medicare claims appeals: from audit to omha decisional independence ... pre-hearing conferences ......
TRANSCRIPT
1
+
American Health Lawyers Association
March 2013
Medicare Claims Appeals:From Audit to OMHA
Donna K. ThielPartnerKing & Spalding, LLCWashington, DC
+
The Appeals Process
Original Medicare Appeals Processhttp://www.cms.gov/Medicare/Appeals-and-Grievances/OrgMedFFSAppeals/index.html
2
+ Issues Addressed Today
Different Procedures For Direct Challenges To Local and National Coverage Decisions
Different process for Enrollment/disenrollment
Claims, Not Cost Reporting
Medical Necessity Is The Primary Issue Statistical Validity Of Sample
Timeliness of Reopening
Waiver Of Recovery/ABN
3
+ Who Denied the Claim?
Pre-Payment Medicare Contractors (MACs)
Providers
Practitioners
DMACs: DMEPOS Claims
Post-Payment MACs and DMACs
Specialty Auditors
RACs ZPICs PSCs
4

3
+ Medicare Administrative Contractors
15 MACs and 4 DMACs for redeterminations.
2 Part A QICs (Maximus - both jurisdictions)
2 Part B QICs (First Coast Service Options and Q2 Administrators)
1 DME QIC (C2C)
5
+Specialty Auditors
Zone Program Integrity Contractors
Recovery Audit Contractors
ZPICs/RAC are authorized to conduct audits, interview beneficiaries and providers, initiate administrative sanctions (including suspending payments, determining overpayments, and referring providers for exclusion from Medicare), and refer providers and beneficiaries to law enforcement.
The ZPICs/RAC also are expected to use "innovative data analysis methodologies for the early detection and prevention of abusive use of services, as well as possible fraud, waste and abuse schemes."
6

4
+ZPICs
ZPICs were created to perform program integrity for Medicare Parts A, B, C (Medicare Advantage) D (Prescription Drugs), Durable Medical Equipment (DME), Home Health and Hospice.
When Medicare began the process of moving Part A and Part B intermediaries and carriers into the Medicare Contractor system, CMS also moved the program integrity component of their duties into program safeguard contractors or PSCs. The ZPICs replaced the existing Program Safeguard Contractors (“PSCs”)
The ZPICs are paid by CMS, but unlike the RACs, reimbursement to a ZPIC is not contingent upon any overpayment amounts recovered by the ZPIC.
7
+Specialty Auditors: Zone Program Integrity Contractors
ZPICs perform program integrity for Medicare Parts A, B, C (Medicare Advantage) D (Prescription Drugs). The ZPICs replaced the existing Program Safeguard Contractors (“PSCs”)
Reimbursement to a ZPIC is not contingent upon any overpayment amounts recovered by the ZPIC.
ZPICs calculate overpayments based on Statistical Sampling
Seehttp://www.cms.gov/MLNProducts/downloads/ContractorEntityGuide_ICN906983.pdf
Zone 7 is devoted almost solely to Florida, considered a "hot zone" because of a high incidence of Medicare fraud. Other "hot zones" include California and Texas (Houston and Dallas). Zone 2 covers a vast territory of largely western and southwestern states where there has not historically been a high prevalence of Medicare billing issues
8
5
+Overpayment Based on Sampling
Universe: All claims in two year period
Frame: Eliminates cases outside the audit design
Sample Design: How large a sample based on precision/error rate
Sample: Random Selection of Claims
By Beneficiary or By Claim
These claims will be the subject of the appeal
Sample: 31 claims, Claims Denied: 31
Error Rate: 100
Actual Overpayment: $44,155.84
Extrapolated Overpayment $ 5,751,331
9
+Recovery Audit Contractors (RACs)
4 RACs- Same jurisdiction as DME MACs
Region A: Diversified Collection Services
Region B: CGI
Region C: Connolly, Inc.
Region D: HealthDataInsights, Inc.
2
10

6
+Bonus on RAC results
RACs are paid on a contingency fee based on the amount of over and underpayments corrected Contingency Fees Region A -12.45% Region B - 12.50% Region C - 9% Region D - 9.49%
Contingency fee returned if denials are overturned on appeal
RACs are not authorized to investigate fraud but are required to refer possible fraud to CMS
Suspension of Payments
11
+The Appeal Process: Part A and Part B
12
7
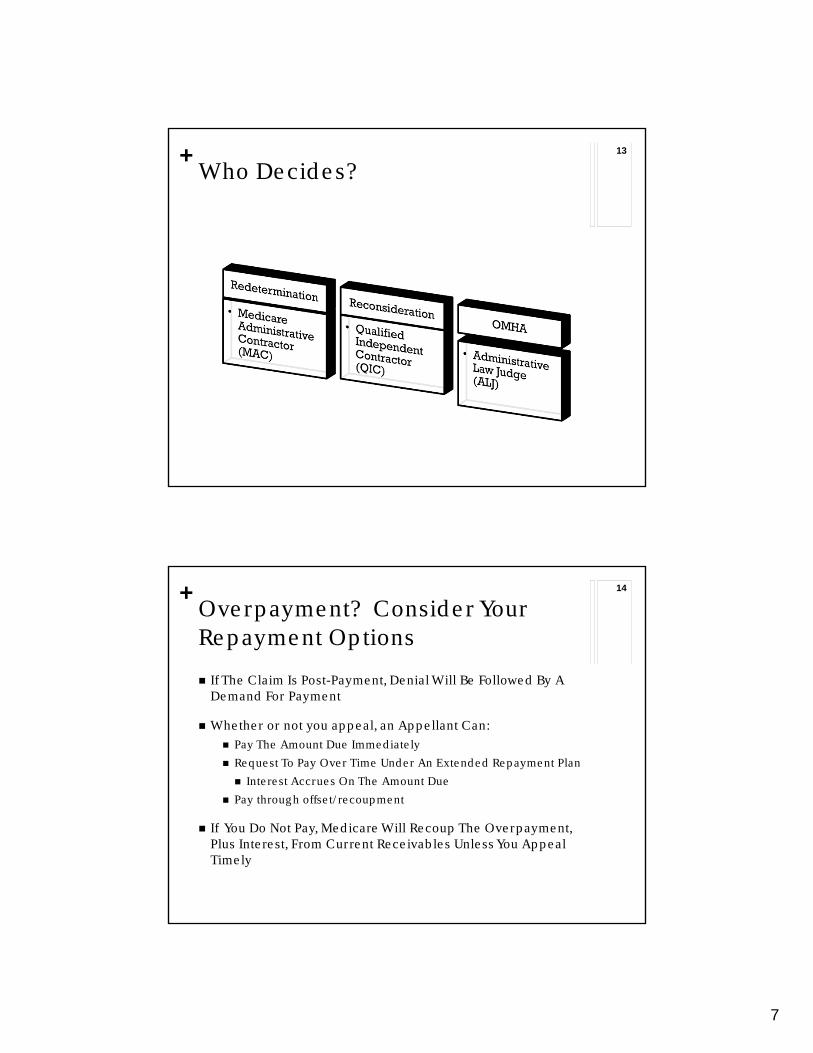
+Who Decides?
13
+Overpayment? Consider Your Repayment Options
If The Claim Is Post-Payment, Denial Will Be Followed By A Demand For Payment
Whether or not you appeal, an Appellant Can: Pay The Amount Due Immediately
Request To Pay Over Time Under An Extended Repayment Plan
Interest Accrues On The Amount Due
Pay through offset/recoupment
If You Do Not Pay, Medicare Will Recoup The Overpayment, Plus Interest, From Current Receivables Unless You Appeal Timely
14

8
+
Staying Recoupment Pending Appeal
Medicare will not recoup an overpayment if you appeal ‘super’ timely. Section 935(f)(2) of the Medicare
Modernization Act 42 USC 1395ddd(f)(2)
Redetermination: Appeal within 30 days of the notice of overpayment to stay recoupment. Ordinary Appeal deadline for
Redeterminations is 120 days If you lose, you can pay, request an
ERP or appeal to the second level
Reconsideration: Appeal within 60 days of Redetermination to stay the recoupment Appeal deadline for
Reconsideration is 180 days
+Getting Started
Medicare Claims Processing Manual Chapter 29 - Appeals of Claims Decisions http://www.cms.gov/Regulations-and-
Guidance/Guidance/Manuals/downloads/clm104c29.pdf
Once an initial claim determination is made by a contractor, beneficiaries, providers, participating physicians and suppliers have the right to appeal the determination
All appeal requests must be made in writing
16
9
+Requesting an Appeal
A written request must include (at Every Level):
Beneficiary name
Medicare Health Insurance Claim (HIC) number•
Specific service and/or item(s) for which a redetermination is being requested
Specific date(s) of service
Name and signature of the party or the representative of the party
The appellant should attach any supporting documentation to the request for Appeal. See discussion below about establishing the record
A request may be filed on Form CMS-20027
www.cms.gov/Medicare/CMS-Forms/ CMS-Forms/CMS-Forms-List.html
17
+Getting Started: Parties Who may appeal?
Beneficiaries, Providers, Suppliers
Physicians and other suppliers who do not take assignment on claims have limited appeal rights
Non-Party Must Submit Authorization Of Representative
42 CFR § 405.910 CMS Form 1696, www.cms.gov/Medicare/CMS-Forms/CMS-Forms/CMS-Forms-
Items/CMS012207.html
Authorization Of Representative is Different than Assignment
Beneficiaries may transfer their appeal rights to non-participating physicians or suppliers who provide the items or services and do not otherwise have appeal rights
Form CMS-20031 must be completed and signed by the beneficiary and the nonparticipating physician or supplier to transfer the beneficiary’s appeal rights.
18
10
+
Level One: Redetermination
+Level One: Redetermination
Written Request To MAC/DMAC
Must Be Filed In 120 Days From Initial Determination (Denial)
Must Be Decided In 60 Days
Recoupment Can Be Stayed If Appeal Is Filed By Day 30
20

11
+Overpayment Based on a Sample
Keep all claims in the sample together
Note on your pleadings that the cases are part of a statistical sample
Request Documentation on the Sampling Methodology
Hire a Statistician to Evaluate the Sampling
Ensure none of the claims in the Sample have been appealed before
21
+
Level Two: Reconsideration

12
+Level Two: Reconsideration
A party to the redetermination may request a reconsideration if dissatisfied with the redetermination.
Written Request to QIC
Written reconsideration request must be filed with the QIC within 180 days of receipt of the redetermination.
23
+Reconsideration No monetary threshold
A request for a reconsideration may be made on Form CMS-20033 www. cms.gov/Medicare/CMS-Forms/CMS-Forms/CMS- Forms-
List.html.
If the form is not used, the written request must contain all information noted above PLUS: A copy of the RA or Redetermination
Any additional documentation to address the Decision below
Address denial in Redetermination but do not limit your argument to that decision
Documentation that is submitted after the reconsideration request has been filed may result in an extension of the timeframe a QIC has to complete its decision.
24

13
+Qualified Independent Contractor
The QIC Is A Panel Of Physicians Or Other Appropriate Health Care Professionals
Must Have Sufficient Medical Legal And Other Expertise Including Knowledge Of Medicare Program Only MDs Can Review MD Claims
Reconsiderations are conducted on-the-record If the QIC cannot complete its decision in the applicable
timeframe, it will inform the appellants of their right to escalate the case to an ALJ
Only evidence submitted before the issuance of the QIC decision can be considered in subsequent appeals, unless
good cause is shown for any delay.
+
Level Three: Office of Medicare Hearings and Appeals

14
+Request for ALJ Hearing
If at least $140 remains in controversy following the QIC’s decision, a party to the reconsideration may request an ALJ hearing
Appeal must be filed in writing within 60 days of receipt of the Reconsideration decision.
Reconsideration decision letter contains procedures for requesting an ALJ hearing. Form CMS-20034 may be used to file a request
Appellants must also send a copy of the ALJ hearing request to all other parties to the QIC reconsideration. (Beneficiary?)
27
+Request for an ALJ hearing.
42 CFR §405.1014(a) The request for an ALJ hearing must be made in writing. The
request must include all of the following— (1) The name, address, and Medicare health insurance claim
number of the beneficiary whose claim is being appealed. (2) The name and address of the appellant, when the appellant is
not the beneficiary. (3) The name and address of the designated representatives if any. (4) The document control number assigned to the appeal by the
QIC, if any. (5) The dates of service. (6) The reasons the appellant disagrees with the QIC's
reconsideration or other determination being appealed. (7) A statement of any additional evidence to be submitted and the
date it will be submitted.
28

15
+Requesting an ALJ Hearing
Jurisdictional Elements QIC reconsideration/dismissal/Escalation
Amount in Controversy ($140) (2013)
Timely Request (60 days)
Party standing
Requests for Hearing Send to Centralized Docketing
Copying Parties
29
Part A/B Appeals42 C.F.R. §405,
sub I
Part C Appeals42 C.F.R. §422,
sub M
Part D Appeals42 C.F.R. §423,
sub U
+OMHA Locations
Arlington, Virginia (Mid-Atlantic)
Cleveland, Ohio (Midwestern)
Irvine, California (Western)
Miami, Florida (Southern)
HHS OMHA Centralized Docketing200 Public Square, Suite 1260Cleveland, OH 44114-2316
30

16
+ALJ Authority
ALJ Decisional Independence New look at the claim (de novo review)
ALJ is Finder of Fact
Must apply Statutes, Regulations, CMS Rulings, NCDs
Substantial Deference—LCDs, CMS Manuals
Application of LCD, Manual Instructions
Whether Sampling Met CMS Requirements
Liability Issues §1879 Limitation on Liability
§1870 Overpayment Waiver
31
+Hearing Request Issues
Aggregating Claims Used to meet the amount in controversy requirement
Confirm
Consolidated Hearings Cases must be before the same ALJ
Evidence Document your submissions at lower levels
Good cause must established for submitting evidence for the first time at the ALJ level (42 CFR §405.1028)
32

17
+Conduct of Hearings
Pre-Hearing Conferences
ALJ Assignment Random Rotation
National Jurisdiction
42 CFR §405.1020 Video-Teleconference (VTC)
Teleconference
In-Person
CMS or Contractor Involvement
33
+Decisions Time Frame
Possible Delays
All parties not copied on the request for hearing (§405.1014) Untimely request for hearing (§405.1014) Request for hearing sent to the incorrect entity (§405.1014) Discovery requested (§405.1016, §405.1037) Written evidence is submitted late (§405.1018) Hearing is rescheduled at the Appellant’s request (§405.1020) Appellant has material missing evidence (§405.1030) Appellant waives timeframe (§405.1036) Party request for opportunity to comment on the record
(§405.1042) Consolidated hearing granted at request of appellant
(§405.1044)
34

18
+
Level Four: Appeals Council
+Appeals Council
ALJ Decision is binding on the parties, unless reopened or Appeals Council decides to review
CMS can refer cases for “Own Motion Review”
If a party to the ALJ hearing is dissatisfied with the ALJ’s decision, the party may request a review by the Appeals Council
Must be filed within 60 days of ALJ Decision
No Financial Threshold
Must specify the issues and findings that are being contested
36

19
+
Level Five: Federal Court
+Federal Court
Party
Any party to the Medicare Appeals Council decision
Appellant who requests escalation to Federal district court if the Appeals Council does not complete its review of an administrative law judge's (ALJ's) decision within the applicable adjudication period,
Amount remaining in controversy must satisfy the requirements set forth in 42 CFR §405.1006
$1400 for 2013
Timely
60 days to request review
Standard of review: substantial evidence based on the record
38

20
+
Practice Tips
+Making Your Case
Review Starts with the Premise that something less (or less expensive) could have been done
Rapid Response for Admission or Initiation Patient failed to improve on prior therapy or in a different setting?
Patient sick enough (fragile enough) to require admission, adjuvant therapy, special equipment?
The risks of not engaging the services/items
Treatment has been considered, or tried or ruled out
40

21
+Making the Prima Facie Case
Avoid “Technical Denials”
Audit for any Specialized Documentation You Must have To Establish Coverage Prescription/Orders
Recertification
CMN
Signatures
� Audit for Facts You Must Prove To Establish Coverage Prerequisites Satisfied
Other Aspects of Care Management
41
+Challenge of Establishing Medical Necessity
Establish the Link between Payor’s Coverage Criteria and the Clinical Case
Document Severity Illness or Conditions or Comorbidities
Document Intensity Of therapy, Of testing, Of treatment
Document Plan of Care Consistent with Coverage Policy
Explain Deviations from Policy
42

22
+Timing is Everything
Document Patients condition at the time the order was placed
Chronic Illness must be addressed (diabetes, COPD, CHF Immobility do not go away but address implications on a continuing basis (every day!)
Entire record should reflect severity/risk that justifies the treatment continuously
Document Progress (relative to last note) or lack of it
43
+Defending Your Claims
• Do Not Assume That The Adjudicator Will Be Familiar With The Relevant Benefit Or Its Coverage Criteria
• Set Out The Relevant Coverage Policy• Medicare Statute, Regulations, Manuals, LCDs, Or NCDs
• Payor Contracts
• Describe your Products • Mechanisms of Action
• Documentation Methods
44

23
+Avoid These Pitfalls
Delay Don’t Procrastinate In Starting The Appeal Process Do Not Put Off Collecting Medical Records For The ‘Next Level Of
Appeal’
Submitting Evidence As If It Speaks For Itself Tell The Story Of Your Services Draft A Cover Page To Be Appended To Each Set of Documents Telling
The Patient’s Story, Referring To Specific Notations In The Record Summarize Critical Elements In The Patient’s Case and Cite to the
Record
45
46