mechanical vs. manual cpr for cardiac arrest in adult patients linda hume lock haven university pa...
TRANSCRIPT

Mechanical vs. Manual CPR for Cardiac Arrest in Adult Patients
Linda Hume
Lock Haven University PA Program
February 25, 2009
http://www.zoll.com/uploadedImages/Common_Resources/AutoPulse_2007_motionV1-e3.jpg

PICO Question
• Patient: Cardiac arrest patients 18 years of age and older who are brought to the ER
• Intervention: Mechanically delivered CPR• Comparison: Manually delivered CPR• Outcome: Survival to hospital hospital admission
Question:In cardiac arrest patients 18 years of age and older who are brought to the ER, does mechanically delivered CPR offer an advantage over manual CPR in survival to hospital admission?

Cardiac Arrest• About 350,000 sudden cardiac
arrest deaths occur in the United States each year (Cooper et al, 2006, p 2839)
• This represents over 1/3 of all deaths in the country) (Ong et al, 2006, p 2629)
• CPR was introduced in 1969 (Gaxiola and Varon, 2008, p 923)
• Between 225,000 and 700,000 people receive CPR each year (Gaxiola and Varon, 2008, p 923)
• Initial rhythm in 40% of out-of-hospital arrests is ventricular fibrillation – a treatable/“shockable” rhythm (American Heart, 2005, p IV-19)
http://www.caregiver-helpline.com/images/chart.jpg
http://www.aedhq.com/files/images/causeOfDeath.gif

Risks for a Poor Outcome
• Unwitnessed collapse• Older patient age• Long EMS response time
– Studies vary between 6.6 and 8 minutes (Hallstrom et al, 2006, p 2626) (Ong et al, 2006, p 2636)
– Most communities have a response time of 7-8 minutes (American Heart, 2005, IV-19)
• Nonpublic location• Initial rhythm of asystole or
pulseless electrical activity(Hallstrom et al, 2006, p 2625)
http://www.cartoonstock.com/newscartoons/cartoonists/mba/lowres/mban752l.jpg

Surviving Arrest• Early defibrillation is key to
survival of cardiac arrest– Important to maintain
circulation while waiting for defibrillation to be available and appropriate for use
– Studies have indicated that defibrillation within 3 minutes of cardiac arrest results in a 74% increase in chances of survival
(Cooper et al, 2006, p 2847) http://entertainment.webshots.com/photo/2060520010102272392olryWh

•Each minute of cardiac arrest without CPR equates to a 7-10% decrease in chances of return of spontaneous circulation (ROSC) (Cooper et al, 2006, p 2846)
Importance of CPR
http://www.wakegov.com/NR/rdonlyres/D7D7B8D1-535C-4418-81D5-90832981D372/1247/chart.gif

CPR• CPR consists of a compression (ejection) phase and a decompression
(refilling) phase (Gaxiola and Varon, 2008, p 924)
• Goal of providing CPR is to increase time a patient is in a “shockable” rhythm until defibrillation is available (American Heart, 2005, p IV-19)
– Also provides perfusion to the brain, coronary arteries, and lungs, allowing O2 transport in the body
• Each minute that CPR is provided following a witnessed collapse, chances of ROSC decline 3-4% per minute (compared to 7-10% without CPR) (American Heart, 2005, p IV-19)
• Coronary Perfusion Pressure is another important determinant in ROSC– A CPP of at least 15 mmHg is necessary for ROSC to occur (Australian Government, 2008, p 2)
– Levels over 40 mmHg are associated with diminished outcome (Gaxiola and Varon, 2008, p 927)
• Current gold standard therapy is manually delivered CPR

Flowchart for CPR (Updated 2005):
http://circ.ahajournals.org/cgi/content-nw/full/112/24_suppl/IV-19/FIG2

Cons of Manual CPR• Chest compressions are interrupted due to provider
fatigue, patient transport, and “hands off” time for defibrillation (Hallstrom et al, 2006, p 2621)
• Manual chest compressions are dangerous for EMS providers in the back of moving vehicles (Zoll, 2006)
• Chest compressions are often not delivered at an appropriate depth– Typically only 14 mmHg of CPP is provided (Ong et al, 2006, 2634)
• Standard CPR provides only ~13% of normal CPP (Ong et al, 2006, p 2635)
• Failure to allow full chest re-expansion (decompression)
• Providers must keep track of both compression counts and respiration counts

Common Errors in Resuscitation
• Failure to recognize arrest• Failure to act rationally• Failure to anticipate the next move• Failure to remain calm and focused• Failure to keep skills current• Failure to provide effective compressions• Failure to provide effective ventilations• Failure to know and locate necessary equipment• Failure to debrief or problem solve after a code(Strzyzewski, 2006, p 10-14)
http://cardiophile.com/wp-content/uploads/2008/01/heart-in-hands.jpg

Mechanical CPR Devices
• Shortly after the introduction of CPR, interest arose in the development of mechanical devices that could decrease exhaustion associated with performing CPR, and control consistency of depth and force of compressions
• First machine was developed by Bramson: it used compressed gas to drive a spring loaded piston with a force of 60-75 lbs onto the patient’s sternum
(Gaxiola and Varon, 2008, p 923-924)

Cooper et al, 2006, p 2846

AutoPulse/LifeBelt CPR
• Developed in 2000 by Zoll, the AutoPulse has been on the market for 4 years, and approved for use in PA for 2 years (Zoll, 2006)
• Provides compression of sternum and lateral walls of thorax– Provides better blood flow – “forward flow” (Cooper at al, 2006, p 2645)
– Generates 36% of normal blood flow, and a CPP of 20 mmHg (Gaxiola and Varon, 2008, p 928)
• Provides a consistent depth of compressions over a larger area of the chest
• Delivers the correct frequency of chest compressions• Not interrupted by transport or defibrillation• Not compromised by provider exhaustion
Cooper et al, 2006, p 2846

ACDR/ACDC• Hand-held device with a suction cup to provide
compressions and active decompressions (Lafuente-Lafuente and Melero-Bascones, 2008, p 1)
– Increases intrathoracic flow during decompression to allow for a greater volume of blood flow with next compression
• Developed after anecdotal evidence of successful resuscitation using a toilet plunger (Cooper et al, 2006, p 2845)
• Pressure gauge in device provides compression and decompression force feedback for user to alter effort (Lafuente-Lafuente and Melero-Bascones, 2008, p 3)
• Many different models of this device have been developed by different manufacturers– Models involving pneumatically delivered compressions are
available in hospitals, however these are not practical for out-of-hospital use
http://digital-infiniti.com/images/Large%20Size%20Sink%20Plunger.jpg
Cooper et al, 2006, p 2846

Manual CPR vs. Mechanical CPRStudies
http://www.salem-news.com/stimg/april072008/cpr-2.jpg
http://www.enquirer.com/editions/2004/09/01/autopulse.jpg

Manual Chest Compression vs. Use of an Automated Chest Compression Device
Following Out-of-Hospital Cardiac Arrest
• 2006 randomized trial by Hallstrom et al• Conducted in Calgary, Alberta; Columbus, OH; Pittsburgh,
PA; Seattle, WA; and Vancouver, BC• 1,377 patients were involved in the study• Initial improvement in survival of patients who received the
mechanical CPR device 4 hours after 911 call– Indicates increased survival rate to hospital admission– Not a statistically significant improvement 24.7% (manual) vs.
26.4% (mechanical)
(Hallstrom et al, 2006, p 2620-2627)

Manual Chest Compression vs. Use of an Automated Chest Compression Device
Following Out-of-Hospital Cardiac Arrest• No significant improvement to hospital discharge was seen
• Cannot be explained: all research prior to conducting the trial indicated an improvement was to be expected
• Explanations offered for this outcome include:
– Increased time to machine application due to set up
– Application of the machine to candidates in whom manual CPR would not be considered
– A synergistic effect of the machine with medications
– Attributed to difference in study protocol at one site that was associated with most of the adverse outcomes associated with the AutoPulse
(Hallstrom et al, 2006, p 2620-2627)

Use of an Automated, Load-Distributing Band Chest Compression Device for Out-of-
Hospital Cardiac Arrest Resuscitation
• 2006 study conducted by Ong et al• Conducted in Richmond, VA• 1,067 patients involved in the study• An improvement in survival to hospital admission was seen
in patients who had the automatic CPR device applied– 11.1% (manual) vs. 20.9% (mechanical)
• Mechanical CPR provided higher intrathoracic pressures than were safely possible with manual CPR
(Ong et al, 2006, p 2629-2636)
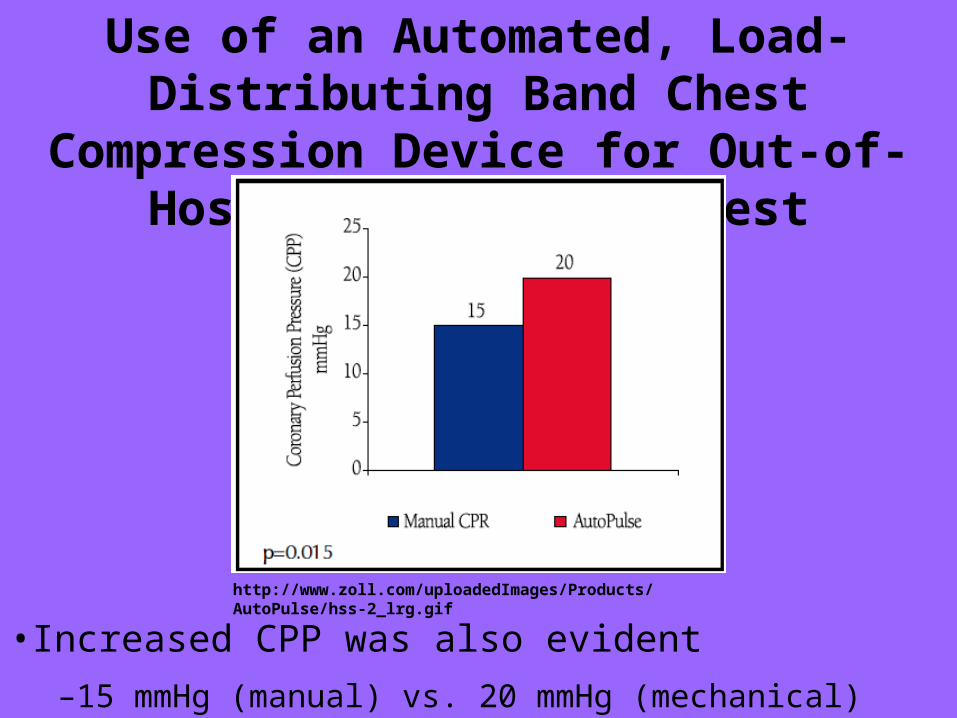
Use of an Automated, Load-Distributing Band Chest Compression Device for Out-of-
Hospital Cardiac Arrest Resuscitation
•Increased CPP was also evident
–15 mmHg (manual) vs. 20 mmHg (mechanical)
http://www.zoll.com/uploadedImages/Products/AutoPulse/hss-2_lrg.gif

Use of an Automated, Load-Distributing Band Chest Compression Device for Out-of-
Hospital Cardiac Arrest Resuscitation
• Greater percentage of coronary and cerebral flow was evident
– When combined with medications, patients were provided normal heart and brain flow levels and pressures
http://www.zoll.com/uploadedImages/Products/AutoPulse/ahs-1_lrg.gif

Use of an Automated, Load-Distributing Band Chest Compression Device for Out-of-
Hospital Cardiac Arrest Resuscitation
• Greater survival to hospital discharge– 2.9% manual CPR, 9.7% mechanical CPR
http://www.zoll.com/uploadedImages/Products/AutoPulse/AutoPulsesurvivalgraph.jpg

Out-of-Hospital Cardiopulmonary Resuscitation with the AutoPulse
• 2007 study conducted by Krep et al involving 46 patients• Studied the safety, effectiveness, and practicability of the
AutoPulse machine• The results demonstrate that the AutoPulse is:
– Effective in providing adequate compressions• Determined by end-tidal CO2 volumes which correlate with cardiac output
– Safe for patients in cardiac arrest• No severe compression injuries were seen (rupture of liver, rib fracture)• Only injury noted was mild abrasions over the lateral chest area
– Practical for use in cardiac arrest situations• In 2/3 of the applications, set up was performed within 2 minutes• Lightweight design makes the AutoPulse easy to carry to the patient• AutoPulse is the same shape as a backboard and fits easily on a cot for patient
transfer, or can be used for transfer itself
(Krep et al, 2007, p 86-94)

Active Compression-Decompression for Cardiopulmonary Resuscitation
• 2008 Cochrane review• Evaluated ten trials which used the ACDR method of
resuscitation, eight were conducted in out-of-hospital settings
• Out-of-hospital trials involved a total of 4,162 patients• No differences were found in the group who had the ACDR
device applied when compared with those who received manual CPR in survival of arrest or complications from resuscitation
• Authors concluded that ACDR resuscitation is not associated with a clear benefit during resuscitation
(Lafuente-Lafuente and Melero-Bascones, 2008, p 1-4)

Active Compression-Decompression for Cardiopulmonary Resuscitation
• Many of the benefits associated with a device such as the AutoPulse were not provided by ACDR devices– Not a true mechanical device – requires constant manual
manipulation to operate• Also requires more training than standard manual CPR
– Consistency of depth of compressions is regulated by provider alteration of effort
– Frequency of compressions are not regulated– Does not allow for constant compressions during transport– Requires interruptions for defibrillation– Increase in provider fatigue
• Requires greater physical effort
(Lafuente-Lafuente and Melero-Bascones, 2008, p 1-4)
Summary of Studies• Use of ACDR in the out-of-hospital field is not true
mechanical CPR and is associated with no improvement in survival to hospital admission (Lafuente-
Lafuente and Melero-Bascones, 2008, p 2)
• The use of an automated CPR device such as the AutoPulse is associated with an increase in survival to hospital admission (Hallstrom et al, 2006, p 2625) and (Ong et al, 2006, p 2633)
– Hallstrom et al: 26.4% vs. 24.7%– Ong et al: 20.9% vs. 11.1%
• The AutoPulse is also safe, effective, and practical for use in out-of-hospital cardiac arrests (Krep et al, 2007, p 86)

Benefits of Mechanical CPR• Consistent compression rate• Consistent compression depth• Increase in CPP• Increase in coronary and cerebral blood flow• Continuous CPR during transport and defibrillation• Use of a mechanical CPR device also allows EMS providers to
concentrate on other aspects of resuscitation such as defibrillation and respirations
• Mechanical CPR devices allow EMS providers to remain seated during patient transport which results in fewer injuries to EMS workers and less use of the hospital
(Zoll, 2006)

Application of Findings• Use of mechanical CPR devices allows for better patient
care and outcomes following cardiac arrest• Allotting money for the future purchase of the AutoPulse
should be considered in all EMS agencies– $15,000 - $17,000 per unit (Zoll, 2006)
• Ong et al also found that patients who received field CPR while waiting for application of the AutoPulse had a 16 fold increase in survival over those who do not (p 2636)
– All patients should receive manual CPR while waiting for application of the AutoPulse
– Defibrillation should be administered as soon as it is available and appropriate

ReferencesAmerican Heart Association. (2005). 2005 American Heart Association Guidelines for Cardiopulmonary
Resuscitation and Emergency Cardiovascular Care. Circulation: Journal of the American Heart Association, 112(24), IV 19 – IV 34. Retrieved February 11, 2009 from http://circ.ahajournals.org/content/vol112/24_suppl/#_____AMERICAN_HEART_ASSOCIATION_GUIDELINES_FOR_CARDIOPULMONARY_RESUSCITATION_AND_EMERGENCY_CARDIOVASCULAR_CARE.
Australian Government Department of Health and Aging. (2008). Horizon Scanning Technology Prioritising
Summary: Autopulse Automated Compression Device for CPR. Australia and New Zealand Horizon Scanning Network. Retrieved January 11, 2009 from http://www.horizonscanning.gov.au/internet/horizon/publishing.nsf/Content/prioritising-summaries-2008-2.
Bobrow, B.J., Clark, L.L., Ewy, G.A., et al. (2008). Minimally Interrupted Cardiac Resuscitation by Emergency
Medical Services for Out-of-Hospital Cardiac Arrest. The Journal of the American Medical Association, 299(10). 1158-1165. Retrieved January 18, 2009 from www.EBSCOhost.com.
Cooper, J.A., Cooper, J.D., Cooper, J.M. (2006). Cardiopulmonary Resuscitation: History, Current Practice, and
Future Direction. Circulation: Journal of the American Heart Association, 114, 2839-2849. Retrieved January 18, 2009 from http://circ.ahajournals.org/cgi/reprint/114/25/2839.
Ewy, G.A. (2007). Continuous-Chest-Compression Cardiopulmonary Resuscitation for Cardiac Arrest.
Circulation: Journal of the American Heart Association, 116. 2894-2896. Retrieved January 18, 2009 from http://circ.ahajournals.org/cgi/content/full/116/25/2894.
Gaxiola, A., Varon, J. (2008). Evolution and New Perspective of Chest Compression Mechanical Devices.
American Journal of Emergency Medicine, 26, 923-931. Retrieved January 11, 2009 from www.mdconsult.com.

Hallstrom, A., Rea, T.D., Sayre, M.R., et al. (2006). Manual Chest Compression vs. Use of an Automated Chest Compression Device During Resuscitation Following Out-of-Hospital Cardiac Arrest: A Randomized Trial. The Journal of the American Medical Association, 295(22), 2620-2628. Retrieved January 11, 2009 from www.EBSCOhost.com.
Krep, H., Mamier, M., Breil, M., et al. (2007). Out-of-Hospital Cardiopulmonary Resuscitation with the
AutoPulse System: A Prospective Observational Study With a New Load-Distributing Band Chest Compression Device. Resuscitation, 73, 86-95. Retrieved February 11, 2009 from http://www.zoll.com/uploadedFiles/Products/AutoPulse/Krep%20AutoPulse%20Resuscitation.pdf.
Lafuente-Lafuente, C., Melero-Bascones, M. (2008). Active chest compression-decompression for
cardiopulmonary resuscitation (Review). The Cochrane Collaboration, John Wiley and Sons. Retrieved January 11, 2009 from http://www.mrw.interscience.wiley.com.navigator-lhup.passhe.edu/cochrane/clsysrev/articles/CD002751/pdf_fs.html.
Ong, M.E.H., Ornato, J.P., Edwards, D.P., et al. (2008). Use of an Automated, Load-Distributing Band Chest
Compression Device for Out-of-Hospital Cardiac Arrest Resuscitation. The Journal of the American Medical Association, 295(22). 2629-2637. Retrieved January 11, 2009 from www.EBSCOhost.com.
Steen, P.A. (2005). The Future of CPR. Acta Anaesthesiologica Scandinavica, 49(7). 909-912. Retrieved
January 11, 2009 from www.EBSCOhost.com. Strzyzewski, N. (2006). Common Errors Made in Resuscitation of respiratory and Cardiac Arrest. Plastic
Surgical Nursing, January-March 2006, 26(1). 10-16. Retrieved January 11, 2009 from www.EBSCOhost.com.
Zoll. (2006). Autopulse: Consistent Compressions. No Interruptions. Zoll Medical Corporation. Buyers
Information Packet. Chelmsford, MA.

Picture Creditshttp://www.zoll.com/uploadedImages/Common_Resources/AutoPulse_2007_motionV1-e3.jpg
http://digital-infiniti.com/images/Large%20Size%20Sink%20Plunger.jpg
http://www.btvfc.org/autopulse.jpg
http://www.wakegov.com/NR/rdonlyres/D7D7B8D1-535C-4418-81D5-90832981D372/1247/chart.gif
http://www.aedhq.com/files/images/causeOfDeath.gif
http://www.caregiver-helpline.com/images/chart.jpg
http://entertainment.webshots.com/photo/2060520010102272392olryWh
http://www.cartoonstock.com/newscartoons/cartoonists/mba/lowres/mban752l.jpg
http://www.clubs.psu.edu/up/psichi/images/WonderingHead_questionMark.JPG
http://2.bp.blogspot.com/_HDA0VuaXfOs/SLJaLaXA5EI/AAAAAAAAC_g/mBhjhu206x0/s400/question_mark.jpg
http://cardiophile.com/wp-content/uploads/2008/01/heart-in-hands.jpg
http://www.salem-news.com/stimg/april072008/cpr-2.jpg
http://www.enquirer.com/editions/2004/09/01/autopulse.jpg
http://circ.ahajournals.org/cgi/content-nw/full/112/24_suppl/IV-19/FIG2
http://www.zoll.com/uploadedImages/Products/AutoPulse/hss-2_lrg.gif
http://www.zoll.com/uploadedImages/Products/AutoPulse/ahs-1_lrg.gif
http://circ.ahajournals.org/cgi/reprint/114/25/2839

News Clip: