital (ex. PHTLS, TECC) Public Information or Education Special Populations System Evaluation
EVENT INFORMATION (Attach additional materials as needed) Event Title:
Event Start Date:
Event Location: Instructing Company (if applicable)
Have you received funding for this event in the past? No Yes Date:_______________ Will this event be OPEN to others in the region? No Yes Will this event receive funding from another source? No Yes Amount $___________ Please describe the event (Scope, target audience/population, process, collaborators, etc)
Please provide a statement on how the event will benefit your region’s trauma system: (Desired outcomes – i.e. # or type of participants impacted, # of materials distributed, # of individuals trained, relationships built, etc)
SFY 2020 Trauma Funding Request Application
✔
Corri Frigon ClinicalProfessionalDevelopment
Ascension Via Christi Hospital Manhattan
1823 College Avenue - Manhattan, KS 66502 785.587.4264
✔
✔
✔
Emergency Nursing Pediatric Course (ENPC)
October 22-23, 2019
Ascension Via Christi Hospital - Manhattan, KS
✔
✔
✔
2016
ENPC is a 1.5 day course that uses systematic approach to initial assessment, and empowers nurses with the knowledge, criticalthinking skills, and hands-on training to provide expert care for pediatric trauma patients. The course will prepare emergency nurses atAscension Via Christi Manhattan and nurses at surrounding NE Kansas hospitals to provide quality trauma care for their community.
It is imperative that the nursing staff are trained and competent in the stabilization and transfer of trauma patients. Our goal is to equipall ED nurses in our hospital, many of which are new graduates, to provide the best care and prepare the patient prior to transfer to ahigher level of care.
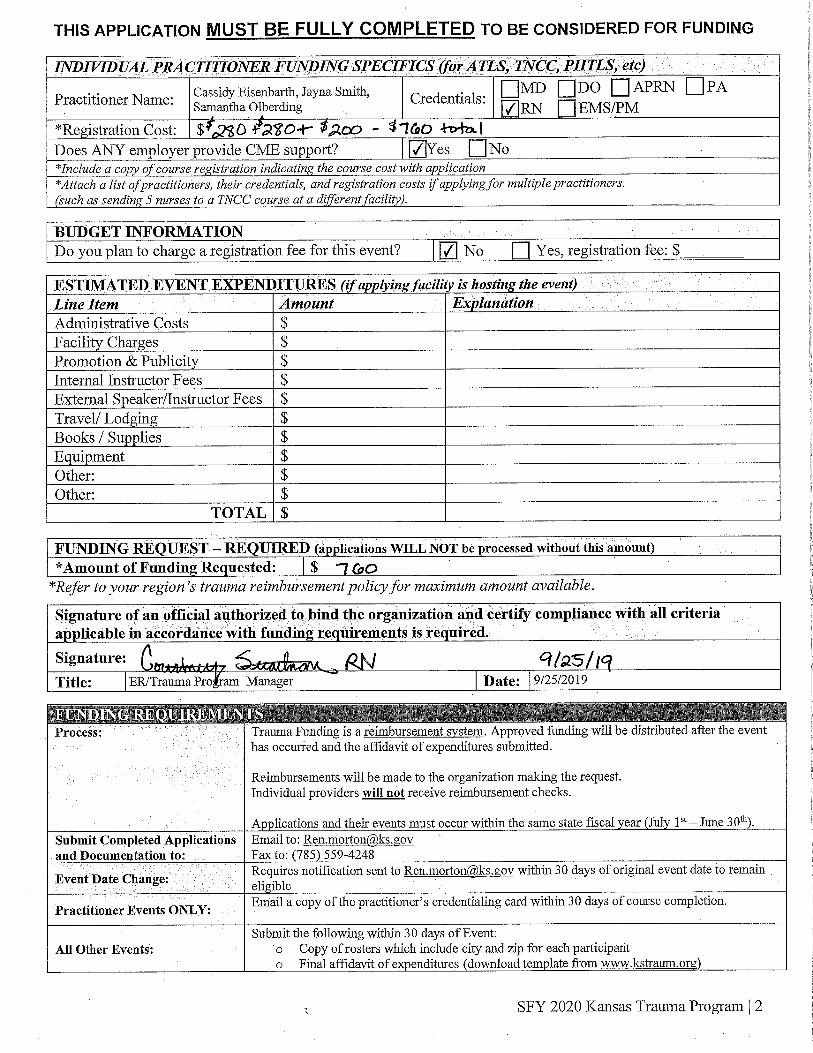
THIS APPLICATION MUST BE FULLY COMPLETED TO BE CONSIDERED FOR FUNDING
SFY 2020 Kansas Trauma Program | 2
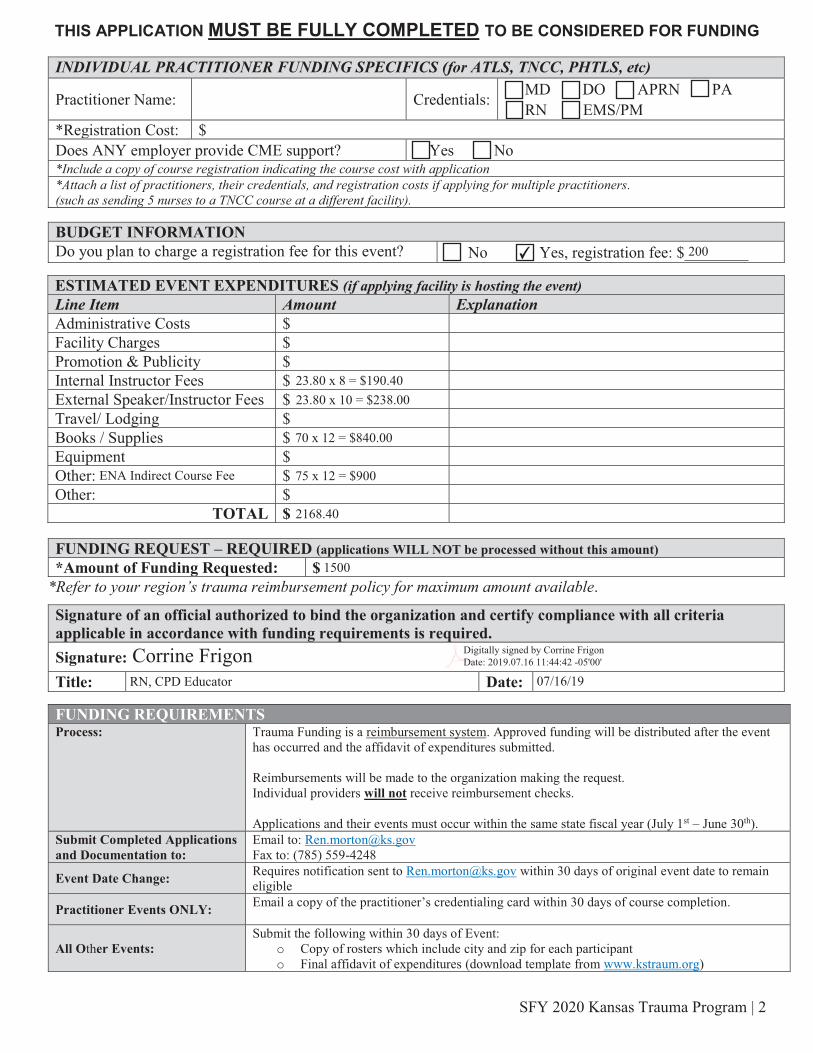
INDIVIDUAL PRACTITIONER FUNDING SPECIFICS (for ATLS, TNCC, PHTLS, etc)
Practitioner Name: Credentials: MD DO APRN PA RN EMS/PM
*Registration Cost: $ Does ANY employer provide CME support? Yes No *Include a copy of course registration indicating the course cost with application *Attach a list of practitioners, their credentials, and registration costs if applying for multiple practitioners. (such as sending 5 nurses to a TNCC course at a different facility).
BUDGET INFORMATION Do you plan to charge a registration fee for this event? No Yes, registration fee: $________
ESTIMATED EVENT EXPENDITURES (if applying facility is hosting the event) Line Item Amount Explanation Administrative Costs $ Facility Charges $ Promotion & Publicity $ Internal Instructor Fees $ External Speaker/Instructor Fees $ Travel/ Lodging $ Books / Supplies $ Equipment $ Other: $ Other: $
TOTAL $ FUNDING REQUEST – REQUIRED (applications WILL NOT be processed without this amount) *Amount of Funding Requested: $
*Refer to your region’s trauma reimbursement policy for maximum amount available.
Signature of an official authorized to bind the organization and certify compliance with all criteria applicable in accordance with funding requirements is required. Signature: Title: Date:
FUNDING REQUIREMENTS Process: Trauma Funding is a reimbursement system. Approved funding will be distributed after the event
has occurred and the affidavit of expenditures submitted. Reimbursements will be made to the organization making the request. Individual providers will not receive reimbursement checks. Applications and their events must occur within the same state fiscal year (July 1st – June 30th).
Submit Completed Applications and Documentation to:
Email to: [email protected] Fax to: (785) 559-4248
Event Date Change: Requires notification sent to [email protected] within 30 days of original event date to remain eligible
Practitioner Events ONLY: Email a copy of the practitioner’s credentialing card within 30 days of course completion.
All Other Events: Submit the following within 30 days of Event:
o Copy of rosters which include city and zip for each participant o Final affidavit of expenditures (download template from www.kstraum.org)
✔ 200
23.80 x 8 = $190.4023.80 x 10 = $238.00
70 x 12 = $840.00
75 x 12 = $900
2168.40
ENA Indirect Course Fee
1500
Corrine Frigon Digitally signed by Corrine Frigon Date: 2019.07.16 11:44:42 -05'00'
RN, CPD Educator 07/16/19

THIS APPLICATION MUST BE FULLY COMPLETED TO BE CONSIDERED FOR FUNDING
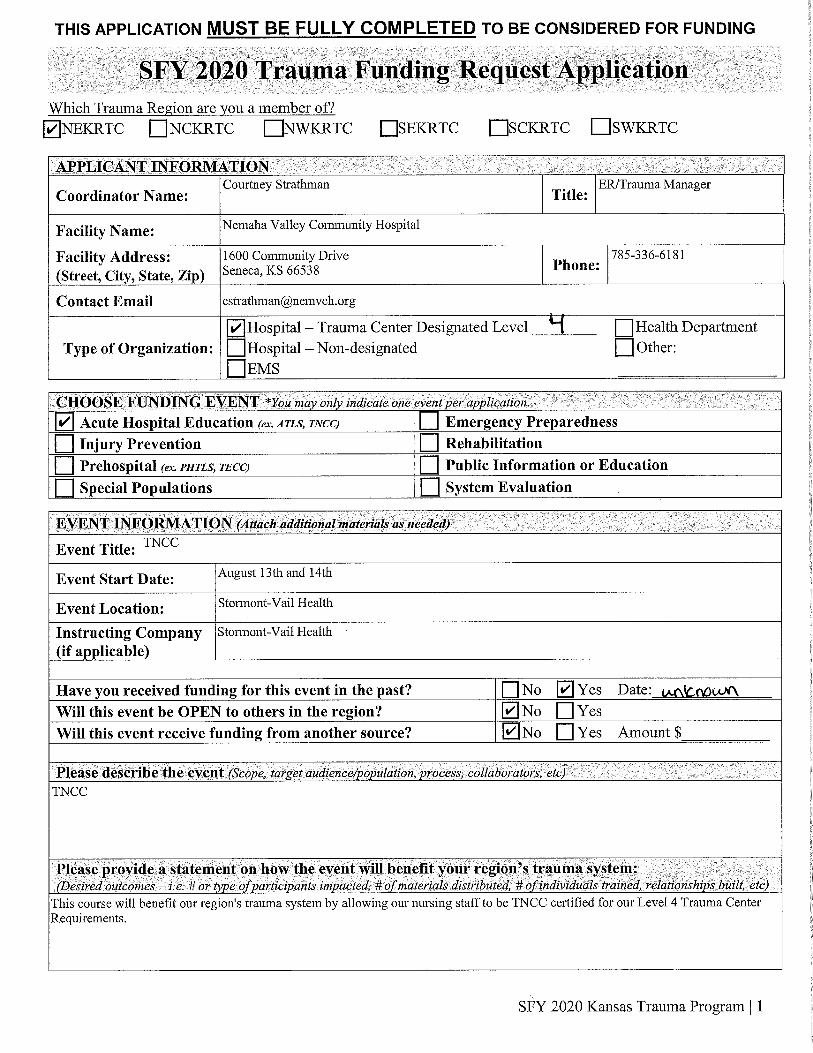
SFY 2020 Kansas Trauma Program | 1
Which Trauma Region are you a member of? ☐NEKRTC ☐ NCKRTC ☐NWKRTC ☐SEKRTC ☐SCKRTC ☐SWKRTC APPLICANT INFORMATION
Coordinator Name: Title:
Facility Name:
Facility Address: (Street, City, State, Zip)
Phone:
Contact Email
Type of Organization: Hospital – Trauma Center Designated Level ________ Health Department Hospital – Non-designated Other: EMS ____________________
CHOOSE FUNDING EVENT *You may only indicate one event per application. Acute Hospital Education (ex. ATLS, TNCC) Emergency Preparedness Injury Prevention Rehabilitation Prehospital (ex. PHTLS, TECC) Public Information or Education Special Populations System Evaluation
EVENT INFORMATION (Attach additional materials as needed) Event Title:
Event Start Date:
Event Location: Instructing Company (if applicable)
Have you received funding for this event in the past? No Yes Date:_______________ Will this event be OPEN to others in the region? No Yes Will this event receive funding from another source? No Yes Amount $___________ Please describe the event (Scope, target audience/population, process, collaborators, etc)
Please provide a statement on how the event will benefit your region’s trauma system: (Desired outcomes – i.e. # or type of participants impacted, # of materials distributed, # of individuals trained, relationships built, etc)
SFY 2020 Trauma Funding Request Application
✔
Corri Frigon CPD Educator
Ascension Via Christi Hospital Manhattan
1823 College Avenue - Manhattan, KS 66502 785.587.4264
✔
✔
Trauma Nursing Core Course (TNCC)
January 28-29, 2020
Ascension Via Christi Hospital - Manhattan, KS
✔
✔
✔
2016
TNCC is a 2 days course that uses systematic approach to initial assessment, and empowers nurses with the knowledge, critical thinkingskills, and hands-on training to provide expert care for trauma patients. The course will prepare emergency department nurses atAscension Via Christi Manhattan and nurses at surrounding NE Kansas hospitals to provide quality trauma care for those in theircommunities and all that present to their EDs.
It is imperative that the nursing staff are trained and competent in the stabilization and transfer of trauma patients. Our goal is to equipall ED nurses in our hospital, many of which are new graduates, to provide the best care and prepare the patient prior to transfer to ahigher level of care.
THIS APPLICATION MUST BE FULLY COMPLETED TO BE CONSIDERED FOR FUNDING
SFY 2020 Kansas Trauma Program | 2
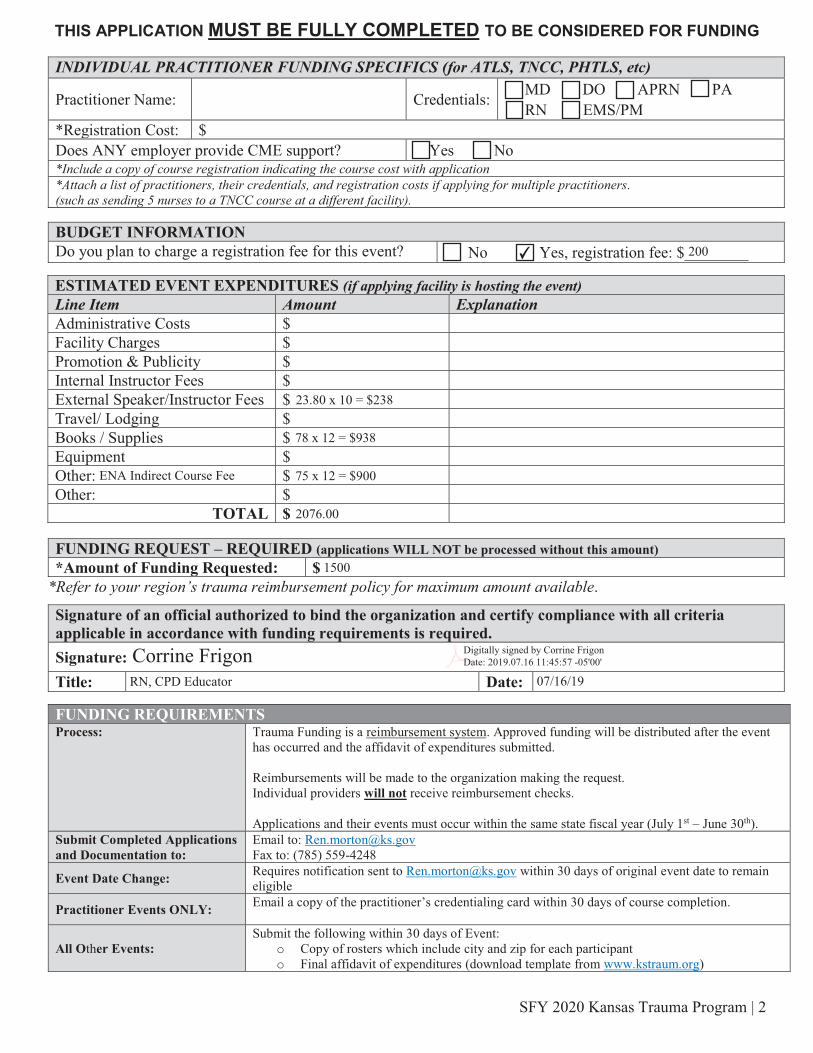
INDIVIDUAL PRACTITIONER FUNDING SPECIFICS (for ATLS, TNCC, PHTLS, etc)
Practitioner Name: Credentials: MD DO APRN PA RN EMS/PM
*Registration Cost: $ Does ANY employer provide CME support? Yes No *Include a copy of course registration indicating the course cost with application *Attach a list of practitioners, their credentials, and registration costs if applying for multiple practitioners. (such as sending 5 nurses to a TNCC course at a different facility).
BUDGET INFORMATION Do you plan to charge a registration fee for this event? No Yes, registration fee: $________
ESTIMATED EVENT EXPENDITURES (if applying facility is hosting the event) Line Item Amount Explanation Administrative Costs $ Facility Charges $ Promotion & Publicity $ Internal Instructor Fees $ External Speaker/Instructor Fees $ Travel/ Lodging $ Books / Supplies $ Equipment $ Other: $ Other: $
TOTAL $ FUNDING REQUEST – REQUIRED (applications WILL NOT be processed without this amount) *Amount of Funding Requested: $
*Refer to your region’s trauma reimbursement policy for maximum amount available.
Signature of an official authorized to bind the organization and certify compliance with all criteria applicable in accordance with funding requirements is required. Signature: Title: Date:
FUNDING REQUIREMENTS Process: Trauma Funding is a reimbursement system. Approved funding will be distributed after the event
has occurred and the affidavit of expenditures submitted. Reimbursements will be made to the organization making the request. Individual providers will not receive reimbursement checks. Applications and their events must occur within the same state fiscal year (July 1st – June 30th).
Submit Completed Applications and Documentation to:
Email to: [email protected] Fax to: (785) 559-4248
Event Date Change: Requires notification sent to [email protected] within 30 days of original event date to remain eligible
Practitioner Events ONLY: Email a copy of the practitioner’s credentialing card within 30 days of course completion.
All Other Events: Submit the following within 30 days of Event:
o Copy of rosters which include city and zip for each participant o Final affidavit of expenditures (download template from www.kstraum.org)
✔ 200
23.80 x 10 = $238
78 x 12 = $938
75 x 12 = $900
2076.00
ENA Indirect Course Fee
1500
Corrine Frigon Digitally signed by Corrine Frigon Date: 2019.07.16 11:45:57 -05'00'
RN, CPD Educator 07/16/19
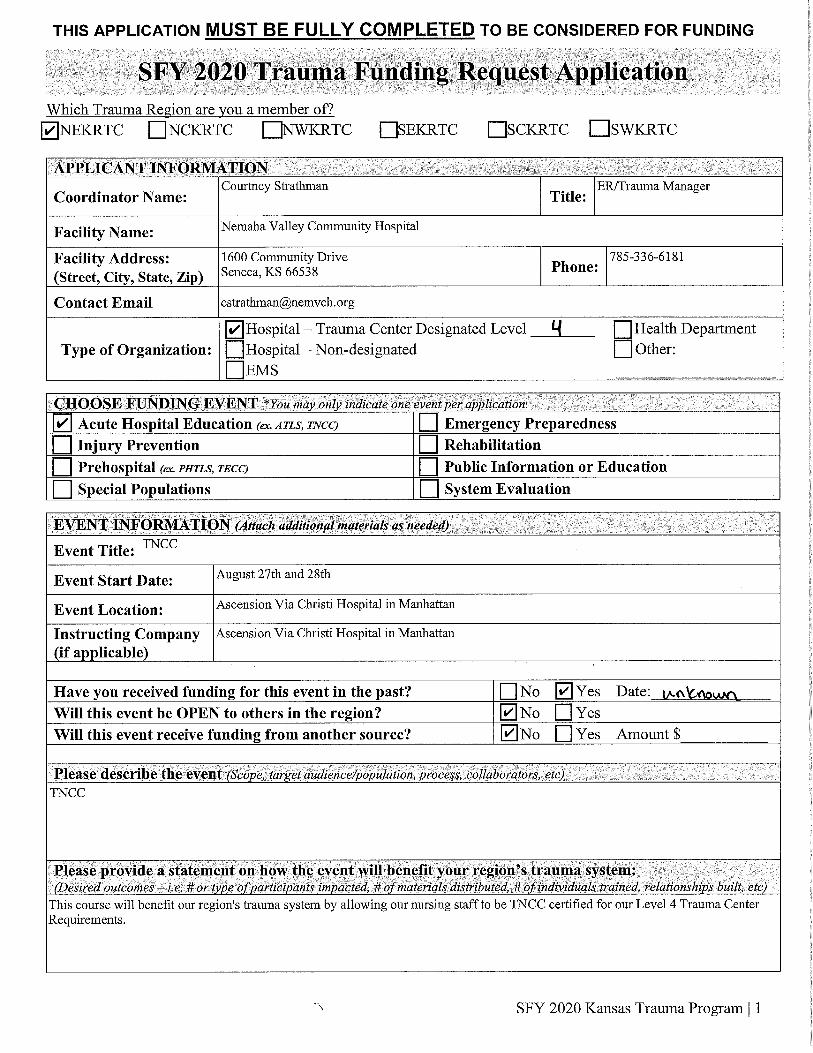
THIS APPLICATION MUST BE FULLY COMPLETED TO BE CONSIDERED FOR FUNDING
SFY 2020 Kansas Trauma Program | 1
Which Trauma Region are you a member of? ☐NEKRTC ☐ NCKRTC ☐NWKRTC ☐SEKRTC ☐SCKRTC ☐SWKRTC APPLICANT INFORMATION
Coordinator Name: Title:
Facility Name:
Facility Address: (Street, City, State, Zip)
Phone:
Contact Email
Type of Organization: Hospital – Trauma Center Designated Level ________ Health Department Hospital – Non-designated Other: EMS ____________________
CHOOSE FUNDING EVENT *You may only indicate one event per application. Acute Hospital Education (ex. ATLS, TNCC) Emergency Preparedness Injury Prevention Rehabilitation Prehospital (ex. PHTLS, TECC) Public Information or Education Special Populations System Evaluation
EVENT INFORMATION (Attach additional materials as needed) Event Title:
Event Start Date:
Event Location: Instructing Company (if applicable)
Have you received funding for this event in the past? No Yes Date:_______________ Will this event be OPEN to others in the region? No Yes Will this event receive funding from another source? No Yes Amount $___________ Please describe the event (Scope, target audience/population, process, collaborators, etc)
Please provide a statement on how the event will benefit your region’s trauma system: (Desired outcomes – i.e. # or type of participants impacted, # of materials distributed, # of individuals trained, relationships built, etc)
SFY 2020 Trauma Funding Request Application
✔
Corri Frigon ClinicalProfessionalDevelopment
Ascension Via Christi Hospital Manhattan
1823 College Avenue - Manhattan, KS 66502 785.587.4264
✔
✔
Trauma Nursing Core Course (TNCC)
August 27-28, 2019
Ascension Via Christi Hospital - Manhattan, KS
✔
✔
✔
2016
TNCC is a 2 day course that uses systematic approach to initial assessment, and empowers nurses with the knowledge, critical thinkingskills, and hands-on training to provide expert care for trauma patients. The course will prepare emergency department nurses atAscension Via Christi Manhattan and nurses at surrounding NE Kansas hospitals to provide quality trauma care for those in theircommunities and all that present to their EDs.
It is imperative that the nursing staff are trained and competent in the stabilization and transfer of trauma patients. Our goal is to equipall ED nurses in our hospital, many of which are new graduates, to provide the best care and prepare the patient prior to transfer to ahigher level of care.

THIS APPLICATION MUST BE FULLY COMPLETED TO BE CONSIDERED FOR FUNDING
SFY 2020 Kansas Trauma Program | 2
INDIVIDUAL PRACTITIONER FUNDING SPECIFICS (for ATLS, TNCC, PHTLS, etc)
Practitioner Name: Credentials: MD DO APRN PA RN EMS/PM
*Registration Cost: $ Does ANY employer provide CME support? Yes No *Include a copy of course registration indicating the course cost with application *Attach a list of practitioners, their credentials, and registration costs if applying for multiple practitioners. (such as sending 5 nurses to a TNCC course at a different facility).
BUDGET INFORMATION Do you plan to charge a registration fee for this event? No Yes, registration fee: $________
ESTIMATED EVENT EXPENDITURES (if applying facility is hosting the event) Line Item Amount Explanation Administrative Costs $ Facility Charges $ Promotion & Publicity $ Internal Instructor Fees $ External Speaker/Instructor Fees $ Travel/ Lodging $ Books / Supplies $ Equipment $ Other: $ Other: $
TOTAL $ FUNDING REQUEST – REQUIRED (applications WILL NOT be processed without this amount) *Amount of Funding Requested: $
*Refer to your region’s trauma reimbursement policy for maximum amount available.
Signature of an official authorized to bind the organization and certify compliance with all criteria applicable in accordance with funding requirements is required. Signature: Title: Date:
FUNDING REQUIREMENTS Process: Trauma Funding is a reimbursement system. Approved funding will be distributed after the event
has occurred and the affidavit of expenditures submitted. Reimbursements will be made to the organization making the request. Individual providers will not receive reimbursement checks. Applications and their events must occur within the same state fiscal year (July 1st – June 30th).
Submit Completed Applications and Documentation to:
Email to: [email protected] Fax to: (785) 559-4248
Event Date Change: Requires notification sent to [email protected] within 30 days of original event date to remain eligible
Practitioner Events ONLY: Email a copy of the practitioner’s credentialing card within 30 days of course completion.
All Other Events: Submit the following within 30 days of Event:
o Copy of rosters which include city and zip for each participant o Final affidavit of expenditures (download template from www.kstraum.org)
✔ 200
23.80 x 10 = $238.00
78 x 10 = $780
75 x 10 = $750
1768.00
ENA Indirect Course Fee
1050
Corrine Frigon Digitally signed by Corrine Frigon Date: 2019.07.16 11:43:32 -05'00'
RN, CPD Educator 07/16/19




2019-07-19 14:27 Coffey Co Fosp ER 620 364 2012 >> KDFE P 2/3THIS APPLIGATION MDST BE FULLY COMPLETED T0 BE CONSIDERED FOR FUNDINGr' '''r''''''''''''''''V71''''''''''''T ' ' . ' . i' . '.' ' ; F . ' h r ' j 2 f/2. ( l,k ( t, ,yj gj t f )1 j ,î jt) ,J,' LiL @ k : ) : ' $ ' . jl (' r lj t y: y ; k ;; j rj/.,' .ï. ' l j ' tj : j , ; ,., , ,. ,. 'j ' . ? Jh' ', ; ' ' t ' y ', $ ' j $ . j' ' y j . ', j '
)0$tTl f ' à ''à' '''m ' 'atryt 'u'u di''ng ''Rèqkùest, 'App -hcationl ,sFY) 202 , .,?W hich Trauma Recion are vou a member ooEINEKRTC EJNCKRTC EDNWKRTC EJSEKRTC EZSCKRTC EZSWKRTC
zf!kzl?' IE.II-, 1( 4::2-4!k1,$r 'J.7 )f 1,.1 )t? dt:)' ' $ ')(? 2124::), 1)11: t'I'èlz'i i''tif''? ' 1hi;' ).t!' (ïâ?-;7'(''yt:t r':f'( k' F' 7. '; -''F' ' à-ï9 p; 1-' 5?- '?' -; ' '' f' rs. ' $ . ''. ' . t - : ' /' '- ' ) ' ' '' .' $ ' ' '. . . ' .r h . $ ' ' . ) ' $ . . $pcred schulte cMS IlircctorCoordinator Name: Title:
Facility Namc: Coffey Ceunty EMS
Facility Address: s()l x. 4th st, Burlington, Ks. 66839 pjjone: 620*3644551(Strcet. Cl , state, ziCentact Email [email protected]
I-lHospital - Trauma Centcr Dcsignated Lcvel Health DcpartmentType ôf Organization: r-lHospital -Non-desûgnated Other:
/ EMS
CHOOSE Ft'rNDING EVE' NT bkjkbtibiti 1 'bk ''lkjpz/killlklhJkG# ihl liootio. .$ tk .$,k . . , ' ' ' 1Acutc Hospital Education lexAru, rNcc) Emem ency Pre aredness
Injur.y Prevention Rchabilitation1-17 Prchospital (e.< zzzzrzz', rEco Public Informatien er Educatien
Spccial Pôpulations System Evaluatlon
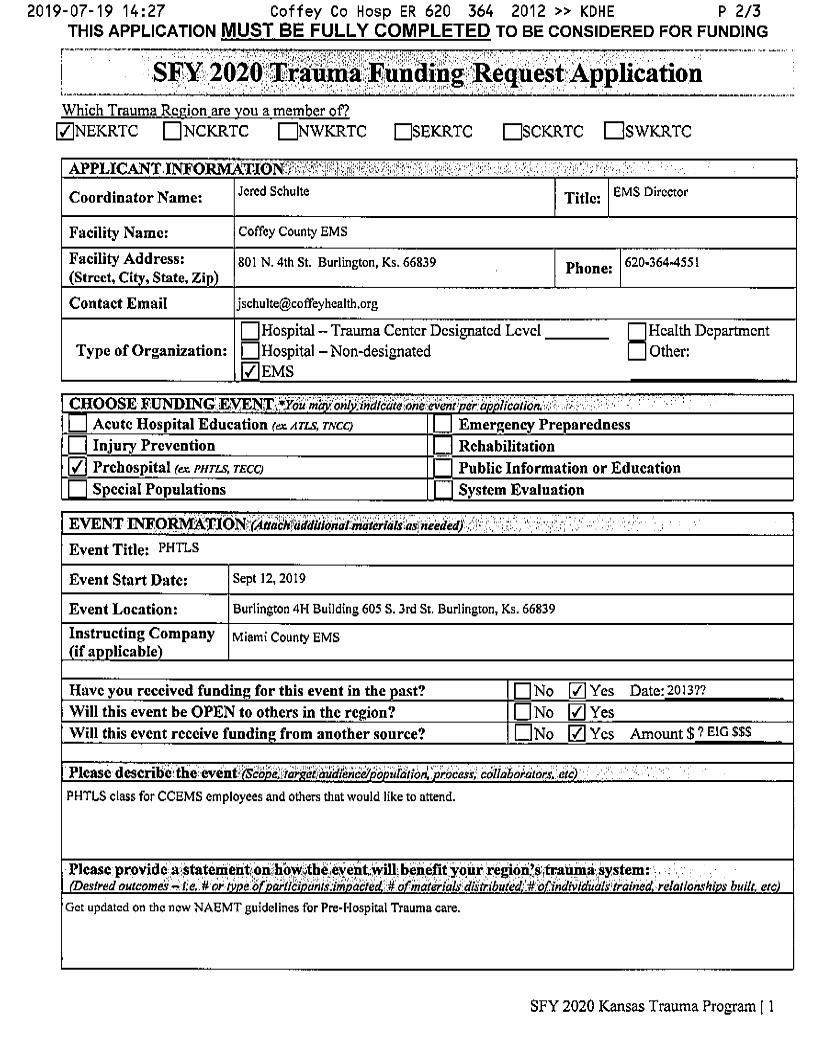
EVENT IN'FO , :T.1bNtLrà#JJbtàJJâ)ègJ?1JkJrkJatz''xë:redek)'', ''S'. ' '' ' 4 ' '' '' ' )I7 ', ' ' 'Event Title: PHTLS
Event Start Datc: Sept 12, 2019
Event Location: Burlingten 414 Bulldlng 605 S. 31 S1. Burllngton, Ks. 66839
Instructing Company uiami county EMsif a licable
Havc you reccived funding for this event in the ast? No U-1v/' Yes Date: 20137?Will this event be OPEN tfl othcrs in thc rtgion? N NO U-17 YesWill this evcnt rcctive fundin from another seurcv? Z NO 17.77 Yçs Amount $ 7 E!G $$$
Pltast describi'tie evenihi' dlg ''è' ïçjtè ' kçzrllàlâkW 'b xïistw' '' Vc:4,v,: bkllaboètitorn eft; ' .PHTLS class f0r CCEMS employees and others that would Iike to attend.
Pkas: provide atptateped,tlkonihbvilthiufeïex, twilltbeùifit yqur.ziegivpyit'ra. àmiiiystemr . , ;t'ed outcomé - te..# (V e b ' :-' iiti ' 'aitisàtià'' îk'/'iW' b o ./ncilr/ft Isbdâtributèt ...#* b .'ind '-IwJU' 'alsëtèainnd rte//oa-s'l?f s built etce.v
Get updated on the new NAEMT suldelines for Pre-hlospital Trauma care.
SFY 2020 Kansas Trauma Progrmn I 1

2019-07-19 14:29 Coffey Co Fosp ER 620 364 2012 >> KDFE P 3/3THIS APPLICATION MUST BE FULLY COMPLETED TO BE CONSIDERED FOR FUNDING
JM UM J>A4tW Dt)NfA! IW SPECJFICSLP ATM ; 7Ncc,''*NTJk5', ztz) 'n MD r.7DO CIAPRN CIPAPractitioner Name: Credentials; RN EMS/PM
*Re istration Cost: $Does ANY employer provide CME support? es N NO*lncludv J co p o coursc re istration indicatîn the rtlN?..vc cost wû/b a Ilcatlon*/I//Jc/7 a Iist ofpractitionersb f/lc/r credentials, and rega/zp//tw co,b'ts fapplyingfor /:////1)J/(f practitioaers.JNc/: as sendin 5 nurses to a TNCC cour,b'q t?/ a di erlla/ acili .
BUDGET N ORM ATION ', ' ' : 'ï '' ' 'Do you plml to charge a registration fee for this event? Z No V Yes, registration fee: $ 20.00EST/MATED EVENT EM ENDIKURES't l . a lfzzi '' abll' 'âvt/liwn tllkoknt ' , 'Lîne Item , ' '''i : ''. :Amèunt 'l; 7 , ''' ' ' '' '' $ .'? F..x lànatlon ? h ''' ' '' 'Administrativc Costs $ 100.00 setting up class, Prepadng classroomx etc.Faclllt Char es $Promotion & Publicit $Internal Instructor Fees $External S eaker/lnstnlctor Fees $ 250.00Travel/ Lod in $Books / Su lies $ 800.00 10 books6 ui ment $Other: $ 350.00 NAEMT Fee'sOther: $ 150,00 Lunch. Drinks & Snacks for 2 da s.
TOTAL $ 1650.90
FUNDING RE 'UEST .+ RE . D,ê: à ' Iieitiiid wrtkrxo:r bq' kaiifiqd wlthoùtthls kmount*Amount of Fundin Re uested: S 1200.00*Re#r lo your region 's trauma reimbursementpolicyfor maximum amount avaîlable.
Si atum ôf mkofjkiàl' ih riz' ' idlidkbii' d theâirtàn-lzatiop'andFkèrt'ify' ''' li: ' with all triteriaê,n . !:t!., ..Pt , ,1, v ,j,),, 0...4., . ,$....,. , . , 't . , . ., $,copp. 'c'' . 'a licable in ardaxtèwitihflkkflli it uiremenis is re uireè .. ' '''Signature:
Title: 3 z' ce/no/e- Datv: -- '-
Process: , ' $ . Trauma Funding ls a reimbursement svstem. Approved funding will be distributed after the eventhas occurred and the affidavil of expenditures submited.
.1 ', Rcîmburscmcnts wîll be made to the orgaalzation making the request.
tndividual providers will not receive reimbursement chccks.; . '
' .. h 1 $ . u, .( .' .. . . ' bfL ' A Iications and thcir cvcnts must occur within the same statc Gscal car JuI 1'l - June 30 ' .Submit Completed Appllcatllms Email tQ: Ren,mortonmfl kq. .stovand Documcntatioirtol.t.. . 7: 6, ' '.- FM t0: 785 559..4248
$ F ;ï '. ' ' , Requires notiscalion sent lo ken.mortona ks,krov within 30 days of original event dale to remainEvent Date Chaùgei ! , . y ' ', h.);$ k. jj jj):;. ' .' c' '
.i ' Email a copy of the practitioner's crcdentialing card within 30 days of course completion.Peaditipne/ Evekb ONL'Y: .'. .' ''. 'f'; .? 7 J. p' t
, . ' ' Submgt the followlng wlthin 30 days of Event:
All Other Events: . o Copy of rosters whlch include clty and zlp for each participant' o Flnal aftidavlt of cx cndiyurcs download tcm late from www.kstkmtlm.or
SIW 2020 Kansas Trauma Program I 2


Regional Health Report
Region: Northeast Date: October 7, 2019
Summary Funding Distribution 9 facilities out of 36 have received funding for RTTDC, TNCC or ATLS.
25% of the region’s facilities are benefitting from the regional trauma council’s funds.
0 facilities out of 13 hospitals, 12 Local Health Departments, and 12 prehospital services have applied for fall prevention funding in the last three years.
1 PHTLS/TECC course has been funded in the last three years.
2 RTTDC have been funded in the last three years.
1 prehospital service has applied for funding in the last three years, during last year’s mini-grant cycle
3 out of 27 Health Departments applied for funding during last year’s mini-grant cycle.
63% of the funding from 2017-2019 went to ATLS; 26% went to TNCC; 4% went to PHTLS; 7% went to RTTDC excluding mini-grant allocations.
Level IVs The Northeast Region has one Level-I facility, two Level-II facilities and 12
Level-IV facilities.
4 Level-IV facilities are undergoing the designation renewal process.
Attendance Attendance is on track for executive committee members.
Reminder that executive committee members may not miss more than two
consecutive meetings without justification.
The NE Region has 4 vacant council seats. (1 physician, 1 EMS, 2 LHD) Diversions This information will be forthcoming Data Submission This information will be forthcoming

FundingDistribution Friday, September 27, 2019
1:21:20 PM
Organization Course Awarded Amt Award Date
Anderson Co
ATLS $650.00 8/14/2017
$650.00Facility Total from 2017 - 2019
Children's Mercy South
MiniGrant $660.00 4/8/2019
$660.00Facility Total from 2017 - 2019
Coffey County Hospital
RTTDC $1,697.79 12/10/2018
$1,697.79Facility Total from 2017 - 2019
Community HealthCare System
ATLS $650.00 10/9/2017
ATLS $650.00 5/1/2018
$1,300.00Facility Total from 2017 - 2019
Community Memorial Healthcare
TNCC $1,500.00 5/1/2018
MiniGrant $520.00 4/8/2019
$2,020.00Facility Total from 2017 - 2019
Hiawatha Community Hospital
MiniGrant $1,991.21 3/22/2019
ATLS $695.00 4/8/2019
ATLS $695.00 4/8/2019
TNCC $1,500.00 4/8/2019
$4,881.21Facility Total from 2017 - 2019
Holton Community Hospital
ATLS $650.00 4/10/2017
ATLS $650.00 6/12/2017
ATLS $575.00 5/1/2018
RTTDC $773.50 10/8/2018
ATLS $575.00 12/10/2018
ATLS $850.00 12/10/2018
ATLS $850.00 2/11/2019
ATLS $575.00 2/11/2019
Page 1 of 3

Organization Course Awarded Amt Award Date
$5,498.50Facility Total from 2017 - 2019
Junction City Fire Department
PHTLS $640.00 4/8/2019
$640.00Facility Total from 2017 - 2019
Nemaha Valley Community Hospital
MiniGrant $2,000.00 3/22/2019
$2,000.00Facility Total from 2017 - 2019
Pottawatomi County
MiniGrant $848.00 4/8/2019
$848.00Facility Total from 2017 - 2019
Providence Medical Center
TNCC $260.00 6/12/2017
TNCC $1,500.00 4/8/2019
$1,760.00Facility Total from 2017 - 2019
Ransom Memorial Health
ATLS $650.00 12/11/2017
TNCC $735.00 5/1/2018
ATLS $850.00 6/11/2018
ATLS $575.00 10/8/2018
ATLS $575.00 10/8/2018
TNCC $1,155.00 2/11/2019
TNCC $450.00 4/8/2019
MiniGrant $1,600.00 4/8/2019
ATLS $850.00 4/8/2019
$7,440.00Facility Total from 2017 - 2019
Riley County Health Department
MiniGrant $960.00 4/8/2019
$960.00Facility Total from 2017 - 2019
Sabetha Community Hospital
MiniGrant $552.00 4/8/2019
$552.00Facility Total from 2017 - 2019
SafeKids Prairie Band Pottawatomi
MiniGrant $1,600.00 4/8/2019
Page 2 of 3
Organization Course Awarded Amt Award Date
$1,600.00Facility Total from 2017 - 2019
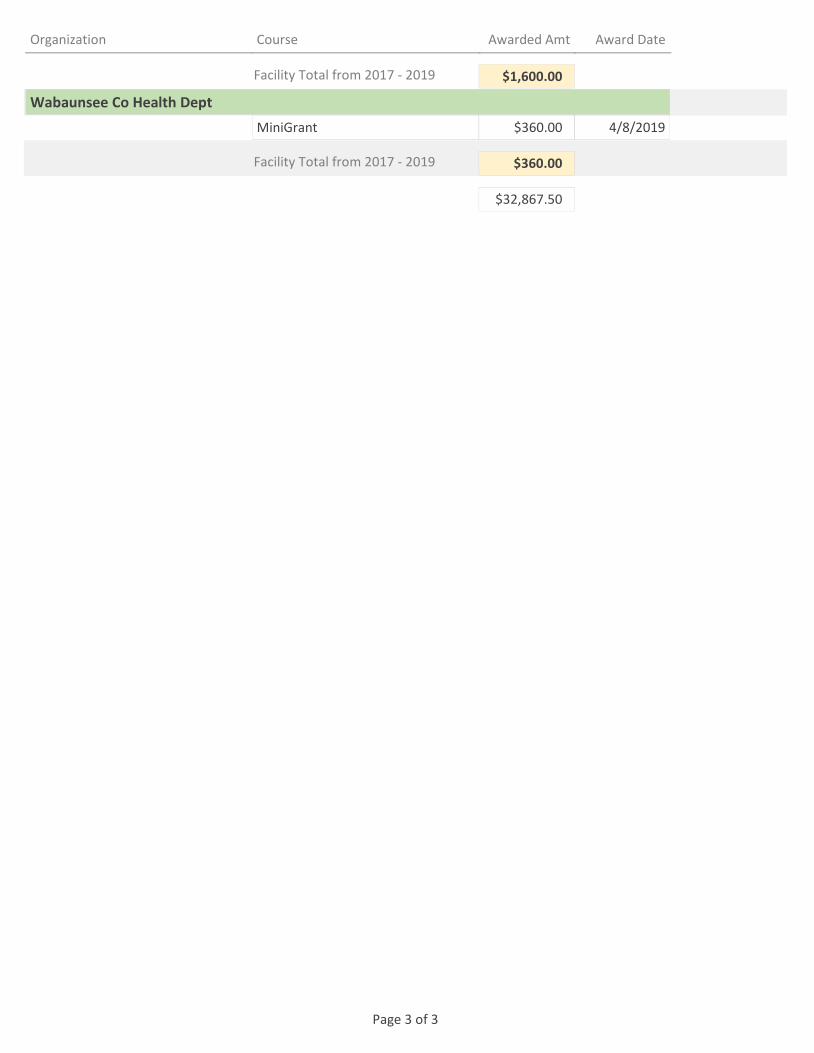
Wabaunsee Co Health Dept
MiniGrant $360.00 4/8/2019
$360.00Facility Total from 2017 - 2019
$32,867.50
Page 3 of 3

NC Level IV Report Friday, September 27, 2019
1:27:46 PM
OrganizationStatus Expiration Date Status Date
Cert. Pending
Providence Medical Center 04-Apr-19 12-Sep-19
Current
Anderson County Hospital 13-Apr-20
Holton Community Hospital 12-May-20
Community HealthCare System, Onaga
24-Aug-20
Newman Regional Health 07-Feb-21
Sabetha Community Hospital 06-Mar-21
Hiawatha Community Hospital 31-Dec-21
Lawrence Memorial Hospital 07-Jan-22
PRQ Review
Nemaha Valley Community Hospital 31-Jul-19 17-Jun-19
Community Memorial Healthcare - Marysville
31-Oct-19 21-Aug-19
Reminder Sent
Miami County Medical Center 30-Nov-19 16-Jul-19
Survey Scheduled
Ransom Memorial Hospital 05-Apr-19 18-Oct-19
12
Page 1 of 1

Attendance Friday, September 27, 2019
1:53:04 PM
OrganizationDateAttendedMeeting Attended
ACT
Q3 2019
Childrens Mercy8/7/2019
Kansas Emergency Nurses Association8/7/2019
Kansas Hospital Association8/7/2019
MARC8/7/2019
Overland Park Regional Medical Center8/7/2019
Stormont-Vail HealthCare Inc8/7/2019
Stormont-Vail HealthCare Inc8/7/2019
Stormont-Vail HealthCare Inc8/7/2019
Stormont-Vail HealthCare Inc8/7/2019
Stormont-Vail HealthCare Inc8/7/2019
University of Kansas Medical Center8/7/2019
University of Kansas Medical Center8/7/2019
Regional Symposium
Q2 2019
Childrens Mercy South4/8/2019
Franklin County EMS4/8/2019
Overland Park Regional Medical Center4/8/2019
Overland Park Regional Medical Center4/8/2019
Stormont-Vail HealthCare Inc4/8/2019
University of Kansas Medical Center4/8/2019
University of Kansas Medical Center4/8/2019
RTC Executive Mtg
Q1 2019
Anderson County EMS2/11/2019
Childrens Mercy South2/11/2019
Hiawatha Community Hospital2/11/2019
Holton Community Hospital2/11/2019
Page 1 of 2

OrganizationDateAttendedMeeting Attended
Kansas Emergency Nurses Association2/11/2019
MARC2/11/2019
NE HCC2/11/2019
Nemaha Valley Community Hospital2/11/2019
Overland Park Regional Medical Center2/11/2019
Ransom Memorial Hospital2/11/2019
Stormont-Vail HealthCare Inc2/11/2019
Stormont-Vail HealthCare Inc2/11/2019
Stormont-Vail HealthCare Inc2/11/2019
University of Kansas Medical Center2/11/2019
University of Kansas Medical Center2/11/2019
University of Kansas Medical Center2/11/2019
Q2 2019
Childrens Mercy South4/8/2019
Franklin County EMS4/8/2019
Overland Park Regional Medical Center4/8/2019
Overland Park Regional Medical Center4/8/2019
Stormont-Vail HealthCare Inc4/8/2019
University of Kansas Medical Center4/8/2019
Page 2 of 2