medication influence on cardiovascular outcomes jamie mccarrell, pharm.d., bcps, cgp assistant...
TRANSCRIPT
Medication Influence on Cardiovascular Outcomes
Jamie McCarrell, Pharm.D., BCPS, CGPAssistant Professor, TTUHSC SOP/SOM
Objectives
• Identify high-risk medications known to influence cardiac electrical activity.
• Describe recent literature regarding potential drug interactions that lead to adverse cardiac outcomes.
• Review new oral anticoagulant medications regarding efficacy, safety, and place in therapy.
• Given a patient case, optimize pharmacotherapy to improve patient outcomes and minimize adverse effects.
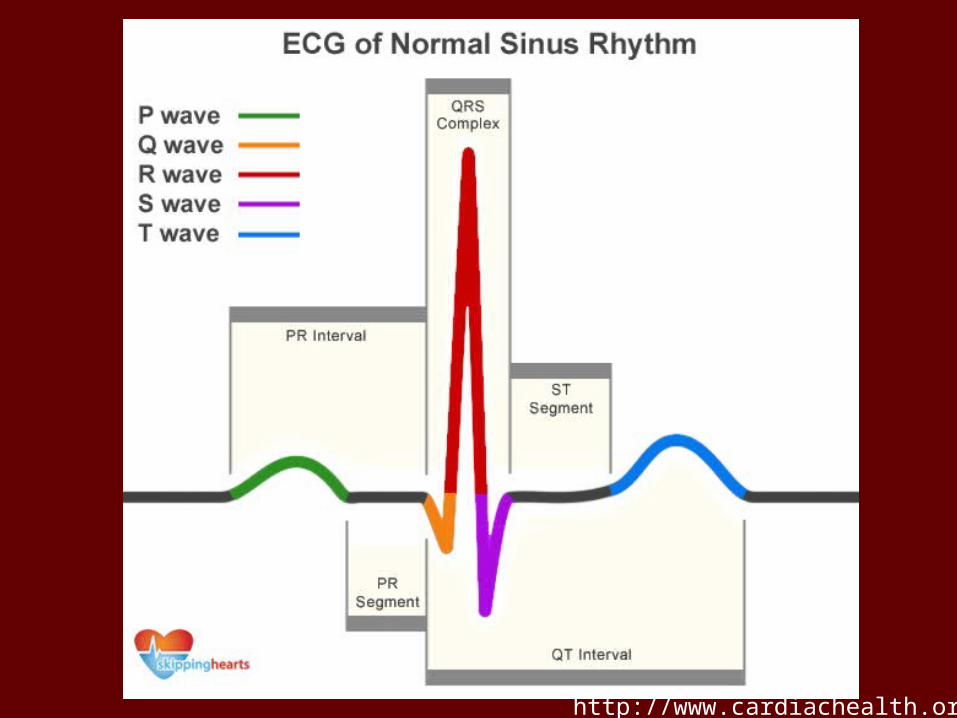
http://www.cardiachealth.org/
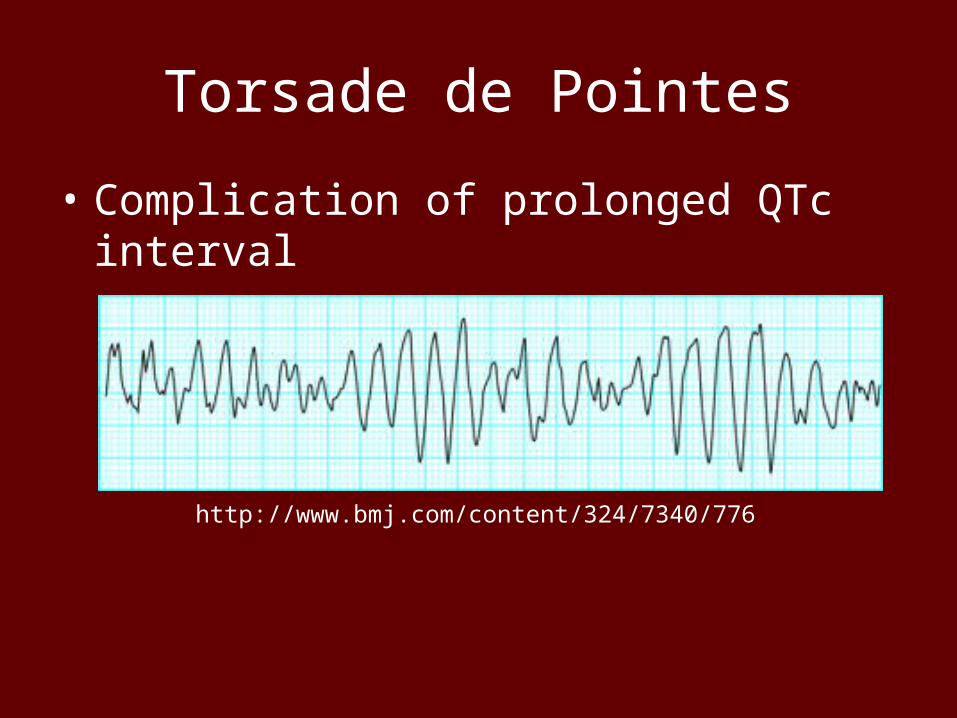
Torsade de Pointes
• Complication of prolonged QTc interval
http://www.bmj.com/content/324/7340/776
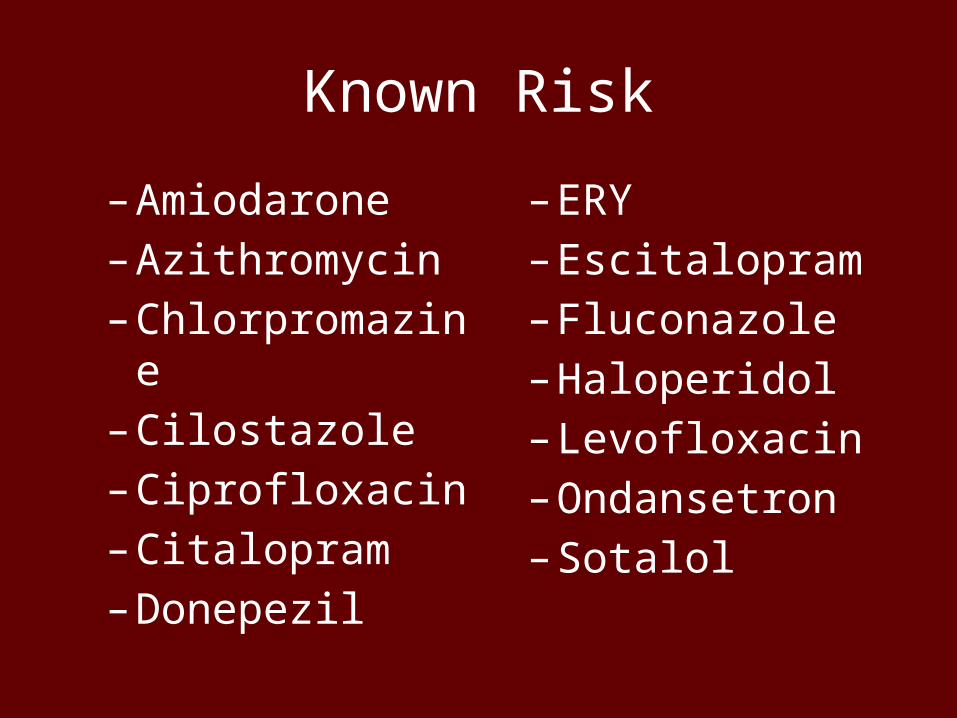
Known Risk
–Amiodarone–Azithromycin–Chlorpromazine–Cilostazole–Ciprofloxacin–Citalopram–Donepezil
– ERY– Escitalopram– Fluconazole–Haloperidol– Levofloxacin–Ondansetron– Sotalol
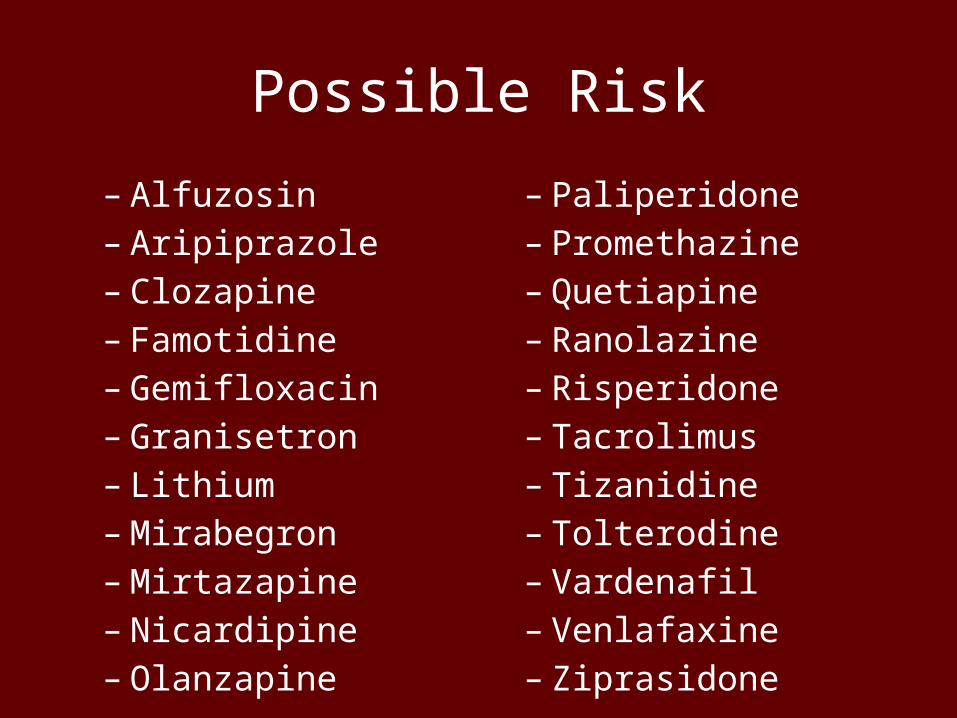
Possible Risk
– Alfuzosin– Aripiprazole– Clozapine– Famotidine– Gemifloxacin– Granisetron– Lithium– Mirabegron– Mirtazapine– Nicardipine– Olanzapine
– Paliperidone– Promethazine– Quetiapine– Ranolazine– Risperidone– Tacrolimus– Tizanidine– Tolterodine– Vardenafil– Venlafaxine– Ziprasidone
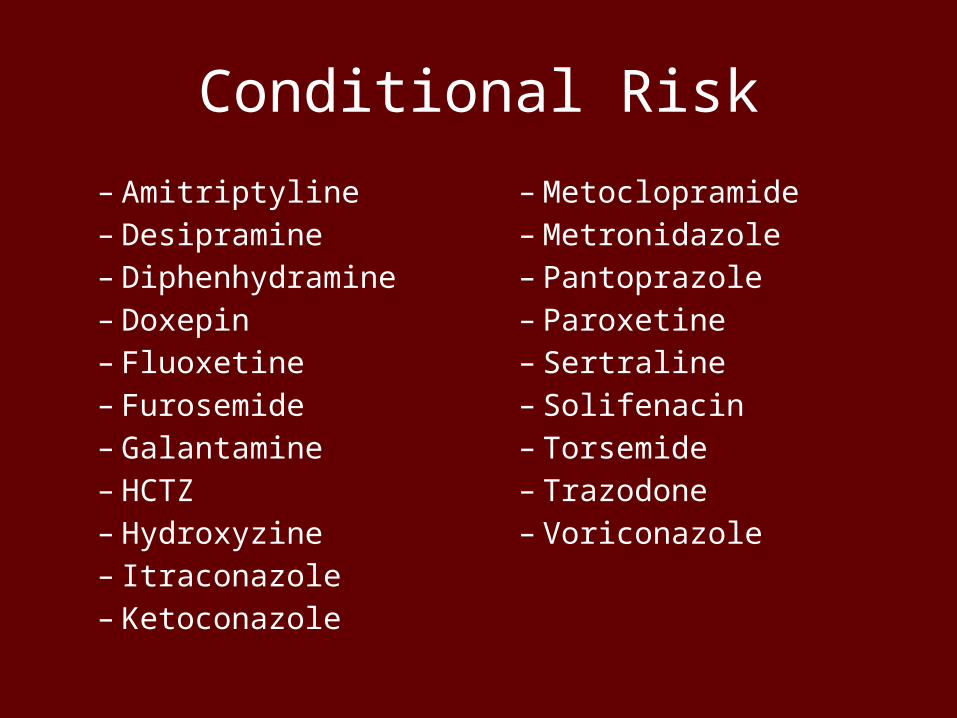
Conditional Risk
– Amitriptyline– Desipramine– Diphenhydramine– Doxepin– Fluoxetine– Furosemide– Galantamine– HCTZ– Hydroxyzine– Itraconazole– Ketoconazole
– Metoclopramide– Metronidazole– Pantoprazole– Paroxetine– Sertraline– Solifenacin– Torsemide– Trazodone– Voriconazole
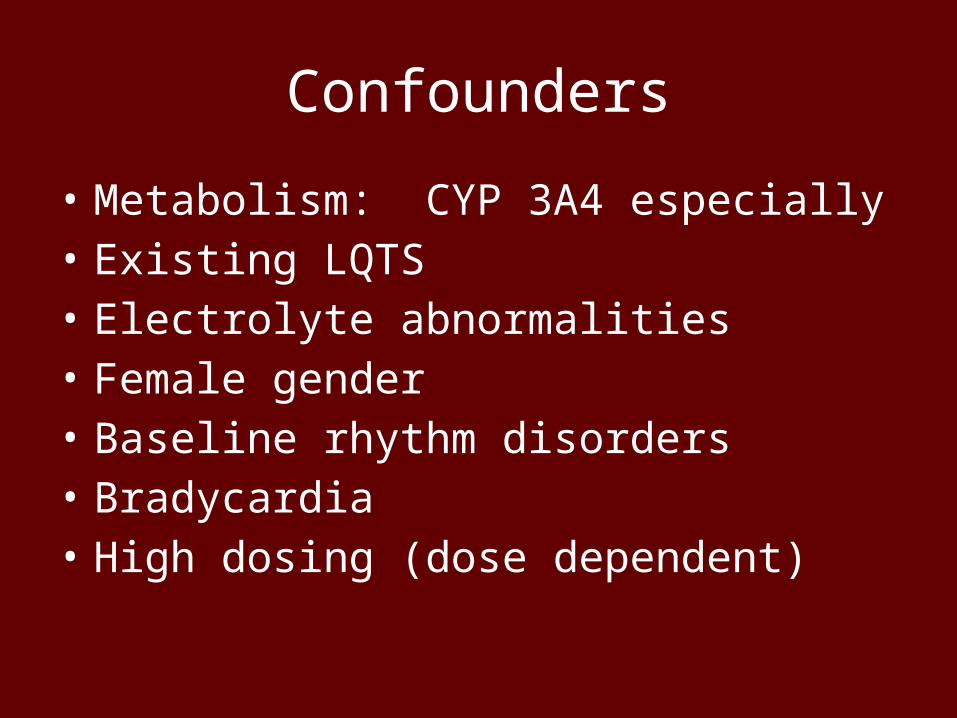
Confounders
• Metabolism: CYP 3A4 especially• Existing LQTS• Electrolyte abnormalities• Female gender• Baseline rhythm disorders• Bradycardia• High dosing (dose dependent)
Safety in Numbers
• Know the numbers!– EKG at baseline if possible for high-risk or multiple
medications– If available, know the potential increase in QTc for
the medication you are using– Flag these patients somehow…all PRN
medications, new starts, etc should be considered in light of prolonged QTc potential
NEW CONCERNS – SUDDEN CARDIAC DEATH
Journal Club
Bactrim® + ACE/ARBs
Fralick M, Macdonald EM, Gomes T, et al. Co-trimoxazole and sudden death in patients receiving ingibitors of
renen-angiotensin system: population based study. BMJ. 2014;349:g6196. doi:10.1136/bmj.g6196.
Bactrim® + ACE/ARBs
• Evaluated over 39,000 sudden deaths– Exposure to outpatient Abx = 1,027– Matched with 3733 controls
• Compared to amoxicillin + ACE/ARB…– Bactrim + ACE/ARB had OR = 1.54 (1.29 – 1.84) at
14 days.– 3 sudden deaths per 1,000 Bactrim Rxs– Cipro also has risk with OR 1.29 (1.03 – 1.62)
• Thought to be due to acute hyperkalemia
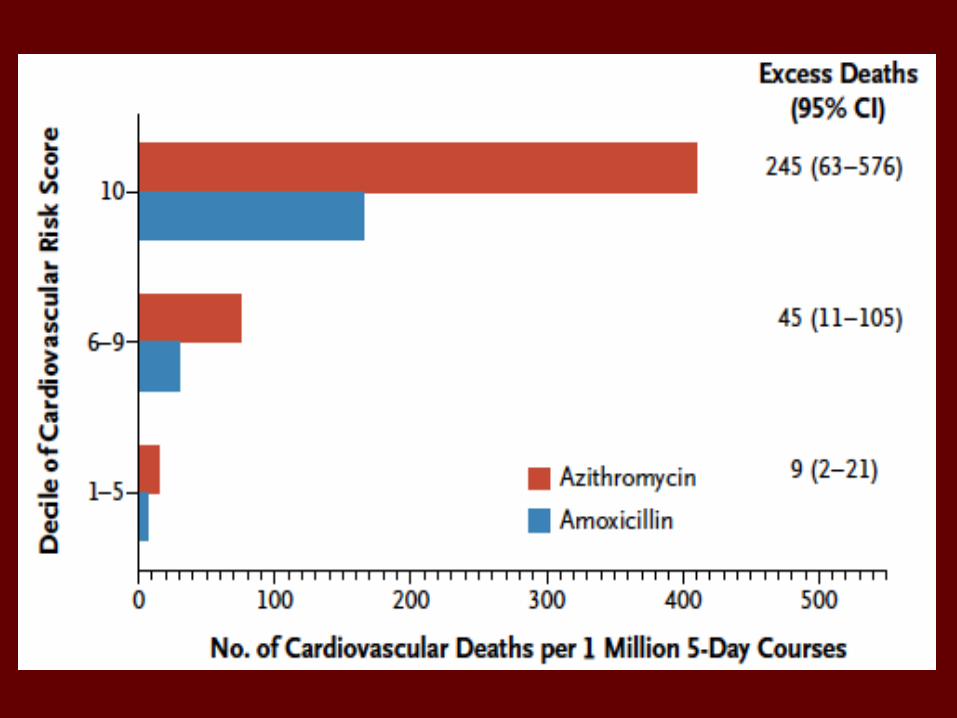
Azithromycin
NEJM, 2012
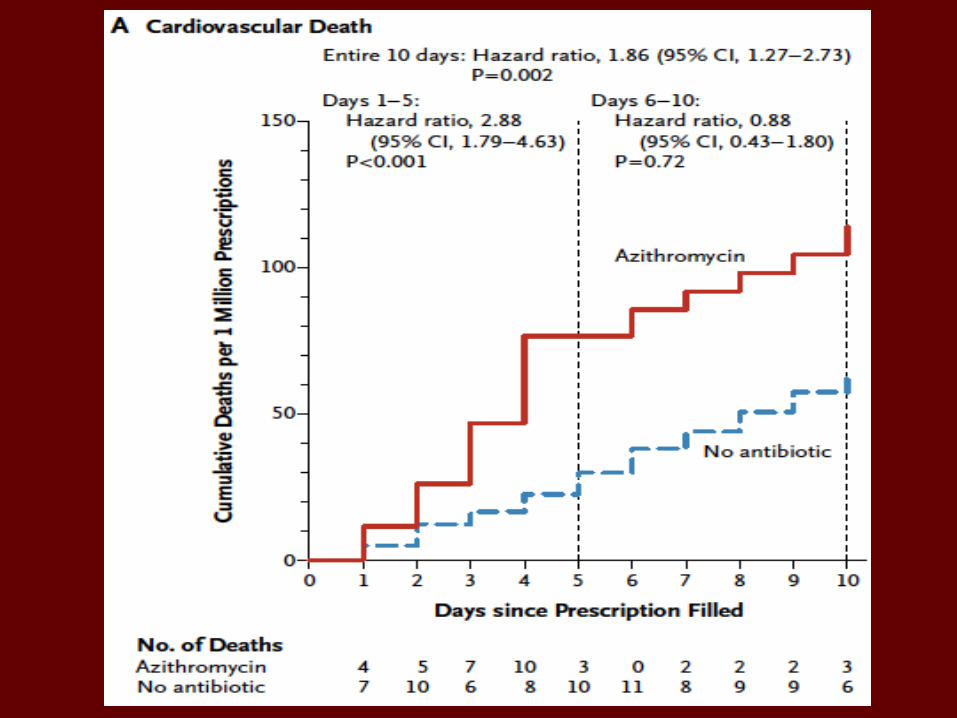
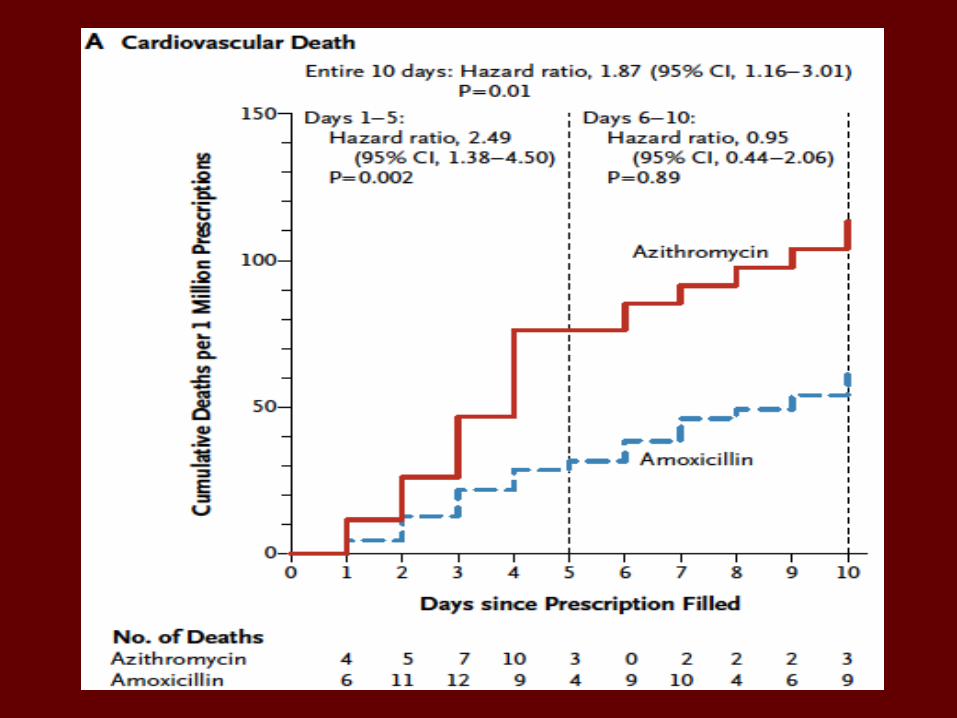
Azithromycin
• Nearly 350,000 azithromycin Rxs– Compared CV death outcomes to:• No antibiotic use• Amoxicillin• Ciprofloxacin• Levofloxacin
ORAL ANTICOAGULANTSStroke Prevention
Dabigatran (Pradaxa®)
• Direct thrombin inhibitor• RE-LY trial– 150 mg PO BID– CrCl < 30 was excluded from trial
– Canadian labeling: CrCl < 30 is contraindicated
• Major bleed = warfarin for >75 y.o. cohort – No antidote– Intracranial bleed better for dabigatran
• Australia/New Zealand audit (postmarket 2012)– 2 months, 78 cases of bleeding with dabigatran
• FDA Review – rates similar to RE-LY trial (11/2012)
Rivaroxaban (Xarelto®)
• Oral factor Xa inhibitor• ROCKET-AF trial– Non-inferiority study– Mean age 73, 14000 pts, 45 countries– More GI bleeds, less brain bleeds (vs warfarin)– Moderate renal insuff = higher rates of strokes and
bleeding• 20 mg PO once daily if normal renal fxn• No antidote
Apixaban (Eliquis®)
• Oral factor Xa inhibitor• ARISTOTLE trial– 5 mg PO BID– 1.6% vs 1.27% (p=0.01 for superiority) for stroke
or systemic embolism– 3.09% vs 2.13% (p<0.001) for major bleeding– Cohort evaluation determined that these hold
true for all age groups• No antidote
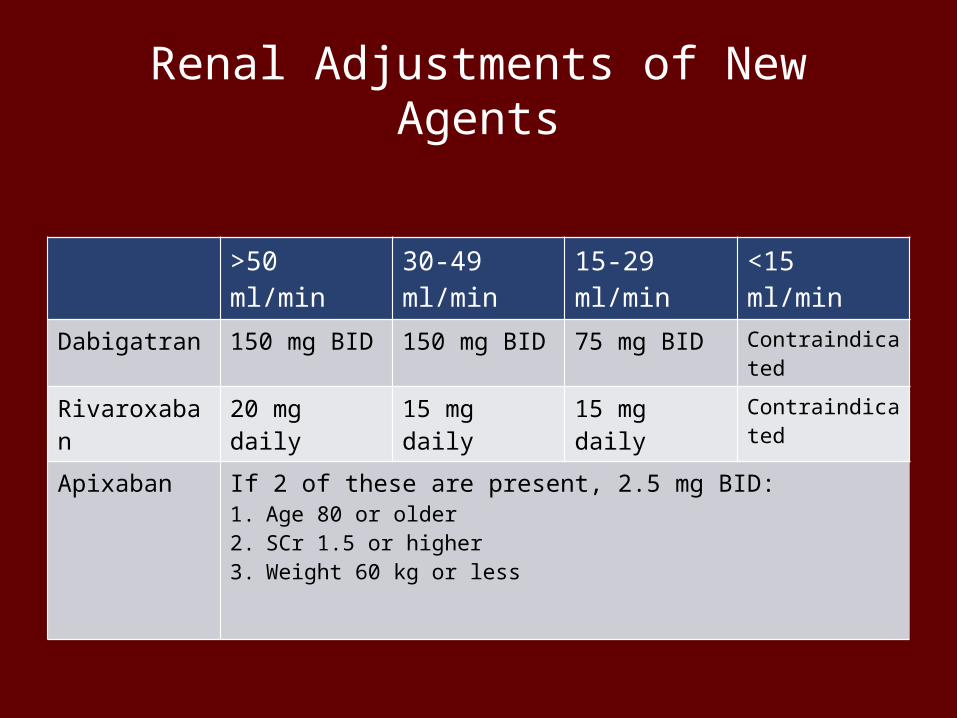
Renal Adjustments of New Agents
>50 ml/min 30-49 ml/min 15-29 ml/min <15 ml/min
Dabigatran 150 mg BID 150 mg BID 75 mg BID Contraindicated
Rivaroxaban 20 mg daily 15 mg daily 15 mg daily Contraindicated
Apixaban If 2 of these are present, 2.5 mg BID:1. Age 80 or older2. SCr 1.5 or higher3. Weight 60 kg or less
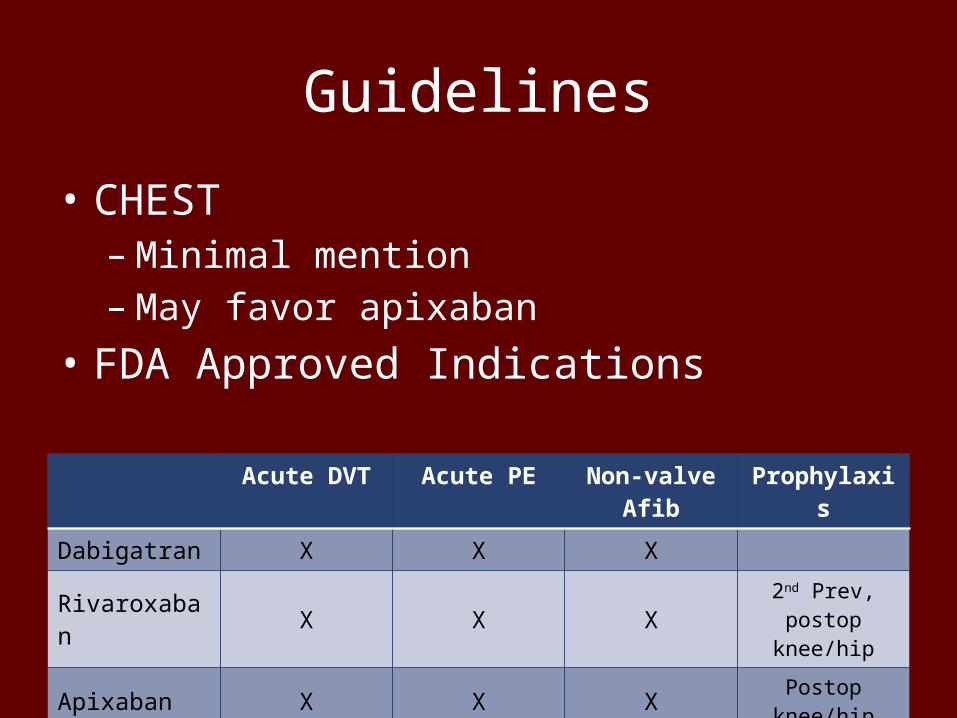
Guidelines
• CHEST– Minimal mention– May favor apixaban
• FDA Approved Indications
Acute DVT Acute PE Non-valve Afib Prophylaxis
Dabigatran X X X
Rivaroxaban X X X 2nd Prev, postop knee/hip
Apixaban X X X Postop knee/hip
Common Questions
• Warfarin– Management of INR out of range• High INR without bleeding• Low INR• When to use vitamin K?
– Initiation• Loading dose?• When to monitor INR?• Bridging?
CV OUTCOMES WITH ANTIPSYCHOTICS
A Quick Look
26
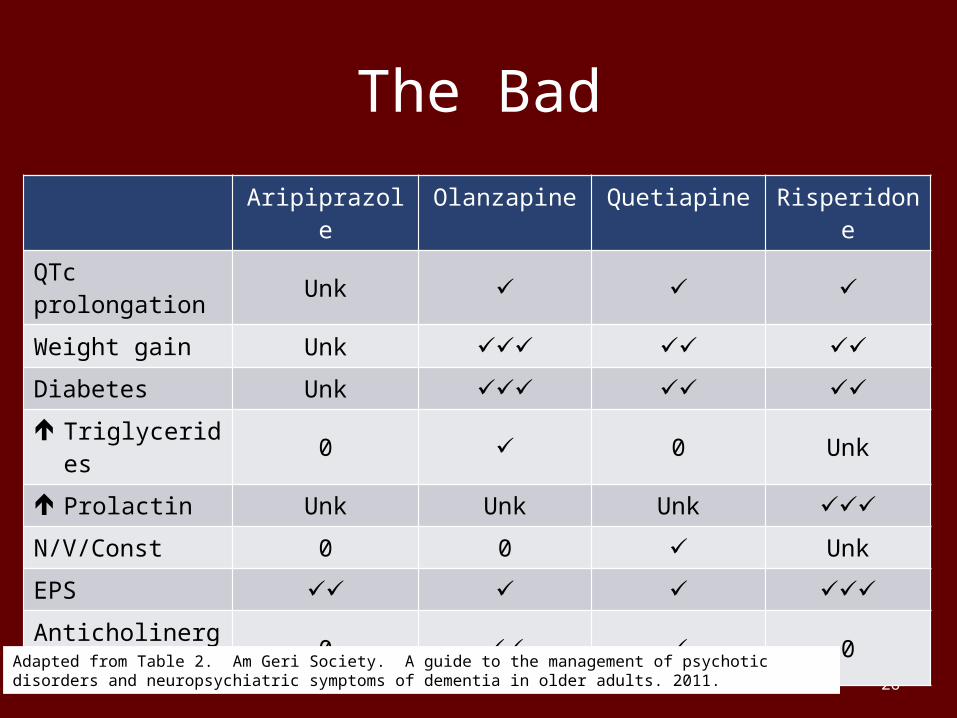
The BadAripiprazole Olanzapine Quetiapine Risperidone
QTc prolongation Unk ✓ ✓ ✓Weight gain Unk ✓✓✓ ✓✓ ✓✓Diabetes Unk ✓✓✓ ✓✓ ✓✓ Triglycerides 0 ✓ 0 Unk Prolactin Unk Unk Unk ✓✓✓N/V/Const 0 0 ✓ UnkEPS ✓✓ ✓ ✓ ✓✓✓Anticholinergic 0 ✓✓ ✓ 0
Adapted from Table 2. Am Geri Society. A guide to the management of psychotic disorders and neuropsychiatric symptoms of dementia in older adults. 2011.
27
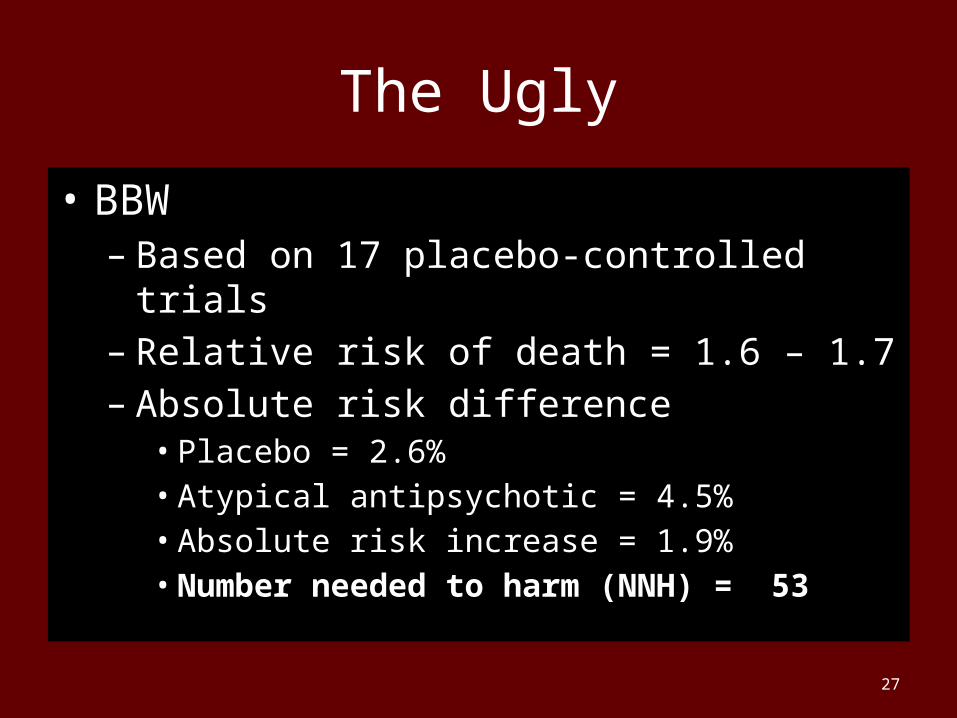
The Ugly
• BBW– Based on 17 placebo-controlled trials– Relative risk of death = 1.6 – 1.7– Absolute risk difference• Placebo = 2.6%• Atypical antipsychotic = 4.5%• Absolute risk increase = 1.9%• Number needed to harm (NNH) = 53
28
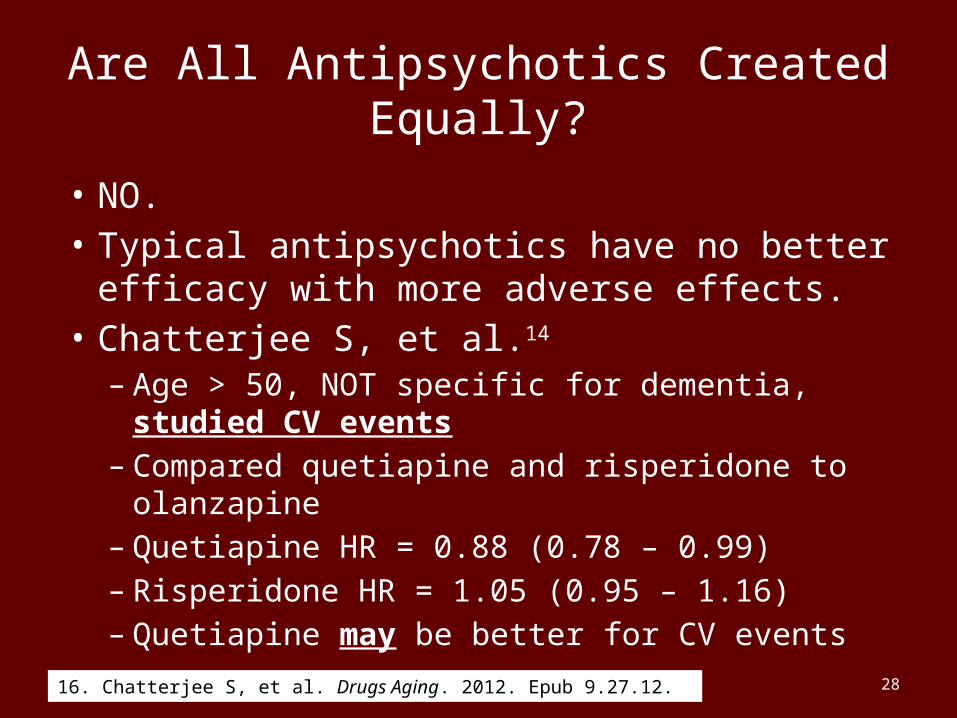
Are All Antipsychotics Created Equally?
• NO.• Typical antipsychotics have no better efficacy
with more adverse effects.• Chatterjee S, et al.14
– Age > 50, NOT specific for dementia, studied CV events
– Compared quetiapine and risperidone to olanzapine– Quetiapine HR = 0.88 (0.78 – 0.99)– Risperidone HR = 1.05 (0.95 – 1.16)– Quetiapine may be better for CV events
16. Chatterjee S, et al. Drugs Aging. 2012. Epub 9.27.12.
29
Are All Antipsychotics Created Equally?
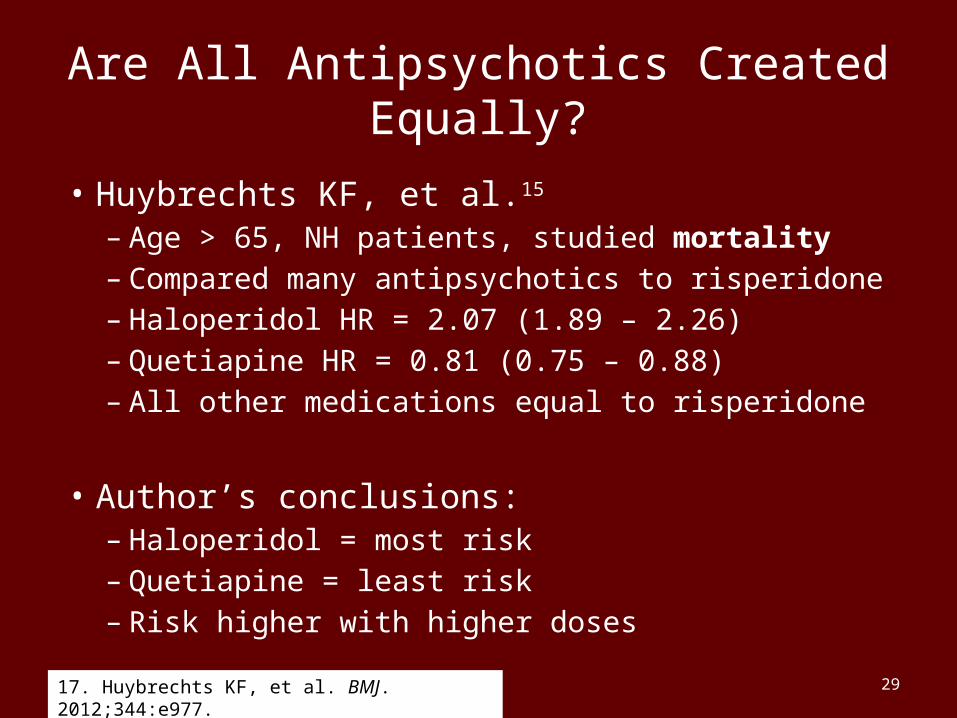
• Huybrechts KF, et al.15
– Age > 65, NH patients, studied mortality– Compared many antipsychotics to risperidone– Haloperidol HR = 2.07 (1.89 – 2.26)– Quetiapine HR = 0.81 (0.75 – 0.88)– All other medications equal to risperidone
• Author’s conclusions: – Haloperidol = most risk– Quetiapine = least risk– Risk higher with higher doses
17. Huybrechts KF, et al. BMJ. 2012;344:e977.
CMS Initial Goals
• 2011 – CMS initiative announced• 12% reduction in antipsychotic use across the
board nationally• Reasons:– Poor data for efficacy– Good data for adverse effects– Cost – $7.6 BILLION for part D (8.4% of total
2011 part D budget)• How did we do????
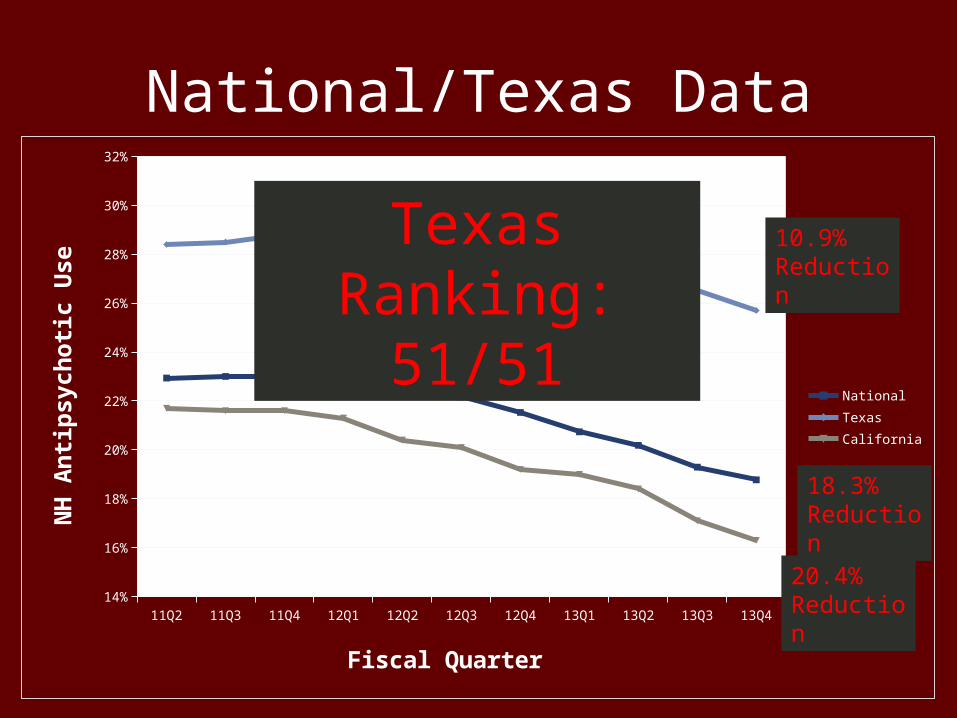
National/Texas Data
11Q2 11Q3 11Q4 12Q1 12Q2 12Q3 12Q4 13Q1 13Q2 13Q3 13Q414%
16%
18%
20%
22%
24%
26%
28%
30%
32%
NationalTexasCalifornia
Fiscal Quarter
NH
Anti
psyc
hotic
Use
10.9% Reduction
Texas Ranking:51/51
20.4% Reduction
18.3% Reduction
CMS New Goals
• 25% reduction by end of 2015*• 30% reduction by end of 2016*• Will be checking to make sure that the meds aren’t just
replaced with anxiolytics and other sedatives
*Measured as reduction from 11Q4
Patient Case
• Divide into small groups (4-5) of different disciplines if possible
• Take a few minutes to read and discuss the simple case
Patient Case
• Question 1 – What drug regimen would you use to treat HH’s Afib?
• Question 2 – Is HH a low, moderate, or high stroke risk?
• Question 3 – Based on risk, what drug regimen would you start for stroke prevention?
Patient Case
• Question 4 – The decision is made to start Apixaban. What dose?
• 6 months later, HH decides that he can’t live with taking a blood thinner with no antidote. He wants warfarin now. How do you convert to warfarin?
Medication Influence on Cardiovascular Outcomes
Jamie McCarrell, Pharm.D., BCPS, CGPAssistant Professor, TTUHSC SOP/SOM