medical genetics assoc. prof. Ömer faruk bayrak department of medical genetics yeditepe university
TRANSCRIPT
Medical Genetics
Assoc. Prof. Ömer Faruk BayrakDepartment of Medical GeneticsYeditepe University
Classical and Modern Genetics1. Humans have long understood that offspring tend to resemble
parents, and have selectively bred animals and plants for many centuries. The principles of heredity were first explained by Mendel in the mid nineteenth century, using defined crosses of pea plants.
2. In the last century, genetics has become an important biological tool, using mutants to gain an understanding of specific processes. This work has included:a. Analyzing heredity in populations.b. Analyzing evolutionary processes.c. Identifying genes that control steps in processes.d. Mapping genes.e. Determining products of genes.f. Analyzing molecular features of genes and regulation of gene
expression.
1900
1901
1902
1918
1931
19551937
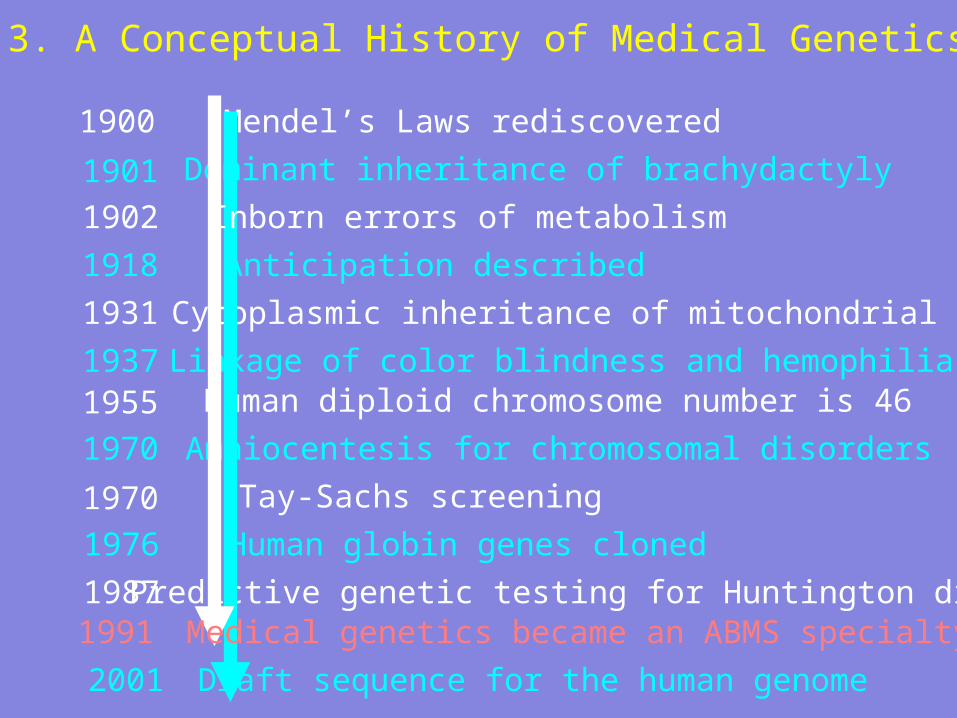
Mendel’s Laws rediscovered
Anticipation described
Dominant inheritance of brachydactyly
Cytoplasmic inheritance of mitochondrial DNA
Linkage of color blindness and hemophiliaHuman diploid chromosome number is 46
Amniocentesis for chromosomal disorders
Tay-Sachs screening
Predictive genetic testing for Huntington disease
1970
1987
1970
3. A Conceptual History of Medical Genetics
Inborn errors of metabolism
Human globin genes cloned1976
Draft sequence for the human genome2001
1991 Medical genetics became an ABMS specialty
Classical and Modern Genetics
4. Completion of genomic sequencing for an increasing number of organisms has spawned the new field of genomics. Knowledge of individual genes and their regulation will be important to basic biological research, as well as to specific applications such as medical genetics.
5. Powerful new techniques in genetics raise important ethical, legal and social issues that will need thoughtful solutions.
Human Genome Project• Proposed in 1985• 1988. Initiated and funded
by NIH and US Dept. of Energy ($3 billion set aside)
• 1990. Work begins.• 1998. Celera announces a 3-
year plan to complete the project years early
• Published in Science and Nature in February, 2001
What we’ve learned from our genome so far…
• There are a relatively small number of human genes, less than 30,000, but they have a complex architecture that we are only beginning to understand and appreciate.
-We know where 85% of genes are in the sequence. -We don’t know where the other 15% are because
we haven’t seen them “on” (they may only be expressed during fetal development).
-We only know what about 20% of our genes do so far.
• So it is relatively easy to locate genes in the genome, but it is hard to figure out what they do.

How much data make up the human genome?
3 pallets with 40 boxes per pallet x 5000 3 pallets with 40 boxes per pallet x 5000 pages per box x 5000 bases per page = pages per box x 5000 bases per page = 3,000,000,000 bases!3,000,000,000 bases!
To get accurate To get accurate sequence requires sequence requires 6-fold coverage. 6-fold coverage.
Now: Shred 18 pallets Now: Shred 18 pallets and reassemble.and reassemble.
Human genome content
• 1-2 % codes for protein products• 24% important for translation• 75% “junk”• Repetitive elements
– Satellites (regular, mini-, micro-)– Transposons– Retrotransposons– Parasites
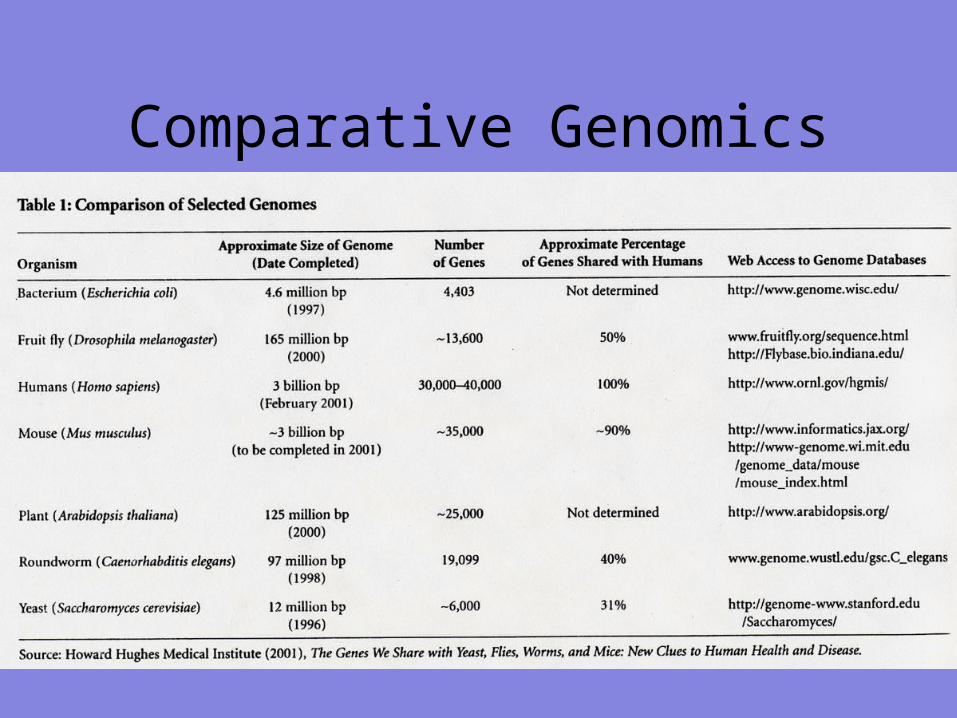
Comparative Genomics

What Do Medical Geneticists Do
Diagnosis and treatment of genetic disease
Presymptomatic testing for genetic disease
Carrier testing, especially for high risk people
Genetic counseling during pregnancy
Genetic Evaluation Data gathering
History, especially family history
Physical examination - major and subtle findings
Pattern recognition
Laboratory testing – EMG, DNA
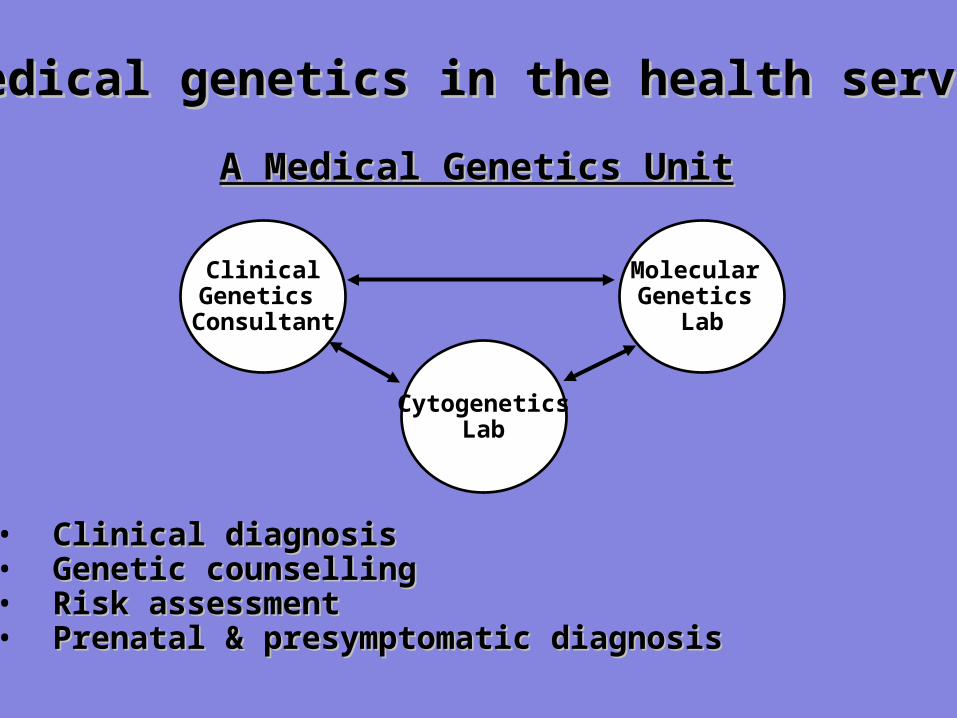
ClinicalGenetics
Consultant
CytogeneticsLab
Molecular Genetics
Lab
A Medical Genetics UnitA Medical Genetics Unit
• Clinical diagnosisClinical diagnosis• Genetic counsellingGenetic counselling• Risk assessmentRisk assessment• Prenatal & presymptomatic diagnosisPrenatal & presymptomatic diagnosis
Medical genetics in the health serviceMedical genetics in the health service
What Should You Know?• Basic understanding of clinical
genetics
• Be able to draw, and understand, a family tree
• Have awareness of when you should be considering a genetic condition
• Have a working knowledge of the most important genetic conditions
• Know how & when to refer to local specialist genetics services
Genetic diseases
• traditionally - 3 types of diseases• 1. genetically determined• 2. environmentally determined• 3. 1. + 2.• today - distinctions are blurred• up to 20% of pediatric in-patients have genetic abnormality• about 50% of spontaneous abortuses have chromosomal
aberration• only mutations that are not lethal are reservoir of genetic
diseases
Role of Genes in Human Disease
• Most diseases / phenotypes result from the interaction between genes and the environment
• Some phenotypes are primarily genetically determined– Achondroplasia
• Other phenotypes require genetic and environmental factors– Mental retardation in persons with PKU
• Some phenotypes result primarily from the environment or chance– Lead poisoning
Terminology
• hereditary = derived from parents • familial = transmitted in the gametes through
generations• congenital = present at birth (not always
genetically determined - e.g. congenital syphilis, toxoplasmosis)
• ! not all genetical diseases are congenital - e.g. Huntington disease - 3rd to 4th decade of life
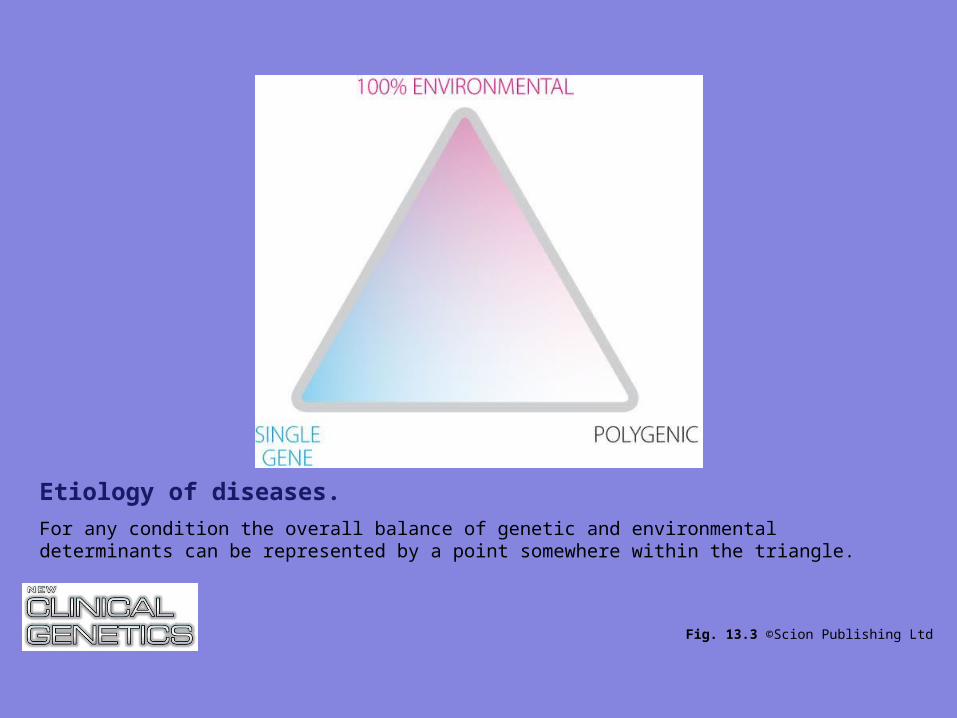
Fig. 13.3 ©Scion Publishing Ltd
Etiology of diseases.
For any condition the overall balance of genetic and environmental determinants can be represented by a point somewhere within the triangle.
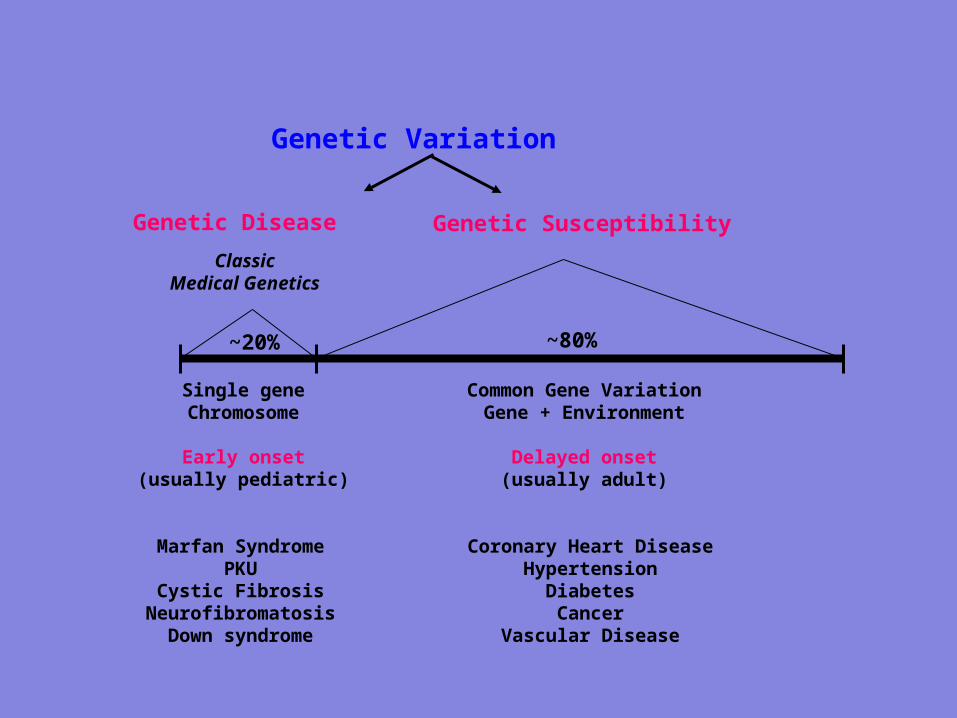
~20%
ClassicMedical Genetics
Single geneChromosome
Early onset(usually pediatric)
Marfan SyndromePKU
Cystic FibrosisNeurofibromatosis
Down syndrome
Genetic Disease
Genetic Variation
~80%
Genetic Susceptibility
Common Gene VariationGene + Environment
Delayed onset(usually adult)
Coronary Heart DiseaseHypertension
DiabetesCancer
Vascular Disease
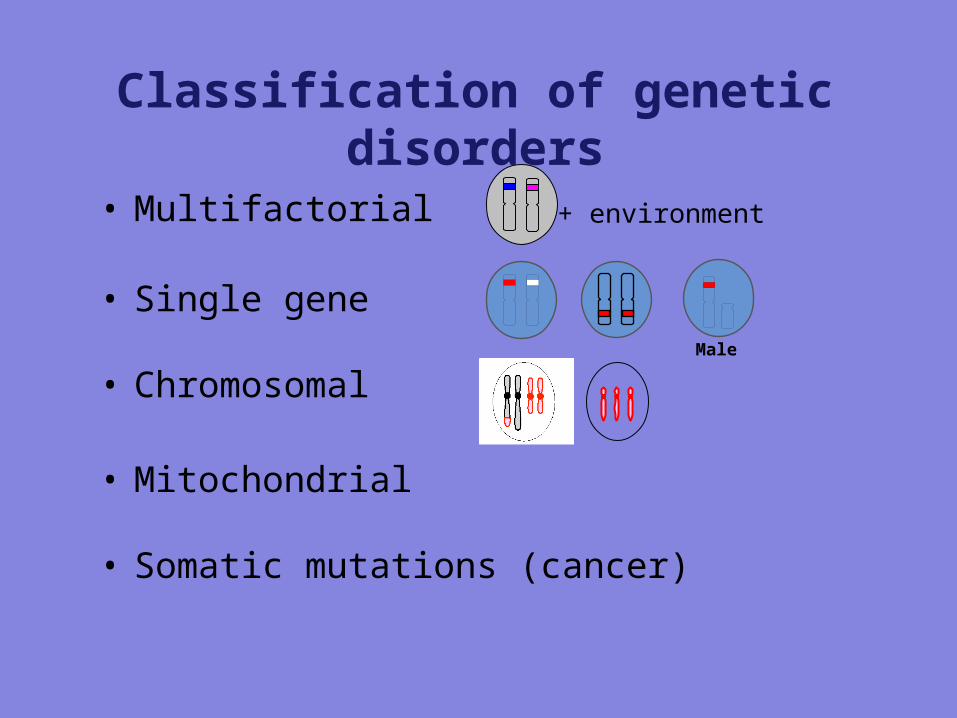
Classification of genetic disorders
• Multifactorial
• Single gene
• Chromosomal
• Mitochondrial
• Somatic mutations (cancer)
Male
+ environment
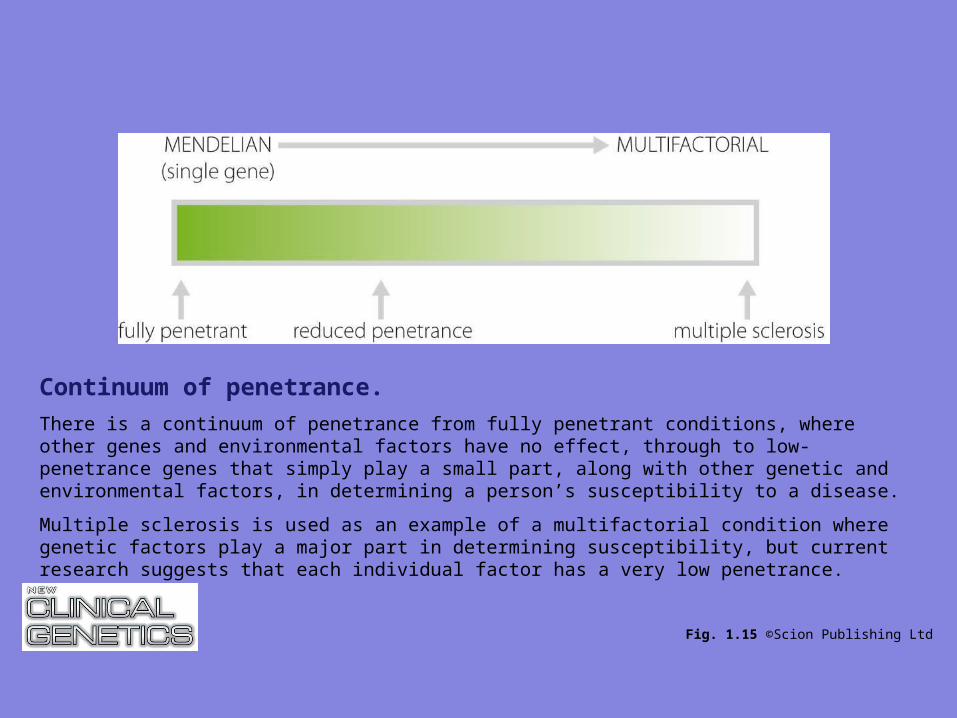
Fig. 1.15 ©Scion Publishing Ltd
Continuum of penetrance.
There is a continuum of penetrance from fully penetrant conditions, where other genes and environmental factors have no effect, through to low-penetrance genes that simply play a small part, along with other genetic and environmental factors, in determining a person’s susceptibility to a disease.
Multiple sclerosis is used as an example of a multifactorial condition where genetic factors play a major part in determining susceptibility, but current research suggests that each individual factor has a very low penetrance.
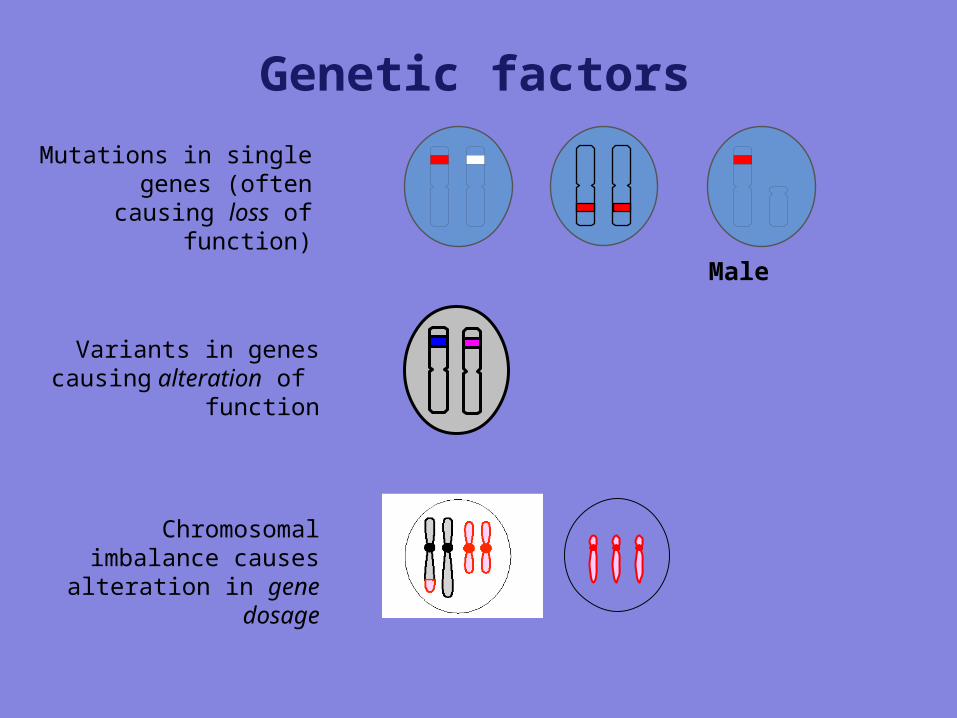
Genetic factors
Male
Mutations in singlegenes (often causing
loss of function)
Variants in genes causing alteration of
function
Chromosomal imbalance causes alteration in gene
dosage
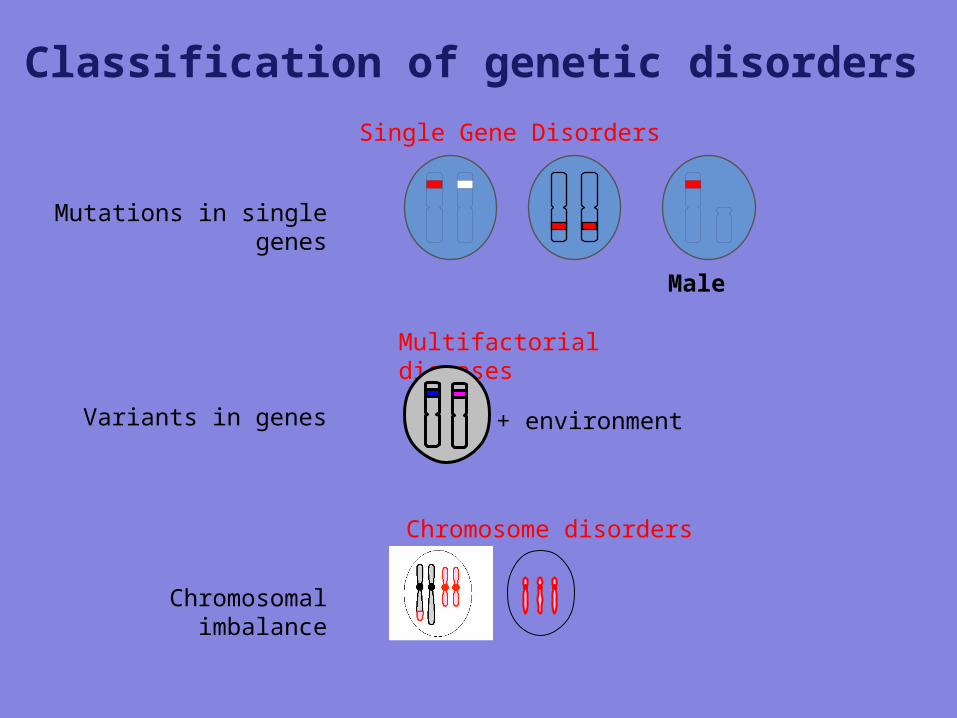
Classification of genetic disorders
Male
Mutations in single genes
Variants in genes
Chromosomal imbalance
Single Gene Disorders
Multifactorial diseases
Chromosome disorders
+ environment
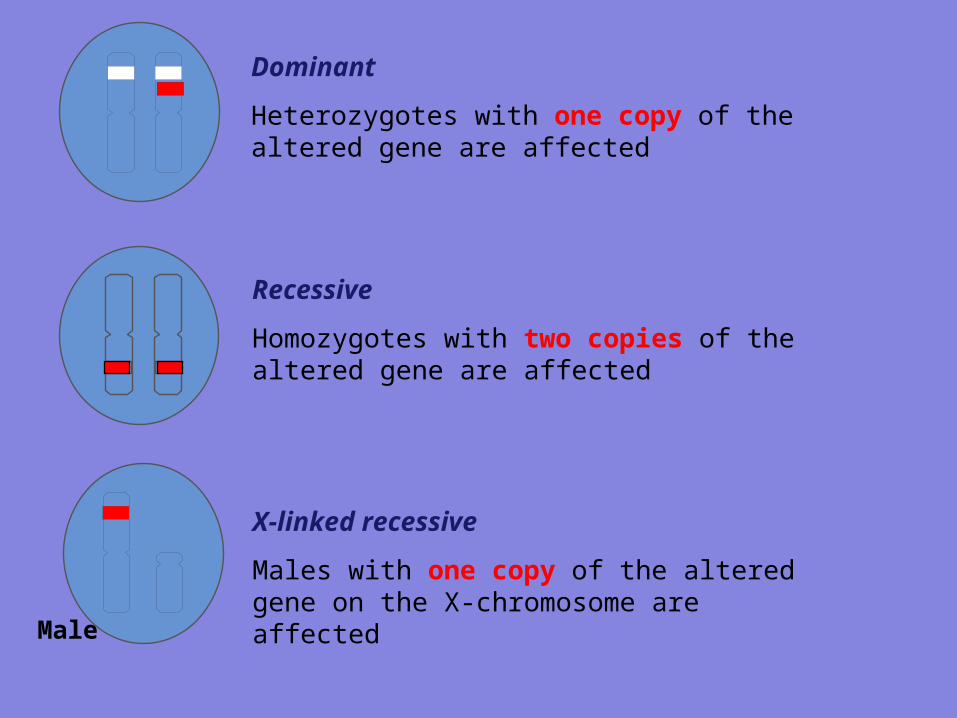
Recessive
Homozygotes with two copies of the altered gene are affected
Dominant
Heterozygotes with one copy of the altered gene are affected
X-linked recessive
Males with one copy of the altered gene on the X-chromosome are affected
Male
Genetic disorders• Multifactorial (common)
- “Environmental” influences act on a genetic predisposition to produce a liability to a disease.- One organ system affected.- Person affected if liability above a threshold.
• Single gene (1% liveborn) - Dominant/recessive pedigree patterns (Mendelian inheritance). - Can affect structural proteins, enzymes, receptors, transcription factors.
• Chromosomal (0.6% liveborn)- Thousands of genes may be involved.- Multiple organ systems affected at multiple stages in gestation.- Usually de novo (trisomies, deletions, duplications) but can be inherited (translocations).
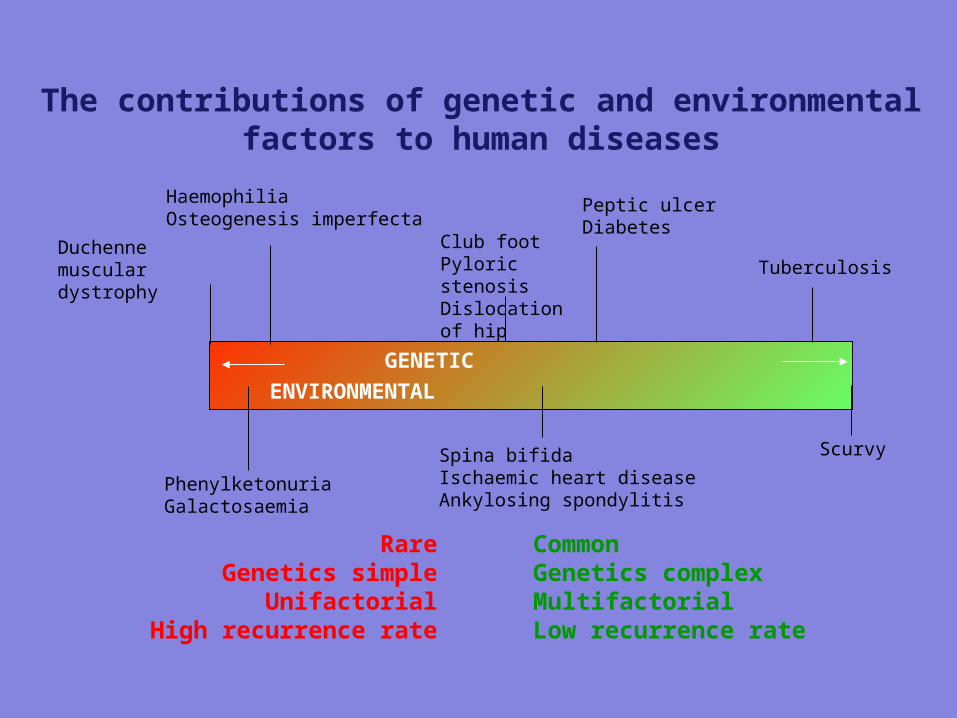
GENETIC ENVIRONMENTAL
Duchenne muscular dystrophy
HaemophiliaOsteogenesis imperfecta
Club footPyloric stenosisDislocation of hip
Peptic ulcerDiabetes
Tuberculosis
PhenylketonuriaGalactosaemia
Spina bifidaIschaemic heart diseaseAnkylosing spondylitis
Scurvy
The contributions of genetic and environmental factors to human diseases
RareGenetics simple
UnifactorialHigh recurrence rate
CommonGenetics complexMultifactorialLow recurrence rate
• Multifactorial“Environmental” influences act on a genetic predispositionOne organ system affected
• Single geneDominant/recessive pedigree patternsStructural proteins, enzymes, receptors, transcription
factors
• ChromosomalMultiple organ systems affectedInherited or de novo
• EnvironmentalDrugs, infections
The Family History is a powerful toolfor estimating genetic risk
Obtain information on children, sibs, and parentsAge/date of birth
Health statusAge at death
Cause of death
This is the ‘nuclear’ family
Expand as necessary to grandparents, uncles & aunts, etc.
The Family History
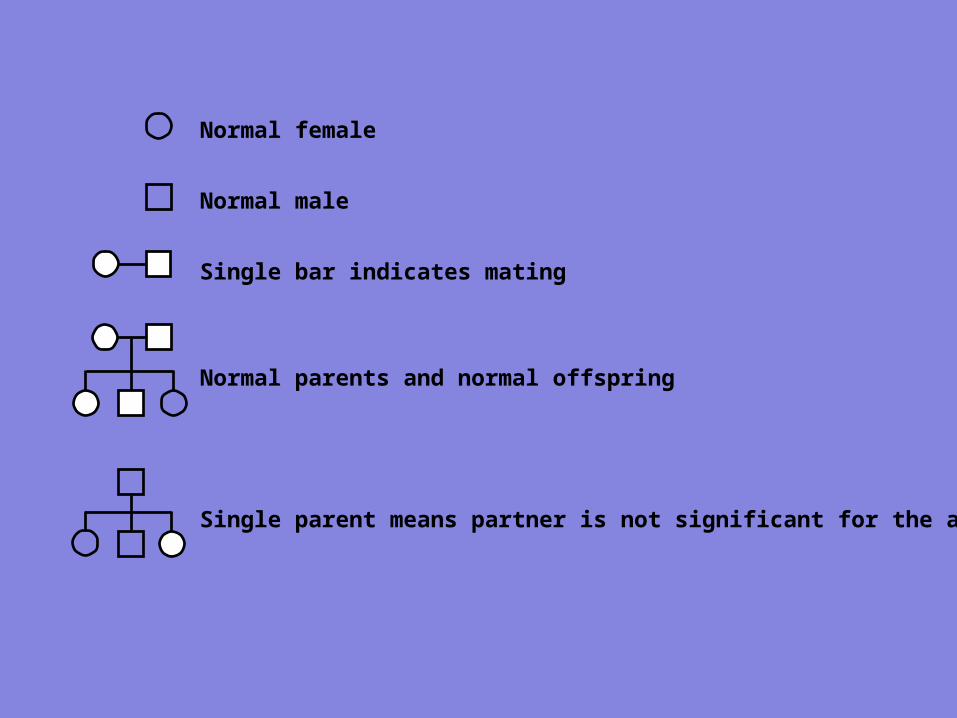
Normal female
Normal male
Single bar indicates mating
Normal parents and normal offspring
Single parent means partner is not significant for the analysis
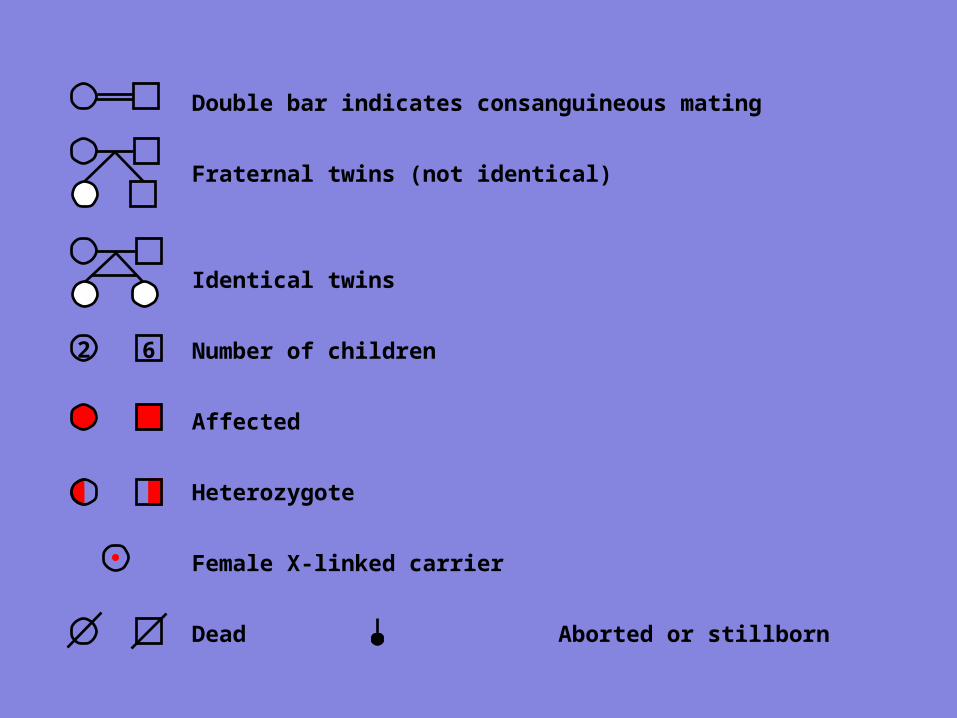
Double bar indicates consanguineous mating
Fraternal twins (not identical)
Identical twins
Number of children
Affected
Heterozygote
Female X-linked carrier
Dead Aborted or stillborn
62
2 3
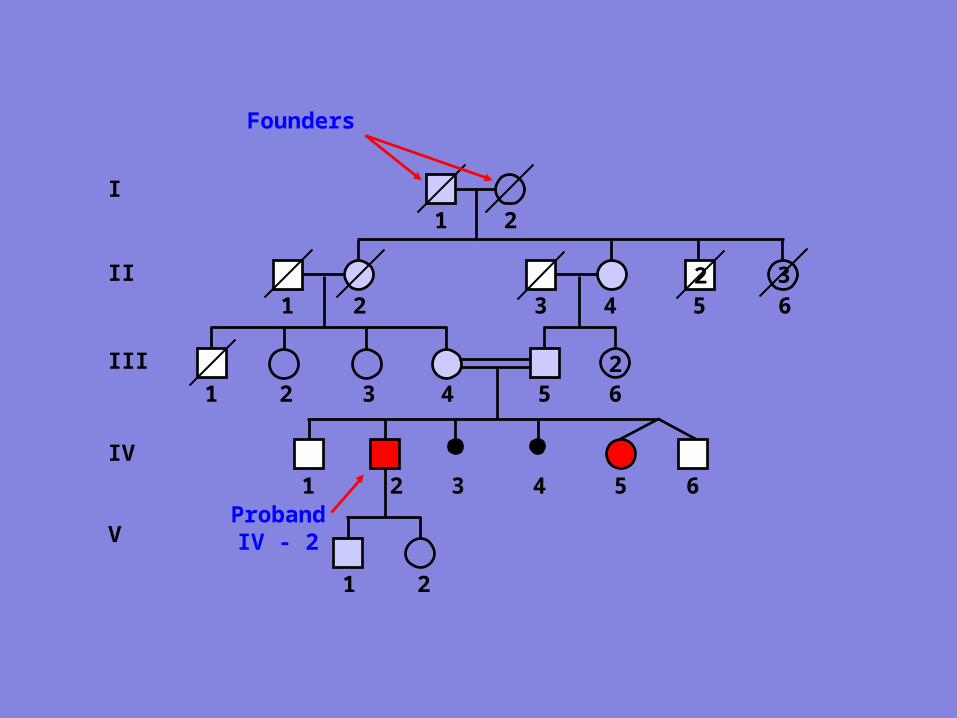
I
II
III
IV
2
1 2
1 2 3 4 5 6
1 2 3 4 5 6
1 2 3 4 5 6
Founders
ProbandIV - 2V
1 2
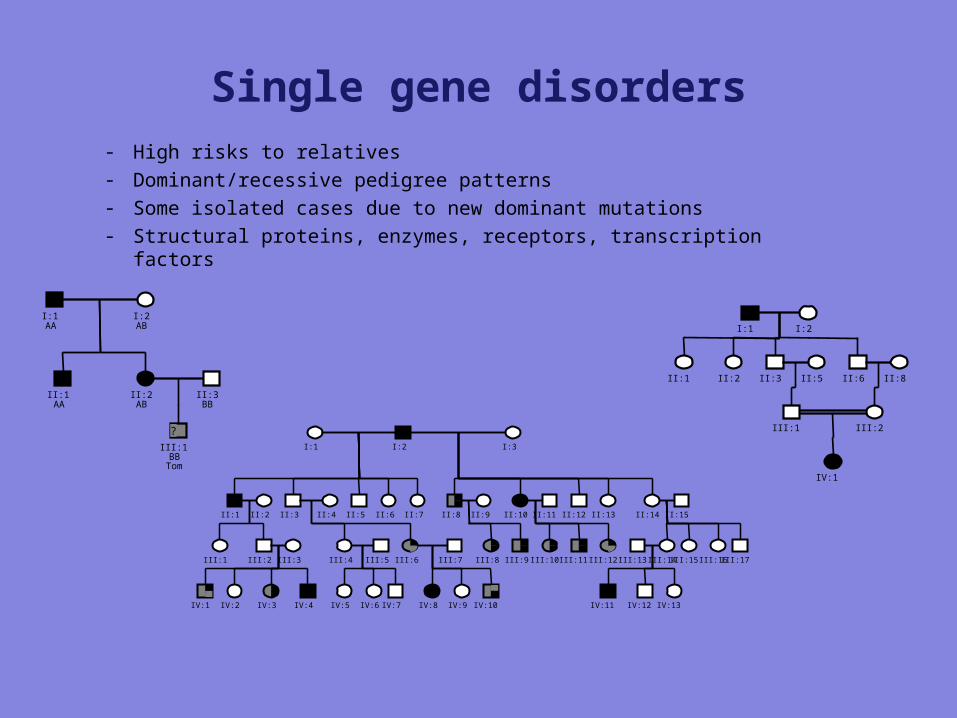
Single gene disorders- High risks to relatives- Dominant/recessive pedigree patterns- Some isolated cases due to new dominant mutations- Structural proteins, enzymes, receptors, transcription factors
I:1AA
I:2AB
II:1AA
II:2AB
II:3BB
?
III:1BB
Tom
I:2I:1 I:3
II:1 II:2 II:3 II:4 II:5 II:6 II:7 II:8 II:9 II:10 II:11 II:12 II:13 II:14 II:15
III:1 III:2 III:3
IV:1 IV:2 IV:3 IV:4
III:4 III:5
IV:5 IV:6 IV:7
III:6 III:7
IV:8 IV:9 IV:10
III:8 III:9 III:10 III:11 III:12 III:14III:13 III:15 III:16 III:17
IV:11 IV:12 IV:13
I:1 I:2
II:1 II:2 II:3 II:5 II:6 II:8
III:1 III:2
IV:1
1. Disorders with multifactorial inheritance (polygenic)
• influence of multiple genes + environmental factors• relatively frequent• Diabetes mellitus (see Endocrine pathology)• Hypertension (see Circulation)• Gout (discussed here + see Crystals)• Schizophrenia (Psychiatry)• Congenital heart disease - certain forms (see Heart)• Some types of cancer (ovarian, breast, colon) (see Neoplasms)• often familial occurrence - probability of disease is in 1st
degree relatives about 5-10%; 2nd degree relatives - 0,5-1%
2. Monogenic (mendelian) disorders
• mutation of 1 gene, mendelian type of inheritance
• today about 5000 diseases
• Autosomal dominant
• Autosomal recessive
• X-linked

Autosomal dominant disorders
• both homozygotes and heterozygotes are affected
• usually heterozygotes (inherited from one parent)
• both males and females are affected• transmission from one generation to the
other• 50% of children are affected
2. Autosomal recessive
• majority of mendelian disorders• only homozygotes are affected, heterozygotes
(parents) are only carriers• 25% of descendants are affected• if the mutant gene occurs with low frequency -
high probability in consanguineous marriages• onset of symptoms often in childhood• frequently enzymatic defect• testing of parents and amnial cells
X-linked diseases
• transmitted by heterozygous mother to sons• daughters - 50% carriers, 50% healthy• sons - 50% diseased, 50% healthy• Children of diseased father - sons are healthy, all
daughters are carriers• Hemophilia A (defect of Factor VIII)• Hemophilia B (defect of Factor IX)• Muscle dystrophy (Duchen disease)
3. Chromosomal aberrations (cytogenetic disorders)
• alternations in the number or structure of chromosomes• autosomes or sex chromosomes• studied by cytogenetics• cell cycle arrested in metaphase (colchicin) - staining by
Giemsa method (G-bands) - photographing - karyotype• 2 sets of 23 chromosomes• 22 pairs of autosomes, 2 sex chromosomes (XX or XY)• cytogenetic disorders are relatively frequent! (1:160
newborns; 50% of spontaneous abortions)
Numerical abnormalities
• euploidy - normal 46 (2n)• polyploidy (3n or 4n) - spontaneous abortion• aneuploidy• trisomy (2n+1) - 47 - compatible with life• monosomy (2n-1) - autosomal - incompatible
with life• - sex chromosomal -
compatible with life
Structural abnormalities
• breakage followed by loss or rearrangement• deletion, translocationGenerally: • loss of chromosomal material is more dangerous than gain• abnormalities of sex chromosomes are better tolerated
than autosomal• abnormalities of sex chromosomes sometimes
symptomatic in adult age (e.g. infertility)• usually origin de novo (both parents and siblings are
normal)
Prenatal diagnostics
• amniocentesis - analysis of amniotic fluid• cytogenetic analysis (karyotype - e.g. Down)• biochemical activity of various enzymes (e.g. Tay-
Sachs)• analysis of various specific genes (CF gene - PCR)• sex of the fetus (X-linked disorders - hemophilia)
Recommended reading list - textbooks
• Human Molecular Genetics 3– Strachan & Read
• Garland Publishing, ISBN 0-8153-4182-2
• Principles of Medical Genetics– Gelehrter, Collins & Ginsburg
• Lippincott, Williams & Wilkins, ISBN 0683034456
• Genetics in Medicine– Nussbaum, McInnes & Willard
• Elsevier, ISBN 0721602444
Journals
• Nature Genetics– http://www.nature.com/ng/index.html
• Nature Reviews Genetics– http://www.nature.com/nrg/index.html
• Trends in Genetics– http://www.trends.com/tig/default.htm