medcomiv · with the dsi report edb over (sektor ... draw attention to the need for cross-sector...
TRANSCRIPT

MedCom IV Status, plans and projects
MedCom – the Danish Healthcare Data Network / Dec. 2003 / MC-S177
● Internet strategy ● Local authorities and healthcare communication● Hospitals and healthcare communication ● International activities
Clinical service
c. 40%
Other hospitals
c. 10%
Other service
c. 13%
Administration
c. 4%
Primary sector
c. 13%Medicalpractice
Nursinghomes
Homecare
Specia-lists
Otherclinicaltreatmentunits
EPRc. 23%
Clinicaltreatmentunit
HOSPITAL
MedCom IV Status, plans and projects
KPLL
LocalauthorityCounty
Healthcareportal
HealthcareDIX
Dan Net
KMDnetwork
Doctors’systems
Pharmacynetwork
Internet

MedCom IV – status, plans and projects2
ContentsAims of MedCom 2
Introduction 3Healthcare on the move 3
History 4
The MedCom steering group 6Commentary: The Minister of the Interior and
Health, Lars Løkke Rasmussen 7Perspective: MedCom certifies communication 8
The Internet strategy 9
The infrastructure project 9Commentary: The Chairman of the Association of
County Councils, Kristian Ebbensgaard 12Perspective: The Internet strategy and the
Healthcare Portal 12Web lookup of laboratory data 12Web requesting of tests for clinical biochemistry
and clinical immunology 14Web lookup of X-rays images and descriptions 16Teledermatology network 17EDI via the Internet 19
Aims ofMedComMedCom aims to contribute to the development, testing,dissemination and qualityassurance of electronic com-munication and information in the healthcare sector with a view to supportingcoherent treatment, nursingand care.
The local authorities and healthcare communication 20The Hospital-Local Authority XML project 20The Hospital-Local Authority project and
Common Language 22Commentary: The Minister of Social Affairs,
Henriette Kjær 22The LÆ form project 23Commentary: The Chairman of the National
Association of Local Authorities, Ejgil W. Rasmussen 24Perspective: The IT Lighthouse’s local authority-
medical practice communication 24
The hospitals and healthcare communication 25From hospital to hospital 25The XML EPR project 27Perspective: XML EPR 27Commentary: Head of Department in the Ministry
of the Interior and Health, Vagn Nielsen, chairman of the MedCom steering group 32
Perspective: The XML EPR communication project and G-EPR 32
MedCom’s SUP project 33
International activities 36
International interaction 37International projects 1996-1999 37Commentary: Ilias Iakovidis, Ph.D.
Deputy Head of Unit-eHealth, European Commission, DG Information Society 38
International projects 2000-2002 38International projects 2002-2004 39Nordic co-operation 39Perspective: Nordic Health care Network group 40
Statistical material 41
Good EDI letters 41What can the counties do now? 42
Danish Centre for Health Telematics 43

around a million messages amonth. The figure is now twicethat level.
Alongside all this develop-ment, there has been intensivework on the consolidation andquality assurance of communica-tion. There has also been consid-erable positive experience of thesignificant work involved in car-rying out organisational changesunder the impact of the newinformational technology. Onlyif organisational changes aremade can the improved commu-nication really prove effective.
New perspectives
The dentists, physiotherapistsand occupational therapists arerelatively new users of the health-care data network. Promising trials are underway with tele-medicine, and the Internet hascome into the picture. The ex-pansion and development of theInternet has made it appropriateto look at the opportunities touse Internet technology to meetsome of the communicationneeds of the healthcare sector.
And this is where one of theprincipal focal areas of MedComIV has been. The Internet opensup completely new opportunitiesboth in relation to the patientand in dialogue with healthcareprofessionals. It is important togather experience with this com-munication through a largenumber of practical projects. Atthe same time, MedCom IV hasbeen concerned with the expan-sion and quality assurance ofEDI communication, as well asthe development and implemen-tation of communication to andfrom electronic patient records.
Introduction 3
cation across the regions. Theidea was to develop joint national communication stan-dards for the most importantforms of messages and to makethe regional healthcare data net-works building-blocks in anational healthcare data network.Coordination, development andexchange of experience becameimportant tasks for MedCom inthe efforts made to promote ITcommunication in the healthcaresector.
A particular dimension of thedevelopment work throughoutthe period has been interactionwith private business. At first themarket for the IT solution in thisarea was virtually non-existent. A market of this kind has beenbuilt up alongside the develop-ment of the healthcare data net-work under close and construc-tive co-operation between users,suppliers and MedCom.
From the doctor to the whole health-care sectorIn the first phase of develop-ment, the general practitionerwas the pivotal point in commu-nication, which primarily passedbetween medical practices, hospi-tals, laboratories and pharmacies.Then the local authorities alsojoined in and became an impor-tant partner in cooperation, inhome care and other areas.
Messages in the form of pre-scriptions, laboratory results, X-ray results, discharge letters etc.were exchanged in steadily in-creasing numbers between moreand more users. By the end ofthe nineties, the healthcare datanetwork was already forwarding
Healthcarecommunica-tion on themove
Communication is a key word ina healthcare sector, which reflectsspecialisation and division oflabour between a large numberof specialists and specialistgroups across sectors. Qualityand efficiency in patient treat-ment are entirely dependent onrapid, reliable and error-freeexchange of information betweenall parties concerned with thepatient.
It was therefore natural forthe healthcare sector at the endof the eighties to start examiningthe options for using data com-munication. It started with a fewenthusiasts, who could see thesense in transferring standardmessages electronically. The ideaquickly caught on, and the use ofelectronic communication devel-oped in both breadth and depth– more and more users joined in,and the potential applicationswere extended to include newtypes of messages.
One healthcare datanetwork, severalregional networksThe small, dispersed projectswere soon brought together inactual regional healthcare datanetworks, the project organisa-tion MedCom was founded backin 1994, both to control devel-opment and to ensure communi-
Introduction

Millions of messages252423222120191817161514131211109876543210
MedCom I: 1994-1996To counteract the tendency forthe counties each to “re-inventthe wheel”, Funen County in1992 submitted a proposal toorganise a joint nation-wide pro-ject bringing together nationalgovernment, the counties, privatecompanies and healthcare organisations under the name of:“MedCom – The DanishHealthcare Data Network”.
The purpose of MedCom wasto develop nation-wide standardsfor the most common communi-cation flows between medicalpractices, hospitals and pharma-cies: referrals and discharge let-ters, laboratory results, X-ray let-ters, prescriptions and hospitalbilling, totalling over 30 millionmessages a year.
The development projects ranfrom 1994 to 1996 as 25 pilotprojects spread across the wholecountry, which together involvedthe majority of the suppliers ofIT to hospitals and medical prac-tices. However, the disseminationof the standards went slowly. Adecision was therefore made tocarry out a second project –MedCom II.
MedCom IV – status, plans and projects4
It started in theeightiesThe history of the healthcaredata network goes back to theend of the 1980s, when interestin electronic communicationbetween the various parties inthe healthcare sector grew. Localprojects were launched on theinitiative of the Association ofCounty Councils, at the hospi-tals in Vejle and Silkeborg andelsewhere. The projects, togetherwith the DSI report EDB over(sektor) grænser (Computing Across(Sector) Boundaries) helped todraw attention to the need forcross-sector communication from1991 on.
Alongside these projects, a tri-
al involving communicationbetween 10 pharmacies and 11medical practices was held onAmager in 1989-90. The trialwas pioneering in EDI commu-nication in Denmark, and thesame technological platform hasbeen used for communicationright up to the present day.
The first regionalprojectsThree large regional EDI pro-jects started in 1992:
● FynCom in Funen County● The Odder project in Århus
County● KPLL in Copenhagen
All three projects were based onthe technology used in the“Amager trial”.
History
The spread and use of the healthcare data network has developed appreciably over the last ten years. Today, 2.3 million messages a monthare communicated.
92 93 94 95 96 97 98 99 00 01 02
Pilot projects inMedcom I
●●●●
●●●●●●
●●●●
●●●●
●●●
●●
●●
●●
●●
●
●●●

MedCom II: 1997-2000The primary purpose of Med-Com II was to ensure rapid andlarge-scale dissemination of thestandards developed under theMedCom I project. The local-authority healthcare sector wasbrought into the project togetherwith the area of dentistry andtelemedicine. Internet technolo-gy also started to be used.
Following the implementationof MedCom II, EDI communi-cation between hospitals, medi-cal practices and pharmaciesbecame everyday reality in allDanish counties, and 1.3 millionmessages a month wereexchanged. Altogether more than2000 medical practices, pharma-cies, hospitals and laboratorieswere connected to the healthcaredata network at the end of 1999,and between a third and a half ofall standardised communicationbetween the parties in thehealthcare sector was exchangedelectronically.
MedCom III: 2000-2001 As communication in MedComII came into use on a large scale,it became clear that fundamentalquality assurance of the EDIcommunication was necessary, as
History 5
the standards were used differ-ently by the various suppliers.
At the same time, a decisionwas taken to launch four smallerproject lines: the Hospital Area,Telemedicine/Internet, Local-Authority Communication andInternational Projects.
MedCom today
Electronic EDI communicationhas now overtaken daily, paper-based communication in the primary healthcare sector. By farthe majority of doctors, hospi-tals, laboratories and pharmaciesuse electronic communicationinstead of writing letters – andthis is the most common form ofcommunication in the majorareas of the primary healthcaresector.
Spread Number %
General practitioners 1939 88%Specialists 444 57%Pharmacies 331 100%Hospitals 64 100%Local authorities 24 26%
Gains Saving
Medical practice 50 min./dayTelephone follow-up to hospitals 66%Per message DKK 25
Total electronic communication:
2.3 million messages a month.70% of all communication in the primary healthcare sector.
MedCom II:
193 dissemination projects
12 local-authority projects
8 dentist projects
10 telemedicine projects
MedCom III reflected a consolida-tion of the healthcare data net-work throughout the country andfour project lines – Hospital, LocalAuthority, Telemedicine/Internetand International Projects – whicheach separately covered a group ofregions.
Consolidation
Hospitals
Local authority
Telemedicine/Internet
International projects

MedCom IV – status, plans and projects6
The columns show for each county how high a proportion of medical practices have computers and EDI. It can be seen that most GPs haveboth, but there is a small group who do not have either computers or EDI.A small group have computers, but do not use EDI communication.
MedCom IV: 2002-2005A substantial part of the work inMedCom III consisted in estab-lishing the basis for the subse-quent MedCom projects in twoimportant areas, the introductionof Internet-based communica-tion in the healthcare sector andre-use of MedCom’s standards inthe hospital area.
The “Doctors site number” curve shows the proportion of doctors who useEDI communication, while the “Local authorities” curve shows the pro-portion of local authorities connected to the healthcare data network. Theother curves show how large a proportion of discharge letters, laboratoryrequests, laboratory results, prescriptions, referrals and bills from generalpractice to the National Health Insurance Scheme proceed electronically.
Only in laboratory requesting and communication with the local-authority health visiting service is there still a need for further develop-ment and dissemination projects.
The MedCom steering group
● Vagn Nielsen, Head of
Department, Ministry of the
Interior and Health (Chairman)
● Leif Vestergaard Pedersen,
County Health Director, Århus
County (Deputy Chairman)
● Karin Meinicke Andersen,
Head of IT, Danish Pharma-
ceutical Association
● Lene Bilslev-Jensen, Head of
Section, Ministry of Finance,
The Digital Taskforce
● Steen Christophersen, Vice
President IT, H:S Informatik
● Leif Hagerup, Chief of
Section, Association of
County Councils
● Morten Hein, Head of Sec-
tion, Ministry of Social Affairs
● Henrik Bjerregaard Jensen,
Centre Manager, MedCom
● Ralf Klitgaard Jensen, Chief
of Section, National Associa-
tion of Local Authorities
● Anders Kristian Jørgensen,
Vice President, Dan Net A/S
● Arne Kverneland, Chief of
Section, Nat. Board of Health
● Peder Larsen, Deputy
Director, Funen County,
Healthcare Secretariat
● Jørn Jan Nielsen, Deputy
Chief of Section, Copenhagen
Local Authority, Healthcare
Directorate
MedCom statusPercentage of possible messages
Medical practices, 1 April 2003Percentage of all GPs
100
80
60
40
20
0
1998 1999 2000 2001 2002 2003
Doctors site no.Referral
Having EDIHaving computers
DischargeBilling
Lab res.Lab req.
PrescriptionsLocal auth.
100
90
80
70
60N.Jut. Vib. Årh. Ring. Ribe Vejle S.Jut. Fun. W.Z. St.str. Rosk. Fr.b. CHC Cop. Born. Total
0
0
0
0
0
0

Commentary
An importantdriving forceThe Minister of the Interior and
Health, Lars Løkke Rasmussen
“The Danish Government
actively supports the MedCom
co-operation, because it con-
tinues to constitute an important
driving force in the development
and expansion of electronic
communication across the health
service,” says Lars Løkke
Rasmussen, the Minister of the
Interior and Health.
“In a specialised health service, ensuring that staff have rapid and
secure access to all relevant clinical information on patients is a great
challenge. It is essential that healthcare staff are able to communicate
effectively across the boundaries of institutions, units and sectors.
The projects underway in MedCom IV focus in particular on com-
munication in the hospital sector and communication between local
authorities and hospitals, as well as GPs. In addition, the establish-
ment of the new Internet-based healthcare data network is opening
the door for new nationwide forms of communication, including
secure web-mail, videoconferencing and lookup, for example in X-ray
systems.
I anticipate that the communication projects will lead to increased
quality and coherence in patient progressions and provide the basis
for improved information and service to patients. I also anticipate
that the projects will act as catalysts for changes in old routines and
procedures in the health service, so that the resources can be used in
the best possible way.”
History 7
The MedCom IV project istherefore building on previousMedCom projects and consistsof four project lines:
1. The Internet Strategy, thepurpose of which is to intro-duce a nation-wide, Internet-based healthcare data networkand achieve large-scale use ofweb lookup, telemedicine andother Internet-based forms ofcommunication in the health-care sector.
2. The Local-Authority pro-jects, the purpose of which isto achieve large-scale use ofMedCom’s standards for com-munication between hospitalsand local-authority home carecovering 75% of all Danishlocal authorities.
3. The XML-EPR Communi-cation project, the purpose ofwhich is to achieve large-scalenation-wide use of all relevantMedCom messages for com-munication internally in hos-pitals and between hospitals.
4. MedCom’s SUP project, thepurpose of which is to achieveInternet access to PAS andEPR patient records bothwithin a county and acrosscounty boundaries.
All general medical practices are now joining A number of new IT opportuni-ties for general practitioners wereintroduced in the new agreementbetween the Association ofCounty Councils and the GPs,which came into effect on 1April 2003.
By 1 January 2004 all doctorswho have received a computerbilling fee in January 2003 mustbe able to communicate accord-ing to all the MedCom approvedstandards as they existed in
October 2002. They must followthe standards for prescriptions,billing, discharge summaries and
laboratory results in their com-munication, and – to the extentthat it is safe and practical to doso – referrals and laboratoryrequests as well.
All doctors who did notreceive a computer billing fee inJanuary 2003 must join by 1January 2005. In addition, pro-vision is made to offer patients e-mail consultation and giveresults to patients by e-mail, aswell as appointments and pre-scription renewal on the Inter-net.

Specialists join in EDI
The new agreement betweenthe Association of CountyCouncils and the Danish Asso-ciation of Medical Specialistsmakes it possible to offergrants enabling specialists inprivate practice to acquire ITand establish facilities for EDIcommunication and Internetaccess.
The grant is DKK 15,000for full-time practitioners,DKK 20,000 for part-timepractitioners, and a grant ofDKK 5,000 is paid for theestablishment of EDI commu-nication alone. To qualify for agrant, it is necessary to pur-chase a doctors’ system capableof handling all MedCom messages with the exception of MEDREQ. It is also a require-ment that the specialist’s practice is connected to the
healthcare data network andthat he or she uses all relevantmessages in the communica-tion that currently takes placein the county concerned.
The grant scheme started
on 1 January 2003, and in thefirst few months of the yearalone 86 new specialist prac-tices started using EDI, threetimes as many as in the wholeof 2002.
MedCom IV – status, plans and projects8
Perspective
MedCom certifies communication
Error-free communication of EDI messages in the healthcare data network is entirely dependent on both the
sender and the recipient using standards and syntax correctly. This makes demands on the computer systems at
both ends of the communication.
Previously the standards for the individual messages were tried out in pilot projects county by county and
supplier by supplier, and the systems were gradually adapted. It was a process that was time-consuming and
demanded considerable resources for all parties involved.
As part of the quality assurance of communication, users and technical staff have developed and introduced
“Good EDI Letters”, with MedCom as the intermediary. Thus the documentation of the standards has been
made very precise, and it is to a large extent possible to carry out the adaptation of sender and recipient
systems before the EDI message is put to use.
MedCom offers all systems houses and counties testing and certification of the sending and receiving of
each individual EDI type. If the systems house or county complies with the standard for the type of letter
concerned, MedCom issues a certificate of approval. The approval is published on the MedCom website.
Only systems that have undergone testing and approval may use the MedCom stamp of approval. Counties,
Copenhagen Hospital Corporation (CHC) and national laboratories have undertaken only to use and communi-
cate with systems and messages approved by MedCom.
DisseminationProportion of GPs and specialists in the healthcare data network
100
90
80
70
60
50
40
30
20
10
0
%
1997 1998 1999 2000 2001 2002 2003
Doctors site no. Full-time specialists Part-time specialists

Internet strategy 9
Within the health service, theInternet today is used for lookupin referral information and clini-cal guidelines. Use of the Inter-net is, however, limited by thelack of security in the openInternet. If the Internet is tosupplement or be an alternativeto the VANS-based healthcaredata network, it will need to bepossible to pass on the structuredEDI messages via Internet tech-nology, and for the messages tobe integrated into the computersystems that take part in thecommunication. Expanded useof Internet technology makesfundamental demands withregard to security, infrastructure,certification, user administrationand so on.
The Infrastruc-ture project
The aim of this project is toestablish a nation-wide secure IP-based network for communica-tion between the parties in thehealth service. The basic idea isto build up the network by link-ing together existing secure intra-nets in counties, local authoritiesand other organisations.
The first phase in establish-ment is to carry out a pilot pro-ject involving the construction ofa prototype, by which the rele-vant forms of communicationcan be tested in daily operationbetween the participants in theproject.
With a healthcare internet,the way is cleared for communi-cation options that were notavailable in the traditional
The Internet strategyThe Primary Group
The purpose of the Primary Group
is to monitor and carry out Med-
Com projects under the Internet
strategy and in the area of local
authorities. In addition, it fulfils
tasks in relation to problem-
solving and enhancement in con-
junction with the EDI communi-
cation already in existence. The
Group consists of project leaders
and other key individuals from
counties, CHC, local authorities
and other organisations in the
healthcare sector.
● Birte Elgaard Andersen,
Copenhagen County
● Karin Meinicke Andersen,
Danish Pharmaceutical
Association
● Karin Argir, Capio Diagnostik
● Lone Behnfeld,
South Jutland County
● Karin Bisgaard,
West Zealand County,
● Bente Christensen, Vejle
County
● Ib Thyge Christensen,
Frederiksborg County
● Anne Danborg,
Skovbo Local Authority
● Kjeld Erbs, Århus County
● Ronnie Eriksson, Association
of County Councils
● Anne-Marie Falch,
North Jutland County
● Lene Meyer Grosen,
Frederiksborg County
● Jens Grønlund, Viborg County
● Susanne Larsen Grøntoft, CHC
● Merete Halkjær,
Copenhagen Local Authority
● Finn Roth Hansen,
West Zealand County
● Jan Stokkebro Hansen,
Copenhagen County
● Niels Hornum, KPLL
● Rose-Marie Jensen,
Bornholm County
● Lisbeth Jørgensen,
Funen County
● Tine Korsholm,
Ringkjøbing County
● Tove Lehrmann, Funen County
● Søren Lorentzen,
Frederiksborg County
● Niels Munk-Jensen, FAPS
● Birgit Nielsen, Storstrøm
County
● Claus Nielsen, National Associa-
tion of Local Authorities
● Lisbeth Nielsen, Association
of County Councils
● Tove Charlotte Nielsen,
Vejle County
● Helle Stockfleth Olsen,
Statens Serum Institut
● Jens Parker, PLO
● Peter Pedersen, CHC
● Susanne Duedal Pedersen,
National Board of Health
● Jens Henning Rasmussen,
Roskilde County
● Henning Voss, Centre for
Healthcare Telematics
● Kim L. Østerbye, Ribe County
● Karin Demkjær, MedCom
● Lars Hulbæk, MedCom
● Gitte Henriksen, MedCom
● Henrik Bjerregaard Jensen,
MedCom
● Ib Johansen, MedCom
● Dorthe Skou Lassen, MedCom
● Jens Rahbek Nørgaard,
MedCom
● Claus Duedal Pedersen,
MedCom
● Iben Søgaard, MedCom
MedCom IV – status, plans and projects10
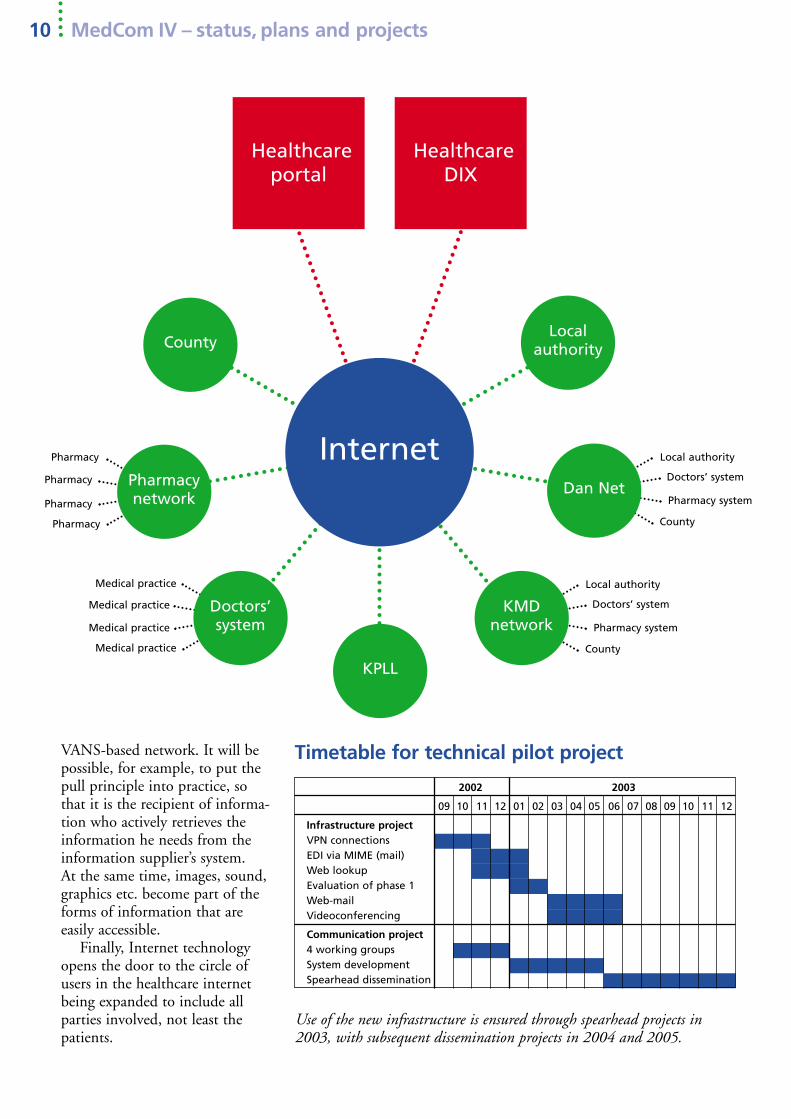
Timetable for technical pilot project
Use of the new infrastructure is ensured through spearhead projects in2003, with subsequent dissemination projects in 2004 and 2005.
VANS-based network. It will bepossible, for example, to put thepull principle into practice, sothat it is the recipient of informa-tion who actively retrieves theinformation he needs from theinformation supplier’s system. At the same time, images, sound,graphics etc. become part of theforms of information that are easily accessible.
Finally, Internet technologyopens the door to the circle ofusers in the healthcare internetbeing expanded to include allparties involved, not least thepatients.
KPLL
LocalauthorityCounty
Healthcareportal
HealthcareDIX
Pharmacy
Pharmacy
Pharmacy
Pharmacy
Medical practice
Medical practice
Medical practice
Medical practice
Pharmacy system
Doctors’ system
Local authority
County
Dan Net
Pharmacy system
Doctors’ system
Local authority
County
KMDnetwork
Doctors’system
Pharmacynetwork
Internet
2002 2003
09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12
Infrastructure projectVPN connectionsEDI via MIME (mail)Web lookupEvaluation of phase 1Web-mailVideoconferencing
Communication project4 working groupsSystem developmentSpearhead dissemination

Internet strategy 11
The purpose of the Infrastructure
Group is to ensure that MedCom’s
infrastructure projects are imple-
mented. The Group is temporary
and consists of project leaders and
network managers from organisa-
tions that have decided to estab-
lish VPN connections to the
healthcare data network under
the pilot project. The temporary
Infrastructure Group will be
replaced by a permanent group
when the project is ready for daily
operation.
● Karin Meinicke Andersen,
Danish Pharmaceutical
Association
● Orla Antonsen, Viborg
Hospital
● Allan Bech, Copenhagen
County
● Martin Bech, UNI-C
The Infrastructure Group
● Flemming Engstrøm,
Copenhagen Local Authority
● Jørgen Granborg, A-Data ApS
● Jens Grønlund, Viborg County
● Jan Stokkebro Hansen,
Copenhagen County
● Peter Illum Hansen, Funen
County
● Lars Hillerup, Vejle County
● Niels Hornum, KPLL
● Erik Jacobsen,
Datagruppen MultiMed ApS
● Henrik Thuren Jensen,
Profdoc A/S, Darwin
● Lisbeth Jørgensen, FynCom
● Børge Knudsen, Ribe County
● Ib Lucht, UNI-C
● Bo Nielsen, bo soft A/S
● Tove Charlotte Nielsen,
Vejle County
● Jens Parker, Lægehuset
● Morten Pedersen,
Datapharm A/S
● Peter Pedersen, CHC
● Morten Pedersen,
Association of County Councils
● Palle Runer, DataPharm A/S
● Ole Sprøgel, Dan Net
● Jan Staack, CHC
● Lise Wormstrup, KMD A/S
● Kim Østerbye, Ribe County
● Lars Hulbæk, MedCom
● Henrik Bjerregaard Jensen,
MedCom
● Jens Rahbek Nørgaard,
MedCom
● Claus Duedal Pedersen,
MedCom
● Karin Meinicke Andersen,
Danish Pharmaceutical
Association
● Hans Elmquist,
West Zealand County
● Susanne Enevoldsen,
Ringkjøbing County
● Flemming Engstrøm,
Copenhagen Local Authority
● Jørgen Granborg, A-Data ApS
● Jens Grønlund, Viborg County
● Helge Hansen,
South Jutland County
● Peter Illum Hansen, Funen
County
● Lone Hassingboe,
North Jutland County
● Søren Herget, West Zealand
County
VPN contacts
● Lars Hillerup, Vejle County
● Niels Hornum, KPLL
● Erik Jacobsen,
DataGruppen MultiMed ApS
● Niels Kinnerup,
West Zealand County
● Jan Kold-Larsen,
Copenhagen County
● Carsten Lind,
Frederiksborg County
● Claus Lohfeld, Århus County
● Kenneth Mogensen,
Storstrøm County
● Bo Nielsen, bo soft A/S
● John Møller Nielsen,
Eterra Danmark A/S
● Tove Charlotte Nielsen,
Vejle County
● Hans Birger Olsen,
Bornholm County
● Allan Pedersen, Viborg
County
● Jens Henning Rasmussen,
Roskilde County
● Palle Runer, DataPharm A/S
● Lennart Sorth, UNI-C
● Ole Sprøgel, Dan Net A/S
● Jan Staack, CHC
● Aksel Worm, Copenhagen
Local Authority
● Lise Wormstrup, KMD A/S
● Kim L. Østerbye, Ribe
County

Web lookup of laboratorydata
The idea in the “Lookup of Lab-oratory Data via the Web” pro-ject is to give healthcare profes-sionals Internet access to patientdata stored in another county,hospital or laboratory database.It will typically be relevant in situations where the healthcareprofessional has to treat a patientwithout having any knowledgeof the patient’s data, for examplein the case of emergency hospitaladmissions. Quick and easyaccess to relevant patient data inthose cases will boost both quality and efficiency in patienttreatment.
Provision for Web lookup willgenerally be useful where it wasnot “known” that patient datawould be needed. This appliesfor example in the treatment offree-choice patients and patients
MedCom IV – status, plans and projects12
Perspective
The Internet strategy and the Healthcare Portal
The MedCom standards, which are used at present in the healthcare
data network, can be directly re-used for data exchange via the Public
Healthcare Portal, which is being developed on the initiative of the
Association of County Councils.
Today, more than 40 types of letter based on MedCom standards
have been established. The MedCom standards are based on con-
sensus among healthcare professionals on content and application.
On this basis, documentation and test messages have been prepared,
sender systems have been approved in the testing of content and
syntax, and in a similar way recipient systems have been approved
through the testing of reception and presentation.
By linking together existing secure intranets, MedCom has estab-
lished the healthcare internet, known as HealthcareDIX (Sundheds-
DIX), via VPN connections to VPN nodes. Operation is user-financed,
and 13 counties, CHC, Copenhagen Local Authority, two doctors’
systems, KPLL and Dan Net are currently taking part in the network.
The work on the healthcare internet consists here and now in the
development of a series of Web-based services, which are made avail-
able to the parties connected to the network.
HealthcareDIX is therefore ideally suited to fulfilling the com-
munication needs the Public Healthcare Portal has to meet.
Commentary
MedCom and the Healthcare PortalKristian Ebbensgaard, Chairman of the Association of County Councils
“MedCom plays a key role in the communication between hospitals and
GPs. The counties have taken an active part in the co-operation, which has
nurtured electronic communication without equal in the rest of Europe,”
says Kristian Ebbensgaard, county chief executive and chairman of the
Association of County Councils.
"The Association of County Councils has taken the initiative for the
joint public healthcare portal. We owe our ability to implement such an
ambitious project partly to the standardisation and infrastructure created
within MedCom.
With MedCom IV, MedCom is now moving into the hospitals and
seriously making a start on Internet technology. The primary local authori-
ties are also on the way to becoming active participants in MedCom.
A proper foundation for effective communication throughout the Danish health service has been created.”

Internet strategy 13
who are being treated in anothercounty, because they need anational or regional function.
Previous projects have shownthat great gains can be made forboth the patient and the healthservice by ensuring access to laboratory results and ECGs.
The reasons why this solutionhas not been put into practicealready are both technologicaland organisational in nature. It isnot until the closed healthcareinternet is established that there is a genuinely realistic prospect ofcarrying out a project aimed atmassive dissemination of lookupin laboratory data via the Web.
The overall aims of the projectare:● to assure the patient that all
relevant information canalways be accessed in connec-tion with treatment and in-vestigation
● to make sure that relevantresults are always available tothe attending healthcare pro-fessional, across county andorganisational boundaries
● to minimise the number ofduplicate investigations andin that way prevent thepatient being subjected tounnecessary investigations
● to establish a supplement tothe existing EDI communica-tion and create the possibilityof improving diagnoses andthe planning of treatment
The objective of the project isthat the counties and laboratoriestaking part have Internet-basedaccess to relevant data for exter-nal users developed and imple-mented and to provide access tothe service via the closed health-care internet.
The establishment of lookupprovision in laboratory systems isto be seen in the context of theforthcoming Public HealthcarePortal. If the Healthcare Portal isseriously to be the Web entryport to the health service, it isessential that services are devel-oped that make it appropriateand attractive for healthcare professionals to use the portal. A huge expansion of lookupsolutions to laboratory data,which can be made available viathe portal, will contribute tomaking the portal a natural toolfor healthcare parties to employ.
In relation to the national ITstrategy, Web access to laboratorydata will support the develop-ment of various telemedicine services.
Project Group
● Anni Christensen,
Department of Clinical
Biochemistry, Esbjerg Varde
Central Hospital
● Marianne Ebbell,
Central Laboratory, Næstved
Central Hospital
● Lone Espensen, Department
of Clinical Immunology,
Odense University Hospital
● Niels Hornum, KPLL
● Michael Johansen, B-DATA
● Lisbeth Jørgensen,
Funen County
● Kate Kusk, Viborg County
● Dorthe Skou Lassen,
Funen County
● lse Mortensen, Clinical
Biochemistry Section,
Hillerød Hospital (observer)
● Lisbeth Ramsvatn, Institute
of Pathology, Hillerød
Hospital (observer)
● Maja Stephansen,
Storstrøm County
● Kim Østerbye, Ribe County
● Lars Hulbæk, MedCom
● Claus Duedal Pedersen,
MedCom
● Iben Søgaard, MedCom
Timetable for Web lookup of laboratory data
2002 2003
09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12
Communication project Project preparationCo-operation agreementsSystem developmentSpearhead dissemination

MedCom IV – status, plans and projects14
Web requesting of tests for clinical biochemistryand clinical immunology
The project on the requesting ofanalyses in departments of clini-cal biochemistry and immunolo-gy will mean saying goodbye topre-printed request forms. Thedepartments will be able toreceive electronic requests whichthe doctors have filled in via astandard Web browser.
With the WebReq program,all doctors can send an electronicrequest in MEDREQ format as anormal EDI file to Clinical Bio-
chemistry and Immunology.WebReq enables the connecteddoctors’ systems to have labora-tory-specific information storedin a central place, so that theyare free to record and maintainthis information in the local doctors’ system. This provides anumber of benefits:
● Same procedure in the labora-tory for both EDI and Webrequesting
All departments of clinical bio-
chemistry and laboratories as
well as all suppliers of doctors’
systems are invited to take part
in the project. A WebReq project
group with the following
participants has been set up to
monitor and implement the
project:
● Dorthe Black, KPLL
● Niels Jørgensen Christensen,
Aarhus County Hospital
● Kjeld Erbs, Århus County
● Lotte Estrup, KPLL
● Finn Roth Hansen, West
Zealand County (observer)
● Rita Henriksen,
Esbjerg Central Hospital
● Niels Hornum, KPLL
● Bodil Jacobsen, Vejle Hospital
● Erik Jacobsen,
Datagruppen Multimed
● Lisbeth Jørgensen, Funen
County (observer)
● Margit Kisbye, Funen
Svendborg Hospital (observer)
● Kate Kusk, Viborg County
● Birgit Juhl Madsen,
Vejle Hospital
● Tove Charlotte Nielsen,
Vejle County
● Dora Simonsen, Viborg Hospital
● Tom Valbjørn, KPLL
● Kim Østerbye, Ribe County
● Karin Demkjær, MedCom
● Gitte Henriksen, MedCom
● Ib Johansen, MedCom
● Claus Duedal Pedersen,
MedCom
● Iben Søgaard, MedCom
Project Group
● No further investments incomparison with EDIrequesting
● Same interface regardless oflaboratory
● Freedom of choice betweenEDI and Web requesting
● Not dependent on choice oflaboratory and laboratory system
● Can easily be used by all doctors’ systems withoutmajor programming effort
● Provision for changes in laboratory systems and doctors’ systems withoutinvolving all users
● Easy access for doctors to setup their own profiles andtheir own tests
● Provision for easy re-orderingof previous tests
● Provision for printing outPTB (sampling forms)
The doctor obtains access to thesystem using a normal Webbrowser via VPN/SSL and latervia the healthcare internet. Usershave to log onto the system withan access code (external number)and a password. In WebReq, thedoctor can parameter-transfernecessary patient data and rele-vant practice information, inclu-ding default laboratory choices,so that a WebReq call can bebuilt into the individual doctors’system as a fixed routine andconsequently minimise the num-ber of manual registrations.
The procedure for requestingusing WebReq is quite straight-forward. When a request is filledin, it is approved, and a standardPTB form is completed. Alterna-tively, one of the laboratory’s

Internet strategy 15
Instruction film on laboratoryrequest
The introduction of electroniclaboratory requesting necessi-tates incorporating a number
of new procedures into medi-cal practices. To show how anefficient and practical proce-dure in relation to electronicrequesting proceeds, MedComhas prepared a number ofinstruction videos that reviewthe various requesting proce-
dures and the associated takingand labelling of samples.
The videos can be down-loaded from the MedComwebsite, www.medcom.dk.They have also been issued ona CD, available free of chargefrom MedCom.
pre-printed forms is used. Thesamples are taken, and therequest is sent off in normalMEDREQ-EDI format to therecipient laboratory.
The doctor receives a reportback from the laboratory asMEDRPT in the traditional way,but the request can also be sentas a copy to the requester withthe aim of being able to read therequested analyses into the localdoctors’ system.
Timetable for Web requesting
2003
01 02 03 04 05 06 07 08 09 10 11 12
Project descriptionCo-operation agreementsWebReq module readyMeetings with suppliersTesting of systemsPilot operationPilot operation completedFine-tuning of software, if necessaryDissemination

MedCom IV – status, plans and projects16
The “Lookup of X-ray Imagesand Descriptions via the Inter-net” project aims to providehealthcare professionals withdirect access to central patientinformation stored in the X-raysystem of another county or hospital. It is very relevant inconnection with emergency ad-missions, treatment of free-choicepatients and national and region-al patients or in the preparationof the treatment of a new patient.The healthcare professional canobtain the information quicklyvia Web lookup, so that thepatient’s treatment is efficient and of the highest quality.
Web lookup also makes it possible to establish different tele-medicine services, such as askingan expert for a second opinion.As the shortage of experts in thearea of radiology increases, tele-medicine solutions of this typewill steadily gain ground.
Finally the lookup solutionwill be useful for GPs when theyhave to inform patients abouttheir illness and treatment, as X-rays often encourage dialoguewith the patient. Access for doctors to X-rays additionallysupports the upgrading of skills
among both GPs and specialists.The reasons why this solution
does not already exist are bothtechnological and organisationalin nature. It is only with theestablishment of the closedhealthcare internet that it is genuinely realistic to carry out aproject that disseminates alookup solution of both X-raydescriptions and various types ofimages stored in digital form.
The overall aims of the pro-ject are:
● to assure patients that all rele-vant information can alwaysbe accessed for treatment andinvestigation
● to make sure that relevant X-ray descriptions and imagesare always available to theattending healthcare profes-sional, across county andorganisational boundaries
● to minimise the number ofduplicate investigations andin that way prevent thepatient being subjected tounnecessary investigations
● to establish a supplement tothe existing EDI communica-tion and create the possibilityof improving diagnoses andthe planning of treatment
The objective of the project isthat the counties and laboratoriestaking part have Internet-basedaccess to relevant data for exter-nal users developed and imple-mented and to provide access tothe service via the closed health-
care internet. The establishmentof lookup provision in laboratorysystems is to be seen in the con-text of the forthcoming PublicHealthcare Portal. Massive dis-semination of lookup solutionsto image diagnostic data, whichcan be made available via theportal, will contribute to givingthe portal the healthcare contentthat makes it a natural tool forhealthcare parties to employ.
Web lookup of X-raysimages anddescriptions
Project Group
● Dan Gedebjerg, Esbjerg Varde
Central Hospital (observer)
● Finn Roth Hansen,
West Zealand County
● Bjarne Hjorth, Odense
University Hospital
● Lisbeth Jørgensen, Funen
County
● John Kiil, West Zealand
Hospital
● Lillian Kofoed,
Kalundborg Hospital
● Tove Charlotte Nielsen,
Vejle County (observer)
● Marianne Richelsen,
Hillerød Hospital
● Kim Østerbye, Ribe County
(observer)
● Lars Hulbæk, MedCom
● Claus Duedal Pedersen,
MedCom
● Iben Søgaard, MedCom
Timetable for Web lookup of X-ray data
2002 2003
09 10 11 12 01 02 03 04 05 06 07 08 09 10 11 12
Communication project Project preparationCo-operation agreementsSystem developmentSpearhead dissemination

Internet strategy 17
This project, which is concernedwith establishing a nation-wide“teledermatology network”, isbased on MedCom’s TeleMedproject from 1999. During thecourse of three months of operation, MedCom tested thesending of digital skin images tosupplement the traditional co-operation and pattern of referralbetween medical practices anddermatology specialists.
Experience from this projectshowed that it is possible tomake gains in the form of:
● Easily available specialist support
● Improved patient service, fewer visits to doctors, noextra transport, waiting timeand absence for the patient
● Improvement in the quality oftreatment
● Regular continuing trainingof the doctor
● Simpler check-up/follow-uptreatment in general practice
● Support of the patient’s freechoice of specialist
The overall objectives of the tele-dermatology project are to:
● Replace/supplement generalreferrals to skin specialistswith telemedicine consulta-tions
● Ensure patients have of equaland quick access to specialistassessments of skin imagesthrough their own doctor
● Support continuing trainingof GPs through communica-tion with skin specialists
● Establish nation-wide pro-vision for telemedicine skinimage consultation
In relation to the future nationalIT strategy for the health service,the establishment of a telederma-tology network will be the firststep towards putting into effectthe recommendations made inthe Ministry of Health’s tele-medicine report from 2001.
The establishment of tele-dermatology is to be viewed inthe context of the future PublicHealthcare Portal. Via theHealthcare Portal, GPs canobtain an overview of providersof teledermatology consultation,and guidance and recommenda-tions in connection with tele-dermatology should also be avail-able here. In the longer term, a
Teledermatology network
teledermatology network can besupplemented by a national skinimage database of particularlyinteresting and/or typical skinailments, as known from Erlangen University in Germany.
Project Group
● Birte Elgaard Andersen,
Copenhagen County
● Kjeld Erbs, Århus County
● Jens Grønlund, Viborg County
● Bo Gundtofte, Roskilde
County (observer)
● Finn Roth Hansen,
West Zealand County
● Lisbeth Jørgensen, Funen
County
● Tonny Karlsmark,
Bispebjerg Hospital
● Finn Klamer, Øster Jølby, Mors
● Tine Korsholm, Ringkjøbing
County
● Ove Kristensen, West Zealand
● Søren Lorentzen, Frederiks-
borg County (observer)
● Peter Pedersen, CHC
● Bjørn Perrild, Kongens
Lyngby
● Hanne Boje Rasmussen,
Odense
● Peter Wendelboe, Grenaa
● Lars Hulbæk, MedCom
● Claus Duedal Pedersen,
MedCom
● Iben Søgaard, MedCom

MedCom IV – status, plans and projects18
from the Institute of Patholo-gy at Vejle Hospital to medicalpractices and the exchange ofskin images between GPs inVejle County and specialists inskin diseases in Århus County.The trial was an unconditionalsuccess. MedCom has there-fore decided to draw up joint
Danish guidance for this EDImessage, known as MEDBIN.
MEDBIN is used today forthe transfer of skin images andis employed in MedCom’s dermatology project and forthe transfer of medication up-dating files and electrocardio-grams.
Edifact – with MEDBIN elements
PNA+PAT+PatCPR:::CPR:IM+++SU:PatEnavn+
FO:PatFnavn'
RFF+XPI:PatErstatCPR'
Binary elements S11+11'
UNO+Objektlbnr+AID:Objektrefnr+OBJ:
OBJEKTTYPE:OBJEKTEXTENSION:91+
Objektstoerrelse:14:1:A'
The object file SelveObjektet
UNP+Objektstoerrelse+Objektlbnr'
Number of repetitions UNO/UNP can be repeated up to 10 times.
The max. size of the ActualObject
(SelveObjektet) is 20 Mbyte
MEDBIN – images by EDIFACTIn conjunction with imple-mentation of the consolidationproject and with inspirationfrom the EU CoCo project,the idea arose of employingexisting EDI solutions totransfer items other thansmaller text-based documents.These may, for example, beimages and text documents ofsignificant size. Mention canbe made here of X-ray imagesand pathology images as wellas a common basis of data formedication and patient listingfor general practice.
In co-operation with Data-gruppen MultiMed, KMD,Vejle County, B-Data andÅrhus County, in the spring of2002 MedCom carried out atrial on the exchange of images
Eye fundus image X-ray image ECG
Initial dissemination of tele-dermatology can additionallyform the basis for increasedinterdisciplinary co-operationbetween the home care service,medical practices and dermatolo-gists in the area of wounds.Finally teledermatology can pre-pare the way for other tele-medicine solutions in relation togeneral practice in the future, forexample in cardiology.
Timetable for teledermatlogy
2002 2003
10 11 12 01 02 03 04 05 06 07 08 09 10 11 12
Communication project Project preparationCo-operation agreementsHealthcare recommend.System devel. (MedBin)Spearhead dissemination

● Jørgen Granborg,
A-Data ApS, PLC
● Carsten Jacobsen, KMD A/S
● Erik Jacobsen, DataGruppen
MultiMed ApS
● Bo Nielsen, bo soft A/S
● Morten Pedersen,
Datapharm A/S
● Michael Rasmussen,
Dan Net A/S
● Palle Runer, DataPharm A/S
● Ole Sprøgel, Dan Net A/S
● Lise Wormstrup, KMD A/S
● Lars Hulbæk, MedCom
● Claus Duedal Pedersen,
MedCom
● Martin Bech, UNI-C
● Ib Lucht, UNI-C
Internet strategy 19
EDI via Internet
In connection with the testing ofthe technical infrastructure, co-operation agreements with theVANS suppliers in the present-day healthcare data networkensure that the suppliers togetherwith any other future networkproviders in the Internet-basedhealthcare data network are ableto handle EDI mail via the Inter-net over the HealthcareDIX(SundhedsDIX).
The purpose of this is toensure coherence between theexisting healthcare data networkand the future healthcare datanetwork in the area of EDI. Itrequires all parties in the Inter-net-based healthcare data net-work to apply the same envelopestandard. Only a change in envelope wrapping is concerned,as the EDI standards are appliedin the same way as today. Tosupport the dissemination ofEDI mail via the Internet, thereis a need for MedCom to ensureuniform envelope wrapping byoffering supplier testing in theperiod 2003-2005, in accordancewith the EDI mail standard. Thedissemination of EDI mail canaccordingly be based on the freemarket.
The trial, which was com-pleted in September 2003,involved KMD, Dan Net, Data-Gruppen MultiMed, A-Data,Apotekernettet, DataPharm andCitoData (bo soft A/S).
Project Group
HealthcareDIX
EDI exchange via the HealthcareDIX is based on decentralised mail-exchange servers (MX).
PharmacyNetwork
MXMX
MXMX
MX

MedCom IV – status, plans and projects20
The reason for the Hospital-Local Authority XML project isto expand the use of a number ofelectronic messages – the elec-tronic admission message, ad-mission report and dischargemessage. All three messagesstrengthen communication be-tween hospital and local authori-ty, where there has traditionalbeen problems in ensuring com-munication on admission to anddischarge from hospital.
As of September 2002, only17% of the Danish populationwere covered by messages of thistype, despite the opportunitiesthat exist in facilitating the pro-cedure and ensuring betterpatient treatment by virtue ofelectronic communication.
The target group for the pro-ject is primarily those hospitalsand local authorities that do notuse these electronic messages. Atthe same time, those hospitalsand local authorities that alreadyexchange advices and admissionresults have long wanted to ex-pand electronic communication.There is a need to make possiblea regular exchange of informa-tion before, during and after anadmission.
This desire, with a solid foun-dation in healthcare, can be metby supplementing the standardmessages with the possibility of
● for the project to support other key initiatives in rela-tion to the healthcare sector,including in particular:– Building-up of the XML
database of the Ministry ofScience
– The work of the NationalBoard of Health with G-EPR
– Further development by theNational Association ofLocal Authorities/Ministryof Social Affairs of Com-mon Language
– Build-up of the PublicHealthcare Portal
– The work of the DigitalTaskforce on legal barriersto digital administration.
The Hospital-Local AuthorityXML project is to be seen in thecontext of the general work onEDI-XML translation. This workis necessary with a view topreparing the Public HealthcarePortal.
The EDIFACT standards foradvices and admission results aretechnically the simplest of allMedCom standards. It is there-fore logical to use these standardsfor a first testing of options inEDI-XML translation.
The project is to ensure thatcoherence is created between thedevelopment of the healthcaredata network and the overallXML work in the Ministry ofScience. At the same time, aframework was created forexpanding basic communicationsolutions among hospitals andlocal authorities.
sending and receiving technicaland clinical messages and allECR systems in the local authorities and all PAS systemsin the hospitals.
At the same time, the projectis aimed at expanding the use ofcorrespondence messages andwarning of completion of treat-ment. The correspondence mes-sage can fulfil a large number ofcommunication needs for whichthere is a demand in the hospi-tals and local authorities. Thefree-text field of the message canbe filled in for instance by re-using existing recordings fromECRs, including information onmedication and services providedand functional assessment. Fromthe hospital, action and retrain-ing plans can be written directlyinto the correspondence moduleof the PAS system.
The aim of the Hospital-Local Authority XML project istherefore:
● to ensure that the use ofadvice of admission, admis-sion result and advice of dis-charge is extended to hospitalsand local authorities that cover 75% of the Danishpopulation at the end of 2004
● to ensure the necessary tech-nical conditions for a sharpincrease in the use of the cor-respondence message andwarning of completion oftreatment, so that countiesrepresenting 75% of the Danish population offer thesecommunication options tointerested local authorities atthe end of 2004
The local authorities andhealthcare communication
Hospital-LocalAuthority XML project

North Jutland
County:
Aalborg
Læsø
Funen County:
Odense
Årslev
Ørbæk
Ryslinge
Rudkøbing
Svendborg
Vejle County:
Fredericia
West Zealand
County:
Holbæk
Slagelse
Frederiksborg
County:
Frederiksværk
Stenløse
Slangerup
Helsingør
Roskilde County:
Skovbo
Roskilde
Køge
Vallø
CHC:
Copenhagen
Frederiksberg
Copenhagen
County:
Søllerød
Lyngby-Tårbæk
Storstrøm County:
Højreby
Næstved
Nakskov
Sakskøbing
Participants in project
● County taking part in the
local-authority project
● County not taking part in the
local-authority project
● Local authority in the healthcare
data network
● Local authority in the healthcare
network additionally taking part
in the Hospital-Local Authority
XML project
The local authorities and healthcare communication 21
MedCom IV Local-Authority Group
● Lene Meyer Grosen, ProjectManager, Frederiksb. County
● Marianne Strand, Project Manager, Stenløse Loc. Auth.
● Kim Snekkerup, Administrative Consultant,Frederiksværk Local Authority
● Lisbeth Rasmussen, SeniorNursing Officer, Fun. County
● Alice Kristensen, ProjectManager, Svendborg LocalAuthority
● Lissi Veltzé, Home Care Manager, Ørbæk Local Auth.
● Susanne Grøntoft Larsen,Sen. Systems Consultant, CHC
● Merete Halkjær, IT Cons.,Copenhagen Local Authority
● Anne-Marie Falch, ProjectManager, North Jutl. County
● Isabelle Andersen, Head ofDay Care, Læsø Local Auth.
● Kirsten Skovrup, Head of Section, Aalborg Local Auth.
● Jens Henning Rasmussen,Head of IT, Roskilde County
● Agnete Seidelin, Project Co-ordinator, Roskilde Loc. Auth.
● Anne Danborg, Head ofHome Care, Skovbo LocalAuthority
● Birgit Nielsen, Project Manager, Storstrøm County
● Søren Skafte Jensen, IT Officer, Nakskov Local Auth.
● Kim Østerbye, Senior IT Consultant, Ribe County
● Lene Bilslev-Jensen, ProjectCons., The Digital Taskforce
● Bentt Nielsen, DevelopmentConsultant, National Boardof Social Services
● Dorthe Skou Lassen, ProjectManager, MedCom
● Lars Hulbæk, Project Manager, MedCom
● Iben Søgaard, Project Secretary, MedCom
2002 Project preparation
2003 January Supplier co-operation agreements and pilot participant co-operation agreements signed.
May Information to all Danish local authorities concerning dis-semination activities in 2004.
September Supplier testing and MedCom certification carried out.
December Minimum of 3 months of pilot operation carried out.
Continued Marketing from relevant parties behind MedCom. dissemina- tion in 2003
2004 Dissemination co-operation agreements with counties/ CHC
End Spearhead dissemination in (at least) one county with alllocal authorities carried out.
Whole of 04 Marketing from relevant parties behind MedCom.
Hospital-Local Authority XML project timetable
●
●
●
●●
●●●●
●●
●●●●
●●●●
●
●
● ●
●
●
●
●

MedCom IV – status, plans and projects22
Common Language II is a con-ceptual framework which thelocal authorities can use to de-scribe the functional capacity ofcitizens whose needs are assessedby the local authority and theservices provided in the area ofthe elderly and disabled. Com-mon Language II provides anoverview of the citizen’s overallfunctional capacity.
The overriding objective ofCommon Language II is to create political and technical co-herence in the effort that ismade. The target group forCommon Language II is poli-ticians and specialised staff, primarily the needs assessors.
Common Language II consti-tutes a clinical database that col-lects information on all citizenswhose needs are assessed and can
be used for broader technicaldevelopment, as well as manage-rial and political priority-setting.Common Language II has notbeen developed to be used in theclinical situation, where servicesare provided at the home of theindividual citizen.
A needs assessor makes afunctional assessment through
eight areas of assessment at fourlevels of functional capacity andrecords the allocation of servicesin a services catalogue. In addi-tion, the effect of the home andthe use of technical aids on theperson’s functional capacity isassessed. The registration of tech-nical aids follows a classificationsystem in accordance with aninternational standard on “Tech-nical Aids for Disabled Persons”.
Common Language II is basedon ICF, which forms part of theHealth Service Classification System (SKS). The developmentof Joint Language II is being co-ordinated and integrated with thework of the National Board ofHealth with ICF within SKS.
MedCom is monitoring devel-opment by being represented inthe National Association of LocalAuthorities (KL) reference groupfor Common Language.
The development of CommonLanguage II is being dealt withby KL and can be followed onthe KL website: www.kl.dk/fs
The Hospital-Local Authorityproject and Common Language
Commentary
Better coherenceThe Minister of Social Affairs, Henriette Kjær
“Many elderly people find that they have to tell the same story time after
time. The same personal information has to be given to the home care
service, the hospital, the GP and perhaps the home care service again,”
says Henriette Kjær, the Minister of Social Affairs "That isn’t clever, it’s
inappropriate!
It also happens that elderly people simply ’slip out’ of the system,
because during the course of an illness changes may have occurred in the
elderly person’s home care – and he or she is simply discharged. The
systems therefore have to become better at talking to each other.
Under the MedCom co-operation, targeted effort is made to
disseminate the electronic communication between hospitals and local
authorities, so that better coherence is created between the social and healthcare sectors. The result might
perhaps be that elderly people avoid having to give the same information repeatedly. It would, in any case,
be a good start.”

The local authorities and healthcare communication 23
The project on LÆ forms is in-tended to ease the written com-munication between the localauthorities and general practition-ers and between the local authori-ties and specialists both in hospi-tals and in private practice.
LÆ forms are used in manyareas in municipal administration,for instance in connection withvoluntary early-retirement pen-sion and sickness benefit. Elec-tronic versions of the forms are anatural part of doctors’ practicesystems, but at present the formsare not sent electronically.
The LÆ forms are standard-ised by the certification commit-tee of the Danish Medical Asso-ciation, which consists of repre-
sentatives of general practitionersand the National Association ofLocal Authorities. The procedurein using LÆ forms comprisestwo steps:
1. A request is sent from thelocal authority requestingcompletion of a certificate.The application can be sent toa GP or to a specialist in pri-vate practice.
2. The recipient sends relevantinformation back to the localauthority on a certificate.
The purpose of the LÆ formproject is to make it possible tocarry out both steps one and twoelectronically.
Timetable
April-Oct. 2003: Pre-analysis.November 2003: Start-up oftechnical pilot project.
The LÆ formproject
Project Group
The participants in the project’s
pre-analysis group are:
● Morten Hein,
Ministry of Social Affairs
● Marie Munk Jensen,
Ministry of Finance
● Anne Marie Nielsen,
Esbjerg Local Authority
● Claus Nielsen, National Asso-
ciation of Local Authorities
● Lars Nielsen,
Odense Local Authority
● Mette Brøsted Nielsen,
Esbjerg Local Authority
● Jens Parker, General Prac-
titioner, Copenhagen
● Charlotte Henius Meier, Nat.
Assoc. of Local Authorities
● Morten Elbæk Petersen, The
Public Healthcare Portal
● Marianne Rosted,
Aalborg Local Authority
● Kurt Samsø, Århus
Local Authority
● Dorte Schwartz,
Copenhagen Local Authority
● Lene Bilslev-Jensen,
Ministry of Finance
● Lars Hulbæk, MedCom
● Dorthe Skou Lassen,
MedCom
●●
●
●
●
● The partici-
pating municipalities are:
Aalborg, Århus, Esbjerg,
Odense and Copenhagen
The LÆ form project is intended to prepare the way for the electronicexchange of more of the forms used in the healthcare sector. The project istesting integration between the basic systems of the healthcare sector via acentral form server, which is accessed through the Healthcare Portal andthe HealthcareDIX.
LocalauthorityCounty
Medical practice
Medical practice
Medical practice Medical practice
County
Local authority
Dan Net
Medical practiceCounty
Local authority
KMDnetwork
Doctors’system
Internet
Formserver
Healthcareportal
HealthcareDIX

MedCom IV – status, plans and projects24
Commentary
Co-operation and coherenceEjgil W. Rasmussen, Mayor
Chairman of the National Association of Local Authorities
“Good co-operation between healthcare professionals in local authorities
and counties is vital if we are to be able to make a coherent effort,
particularly in relation to the elderly and in community healthcare in the
local authorities,” says Ejgil W. Rasmussen, Chairman of the National
Association of Local Authorities.
“Unfortunately, far too often we see failure of communication when a
person moves between the various bodies involved. Electronic communi-
cation between the parties may help towards them all being updated for
example on a person’s insulin treatment, so that the home care service
healthcare service can implement the necessary cost changes or so that the
necessary action plan reaches all the parties who are concerned with the person.
The National Association of Local Authorities has therefore actively re-entered the MedCom co-operation.
In line with the local authorities having reached almost 85% coverage of electronic care records, the oppor-
tunities for electronic co-operation have substantially increased. And new areas are appearing in the fields of
healthcare and vulnerable children and adolescents. Here it is important that the experts become aware of any
failures as early as possible.”
Perspective
The IT Lighthouse’s local authority-medicalpractice communication
The IT Lighthouse project “Exchange of information in the healthcare
sector” comprises a range of communication flows between the care
system of Aalborg Local Authority and four general practitioners with
four different doctors’ systems. It specifically relates among other things
to communication on home care status, prescription renewal and correspondence.
Home care status: Regular updating of the doctors’ system with information on services provided by the
local authority to the patient/client.
Prescription renewal: Prescription renewals directly from the medication card of the care system to the
doctors’ system.
Correspondence: Patient-attributable, but non-structured exchange of information.
In April 2003, the statistics for communication between the local authority and the four doctors showed that 14
correspondence messages, 2196 messages on home care healthcare status and 212 prescription renewals were
sent in the course of the month.
The project is being carried out under the project management of Aalborg Local Authority.
Further information can be found at: http://www.detdigitalenordjylland.dk/index.php/m/142
Pho
tog
rap
h: S
øre
n W
esse
lto
ft F
oto
gra
fi

Hospitals and healthcare communication 25
The aim behind MedCom’s hos-pital projects is to support theelectronic communication ofpatient data between hospitals indifferent counties.
No nation-wide communicationbetween hospitals Today it is possible to carry outEDI communication betweenany hospital and any medicalpractice, regardless where in thecountry the hospital or medicalpractice is located. It is not, however, possible at present tocarry out EDI communicationbetween hospitals in differentcounties.
The projects are intended tosupport the introduction of EPRsystems in the hospitals andensure that information can beexchanged between IT systems intreatment units in different coun-ties – and therefore also to sup-port the communication betweentreatment units and other partieswithin the hospitals and betweenhospitals in the same county.
The objective is that by theend of 2005:
● the XML communicationproject has resulted in large-scale nation-wide use of allrelevant MedCom messagesfor communication betweenhospitals.
The XML EPR communicationproject is essentially based onthe experience acquired in Med-Com’s present communicationprojects with the primary sector,while the SUP project is basedon a similar project carried outby the counties of Vejle, Viborgand Århus.
● MedCom’s SUP project hasresulted in participating coun-ties having established extractsystems and transfer of EPRsand patient data to a county/inter-county SUP database/browser, from which secureInternet access to relevantinternal and external users isestablished.
The hospitals and health-care communication
From hospitalto hospital
MedCom’s two hospital projects
are co-ordinated by the Hospital
Project Managers Group.
● Karin Argir, Capio Diagnostik
● Lone Behnfeld,
South Jutland County
● Hans Henrik Bøttger,
Århus County
● Anne-Marie Falch,
North Jutland County
● Ole Filip Hansen,
Viborg County
● Morten Hansen, Vejle County
● Lone Hassingboe,
North Jutland County
● Hans Erik Henriksen, IBM
● Svend Holm Henriksen,
Odense University Hospital
● Søren Rosenørn Jakobsen,
Acure
● Michael Johansen, B-DATA
● Jørgen Schøler Kristensen,
DADL
● Per Wagner Kristensen, DADL
● Dorthe Skou Lassen,
Funen County
● Søren Lorentzen,
Frederiksborg County
● Finn Mathiesen,
Danish Society of Radiology
● Lisbeth Nielsen,
Association of County Councils
● Sanne Nørgaard,
CSC Scandihealth
● Helle Stockfleth Olsen,
Statens Serum Institut
● Jan Petersen,
National Board of Health
● Jørgen Hjelm Poulsen, Danish
Society for Clinical Biochemistry
● Jens Peder Rasmussen,
Systematic
● Kim Østerbye, Ribe County
● Karin Demkjær, MedCom
● Lars Hulbæk, MedCom
● Gitte Henriksen, MedCom
● Henrik Bjerregaard Jensen,
MedCom
● Ib Johansen, MedCom
● Jens Rahbek Nørgaard,
MedCom
● Claus Duedal Pedersen,
MedCom
● Iben Søgaard, MedCom
The Hospital Project Managers Group

33
534 32
32588
12
1 1398 4766 227
266
Laboratory communication between counties
MedCom IV – status, plans and projects26
Taken together, the two projects will signify a markedimprovement in electronic com-munication:
● The XML EPR communica-tion project will boost theefficiency of daily routinecommunication between thetreatment units of the hospi-tals and between these andthe clinical diagnosis units inthe form of referrals, reports,discharge summaries, labora-tory results etc., in the same
way as has been done forcommunication with the pri-mary sector.
● MedCom’s SUP project willprovide easy and unimpededbrowser access to record dataacross hospitals and internallyfor the large groups of doctorsand nurses who are not usingthe EPR and PAS systemsconcerned beforehand.
The projects are co-ordinatedwith the National Board of
Health’s national G-EPR devel-opment, which in the longerterm is intended to result in sub-stantially more uniform andadvanced EPR systems in theDanish healthcare sector.
MedCom’s XML EPR stan-dards will therefore be broadenedin the autumn of 2003, so thatthey are prepared for the com-munication of the correspondingmessages as EPR systems basedon G-EPR are introduced.
With the introduction of the“Good Laboratory Results”and common IUPAC analysiscodes in all the counties andnational laboratories, itbecame possible to exchangelaboratory results between theclinical biochemistry systemsof the various counties.
CSC-Labka and B-Data
have developed a module, so that RPT01 – clinical bio-chemistry results can be received directly from otherlaboratories.
Samples which are forward-ed from the local laboratoryfor analysis in an out-of-county or service laboratoryare received and introduced
automatically into the cumula-tive reply schema of the locallaboratory, immediately afterapproval in the service labora-tory. Without any manual keying at all. The same MedCom standard, RPT01,which is used to send resultsto medical practices is used.
N. J
utl
and
Vib
org
Årh
us
Rin
gkø
bin
g
Rib
e
Vej
le
S. J
utl
and
Fun
en
W. Z
eala
nd
Sto
rstr
øm
Ro
skild
e
Fred
erik
sb.
CH
C
Co
pen
hag
en
Bo
rnh
olm
KPL
L
SSI
Gre
enla
nd
RPT01 between counties, April 2003
From / To
North JutlandViborgÅrhusRingkøbingRibeVejleSouth JutlandFunenWest ZealandStorstrømRoskildeFrederiksborgCHCCopenhagenBornholmKPLLSSIMedilab
Århus County 0 500 1000 1500
2 Within hospital3 Hospitals within county4 Hospitals betw. counties5 Primary sector
Funen County 0 200 400 600 800 1000
1 Within department2 Within hospital3 Hospitals within county4 Hospitals betw. counties5 Primary sector6 Other
Clinical service
c. 40%
Other hospitals
c. 10%
Other service
c. 13%
Administration
c. 4%
Primary sector
c. 13%Medicalpractice
Nursinghomes
Homecare
Specia-lists
Otherclinicaltreatmentunits
EPRc. 23%
Clinicaltreatmentunit
HOSPITAL
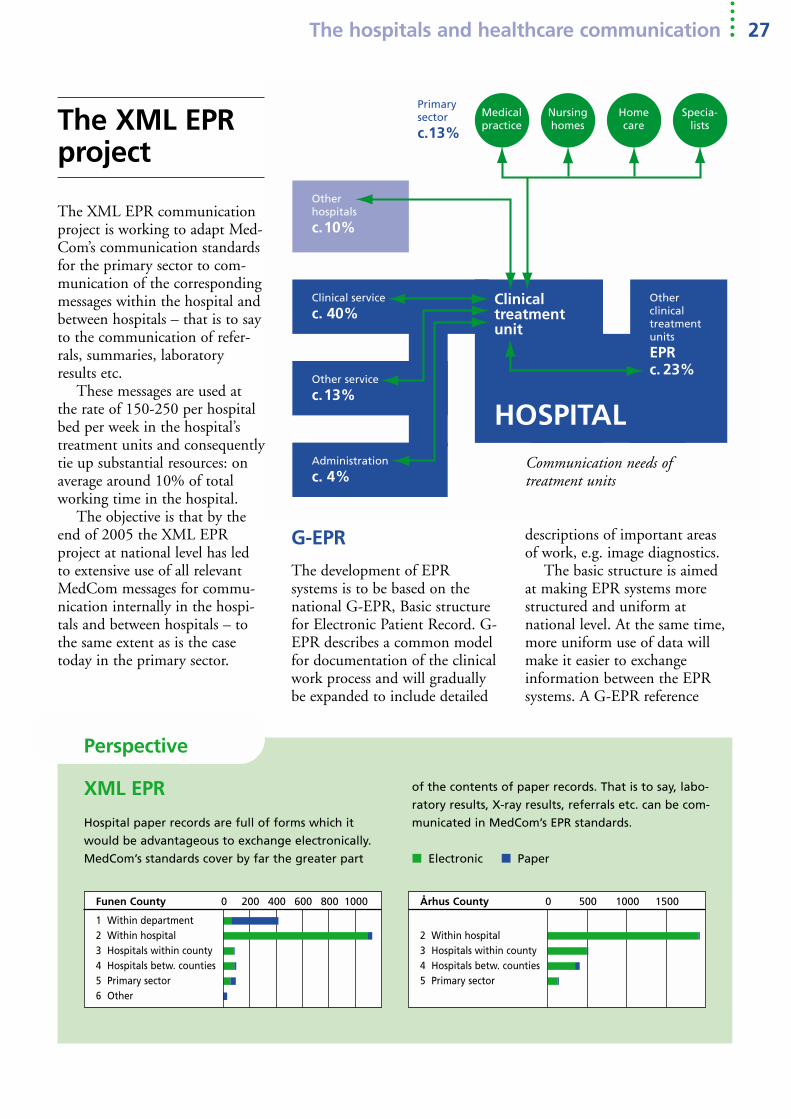
descriptions of important areasof work, e.g. image diagnostics.
The basic structure is aimedat making EPR systems morestructured and uniform atnational level. At the same time,more uniform use of data willmake it easier to exchange information between the EPRsystems. A G-EPR reference
The XML EPRproject
The hospitals and healthcare communication 27
Communication needs of treatment units
G-EPR
The development of EPR systems is to be based on thenational G-EPR, Basic structurefor Electronic Patient Record. G-EPR describes a common modelfor documentation of the clinicalwork process and will graduallybe expanded to include detailed
The XML EPR communicationproject is working to adapt Med-Com’s communication standardsfor the primary sector to com-munication of the correspondingmessages within the hospital andbetween hospitals – that is to sayto the communication of refer-rals, summaries, laboratoryresults etc.
These messages are used atthe rate of 150-250 per hospitalbed per week in the hospital’streatment units and consequentlytie up substantial resources: onaverage around 10% of totalworking time in the hospital.
The objective is that by theend of 2005 the XML EPR project at national level has ledto extensive use of all relevantMedCom messages for commu-nication internally in the hospi-tals and between hospitals – tothe same extent as is the casetoday in the primary sector.
Perspective
XML EPR
Hospital paper records are full of forms which it
would be advantageous to exchange electronically.
MedCom’s standards cover by far the greater part
of the contents of paper records. That is to say, labo-
ratory results, X-ray results, referrals etc. can be com-
municated in MedCom’s EPR standards.
■ Electronic ■ Paper

MedCom IV – status, plans and projects28
implementation has been startedup which comprises a test data-base for the testing of G-EPR.
In line with the introductionof EPR systems based on G-EPR, new ways of obtainingmore flexible access to data inthe healthcare sector will arise. G-EPR thus creates the frame-work for the long-term develop-ment of EPR systems and jointuse of patient systems in Den-mark. The XML EPR communi-cation project is to be viewed aspart of a realistic option for com-munication between EPR sys-tems, based on a joint G-EPRstructure.
While G-EPR necessitates thedevelopment and introduction ofa new type of EPR systems, theXML EPR communication pro-
ject is based on existing IT systems and on communicationbetween the IT systems used inthe healthcare sector today.
OiO – Public information OnlineMedCom’s XML documentationis drawn up in accordance withthe guidelines for OiO – PublicInformation Online (seewww.oio.dk/xml). OiO is a col-lective concept for the documen-tation of standards for the publicsector drawn up by the Ministryof Science, Technology andDevelopment in co-operationwith the National Association ofLocal Authorities and the Asso-ciation of County Councils.
Implementation ofXML EPRThe methods and timetables forthe introduction of EPR systemsdiffer widely in the individualcounties and CHC. For this reason, the XML EPR communi-cation project is divided into twoimplementation periods: Group2004 and Group 2005 – andinto three communication pack-ages: the Primary Package, theHospital Package, the ClinicalPackage.
It is intended that every coun-ty or CHC chooses which com-munication packages and whichimplementation periods are bestsuited to its own IT strategy.
Each communication packagecovers fundamental communica-
Hospital Package
Between hospitals and EPR and PAS:XML Discharge summaryXML Outpatient summaryXML Hospital referralXML Booking resultXMLEDI Correspondence letterXML Personal master dataXML Medication data
Clinical Package
Between radiology departments,EPR and any PAS:XML Image diagnostics summaryXML Image diagnostics referral
Between laboratories, EPR and anyPAS:XML Laboratory resultsXML Pathology resultsXML Microbiology resultsXML Immunology resultsXML Laboratory requestXML Pathology requestXML Microbiology request
Primary Package
Between EPR and medical practice –possibly via PAS:XMLEDI Discharge summaryXMLEDI Outpatient summaryXMLEDI Hospital referralXMLEDI Booking resultXMLEDI Correspondence letter
Between EPR and home care –possibly via PAS:XMLEDI Admission adviceXMLEDI Admission resultXMLEDI Discharge adviceXMLEDI Warning of completion of
treatmentXMLEDI Correspondence letter
l service
Otherhospitals
service
istration
Primary sector Medical
practiceNursing
homeHomecare
Specia-lists
OtherclinicaltreatmentunitsEPR
Clinicaltreatmentunit
HOSPITAL
Clinical service
Other hospitals
Other service
Administration
Primary sector Medical
practiceNursinghome
Homecare
Speclist
Otherclinicaltreatmentunits
EPR
Clinicaltreatmentunit
HOSPITAL
Clinical service
Otherhospitals
Other service
Administration
Primary sector
Medicalpractice
Nursinghome
Homecare
Specia-lists
Otherclinicaltreatmentunits
EPR
Clinicaltreatmentunit
HOSPITAL

The hospitals and healthcare communication 29
What can be done more easily?
● The whole communication packages are disseminated at once – greater impact and overview.In the primary sector the individual messages are introduced individually over the years. Dissemi-nation of whole communication packages on a large scale will make both system development andimplementation substantially more efficient.
● Prior testing bypasses MedCom. In the primary sector, a number of pilot projects were carriedout in 1994-1996 which were to test communication for the first time. Today it is possible to carryout prior testing of both the sending and receipt of messages, so that it is possible to start directlywith dissemination.
● Mandatory positive and negative acknowledgement safeguards logistics. In 2002, mandatoryacknowledgement for the primary communication was introduced. This eases administration andfault-tracing, and it is consequently expected to be used on the hospital side from the outset.
tion needs between treatmentunits and other major parties:
● The Hospital Package coverscommunication between hos-pitals and mutually betweentreatment units.
● The Clinical Package coverscommunication betweentreatment units and labora-tories and radiology depart-ments.
● The Primary Care Packagecovers communicationbetween treatment units,medical practices and thehome care service.
The Correspondence Letter mes-sage should be included in allcommunication packages, as thismessage is already implementedtoday in all doctors’ systems andis in addition expected to be im-plemented in all local-authoritycare systems. The Correspon-dence Letter will therefore be theonly message capable of beingsent between almost all parties inthe healthcare sector, apart fromlaboratories and radiologydepartments.
Depending on which commu-nication packages the individualcounty/CHC chooses to takepart in, it will be necessary toinvolve the IT suppliers which
the counties are already using atpresent in the areas concerned.Communication of the ClinicalPackage, for example, will in-volve the county’s laboratory systems, radiology systems andEPR systems.
After the implementationperiod, it will be possible tocommunicate the messages con-cerned between all hospitaldepartments and all hospitals
which have implemented thesame communication packagesboth within the country and atnational level.
The XML EPR communica-tion project is equivalent in sizeand implementation to the pro-jects carried out in the primarysector since 1994. The projectmay involve roughly the samenumber of IT systems andrequire the development of
Timetable for the XML EPR communication project
MedCom IV 2002 2003 2004 2005
1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4
XML EPR projectHospital group
Prim. and clin. packagesG-EPR co-ordinationComm. studyTechnical groupHealthcare adjustmentXML standardsSupplier bids TKSystem developmentTestingDissemination group ADissemination group B
Hospital PackageG-EPR adjustmentXML standardsSupplier bids TKSystem developmentTestingDissemination group ADissemination group B

MedCom IV – status, plans and projects30
Participants
With the exception of Ringkøbing, all countieswest of the Great Belt havedecided to take part inMedCom’s XML EPR project. Counties east ofthe Great Belt have not yet taken a decision in theautumn of 2003.
roughly the same number ofcommunication interfaces. Onthe basis of experience fromcommunication in the primarysector, however, it is possible tosubstantially improve efficiencyand simplify implementation anddissemination.
In a single area, howeverimplementation is more com-plex. In the primary area EDI-FACT is used as communicationsyntax, while XML syntax is usedin the hospital area. For this reason it is necessary to convertthe EDIFACT message of thePrimary Package to XML syntax.
Almost all IT suppliers haveopted to take part in the com-munication with the primarysector. Provided this remains thecase for communication in thehospital area, the project willaltogether comprise over fortyclinical IT systems.
Clinical service
Otherhospitals
Other service
Admini-stration
Primary sector
Medicalpractice
Nursing home
Homecare
Specia-lists
Otherclinicaltreat-mentunitsEPR
Clinicaltreatmentunit
HOSPITAL
Clinical service
Otherhospitals
Other service
Admini-stration
Primary sector
Medicalpractice
Nursing home
Homecare
Specia-lists
Otherclinicaltreat-mentunitsEPR
Clinicaltreatmentunit
HOSPITAL
Use of Clinical IT today: Virtually full IT coverage everywhere – however only 7% EPR in treatment units and 50% ECR in homenursing.
XML between and in hospitals. EDIFACT to the primary sector. XML EDIFACT conversion of the primary package
Number Interfaces Interfacessystems per system total
EPR systems 8 35 280PAS systems 6 25 150X-ray systems 8 6 48Laboratory systems 6 8 48Blood-bank systems 4 4 16Pathology systems 4 6 24Microbiology systems 5 6 30Total 41 90 596
Number of interfaces if all communication packages are implemented
Unchanged
EDIFACT with
primary sector.
XML between
hospitals in diffe-
rent counties,
internally
between depart-
ments and
between hospitals
in the county.
Full coverage
with EPR and
S&A. Only 50%
ECR in home care
Full coverage
with PAS. Only
7% EPR in treat-
ment units
Full coverage
with LIS and RIS

The hospitals and healthcare communication 31
Dose dispensing and new prescriptionMedCom is taking part in the development of anew message for the electronic exchange of doseinformation between pharmacies. XML mes-sages have now been developed for this areaunder MedCom, so that both information onmedication which can be dose-dispensed andbilling information can be transferred electroni-cally between the pharmacies.
The messages were tested in the first quarterof 2003 in a pilot project between the various
The doctor sends a prescriptionto the pharmacy
The phar-macyreceives theprescriptionand issues adosage card
The pharmacy sends the dosage card to thedoctor following a request from the latter
The pharmacy sends the dosage card to thepacking pharmacy
The packing phar-macy sends anacknowledgement,confirmation oforder and bill tothe pharmacy
pharmacy systems currently used in those phar-macies that can dose-pack.
In connection with a planned review of theEDI prescription in the autumn of 2002, a wishwas expressed by the Dose Dispending Group for it to be possible to state on the prescriptionwhether it is desired that a drug is dose-dispensed.
Following an agreement with the DanishMedicines Agency this is now possible, and Med-Com has produced a new version of the EDI-FACT prescription with associated examples oftext and has sent it out to all relevant suppliers.
To support the work of IT suppliers on XML EDIFACT conversion, MedCom has developed a Web-based converter, available via www.medcom.dk or directly at the address http://web.health-telematics.dk/xmledi

MedCom IV – status, plans and projects32
Perspective
The XML EPR communication project and G-EPRIt has been decided that the development of EPR systems is
to be based on the national G-EPR, Basic structure for
Electronic Patient Record. G-EPR describes a common model
for documentation of the clinical work process and will
gradually be expanded to include detailed descriptions of
important areas of work, e.g. image diagnostics.
The development of G-EPR is expected to take place over
a prolonged period, as all the elements in the basic structure
are not yet ready.
A number of solutions partially based on G-EPR will therefore be put into use and developed gradually as
the individual elements in the main structure are completed and migration to a full EPR based on G-EPR takes
place.
All these systems and their variants should be assured of communication coherence and co-existence. It is
intended that this coherence is ensured by:
● MedCom IV’s XML EPR standards being assured of G-EPR compatibility in the development of XML-extended
standards, which in addition to the content of present-day elements are expanded to include G-EPR ele-
ments, as these are developed.
● G-EPR migration solutions incorporate communication solutions based on XML EPR.
The XML EPR communication project is therefore to be seen as part of a realistic option for communication
between EPR systems, which is based on a joint G-EPR structure.
Commentary
Digitisation supports quality and coherenceVagn Nielsen, Head of Department, Ministry of the Interior and Health,
Chairman of the MedCom Steering Group
With the startup of MedCom’s XML EPR communication project, the focus has been on the communication of
referrals, summaries, laboratory results etc. within the hospitals and between the hospitals.
The routine communication of these message types is quite extensive in the hospital sector, and it is there-
fore expected that the digitisation of this area will contribute to a major boost in the quality and coherence of
patient progressions.
I would like to emphasise the fundamental need for the project to be in agreement with the national
standardisation work (Basic structure for Electronic Patient Record) taking place under the National Board of
Health. Against this background, it is anticipated that the project will also boost the dissemination in the
hospital sector of electronic patient records based on G-EPR, Basic structure for Electronic Patient Record.

basis. Simple Internet lookupwill often be more appropriatefor such groups of personnelthan having to use the complexproduction systems concerneddirectly.
It is intended that every coun-ty/CHC chooses which EPRand/or PAS systems are to beimplemented in which imple-mentation periods, on the basisof what fits in best with thecounty/CHC’s own IT strategy.
The SUP project means thatextract programs are establishedfrom the PAS and EPR systemsof the county.
These extracts of patient dataare transferred via a nation-wideMedCom XML standard to anSUP database/browser, whichmakes it possible to gain accessto viewing selected record dataand patient information via a
The purpose of MedCom’s SUPproject is to provide access toviewing PAS and EPR patientrecords via a fairly general Inter-net browser – both within thecounty and across county bound-aries.
After the project has been car-ried out, it is expected that thecounty/CHC has put into effect:
● electronic SUP extracting ofpatient record data from alldepartments that use the ITsystems mentioned
● Internet access for relevanthealthcare professionals intheir own county and othercounties who have a legiti-mate need justified in health-care terms for the information
The project is intended to pro-vide access to viewing selectedpatient data in the PAS and EPRsystems of others – whether theseare used elsewhere in the samecounty or in other counties.
In addition, a major usergroup will be doctors and nurseswho are not users of the PASand/or EPR systems on a daily
fairly general Internet browser. The SUP database/browser
can either be established as acounty database or jointlybetween several counties.
All users with secure Internetaccess can gain access to an SUPdatabase in the same way asaccess is obtained to other web-sites on the Internet.
On the website, the user isasked for his password – and ifthe user is set up in the SUPdatabase, he can obtain an over-view of the extracts of the patientrecord contained in the databaseby searching on the patient’s civilregistry (cpr) number.
Continued browsing in anSUP record is illustrated belowand proceeds according to thesame principles as are normallyapplied on the Internet.
Use of the SUP browser is
MedCom’s SUP project
SUP – Standardised Extract of Patient Data
The hospitals and healthcare communication 33
SUP
Internet
browser
SUP
DB
Internet
server➡
MedCom
XML standard
SUP
extract program
The user chooses record D and obtains an overviewof the contents of the record.
The user chooses note overview – and reads a note.
PAS:
EPR

MedCom IV – status, plans and projects34
logged in the same way as theuse of other patient systems. Useis checked by the county’s securi-ty organisation in the same wayas the use of other IT systems –with the difference that access byexternal users also has to bechecked.
The closed HealthcareIntranetA closed, nation-wide Health-careIntranet (SundhedsIntranet)is being constructed in 2003 aspart of MedCom’s Internet strategy. The HealthcareIntranetis based on linking togetherexisting county intranets in set-ting up VPN connections to anation-wide node (the Health-careDIX – SundhedsDIX). Thenode is operated by UNI-C.
The communication of SUPextracts is expected to take placein the use of the nation-wideHealthcareIntranet in such a waythat
● SUP extracts from EPR andPAS systems are transferred tothe SUP database via theHealthcareIntranet.
● users who have access to SUPextracts from records on theSUP servers of others have tobe able to use PC installationsthat have installed VPNaccess to the secure Health-careInternet.
Timetable
Most counties in western Den-mark have decided to take partin MedCom’s SUP project.
The aim of the project is toprovide access to the EPR andPAS patient data of the countiesvia a general Internet browser.For this to be possible, regularextracts of patient data fromEPR and where appropriate PASsystems to the SUP system haveto be established.
The project is based on theexisting SUP project, which isbeing carried out by the countiesof Vejle, Viborg and Århus. Inthis project it is planned that aVersion 2 will be put into effectwith extracts of record data fromVejle County. The project isbased on an SUP database de-veloped by IBM and an SUPbrowser solution developed by B-
data. The project will be part ofthe Public Healthcare Portal.
The aim of MedCom’s projectis to expand the SUP solution toall the participating counties. Ithas not yet been clarifiedwhether the individual countiesin this context will put intoeffect their own SUP solutions orjoin forces on common develop-ment and operation.
With a view to speeding upcommissioning of the SUP system and minimising risk andcosts, it is expected that all theparticipating counties will joinforces for a common SUP solu-tion in a start-up period up tothe autumn of 2004. The start-up period is based on a solutioncurrently being put into practicein Vejle.
In this event, it is expectedthat:
● the SUP solutions of thecounties can be implementedwith access via the HealthcarePortal at the beginning ofMarch 2004.
● programming of SUP extractsystems from the counties’EPR and PAS systems canstart at the beginning ofDecember 2003.
● Vejle County puts into effectSUP extracts with access viathe Healthcare Portal in mid-November 2003.
● completed tender documentsare available for extract sup-pliers at the end of October2003.
● costs in the establishment andoperation of the commonsolution have been clarified inmid-September 2003.
The SUP project uses the closedHealthcareIntranet
HealthcareDIX
County Network
Vejle County
CountyNetwork

Project manager EPR system PAS system
North Jutland County Anne Marie FalchViborg County Ole Philip Hansen B-DataÅrhus County Hans Henrik Bøttger AAAVejle County Morten Hansen IBM + CSCSouth Jutland County Klaus Bo EPJi GS ÅbenRibe County Kim Østerbye Accure/NoraFunen County Dorthe Skou Lassen MediCare FPAS
Participants
With the exception ofRingkøbing, all countieswest of the Great Belt havedecided to take part inMedCom’s SUP project.
The hospitals and healthcare communication 35
Timetable for SUP start-up project
2003 2004
SUP Start-up project Aug Sep Oct Nov Dec Jan Feb Mar Apr Maj June July Aug Sep Oct Nov Dec
Counties’ attitude to SUP Start-up project 19Vejle SUP in operation via Healthcare PortalOverheads and organisation of
joint SUP solution 8Completed tender documents for
extract systems 30Bids received from suppliers 27Adjustment of existing SUP DB/BrowserExtract systems:
DevelopmentImplementation and mappingTesting
Dissemination: Users joiningDIX and SUP via portal
Improvements and possible invitation to tender

MedCom IV – status, plans and projects36
Work was also done in otherEuropean countries in the nine-ties on the development of EDI-based communication in thehealthcare sector – based on thesame technological foundation asin Denmark.
The UK, the Netherlands andthe Scandinavian countries havebeen working on large, EDI-based healthcare data networkssince the start of the nineties.Similar projects and nationalstrategies have seen the light ofday in all European countries inrecent years. No other countrieshave, however, achieved a level ofuse that comes close to that inDenmark. Co-operation organi-sations have also been establishedin IT within the healthcare sec-tor in other European countries– organisations that are more orless similar to MedCom. On theinitiative of the Swedish Care-Link, these organisations havebeen brought together in anorganisation known as ELO,which at present comprises:
Denmark:
MedCom.www.medcom.dk
Finland:
STAKES – Researchand development cen-
tre for the social and health-care area. The task of STAKES is to pro-mote welfare and health. Theobjective is for the whole Finnishpopulation to have equal accessto effective social and healthcareservices of high quality.www.stakes.fi
France:
EDISANTE – L’échangede données informatisé
dans la Santé. Web-basedexchange of healthcare data. Thisassociation of players in thehealthcare area works to developand promote use of the Internetto pass on healthcare data.www.edisante.org
Netherlands:
Nictiz – Nationaal ICTInstituut in de Zorg.
Nictiz is attached to the DutchMinistry of Health and is aimedat disseminating electronicpatient records and ensuring electronic communication in theDutch health service.www.nictiz.nl
Italy:
FIASO – FederazioneItaliana Aziende
Sanitarie e Ospedaliere. Association for healthcare andhospital operation in Italy. FIASO puts the citizen at thecentre in relation to the servicesthat can be obtained through thehealth service. www.fiaso.it
Norway:
KITH – Informasjons-teknologi for et bedre
helsevesen. Information techno-logy for a better health service.The principal aim of KITH is toensure that information and com-munication technology are usedto achieve effective and reason-able co-operation and develop-ment in the health service.www.kith.no
United Kingdom:
UkeHA – UK eHealth Association.
Electronic forum for healthcarecommunication in the UnitedKingdom. UkeHA represents allorganisations and individualswith an interest in the develop-ment of eHealth – electronichealthcare communication in theUnited Kingdom.www.ukeha.org.uk
Czech Republic:
Medtel. Medical Tele-matik is an independent
non-profit organisation whichaims to ensure electronic health-care communication in theCzech Republic and between theCzech Republic and other European countries. Medtel isfinanced by the Czech Ministryof Health. www.medtel.cz
Sweden:
Carelink – the Swedishnetwork for healthcare
communication. Carelink is anational co-operative body, theaim of which is to promote theuse of IT in the Swedish healthservice. www.carelink.se
Germany:
ATG – AktionsforumTelematik im Gesund-
heitswesen. Action forum forhealthcare telematics. The aim ofATG is to integrate telematics asan important tool in the healthservice for the development ofup-to-date treatment and care ofhigh quality. www.atg.gvg-koeln.de
International activities

Internationalinteraction
The Danish development worktook on an international dimen-sion as long ago as the earlynineties. The background was awish on the part of the Danes toenter into close co-operationwith related communication projects abroad in order to gainand provide inspiration. In brief,the intention was to achieve synergies in the interactionbetween these projects acrossnational boundaries.
Experience has shown that theeffort put into international co-operation was both correct andnecessary. There are countlessexamples of how experience froma national project has been ofbenefit at the international level
– and vice-versa. Ideas and ex-periences from similar projects invirtually every EU member statehave had a great impact on thesituation and the prospects forthe use of information and com-munication technology in theDanish health service. At thesame time, we find that the Danish development work hasalso left its mark in the way oth-er countries have chosen toexploit the potential of the newtechnology.
Internationalprojects 1996-1999
CoCoCoordination and Continuity inHealth Care was the main heading of the CoCo project,which brought together 11regional project organisations in10 countries.
The majority of the projectsfocused on the communicationto and from the GP, in the formof written messages – prescrip-tions, referrals, discharge letters,requests etc. However, CoCoalso covered projects relating tomultimedia communicationbetween the primary and sec-ondary sectors.
The building-blocks in CoCowere the regional projects. CoCopassed on standards, guidelines,test systems and other services tothe regions. Communication wascarried out and tested in pilotprojects. The pilot projectsemphasised that the regional net-works could be slightly differentwith regard to size and aim, butthat they should be built up onthe basis of the same standardsand the same structure.
PRIMACOM
PRIMACOM – PRIMAry CarePhysicians COMmunicationNetwork carried out and evaluat-ed pilot projects in Hungary andSlovenia with western Europeanco-operating partners. This workcomprised:
● development of the necessarytools and guidelines
● establishment of contactbetween software firms inDenmark, Italy, Hungary andSlovenia
● electronic contact betweenhealthcare professionals
● communication of structuredmessages to ensure re-use ofdata in different systems,which are based on Europeanstandards, existing infrastruc-ture and regional systems
WISE
13 organisations in 10 EU mem-ber states joined forces in theWISE co-operation – Workingin Synergy for Europe – toexchange knowledge and experi-ence in efforts to establish andexpand regional healthcare datanetworks in Europe. WISE was akind of umbrella for EU projectsconcerned with regional health-care data networks, includingCoCo. The idea behind WISEwas to view the regional andnational effort in healthcarecommunication in an inter-national perspective and broadenexperience and solutions at European level. WISE focusedon User Group Support, SynergyPromotion and External Promo-tion. One of the results of theproject was the book “BuildingRegional Health Care Networksin Europe”, published by IOSPress.
Websites
MedCom:
www.medcom.dk
CoCo:
www.medcom.dk/dansk/coco
PrimaCom:
www.primacom.dk
Picnic:
www.medcom.dk/picnic
JUST:
www.justweb.org
ciTTis:
www.cittis.dk
Open ECG:
www.openecg.net
HC-INTEREST:
www.hc-interest.dk
International activities 37

MedCom IV – status, plans and projects38
Internationalprojects 2000-2002
PropractitionThe Propractition project focuseson the continuing training ofhealthcare professionals using theInternet and websites. The objec-tive of Propractition is to teachdoctors to co-operate, so thattwo doctors each in their ownhospital, for example, can reachagreement on diagnosis andtreatment in difficult cases.
PICNIC
PICNIC – Professionals and Citizens Network for IntegratedCare. The EU project involvesregional system suppliers, tech-nology centres, companies anduniversities in nine EU memberstates.
The objective of PICNIC isto support/assist the regional sys-tem suppliers in implementingthe next generation of secure,user-friendly healthcare data net-works and to bring together theEuropean market for healthcaretelematics services.
PICNIC provides/offersOpen Source components forWeb services for the healthcaredata network and a structure forlocal healthcare data networks.Components have been imple-
mented in the pilot projects thatoffer
● telemedicine collaborationservices
● shared record services● reimbursement services
JUST
Fifteen partners from sevencountries are taking part in theJUST project. JUST supplies ITsupport for training in action tobe taken in the event of acci-dents, among other things in theform of a CD with an interactivemultimedia course and a website.Both aim to teach volunteershow they can help when theyencounter cardiac arrest, an asthma attack or a person who isunconscious. The contents of the
Commentary
A development of national as well as international significance Commentary by Ilias Iakovidis, Ph.D., Deputy Head of Unit-eHealth,
European Commission, DG Information Society
Within the vast working area of eHealth, which focuses on application of
information and communication technology, the fast and reliable commu-
nication of vital health data has a high priority. Electronic communication
is the cornerstone of effective and quality health services and is highly
advantageous not only to professionals but certainly also to the patients.
The EU is supporting initiatives in this field during the last 15 years and
has in different ways supported a cross border co-operation on eHealth
applications with the ultimate objective of supporting citizen centred
health care.
MedCom, the Danish health data net, has consistently participated in the international co-operation and has
contributed to the exchange of experience and inspiration. At the same time, MedCom has managed to initiate
a development of the Danish health data net, which has been recognised with honourable mention as the
“best practice” example in the recent eHealth 2003 Ministerial Conference.
MedCom and the Danish health data net have acquired valuable experiences that should play part in the
development of future eHealth systems and services not only in Denmark but also to serve as example to all the
countries that are preparing their deployment strategies. The European Commission follows new MedCom
projects with great interest and it is very gratifying that the Research and Development programmes of EU is
part of the success of MedCom.

CD comply with internationalrecommendations and are usedby several European organisa-tions in conjunction with first-aid courses for volunteers.
Internationalprojects 2002-2004
ciTTisThe aim of this INTERRREGproject is to develop a structurethat can bring together all formsof telemedicine solutions, so thatthey can be used in the collabo-ration between healthcare profes-sionals across all forms of tele-medicine solutions. Co-operationin telemedicine involves the useof a protocol which shows thedata stream in connection withthe co-operation between health-care professionals. The clinicaldocuments and images are trans-ferred by means of Europeanstandards.
A large part of the INTER-REG project will focus on theorganisational changes that fol-low when it is possible for co-operation to take place acrossorganisational and geographicalboundaries. The project willdevelop guidelines on how bestto implement the new IT co-operation service.
The IT co-operation service isan environment where it is possi-ble to carry out examination,monitoring, treatment andadministration of patients usingdirect access to expert knowledgeand patient information, regard-less where the patient or the relevant information is in purelygeographical terms.
OpenECG
OpenECG aims to increaseknowledge of and disseminatethe use of the electronic ECGstandards. OpenECG bringstogether representatives fromnational cardiology centres, hos-pital directors and producers ofand dealers in ECG equipment.
An open ECG portal will helpproducers and system integratorsin creating equipment and soft-ware which together can ensuresmooth exchange of electrocar-diograms. System managers andusers can find the necessaryinformation to draw up suitableand clear specifications in con-nection with the purchasing ofnew IT systems via the portal.
HC-INTEREST
The Nordic project HC-INTEREST – Health Carerecord INTEroperability andRecord STructure – has createdthe basis for Electronic HealthCare Records (EHR), which canbe used in all the Nordic coun-tries. The objective is to exchangeand consequently re-use informa-tion in different EHR systems.
The project is based on Euro-pean standards for EHR modelsand messages and combines thesewith national enhancements, sothat models and messages suitNordic needs. Medical treatmentwas used as a test area on thebasis of the Danish NationalBoard of Health model. TheHC-INTEREST project has
● produced proposals for thebasic elements of a har-monised EHR structure
● developed operational EHRmessages on the basis of theproposed basic elements in thestructure and terminologicalstandards
International activities 39
● tested the EHR messages in apilot project where medicalmessages were generated/com-bined on the basis of the basicelements and the models
Nordic co-operation
In 2001, Nordic co-operationwas initiated between organisa-tions working on healthcare datanetworks at national level. KITHfrom Norway, CareLink fromSweden, STAKES from Finland,the Icelandic Ministry of Healthand MedCom have since mettwice a year.
The aim is to develop experi-ence and establish projects acrossboundaries. In several casesknowledge of communicationsolutions or the infrastructure inhealthcare data networks hasbeen re-used in another Nordiccountry.

MedCom IV – status, plans and projects40
Perspective
Nordic Health care Network groupSince the beginning of 2000, there has been ever closer co-operation between the organisations in the five
Nordic countries which are working on the application and implementation of IT solutions and electronic
communication in the health service.
Norway, Sweden and Denmark are all involved in the work of establishing nation-wide closed IP-based
healthcare data networks. This firstly led to a number of bilateral meetings, exchange of documents and
experience, to the great satisfaction of all the participants.
Plans for IP-based healthcare data networks became reality in the spring of 2003.
In Sweden, the Swedish Sjunet network has already gone through its second tendering round, and is a well-
established network in which all the county councils (landsting) take part.
In Norway, five regional networks have been set up following the re-organisation of the healthcare sector
into five regions, and it is planned that these networks will be linked together.
In Denmark, MedCom is well under way with a large-scale pilot project in which all the counties, pharma-
cies, Copenhagen Local Authority, a number of GPs and other parties are connected to a closed network.
Broadly speaking, Norway has focused on developing telemedicine, Sweden on establishing a secure IP-
based infrastructure and Denmark has developed and implemented EDIFACT communication on a large scale.
Against this backdrop, the first meeting of the Nordic Health care Network was held in conjunction with
the Vitalis conference in Gothenburg on 4 March. It was decided at the meeting to form a permanent Nordic
working group and make the group a sub-group of NTA.
Aims of the Nordic Health care Network
The establishment of the Nordic Health care Network serves several purposes, but overall the network is
intended to foster greater exchange of experience and ideas between the Nordic countries. Experience to date
has shown that there are great similarities and interesting differences between the structure of the health
service, the use of IT and the development and implementation of IT in the health service in the Nordic coun-
tries. The aim of the Nordic Health care Network is to utilise these similarities and differences to:
● ensure the greatest possible re-use of solutions across national and regional boundaries in the Nordic
countries
● assist in creating an open and homogeneous Nordic market for IT solutions for the health service
● create contact and the possibility of exchange of experience between national and regional projects
● inform broadly about Nordic solutions and projects
● support the development of a Nordic market for healthcare services
● solve practical problems in connection with healthcare projects in the Nordic countries
Published in December 2003 by MedCom, Rugårdsvej 15, 2., 5000 Odense C. Editor: Lars Hulbæk, MedCom. Text: arki•tekst kommunikation. Layout/dtp: Christen Tofte. Printed in Denmark by: one2one. Print run: 1000. ISBN: 87-90839-67-6
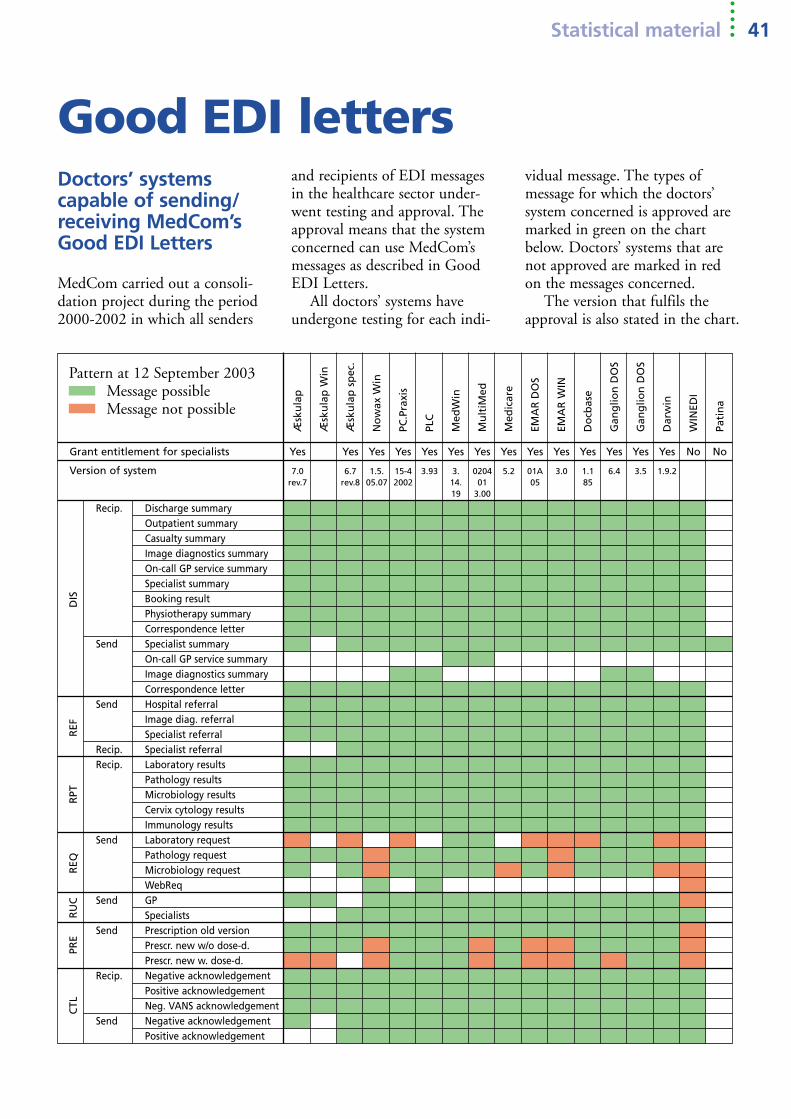
Æsk
ula
p
Æsk
ula
p W
in
Æsk
ula
p s
pec
.
No
wax
Win
PC.P
raxi
s
PLC
Med
Win
Mu
ltiM
ed
Med
icar
e
EMA
RD
OS
EMA
R W
IN
Do
cbas
e
Gan
glio
n D
OS
Gan
glio
n D
OS
Dar
win
WIN
EDI
Pati
na
Statistical material 41
Good EDI lettersDoctors’ systems capable of sending/receiving MedCom’sGood EDI Letters
MedCom carried out a consoli-dation project during the period2000-2002 in which all senders
and recipients of EDI messagesin the healthcare sector under-went testing and approval. Theapproval means that the systemconcerned can use MedCom’smessages as described in GoodEDI Letters.
All doctors’ systems haveundergone testing for each indi-
vidual message. The types of message for which the doctors’ system concerned is approved aremarked in green on the chartbelow. Doctors’ systems that arenot approved are marked in red on the messages concerned.
The version that fulfils theapproval is also stated in the chart.
DIS
REF
RPT
REQ
RU
CPR
EC
TL
Pattern at 12 September 2003Message possibleMessage not possible
Grant entitlement for specialists Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes No No
Version of system 7.0 6.7 1.5. 15-4 3.93 3. 0204 5.2 01A 3.0 1.1 6.4 3.5 1.9.2rev.7 rev.8 05.07 2002 14. 01 05 85
19 3.00
Recip. Discharge summaryOutpatient summaryCasualty summaryImage diagnostics summaryOn-call GP service summarySpecialist summaryBooking resultPhysiotherapy summaryCorrespondence letter
Send Specialist summaryOn-call GP service summaryImage diagnostics summaryCorrespondence letter
Send Hospital referralImage diag. referralSpecialist referral
Recip. Specialist referralRecip. Laboratory results
Pathology resultsMicrobiology resultsCervix cytology resultsImmunology results
Send Laboratory requestPathology requestMicrobiology requestWebReq
Send GPSpecialists
Send Prescription old versionPrescr. new w/o dose-d.Prescr. new w. dose-d.
Recip. Negative acknowledgementPositive acknowledgementNeg. VANS acknowledgement
Send Negative acknowledgementPositive acknowledgement

MedCom IV – status, plans and projects42
Overview of EDIFACT messages in operation in the individual counties and CHC
Green indicates that themessages are underway andhave been disseminated tomore than 50% of possiblemessages. The numbers inthe boxes indicate whatpercentage of messages aresent electronically.
Yellow indicates that themessage has been startedand is being disseminated.
Red indicates that the message has not yet beenput into use.
No
rth
Ju
tlan
d
Vib
org
Årh
us
Rin
gkø
bin
g
Rib
e
Vej
le
Sou
th J
utl
and
Fun
en
Wes
t Ze
alan
d
Sto
rstr
øm
Ro
skild
e
Fred
erik
sbo
rg
CH
C
Co
pen
hag
en
Bo
rnh
olm
KPL
L
SSI
Cap
io
What can the counties do now?
Positionat 19 September 2003
Counties Lab.
EDI-doctors % 94 92 91 82 87 96 98 89 92 86 88 90 81 79 89Spec. H doctors % 65 78 50 72 42 67 81 69 70 60 51 64 53 52 80
3 Discharge summary 94 92 91 82 65 96 98 89 92 86 88 90 81 79 894 Outpatient summary 94 92 91 82 65 96 98 89 92 40 88 10 5 0 895 Casualty summary 94 92 91 82 0 96 98 89 92 86 88 90 51 20 896 Image-diagnostics summary 94 92 20 82 87 96 98 89 92 86 88 0 70 0 89
16 On-call GP service summary 94 92 91 82 87 96 98 89 92 86 88 90 81 79 8943 Specialist summary 52 66 38 30 65 55 70 55 52 45 41 46 41 40 6850 Physiotherapy summary 12 13 15 18 15 17 25 15 12 12 13 14 12 13 1649 Booking result 51 60 5 0 0 50 0 60 25 20 25 0 0 0 0
1 Admission referral 65 26 0 70 65 51 74 59 20 51 6 0 5 0 07 Image-diagnostics referral 65 65 10 51 74 59 22 51 0 0 0 0 70 0 0
44 Specialist referral 6 25 10 8 5 5 5 4 10 4 1 3 1 1 3
9 Clinical chemistry results 94 92 91 60 87 96 98 89 92 86 88 90 80 79 8911 Pathology results 94 92 91 82 87 96 98 89 92 86 88 90 80 79 8913 Clinical microbiology results 94 92 91 82 87 96 98 89 92 86 88 0 80 79 89 5554 Clinical immunology results 94 92 0 78 87 96 0 89 0 86 88 0 0 0 0 0
8 Clinical chemistry request 0 2 0 0 0 0 0 0 0 0 0 0 0 0 010 Pathology request 0 32 0 0 0 63 0 54 0 0 10 45 0 0 012 Clinical microbiology request 0 32 0 0 0 0 0 0 0 0 0 0 0 0 0 0
14 GP billing 54 73 20 52 43 75 71 50 70 20 55 71 48 45 014 Specialist billing 39 43 13 33 21 25 58 25 50 26 24 27 21 36 015 Pharmacy billing 100 100 70 100 36 74 100 85 88 79 100 100 86 55 048 Dentist billing 12 4 6 15 12 27 9 32 18 1 22 30 17 27 047 On-call GP service billing 100 100 100 100 100 100 100 100 100 100 100 100 100 10053 Physiotherapist billing 10 2 30 4 8 9 13 10 40 4 25 14 46 42 0SSI billing 100 100 0 100 100 100 100 100 100 100 100 100 100 100 0 88MediLab billing 100 100 100 100 100 100 100 100 100 100 100 100 0 94KPLL billing 100 100 100 100 100
25 GP prescription 80 82 68 59 64 75 77 70 66 61 60 54 37 43 8417 On-call service prescription 90 90 90 90 90 90 90 90 90 90 90 90 90 90 90

Staff 43
Centre manager Henrik BjerregaardJensenMedComMobile +45 4036 [email protected]
Deputy Manager Ib JohansenMedComMobile +45 4036 [email protected]
Secretary Anita [email protected]
Consultant Claus Duedal Pedersen MedComMobile +45 4036 8629 [email protected]
Project assistant Gitte HenriksenMedComMobile +45 2342 [email protected]
Secretary Iben Søgaard [email protected]
ConsultantJens Rahbek Nørgaard MedcomMobile +45 2482 [email protected]
Centre for Health Telematics
Consultant Lars HulbækMedComMobile +45 4036 [email protected]
SecretaryPia Reinhardt Juel MedcomMobile +45 2066 8700 [email protected]
Secretary Annette Larsen [email protected]
Consultant Dorthe Skou Lassen MedCom/FynComMobile +45 4040 [email protected]
Consultant Karin Demkjær MedCom/FynComMobile +45 2320 [email protected]
Secretary Karina HasagerFynComMobile +45 2612 0361 [email protected]
Consultant Lisbeth Jørgensen FynComMobile +45 2427 [email protected]
Deputy Chief of Section Tove Lehrmann FynComMobile +45 4036 8618 [email protected]
Consultant Henning Voss InternationalMobile +45 3034 [email protected]
Secretary Jennie Søderberg InternationalMobile +45 4026 6308 [email protected]
Consultant Niels Rossing InternationalMobile +45 2178 [email protected]
Consultant Tove Kaae InternationalMobile +45 2427 5739 [email protected]
Building assistant Alis JørgensenThe CentreMobile +45 5131 8566

MedCom IV – status, plans and projects
MedCom IV projects
➊ Infrastructure project
➋ Web lookup, laboratory
➌ Web requesting
➍ Web lookup, X-rays
➎ Teledermatology
➏ Hospital-local authority
➐ LÆ forms
➑ XML EPR
➒ SUP
● Local authorities
FUNEN COUNTY
Rugårdsvej 15, 2.sal, 5000 Odense C
Telephone +45 6613 3066, Fax +45 6613 5066
www.medcom.dk
Ministry of the Interior and Health
Slotsholmsgade 10-12, 1216 Copenhagen K
Telephone +45 3392 3360, Fax +45 3393 1563
➊
➊➍➏➏➏
➊➎➏ ➏➏ Cph. County
➊➎ CHC
➊➐ Cph. Local authority
➊➋➌ KPLL
➊➏➏➏
➊➍➎
➊➋➏
➊➋➍➎➏➑➒ ➏➏➐
➊➑➒
➊➋➌➍➑➒ ➐
➊➌➑➒
➊➌➎➑➒ ➐
➊➎
➊➋➌➎➑➒
➊➏➑➒ ➏➐