medication safety issues associated with currently used...
TRANSCRIPT

Medication safety issues associated with currently used first-line antiretroviral regimens in Uganda
Kay Seden1, Daniel Kiiza2, Eva Laker2, Joseph Walter Arinaitwe3, Catriona Waitt1, Mohammed Lamorde2, Saye Khoo1
1. University of Liverpool, UK; 2. Infectious Diseases Institute, Makerere University, Uganda; 3. AIDS Treatment Information Centre (ATIC), Infectious Diseases Institute, Makerere University, Uganda
19th International Workshop on Clinical Pharmacology of Antiviral Therapy 2018, 22 - 24 May 2018; Baltimore, Maryland, USA
Abstract: 09
Conflict of interest statement
• ML has received research grants from ViiV, Janssen pharmaceuticals NV
• SK has received support for the HIV Drug Interactions website (www.hiv-druginteractions.org) from ViiV
Healthcare, Gilead Sciences, Merck, and Janssen
• All other authors have none to declare
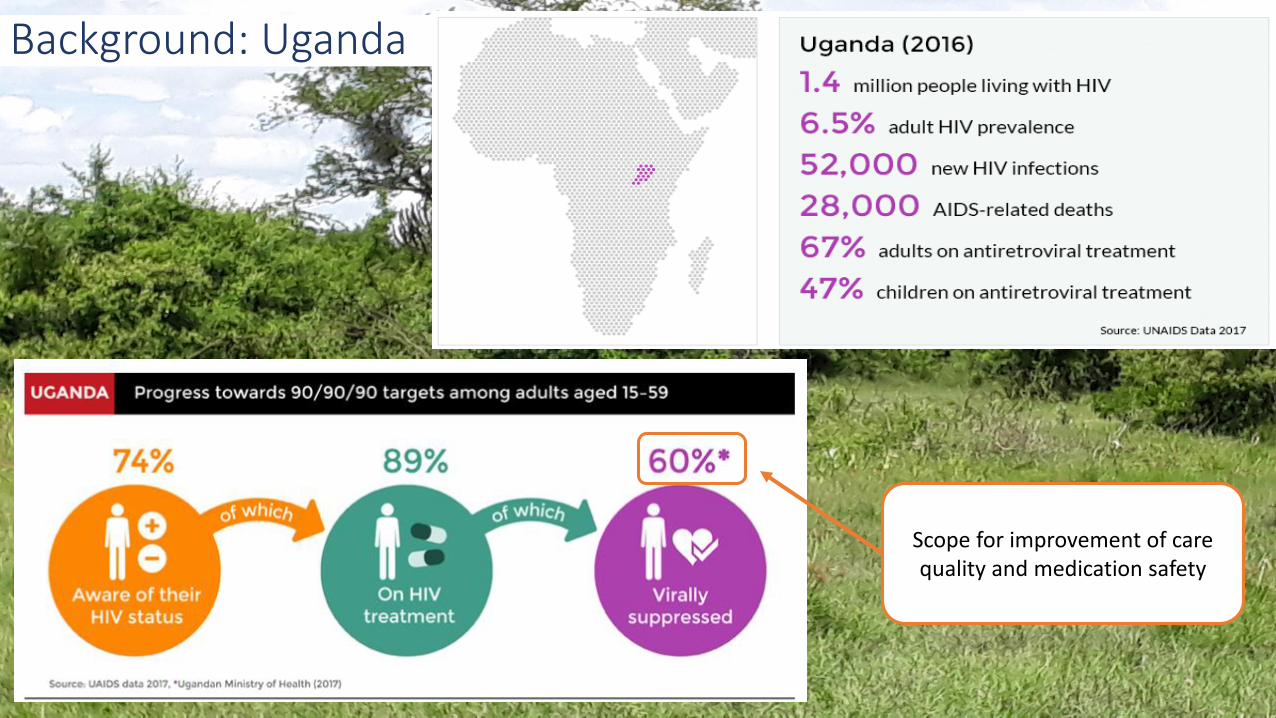
Background: Uganda
Scope for improvement of care quality and medication safety

Background: medication safety issues
• May increase the risk of drug toxicity, or reduce clinical effect of one or more drugs
• Clinically significant drug-drug interactions (CSDDIs) affect 26.7% of Ugandan outpatients taking antiretrovirals (ARVs)1
• In sub-Saharan Africa, recognition and management of DDIs is restricted by patients accessing medicines via separate silos of care, and un-regulated purchase of medicines
Drug-drug interactions
(DDIs)
• May affect quality of life, cause morbidity or mortality
• May affect adherence
• May be under-reported in this setting, or tolerated due to lack of alternative regimens
Adverse drug events
(ADEs)
Seden K, Kiiza D, Laker E, Arinaitwe JW, Waitt C, Lamorde M, Khoo S. Task shifting and mobile technology for HIV drug-drug interaction screening in Uganda. 22nd International AIDS Conference (AIDS 2018), 23-27 July, 2018 in Amsterdam, Netherlands. Abstract: Poster A-899-0383-05296

Technician interviews patient
and completes CRF
Pharmacist receives documents in
shared file for triage
PMSI screening and ADE causality
validation and review
Populate prescriber feedback form
Feedback form received in shared file
Feedback form placed in clinic
notes
Background: study design
Prescriber review/action
Central shared drive
Longitudinal observational study in adults taking antiretrovirals (SAPU)
• Prevalence of medication safety issues (prescribing error, drug interactions, adverse drug reactions)
• Prevalence and cause of medication-related hospital admissions
• Prescriber recognition of medication safety issues
• Feasibility, acceptability and utility of an intervention (via prescriber questionnaire)

Methods & population: early analysis
• Consecutive eligible patients from 3 diverse clinics
• Adult HIV-positive outpatients, taking current first-line ARVs
• DDI screening/severity assessment and assessment of ADE causality was undertaken by pharmacists and clinicians, using standardized tools1,2,3,4
1. University of Liverpool HIV Drug Interaction tool. www.hiv-druginteractions.org. 2. Gallagher RM, Kirkham JJ, Mason JR et al. Development and inter-rater reliability of the Liverpool adverse drug reaction causality assessment tool. PLoS One 2011; 6: e28096.3. U.S. Department of Health and Human Services, National Institutes of Health, Division of AIDS. Division of AIDS (DAIDS) Table for Grading the Severity of Adult and Pediatric Adverse Events, [July 2017]. https://rsc.tech-res.com/docs/default-source/safety/division-of-aids-(daids)-table-for-grading-the-severity-of-adult-and-pediatric-adverse-events-corrected-v-2-1.pdf.
4. Medical Dictionary for Regulatory Activities (MedDRA) version 19.0, www.meddra.org
• Early analysis undertaken to inform patient care locally and internationally
• Data have informed national plans to roll-out dolutegravir
• 469 consecutive patients (50% of total SAPU study recruitment)
• 416 patients taking first-line ARV regimens

Results: patient characteristics
1st line regimen 416 (88.7)TDF/3TC/EFV n(%) 262 (63)ZDV/3TC-EFV n(%) 37 (14.1)ZDV/3TC/NVP n(%) 95 (22.8)TDF/3TC-NVP n(%) 21 (5)ABC/3TC-EFV n(%) 1 (0.2)Female n(%)
Male
287 (69)
129 (31)Time on treatment (months)
median (IQR)
36 (19-57)
Age (years) median (IQR) 35 (28-44)Weight mean (Standard error)
Female
Male
60kg (0.53)
59.7kg (0.67)
60.5kg (0.85)Site CE n(%) 177 (42.5)UD n(%) 135 (32.5)RD n(%) 104 (25)
72% of first-line patients were taking EFV
Majority had been taking first line regimens long-term (75% took 1st line for ≥19 months)
Majority were female (comparable to clinic populations)

Results: summary
Serious
Moderate
Minor
No ADEs
Clinically significant drug interactions
180 (43.3%) of 416 patients on 1st line
regimens reported a current side effect at the
time of interview, which was considered to be
an adverse drug event. 252 ADEs were
reported in total (95%CI 38.5- 48.2%)
25,5%
74,5%
Adverse Drug Events
106 (25.5%) of 416 patients on
1st line regimens had ≥1 CSDDI
(95%CI 21.4- 30.0%)
Patients with CSDDIs more likely to report an ADE (OR 1.86, 95%CI 1.16 - 2.98, p=0.0059)
EFV-based regimen associated with reporting ADEs (OR 1.84, 95%CI 1.15 - 2.98, p=0.007)
but not presence of a CSDDI (OR 0.76, 95%CI 0.46 - 1.27, p=0.2650

Reported/detected ADEs (System Organ Class) Prevalence (%)
All 252
Nervous system/Psychiatric disorders 145 (57.5)
General disorders & administration site conditions 33 (13.1)
Gastrointestinal disorders 31 (12.3)
Skin & subcutaneous tissue disorders 12 (4.8)
Eye disorders 9 (3.6)
Reproductive system & breast disorders 5 (2.0)
Musculoskeletal & connective tissue disorders 4 (1.6)
Investigations 4 (1.6)
Cardiac disorders 3 (1.2)
Blood & Lymphatic system disorder 3 (1.2)
Renal & urinary disorders 2 (0.8)
Ear & labyrinth disorders 1 (0.4)
Results: adverse drug events
Dizziness 83
Headache 18
Neuropathies 17
Somnolence 14
Nightmares 6
Memory impairment 2
Dysgeusia 1
Anxiety 1
Psychosis 1
Insomnia 1
Hallucinations 1
Some ADEs not evaluable due to lack of laboratory
monitoring (renal function, haemoglobin)
72.6% of 252 total ADEs were possibly
or probably related to EFV
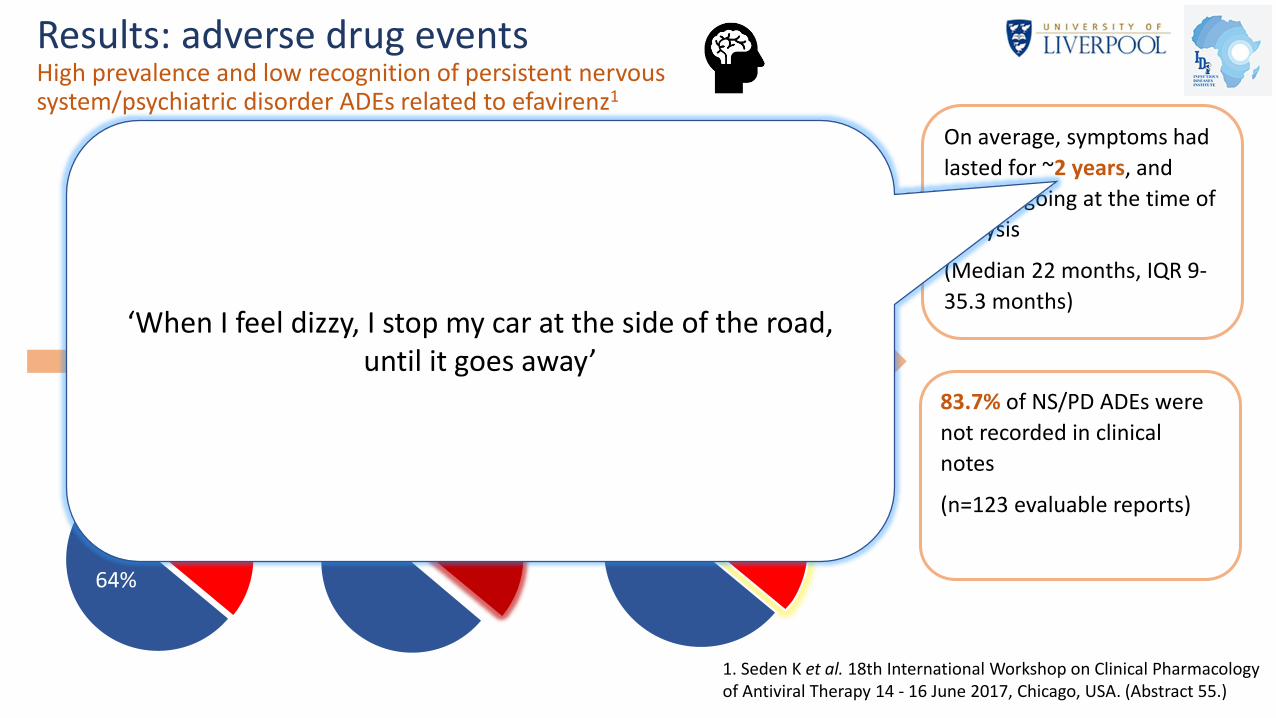
Results: adverse drug eventsHigh prevalence and low recognition of persistent nervous system/psychiatric disorder ADEs related to efavirenz1
36% of 300
patients taking
EFV reported
NS/PD ADEs
On average, symptoms had
lasted for ~2 years, and
were ongoing at the time of
analysis
(Median 22 months, IQR 9-
35.3 months)
83.7% of NS/PD ADEs were
not recorded in clinical
notes
(n=123 evaluable reports)
36%
64%
Dizziness accounted
for 64% of symptoms,
affecting 27% of 300
patients on EFV
58% of symptoms
rated by patients at
≥5/10 severity
1. Seden K et al. 18th International Workshop on Clinical Pharmacology of Antiviral Therapy 14 - 16 June 2017, Chicago, USA. (Abstract 55.)
‘When I feel dizzy, I stop my car at the side of the road, until it goes away’

Results: clinically significant drug interactionsAntimicrobials
14,4
21,4
64,2
35.8% of 416 patients on 1st line regimens took
antimicrobials in the previous month
14.4% of 416 patients had a CSDDI between 1st
line ARVs and antimicrobials (accounting for ~40%
of all CSDDIs)
40.3% of 149 patients taking
antimicrobials had a CSDDI
Antimicrobials included: antibiotics, antimalarials, anthelmintics, antivirals
CSDDIs between ARVs and antimicrobials may reduce antimicrobial efficacy, leading to: 1. Inadequate treatment of infection2. risk of resistance
46%
9%
25%
15%
5%
InappropriateindicationInappropriatechoiceInadequateduration
Seden K et al. 19th International Conference on AIDs and STIs in Africa, 4 - 9 Dec 2017, Abidjan, Côte d'Ivoire

Results: clinically significant drug interactionsChronic conditions
Potential for EFV and NVP to decrease exposure to available antihypertensivessuch as amlodipine and nifedipine.
Of 10 patients taking antihypertensives, all
10 had a potential CSDDI. Of these patients,
9/10 had uncontrolled hypertension
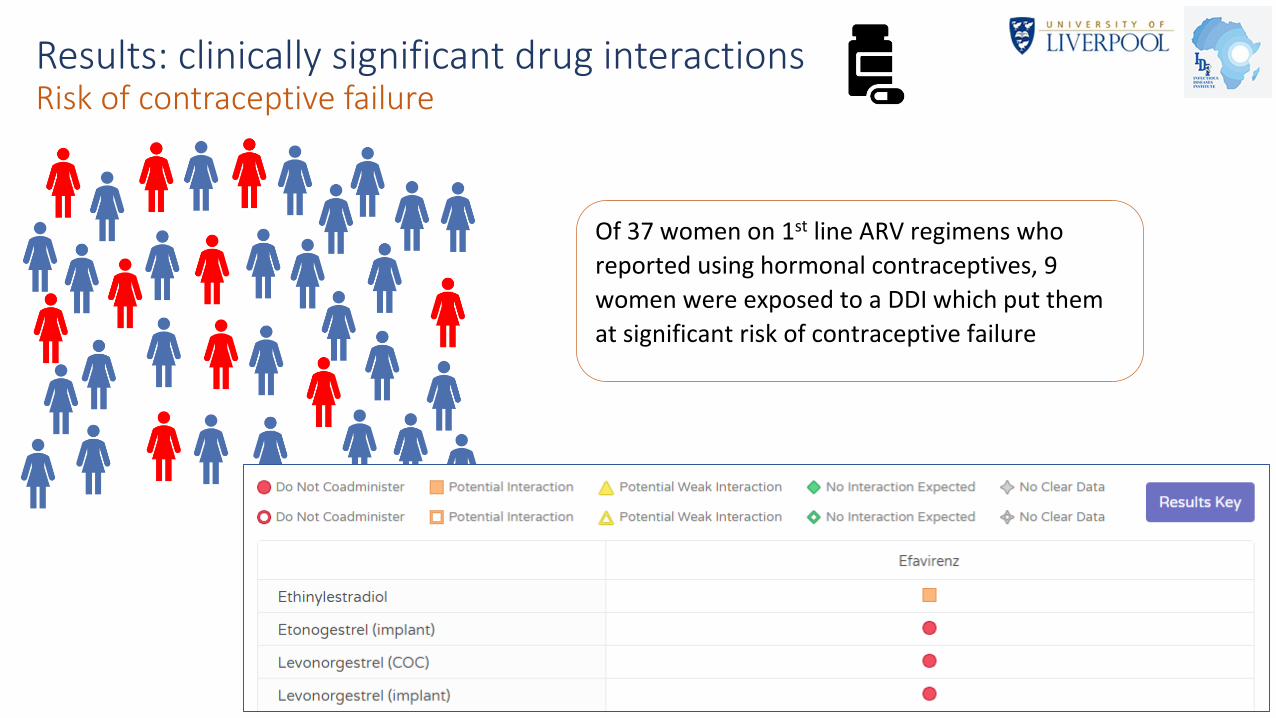
Results: clinically significant drug interactionsRisk of contraceptive failure
Of 37 women on 1st line ARV regimens who
reported using hormonal contraceptives, 9
women were exposed to a DDI which put them
at significant risk of contraceptive failure
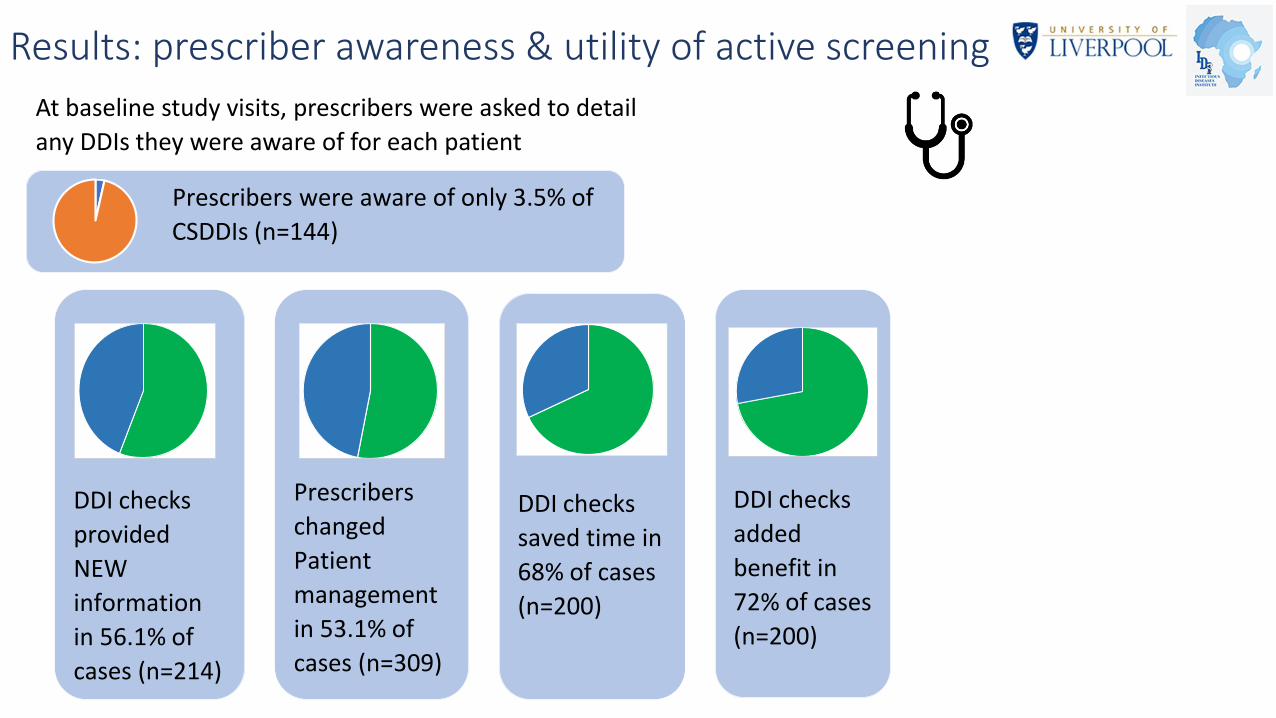
Results: prescriber awareness & utility of active screening
At baseline study visits, prescribers were asked to detail
any DDIs they were aware of for each patient
Prescribers were aware of only 3.5% of
CSDDIs (n=144)
DDI checks
provided
NEW
information
in 56.1% of
cases (n=214)
Prescribers
changed
Patient
management
in 53.1% of
cases (n=309)
DDI checks
saved time in
68% of cases
(n=200)
DDI checks
added
benefit in
72% of cases
(n=200)

Conclusions & recommendations
• Currently available ARVs for 1st-line regimens in sub-Saharan Africa comprise drugs which are the most
susceptible to CSDDIs, and with the highest propensity to cause ADEs, of all the globally available ARVs.
• Low resource settings are the least able to consistently monitor patients, switch regimens due to toxicity,
or tailor treatment to individuals
1. Compared to currently used 1st-line ARV regimens, roll-out of newer ARVs with lower potential for DDIs and
debilitating ADEs (such as dolutegravir) may:
▪ Reduce the risk of contraceptive failure
▪ Reduce risk of antimicrobial treatment failure and microbial resistance
▪ Reduce significant morbidity due to adverse drug reactions
2. Patients experiencing, or at high risk of debilitating ADEs or CSDDIs related to current first-line ARV regimens
should be prioritised for switching to dolutegravir.
3. Active screening for medication safety issues using task shifting and mobile technology is feasible, acceptable
to prescribers and led to a change in clinical management in more than half of patients screened
Acknowledgements
We would like to thank the staff and patients of all health centres and hospitals involved in the study, for their ongoing commitment to patient safety
Saye Khoo
Catriona Waitt
Mohammed Lamorde
Joseph Walter Arinaitwe
Eva Laker
Daniel Kiiza
Oliver Sapiri
Andrew Luswata
Byron Kawooya
Daniel Oula
This work was jointly supported by the UK Medical Research Council (MRC) and the UK Department for International Development (DFID) under
the MRC/DFID Concordat agreement and is also part of the EDCTP2 programme supported by the European Union.