medicaid beneficiary fair hearings training 2017 … hrgs...medicaid beneficiary fair hearings...
TRANSCRIPT

1
Medicaid Beneficiary Fair Hearings Training
& 2017 Managed Care Regulations Changes
Home & Community Based
Waiver Conference
November 15, 2016

2
OUTLINE
I. Purpose of Training II. Purpose of a Hearing III. Right to Hearing for Medicaid Beneficiaries IV. An Action – what is it? V. Notice of an action to the Beneficiary VI. Request for Hearing VII. Preparation for Hearing VIII. The Hearing IX. No Ex Parte (one-sided) Communications X. How to Contact the Michigan Administrative
Hearing System (MAHS) Benefits Division XI. New 2017 Managed Care Regulations XII. Questions
3
I. PURPOSE OF TRAINING What does the Michigan
Administrative Hearing System (MAHS) Benefits (DCH) Division do? What are the rights of Medicaid
beneficiaries; Due Process? An Administrative Hearing – What is
it?
Do Administrative Hearings apply to Afford. Care Act, Healthy Michigan Plan &
Integrated Care Demonstration (ICDE)?
4
II. PURPOSE OF A HEARING
Constitutional right of due process
Federal Social Security Act and Medicaid
Federal Regulations
Medicaid – an entitlement
US Supreme Court – Goldberg v Kelly
Due Process standards

5
III. RIGHT TO A HEARING FOR MEDICAID Agency must grant an opportunity for a
hearing to:
Any applicant who requests it because his/her request is denied or not acted upon with reasonable promptness/acted upon promptly.
42 CFR 431.200(a), 220(a)(1)
and 42 CFR 438.400(a)(1)
Any beneficiary who requests it because he or she believes the agency has taken an action erroneously.
42 CFR 431.220(a)(2)
6
IV. An Action – what is it? A. MA Applicants and Beneficiaries
Action: Reduction, suspension, termination or denial of Medicaid eligibility or
covered service. 42 CFR 431.201
B. (Managed Care Organization [MCO]/Prepaid Inpatient Health Plan [PIHP])
Action:
• Denial or limited authorization of a requested service, including the type or level of service.
• Reduction, suspension, or termination of a previously authorized service.
• Denial, in whole or in part, of payment for a service.
• Failure to make a standard authorization decision and provide notice about the decision within 14 calendar days from the date of receipt of a standard request for service.
• Failure to make an expedited authorization decision within three (3) working days from the date of receipt of a request for expedited service authorization.
• Failure to provide services with 14 calendar days as authorized by the PIHP.
• Failure of the PIHP to act within 45 calendar days from the date of a request for a standard appeal.
• Failure of the PIHP to act within three (3) working days from the date of a request for an expedited appeal.
• Failure of the PIHP to provide disposition and notice of a local grievance/complaint within 60 calendar days of the date of the request.
• Right for resident of rural area with only one MCO to obtain services out of network
NOTE: The term “action” is also referred to as an “adverse action”. 42 CFR 438.400(b)
7
V. NOTICE TO THE BENEFICIARY
OF AN ACTION – PIHP/MCO
Two types of notice: I. Adequate Action (denial of a requested service) II. Advance Action (reduction, termination or suspension of an authorized service)
I. ADEQUATE NOTICE MUST: 1. Be mailed not later than the date of action; and 2. State what action the Agency intends to take; and 3. State the reason for the intended action; and 4. State the specific regulation(s) that support the proposed action; and 5. Give an explanation of the individual’s right to request an evidentiary hearing and how to
access it; and 6. Give an explanation of the individual’s right to request a local level appeal and how to
access it; and
7. State she may represent herself or use legal counsel, a relative, friend or other spokesperson.
42 CFR 438.404
8
NOTICE TO THE BENEFICIARY OF AN ACTION – PIHP/MCO (Cont.)
II. ADVANCE NOTICE MUST:
1. Be mailed at least 12 days before the date of action; and
2. State what action the Agency intends to take; and
3. State the reason for the intended action; and
4. State the specific regulation(s) that support the proposed action; and
5. Give an explanation of the individual’s right to request an evidentiary hearing and how to access it; and
6. Give an explanation of the individual’s right to request a local level appeal and how to access it (if applicable); and
7. Give an explanation of the circumstances under which services are continued if a hearing
or local level appeal is requested; that the individual must specifically request services be continued and that the agency may institute recovery procedures if appeal not successful.
8. State that she may represent herself or use legal counsel, a relative, friend or other spokesperson. 42 CFR 438.404

9
NOTICE TO THE BENEFICIARY OF AN ACTION – MA Beneficiary
I. ADEQUATE NOTICE MUST: 1. Be mailed not later than the date of action; and 2. State what action the Agency intends to take; and 3. State the reason for the intended action; and 4. State the specific regulation(s) that support the proposed action; and 5. Give an explanation of the individual’s right to request an evidentiary
hearing and how to access it; and 6. State that she may represent herself or use legal counsel, a relative,
friend or other spokesperson.
42 CFR 431.210

10
NOTICE TO THE BENEFICIARY OF AN ACTION – MA Beneficiary (Continued)
II. ADVANCE NOTICE MUST:
1. Be mailed at least 12 days before the date of action; and
2. State what action the Agency intends to take; and
3. State the reason for the intended action; and
4. State the specific regulation(s) that support the proposed action; and
5. Give an explanation of the individual’s right to request an evidentiary hearing and how to access it; and
6. Give an explanation of the circumstances under which services are continued if a hearing is requested and that the agency may institute recovery procedures; and
7. State that she may represent herself or use legal counsel, a relative, friend or other spokesperson.
11
ADEQUATE NOTICE OF ACTION – PIHP/MCO
ADEQUATE ACTION NOTICE Date Name Address City, State, Zip RE: Beneficiary’s Name: Beneficiary’s Medicaid ID Number: Dear : Following a review of the mental health services for which you have applied, it has been determined that the following service(s) shall not be authorized. Service(s) Effective Date _____________ _____________ The reason for this action is <reason> . The legal basis for this decision is <Specific regulation, i.e., 42 CFR 440.230(d).> If you do not agree with this action, you may request a Michigan Administrative Hearings System (MAHS) fair hearing within 90 calendar days of the date of this notice. Hearing requests must be made in writing and signed by you or an authorized person. To request a fair hearing, complete the “Request for Hearing” form and mail to:
MICHIGAN ADMINISTRATIVE HEARING SYSTEM BENEFIT SERVICES DIVSION/DCH
PO BOX 30763 LANSING, MI 48909
12
ADEQUATE ACTION NOTICE – PIHP/MCO
Page 2
You have a right to an expedited hearing if waiting for the standard time for a hearing would seriously jeopardize your life or health or would jeopardize your ability to attain, maintain, or regain maximum function. To request an expedited hearing, you must call, toll-free, 877-833-0870.
If you do not agree with this action, you may also request a local appeal, either orally or in writing, with your Prepaid Inpatient Health Plan (PIHP) within 45 calendar days of the date of this notice by contacting:
<Name of PIHP office/individual responsible for local appeal process>
<Address> <City, State ZIP>
<Phone Number – Voice> <Phone Number – FAX>
You have a right to an expedited local appeal if waiting for the standard time for a local appeal would seriously jeopardize your life or health or would jeopardize your ability to attain, maintain, or regain maximum function. To request an expedited local appeal, you must call your PIHP.
You may request both a fair hearing and a local appeal. The fair hearing and local appeal processes may occur at the same time. You may contact the Michigan Administrative Hearing System, toll free, at 877-833-0870 or the PIHP if you have further questions.
Enclosures: Hearing Request Form
13
ADVANCE ACTION NOTICE – PIHP/MCO Page 2
You have a right to an expedited hearing if waiting for the standard time for a hearing would seriously jeopardize
your life or health or would jeopardize your ability to attain, maintain, or regain maximum function. To request an
expedited hearing, you must call, toll-free, 877-833-0870. You will continue to receive the affected services until the hearing decision is rendered if your request for a fair
hearing is received prior to the effective date of action and you request that the services be continued. If you continue to receive benefits because you requested a fair hearing you may be required to repay the benefits.
This may occur if: - The proposed termination or denial of benefits is upheld in the hearing decision. - You withdraw your hearing request. - You or the person you asked to represent you does not attend the hearing. If you do not agree with this action, you may also request a local appeal, either orally or in writing, with your
Prepaid Inpatient Health Plan (PIHP) within 45 calendar days of the date of this notice by contacting:
<Name of PIHP office/individual responsible for local appeal process> <Address>
<City, State ZIP> <Phone Number – Voice> <Phone Number – FAX>
You have a right to an expedited local appeal if waiting for the standard time for a local appeal would seriously
jeopardize your life or health or would jeopardize your ability to attain, maintain, or regain maximum function. To
request an expedited local appeal, you must call your PIHP. You may request both a fair hearing and a local appeal. The fair hearing and local appeal processes may
occur at the same time. You may contact the Michigan Administrative Hearing System toll free, at 877-833-
0870 or the PIHP if you have further questions. Enclosures: Hearing Request Form
14
ADEQUATE NOTICE OF ACTION - MA Beneficiary
ADEQUATE ACTION NOTICE Date Name Address City, State, Zip RE: Beneficiary’s Name: Beneficiary’s Medicaid ID Number: Dear : Following a review of the [type of service] services for which you have applied, it has been determined that the following service(s) shall not be authorized. Service(s) Effective Date _____________
_____________ The reason for this action is <reason> . The legal basis for this decision is <specific regulation>. If you do not agree with this action, you may request a Medicaid fair hearing within 90 calendar days of the date of this notice. Hearing requests must be made in writing and signed by you or an authorized person. To request a fair hearing, complete the “Request for Hearing” form, and return it in the enclosed pre- addressed envelope, or mail to:
MICHIGAN ADMINISTRATIVE HEARING SYSTEM BENEFIT SERVICES DIVISION/DCH
PO BOX 30763 LANSING, MI 48909
15
ADEQUATE ACTION NOTICE – MA Beneficiary Page 2 You have a right to an expedited hearing if waiting for the standard time for a hearing would seriously jeopardize your life or health or would jeopardize your ability to attain, maintain, or regain maximum function. To request an expedited hearing, you must call, toll-free, 800-648-3397. You will continue to receive the affected services until the hearing decision is rendered if your request for a fair hearing is received within 10 days of the date of the notice or prior to the effective date of action. You may contact the Michigan Administrative Hearing System toll free, at 800-648-3397 or the PIHP if you have further questions. Enclosures: Hearing Request Form
16
ADVANCE NOTICE OF ACTION - MA Beneficiary
ADVANCE ACTION NOTICE
Date Name Address City, State, Zip RE: Beneficiary’s Name: Beneficiary’s Medicaid ID Number: Dear ____________: Following a review of the [type of service] services and supports that you are currently receiving, it has been
determined that the following service(s) shall be <reduced, terminated or suspended> effective <date>.
Service(s) Effective Date _____________________________ _______________ _____________________________ _______________ The reason for this action is <reason>. The legal basis for this decision is <specific regulation>. If you do not agree with this action, you may request a Medicaid fair hearing within 90 calendar days of the
date of this notice. Hearing requests must be made in writing and signed by you
or an authorized person. To request a fair hearing, complete the enclosed "Request for Hearing" form, and return it in the enclosed pre-
addressed envelope, or mail to:
MICHIGAN ADMINISTRATIVE HEARING SYSTEM
BENEFIT SERVICES DIVISION P.O. BOX 30763
LANSING, MICHIGAN 48909

17
ADVANCE ACTION NOTICE – MA Beneficiary Page 2
You have a right to an expedited hearing if waiting for the standard time for a hearing
would seriously jeopardize your life or health or would jeopardize your ability to
attain, maintain, or regain maximum function. To request an expedited hearing, you
must call, toll-free, 800-648-3397. You will continue to receive the affected services until the hearing decision is
rendered if your request for a fair hearing is received within 10 days of the date of
the notice or prior to the effective date of action. If you continue to receive benefits because you requested a fair hearing you may be
required to repay the benefits. This may occur if: -The proposed termination or denial of benefits is upheld in the hearing decision. -You withdraw your hearing request. -You or the person you asked to represent you does not attend the hearing. You may contact the Michigan Administrative Hearing System, toll free, at
800-648-3397 or the PIHP if you have further questions. Enclosures: Hearing Request Form

18
VI. REQUEST FOR HEARING
The Medicaid agency or provider may not limit or interfere with applicant’s or recipient’s freedom to make a request for hearing.
Request must be in writing.
Request for hearing must not exceed 90 days from date notice of action is mailed.

19
REQUEST for HEARING for MEDICAID ENROLLEES or WAIVER APPLICANTS
Instructions
To appeal an action related to cash assistance, food assistance, or other assistance programs, you must use the Request for Hearing form (DHS-18) available online at www.michigan.gov/mdhhs >> Doing Business with MDHHS >> Forms and Applications >> Other. Medicaid enrollees or waiver applicants may use this form to request a hearing. You may also submit your signed hearing request in writing on any paper. This form is also available on-line at www.michigan.gov/mdhhs >> Assistance Programs >> Medicaid >> Medicaid Fair Hearings.
A hearing is an impartial review of a decision made by the Michigan Department of Health and Human Services or one of its contract agencies that a client believes is wrong.
GENERAL INSTRUCTIONS:
Read ALL instructions before completing the attached form.
Complete Section 1 using the name of the client (even if the client has a guardian or is a minor).
Complete Section 2 only if you want someone to represent you at the hearing.
Do NOT complete Section 4.
Attach a copy of the notice or letter from the Agency telling you about the change you want to appeal.
Please make a copy for your records.
If you have any questions, please call toll free: 1 (877) 833 - 0870.
After you complete this form, mail or fax to:
MICHIGAN ADMINISTRATIVE HEARING SYSTEM
FOR THE DEPARTMENT OF HEALTH AND HUMAN SERVICES PO BOX 30763
LANSING MI 48909 Fax (517) 373-4147
You may choose to have another person represent you at a hearing.
This person can be anyone you choose but he/she must be at least 18 years of age.
You MUST give this person written permission to represent you.
You may give written permission by checking YES in SECTION 2 and having the person who is representing you complete SECTION 3. You MUST still complete and sign SECTION 1.
Your guardian or conservator may represent you. A copy of the court order naming the guardian must be included with this request.
The Michigan Department of Health and Human Services (MDHHS) does not discriminate against any individual or group because of race, religion, age, national origin, color, height, weight, marital status, genetic information, sex, sexual orientation, gender identity or expression, political beliefs or disability.
If you need help with reading, writing, or hearing, you are invited to make your needs known to the Michigan Department of Health and Human Services.
If you do not understand this, call the Michigan Department of Community Health at (877) 833-0870.
Si Ud. no entiende esto, llame a la oficina del Departamento de Salud Comunitaria.
1 (877) 833 - 0870
Completion: Is Voluntary
DCH-0092 (MAHS) INSTRUCTION SHEET (Rev. 10/15) See the Request Form Underneath
20
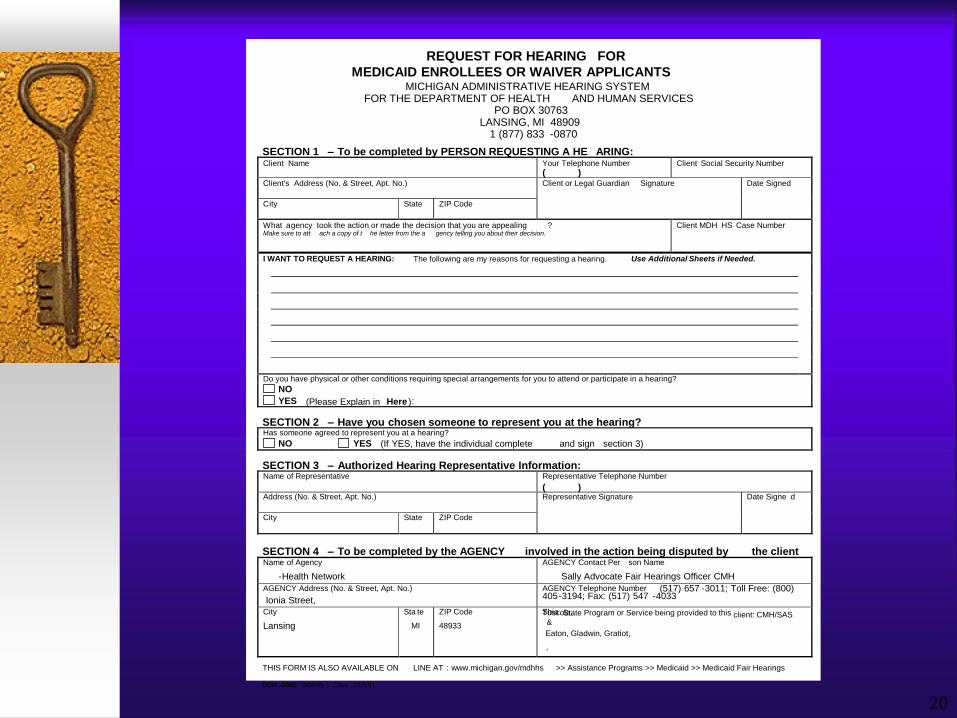
REQUEST FOR HEARING FOR MEDICAID ENROLLEES OR WAIVER APPLICANTS
MICHIGAN ADMINISTRATIVE HEARING SYSTEM FOR THE DEPARTMENT OF HEALTH AND HUMAN SERVICES
PO BOX 30763 LANSING, MI 48909
1 (877) 833 - 0870
SECTION 1 – To be completed by PERSON REQUESTING A HE ARING: Client Name
Your Telephone Number
( ) Client Social Security Number
Client's Address (No. & Street, Apt. No.)
Client or Legal Guardian Signature
Date Signed
C ity
State
ZIP Code
What a gency took the action or made the decision that you are appealing ? Make sure to att ach a copy of t he letter from the a gency telling you about their decision.
Client MDH HS Case Number
I WANT TO REQUEST A HEARING: The following are my reasons for requesting a hearing. Use Additional Sheets if Needed.
Do you have physical or other conditions requiring special arrangements for you to attend or participate in a hearing?
NO
YES (Please Explain in Here ) :
SECTION 2 – Have you chosen someone to represent you at the hearing? Has someone agreed to represent you at a hearing?
NO YES (If YES, have the individual complete and sign section 3)
SECTION 3 – Authorized Hearing Representative Information: Name of Representative
Representative Telephone Number
( ) Address (No. & Street, Apt. No.)
Representative Signature
Date Signe d
City
State
ZIP Code
SECTION 4 – To be completed by the AGENCY involved in the action being disputed by the client Name of Agency
- Health Network
AGENCY Contact Per son Name
Sally Advocate Fair Hearings Officer CMH
AGENCY Address (No. & Street, Apt. No.)
Ionia Street,
AGENCY Telephone Number (517) 657 - 3011; Toll Free: (800) 405 - 3194; Fax: (517) 547 - 4033
City
Lansing
Sta te
MI
ZIP Code
48933
State Program or Service being provided to this client: CMH/SAS
Eaton, Gladwin, Gratiot,
,
Shia
& Tuscola.
THIS FORM IS ALSO AVAILABLE ON LINE AT : www.michigan.gov/mdhhs >> Assistance Programs >> Medicaid >> Medicaid Fair Hearings
DCH - 0092 ( MAHS ) ( Rev 1 0 / 1 5 )
21
VII. PREPARATION FOR HEARING • READ THE APPEAL
• CONTACT APPROPRIATE WITNESSES
• PREPARE A HEARING SUMMARY:
Define the issue/action taken
Determine whether proper notice was sent
Research applicable policy
Write a short chronological narrative detailing what occurred
Include any documents considered as evidence:
The Appeal
The Notice
Medical documentation, if relevant to the action taken
Other documents that may have been considered
Applicable Policy
Number the pages – of hearing summary and all attachments
Send a copy of the hearing summary and all documents for the judge at the hearing to the Petitioner and Authorized Hearing Representative at least seven (7) days prior to the scheduled hearing date.
22
VIII. THE HEARING
At the hearing:
The Administrative Law Judge (ALJ) will introduce the case and the parties.
The ALJ will swear in witnesses.
The hearing typically begins with the Department’s representative presenting its case.
The Department will introduce its hearing summary into the record.
The Department will question its witnesses, if any.
The Appellant will have an opportunity to question the Department’s witnesses and object to any documents in the hearing summary.
The Appellant will present his/her side of the story.
The Department’s Representative will have an opportunity to question the Appellant and his/her witnesses.
Both the Appellant and the Department’s Representative may provide a closing statement.
Both the Appellant and the Department’s Representative may be asked to provide additional documentation to the ALJ.

23
VIII. AT THE HEARING - Continued
Role of the Administrative Law Judge
Conducts complex hearings in accordance with rules of evidence, DCH policy, and state and federal regulations and statutes. Authority for hearings are found in the Mental Health Code, Public Health Code, Social Welfare Act, the Administrative Code, the Administrative Procedures Act, Social Security Act and federal regulations. Reviews case files prior to hearing to identify issues, relevant legal authority, and procedural questions. Administers oaths and affirmations. Maintains order and makes a complete formal record of the proceedings. Regulates participation of parties. Rules on motions, objections, the relevance of testimony and exhibits, offers of proof and other procedural matters, and receives relevant evidence. Questions witnesses if necessary or desirable. Hears arguments of the parties and/or counsel upon completion of presentation of evidence. Receives expert testimony of physicians and other professionals in specialized fields. Reviews cases, issues final decisions and orders, or issues recommended decisions for the Department Director’s review. Reviews files, records, and briefs. Performs research on legal and policy questions. Makes findings of fact and determinations of law. Issues final decisions and orders, or recommended decisions.

24
IX. EXPARTE COMMUNICATIONS
Are Prohibited (Including one-party phone calls & requests for adjournments.) Any document sent to MAHS must be served on opposing party.
25
X. HOW TO CONTACT MAHS Benefit Services Division
Address: PO Box 30763 Lansing, MI 48909 Telephone: (517) 373-0722 (877) 833-0870 for Medicaid Appellant use Facsimile: (517) 373-4147 Email: [email protected] MAHS Website: www.michigan.gov/LARA>>MAHS To locate Hearings Pamphlet and Forms on DHHS Website www.michigan.gov/mdhhs
•Assistance Programs >>
•Medicaid >>
•Medicaid Fair Hearings •Scroll to bottom of page •http://michigan.gov/mdhhs/0,5885,7-339-71547_4860---,00.html

CHANGES TO THE MANAGED CARE REGULATIONS
42 CFR 438
Effective July 1, 2017 for
Managed Care Organizations (MCO’s)
Prepaid Inpatient Health Plans (PIHPs)
Prepaid Ambulatory Health Plans (PAHPs)
NEW TERMINOLOGY § 438.400
Adverse benefit determination means, for an MCO, PIHP, or PAHP:
The denial or limited authorization of a requested service.
The reduction, suspension, or termination of a previously authorized service.
The denial, in whole or in part, of payment for a service.
The failure to provide services in a timely manner, as defined by the State.
The failure of an MCO, PIHP, or PAHP to act within the timeframes provided.
For residents in rural areas with only one MCO, the denial of his or her right to obtain services outside of the network.
The denial of an enrollee's request to dispute a financial liability, including cost sharing, copayments, premiums, deductibles, coinsurance, and other enrollee financial liabilities.
42 CFR 438.400(b)-(1) through (7)

NEW TERMINOLOGY CONTINUED § 438.400
Appeal means a review by an MCO, PIHP, or PAHP of an adverse benefit determination.
Grievance means an expression of dissatisfaction about any matter other than an adverse benefit determination. Grievances may include, but are not limited to, the quality of care and aspects of interpersonal relationships. Grievance also includes an enrollee’s right to dispute an extension of time proposed by the MCO, PIHP or PAHP to make an authorization decision.
State fair hearing means a due process evidentiary hearing after the enrollee’s appeal of the MCO adverse benefit determination has been exhausted.
42 CFR 438.400(b)
MCO NOTICE TIMELINE REDUCTIONS
An MCO, PIHP, PAHP must give timely and adequate notice of adverse benefit determination (ABD) in writing.
The notice must give right to request an internal MCO within 60 days of ABD, and if ABD is upheld, a right to request State Fair Hearing within 120 days of notice that ABD was upheld.
Timeline for MCO to make ABD Current CFR = 45 days – 2017 CFR reduced to 30 days
Expedited ABD Current CFR = 3 Working days– 2017 CFR reduced to 72 hours
42 CFR 438.400(b)

APPEALABLE ACTIONS NOW INCLUDE QUESTIONS OF FINANCIAL LIABILITY
Hearable issues now include disputes regarding financial liability including questions concerning:
Cost sharing
Copayments
Premiums
Deductibles
Coinsurance
Other beneficiary financial liabilities 42 CFR 438.400(b)(7)

INTERNAL APPEALS MUST BE EXHAUSTED
Beneficiaries will have at least one level of internal appeal with Managed Care Organizations (MCO’s), which must be exhausted prior to requesting a Medicaid Fair Hearing.
Exception: MCO fails to follow notice and time
requirements; = exhausted and launches right to SFH.
42 CFR 438.408(c)(3); 402

REQUEST FOR STATE FAIR HEARING (SFH) TIME INCREASED TO 120 DAYS
By July 1, 2017, Beneficiaries will have 120 days from the date of MCO notice of resolution to file Request for State Fair Hearing.
Currently the time period is 90 days.
State fair hearing: The enrollee must request a State fair hearing no later than 120 calendar days from the date of the MCO’s, PIHP’s, or PAHP’s notice of resolution. 438.408(f)(2)

CHANGES NEEDED PRIOR TO 7/1/2017
MCO notice of resolution language regarding filing request for State Fair Hearing needs to be changed from the current 90 days to 120 days.
MAHS must change its intake process to accept a MCO beneficiary request for State Fair Hearing up to 120 days; currently denies after 90 days.

WHAT THE CHANGES MEAN TO YOU
CMS continues to provide guidance to states on implementation of the new managed care regulations.
The DHHS and MAHS are working together to plan for the managed care regulation changes. When available, further details will be shared; these slides are only intended as an overview.

35
XI. QUESTIONS