medication safety
DESCRIPTION
ATRANSCRIPT

Medication Safety

DEFINITIONS:
Drug-related problems (DRPs) – events associated with
drug therapies that can hamper optimal patient health
outcome.
Medication misadventures – incidents associated with
indicated drug therapy resulting in patient harm.
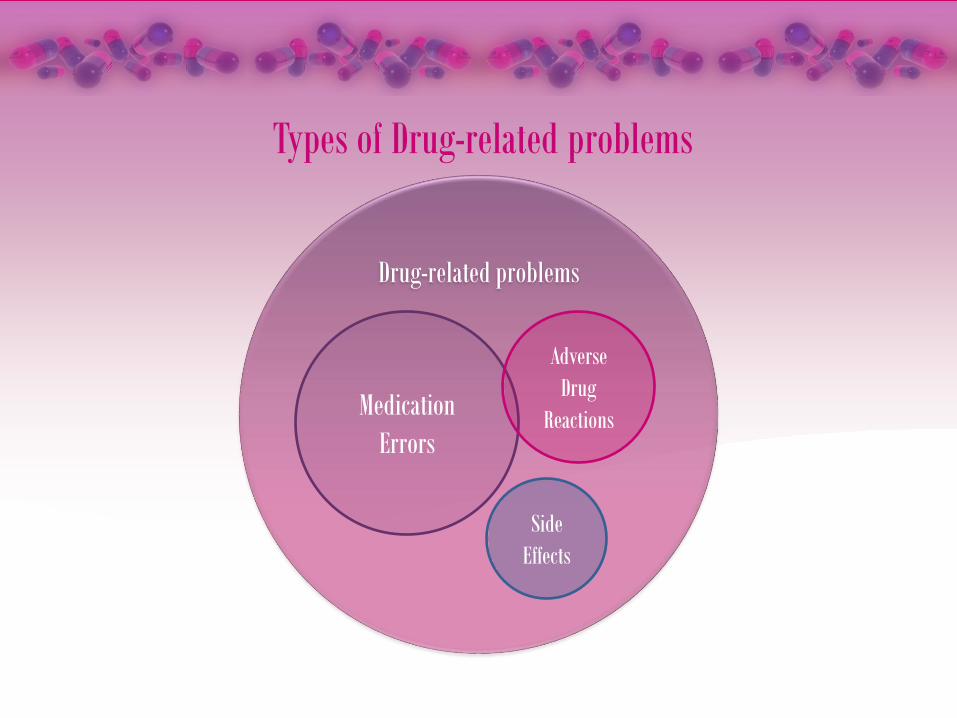
Types of Drug-related problems
Drug-related problems
Medication
Errors
Adverse
Drug
Reactions
Side
Effects

MEDICATION ERRORS - mistakes in the medication use process that may result in
negative outcomes.
Categories:
A. According to their impact on patients
NO ERROR ERROR, NO HARM ERROR, HARM ERROR, DEATH
CATEGORY A:
Capacity to cause error
CATEGORY B:
Error occur, Didn’t reach the
patient
CATEGORY C:
Error occur, Reached the patient
but didn’t cause harm to patient
CATEGORY D:
Error occur, Reached the patient
but cause harm to patient
CATEGORY E:
Error occur, temporary harm to
patient & require intervention
CATEGORY F:
Error occur, temporary harm to
patient & require hospitalization
CATEGORY G:
Error occur, permanent harm
CATEGORY H:
Error occur, Require intervention
necessary to sustain life
CATEGORY I:
Error occur, result to patient’s
death

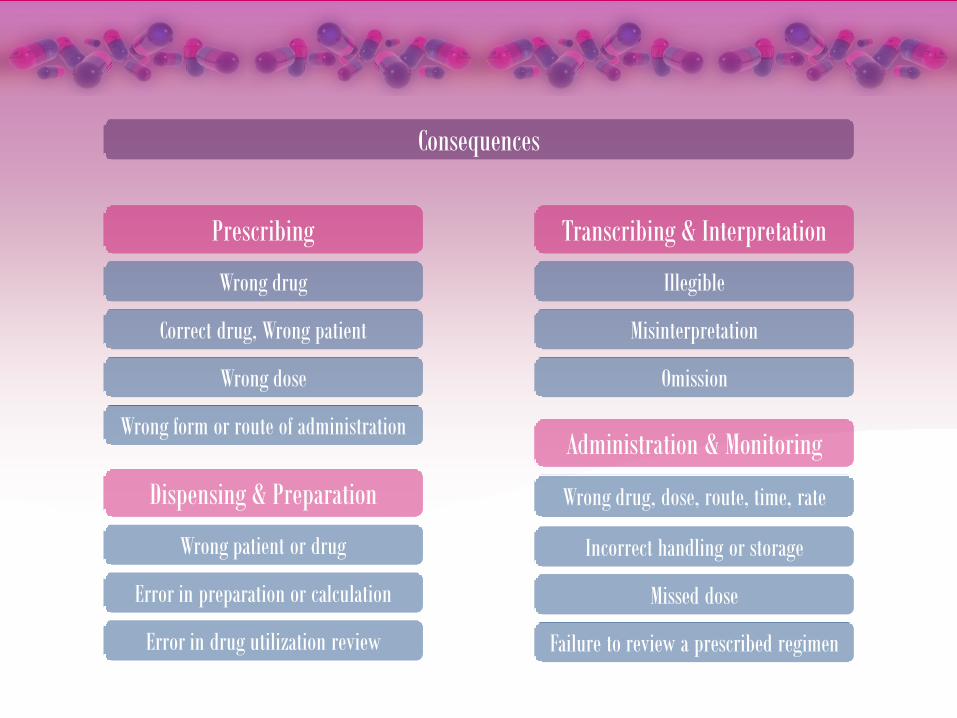
B. According to where they exist in the medication use system
Administration errors – patients are administered something other
than that prescribe for the patient.
Dispensing errors – mistakes made during the dispensing process.
Prescribing errors – prescriptions have an incorrect drug selection,
dosage form, quantity, route, concentration, rate and instruction for
use of a drug product.
Monitoring errors – failure to review a prescribed regimen for
appropriateness or the failure to use appropriate clinical or
laboratory data for adequate assessment of patient response to
prescribed therapy.
Transcription errors – misinterpretation of prescriptions
Prescribing
Wrong drug
Correct drug, Wrong patient
Wrong dose
Wrong form or route of administration
Error in preparation or calculation
Dispensing & Preparation
Transcribing & Interpretation
Misinterpretation
Omission
Wrong drug, dose, route, time, rate
Administration & Monitoring
Illegible
Wrong patient or drug
Error in drug utilization review
Incorrect handling or storage
Missed dose
Failure to review a prescribed regimen
Consequences
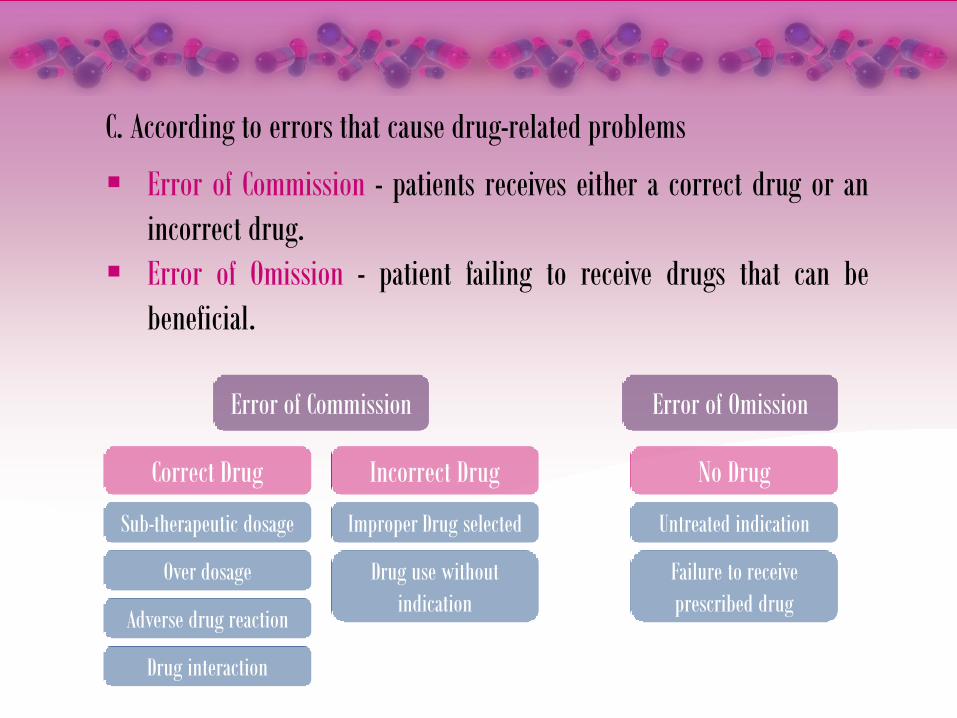
C. According to errors that cause drug-related problems
Error of Commission - patients receives either a correct drug or an
incorrect drug.
Error of Omission - patient failing to receive drugs that can be
beneficial.
Error of Commission
Correct Drug
Sub-therapeutic dosage
Over dosage
Adverse drug reaction
Drug interaction
Improper Drug selected
Drug use without
indication
Untreated indication
Failure to receive
prescribed drug
Incorrect Drug No Drug
Error of Omission
D. According to errors associated with outcome
Negative Outcome
Drug-related morbidity - failure of a drug to achieve its intended health
outcome due to unresolved DRPS.
Sentinel Events – unexpected incidents resulting in death or the
potential for serious physical or psychological injury.
No Negative Outcome
Latent Injury - propensity or predisposition for harm during the process
of care that actually does not result in patient injury.
Potential Injury – mistakes in prescribing, dispensing, or medication
administration that have the potential to cause injury but did
not.
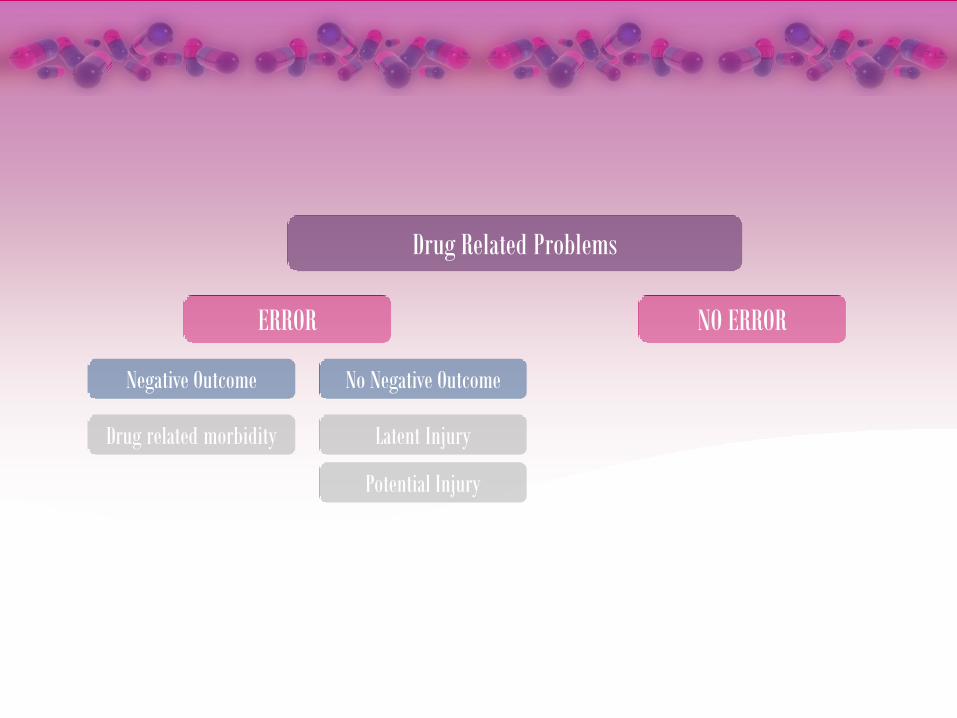
Drug Related Problems
ERROR
Negative Outcome
NO ERROR
No Negative Outcome
Latent Injury
Potential Injury
Drug related morbidity
ADVERSE DRUG REACTIONS (ADRs) – DRPs that are unexpected, unintended,
undesired, or excessive responses to a drug that require some type of
medical response or resulting in a negative outcome.
Allergic reactions – immunologic hypersensitivity to drugs
Idiosyncratic reactions – abnormal responses drugs that are
peculiar to individual.
Adverse drug events (ADEs) – ADRs that result in an injury due to the
use or lack of intended use of a drug.
SIDE EFFECTS – well-known reactions that require little or no change in
patient management. They are no ADRs
PREVENTING MEDICATION ERRORS
INSTITUTE OF MEDICINE
Involve patient in medication use process
Consumer-oriented medication
Access to patient information
Improved medication labeling
Improved Health information technology
Increased congressional funding
Active health care payers

PREVENTING MEDICATION ERRORS
RECOMMENDATION TO PHARMACIST
Keep up with medication literature
Verify accuracy of prescription
Verify patient’s identity
Engage patient in managing their own medication
Educate patient in preventing medication errors
Electronic prescribing should be used.
Trivial warnings should be avoided
Improved prescription filling technology
Monitor patients for high risk of side effects
Review patient medication
CULTURE OF SAFETY
Culture of Safety - exist where safety is the key element of everyone’s job.
MODELS OF QUALITY IMPROVEMENT
Status quo is unacceptable
Safety can be enhanced by improving the core process of medication use
process.
Safety efforts must be patient centered
Quality must be measured
Solutions to safety problems should address the system, not individuals

MODELS OF QUALITY IMPROVEMENT
PDSA Cycle of Safety Improvement
PLAN – Clarify the purpose of the quality improvement effort.
DO – Implementation is done in a small scale to allow adjustment to the plan as
experienced with the problem gained .
STUDY – “check”; studies the effect of the change on safety measure.
ACT – a new goal is established that further improves the safety of patient within
the medication use process.

MODELS OF QUALITY IMPROVEMENT
Measures of Health Care Quality - Donabedian sated that quality measures can
be divided into the following categories:
STURCTURES – These are measures of the presence of something that is
reasonably associated with quality.
PROCESSES – These are actions reasonably associated with quality such
as the checking of patient medication profiles prior to dispensing, double
checking technician work and electronic prescribing.
OUTCOME – the quality of safety systems needs to be assessed by their
impact on patient health outcomes.
MONITORING, REPORTING & COMMUNICATING
ADR- Monitoring and Reporting Programs
Based on reports of suspected ADRs by health professionals.
Monitor for alerting orders (prescription which alert pharmacists that an
ADR may have occurs and that an investigation needs to be
conducted)
a. Traces drugs use to treat ADRs
b. Discontinuation or decrease in dosage of drug
c. Stat orders for laboratory assessment of therapeutic drug levels
MONITORING, REPORTING & COMMUNICATING
Medication Reconcillation – is a process of resolving discrepancies with what a
patient has been taking in the past with what the patient should be taking at
the moment.
STEPS:
1. Verification – most up-to-date medication
2. Clarification – medication and dosage are checked for
appropriateness.
3. Reconciliation – Clinical decisions are then made based upon a
comparison of newly prescribed medication.
4. Transmission – Therapy changes are communicated to those
people who need to know about the changes.

NATIONAL QUALITY ORGANIZATION
The Institute of Medicine (IOM)
Institute for healthcare Improvement (IHI)
National Quality Forum (NQF)
The Leapfrog Group
The Joint Commission
Centers for Medicare and Medicaid Services (CMS)
Agency for Healthcare Research and Quality (AHRQ)
National Committee for Quality Assurance (NCQA)
American Society of Health-System Pharmacy (ASHP)
Pharmacy Quality Alliance (PQA)

