measuring the impact of mechanical contractor design …
TRANSCRIPT

The Pennsylvania State University
The Graduate School
College of Engineering
MEASURING THE IMPACT OF MECHANICAL CONTRACTOR DESIGN
INVOLVEMENT ON BUILDING SYSTEM AND PROJECT-LEVEL OUTCOMES:
A COMPARATIVE CASE STUDY
A Thesis in
Architectural Engineering
by
Bryan W. Franz
© 2011 Bryan W. Franz
Submitted in Partial Fulfillment of the Requirements
for the Degree of
Master of Science
August 2011

ii
The thesis of Bryan W. Franz was reviewed and approved* by the following:
David R. Riley
Associate Professor of Architectural Engineering
Thesis Advisor
John I. Messner
Associate Professor of Architectural Engineering
Robert M. Leicht
Assistant Professor of Architectural Engineering
Chimay J. Anumba
Professor of Architectural Engineering
Head of the Department of Architectural Engineering
*Signatures are on file in the Graduate School.

iii
ABSTRACT
Due to rising energy costs and increasing attention to indoor environmental quality, the
application of sustainable or “green” practices in healthcare facilities is gaining momentum. Healthcare
owners spend nearly $5 billion annually for electricity to operate 24-hour facilities, the highest of all
building industry sectors. Additionally, cases of hospital-acquired infections currently surpass 1.7 million
and are a leading cause of mortality in the U.S. HVAC and mechanical systems are a vital component of
all healthcare facilities, accounting for nearly 45% of the building’s energy usage. The need for strict
infection control and sensitive bio-engineering equipment, coupled with the potential for literally life-
threatening failures, demands that mechanical systems be installed with the highest degree of reliability
and precision. In response, many healthcare owners are turning to design-build contracts, which
empower a single contractor with the responsibility of designing, installing and commissioning a
functioning mechanical system.
Efforts to understand the impacts of integrated forms of delivery on project success have led to
the development of high-performance metrics heavily focused on using project-level metrics and
indicators to predict outcomes; however, specialty contractors at the building system-level have an
increasingly important role in the design of sustainable buildings. In a typical healthcare facility, where
the design and installation of mechanical systems represent between 20% and 50% of the project cost,
understanding building system-level relationships is crucial to predicting overall project success. To
begin understanding how the early involvement of specialty contractors relates to project success and the
performance of building systems, this research develops a comparison method to evaluate the
contributions of the mechanical contractor during design and construction.
Relationships are traced with a comparative case study of two similar hospital facilities, using
existing project-level performance metrics, to identify the relationships between integrated mechanical
system delivery and project outcomes. By combining detailed data, obtained from primary source
documents, with secondary source semi-structured team interviews, this research uses explanation-
building techniques to identify causal relationships. Results indicate improved cost and schedule
predictability at both the project and mechanical building system-level with an integrated design-build
delivery. Additionally, under a design-build arrangement, the mechanical contractor has the opportunity
and incentive to engage in iterative system design, which can improve the energy efficiency of the facility
and reduce the likelihood of construction safety accidents.

iv
TABLE OF CONTENTS
LIST OF FIGURES………………………………………………………………………………………………...vii LIST OF TABLES…………………………………………………………………………………………………viii LIST OF EQUATIONS………………………………………………………………………………………….…ix Chapter 1 INTRODUCTION ........................................................................................................................ 1
1.1 Background ................................................................................................................................... 1 1.2 Integrated Design Efforts in Healthcare ........................................................................................ 2 1.3 Measuring Outcomes in High-Performance Buildings ................................................................. 2 1.4 Moving from Project-Level to Building System-Level ................................................................ 3 1.5 Problem Statement ........................................................................................................................ 4 1.6 Research Questions ....................................................................................................................... 4 1.7 Description of the Research .......................................................................................................... 5 1.8 Summary of Contributions ............................................................................................................ 6 1.9 Reader’s Guide .............................................................................................................................. 6
Chapter 2 LITERATURE REVIEW ............................................................................................................. 7
2.1 Introduction ................................................................................................................................... 7 2.2 The Integrated Design Process ...................................................................................................... 7
2.2.1 Value of Integrated Design to System-Level Outcomes in Healthcare ................................. 9 2.2.2 Measuring Project-Level Outcomes .................................................................................... 10
2.3 Role of Specialty Contractors in the Design Process .................................................................. 12 2.3.1 Impact of Procurement on Design Involvement ................................................................. 13 2.3.2 Contributions from the Mechanical Contractor .................................................................. 13
2.4 Evolution of Design Integration .................................................................................................. 14 2.4.1 Challenges to Developing Integrated Teams ...................................................................... 15 2.4.2 Using BIM to Improve Collaboration ................................................................................. 15 2.4.3 Balancing Risk/Reward for Team Members ....................................................................... 16 2.4.4 Costs of Integrated Design .................................................................................................. 17
2.5 Summary of Literature Review ................................................................................................... 17 Chapter 3 RESEARCH METHODOLGY .................................................................................................. 18
3.1 Research Goal & Objectives ....................................................................................................... 18 3.2 Case Study Identification ............................................................................................................ 20 3.3 Types of Project Data .................................................................................................................. 20
3.3.1 Schedules ............................................................................................................................ 23 3.3.2 Change Order Logs ............................................................................................................. 23 3.3.3 Quality Control Logs .......................................................................................................... 24 3.3.4 Safety Reports ..................................................................................................................... 25 3.3.5 Energy Models and LEED Scorecard ................................................................................. 25

v
3.3.6 Requests for Information .................................................................................................... 26 3.4 Data Analysis Process ................................................................................................................. 26
3.4.1 Defining Project Attributes ................................................................................................. 27 3.4.2 Causal Analysis and Explanation-Building ........................................................................ 29
3.5 Summary ..................................................................................................................................... 31 Chapter 4 DATA COLLECTION ............................................................................................................... 32
4.1 Case Study Background .............................................................................................................. 32 4.1.1 Case A Overview ................................................................................................................ 33 4.1.2 Case B Overview ................................................................................................................ 34
4.2 Summary of Control Variables ................................................................................................... 34 4.2.1 Validating Differences in Project Size ................................................................................ 36 4.2.2 Validating Differences in Clinic-to-Hospital Area Ratios .................................................. 37
4.3 Sources of Project Data ............................................................................................................... 38 4.3.1 Project Documentation ........................................................................................................ 38 4.3.2 Site Observations ................................................................................................................ 38 4.3.3 Semi-Structured Interviews ................................................................................................. 39
4.4 Summary of Independent Project Variables ............................................................................... 39 4.4.1 Contract Type, Organizational Structure, Procurement, Design Integration ...................... 39 4.4.2 Owner Commitment ............................................................................................................ 40 4.4.3 Team Commitment ............................................................................................................. 43 4.4.4 Team Characteristics ........................................................................................................... 45
4.5 Summary of Dependent Outcome Variables ............................................................................... 47 4.5.1 Schedule Growth ................................................................................................................. 47 4.5.2 Cost Growth ........................................................................................................................ 48 4.5.3 Requests for Information .................................................................................................... 50 4.5.4 Quality Control Reports ...................................................................................................... 51 4.5.5 Safety Reports ..................................................................................................................... 52 4.5.6 LEED Scorecard and Energy Performance ......................................................................... 52
4.6 Summary ..................................................................................................................................... 55 Chapter 5 DATA ANALYSIS AND DISCUSSION .................................................................................. 57
5.1 Identifying Differences in Project Attributes .............................................................................. 57 5.2 Identifying Outcome Differences ................................................................................................ 58 5.3 Understanding Cost and Schedule Predictability Outcomes ....................................................... 60
5.3.1 Value of Predictability on Projects ..................................................................................... 60 5.3.2 Method for Comparing Predictability ................................................................................. 61 5.3.3 Evidence of Cost Predictability ........................................................................................... 61 5.3.4 Evidence of Schedule Predictability ................................................................................... 63
5.4 Determining Cause and Effect for Predictability Outcomes ....................................................... 64 5.4.1 Identification of Unique Causal Factors Impacting Predictability Outcomes ..................... 64

vi
5.4.2 Identification of Influencing Project Attributes on Causal Factors ..................................... 66 5.5 Relating Project Attributes to Predictability Outcomes .............................................................. 67
5.5.1 Organizational Structure → Cost Predictability ................................................................. 68 5.5.2 Organizational Structure → Schedule Predictability .......................................................... 71 5.5.3 Contract Type → Cost Predictability .................................................................................. 78 5.5.4 Owner Commitment → Cost Predictability ........................................................................ 80 5.5.5 Team Commitment → Schedule Predictability .................................................................. 81
5.6 HVAC Building System Performance Outcomes ....................................................................... 83 5.7 Jobsite Safety Outcomes ............................................................................................................. 86 5.8 Summary ..................................................................................................................................... 88
Chapter 6 CONCLUSIONS AND CONTRIBUTIONS ............................................................................. 90
6.1 Research Conclusions ................................................................................................................. 90 6.2 Research Limitations................................................................................................................... 91 6.3 Research Contributions ............................................................................................................... 92 6.4 Recommendations for Future Research ...................................................................................... 93
REFERENCES ........................................................................................................................................... 94
APPENDIX A: Glossary of Terms…………………………………………………………………………...97
APPENDIX B: Sample Semi-Structured Interview Questions.………………………………………..…...98
APPENDIX C: Summary of Independent Project Variables for Case A and B......……………………….99
APPENDIX D: Diagram for Relating Outcomes of Improved Predictability on Case A and B...............105

vii
LIST OF FIGURES
Figure 1-1: Existing usage of high-performance metrics as a project-level slice through all building types, compared with the building system-level slice specific to healthcare buildings .......................................... 4 Figure 2-1: Information flow model for product design (Shooter et al. 2000) ............................................ 8 Figure 2-2: Over the wall model for traditional construction design (Evbuomwan & Anumba 1998) ....... 8 Figure 2-3: Integrated design process with optimal collaborative effort (7group & Reed 2009) ................. 9 Figure 2-4: Summary of benefits provided by design-build mechanical contractors ................................. 14 Figure 3-1: Map of data collection process ................................................................................................. 21 Figure 3-2: Map of data collection and data analysis process for case comparison ................................... 30 Figure 5-1: Independent project variable relationships with predictability outcomes ................................ 67 Figure 5-2: Case comparison of mechanical contractor construction costs ................................................ 70 Figure 5-3: Case comparison of mechanical contractor general conditions ............................................... 71 Figure 5-4: Timeline comparison of Case A and Case B with notations .................................................... 73 Figure 5-5: Case comparison of linear project-level design and construction rates ................................... 76 Figure 5-6: Case comparison project completion by duration, with delivery speeds ................................. 78 Figure 5-7: Percent design completion with percent cost growth, project and mechanical ........................ 80 Figure 5-8: Case A award-fee distribution by category .............................................................................. 82 Figure 5-9: Percentage of Case A award-fee pool available at each period ............................................... 83 Figure 5-10: Safety performance comparison between Case A and Case B ............................................... 87

viii
LIST OF TABLES
Table 1-1: Existing project-level variables for evaluating HPG buildings (Korkmaz 2005) ........................ 3 Table 2-1: Comparison of project success measures (Chan 2002) and variables (Korkmaz 2010) ........... 12 Table 3-1: Proposed dependent variables of study with associated metrics and source documents ........... 22 Table 3-2: Incidence rates for construction sector by size (U.S. Bureau of Labor Statistics 2008) ........... 25 Table 3-3: Independent project variables with proposed level of integration ranking ................................ 28 Table 4-1: Summary of control variables for Case A and Case B .............................................................. 36 Table 4-2: Calculated R.S. Means size factors and cost multipliers ........................................................... 36 Table 4-3: Estimated project unit cost, adjusted for differences in use areas between cases ..................... 37 Table 4-4: Summary of project delivery independent variables for Case A and Case B ............................ 40 Table 4-5: Data sources for determining owner commitment .................................................................... 42 Table 4-6: Summary of owner commitment independent variable criteria ................................................ 42 Table 4-7: Data sources for determining team commitment ....................................................................... 44 Table 4-8: Summary of team commitment independent variable criteia .................................................... 44 Table 4-9: Data sources for determining team characteristics .................................................................... 46 Table 4-10: Summary of team characteristics independent variable criteria .............................................. 46 Table 4-11: Summary of schedule performance data for Case A and Case B ............................................ 48 Table 4-12: Summary of cost performance data for Case A and Case B .................................................... 49 Table 4-13: Summary of RFI data for Case A and Case B ......................................................................... 51 Table 4-14: Summary of quality control and quality assurance data .......................................................... 51 Table 4-15: Summary of safety data for Case A and Case B ...................................................................... 52 Table 4-16: Summary of LEED and energy data for Case A and Case B .................................................. 53 Table 4-17: Summary of energy modeling results and energy performance .............................................. 54 Table 5-1: Selection of independent project variables for further analysis ................................................. 58 Table 5-2: Grouping of case study outcome metrics into contextual outcomes ......................................... 59 Table 5-3: Project and mechanical system unit cost comparison with percent difference .......................... 62 Table 5-4: Percentage breakdown of mechanical contractor change orders with percent difference ......... 63 Table 5-5: Schedule unit durations with percent difference ....................................................................... 63 Table 5-6: Causal factors impacting cost predictability, by case occurrence ............................................. 65 Table 5-7: Causal factors impacting schedule predictability, by case occurrence ...................................... 65 Table 5-8: Sorted causal factors for predictability, by influencing project attribute .................................. 66 Table 5-9: Timing comparison table for milestones and selected design processes ................................... 75 Table 5-10: Mechanical system description and maintenance information by case ................................... 85 Table 5-11: Building energy performance and cost savings by case .......................................................... 86

ix
LIST OF EQUATIONS
Equation 5-1: Percent difference ................................................................................................................ 61
Equation 5-2: Percent growth ..................................................................................................................... 61

1
Chapter 1
INTRODUCTION
1.1 Background
Due to rising energy costs and increasing attention to indoor environmental quality, the
application of sustainable or “green” practices in healthcare facilities is gaining momentum.
Healthcare owners spend nearly $5 billion annually for electricity to operate 24-hour facilities,
the highest of all building industry sectors (U.S. Department of Energy 2003). Cases of hospital-
acquired infections currently surpass 1.7 million and are a leading cause of mortality in the U.S.,
exceeding the deaths attributable to AIDS, cancer and automobile accidents (Klevens et al. 2007).
Green hospitals address both issues, with the promise of reduced energy usage, lower operating
expenses and improved clinical outcomes. Since the first LEED-certified healthcare facility was
opened in 2003, over 120 hospital projects have been publically registered with the U.S. Green
Building Council (USGBC). While the market for sustainable healthcare facilities is still
developing, initial research shows that an integrated design process, involving multiple
disciplines early in project development, is central to implementing green goals or strategies at a
reasonable initial cost.
Heating, ventilation and air-conditioning (HVAC) and mechanical systems are a vital
component of all healthcare facilities, accounting for nearly 45% of the building’s energy usage
(Consortium for Energy Efficiency 2005). In addition to 24-hour operational demands, hospitals
have specific mission-critical functions that are essential for patient care. The need for strict
infection control and sensitive bio-engineering equipment, coupled with the potential for literally
life-threatening failures, demands that mechanical systems be installed with the highest degree of
reliability and precision. In response, many healthcare owners are turning to design-build
contracts, which empower a single contractor with the responsibility of designing, installing and
commissioning a functioning mechanical system. Research shows that the mechanical
contractor’s design knowledge and field expertise can reduce energy costs and enhance reliability
through innovative system design, awareness of work spaces and right-sized equipment (Riley,

2
Sanvido, et al. 2005). Measurement of contractor contributions to design is necessary to identify
the relationships between early trade involvement and project outcomes, and to understand how
and when contractors add the most value to design.
1.2 Integrated Design Efforts in Healthcare
Integrated design practices and collaborative team efforts are frequently cited as key
contributors to the achievement of project goals in healthcare facilities. Case studies of the
Children’s Hospital of Pittsburgh UPMC and Penn State’s Hershey Medical Center suggest that
early team involvement, strong stakeholder commitment and transparent goals are characteristics
of integrative design that are correlated with higher LEED ratings (Bilec et al. 2009). Similarly,
the Dell Children’s Medical Center in Austin, Texas attributed its LEED Platinum rating to an
unwavering team commitment and the establishment of explicit goals during early phases of
design (Cassidy 2010). Clearly, the complexity of hospital and medical facilities necessitates a
shift away from traditional “over-the-wall” design practices and towards an integrated,
interdisciplinary approach. The most recent model of integrated design, the 7group’s 4E concept,
suggests that meaningful collaboration is only achieved when Everybody is Engaging Everything
Early (7group and Reed 2009). The 4E philosophy proposes that a unified, whole-building
design results from a series of iterative scope refinements, workshops and value assessments.
The synthesis of construction expertise with design knowledge and feedback sessions adds value
to the building process by eliminating the barriers between architects and contractors. While
integrated design is slowly being adopted in all sectors of the construction industry, the
collaborative process is bringing immediate benefits to healthcare projects.
1.3 Measuring Outcomes in High-Performance Buildings
Efforts to understand the impacts of integrated delivery on project success have led to the
development of high-performance metrics, specifically designed for sustainable buildings.
Evolving from the seminal work of Konchar and Sanvido (1998), which used basic metrics of
cost, quality and schedule performance, Korkmaz (2005) proposed an expanded listing of
variables associated with project success. These new high-performance evaluation measures,
summarized in Table 1-1, provide a more comprehensive, project-level view of factors effecting
the level of integration and likelihood of achieving green or sustainable goals. Unlike product-
based metrics, such as LEED or Green Globes, which award points and ranking based on the

3
achievement of specific green goals, Korkmaz’s measures are a process-based approach that
attempts to predict project outcomes by considering likely success indicators. Trial studies of
these metrics were conducted on eight LEED-certified office buildings in Washington, D.C.,
where results suggested strong relationships between integrated design with construction teams
and higher performance, as measured in terms of cost growth and schedule growth, quality and
sustainability. Since the publication of findings from these initial trial studies, additional testing
of high-performance metrics at the project-level has occurred across all sectors of the
construction industry. Most notable is the work of the Charles Pankow Foundation, which
currently uses this research as the basis for collecting and analyzing data on green
buildings(Molenaar et al. 2009; Korkmaz, M. Horman, Riley, et al. 2010).
Table 1-1: Existing project-level variables for evaluating HPG buildings (Korkmaz 2005)
High-Performance Project-Level Evaluation Variables
Independent Variables Dependent Variables Control Variables Owner commitment Project delivery Project procurement Timing of involvement Integrated design Project team
characteristics Construction process
Cost Time Quality Safety Level of high
performance Overall success
Local regulation Labor availability Geographic location Project size Project complexity Project type Type of building
systems
(Process indicators) (Performance metrics) (External environment)
1.4 Moving from Project-Level to Building System-Level
Present research efforts on integrated design are heavily focused on using project-level
metrics and indicators to predict outcomes; however, specialty contractors at the building system-
level have an increasingly important role in the design of sustainable buildings. From curtain
wall assemblies to HVAC systems, specialty contractors possess the system knowledge and field
expertise to deliver more energy efficient, cost-effective designs. In a typical healthcare facility,
where the design and installation of mechanical systems represent between 20% and 50% of the
project cost, understanding building system-level relationships is crucial to predicting overall
project success. Unfortunately, few researchers have deeply explored or measured outcomes
associated with contributions from MEP contractors to the integrated design process. While
design assistance from specialty contractors is subjectively valued by project teams, contractor
feedback is frequently underutilized because of poor communication or misaligned contract

4
incentives (Gil et al. 2000). Therefore, adapting the usage of high-performance metrics from a
broader project-level approach to the building system-level, as shown in Figure 1-1, will assist in
understanding the role of specialty contractors during design.
Figure 1-1: Existing usage of high-performance metrics as a project-level slice through all building types, compared with the building system-level slice specific to healthcare buildings
1.5 Problem Statement
While the design and construction processes of building systems are often improved by
the integration of specialty contractors during the early stages of project development, no
methodology exists for specifically assessing their contributions to project outcomes.
Furthermore, the number of variables and interactions on typical projects are often staggering,
making clear cause and effect relationships difficult to pinpoint. In theory, the same project-level
metrics developed recently for high-performance buildings could be applied or adapted to the
building system-level and the work of individual specialty contractors. To understand how the
early involvement of specialty contractors relates to project success and the performance of
building systems, this research develops a comparison method to evaluate the contributions of the
mechanical contractor during design and construction.
1.6 Research Questions
1. What methodologies can assess the impact of contributions from the mechanical
contractors involved with an integrated design process?
Commercial Offices
Retail
Educational
Healthcare
Industrial
Building Ty
pes
Several prior studies: Project‐level analysis across all building types
This research: Two case study building system‐level analysis, specific to healthcare buildings

5
2. Are there differences between highly integrated and less integrated building system
approaches which are measurable with existing project-level metrics?
3. How are outcomes at the mechanical building system-level related to overall project-level
outcomes?
1.7 Description of the Research
This research performed a comparative case study, using existing project-level
performance metrics, to identify the relationships between integrated mechanical system delivery
and project outcomes. A nationally recognized design-build mechanical contractor agreed to
participate in a study involving two new hospital construction projects, which were believed to
illustrate outcome differences attributable to varying levels of contractor design integration and
timing of involvement. Case A, which engaged the mechanical contractor in a design-build
capacity, appeared to perform more consistently in cost and schedule outcomes, when compared
to the more traditional construction manager (CM) at risk organizational structure used on Case
B. Differences between these case studies were collected to build case descriptions using the
project-level variables proposed by Korkmaz (2005) to determine how outcome differences were
impacted at both the project-level and building system-level by design contributions from the
mechanical contractor.
By combining project data obtained from primary source documents, including RFIs,
change order logs, schedules and field observation, with secondary source semi-structured team
interviews, this research used explanation-building techniques to identify causal relationships
between project attributes and project outcomes. Project attributes are the independent project
variables, such as delivery method, contract type, procurement strategy and team characteristics,
which are often established early in project development and define the depth and timing of
contractor involvement. Project outcomes are the dependent outcome variables or performance
metrics that measure cost growth, schedule growth, energy performance, quality or work and
safety statistics. Underlying both project attributes and project outcomes are control variables,
including building size, type, funding method, location and complexity, which describe the
external environment or context of a project. Once collected, the detailed project outcome
metrics on both cases were reviewed and categorized into broader contextual outcomes to
eliminate redundancies. After identifying differences in project attributes, explanation-building

6
techniques were used to propose and discuss several potential causal relationships with project
outcomes.
1.8 Summary of Contributions
1. Testing of existing project-level performance metrics at the building system-level in a
comparative case study, focusing specifically on the mechanical contractor.
2. Comparison structure and methodology for reviewing the contributions of specialty
contractors to design and construction performance.
3. Identification of several causal relationships, linking specific project attributes to building
system-level and project-level outcomes.
1.9 Reader’s Guide
Chapter 1 provided an introduction to the research problem, including relevant
background information, problem statement and description of proposed research. Chapter 2
presents a literature review to identify gaps in current knowledge, which serve as the motivation
for this study. The data collection methodology and research analysis techniques are described in
Chapter 3. Chapter 4 provides a detailed account of both cases, including case overviews,
variable descriptions and resulting outcome metrics. Chapter 5 discusses several causal
relationships between project attributes and the notable contextual outcome differences between
cases. Finally, Chapter 6 summarizes the strongest conclusions, states contributions to the
research community and proposes areas of future research.

7
Chapter 2
LITERATURE REVIEW
2.1 Introduction
Hospitals rely on high-performance mechanical systems to provide 24-hour ventilation,
conditioning and sterilization for effective patient care. Consequently, healthcare organizations
spend over $5 billion annually on electricity (U.S. Department of Energy 2003), with HVAC
systems accounting for nearly 45% of the total energy usage (Consortium for Energy Efficiency
2005). When involved with an integrated design and construction process, project teams have a
unique opportunity to improve the efficiency, reliability and sustainability of HVAC systems in
healthcare facilities. Specifically, the design capability and expertise of mechanical contractors
are quantifiable resources in delivering cost-effective, energy and resource efficient building
systems in the growing healthcare construction industry.
2.2 The Integrated Design Process
Inadequacies of traditional or “over the wall” design approaches have encouraged a shift
towards interdisciplinary collaboration during the early stages of project planning. Traditional
design strategies promoted well-defined and sequential steps, which develop building systems
from concept to construction in relative isolation (Evbuomwan & Anumba 1998). For example,
architectural and structural drawings are typically a prerequisite for starting HVAC design,
despite the impact of glazing type and material selection on the heating and cooling loads of
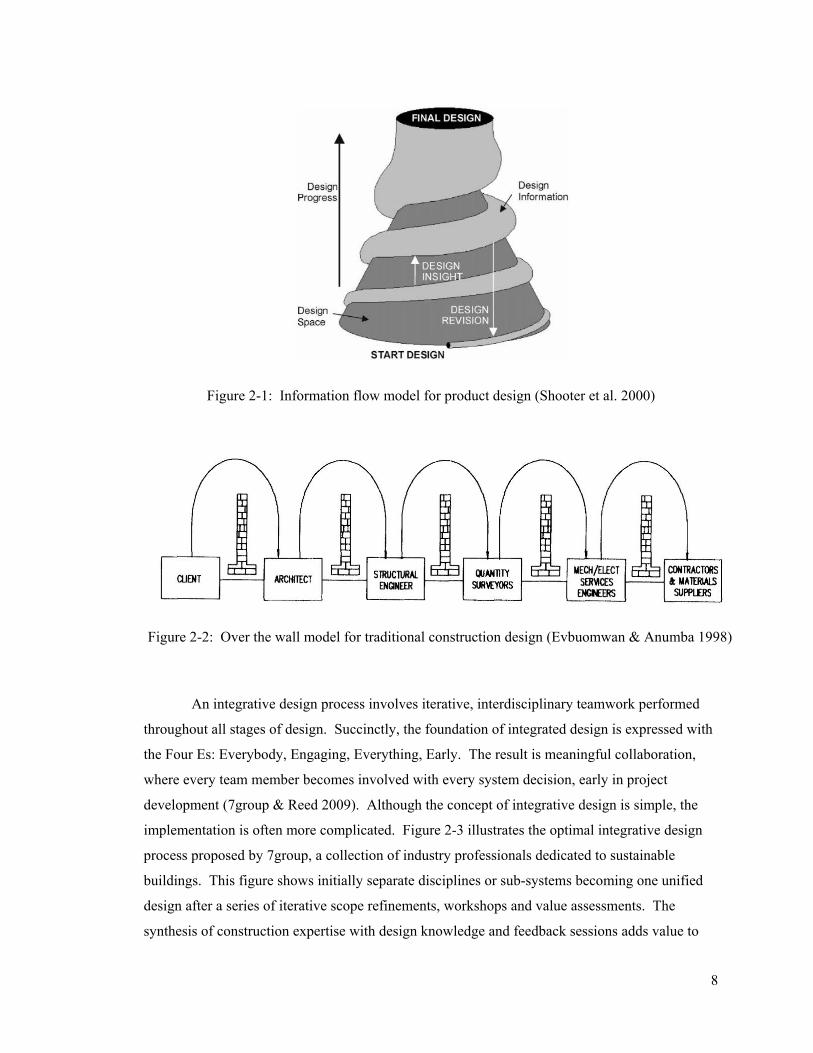
mechanical systems. As shown in comparing Figures 2-1 and Figure 2-2, the concept of
traditional design in construction closely matches an engineering model for product development
(Shooter et al. 2000). Both models depict a linear progression and the gradual addition of design
information without any upstream or downstream feedback. This process of isolated decision-
making and fragmented information flow historically results in expensive change orders,
redundant designs and suboptimal building performance (Kashyap et al. 2003). Therefore,
project teams are incentivized to pursue collaborative design efforts, as a means of meeting the
performance demands of increasingly complex buildings.
8
Figure 2-1: Information flow model for product design (Shooter et al. 2000)
Figure 2-2: Over the wall model for traditional construction design (Evbuomwan & Anumba 1998)
An integrative design process involves iterative, interdisciplinary teamwork performed
throughout all stages of design. Succinctly, the foundation of integrated design is expressed with
the Four Es: Everybody, Engaging, Everything, Early. The result is meaningful collaboration,
where every team member becomes involved with every system decision, early in project
development (7group & Reed 2009). Although the concept of integrative design is simple, the
implementation is often more complicated. Figure 2-3 illustrates the optimal integrative design
process proposed by 7group, a collection of industry professionals dedicated to sustainable
buildings. This figure shows initially separate disciplines or sub-systems becoming one unified
design after a series of iterative scope refinements, workshops and value assessments. The
synthesis of construction expertise with design knowledge and feedback sessions adds value to

9
the building process by eliminating barriers between architects and contractors. While integrated
design is slowly being adopted by the construction industry, current research demonstrates that
the collaborative process is bringing immediate benefits to building system-level performance of
healthcare projects.
Figure 2-3: Integrated design process with optimal collaborative effort (7group & Reed 2009)
2.2.1 Value of Integrated Design to System-Level Outcomes in Healthcare
Hospitals investing in integrative design typically received higher levels of LEED
certification, when compared to facilities with less ambitious goals or more traditional delivery
methods. At the project-level, case studies of the Children’s Hospital of Pittsburgh UPMC and
Penn State’s Hershey Medical Center suggest that early team involvement, strong stakeholder
commitment and transparent project and sustainability goals are characteristics of integrative
design that are correlated with successful hospital delivery (Bilec et al. 2009). For example, early
team selection engages an interdisciplinary design process, combining contractor experience with
engineering knowledge to accomplish project objectives. Similarly, establishing transparent
goals strengthens team commitments and reduces ambiguity during the design of healthcare
facilities. While LEED rating is not an exhaustive or all-inclusive measure of project success, a

10
higher level of certification indicates improved energy efficiency and qualifies the value of
pursuing integrated design for healthcare projects.
The Dell Children’s Medical Center in Austin, TX achieved LEED Platinum rating with
an integrated design approach that produced innovative HVAC systems and lifecycle energy
savings. During development, the project team established three guiding principles: (1) do not
blindly pursue LEED points, (2) achieve a minimum of 12% return-on-investment, and (3)
perform feasibility studies at each stage of design. The team’s commitment to these principles
resulted in the design of an efficient onsite combined heat and power (CHP) plant, right-sized air
handling equipment serving single departments and a highly customized glazing system. At
completion, the medical center realized a very competitive cost per square foot of $305 and was
rated 61% above the ASHRAE 90.1 energy efficiency baseline for similarly scoped hospital
facilities (Cassidy 2010). The Dell Children’s Medical Center’s success in becoming the first
LEED Platinum hospital exemplifies the benefits of integrated design and collaborative project
delivery to building system-level outcomes.
2.2.2 Measuring Project-Level Outcomes
Selection of project delivery, contracting and procurement methods often dictate the
depth and potential for integrated design. By selecting a specific organizational structure, owners
are defining the timing of team involvement and hierarchy for team relationships and interactions.
Similarly, choosing a contracting type establishes incentives and penalties, while allocating risk
among the project team. Previous research, quantifying the differences between organizational
structures, revealed that design-build typically outperforms traditional design-bid-build with an
average 5% less cost escalation and 9% less schedule growth (Konchar & Sanvido 1998). This
study generally compared an input delivery method against output metrics of cost, schedule and
quality and implies that an integrated design and construction process is correlated with project
outcomes. Expanding on this seminal project delivery research, Korkmaz (2005) used statistical
case study analysis and regression to illustrate how design-build contracting, best value selection
and open communication contribute to achieving sustainability goals in High-Performance Green
(HPG) buildings. Conversely, traditional organizational structures, including design-bid-build
and CM at risk, and inexperienced teams were linked to poor building system performance, often
opting to remove energy-saving features for lower first-cost options. Both studies reached similar
conclusions, demonstrating a link between integrated delivery strategies and typical project

11
success indicators; however, the assessment of healthcare facilities requires more exhaustive
metrics than simply cost, schedule and quality.
More recent research identified additional measures common in highly integrated design
and construction processes, as a means of evaluating building performance. Chan (2002)
proposed a series of “objective” or tangible and “subjective” or intangible success criteria that
included conformance to expectations, functionality, aesthetics and reduction in disputes.
Building on these criteria, Korkmaz (2010) identified “independent” and “dependent” variables
useable as metrics for gauging the success of high-performance buildings. There are several core
similarities between Chan’s objective project success measures and Korkmaz’s dependent
outcome variables, as shown in Table 2-1. Independent variables are unique to each project or
process and include owner commitment, team procurement, team characteristics, construction
processes, contract conditions and design integration. Alternately, dependent variables focus on
outcomes and include schedule and cost performance, quality, energy efficiency and safety
(Korkmaz, M. J. Horman & Riley 2010). While limited in scope, pilot studies of Korkmaz’s
measures were conducted on eight LEED-certified office buildings in Washington, D.C. and
results predicted relationships between integrated design efforts and superior project and building
system-level performance.

12
Table 2-1: Comparison of project success measures (Chan 2002) and variables (Korkmaz 2010)
Objective Measures of Success (Chan 2002)
Dependent Outcome Variables (Korkmaz 2010)
Time Cost Health and safety Profitability
Cost: • Cost growth • Unit cost • Cost intensity
Time: • Schedule growth • Construction speed • Delivery speed
Quality and satisfaction: • Turnover quality • Overall quality • System quality
System performance and sustainability: • IEQ rate • Energy rate • Green rate
Subjective Measures of Success (Chan 2002)
Quality Technical performance Satisfaction of project participants, in regards to: • Conflict management • Completion • Functionality • Aesthetics • Professional image • Educational and
social aspects Sustainability Productivity
2.3 Role of Specialty Contractors in the Design Process
Present research efforts on integrated design and construction practices are heavily
focused on project-level applications and outcomes. However, specialty contractors are
developing an evolving role in the design and construction of high-performance buildings. From
curtain wall assemblies to HVAC systems, specialty contractors often possess the system
knowledge and expertise to deliver energy efficient, cost-effective designs. Unfortunately, few
researchers have deeply explored the role and value of specialty contractors in contributing to
project and building system-level outcomes. Tommelein & Ballard (1997c) reported that
contractors are attempting to shift from on-site, handcrafted work to off-site, prefabrication
strategies where feasible, which requires detailed shop and installation drawings. By transferring
production off-site, contractors become even more reliant on the availability and accuracy of
design information. Early involvement of the contractor is one method of improving coordination
between the installer and designer, ensuring that information flow is continuous and iterative.
When involved and held responsible during the early stages of design, specialty contractors add
value by contributing creative system solutions, knowledge of work spaces, fabrication advice,

13
and material lead time estimates. While these support services are valued by project teams, they
frequently remain untapped during design because of poor communication or misaligned contract
incentives (Gil et al. 2000). Therefore, the quantifiable value of specialty contractor involvement
on integrated teams in the healthcare industry remains unmeasured and largely unknown.
2.3.1 Impact of Procurement on Design Involvement
Procurement decisions impact the depth of contractor integration and are strongly
correlated with project performance. For design-build projects, faster delivery speeds are directly
related to the completeness of scope definition at contractor bid invitation and design completion
at award. Similarly, faster construction speeds are attainable with greater flexibility of the
contract schedule (Ling et al. 2004). Research performed by El Wardani et al. (2006) compared
sole source, qualification-based, best value and low bid procurement methods to determine
relative performance benefits in design-build contracts. The results indicated that contractors
selected through best value and pre-qualification demonstrated the fastest delivery and
construction speeds in high-complexity projects. For healthcare construction, this research
supports the early collaborative involvement of specialty contractors with the expertise to manage
potentially ambiguous scopes, changing end-user requirement and sustainable design elements.
2.3.2 Contributions from the Mechanical Contractor
Due to increased emphasis on hospital and medical facility HVAC performance, specialty
mechanical contractors are more often involved in integrated design. Case studies of design-build
mechanical firms confirmed previous specialty contractor research, verifying that creative design
and fabrication improvements were attainable with earlier team collaboration. Additionally,
mechanical contractors possess the expertise needed to effectively reduce HVAC first costs and
improve system efficiency by “right-sizing” equipment (Riley, Sanvido, et al. 2005). These
benefits of design integration, summarized in Figure 2-4, represent an opportunity for project
teams to meet the energy efficiency demands of healthcare facilities. When involved with an
integrated design-build process, the mechanical contractor assumes a leadership role to leverage
engineering experience and knowledge to improve the HVAC system-level performance, while
remaining incentivized to control cost and schedule growth.

14
Figure 2-4: Summary of benefits provided by design-build mechanical contractors
2.4 Evolution of Design Integration
As healthcare facilities rapidly increase in complexity, the formation of project alliances,
design-build arrangements and integrated project delivery (IPD) involving specialty contractors
are being developed to better align incentives among design and construction teams.
Improvements in building system technology and demands for higher performance have shifted
the construction industry from relying on a single master builder and “over-the-wall” approach to
requiring separate and more specialized teams of professionals, often introducing inefficiencies,
fragmentation and interoperability concerns into the project management process (Kent &
Becerik-Gerber 2010). The IPD concept evolved alongside design-build, as a means of
reconnecting and realigning these fragmented teams and information flows with project goals.
According to the American Institute of Architects (AIA), IPD is defined as a collaborative
alliance of people, systems, and practices into a process to collaboratively use the talents and
insights of all participants. This type of integrated delivery attempts to leverage the expertise of
specialty contractors and design professionals during early phases of program development. In
other words, IPD is characterized by risk sharing, instead of risk shifting as found in traditional
design-bid-build, CM at risk and occasionally design-build organizational structures. The
success of an IPD team depends on the owner, architect and builder's ability to collaborate in
achieving project goals, instead of individual goals.
Design Capability
Field Expertise
• Optimally size equipment • Innovative solutions • Engineering drawings as shop drawings • Improve visibility of systems
• Efficient equipment layout • Simplify installation and maintenance • Reduce onsite labor • Simplify commissioning process
Benefits of Involvement and Design ResponsibilityContractor Competencies

15
2.4.1 Challenges to Developing Integrated Teams
While a seemingly sensible approach to promoting an integrated project, the IPD model
is experiencing slow adoption in the construction industry due to several relational and legal
challenges associated with the multi-party contract. Prior research has suggested that team
integration is positively correlated with team effectiveness, emphasizing the importance of
relationships to the success of an IPD or other multi-party contract. A fully integrated team can
be described as having the following characteristics: (1) team focus and objectives, (2) seamless
operation without organizational boundaries, (3) unrestricted cross-sharing of information, (4)
creation of collocated teams, (5) equitable relationships, opportunities and respect for all and (6) a
"no blame" culture (Baiden & Price 2011). Deficiencies in any of these characteristics limit the
successful integration, and subsequently effectiveness, of teams attempting a design-build or IPD
process. Underscoring these integrated team characteristics, research in the field of relational
contracting identified several factors facilitating team relationships, which include: (1) integrated
objectives and risk-reward plan, (2) appropriate risk sharing, (3) motivated owner, (4) trust-based
arrangements and (5) top-down management support (Rahman & Kumaraswamy 2008). These
findings describe an ideally integrated design and construction team, where the potential for
collaboration and coordination is maximized. However, when disagreements do arise, the legal
implications of disputes concerning design responsibility, document ownership, insurance and
project scope within the multi-party contract are largely unaddressed in common law.
2.4.2 Using BIM to Improve Collaboration
Building information modeling (BIM) processes leverage the flow of information
between design and construction teams to improve the efficiency of projects. Currently, the
industry is divided on whether BIM is a required prerequisite to pursuing an IPD approach, with
recent survey results indicating a slight favoring of the non-prerequisite option (Kent & Becerik-
Gerber 2010). However, when implemented, BIM can supplement team integration by: (1)
establishing a framework for describing the work, (2) assisting with team decision-making,
sequencing and supply chain management and, (3) engaging facility managers in design and
construction processes (Zhang & Chen 2010). These supplementary functions promote
collaboration and reduce fragmentation of teams, both important aspects in maintaining the
integrity of design-build or IPD contracts.

16
2.4.3 Balancing Risk/Reward for Team Members
The structure of contracts designed to promote an integrated team environment should
provide a balance of risk and reward among the owner, designer and builder. A typical integrated
project agreement follows three main objectives, including: (1) all parties understand their
liability, (2) establish a mechanism for compensation for a breach of contract and, (3) encourage
all parties to act in the interest of the project (Chapman & Ward 2008). Within the context of
these objectives, several clauses are beneficial in striving for risk/reward balance (Zhang & Chen
2010):
• Risk allocation: Under traditional design-bid-build and design-build delivery, each party
is fully responsible for their own negligence, contractual breaches and performance
warranties. However, within an IPD context, risk allocation is limited to an amount
determined through negotiation when the contract is initiated. Team members may seek
claims against each other, but the maximum liability is capped to protect parties from
excessive claims.
• Profit/loss and liability sharing: IPD contracts are frequently structured into multiple
"layers" of shared liability. The bottom layer encompasses the targeted cost of the project
and includes the direct costs, overhead and negotiated profit of each party. The second
layer above the project cost represents a zone of shared fee, which increases or decreases
with changes in the target cost and provides a strong financial incentive. Any actual costs
incurred above the sum of target cost and shared fee are paid by the owner to limit the
responsibility of designers and builders. Design-build contracts frequently include a form
of shared award-fee or incentive pool to reward performance above and beyond
expectations, but is controlled and issued at the discretion of the owner.
• Liability limitations: Within many IPD agreements, all claims are waived on decisions
made by the team leadership, provided that damages were not the result of willful
negligence of misconduct. This clause shares risk evenly by placing faith in the decisions
made by the project team within the context of an IPD arrangement. However,
negotiations and mediation are still viable procedures for addressing more serious claims
and to avoid costly litigation. Design-bid-build and design-build arrangements do not
typically have limits on damage liability.

17
2.4.4 Costs of Integrated Design
Integrated project design and delivery requires an initial investment, which may be
recovered by improved process efficiency during construction or during the operational phase of
facility ownership. On average, early involvement of the designer, engineer and contractor adds
3% of total project costs for planning and design and nearly 2-months to the design process
(Kozlowski 2004). While owners report benefits during construction, such as fewer change
orders and contracting disputes, the tangible payback occurs through the operational energy
savings of a successfully integrated building system design. Therefore, measuring and
quantifying the outcomes resulting from early design involvement of specialty and influential
contractors will support owners in weighing the initial costs of design and management against
their expected return on investment.
2.5 Summary of Literature Review
Current research does not adequately address the contributions of specialty contractors to
project and building system-level outcomes on high-performance healthcare facilities. Reviewed
research studies indicate that highly integrated teams, that leverage early contractor involvement
during design phases, increase the likelihood of achieving energy efficiency goals and obtaining
LEED certification in healthcare facilities. At the project-level, integrated delivery methods, such
as design-build, consistently outperform traditional deliveries in categories of cost, schedule and
quality. Specifically, mechanical contractors are finding new opportunities in design-build
healthcare projects by adding collaborative value early in project development. Design-build and
IPD agreements attempt to reintegrate previously fragmented owners, designer, builders and
specialty contractors into a truly integrated team. However, recent research suggests that the
success of these approaches is highly dependent on team relationships, trust and collaboration
between all parties. Risk sharing and incentive clauses assist in ensuring strong team alignment
with project goals and BIM processes have the potential for alleviating some of the collaboration
requirements recommend for developing more integrated teams. Since specialty contractor
expertise is becoming more valued by the project teams, understanding the value of integrated
design-build mechanical contractor involvement will assist owners in delivering energy and
resource efficient healthcare facilities.

18
Chapter 3
RESEARCH METHODOLGY
3.1 Research Goal & Objectives
The goal of this research was to understand how an integrated design and construction
process, which included early involvement of the mechanical contractor, impacted building
system and project performance. The study used a comparative analysis of two similar hospital
construction projects, where differing levels of contractor design involvement resulted in notably
divergent and measureable outcomes. Whereas most current research measured the influence of
integrated delivery at the project-level, this study applied the same high-performance metrics to
the building system-level, focusing specifically on the mechanical contractor. The following
research objectives and tasks were performed to advance the research goal:
1) Review existing literature and research methods.
a. Reviewed state-of-the-art metrics currently used by researchers and industry
professionals to assess High-Performance Green (HPG) buildings.
b. Identified a set of parameters or variables to adequately define an integrated
project and establish metric criteria for assessing the project outcomes.
a. Reviewed literature on the role of specialty contractors in design.
2) Identify two hospital case studies and collect data.
a. Identified control variables to describe the external environment of the cases,
which remain constant during design and construction. These include facility
size, type, funding method, location and complexity.
b. Documented all similarities and differences in independent variables
between cases. These include contract type, organizational structure,

19
contractor procurement strategy, owner and team commitment and team
characteristics.
c. Reviewed project schedules, change order logs, quality control logs, RFIs
and meeting minutes to build dependent variable metrics that describe the
performance of each case in terms of cost, schedule, quality, safety and
sustainability.
3) Identify relationships between project attributes and performance outcomes.
a. Used explanation-building techniques to causally link differences in project
attributes with outcomes at the project and building system-level for the
mechanical scope, specifically concerning the following:.
i. What patterns emerge? Did any indicators consistently predict
success or a desirable outcome?
ii. Did the more integrated project team perform better?
iii. How important was the timing and influence of contractor design
feedback?
b. Compared the observed relationships with expectations established in
previous research.
i. How did the building system-level performance relate to or shape the
project-level performance?
4) Present research contributions and summary of future work.
a. Demonstrated a comparison structure, suitable for assessing the contributions
of a specialty contractor’s involvement on integrated design and construction
teams.
i. Adapted project-level metrics to a specific building system and the
work of mechanical contractors.
ii. Organized independent and dependent project variables, in a
manner that is easily understood and readily applied to future case
studies.

20
3.2 Case Study Identification
A multiple-case study approach was used for a comparative investigation into the value
of integrating the mechanical contractor into design and construction activities on healthcare
projects. A nationally recognized mechanical engineering and construction firm approached the
Penn State Department of Architectural Engineering with two contrasting hospital projects,
hereafter referred to as “Case A” and “Case B”, with similarities in size, type, location and
sustainable goals, but purportedly diverging in performance outcomes due to differences in
several project delivery components, including organizational structure, contract type and timing
of contractor involvement. An initial vetting with the mechanical contractor on both cases was
performed prior to data collection, confirming that neither project was an unusual or rare case.
Assuming the role of independent investigator, the researcher pursued a rigorous data collection
methodology to quantify the outcomes on both projects. The similarity of control variables and
access to detailed project information were strengths leveraged in this comparative case study.
3.3 Types of Project Data
This study combined quantitative data from primary source project documents, including
RFIs, change order logs, schedules and meeting minutes and jobsite observations with secondary
sources such as semi-structured team interviews. Multiple sources of evidence from several team
members were used to internally validate records and corroborate the outcomes measured from
the project documents. For instance, change order logs from the construction manager/general
contractor (CM/GC) indicating cost escalation due to poorly-defined scope were confirmed by
contractor perceptions of incomplete or unclear design. Multiple data sources also assisted in
minimizing source bias, since the results of this research may support the business model or
preferred project organizational structure of the mechanical contractor providing much of the
project data. A map of the data collection is provided in Figure 3-1 and includes the following
stages: (1) onsite observation, (2) obtain multiple data sources, (3) follow-up on data as
necessary, and (4) organize data into metrics.

21
Figure 3-1: Map of data collection process
The primary goal of this data collection process was to obtain an accurate “snapshot” of
each case during the construction phase, which enabled a fair and complete comparison of the
case study outcomes. The construction phase was specifically selected for data collection, since
the practical outcomes of specialty contractor design involvement are not always evident or
measurable in early design phases. Additionally, the selected metrics are proven most useful in
measuring in-progress data, generated during the construction process, which allows project
teams to initiate “course corrections” and adapt to project changes. Data obtained through project
documents constituted the dependent outcome variables or performance measures of this
research. A summary of these dependent outcome variables, with their associated metrics and
source documents is provided in Table 3-1. This method of evaluation was directly adapted from
Korkmaz’s (2005) metrics, previously discussed as a method of assessing specifically High-
Performance Green (HPG) buildings.
Onsite ObservationSpent 1-week onsite for each case, observing CM/GC, owner, architect and contractors
Multiple Data SourcesGathered data from project documents, jobsite observation and semi-structured interviews
Follow‐up DataFollow-up discussions to clarify and verify existing data or request additional informationOrganize into Metrics
Generated 30+ metrics describing project and building system performance outcomes
Data Collection Process

22
Table 3-1: Proposed dependent variables of study with associated metrics and source documents
Dependent Outcome Variable Metric Source Document(s) Schedule
Construction schedule performance
((Actual construction time – estimated construction time) /
Actual construction time) x 100 Baseline project schedule, current project schedule, baseline mech. contractor schedule, current mech. contractor schedule
Design schedule performance ((Actual design time – estimated
design time) / Actual design time) x 100
Time per unit Project duration / total units Cost
Construction cost performance ((Actual construction cost –
estimated construction cost) / Actual construction cost) x 100 Initial and current project
contract value, initial and current mech. contract value
Design cost performance ((Actual design cost – estimated design cost) / Actual design cost)
x 100
Cost per unit Project cost / total units
Pending change orders Qty., $ value Project change order log Approved change orders Qty., $ value
Pending mech. change orders Qty., $ value Mech. change order log Approved mech. change orders Qty., $ value
Quality
Quality performance Qty. of "Open" items, Time to "Closed" status QA/QC log
Safety
Reportable incident rate (Number of reported incidents x 200,000) / Hours worked CM/GC safety reports,
Mech. contractor safety reports Lost time (Number of lost time incidents x
200,000) / Hours worked
Sustainability Goals Planned energy performance W/sf, GJ/yr Initial and current energy
model data Actual energy performance W/sf, GJ/yr
Planned LEED certification LEED rating Initial and current LEED scorecard Actual LEED certification LEED rating

23
3.3.1 Schedules
Frequent schedule delays often result in reduced installation quality, due to accelerated
trades and out-of-sequence work. Research shows that traditional schedule analysis, which only
considers planned versus actual dates, is inadequate at explaining the reasons behind delays or
identifying the responsible party (Gransberg & Buitrago 2002). For this case comparison, the
goal of assessing schedule growth was to determine where and how the involvement of the
mechanical contractor in design and construction processes impacts schedule delays or improve
the delivery speed of healthcare projects. The metric to explain schedule changes was percent
growth, with positive values indicating late delivery and negative values showing early finish.
Additionally, separate consideration was given to the mechanical, design and construction
schedules to identify the timing of contractor involvement or requests for design feedback to
enable a stronger comparison between the project and building system-levels on each case.
3.3.2 Change Order Logs
Change orders are the most significant portion of cost growth on construction projects,
often leading to reduced productivity and re-work. Prior research implies that more integrated
processes, which allow the contractor to resolve conflicts during earlier phases of design, can
reduce the occurrence of change orders during construction. In a study limited to mechanical
contracting, the number of change orders relating to unforeseen conditions was reduced by 87%
on design-build projects, when compared to traditional design-bid-build deliveries (Riley, Diller,
et al. 2005). For the purposes of this comparative case study, the following categories of changes
were used to filter the mechanical contractor’s change order logs:
(1) Owner scope change: Owner-initiated, often discretionary;
(2) Contractor scope change: Contractor-initiated, value engineering suggestion or
product substitution approved by owner and designer;
(3) Unforeseen conditions: Contractor or designer initiated, existing site conditions differ
from expected;
(4) Error: Designer liability, incorrectly drawn construction plans or specifications;
(5) Omission: Designer liability, inadvertently omitting item or element from plans; and
(6) Award-Fee or Incentives: Owner-initiated, rewards for performance above and
beyond the original scope, considered cost of work.

24
To sort change orders into these categories, the following questions were answered:
(1) Who requested the change order?
(2) Why was the request made?
Once categorized, change orders were totaled to determine project cost growth and
mechanical system construction cost growth. Owner-initiated change orders, which request
adjustments to scope or design, are not always relevant in revealing differences attributable to
contractor involvement. However, owner-initiated changes provided insight into the owner’s
commitment to project goals, ability to define scope and likelihood of making timely decisions.
Unforeseen conditions, errors and omissions are categories where integrated design practices can
potentially decrease the occurrence and value of change orders and were relevant in highlighting
the divergence in mechanical system cost escalation between cases.
3.3.3 Quality Control Logs
Quality is often an indicator of design completeness and managerial competency of the
project team. Research indicates that the cost-of-quality (COQ), including prevention and failure
correction, can reach 18% of the project cost (Hall & Tomkins 2001). While the proposed
research will not perform a COQ analysis, qualitative assessments illustrated how mechanical
contractor design involvement may reduce instances or types of quality failures. The following
categories summarize the typical causes of quality deficiencies on construction projects:
(1) Communication: Poor information control or misunderstandings;
(2) Personnel: Carelessness, lack of training or poor workmanship;
(3) Management: Lack of planning, poor supervision or insufficient budget;
(4) Design: Complicated or unclear design;
(5) Materials: Defective or damaged materials; and
(6) Force Majeure: Third parties, weather or other uncontrollable conditions.
At a minimum, each case study’s quality control logs included: deficiency description,
responsible party, date opened, date closed and approval signature. From this information,
quality items concerning the mechanical trade were identified and tallied, although follow-up
discussions with the mechanical contractor were needed to clarify causal relationships and ensure
accurate categorization. For instance, installation errors may be attributable to a specific

25
individual, but the root cause could vary from worker inexperience, misunderstandings or poor
supervision. The goal of reviewing quality control logs was to generally correlate the frequency
and type of quality issues with differing levels of mechanical contractor design involvement.
3.3.4 Safety Reports
Construction activities account for nearly 19% of all workplace fatalities, the largest
percentage of any industry sector (U.S. Bureau of Labor Statistics 2008). The responsibility for
jobsite safety belongs with the project team, which often only considers hazard management
during the construction phase. Therefore, a more holistic view or awareness of safety risks,
during the design and planning phases, may improve project delivery. Safety reports were
collected from both the mechanical contractor and CM/GC to determine their current OSHA
recordable incident and lost time rates. The calculated rates were compared against the industry
standard rates for 2010, summarized in Table 3-2, for similarly sized companies. The goal of
documenting safety performance on these case studies was to determine if early contractor design
involvement and responsibility reduces the likelihood or improves awareness of construction
safety risks.
Table 3-2: Incidence rates for construction sector by size (U.S. Bureau of Labor Statistics 2008)
Industry sector
All establishments
Establishment employment size (workers)
1 to 10 11 to 49 50 to 249 250 to 999
1,000 or more
Construction 4.7 3.2 5.4 5.4 4.2 1.9
3.3.5 Energy Models and LEED Scorecard
Energy modeling is an effective method of optimizing HVAC systems by allowing
iterative comparisons of building systems to balance energy efficiency with cost-effectiveness.
Simulations are uniquely valuable during early stages of design, where building geometry,
geographical location, wall characteristics and owner operating schedules can assist in predicting
energy load profiles. For this case study research, collecting energy model results revealed how
integration of the mechanical contractor into design and construction activities impacted the
planned energy performance of each facility. As typically measured, the modeled energy savings
by cost is compared against the cost to operate an ASHRAE Standard 90.1-2001 baseline
building to determine the percent improvement.

26
As part of a highly regulated industry, healthcare facilities are often slower and more
cautious in adopting sustainable practices. According to the U.S. Green Building Council (2009),
only 1% of LEED certified buildings are healthcare facilities. Both case studies in this research
initially targeted a Silver certification under LEED NCv2.2 in accordance with public regulations
and funding requirements to deliver energy conserving buildings. LEED NCv2.2 defines Silver
certification as obtaining between 33 and 38 points, which establishes the success criteria for both
cases. Planned and as-submitted point totals were obtained from each project’s LEED scorecard
for comparison purposes and to understand differences in the key Energy & Atmosphere and
Indoor Environmental Quality categories.
3.3.6 Requests for Information
The request for information (RFI) process addresses inadequacies, errors,
misunderstandings or missing information in the construction drawings and specifications.
Formal responses require a time commitment from the design team and typically result in
contractor change orders, which subsequently delays or negatively impacts construction activities.
As another quantitative comparison, the RFI logs on both cases were collected and filtered to
assess only mechanical-related issues. The goal of reviewing the RFI logs is to determine if early
contractor involvement and design responsibility directly reduce the number of mechanical-
related RFIs.
3.4 Data Analysis Process
Unlike statistical analyses that follow a rigid set of methods or formulas, the organization
of case study data is considerably less structured and more dependent on the researcher's thinking
style and presentation of evidence (Yin 2003). Previous project delivery research utilized
statistics and regression models to match one or more process indicators with a specific outcome,
effectively addressing what variables are important in higher performance buildings, but not
directly explaining how or why these relationships work. Case study research can offer unique
insights into these indicator and outcome relationships by focusing on the real-life context,
circumstances and events surrounding a project. For instance, statistical analyses have correlated
design-build with reduced cost and schedule escalation, but what aspect of a design-build
organizational structure is impacting the outcome? As a single variable, the organizational

27
structure defines the party responsible for design, the degree of owner control of the design and
hierarchy for information flow between team members. This multiple-case comparative study
explored these types of multifaceted variable impacts, within the contexts of Case A and Case B.
3.4.1 Defining Project Attributes
Project attributes are the independent project variables, which are frequently determined
early in the project lifecycle and have impacts on the levels of team integration and involvement
of contractors. A listing of independent variables is provided in Table 3-3, along with a
subjective ranking associated with each variable. The low/medium/high designations are the
opinion of this researcher, conceived from a review of current literature on integrated
construction processes. They are not presented as proven concepts and are included only to form
qualitative determinations of the more integrated case study. The less documented and more
objective variables of owner commitment, team commitment and team characteristics are ranked
by tallying the indicators often associated with higher performance. This method of qualification
evenly considers each statement and does not imply that one indicator is more important or
weighted more heavily than another.
The indicators selected to represent owner commitment and team characteristics were
adapted directly from Korkmaz’s (2010) work, with minor modifications. Firstly, the “Owner
clearly defines scope” and “Owner makes timely decisions” indicators were shifted from team
characteristics to owner commitment. Since the team characteristics variable is intended to
aggregate all project team members, including designers, builders and owners, statements that
specifically reference one party would create an undesired weighting of the variable toward that
team member. Additionally, an owner’s ability to define scope and make timely decisions
appeared less of an intrinsic team characteristic and more the result of commitment to pre-project
planning and staffing decisions. Future research may find advantages in separating the single
team characteristics variable into multiple, more isolated variables unique to each team member
such as: designer characteristics and builder characteristics.

28
Table 3-3: Independent project variables with proposed level of integration ranking
Independent Variable Integration Description Owner Commitment
Vision statement Contractually mandated energy performance or LEED rating
“Green” introduced during Conceptual/SD Strong belief in sustainable concepts Owner is driving force Owner clearly defines scope Owner makes timely decisions
High (6+)
Number of indicators found in highly committed project owners.
Medium (3-5)
Low (0-2)
Team Commitment
Incentive/penalty clauses in contract Architect and contractor design responsibility No blame culture Completed common goals/objectives Valued team feedback and opinions Equal treatment of participants
High (5+) Number of indicators found
within highly committed project teams of designers and contractors.
Medium (3-4) Low (0-2)
Team Characteristics
Experienced with similar projects High competency owner representative Compatible personalities Open communication Located in common/shared offices
High (5+) Number of indicators found
within highly integrated project teams of owners, architects and contractors.
Medium (3-4) Low (0-2)
Contractor Contract Type Cost Plus Fixed Fee High Structure of contractor
contract with owner or CM/GC.
GMP Medium Lump Sum, Unit Price Low
Project Delivery Method Integrated Project Delivery, Design-Build High Overall project delivery
selected by owner. CMR, CMA Medium Design-Bid-Build Low
Contractor Procurement Strategy Best Value, Pre-Qualification High Method or process of
contractor selection. Negotiated, Fixed Budget/Best Design Medium Low Bid, Sole Source Low
Contractor Design Integration Pre-Design, Conceptual (<10%) High Timing of contractor
involvement on project. Schematic, Design Development (<75%) Medium Construction Documents, Bidding (100%) Low

29
The team commitment variable was created to recognize the importance of incentive
alignment between designers and builders, by describing how team integration and shared
responsibility can result in achievement of common project goals. Commitment is strengthened
by several factors, including monetary and non-monetary recognition, a sense of ownership and
opportunities for personal development. The indicators for team commitment summarized in
Table 3-3 were primarily adapted from studies conducted by Baiden (2006), where the extent of
team integration on construction sites was explored and verified over ten common factors in
literature. Six factors were selected, prior to data collection, as relevant to describing the context
of team commitment in this case study comparison. Since team commitment was not a
previously defined variable or indicator in existing project-level metrics, this variable is
experimental and under development for future research.
3.4.2 Causal Analysis and Explanation-Building
The process of relating measured outcomes with project attributes, as mapped in Figure
3-2, involved the following steps: (1) identifying contextual case outcomes based on
commonalities found within the in-progress performance metrics, (2) brainstorming potential
causes for differences in contextual outcomes using fishbone diagrams, (3) sorting causal listing
by occurrence to identify unique factors found on only one case, (4) grouping of unique causal
factors with influencing project attributes and (5) relating contextual outcome differences with
influencing project attributes. Common project attributes and similar measured outcomes present
in both projects were discarded, as theoretically impacting project and building system
performance equally in both cases in a two-case comparison. This analysis methodology
proposed and attempted an analytical, process-based approach to understanding how project
attributes impact both project and building system-level outcomes.

30
Figure 3-2: Map of data collection and data analysis process for case comparison
Sort by Pr
ojec
t Attribu
tes
Gro
uped
uni
que
caus
es a
s inf
luen
ced,
rela
ted
to o
r dic
tate
d by
a sp
ecifi
c pro
ject
attr
ibut
e
Caus
al Ana
lysis
Brai
nsto
rmed
pot
entia
l cau
ses f
or p
rim
ary
outc
ome
diffe
renc
es u
sing
fish
bone
dia
gram
s
Cont
extual Outco
me Differen
ces
Asse
ssed
per
form
ance
met
rics
to id
entif
y re
curr
ent t
hem
es a
nd c
omm
onal
ities
Sort by Occurrenc
eTa
bula
ted
pote
ntia
l cau
ses b
y ca
se o
ccur
renc
e to
iden
tify
uniq
ue c
ause
s for
a si
ngle
cas
e
Projec
t Attribu
te Differen
ces
Iden
tifie
d re
cord
ed d
iffer
ence
s in
cont
ract
ty
pe, o
rgan
izatio
nal s
truc
ture
, etc
.
Relate Pr
ojec
t Attrib
utes to Outco
mes
Use
d re
latio
nshi
p-bu
ildin
g di
scus
sion
to c
ausa
lly d
escr
ibe
how
diff
eren
ces i
n pr
ojec
t attr
ibut
es re
sulte
d in
mea
sure
d di
ffere
nces
in p
roje
ct a
nd b
uild
ing
syste
m o
utco
mes
Data
Analy
sis Pr
oces
s

31
3.5 Summary
The research goal was to understand how an integrated design and construction process,
which included early involvement of the mechanical contractor, impacted building system and
project performance. The study performed a comparative analysis of two similar hospital
construction projects, using the variable notation established by prior research. The data
collection process included a combination of onsite observation, multiple data sources, follow-up
correspondence and the creation of performance metrics to describe case outcomes. Data was
primarily obtained from project documents, including change order logs, schedules, RFIs, safety
reports, QA/QC logs and LEED paperwork. Once collected, the data analysis process involved a
causal analysis, sorting potential causes by case occurrence, linking causes with influencing
project attributes and finally relating the original contextual outcome differences with project
attributes to understand the contributions of an integrated process.

32
Chapter 4
DATA COLLECTION
4.1 Case Study Background
As discussed in Chapter 3, a nationally recognized mechanical contractor approached the
Penn State Department of Architectural Engineering with two new hospital projects, located in
the Northeastern United States. Both projects were purported to have certain similarities,
including facility size, type, location and sustainable goals, while differing in organizational
structure and mechanical design approach. Therefore, an exhaustive case study selection or
screening procedure was seemingly not necessary and not performed. Instead, the researcher
assumed the role of an independent evaluator, carefully reviewing project documents, comparing
performance metrics and attempting to understand their relationship to outcomes. However, prior
to gathering detailed project information, the researcher conducted a preliminary fact-finding
inquiry and vetting of both selected cases. Similar to a feasibility study, this early evaluation
tested the viability and worthiness of the offered cases for allowing an in-depth comparison. The
goals of the investigation included:
(1) Verify similarities in control variables: Building type, size, location and other
project-defining attributes that remain constant and either strengthen or weaken a
case comparison depending on their similarity.
(2) Confirm access to project data: Ease of obtaining project documents, meetings with
team members and permission to use case data for research purposes.
(3) Identify key team members: Project participants or stakeholders with detailed
knowledge of the design and construction processes, history and challenges of each
case.
The inherent strength of the comparative case study results from many similarities in the
control variables observed on both projects, which are highlighted throughout this chapter. For
instance, an early inspection of both cases revealed an unexpected and shared context surrounding

33
their construction, which involved the closing of an existing healthcare facility and dividing the
previously offered medical services between the Case A and Case B facilities.
4.1.1 Case A Overview
Case A was structured as a design-build (DB) delivery and contracted as a joint-venture
between a CM/GC and architecture firm. Prior to awarding the DB contract, the owner on Case
A engaged a separate designer to assist in program development and the creation of bridging
documents for the Request for Proposal (RFP) package. When awarded to contractors, the
architectural design was approximately 30% complete and MEP design was nearly 10%
complete. Despite using a design-build delivery method, the facade and many architectural
elements of Case A were predetermined by the surrounding buildings. The exterior design of
Case A was mandated to closely resemble nearby, existing buildings with historical significance,
which governed strict requirements for the number of floors, building elevation and orientation
and removed some control and flexibility from the design-build team. The anticipated total
construction cost for Case A was greater than $500-million at the time of data collection and
includes the following major phases:
• Phase 1 (> 500,000-ft2): New multistory facility, with combination of in-patient hospital
beds and out-patient clinic offices.
• Phase 2 (> 250,000-ft2): Renovation of existing hospital rooms to include state-of-the-
art medical equipment and services.
• Hospital-to-Clinic Gross Area Ratio: 1:3.4 (excluding renovation scope)
For simplification purposes, the Case A renovation scope is excluded from any case
study comparisons. Renovation projects typically include unforeseen or existing conditions and
extensive off-hour work, which precludes a direct comparison with the exclusively new
construction on Case B. Therefore, the Case A renovation scope in Phase 2 was carefully
separated and excluded from the collected data, leaving only the contributions from Phase 1.

34
4.1.2 Case B Overview
Case B was organized as a CM at risk delivery, with significant design and construction
overlap planned over the project duration. While contractors were not involved in design
activities until the RFP process, the architect was a multi-disciplinary firm, engaging in integrated
mechanical, electrical and structural design with in-house structural and MEP engineers. The
architectural design was nearly 40% complete and the MEP design at 25% complete when the
construction contract was awarded to the CM/GC. At the time of data collection, the project cost
of Case B was greater than $750-million and planned to deliver the following:
• Phase 1 (> 1,000,000-ft2): New, interconnected, multistory facility with a combination
of in-patient hospital space and out-patient clinic offices.
• Hospital-to-Clinic Gross Area Ratio: 1:1.7
According to the project team on Case B, the organizational structure used was described
as a modified design-bid-build approach, meaning that the traditional design-bid-build delivery of
separate design and construction contracts was supplemented with elements of early contractor
involvement. However, design-bid-build concept reported by the project team is functionally
identical to the accepted definition of a CM at risk organizational structure, which adds design
flexibility and schedule fast-tracking, without sacrificing owner control of the design. To avoid
potential confusion over the precise meaning of the modified design-bid-build approach, this
research will use CM at risk to describe the organizational structure of Case B.
4.2 Summary of Control Variables
The strength of conclusions drawn from comparative case studies arise from similarities in
the external environment, or control variables, which establish a reference point and reduce the
likelihood of alternate explanations for measured differences between projects. Rarely are one-
of-a-kind buildings comparable to each other in the construction industry; however, the generally
accepted variables for testing sameness include the following:
• Location impacts project outcomes primarily by dictating the availability of local and
skilled contractors, the types of systems used, the standard of care for designers and
various code or permitting requirements. From a design perspective, since few regional

35
requirements existed prior to LEED v3.0, certain credits are easier to obtain in less severe
or fluctuating climates. Additionally, some cities or jurisdictions offer incentives for
advancing sustainable building features.
• Project type refers to the differences inherent to the public and private sectors. Private
projects exhibit more variation in delivery, whereas public projects typically must adhere
to applicable statutes or directives that govern bidding, contract administration and other
functions of the construction process.
• Building size impacts economies of scale, the number of qualified contractors available to
bid and the amount of management or oversight needed for the project.
• The function of a building dictates how end-users will occupy and operate the facility.
There are common systems, materials, complexities and construction methods employed
on similar building types, which improve the validity of like-with-like comparisons.
• LEED certification represents the completion of sustainability goals, which establish the
design direction and performance of projects. As credit requirements become more
stringent with each revision, the separation grows drastically between a LEED-rated and
non LEED-rated facility. Since both projects were under construction during data
collection and not yet LEED certified, the target rating provided in the RFPs was used to
define this control variable.
Although not explicitly identified in prior research, the scope of work for the mechanical
contractor may also be considered a control variable for a building system-level analysis. In both
Case A and Case B, the contractor was responsible for all HVAC equipment, air distribution
systems, mechanical piping, control systems, insulation and commissioning. The mechanical
system designs on Case A and Case B differed in several aspects, including the percentage of
outdoor air, heat recovery methods and space control as discussed in additional detail in Chapter
5, but the design guidelines and codes followed are similar for all healthcare facilities.
Both cases display strong similarities in control variables as shown in Table 4-1, with the
exceptions of location and size of each facility. Since neither case location was included in the
R.S. Means 2010 location adjustment tables, values from the nearby cities were assumed for Case

36
A and Case B. The percent difference between these location factors is less than 5%, which
indicates similar material and labor costs between projects. In reference to size, the Case B
project is nearly double the gross square-footage of Case A, which traditionally limits the
reasonableness of comparisons. However, cost estimating sources, such as R.S. Means, indicate
that significantly large healthcare projects above 192,500 square-feet show similarities in unitized
construction rates and system breakdowns.
Table 4-1: Summary of control variables for Case A and Case B
Project Location Type Function Size (ft2) LEED Certification
% Complete at Data Collection
Case A NE U.S. Public Hospital/Clinic > 500,000 Silver 90% Case B NE U.S. Public Hospital/Clinic > 1,000,000 Silver 75%
4.2.1 Validating Differences in Project Size
According to R.S. Means 2011 cost references, building size impacts the cost per square-
foot due to the decreasing contribution of exterior walls and economies of scale inherent in larger
projects. The calculation of a “size factor” is achieved by dividing the proposed or actual
building area by R.S. Means’ typical area for the building type. The result of this calculation is
summarized on Table 4-2, using the typical areas of 7,200-ft2 for clinics and 55,000-ft2 for
hospitals. With clinic size factors of 78 for Case A and 113 for Case B, both projects are
significantly larger than the mean medical office area collected by R.S. Means. Similarly, the
hospital size factors of 3 for Case A and 9 for Case B are many times larger than the mean
hospital area. The “cost multiplier” is obtained graphically, using the area conversion scale
provided by R.S. Means. However, since the size factors obtained in both cases are greater than
3.5 and asymptotically approaching a constant on the cost multiplier curve, R.S. Means
recommends using a cost multiplier of 0.90. Therefore, although the gross square-footage is
different between cases, the cost impacts for the variance in size are expected to be minimal.
Table 4-2: Calculated R.S. Means size factors and cost multipliers
Case A Case B R.S. Means Size Factor
R.S. Means Cost Multiplier
R.S. Means Size Factor
R.S. Means Cost Multiplier
Clinic 78 0.90* 113 0.90* Hospital 3 0.91 9 0.90*
* R.S. Means note: For Size Factors greater than 3.5, the Cost Multiplier is 0.90.

37
4.2.2 Validating Differences in Clinic-to-Hospital Area Ratios
In addition to differences in gross square-footage, the clinic-to-hospital ratios are notably
dissimilar on both cases, which require further analysis to support the validity of comparison. As
shown previously in the case study overviews, Case A has a clinic-to-hospital gross area ratio of
3.4:1, compared with the Case B ratio of only 1.7:1 In other words, the Case A facility area is
distributed as three parts clinic to one part hospital, while the Case B facility is nearly two parts
clinic to one part hospital. To determine how this difference in area usage affects the cost of each
project, R.S. Means unit rates were consulted for Hospitals (4-8 Story) and Medical Offices
(Multistory). The high-end unit rates were selected from the R.S. Means square-foot estimate
tables to provide an upper limit, encompassing high-end finishes and methods of construction.
These rates where multiplied by the separate clinic and hospital areas on each case, rounded,
summed and then divided by the combined gross square-footage of the project. The result is an
overall building unit rate shown in Table 4.3, adjusted for the differences in clinic-to-hospital area
ratios. Using this methodology, the estimated unit costs of Case A and Case B are $261 and $263
per square-foot, respectively. As base R.S. Means rates, these values do not include site work,
general conditions, bonds, insurance or other additions commonly needed for construction.
However, two important conclusions are derived from the total combined unit rate in Table 4-3:
(1) the difference between the Case A and Case B unit costs are less than 5% and, (2) the
proportionally larger hospital area on Case B results in a higher unit cost than Case A. Based on
this estimate, the differences in clinic-to-hospital area ratios imply that similar cost per square-
foot rates should be encountered on both cases, with a potentially higher rate on Case B.
Table 4-3: Estimated project unit cost, adjusted for differences in use areas between cases
Hospital –to-Clinic Area Ratio
Estimated Unit Cost ($/ft2)*
Case A 1:3.4 $261 Case B 1:1.7 $263
*Calculated using R.S. Means and adjusting for differencing in hospital-to-clinic ratios

38
4.3 Sources of Project Data
As established in Chapter 3, quantitative data was derived from a combination of project
documentation, onsite observation and informal discussions with key team members. Since both
projects were under construction and at differing stages of completion, a one-week duration
jobsite visit was performed for each case. The majority of data for Case A was collected over the
week of July 12-16, 2010. Case B data was obtained the following week, July 19-23, 2010. At
the time of data collection, Case A was approximately 93% complete and amid commissioning
and punch list activities on Building A and Building B. Construction at Case B was considerably
more active, with an approaching interim turnover date for two clinic buildings and tracking
towards 76% project completion. Following the initial compilation of case data into
spreadsheets, follow-up emails and phone calls were initiated to fill any gaps in information and
to confirm key dates or values.
4.3.1 Project Documentation
RFIs, change order logs, schedules, quality control reports, safety statistics and meeting
minutes were obtained from the party responsible for creating, updating and managing the project
document. For instance, mechanical contractor change order logs were obtained from the
mechanical contractor, while quality control reports originated from the design-build architect on
Case A and CM/GC on Case B. Approximately 50% of the project documentation was collected
in hardcopy format and 50% in electronic media, including spreadsheets and PDFs. Each
document was reviewed and sorted, as outlined in Chapter 3, to extract the specific information
needed to calculate the performance metrics. Where practical, variables were identified primarily
with project documentation, instead of team discussions or interviews, to avoid potential
researcher bias.
4.3.2 Site Observations
Some project variables are not directly measureable or quantitatively assessable.
Observational studies allowed the researcher to subjectively assess team interaction,
communication and culture within the day-to-day jobsite activities. Weekly coordination
meetings, which included safety, commissioning and construction topics, were the primary source
of observational data on both cases. During each meeting, the researcher was introduced as a
graduate student performing a case study on the project and, in all cases, was allowed to observe

39
the meeting participants. The observations noted during both jobsite visits are important in
defining the “team commitment” and “team characteristics” independent variables.
4.3.3 Semi-Structured Interviews
Similar to site observations, informal discussions with key team members were necessary
to describe the independent variables of “team commitment” and “team characteristics”. The
researcher approached each team member with a prepared list of questions with a semi-structured
interview approach, provided in Appendix B, but allowed the discussion to evolve with stories or
examples of team interaction. The goal of these discussions was not to obtain verbatim
transcripts or records, but rather to assist in characterizing each project team for the purposes of
case comparison.
4.4 Summary of Independent Project Variables
The combination of organizational structure, contract type, procurement strategy and
team elements form a set of independent project variables. Project delivery decisions impacts
processes, team interactions and methodologies, which remain relatively constant during the
design and construction of a facility. These interactions are discussed further in Chapter 5, when
building cause and effect relationships between the independent project variables and measured
outcomes on each case.
4.4.1 Contract Type, Organizational Structure, Procurement, Design Integration
The most influential delivery decisions suitable for consideration as independent project
variables, as suggested by Korkmaz (2010) and Chan (2002), include the following:
• The contract type defines the structure of compensation between the owner and GC/CM,
establishing incentive or penalty clauses and allocating risk between parties. Typical
contract types include cost plus fee (CPF), guaranteed maximum price (GMP), lump sum
(LS) and unit price (UP).
• The organizational structure, as selected by the owner, establishes the team hierarchy,
flow of information and service integration for the project. Choices include integrated

40
project delivery (IPD), design-build (DB), construction manager at risk (CMR) and
agency (CMA), and design-bid-build (DBB).
• Procurement refers to the owner or GC/CM’s method of acquiring mechanical
contracting services. Typical method include best value (BV), pre-qualification (PQ),
negotiated (NE), best design (BD), low bid (LB) and sole source (SS).
• Design integration establishes a level for the earliest timing of mechanical contractor
involvement in the design process. This level does not attempt to quantify the
contribution as more beneficial or constructive, but rather indicates only when contractor
assistance was requested.
A summary of the project delivery variables is provided in Table 4-4. Despite similar
procurement strategies, the most significant differences between Case A and Case B are the
organizational structure, design integration and contract type. Therefore, the case comparison
will strive to understand how the combined effects of design-build with a lump sum contract
compare with a CM at risk and cost plus fee contract to delivering similar healthcare facilities.
Table 4-4: Summary of project delivery independent variables for Case A and Case B
Project Contract Type Organizational Structure Procurement Design Integration Case A Lump Sum Design-Build Best Value 30% Arch. / 10% MEP Case B Cost Plus Fee CM at Risk Best Value 40% Arch. / 25% MEP
4.4.2 Owner Commitment
Generally, “owner commitment” measures the dedication of the owner to implementing
sustainable concepts and providing clear direction on the project. Depending on the strength of
commitment, these “big picture” goals may or may not trickle down to the building system-level.
Prior research by Ling (2004) and Korkmaz (2010) revealed the owner’s instrumental role in
identifying sustainability goals during early design phases and offered several indicators to gauge
levels of commitment:
• A vision statement provides the inspiration and framework for planning the project. To
receive credit for this indicator, the statement must be included in the owner’s RFP
documentation to the GC/CM or mechanical contractor.

41
• Contractual LEED requirements hold the mechanical contractor responsible for meeting
the sustainability goals of the building, typically under the energy performance
guidelines. The contractor must indicate a contract clause or scope inclusion holding
them liable for the performance of mechanical systems.
• Introducing LEED during the conceptual design or design development phases
increases the likelihood of sustainable concepts becoming fundamental to the project,
rather than a last minute add-on. Documentation must indicate that LEED requirements
were added prior to the schematic design phase of mechanical system design.
• A strong belief in sustainable concepts ensures that all aspects of the building, including
energy efficiency, materials, indoor air quality, water conservation and site usage are
treated or reviewed equally. Documentation must reveal a whole-building, lifecycle
approach to sustainable design, not lacking significantly in any LEED category.
• Having the owner as a driving force ensures that sustainable goals remain a high-priority
during design and construction. Projects must indicate, either by documentation of
responsibilities or meeting minutes, that the owner maintains high levels of involvement
in the sustainable design process.
The definition of owner commitment was derived primarily from the perspective of high-
performance green (HPG) buildings and does not necessarily include commitment to the project
cost or schedule goals. Previously included as criteria for the independent project variable of
“team characteristics”, the owner’s ability to define scope and make timely decisions are arguably
more indicative of commitment. For example, a clear project program or decision-making
procedure is less of an inherent owner characteristic and more a marker of strong commitment to
predetermined project goals. Therefore, as discussed in Chapter 3, this research expands on the
HPG definition of “owner commitment” to include the following indicators:
• An owner clearly defines scope by incorporating end-user feedback early in design and
communicating change directives without ambiguity. As the prime contract-holder with
the owner, the builder’s opinion was used to gauge the overall effectiveness of the owner
at defining project scope.

42
• An owner making timely decisions ensures that the design process proceeds at pace with
construction and minimizes the likelihood of change orders causing significant
interruption. Similar to scope definition, the builder’s opinion was again requested to
qualify the owner’s ability to make decisions, without affecting the flow or progress of
work.
Table 4-5: Data sources for determining owner commitment
Documents Observation Semi-Structured Interview • Vision statement • Contractual LEED requirement • Introduced LEED during CD or
DD phases of design • Strong belief in sustainable
concepts • Owner is driving force
• Owner clearly defines scope • Owner makes timely
decisions
Project documents and semi-structured interviews were the primary source for
determining evidence of “owner commitment” indicators, as shown in Table 4-5. After
reviewing the RFP and mechanical contract documents, a summary of the findings was prepared
in Table 4-6, which reveals a distinct difference between the levels of owner commitment on each
project. A complete tabular version of the evidence is provided in Appendix B. Case A
demonstrated six of the seven indicators, whereas Case B received credit for two, lacking a vision
statement and contractual LEED requirement to the mechanical contractor. Additionally, the
Case B documents emphasized the architect’s role as the driver of sustainable concepts instead of
the owner. Perhaps due to hierarchies within large public owners, neither builder indicated that
owner decision-making was a timely process.
Table 4-6: Summary of owner commitment independent variable criteria
Criteria: Owner Commitment Case A Case B Vision statement Contractual LEED requirement Introduced LEED during CD/DD Strong belief in sustainable concepts Owner is driving force Owner clearly defines scope Owner makes timely decisions
Total indicators 6 2

43
4.4.3 Team Commitment
As discussed in Chapter 3, the independent variable “team commitment” is based on the
number of integration indicators found and observed on each project. These indicators, as
summarized below, are statements or patterns indicative of highly committed project teams
adapted from Baiden (2006):
• Incentive clauses may appear as performance-based contractor award-fee or shared cost
savings recognized from exceeding specific schedule and budget targets. To receive
credit for this indicator, the mechanical contract must include a provision for
performance incentive, relating to the design and/or construction of HVAC systems.
• A shared architect and contractor design responsibility distributes a portion of the
system performance liability to the constructor, attempting to collectively manage and
appropriately share design risks. The mechanical contract must indicate a performance-
based liability to assist with or fully design a functional HVAC system.
• A “blame culture” is prevalent when the initial reaction to design problems is blaming
other team members as the source of the conflict, rather than accepting responsibility and
working towards a solution. An example of managing an unexpected jobsite problem or
design issue was used to assess the combined team atmosphere of owner, architect and
contractors.
• Completing common goals results from an awareness of broader project objectives and
commitment to working towards the best interest of the whole project, rather than any
individual stake. All team members must demonstrate, via example or documentation, a
group effort in achieving mechanical design goals.
• Valuing team feedback and opinions demonstrates a willingness to respect differing
ideas, weighing carefully the input of each participant without disparagement.
Observation of project meetings was used to subjectively assess if contractor opinions
were solicited and valued.

44
• An equal treatment of team participants strengthens commitment by fostering an
atmosphere of cooperation. However, since many construction projects follow a tiered or
hierarchical contract structure, equal involvement of all parties is difficult to achieve in
practice.
Table 4-7: Data sources for determining team commitment
Documents Observation Semi-Structured Interview • Incentive clauses in contract • Shared architect &
contractor design responsibility
• Lack of “blame culture” • Valued team feedback &
opinions • Equal treatment of
participants
• Completed common goals
A combination of documents, site observation and team discussions were used to
determine the presence of team commitment indicators, as shown in Table 4-7. Simplifying the
tabular evidence in Appendix B, Table 4.8 provides a summary comparison of the indicators
found on both cases. Case A demonstrated a total of five indicators, including: a performance-
based award-fee program, mechanical contractor design liability, working towards common goals
and valuing of team feedback. Case B showed strength in only two areas, completing common
goals and valuing feedback from team members.
Table 4-8: Summary of team commitment independent variable criteia
Criteria: Team Commitment Case A Case B Incentive clauses in contract Shared architect & contractor design responsibility Lack of “blame culture” Completed common goals Valued team feedback & opinions Equal treatment of participants
Total indicators 4 2

45
4.4.4 Team Characteristics
As the most subjective independent variable, “team characteristics” is an aggregate
assessment of the owner, builder, architect and mechanical contractor. The purpose was not to
determine an individual team member’s characteristics, but rather to view the team as a whole.
The following indicators are representative of highly functioning and highly integrated project
teams:
• Prior experience with similar projects allows teams to reuse old lessons and learn from
previous mistakes, improving the delivery of future projects. The prior work history of
the owner, architect, GC/CM and mechanical contractor must reveal projects of similar
size and type completed within the past 10-years.
• A high competency owner representative demonstrates familiarity with the design and
construction process, having both the available resources to manage contract
administration and the authority to make decisions.
• A team composed of compatible personalities typically results in smoother, less conflict-
driven interactions. This indicator was awarded based on meeting observations and
informal team discussions, which must reveal little or no evidence of problems caused by
conflicting personalities.
• Open communication is present when the free exchange ideas, objections and documents
are encouraged within teams. Observations of open team interactions and the presence of
web-based document management software were used as requirements for this indicator.
• Locating teams in shared or common offices improves collaboration by strategically
housing contractors, designers and the owner within the same workspace. A consolidated
layout of field offices was necessary to receive credit for this indicator.

46
Table 4-9: Data sources for determining team characteristics
Documents Observation Semi-Structured Interview • Compatible personalities
• Open communication • Located in shared/common
offices
• Experienced with similar projects
• High competency owner representative
• Owner clearly defines scope • Owner makes timely decisions
Indicators for “team characteristics” were either observed directly during jobsite visits or
revealed by example during discussion with key team members, as shown in Table 4-9. No
documentation was used to determine this variable. A full version of the evidence is provided in
Appendix B, but a summary in Table 4-10 illustrates how both cases have similar team
characteristics. Case A and Case B both received credit for four indicators. Both cases have an
owner, architect, builder and mechanical contractor team with prior experience on large facilities,
public work and clean room construction processes. The owners are highly competent, having
managed large-scale construction projects in the public sector. The interaction among team
members on both jobsites was generally amicable and information flow was open. The
researcher did not observe any specific instances of conflicting personalities, although strong
opinions were often presented during contractor meetings. Neither project used the concept of
collocation or shared offices for team members; however, the separate construction trailers were
conveniently connected with a boardwalk to encourage travel between offices.
Table 4-10: Summary of team characteristics independent variable criteria
Criteria: Team Characteristics Case A Case B Experienced with similar projects High competency owner representative Compatible personalities Open communication Located in shared/common offices
Total indicators 4 4

47
4.5 Summary of Dependent Outcome Variables
Dependent outcome variables include schedule and cost growth, quantity of RFIs, quality
control reports, safety statistics, LEED points and energy performance. The remainder of Chapter
4 presents a “snapshot” of the project at the data collection date and includes calculations or
metrics based on the raw information gathered from project documents. Detailed tables, with raw
data prior to calculation, are not provided due to privacy requests by both case owners.
4.5.1 Schedule Growth
Schedule growth typically refers to the percentage difference between the planned and
actual project duration, from design start to final completion. Since this research specifically
focuses on contributions from the mechanical contractor, metrics for assessing overall design,
mechanical design and construction schedule growth were added to provide additional levels of
detail. Baseline and current construction schedules were obtained from the CM/GC to enable a
comparison between planned and actual durations. When not included on the construction
schedule, planned design deliverable milestones were obtained from the project owner. Actual
design completions were determined from the date on 100% Issued for Construction (IFC)
drawings provided to the project team. All duration calculations were based on calendar days,
without subtracting holidays, weather impacts or periods of low productivity. Where exact dates
were unavailable, the middle of the month was assumed for calculation purposes. For example, a
date listed as March 2009 was entered as March 15, 2009, thereby limiting the potential for error
to only fifteen days.
The results of the case study schedule analyses are provided in Table 4-11, with all
percent growth values rounded to the nearest 5% to protect the anonymity of both cases and
separated into categories of project, overall design, mechanical design and construction. No
schedule changes were measured on Case A in any category, whereas Case B experienced a range
of schedule growth between 25% at the project level and 55% for the mechanical system design.
To allow a fair comparison, accounting for differences in gross square-footage between cases,
durations were unitized or given on a per area basis. While the planned duration per area rates
are dramatically different on both cases, the actual duration per area rates show more similarity.
For instance, the planned mechanical design duration on Case A was 0.57 days per thousand
square-feet and remained nearly constant. However, the planned mechanical design duration on
Case B started at 0.35 days per thousand square-feet and escalated to 0.55 days per thousand

48
square-feet. A similar occurrence is apparent in the planned and actual construction durations,
where Case B finished at 1.08 days per thousand square-feet, closer to Case A at 1.16 days per
thousand square-feet performance. In terms of actual construction time, Case B appears faster in
metrics of duration per inpatient bed, area installed per day and Cost of Work installed per month.
Table 4-11: Summary of schedule performance data for Case A and Case B
Project Schedule Calculations Case A Case B Project schedule growth 0% 25% Planned project duration per area (days/ksf) 1.85 1.09 Actual project duration per area (days/ksf) 1.83 1.36 Overall Design Schedule Calculations Case A Case B Design schedule growth 0% 30% Planned design duration per area (days/ksf) 1.22 0.59 Actual design duration per area (days/ksf) 1.19 0.75 Mechanical Design Schedule Calculations Case A Case B Mechanical design schedule growth 0% 55% Planned mech. design duration per area (days/ksf) 0.57 0.35 Actual mech. design duration per area (days/ksf) 0.57 0.55 Construction Schedule Calculations Case A Case B Construction schedule growth 0% 30% Planned construction duration per area (days/ksf) 1.18 0.81 Actual construction duration per area (days/ksf) 1.16 1.08 Construction duration per impatient bed (days/bed) 16.7 11.7 Area installed per day (ft2/day) 866 924 Cost of Work installed per month ($/30 days) $19,700,000 $20,800,000
4.5.2 Cost Growth
Cost growth measures the percentage difference between planned and actual project cost,
from initial contract signing to the final change order. However, since both cases were under
construction at the time of data collection, final contract values from the GC/CM and mechanical
contractor were not available. Instead, the most recent change order logs were used to estimate
the projected project and mechanical contractor cost at final completion. As discussed in Chapter
3, the change order logs were also examined to categorize the cause or initiator of changes to the
mechanical contract. To impose a fair comparison between a design-build and design-assist
delivery, the design contract for Case B was added to the construction contract value prior to
performing cost calculations. This addition ensures that the total project cost for both cases
includes both the design and construction costs of the facility. The results of the case study cost
analyses are provided in Table 4-12 and rounded to nearest whole values where appropriate.
Since a large proportion of the mechanical contractor change orders on Case A were attributed to

49
award-fee incentives, values within parentheses in Table 4-12 have removed the award-fee
change orders.
Table 4-12: Summary of cost performance data for Case A and Case B
Planned Cost Case A Case B Planned project cost per bed ($/inpatient bed) $9,800,000 $5,700,000 Planned project cost per square foot ($/ft2) $675 $525 Planned mechanical construction cost per square foot ($/ft2) $150 $115 Actual / Anticipated Cost Case A Case B Anticipated project cost per bed ($/inpatient bed) $10,900,000 $8,100,000 Anticipated project cost per square foot ($/ft2) $760 $750 Anticipated mechanical construction cost per square foot ($/ft2) $160 $155 Cost Calculations Case A1 Case B Project cost growth 12% (10 %) 43% Mechanical contract cost growth 8% (6%) 34% Mechanical Change Order Calculations (by $ value) Case A1 Case B Percentage approved owner-initiated CORs 38% (54%) 76% Percentage approved contractor-initiated CORs 22% (31%) 6% Percentage approved unforeseen conditions CORs 10% (15%) 0 % Percentage approved design error CORs 0 % (0 %) 5% Percentage approved design omission CORs 0% (0 %) 13% Percentage approved award fee/incentive CORs 30% (0%) 0 %
1Percentages in parentheses are without award-fee changes issued to the mechanical contractor.
As discussed earlier in Chapter 4, despite differences in gross square footage and clinic-
to-hospital area ratios, the rough R.S. Means cost per square foot rates were predicted to be
similar for both facilities. However, the planned project unit costs of $675 per square foot on
Case A and $525 per square foot on Case B differ by nearly 30%. Potential reasons for the
difference in planned project unit rates could include any combination of variations in the scope
of site work, larger than expected economies of scale, completeness of bid documents at RFP, and
accuracy of estimates or evolution of the scope since initial project definition. Conversely, as
measured, the actual project unit costs of $760 per square foot on Case A and $750 per square
foot on Case B are more consistent with the difference predicted by the R.S. Means analysis,
adjusted for difference in clinic and hospital areas. The project cost growth corresponding to the
planned and actual unit rates on Case A and Case B are 12% and 43%, respectively. Notably, the
mechanical unit costs follow a similar pattern as the project unit costs, resulting in mechanical
cost growth values of 8% on Case A and 34% on Case B.
Review of the mechanical Change Order Requests (CORs) reveals differences in the
distribution of change orders on both case studies. The owner-initiated changes, typically

50
resulting from end-user modifications or upgrades, on Case A were nearly 40% of the total,
compared to approximately 75% on Case B. Case A claimed 20% of changes as contractor-
initiated and 10% from unforeseen conditions, compared to Case B’s 6% and 0% in the same
categories. From a design perspective, Case B showed slightly less than 20% of changes due to
errors and omissions, whereas Case A had no changes directly attributable to the completeness of
design. This result was expected due to the design-build delivery method on Case A, which
entrusts the HVAC design and construction responsibility to the mechanical contractor. Incentive
change order requests (CORs) on Case A accounted for nearly 30% by value of the total change
orders issued to the mechanical contractor. While not always considered a cost of the work,
incentive plans are costs incurred by the owner to encourage and reward contractor performance.
Therefore, the award fee was deemed an important management tool and all costs in Table 4-12
include incentives unless noted otherwise. No award fee or incentive program was present on
Case B.
4.5.3 Requests for Information
The quantity of Requests for Information (RFIs) on Case B was significantly higher than
Case A, as shown in Table 4-13. The calculations were based on the total number of RFIs issued
by the GC/CM to the owner, designer or outside consultant and total number of RFIs associated
with HVAC systems and the mechanical contractor. The data does not include internalized RFIs
between the mechanical contractor and GC/CM in the case of design-build delivery. Therefore,
the quantity of RFIs on Case A is expected to be lower. Since the purpose of RFIs is to clarify
the intention of the contract drawings and specifications, they were not sorted into any specific
categories, other than a separation of mechanical-related RFIs. When unitized by gross square
footage and anticipated project cost, the difference in quantity of RFIs was nearly double, as
evidenced by comparing Case A at 1.69 RFIs per thousand square feet and 2.23 RFIs per million
dollars with Case B at 3.03 RFIs per thousand square feet and 4.23 RFIs per million dollars.
When normalized for actual construction duration, the difference in RFIs was almost triple, with
Case A at 0.99 RFIs per day and Case B at 2.92 RFIs per day. Perhaps a result of design-build
delivery, the percentage of mechanical RFIs was slightly under 5% on Case A and approximately
15% on Case B.

51
Table 4-13: Summary of RFI data for Case A and Case B
RFI Calculations Case A Case B Project RFIs per thousand square feet (RFI/ksf) 1.69 3.03 Project RFIs per million dollars of anticipated project cost (RFI/$) 2.23 4.23 Project RFIs per day of construction duration (RFI/day) 0.99 2.92 Percentage of mechanical RFIs to total project RFIs 5% 16%
4.5.4 Quality Control Reports
Despite differing management responsibility of the quality control (QC) logs, the actual
process of generating, tracking and approving QC issues was similar between cases. On Case A,
the design-build architect, as contracted with the GC/CM, performed all QC administration. On
Case B, the GC/CM directly managed QC, adding any items noted by the architect during
inspections or walkthroughs. Both cases presented similar appearing logs, individual reports and
a plan for managing non-compliance. The award fee program on Case A listed quality
compliance as a condition of success and was subject to review at quarterly intervals.
Unfortunately, both cases allowed work-to-complete and punch list reports to become
intertwined with the normal QC and quality assurance (QA) logs. Work-to-complete reports
track partially complete or incomplete contract scope, whereas punch lists include mostly defects
or discrepancies related to completed scope. Although the quality control logs were not sorted by
category, a number of non-quality issues were observed while tallying the quantity of mechanical
reports. Frequently during phased construction projects, the distinction between poor quality and
incomplete work becomes blurred, especially when contractors are working in multiple areas
simultaneously. For instance, is a missing pipe weld a sign of poor quality or simply incomplete
work? This inconsistency in documenting quality control issues makes drawing conclusions
based on project QA/QC performance difficult and somewhat speculative. Nevertheless, a
summary of the quality control report data is provided in Table 4-14.
Table 4-14: Summary of quality control and quality assurance data
QC/QA Calculations Case A Case B Project QC reports per thousand square feet (QC/ksf) 1.02 0.65 Percentage of "Open" QC reports to project total 6% 33% Percentage of mechanical QC reports to project total 9% 19%

52
The unitized metric for QC/QA shows fewer QC reports on Case B at 0.65 reports per
thousand square feet, compared with Case A at 1.02 reports per thousand square feet. When
considered with the observed, but not quantified addition of work-to-complete and punch list
items, the difference in project completion at the time of data collection may be partially
responsible for low number of reported quality issues on Case B. Of the total QC reports, Case B
demonstrated a higher percentage of “open” or unresolved quality concerns and a higher
percentage of mechanical-related QC issues.
4.5.5 Safety Reports
Both cases demonstrated similar safety programs, with slight differences in transparency,
but the Case A case has fewer recorded incidents in OSHA’s safety metrics of Recordable
Incident Rate (RIR) and Lost Time Case Rate (LTC). The calculation results from the collected
safety statistics are listed in Table 4-15. Both the project RIR of 3.74 and mechanical contractor
RIR of 4.60 were nearly three times greater on Case B , when compared to Case A’s project RIR
of 0.97 and mechanical contractor RIR of 1.65. The differences in LTC are also significant, with
Case B showing a rate of 0.53 and Case A at a much lower rate of 0.08. The correlation between
project and mechanical contractor safety performance appears strong, since the percentage of
mechanical work hours was similar or approximately 20% of the total work hours on both cases.
Table 4-15: Summary of safety data for Case A and Case B
Safety Calculations Case A Case B Project OSHA recordable incident rate (RIR) 0.97 3.74 Mechanical contractor OSHA recordable incident rate (RIR) 1.65 4.60 Project OSHA lost time case rate (LTC) 0.08 0.53 Percentage of mech. contractor work-hours to project work-hours 20% 23% Reportable mech. incidents per month of construction (incident/30 days) 0.16 0.67
4.5.6 LEED Scorecard and Energy Performance
Both projects demonstrated considerable improvement over the planned LEED goals, as
communicated to contractors during the RFP and bidding phases. Original RFP documents listed
LEED Certified as the minimum rating, which was quickly increased to LEED Silver as a result
of successful presentations from contractor and designer teams during the RFP selection
interviews. The most recent LEED scorecard data, representative of the documentation submitted
to USGBC for certification is summarized in Table 4-16 and shows both cases as seeking LEED

53
Gold rating. Both cases followed LEED-NC version 2.2. The percentage breakdown of LEED
categories is also included in Table 4-16, with notable differences in Sustainable Sites, Water
Efficiency and Energy & Atmosphere, which may indicate differing priorities for the design
teams on each project.
Table 4-16: Summary of LEED and energy data for Case A and Case B
LEED Scorecard Case A Case B Total points claimed in LEED submission 41 40 Anticipated LEED rating Gold Gold LEED Calculations (%, No. of Points) Case A1 Case B1 Percentage of Sustainable Sites points to total points 24% (10) 30% (12) Percentage of Water Efficiency points to total points 10% (4) 5% (2) Percentage of Energy & Atmosphere points to total points 17 % (7) 10% (4) Percentage of Materials & Resources points to total points 12% (5) 13% (5) Percentage of Indoor Environmental Quality points to total points 27% (11) 30% (12) Percentage of Innovation & Design Process points to total points 10% (4) 12% (5)
1 Numbers in parentheses are LEED category point totals
Since the focus of this research was the mechanical contractor, specific attention was
given to the energy modeling results and LEED categories of Energy and Atmosphere and Indoor
Environmental Quality. On Case A, energy modeling was performed in-house by the mechanical
contractor and made entirely available to the researcher. However, modeling on Case B was
performed by a third-party consultant hired by the architect and was never completely shared
during data collection. Therefore, the only data found within the modeling results provided on
both cases shown in Table 4-17 and includes the predicted yearly energy savings and percent
improvement over EPAct 2005 regulations. The predicted yearly energy savings on Case A and
Case B differ by approximately 20%, which could be the result of local energy rates or the types
of primary and secondary fuels assumed during modeling. Without the detailed energy model
information on Case B, any further assessment remains speculative. The savings difference
becomes more significant when considered over the gross square footage of each facility, with
Case A claiming a yearly savings of $0.87 per square foot against Case B’s $0.38 per square foot.
Despite differences in predicted savings, both cases show nearly a 30% reduction in energy usage
for EPAct 2005 regulations. The Energy Policy Act of 2005 (EPAct 2005) requires new public
facilities to reduce building energy intensity by 2% each year beginning in 2005, up to a
cumulative maximum of 20% in 2015. The EPAct 2005 energy intensity is measured in BTU per
gross square foot and the reduction is compared against a baseline created in 2003.

54
The energy savings implied in LEED EA Credit 1 does not correspond with the EPAct
2005 percentages. EA Credit 1 is a variable point credit, which awards more points for higher
percent improvement over the ASHRAE 90.1-2004 baseline. As shown in Table 4-17, Case A
claims 6 points and corresponds to a 28% savings, whereas Case B claims 2 points or a 14%
savings. Since the percent savings for EA Credit 1 is based on predicted energy cost, instead of
energy intensity, these values validate the energy model reports, which forecasted Case A with
approximately double the energy cost savings per square foot. Additionally, the LEED method of
calculating energy improvement on a cost basis is less sensitive to reductions in non-mechanical
or HVAC energy users, such as lighting or office equipment. For instance, reducing the wattage
of corridor lighting directly and immediately lowers the energy intensity of the building, but may
not contribute significant energy cost savings if electricity is inexpensive relative to primary
fuels.
Table 4-17: Summary of energy modeling results and energy performance
Energy Model Results Case A Case B Predicted yearly energy savings per square foot ($/ft2) $0.87 $0.38 Energy intensity reduction for EPAct 2005 regulations 31% 27%
LEED-NC 2.2 Energy & Atmosphere Case A Case B Credit 1: Optimize Energy Performance 6 2
Energy cost savings compared to ASHRAE 90.1 baseline 28% 14% Credit 2: On-Site Renewable Energy --- --- Credit 3: Enhanced Commissioning --- 1 Credit 4: Enhanced Refrigerant Management 1 1 Credit 5: Measurement & Verification --- --- Credit 6: Green Power --- ---
LEED-NC 2.2 Indoor Environmental Quality Case A Case B Credit 1: Outdoor Air Delivery Monitoring 1 1 Credit 2: Increased Ventilation 1 --- 1Credit 3: Construction IAQ Management Plan 2 2 1Credit 4: Low-Emitting Materials 4 4 Credit 5: Indoor Chemical & Pollutant Source Control 1 1 Credit 6.1: Controllability of Systems, Lighting 1 1 Credit 6.2: Controllability of Systems, Thermal Comfort --- 1 Credit 7.1: Thermal Comfort, Design 1 1 Credit 7.2: Thermal Comfort, Verification --- 1 Credit 8.1: Daylight & Views, Daylight 75% of Spaces --- --- Credit 8.2: Daylight & Views, Views for 90% of Spaces --- ---
1 IEQ subcategories for Credit 3 and Credit 4 are condensed for simplicity
The IEQ category breakdown in Table 4-17 also highlights differences in the HVAC
systems on each case. The mechanical design on Case A was based on a 100% outdoor air

55
condition, allowing the team to easily collect IEQ Credit 2 for increased ventilation. Alternately,
the Case B design emphasized a 3-duct, variable air volume (VAV) distribution to many patient
rooms, which enabled the team to claim IEQ Credit 6.2 for controllability of thermal comfort.
The Case B team also elected to pursue IEQ Credit 3 for enhanced commissioning and IEQ
Credit 7.2 for verification of thermal comfort, which do not directly result in HVAC energy
savings, but may improve system efficiency over the long term.
4.6 Summary
This chapter presented detailed in-process metric data for Case A and Case B, collected from
multiple sources including project documents, jobsite observations and semi-structured
interviews. The following differences in dependent outcome variables were highlighted:
• Schedule growth on Case A measured effectively 0% for project duration, overall design,
mechanical design and construction duration. Measured schedule growth on Case B of
25% for project duration, 30% for overall design, 55% for mechanical design and 30%
for construction duration.
• Cost growth on Case A measured 8% for mechanical contractor cost and 12% for project
cost. Measured cost growth on Case B of 34% for mechanical contractor cost and 43%
for project cost.
• Measured 45% fewer project RFIs and 85% fewer mechanical-related RFIs per unit area
on Case A, when compared against Case B. Case A calculated 1.69 project RFIs and
0.08 mechanical-related RFIs per square-foot, compared to 3.03 project RFIs and 0.49
mechanical-related RFIs per square-foot on Case B
• Reported safety incidents were nearly three-times lower on Case A, when compared to
Case B. The calculated RIR on Case A was 0.97 for the project and 1.65 for the
mechanical contractor, compared to 3.74 for the project and 4.6 for the mechanical
contractor on Case B.
• Both Case A and Case B have submitted for LEED Gold rating, but show slight
differences in point focus. With differences of at least two points, Case A achieved more

56
points in Energy & Atmosphere and Water Efficiency categories, whereas Case B
claimed more points in Sustainable Sites. The categories of Indoor Environmental
Quality and Innovation & Design Process differed by a single point in both Case A and
Case B.
• Case A claims six points in LEED credit EA 1, which translates into a projected energy
savings over the ASHRAE 90.1 baseline (by cost) of at least 28%. Case B claims two
points for the same credit, indicating a 14% energy savings by cost.

57
Chapter 5
DATA ANALYSIS AND DISCUSSION
As discussed in Chapter 3, previous project delivery research used statistics and
regression models to match one or more process indicators with a specific outcome, effectively
addressing what variables are important in higher performance buildings, but not directly
explaining how or why these relationships work. The discussion topics presented within this
chapter use explanation-building techniques to explore the multifaceted outcome and project
attribute relationships within the contexts of Case A and Case B.
5.1 Identifying Differences in Project Attributes
Reviewing the data in Chapter 4, Case A and Case B differ clearly in four of the seven
defined independent project variables. Summarized in Table 5-1, the organizational structure,
contract type, owner commitment and team commitment variables were selected for further
analysis and relationship considerations with measured outcomes. The procurement strategy and
team characteristic variables were seemingly similar between Case A and Case B. A best value
procurement strategy was used on both cases during the RFP process and the project team
characteristics showed comparable composition and prior experience, similarities which limit the
usefulness of these variables in a causal case study analysis. The design integration variable
indicates a different timing of contractor involvement, with Case B finishing an additional 10% to
15% of the architectural and MEP design before the RFP process. However, upon consideration
of the case context, the “design integration” variable does not appear truly independent. In
experimentation, a variable should only be considered independent when it is isolated from
changes in other independent variables. Design integration cannot stand alone and is
fundamentally impacted by the organizational structure, contract type and procurement strategy
on a project. For instance, design integration indicating very early contractor involvement is
typically not possible when paired with design-bid-build delivery or a hard bid procurement
process. Therefore, this comparative case study will not consider design integration as an
independent variable, but will discuss the impacts and potential of early involvement arising from
several delivery decisions.

58
Table 5-1: Selection of independent project variables for further analysis
Independent Project Variable Case A Case B Organizational Structure Design-Build CM at Risk Contract Type Lump Sum Cost-Plus
Procurement Strategy Best Value Best Value Owner Commitment 6 2 Team Commitment 4 2
Team Characteristics 4 4 Design Integration 30% Arch. / 10% MEP 40% Arch. / 25% MEP
5.2 Identifying Outcome Differences
Presented with an overwhelming amount of quantitative data describing the outcomes of
Case A and Case B, the researcher initially narrowed the scope of redundant data by identifying
recurring themes or commonalities within project and building system-level outcomes. For
instance, as shown in Table 5-2, four cost metrics, three RFI metrics and the distribution of
mechanical contractor change orders support a more generalized outcome of "cost predictability".
This grouping process quickly distilled over thirty metrics into four apparent contextual outcomes
that describe project and building system performance: cost predictability, schedule predictability,
building energy performance and jobsite safety.

59
Table 5-2: Grouping of case study outcome metrics into contextual outcomes
Dependent Outcome Variable Metrics Contextual Outcome
Cost of work installed per month ($/30 days) Planned/actual cost per bed ($/bed) Project cost growth (%) Mechanical contract cost growth (%) Mechanical change order distribution by category (%) Project RFIs per area (RFI/ksf) Project RFIs per million dollars of project cost (RFI/$) Percentage of mechanical-rated RFIs (%)
Cost predictability
Project schedule growth (%) Overall design schedule growth (%) Mechanical design schedule growth (%) Construction schedule growth (%) Planned/actual project duration per area (days/ksf) Planned/actual design duration per area (days/ksf) Planned/actual mech. design duration per area (days/ksf) Planned/actual construction duration per area (days/ksf) Area installed per day (ft2/day) Project RFIs per day of construction duration (RFI/day) Project QC reports per area (QC/ksf) Percentage of “open” QC reports to total (%) Percentage of mechanical-related QC reports to total (%)
Schedule predictability
Total points claimed in LEED submission Anticipated LEED rating Predicted yearly energy savings ($) Predicted yearly energy savings per area ($/ft2) EPAct 2005 energy intensity reduction (%) Points claimed for LEED EA Credit 1 Energy cost savings compared to ASHRAE 90.1 baseline (%)
Building energy performance
Project OSHA recordable incident rate (RIR) Project OSHA lost time case rate (LTC) Mechanical contractor OSHA recordable incident rate (RIR) Recordable mechanical-related incidents per month of
construction (incident/30 days) Percentage of mechanical contractor work-hours to total
project work-hours (%)
Jobsite safety

60
When viewed as a whole, the preponderance of measured dependent outcome variables
presented in Chapter 4 strongly indicates differences in project-level and building system-level
cost and schedule predictability between Case A and Case B. Additionally, Case A and Case B
show notable differences in the mechanical system performance and predicted building energy
savings by cost, despite submitting for similar LEED certifications. Other notable differences in
safety and RFI outcome metrics were observed, but featured less prominently. Therefore, the
discussion in Chapter 5 will focus primarily on understanding the relationships linking
independent project variables of organizational structure, contract type, owner commitment and
team commitment with differences in predictability, energy savings and safety outcomes.
5.3 Understanding Cost and Schedule Predictability Outcomes
The following sections discuss the contextual importance of predictability on Case A and
Case B, methods for measuring predictability using percent growth and percent difference, and
reviewing the evidence supporting greater cost and schedule predictability on Case A.
5.3.1 Value of Predictability on Projects
The results indicate that Case B was both less expensive per square-foot and shorter in
duration per square-foot, despite showing fewer indicators of design integration. However, Case
B did experience significant cost and schedule escalation, leading to a less predictable project.
To assist in planning and financing decisions, many owners desire both accuracy and precision
during the design and construction process. In research terms, accuracy is the closeness of
measured outcomes to their “true” or actual value, whereas precision is the consistency of
measured outcomes after repeated measurements. In construction terms, accuracy and precision
become apparent when comparing the initial cost and schedule estimates to the final value and
duration of the project. Excluding significant additions to scope, highly accurate and precise
projects would display fewer changes in contract value and construction duration, which also
makes them highly predictable. Predictability allows healthcare owners to make informed
decisions during construction, which may include managing cash flow, scheduling delivery of
medical equipment and relocation of personnel for occupancy. Especially for the public owners
on Case A and Case B, cost predictability is essential in securing the correct amount of funding.
Since opening both the Case A and Case B facilities requires the closing and consolidation of
another medical center, schedule predictability is explicitly important to each case.

61
5.3.2 Method for Comparing Predictability
As method of comparison, both percent difference and percent growth calculations are
used to assess the cost and schedule performance on both cases. The percent difference is the
absolute difference between two numbers as a percent of one number, as explained in Equation 5-
1. Unlike percent growth, which compares an old value with a new value as shown in Equation
5-2, the percent difference calculation allows comparisons of two independent measurements of
the same type. For simplicity, percent difference is exclusively used for external comparisons or
one case with another case, while percent change is used only for internal comparisons within a
single case. A low percent difference indicates similarity in the outcomes between cases, whereas
percent growth measures the change in magnitude of an outcome within a single case.
Equation 5-1: Percent difference
Equation 5-2: Percent growth
5.3.3 Evidence of Cost Predictability
Despite a significantly larger percent cost growth, Case B exhibited a lower final or
actual unit cost than measured on Case A. This result was unexpected, as on comparable
projects, the case with larger cost growth would intuitively result in a higher unit cost.
Additionally, prior research frequently implies that design-build deliveries result in lower costs,
which is not supported by this data. As shown in Table 5-3, the planned project unit cost and
planned mechanical system unit cost on Case B are lower and show a 25% difference from Case
A at the start of each project. Without considering the final or actual unit costs, there are many
potential explanations for this difference, including the possibility that Case B benefited more
from economies of scale, utilized fewer high-end finishes, specified a less expensive mechanical
system, underestimated the project scope or obtained more competitive pricing. However, the
similar percent difference of only 1% for the final project unit cost and 3% for the final
mechanical system cost indicate that some process or management differences dissolved the
% Diff =x1 – x2
(x1 + x2) / 2x 100
% Growth =x2 – x1
x1x 100

62
initial cost advantage held by the Case B case. When considered together with the percent
difference in planned and final unit costs, the lower percent change in cost on Case A indicates
greater cost predictability. In other words, the owners on Case B expected a $526 per square foot
facility at contract award, but were ultimately subject to 43% cost growth and a final unit cost of
$750 per square foot. Conversely, the owners on Case A expected to pay $679 per square foot
compared to a final unit cost of $758 per square foot, an increase of 12% and yet within 1% of the
final unit cost on Case B.
Table 5-3: Project and mechanical system unit cost comparison with percent difference
Project Unit Costs Case A Case B % Diff. Planned project cost per square foot ($/ft2) $675 $525 25% Actual project cost per square foot ($/ft2) $760 $750 1%
% Growth 12% 43% Mechanical System Unit Costs Case A Case B % Diff. Planned mechanical construction cost per square foot ($/ft2) $150 $115 24% Actual mechanical construction cost per square foot ($/ft2) $160 $155 3%
% Growth 8% 34%
Although the project change order logs for either Case A or Case B were not made
available during data collection, the breakdown of mechanical contractor change orders provides
some insight into the sources of cost growth. The categorization of mechanical change orders, if
assumed representative of the project change orders, indicates a larger quantity of owner scope
additions and design corrections occurring on Case B. From Table 5-4, the combination of 38%
difference in owner-initiated CORs and 18% difference in design errors and omissions strongly
suggests that the scope of Case B was comparatively under-defined at the start of construction,
resulting in more design changes and more frequent drawing updates. Removing the award-fee
incentive CORs, which constitute a large portion of the Case A mechanical change orders, the
difference in owner-initiated changes becomes less drastic, but still significant. The difference in
owner-initiated CORs, as identified in parentheses in Table 5-2, drops to 22% while the design
COR categories remain the same at 18%.

63
Table 5-4: Percentage breakdown of mechanical contractor change orders with percent difference
Mechanical System Change Orders (by $ value) Case A1 Case B Diff.1 Percentage approved owner-initiated CORs 38% (54%) 76 % 38% (22%) Percentage approved contractor-initiated CORs 22% (31%) 6% 16% (25%) Percentage approved unforeseen conditions CORs 10% (15%) 0% 10% (15%) Percentage approved design error CORs 0% (0%) 5% 5% (5%) Percentage approved design omission CORs 0% (0%) 13% 13% (13%) Percentage approved award fee/incentive CORs 30% (0%) 0% 30% (0%) 1Percentages in parentheses are without award-fee changes issued to the mechanical contractor.
5.3.4 Evidence of Schedule Predictability
On the basis of final or actual unit duration, Case B installed more square-footage in less
time than measured on Case A. Similar to cost performance, this result was unexpected for a
design-bid-build project, which research typically portrays as progressing more slowly than a
fast-tracked or design-build delivery. As shown in Table 5-5, the planned schedule for Case B
ranges from 37% to 70% more aggressive than Case A, in units of planned days per thousand
square foot of building area. The faster planned delivery on Case B may have resulted from
repetitions in design on larger size projects, more overlap of construction activities or
underestimation of durations and work scope. While faster than Case A in unitized terms, the
Case B case incurred significant schedule growth in all categories, resulting in poor schedule
predictability during construction.
Table 5-5: Schedule unit durations with percent difference
Project Overall Unit Duration Case A Case B % Diff. Planned project duration per area (days/ksf) 1.85 1.09 52% Actual project duration per area (days/ksf) 1.83 1.36 29%
% Growth -1% 25% Project Design Unit Duration Case A Case B Planned design duration per area (days/ksf) 1.22 0.59 70% Actual design duration per area (days/ksf) 1.19 0.75 45%
% Growth -2% 27% Project Construction Unit Duration Case A Case B Planned construction duration per area (days/ksf) 1.18 0.81 37% Actual construction duration per area (days/ksf) 1.16 1.08 7%
% Growth -2% 33% Mechanical System Design Unit Duration Case A Case B Planned mech. design duration per area (days/ksf) 0.57 0.35 48% Actual mech. design duration per area (days/ksf) 0.57 0.55 4%
% Growth 0% 57%

64
5.4 Determining Cause and Effect for Predictability Outcomes
Since this research uses an analytical, rather than statistical, approach to understanding
relationships, strong causal inferences are needed between independent project variables and
outcomes. However, independent project variables, such as organizational structure or contract
type, often impact differing or multiple aspects of design and construction processes. For
example, is a design-build organizational structure, a lump sum contract or high owner
commitment responsible for lower cost growth? The answer could involve all, none or some
combination of these variables. Therefore, an Ishkawa or “fishbone” diagram structure is useful
to logically brainstorm various causes of improved cost and schedule predictability. Cause and
effect mapping serves three main purposes: to look beyond symptoms to the root cause, provide
structure to cause identification and ensure that no major ideas are overlooked. Frequently used
in lean manufacturing, a fishbone diagram is created using the following methodology adapted
from the Six Sigma quality management tool (Pyzdek & Keller 2010):
(1) Identify the problem or effect under investigation;
(2) Select major categories for causes, relevant to the problem or effect;
(3) Identify detailed causes, asking “why?” the effect is occurring; and
(4) Review the diagram for completeness and eliminate unlikely causes.
Using “Improved Cost Predictability” and “Improved Schedule Predictability” as the
observed outcomes, two fishbone diagrams were created to identify potential causal relationships
in major categories of process, team and tools. As defined, the process category encompasses the
methods, techniques and procedures used in defining and managing the project. The team
category includes the characteristics and actions of the design and construction team. Finally, the
tools category captures any software or management tools that assist teams in completing a task.
Included in Appendix D, these fishbone diagrams serve to consolidate and graphically illustrate
potential causes contributing to predictability on both cases.
5.4.1 Identification of Unique Causal Factors Impacting Predictability Outcomes
To categorize the listing of potential causes derived from the causal diagramming effort,
a tabular matrix was generated to sort the factors by case occurrence, as shown in Table 5-5 for
cost predictability and Table 5-6 for schedule predictability. The purpose of this categorization
was to identify unique factors on Case A or Case B, which contributed to the measured

65
performance difference in cost and schedule predictability outcomes. Factors common to both
Case A and Case B are less suitable for comparison because they theoretically contribute equally
to the outcomes on both cases and therefore not relevant to a two-case discussion.
Table 5-6: Causal factors impacting cost predictability, by case occurrence
Causal Factors Impacting Cost Predictability Case A Case B Vertical orientation of design and construction teams X Contractor ability to influence and implement design decisions X Contractor financially liable for combined design and construction X Owner conveyed and enforced cost goals with project team X Owner was able to clearly define scope X Highly complete project program at RFP and contract award X End-user feedback received after start of construction X X Unpredictable design changes required rework to work-in-place X Cost reimbursable contract offered limited cost control X
Table 5-7: Causal factors impacting schedule predictability, by case occurrence
Causal Factors Impacting Schedule Predictability Case A Case B Contractor control of design schedule and construction sequence X Contractual incentive program rewarding performance and timely X Used online document management software for sharing drawings X Team made timely decisions to resolve issues X Similar delivery speeds of overall design and construction X Low percent design completion at RFP and contract award X X Contractor feedback on design provided prior to start of construction X X Owner-initiated design changes interrupted the progress of construction X

66
5.4.2 Identification of Influencing Project Attributes on Causal Factors
After identifying unique causal factors contributing to the measured cost and schedule
predictability outcomes, the researcher attempted to discern the influencing project attributes that
enabled, initiated or resulted in each causal factor. Since no prior research attempted this type of
categorization, a matrix format was selected to plot causal factors against the four project
attribute differences between Case A and Case B: organizational structure, contract type, owner
commitment and team commitment. The resulting matrix is summarized in Table 5-8.
Determination of influencing project attributes were made based on literature review and guiding
questions, similar to the following:
• What project attribute(s) dictates the orientation of design and construction teams?
• What project attribute(s) enables the contractor to make and implement design decisions?
• What project attribute(s) illustrate that timely decisions were made by the teams?
Table 5-8: Sorted causal factors for predictability, by influencing project attribute
Org
aniz
atio
nal S
truc
ture
Con
trac
t Typ
e
Ow
ner
Com
mitm
ent
Tea
m C
omm
itmen
t
Case Causal Factors Impacting Cost and Schedule Predictability
Cos
t
A Vertical orientation of design and construction teams A Contractor ability to influence and implement design decisions A Contractor financially liable for combined design and construction performance A Owner conveyed and enforced cost goals with project team A Owner was able to clearly define scope A Highly complete project program at RFP and contract award B Unpredictable design changes required rework to work-in-place B Cost reimbursable contract offered limited cost control
Sche
dule
A Contractor control of design schedule and construction sequence A Contractual incentive program rewarding performance and timely completion A Used online document management software for sharing drawings A Team made timely decisions to resolve issues A Similar delivery speeds of overall design and construction B Owner-initiated design changes interrupted the progress of construction

67
5.5 Relating Project Attributes to Predictability Outcomes
Using the unique causal factors impacting predictability and several influencing project
attribute relationships, the four differences in independent project variables can be linked with
predictability outcomes, as shown graphically in Figure 5-1. There is evidence supporting
organizational structure, contract type and owner commitment as factors impacting the cost
predictability of a project. Additionally, the organizational structure and team commitment
appear to contribute to schedule predictability. A discussion is provided for each arrow,
explaining the rationale and relevancy behind the connection. Where arrows were not drawn
between independent project variables and predictability outcomes, the comparative case study
data was inadequate to support the relationship. The absence of a connection arrow does not
preclude the existence of a relationship, but merely signifies the relationship was inconclusive or
only weakly supported based on the data collected on Case A and Case B.
Figure 5-1: Independent project variable relationships with predictability outcomes
Cost Predictability
Schedule Predictability
1
2
34
5
Organizational StructureCase A Case B
Design-Build CM at Risk
Contract TypeCase A Case B
Lump Sum Cost Plus Fee
Owner Commitment1
Case A Case B6 2
Team Commitment2
Case A Case B4 2
1 Owner commitment based on number of observed criteria (max = 7, min = 0)2 Team commitment based on number of observed criteria (max = 6, min = 0)

68
5.5.1 Organizational Structure → Cost Predictability
Within a design-build organizational structure, the vertical integration of mechanical
contractor and mechanical designer under the CM/GC results in lower transaction costs.
Expanding the economic definition to the construction industry, direct and indirect transaction
costs can arise from information exchanges, as well as monetary exchanges. For example,
response and review time, price negotiation and coordination effort are all examples of
transaction costs associated with a change directive. Vertically integrated supply chains, such as
the design-build organization on Case A, streamline these types of information exchanges and
reduce their cost impact. Because of the organizational separation of the contractor and designer
on Case B, the transaction costs were inherently higher. Transactions costs logically increase
when team members are located offsite, usage of communication tools are limited or team
incentives are misaligned. However, high transaction costs do not always translate into poor cost
predictability. In a project with few information exchanges between the contractor and designer,
high transaction costs may remain insignificant when compared against the overall project value.
On Case B, the high number of owner-initiated change orders and design revisions required
constant communication between the CM/GC and architect, which magnified the cumulative
effect of high transaction costs. The number of wasteful hours increases rapidly and can result in
a significant cost impact.
To illustrate the differences in transaction costs between cases, the mechanical contractor
was asked to describe an unexpected change or conflict during construction that included a
typical team interaction and resolution. The results of this request are summarized in the
following examples:
Example A: During the week of observation on Case A, start-up testing on the emergency
generator revealed a design flaw with the muffler wall penetration. While
operational, heat from the muffler transferred through the penetrated precast wall,
causing plywood on the interior face to begin smoldering. Meetings between the
mechanical and electrical contractors, design-build architect and CM/GC were held
onsite to determine the cause and revisit the insulation specified for the muffler.
Within two days, the team issued a revised penetration detail and no modification
to the contract value was required or requested.
1

69
Example B: The mechanical engineer under the architect on Case B designed a fan coil unit for
an exterior stairwell. During construction, a roof hatch was added by the owner to
the stairwell, which conflicted with location and ducting of the fan coil unit.
Installation of the unit was delayed, while RFIs from the mechanical contractor and
CM/GC were issued, reviewed and discussed with offsite architects. From the
identification of the problem to the eventual resolution, the team waited nearly ten
months and relocated the majority of sprinklers, chilled water pipe and ductwork in
the stairwell at added cost for the owner.
According to the Case B team, Example B was admittedly an extreme case and the
process extended longer than normal. However, the differences in transaction costs remain
evident in the manner that information flowed between the design and construction teams. The
vertical integration on Case A gave the mechanical contractor more autonomy and control in
resolving conflicts without adding additional cost to the project.
Beyond anecdotal evidence, the presence of increased transaction costs and inefficiencies
that accompany change directives are also found in actual cost reports from the mechanical
contractor. As discussed previously, a large number of owner-initiated and design-oriented
change orders were issued to the mechanical contractor on Case B, increasing the cost of the
HVAC construction package from $115 per square-foot to $155 per square-foot. Figure 5-2
presents actual cost data, separated into major categories, as a percentage of the total mechanical
contractor construction cost or work. This additional analysis compiled the mechanical
contractor cost codes into categories of subcontractors, general conditions, HVAC materials,
HVAC equipment, coordination labor, project management labor, shop labor and field labor.
Costs associated with engineering and design labor were intentionally omitted from this analysis,
since the scope of these services varied significantly between cases and would skew the
remaining categories. Notable differences are apparent in field labor, which account for 38% of
total costs on Case A and 42% on Case B. The HVAC equipment costs on Case A are 4% higher
than Case B, indicative of the higher expected first cost of the system. Higher material costs for
Case B somewhat reduce the lower first cost advantage, as evidenced by the combined HVAC
materials and equipment category costs of 48% of the total for Case A and 45% for Case B.
However, Case A also subcontracted a slightly larger scope of work (by cost), which may
partially account for lower field labor and HVAC material costs. Assuming a portion of the field
labor on Case A is purchased under the subcontract category, a difference of 2-3% would remain

70
and may be attributable to less productive rework for the large number of change orders and
design revisions on Case B. Similarly, the differences in general condition costs reflect on the
significant schedule growth on Case B and need for additional administration to manage change
directives. Conservatively, the transaction costs on Case B could total between 4-6% of the total
mechanical contractor work package. In other words, upwards of $6 to $9 per square-foot of the
$155 per square-foot system cost on Case B may be attributable to non-productive work,
including rework, administration and general conditions expenses.
Figure 5-2: Case comparison of mechanical contractor construction costs
Figure 5-3 illustrates differences in cost allocation between mechanical contractor’s
general conditions on Case A and Case B. The team on Case A spent comparably more project
management and coordination labor hours than Case B, with fewer jobsite expenses. Several
factors could influence this distribution of general conditions costs, including the possibility of
design-build requiring additional management time from the mechanical contractor and the
longer duration on Case B increasing jobsite expenses.
Field Labor, 38%
Field Labor, 42%
0% 25% 50% 75% 100%
Case A
Case B
Percentage of Total General Conditions Cost (%)
HVAC Equipment, 19%
HVAC Equipment, 15%
HVAC Materials, 19%
HVAC Materials, 20%
Subcontracted Work, 20%
Subcontracted Work, 17%
Shop Labor, 5%
Cost Allocation for Mechanical Contractor Construction Scope (excludes design/engineering services)
Shop Labor, 5%

71
Figure 5-3: Case comparison of mechanical contractor general conditions
5.5.2 Organizational Structure → Schedule Predictability
Organizational structures that shift design responsibilities to the contractor can
benefit from better alignment of design deliverables with the construction schedule. Under more
horizontally integrated structures, such as design-bid-build or CM at risk, the architect is
traditionally commissioned to provide design packages according to a predetermined list of
milestones. These design packages are often self-contained and furnished for each phase of
construction. On Case B, the design deliverables were initially planned for issuance every two to
three months and included "Site Grading & Utilities", "Foundations", "Building Envelope",
"MEP Core & Shell", "Interior Fit-out" and "Lobby Finishes". These packages are sequenced
very linearly, with seemingly clear delineation between content. However, where should the
contractor expect the under-slab plumbing design? Borrowing from lean manufacturing
terminology, the traditional delivery of design packages typically lacks the "pull" dynamic. In
other words, the progression of design is not always driven by downstream pull from
construction, but is instead frequently pushed by the next deliverable milestone. A contractor
may receive drawings not needed for many months, while simultaneously lacking a portion of the
design needed currently. Granting the contractor both design and construction responsibility, as
found on the design-build organization on Case A, incentivizes the timing and content of design
deliverables to match construction activities. A vertically integrated organizational structure does
not guarantee or inherently improve this alignment, but rather allows the construction team to
assist in planning design deliverables.
Project Management, 42%
Project Management, 33%
Coordination, 39%
Coordination, 35%
Jobsite Expenses, 19%
Jobsite Expenses, 32%
0% 25% 50% 75% 100%
Case A
Case B
Percentage of Total General Conditions Cost (%)
Cost Allocation for Mechanical Contractor General Conditions
2

72
To illustrate how contractor design responsibility may have improved the construction
schedule flow on Case A, project timelines were created from schedule data on both cases, as
shown in Figure 5-4. A series of milestones, relevant to the overall project and mechanical
design processes, were selected as points of comparison and included: design start, RFP issued to
contractor, mechanical design start, 10% mechanical design, 65% mechanical design, design
completion, construction groundbreaking and final completion. Similarly, a listing of design
processes, identified by the project teams during discussions, were collected and plotted along the
timeline. These design processes are not intended to be inclusive of all activities performed by
the architect or mechanical contractor, and only represent the researcher’s attempt to narrow the
scope to activities commonly associated with integrated teams. The process list includes: energy
model creation, end-user feedback session, design charrette, award-fee evaluation, lifecycle
analysis submission, constructability review, shop drawing coordination and LEED
documentation submission. Visually, Case A and Case B share similar overlapping activities,
with the design duration stretching to nearly the midpoint of construction. Significant design and
construction overlap is expected in the design-build organization on Case A, but a similar overlap
was also observed in CM at risk on Case B. The extended duration of design activities was
unplanned on Case B and likely a factor in extending the construction duration nearly one year
beyond the planned turnover date.

73
Figure 5-4: Timeline comparison of Case A and Case B with notations
0% 25% 50% 75% 100%
Pre-Design
Design
Mechanical Design
Construction
A
D 2 3
1
8
B
C
F
G H
E
Case A: Design-Build
4 4
4
5 7
4
Design
Mechanical Design
Construction
A
8
B
C
F
G H
6 6 66 7
D
E
0% 25% 50% 75% 100%
13
Case B: CM at Risk
Mechanical Contract Issued
Planned Duration
Actual Duration
Milestone Process Marker
Symbols
Data Collection
Project MilestonesA : Design startB : RFP issued to contractorC : Mechanical design startD : 10% mechanical designE : 65% mechanical designF : Design completionG : Construction groundbreakingH : Final completion
Design Process1 : Energy model performed2 : End-user feedback session3 : Design charrettes4 : Award-fee evaluation5 : Lifecycle analysis submitted6 : Constructability review7 : Shop coordination8 : LEED documentation submitted

74
To identify differences in the occurrences of activities, a timing table was created to
determine the project percent complete for the milestones and design activities identified on the
timelines. The results of this analysis are summarized in Table 5-9. Unless noted otherwise, the
timings were calculated by dividing the difference in project milestone or design process date and
design start date by the actual project duration in days. Notable project milestone differences
include the start of mechanical design, 10% mechanical design and construction groundbreaking.
The CM at risk delivery on Case B allowed the architect and engineers to begin the mechanical
design prior to contracting with the mechanical contractor. However, the construction on Case B
also started very early at 20% of project completion, compared with Case A at 35% of project
completion. On Case B, the CM/GC was provided design package milestones by the owner
based on commitments from the architect to allow simultaneous work on the hospital and clinic
buildings. However, due to changes and some design delays, the schedule became more linear
with less overlap of buildings, which directly extended the duration of construction. Notable
design process differences include the timing of charrettes and submission of LEED
documentation. On Case B, design charrettes were conducted early at 5% project completion
with the owner, but without contractor involvement. Conversely, Case A held charrettes after the
design-build team was selected and included the mechanical, electrical and fire protection
contractors. The submission of final LEED documentation occurred at 65% project completion
on Case A, earlier than Case B at 80% project completion. While there is no method of
comparison between cases for some design processes, the award fee evaluations on Case B were
performed at approximately 20% intervals and the constructability reviews on Case B were
requested approximately two months prior to issuing IFC packages or at 5% intervals.

75
Table 5-9: Timing comparison table for milestones and selected design processes
Project Milestones Case A Case B Design start 0% 0 % RFP issued to contractors 15% 10% Mechanical design start 25% 5% 10% mechanical design 30% 10% 65% mechanical design 45% 40% Design completion 65% 55% Construction groundbreaking 35% 20% Final completion 100% 100%
Design Process Case A Case B Energy model performed 25% 25% End-user feedback session 35% --- Design charrette 40% 5% Award-fee evaluation #1 40% --- Award-fee evaluation #2 65% --- Award-fee evaluation #3 85% --- Award-fee evaluation #4 100% --- Lifecycle analysis submitted 40% --- Constructability review #1 --- 25% Constructability review #2 --- 30% Constructability review #3 --- 40% Constructability review #4 --- 45% Shop coordination 45% 40% LEED documentation submitted 65% 80%
Since fine granularity of schedule data was not available to compare the exact timing of
design packages with ongoing construction activities, a delivery speed metric can provide insight
into the overall alignment design and construction. Figure 5-5 uses the delivery speeds of the
planned and actual project-level overall design and construction phases to create a simplified
linear balance schedule, comparing production units of square-feet against the project duration in
days. The delivery speed for each phase was calculated by dividing the total square-footage of
the facility by the actual duration of the phase, creating a linear or average rate. In both phases,
Case B shows slightly faster delivery speeds than Case A, but longer durations. Differences
become more apparent when considering the overall design and construction phases on a single
case, where alignment on Case A is evidenced by similar delivery speeds. The overall design
speed of 839 square-feet per day on Case A closely matches the construction speed of 865 square-
feet per day. Conversely, Case B shows an overall design speed of 1,339 square-feet per day,
much faster than the construction speed of 921 square-feet per day. It is unclear whether the
differences in these Case B delivery speeds are the result of design acceleration to support an
early start of construction or a sign that design efforts continued beyond the IFC drawings and
therefore not captured in this analysis. As evidenced by the shaded regions in Figure 5-4, Case B

76
overestimated the rate of design, leading to poor schedule predictability. Interestingly, despite the
difference in planned and actual overall design rates, the construction start on Case B was not
shifted or delayed. Conversely, the nearly identical overall design and construction speeds on
Case A seem to have resulted in improved schedule predictability, since the shaded regions are
very small. Projects with notable differences in delivery speeds, as in Case B, have a higher risk
of one phase outpacing, delaying or otherwise impacting the schedule of another phase.
Figure 5-5: Case comparison of linear project-level design and construction rates
Incr
easin
g Pro
ject C
omple
tion (
ft2 )
Increasing Project Duration (days)
Case Comparison of Project-Level Design & Construction Rates
Case B: Planned Overall Design(1,708 ft2/day)
Case B: ActualOverall Design(1,339 ft2/day)
Case B: ActualConstruction(921 ft2/day)
Case B: Planned Construction
(1,213 ft2/day)
Case A:Planned / Actual
Construction(850-865 ft2/day)
Case A:Planned / Actual Overall Design
(816-839 ft2/day)

77
As shown in Figure 5-6, the mechanical building system-level design and construction
speed on Case B show poor schedule predictability, when compared against Case A. Case B
mechanical design progressed at an actual rate of 1,818 square-feet per day, decreasing from the
planned rate of 2,838 square-feet per day. Similarly, the mechanical construction phase actually
delivered 1,067 square-feet per day, down from the planned 1,484 square-feet per day. The
actual and planned speeds of the same phases on Case A were nearly identical, due to the lack of
measured schedule growth. The actual design and construction delivery speeds, or slopes of the
solid lines in Figure 5-5, at the mechanical building system-level are very similar between Case A
and Case B, with a maximum differences of approximately 150 square-feet per day. However, on
Case A, the mechanical design starts much later than Case B and mechanical construction starts
comparatively earlier. Mobilizing for construction at earlier stages of mechanical design
indicates confidence in the mechanical contractor on Case A to deliver appropriate design
packages, paced with construction activities. In traditional organizational structures, where
contractors and designers are separate entities, there is a strong inclination to work independently,
optimizing their own deliverables and work progress. Increasing the vertical integration of teams,
which can be achieved by shifting design responsibility to the contractor, encourages a
predictable schedule that provides the right amount of design at the right time in construction.

78
Figure 5-6: Case comparison project completion by duration, with delivery speeds
5.5.3 Contract Type → Cost Predictability
The prime and mechanical contracts on Case B were not incentivized for cost
control. As defined by the CM/GC agreement, the contract type on Case B is a fixed-price
incentive contract with successive targets to be paid on a cost-reimbursable basis. Despite the
somewhat lengthy description, this contract most closely matches the accepted definition of cost-
plus fee. During the award process, the successful contractor establishes an initial target cost,
Incr
easin
g Pro
ject C
omple
tion (
ft2 )
Increasing Project Duration (days)
Case Comparison of Contractor-Level Design & Construction Rates
Case B: Planned Mech. Design(2,838 ft2/day)
Case B: ActualMech. Design(1,818 ft2/day)
Case B: ActualMech. Constr.(1,067 ft2/day)
Case B: Planned Mech. Constr.(1,484 ft2/day)
Case A:Planned / Actual
Mech. Constr.(895-913 ft2/day)
Case A:Planned / Actual
Mech. Design(1,758 ft2/day)
3

79
initial target profit or fee and price ceiling with the owner. Monthly payment applications from
the contractor are then paid on a cost-reimbursable basis. Significant management or supervision
is typically required from the owner to verify contractor material invoices and labor hours, as the
payment process is self-auditing. At some production point during construction, typically
between 85% and 100% construction documents, a firm fixed price is negotiated to effectively
convert the contract into a lump sum. The incentive portion of the contract takes effect if the
negotiated firm fixed price is less than the ceiling price, which increases the contractor's fee by
5% of the difference. Since this type of incentive considers only final cost, it becomes less
effective in rewarding process performance. Because of flow-down relationships within the
prime contract language, the MEP contractors were working under the same cost-plus
arrangement as the CM/GC. These limitations became apparent on Case B, where numerous
owner-initiated changes and design corrections created an ambiguous target cost, leaving the
owner with significant cost risk and no contractual means of incentivizing productivity. Three
attempts converting the cost-plus contract into a lump sum were conducted by the owner to
establish a final project cost. The first attempt occurred at 80% design completion and the
remaining two attempts occurred after 100% “Issued for Construction” drawings were distributed
to contractors. Whether these attempts represented a true effort to convert into a lump sum
arrangement or were only a means of obtaining some confidence amid several scope revisions,
they indicate a lack of cost predictability in the cost-plus contract on Case B.
The consolidation of design and construction responsibility under a design-build
contractor can reduce the owner’s cost risk of signing a lump sum contract at earlier stages of
design. In traditional organizational structures, a lump sum contract shifts nearly all cost risk to
the owner by requiring a highly accurate and complete design prior contract award. However, the
mechanical design on Case A was only 10% complete prior to awarding the lump sum design-
build contract. Despite a very preliminary HVAC system description, the design-build
mechanical contractor completed the project with only 8% cost growth. Conversely, as shown in
Figure 5-7, the cost-plus contract on Case B was executed at 25% mechanical design completion,
but currently anticipates a much larger 34% cost growth. This difference in cost predictability
appears at least partially influenced by the contract type on each case, along with the incentives it
creates within a specific organizational structure. Without any modifications to the initial scope,
the design-build contractor must operate below the lump sum amount or assume liability for any
cost overruns, providing a strong incentive to control costs. The owner is effectively protected
from error and omission claims because the contractor is wholly responsible for the design,

80
installation and performance of the system or building. Design errors and omissions on design-
build projects are not significantly lower than design-bid-build organizational structures, but the
subsequent rework or correction costs are absorbed internally by the contractor in lump sum
arrangements, rather than becoming the responsibility of the owner.
Figure 5-7: Percent design completion with percent cost growth, project and mechanical
5.5.4 Owner Commitment → Cost Predictability
The completeness of RFP and program documentation was a contributing factor in
cost predictability, providing a clear basis of design and statement of goals for the design-build
contractor on Case A. Since the owner commitment variable is primarily defined by the owner’s
ability to establish goals and become a driving force on the project, the quality of RFP
documentation becomes an early indicator of commitment. The RFP on Case A included a copy
of the owner program, which including project objective headings such as “Mission Statement”,
“Sustainable Design” and “Energy Conservation”. At the time of issuance to contractors, the
owner program was approximately 90% complete. Taken as a whole, the combined RFP and
owner program on Case A primarily emphasize the performance of the facility. The RFP on Case
B did not share the owner program with contractors and documentation was highly focused on the
Case A: Mechanical, 10%, 8%
Case B: Mechanical, 25%, 34%
Case A: Project, 42%, 12%
Case B: Project, 32%, 43%
0%
10%
20%
30%
40%
50%
0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50%
Cost
Gro
wth (
%)
Design Completion at Award (%)
Case Comparison of Design Completion at Award vs. Cost Growth
DB + LS
DB + LS
CMR + CP
CMR + CP
4

81
occupants of the facility, including evidence-based design recommendations, sustainable material
selection and integration of technology.
When implementing change orders or design revisions on Case B, the direction provided
to contractors was often "Do it now, we'll fix it later". This method of integrating changes
seemed especially detrimental to the cost-plus contract on Case B, where the contractor liability is
minimal and rework directly increases the cost of the project. While a successful short-term
tactic in meeting specific schedule goals, this type of leadership increases the amount of rework,
leading to higher costs and long-term coordination issues. For example, ceiling coordination
drawings revealed limited access for a number of VAV terminal units on Case B. To avoid
delays, the mechanical contractor was instructed to give a “best effort” in increasing the clearance
around controller boxes on the VAV units. Nearly one year later and while performing a
walkthrough, the owner was dissatisfied with some instances of limited access on VAV units and
re-defined the minimum acceptable clearance, which required many modifications to piping and
conduit routes near the controller boxes. By fostering a “Do it now, we’ll fix it later” jobsite
atmosphere, the owner implies that cost control is not a primary concern for the project.
5.5.5 Team Commitment → Schedule Predictability
The formalized award-fee incentive program on Case A strengthened the
commitment of contractors and designers to a timely project completion by rewarding the
achievement of intermediate milestones. No contractual incentive program existed on Case B,
beyond a potential shared savings if the final cost was less than the owner’s ceiling price. Prior to
contracting with the design-builder, the owner on Case A established a written award-fee plan,
which set aside 3% of base contract value as an incentive pool. According to the plan, “the
award-fee pool is a fixed amount and not subject to variances of the work or changes made to the
changes clause of the contract”. Additionally, the “award-fee determinations are not subject to
the dispute clause of the contract”. These statements ensure that no additional incentive is
provided for change orders and no management time is wasted on disputes. Award-fee is “paid
for performance above and beyond contractual requirements” in the categories of safety, quality
control, project management, design submissions, early transition and early completion. These
categories, as shown in Figure 5-8, were given varying amounts of award-fee for distribution,
presumably based on their importance to the owner. Since the completion of Case A and Case B
are required to relocate existing medical services from an existing hospital facility, a timely
5

82
turnover was a key project goal for both owners. When combining the early completion and early
transition categories, nearly 44% of the available award-fee was committed to incentivizing a
timely project completion.
Figure 5-8: Case A award-fee distribution by category
The assessment and distribution of award-fee on Case A was planned over four periods,
intended to align with major design deliverables or construction milestones. As shown in Figure
5-9, Period 1 and Period 4 included construction groundbreaking, early turnover or final
completion of the facility, while Periods 2 and 3 served as intermediate design and construction
evaluations. Clearly, the design-build team on Case A was given a strong financial motivation to
control schedule growth and remain committed to the contract turnover dates.
0% 5% 10% 15% 20% 25% 30% 35% 40%
Case A: Award-Fee Distribution by Categories
Quality Control
Early Transition
Design Submissions
Project Construction Management
Safety
Early Completion

83
Figure 5-9: Percentage of Case A award-fee pool available at each period
5.6 HVAC Building System Performance Outcomes
As discussed in Chapter 4, both case studies share similar control variables of project
location, type, function and LEED certification level, which strengthen conclusions drawn at the
project-level. However, this research is also focused on relationships at the building system-
level, exploring differences in the type and delivery of mechanical systems. Since Case A and
Case B facilities included a combination of acute and ambulatory services, the HVAC designs
were concerned with air movement restrictions, higher percentages of outdoor air ventilation,
infection control and stringent temperature, humidity and pressurization controls. Following the
same ASHRAE design guidelines for healthcare buildings, but likely a differing set of priorities,
the engineers on Case A and Case B arrived at separate solutions for the mechanical systems. A
comparison of the mechanical systems between cases provides evidence that earlier involvement
of the mechanical contractor adds value and predictability in the design of HVAC systems.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 2 3 4
Perc
enta
ge of
Awar
d-Fe
e Poo
l (%)
Award-Fee Period
Case A: Award-Fee Distribution by Period
Cumulative
Per Period
Early Completion
Early Transition
Design Submissions
Project Construction Management
Quality Control
Safety

84
While both cases fulfilled ASHRAE guidelines, the differences in indoor air quality
(IAQ), expected maintenance costs and yearly energy savings show greater value in the Case A
design approach. As summarized in Table 5-10, Case A opted for a 100% outdoor air design,
with enthalpy wheels for heat recovery and a constant-air-volume (CAV) system. Due to
architectural requirements, a large central mechanical room was located in the basement of the
Case A facility. For comparison purposes, the average single-patient room on Case B received
290-CFM of supply air, composed of 72% return air and 28% percent outdoor air. To overcome
the energy burden of exhausting all supply air, enthalpy wheels were first recommended by the
design-build mechanical contractor on Case A during the proposal phase. Although requiring a
higher first cost equipment investment, the addition of enthalpy wheels enabled the designers to
achieve energy savings goals without sacrificing IAQ in patient rooms. The Case B design was
more traditional and emphasized occupant controls, using a variable-air-volume (VAV) system
with decentralized mechanical rooms on each floor of the facility. While the VAV units allow
more customized control of temperature and humidity within patient rooms, the mixing of return
and supply air does not provide the same IAQ levels found in the Case A system.
According to the online ASHRAE Service Life and Maintenance Database, the average
replacement schedule for CAV and VAV systems are 35-years and 30-years, respectively. No
service life averages are currently available for enthalpy wheels due to the relative newness of the
technology in building applications, but initial reports indicate that enthalpy wheels often require
special and regular maintenance attention. Compared to a 100% outdoor air design, which
includes only supply and exhaust duct, the VAV system on Case B requires an additional
operable air valve on the return duct to achieve positive pressurization in many hospital spaces.
From a maintenance perspective, this extra valve is an additional failure point, which may
become costly to repair or replace with a large number of equipped VAV units. Without
historical data on the replacement schedule for enthalpy wheels, it is difficult to directly compare
the maintenance burden between Case A and Case B. However, the mechanical design of Case A
does possess fewer failure points on patient floors due to the CAV system, which may reduce
maintenance costs over the lifecycle of the facility.

85
Table 5-10: Mechanical system description and maintenance information by case
Mechanical System Case A Case B
Summary
100% outdoor air 2-duct CAV system Heat recovery chillers Enthalpy wheel Centralized air distribution
3-duct VAV system Heat recovery chillers Decentralized air distribution
Maintenance
35-year replacement on CAV No ASHRAE data on
replacement of enthalpy wheels; requires special attention
30-year replacement on VAV Return ducts require VAV
controls to achieve positive pressurization, results in twice the number of operable air valves
Advantages / Disadvantages
+ IAQ and infection control - Higher first cost of equipment - Increases fan power for enthalpy
wheel and central mechanical
+ Higher degree of individual control in patient rooms
- Complicated commissioning - More frequent maintenance of
VAVs
As shown on Table 5-11, the predicted energy savings, by cost and intensity, indicate
higher performance from the mechanical system on Case A. LEED EA Credit 1 awards points
based on the percent improvement in energy savings by cost over an ASHRAE 90.1 baseline.
According to the LEED submissions, Case A claimed 6-points in EA Credit 1, which corresponds
to a 28% to 31.5% improvement, whereas Case B could only claim 2-points or a 14% to 17.5%
savings. Despite a clear difference in ASHRAE 90.1 improvement, the energy reduction for
EPAct 2005 was more similar between cases at 31% for Case A and 27% for Case B. EPAct
2005 requires all public facilities in the U.S. to reduce energy intensity (BTU/ft2) by 2% per year,
up to a cumulative maximum of 30% in 2015. Since the EPAct 2005 regulation is based on
energy intensity, where lighting systems have a proportionally high and direct impact, the
measure is undependable in comparing the performance of mechanical systems. Therefore, the
owner on Case A can expect higher yearly savings on building energy costs of approximately
$0.87 per square-foot, compared to $0.38 per square-foot on Case B. Overall, the energy
outcomes on Case B were still significant and the facility achieved many sustainable goals in
water conservation and daylighting; however, Case A is predicting higher energy savings at
roughly the same project unit cost as Case B.

86
Table 5-11: Building energy performance and cost savings by case
Building Energy Performance Case A Case B LEED NC v2.2 EA Credit 1 Points 6 2 % Improvement over ASHRAE 90.1 (by cost) 28% - 31.5% 14% - 17.5% Predicted yearly energy savings per square foot ($/ft2) $0.87 $0.38 % Reduction in Energy Intensity for EPAct 2005 31% 27%
Construction Cost Case A Case B Planned unit cost ($/ft2) $148 $116 Actual unit cost ($/ft2) $160 $155
5.7 Jobsite Safety Outcomes
As a primary concern in the construction industry, jobsite safety is the responsibility of
members on the project team including the owner, designer and contractors. Construction
activities account for nearly 19% of all workplace fatalities, the largest percentage of any industry
sector (U.S. Bureau of Labor Statistics 2010) and many projects often only consider hazard
management during the construction phase. From process considerations in design to daily
planning during construction, project teams have an obligation to ensure a safe work environment
and educate workers on safe jobsite practices. Therefore, a more holistic view or awareness of
safety risks, during the design and planning phases, may improve safety outcomes. Safety reports
were collected from both the mechanical contractor and CM/GC on Case A and Case B to
determine their OSHA recordable incident rates. The goal of documenting safety performance on
these case studies is to determine if early contractor design involvement reduces the likelihood of
injury or improves awareness of construction safety risks.
Despite similar jobsite safety programs managed by the CM/GC and mechanical
contractor, Case A and Case B showed notable differences in the number of recordable incidents.
The Occupational Safety and Health Administration (OSHA) consider an accident recordable if
the injury “resulted in death, days away from work, restricted work or transfer to another job,
medical treatment beyond first aid or loss of consciousness”. Using OSHA’s Recordable Incident
Rate (RIR) metric as a basis for comparison, the safety performance on Case A and Case B are
summarized in Figure 5-10. Lower numbers indicate fewer incidents in relation to the total
number of hours worked. As a percentage of total project work-hours, the mechanical
contractor’s time onsite accounted for 20% on Case A and 23% on Case B. At both the project-
level and mechanical contractor work, Case B recorded nearly three times the number of
incidents occurring on Case A. Both cases were below the industry average RIR, which

87
according to the U.S. Bureau of Labor Statistics in 2008, was 4.7 in the construction industry
across all establishments. Comparable to the schedule and cost results, safety performance at the
mechanical contractor-level appears strongly relatable to the project-level outcomes on Case A
and Case B.
Figure 5-10: Safety performance comparison between Case A and Case B
Many factors have the potential for influencing safety performance, including
information control, personnel training, supervision and design quality. Since the project teams
on Case A and Case B showed similar characteristics, in terms of prior experience, safety
programs and Experience Modification Rates (EMR), the differing levels of contractor
involvement in design may have a role in safety outcomes. On Case A, the mechanical contractor
was responsible for designing and building a functional HVAC system, meeting the initial
performance criteria defined in the owner program and RFP documentation. Because of the well-
defined program and fixed scope of work, the mechanical contractor on Case A was given a
proactive opportunity to plan an effective work flow. Conversely, on Case B the mechanical
contractor was only given design-assist and construction responsibilities, which included
constructability reviews prior to drawing package issuance, accessibility reviews and estimating
services. While remaining in control of the construction processes, the contractor on Case B had
little impact on the overall HVAC system design beyond constructability recommendations,
0.97
1.65
3.74
4.60
0.0
1.0
2.0
3.0
4.0
5.0
6.0
1 2Project OSHA Recordable Incident Rate (RIR)
Mechanical Contractor OSHA Recordable Incident Rate (RIR)
Case A
Case B
Case A
Case B
Construction Industry Average
(DB)
(CMR)
(DB)
(CMR)
Case Comparison of OSHA Safety Performance

88
which were not always accepted by the architect or engineers. Impacted by design changes
beyond their control, the mechanical contractor on Case B was burdened by a more reactive
installation. On Case A, the performance specifications provide more flexibility to the
mechanical contractor in customizing or tailoring the HVAC system to match available field
labor experience, preferred means and methods and knowledge with an efficient design. In other
words, the design responsibility awarded to design-build contractors could result in the selection
of systems or materials that are both more familiar to the contractor and in accordance with the
owner program. Familiarity or previous experience with the design-builder’s chosen HVAC
system and installation techniques could reduce the likelihood of jobsite accidents by raising
awareness and developing best practices over a series of successful projects.
5.8 Summary
Chapter 5 identified, sorted and discussed several causal relationships, linking project
attributes impacted by design involvement from the mechanical contractor, with both project and
building system-level outcomes. Major contextual outcomes evidenced at the project-level
included improved cost and schedule predictability, with explanation-building case discussion
emphasizing the following relationships:
• Vertically integrated design and construction teams on Case A appeared to reduce
transaction costs between designers, engineers and contractors. Evidence was found in
examples provided by the project team describing typical problem resolutions and in
reviewing categorical separations of mechanical construction and general condition costs.
• Contractor design responsibility in the design-build delivery on Case A promoted
schedule accountability and enabled alignment of design deliverables with the
construction schedule. A comparison of detailed timelines for Case A and Case B,
combined with linear plots of project and mechanical system delivery speeds, indicate
higher levels of communication and feedback between the design and construction teams
on Case A.
• When paired with contractor design responsibility, the lump sum contract on Case A
encouraged cost control from the design-build team. Conversely, the cost plus fee
contract used on Case B was ineffective in limiting cost growth. Differences are evident

89
when plotting design completion at award against cost growth, where Case A showed
significantly less cost growth despite a lower design completion.
• A stronger owner commitment on Case A, which included a nearly complete owner
program at RFP issuance and emphasis on project performance, appeared to reduce the
likelihood of cost growth.
• A high team commitment, strengthened by an award-fee incentive program rewarding the
completion of intermediate milestones and performance exceeding contractual
expectations, contributed to an early completion on Case A. From a review of the award-
fee structure, nearly 45% of the incentive pool was coupled with early turnover and
project completion.
At the building system-level, integration of the mechanical contractor resulted in several
improvements to the HVAC system and predicted energy usage on Case A, which were achieved
at roughly the same unit cost as the system constructed on Case B. These mechanical system-
level benefits included the following:
• Indoor air quality and reduced risk of infection due to design of a 100% outdoor air CAV
system for patient spaces in Case A, compared with approximately 30% outdoor air
provided with a VAV system on Case B.
• While both projects used heat recovery chillers to reduce the energy required for cooling
loads, the design-build mechanical contractor on Case A also successfully integrated
enthalpy wheels for energy recovery from exhausted air. While a higher first cost
system, the predicted energy savings per gross square-foot for Case A were nearly double
the savings anticipated on Case B.

90
Chapter 6
CONCLUSIONS AND CONTRIBUTIONS
6.1 Research Conclusions
This research used a comparative case study of two similar healthcare facilities to evaluate
the involvement of the mechanical contractor in the design and construction process by extending
existing project-level metrics, initially developed for High-Performance Green (HPG) buildings,
down to measuring the performance of a single building system and specialty contractor. Based
on a methodical assessment of project documents, jobsite observations and over thirty different
performance metrics, the following conclusions are supported:
A. Cost and schedule predictability outcomes, measured at the mechanical building system-
level on both cases, were directly relatable to outcomes at the project-level. Specifically:
Cost predictability was improved by:
(1) reducing transaction costs between contractors and designers within a design-
build organizational structure,
(2) incentivizing cost control by consolidating design performance and construction
responsibilities under a lump sum contract, and
(3) completion of owner programming requirements prior to contract award.
Schedule predictability was improved by:
(1) contractor alignment of design deliverables with construction activities in a
design-build organizational structure, and
(2) a strong team commitment resulting from incentive programs that reward early
completion.
B. Engaging the mechanical contractor in a design-build arrangement demonstrates
potential for improving the lifecycle energy savings and jobsite safety of healthcare
construction projects.

91
Specialty contractors, specifically mechanical contractors, add value to the project by
contributing construction knowledge and experience early in the design process. Under a
design-build arrangement, the mechanical contractor has the opportunity and incentive to
engage in iterative system design, which improves the energy efficiency of the facility
and reduces the likelihood of construction safety accidents.
6.2 Research Limitations
As case study based research, these conclusions are challenged by both internal and
external validity and researcher and data collection bias. The following limitations should be
considered before overextending the results of this case study comparison to future projects:
• This comparative study used only two cases and may not represent the full sample set of
construction projects within the healthcare industry. Since the analyzed cases were
specifically recommended by the mechanical contractor and not rigorously selected from
a database or pool of healthcare project cases, the ability to generalize from either case
may be limited to projects with similar context. Both Case A and Case B were vetted
prior to data collection to ensure that the project were not unusual or special cases, and
while many similarities were observed between cases, they unquestionably represented
the high-end of size, cost and interior finishes for modern healthcare facilities.
• The research methodology used to compare case outcomes and variable relationships
was analytically based, rather than statistical, and therefore more vulnerable to
researcher bias. While efforts were made to explore several causal explanations for
outcome differences and corroborate results with multiple data sources, an analytical
comparison cannot identify every contributing factor to a specific outcome using only
two cases. Therefore, the research showed preference to affirmative statements for
relationships or “X contributes to Y”, rather than the negative position or “X does not
contribute to Y”.
• A significant amount of project information was provided by the mechanical contractor
on both cases, with years of experience providing design-build construction services.
With a business model focused on delivering and maintaining design-build projects, the

92
close involvement of the mechanical contractor introduced vulnerability to bias in data
collection. Internally, the risk of data bias was mitigated by corroborating cost and
schedule data with both discussions and correspondence with other project team
members, including the CM/GC and owner.
6.3 Research Contributions
The contributions of this research to the AEC industry include:
1) Demonstration of a structured, analytical approach of applying project-level metrics to
measure the performance of specific building system, with a single specialty contractor
involved in the design and construction of healthcare facilities. As specialty contractors
become more influential, due to increases in relative contract value and design
responsibilities, tracking the building system-level performance is crucial in predicting
project-level success.
2) Expansion of the definition of the “Owner Commitment” independent project variable
from a strictly High-Performance Green (HPG) application to encompass decision-
making and scope definition competencies. Making timely decisions and adequately
defining the project scope are criteria representative of the level of planning performed
prior to construction, which requires a strong owner commitment.
3) Introduction of a “Team Commitment” independent project variable to gauge the success
of team integration and commitment to project goals. Based on prior research on
commonalities in effective construction teams, this variable weighs contractual incentive
programs, shared design responsibilities, the presence of a “blame culture”, ability to
complete common goals, valuation of team member feedback and equal treatment of
team members to quantify a level of integrated team commitment.

93
6.4 Recommendations for Future Research
To expand this analytical approach towards project performance relationships, several
recommendations for future research are proposed:
1) Identify and test the process impacts from independent project variables. Independent
project variables or project attributes, including organizational structure, contract type,
procurement strategy, owner commitment, team commitment and team characteristics,
are difficult to relate directly with project outcomes. These project attributes often define
several aspects of design and construction processes. For instance, selecting an
organizational structure establishes the hierarchy, information flow and design
responsibility for the project. From a causal perspective, which of these impacts from the
organizational structure is contributing to a specific outcome? Attempts were made
during this study to link potential outcome causes to corresponding and influencing
project attributes, but further research is needed to identify and test the process impacts of
these independent project variables to enable more detailed and accurate case study
comparisons.
2) Test the building system-level analysis on other influential specialty contractors involved
in the design and construction of healthcare projects. Electrical, structural and façade
enclosure contractors represent a significant portion of the contract value on hospital
projects and are frequently engaged for design-build or design assist services. Since this
research focused exclusively on the mechanical contractor, additional studies are needed
to test the validity of these results for other influential contractors.
3) Assess the effectiveness of contracting incentive programs in promoting goal alignment
and encouraging performance on integrated project teams. As strongly evidenced on
Case A, the award-fee structure provided a strong financial incentive for a timely project
completion by rewarding intermediate design and construction milestones. As more
owners experiment with multi-party contracts, such as integrated project delivery (IPD),
fairly balancing risk and reward within the agreement may be the key creating strong
team interaction and relationships.

94
REFERENCES 7group & Reed, B., 2009. The Integrative Design Guide to Green Building: Redefining
the Practice of Sustainability, Hoboken, NJ: John Wiley & Sons, Inc.
Baiden, B.K. & Price, A.D.F., 2011. The Effect of Integration on Project Delivery Team Effectiveness. International Journal of Project Management, 29(2), pp.129-136.
Baiden, B.K., Price, A.D.F. & Dainty, A.R.J., 2006. The Extent of Team Integration Within Construction Projects. International Journal of Project Management, 24(1), pp.13-23.
Bilec, M.M. et al., 2009. Analysis of the Design Process of Green Children’s Hospitals: Focus on Process Modeling and Lessons Learned. Journal of Green Building, 4(1), pp.121-134.
Cassidy, R., 2010. America’s Greenest Hospital. Building Design & Construction, 51(2), p.48.
Chan, A., Scott, D. & Lam, E., 2002. Framework of Success Criteria for Design/Build Projects. Journal of Management in Engineering, 18(3), pp.120-128.
Chapman, C. & Ward, S., 2008. Developing and Implementing a Balanced Incentive and Risk Sharing Contract. Construction Management and Economics, 26(6), pp.659-669.
Consortium for Energy Efficiency, 2005. Commercial Building Performance: Healthcare Facilities.
El Wardani, M., Messner, J. & Horman, M., 2006. Comparing Procurement Methods for Design-Build Projects. Journal of Construction Engineering and Management, 132(3), pp.230-238.
Evbuomwan, N. & Anumba, C., 1998. An Integrated Framework for Concurrent Life-Cycle Design and Construction. Advances in Engineering Software, 29(7-9), pp.587-597.
Gil, N. et al., 2000. Contribution of Specialty Contractor Knowledge to Early Design. In Eigth Annual Conference of the International Group for Lean Construction. IGLC-8. Brighton, UK.
Gransberg, D. & Buitrago, M., 2002. Construction Project Performance Metrics. In AACE International Transactions of the Annual Meeting. 46th Annual Meeting of AACE International.
Hall, M. & Tomkins, C., 2001. A Cost of Quality Analysis of a Building Project: Towards a Complete Methodology for Design and Build. Construction Management and Economics, 19(7), pp.727-740.

95
Kashyap, M., Khalfan, M. & Zainul-Abidin, N., 2003. A Proposal for Achieving Sustainability in Construction Projects Through Concurrent Engineering. In The RICS Foundation Construction and Building Research Conference. Loughborough, UK, pp. 127-138.
Kent, D. & Becerik-Gerber, B., 2010. Understanding Construction Industry Experience and Attitudes towards Integrated Project Delivery. Journal of Construction Engineering and Management, 136(8), pp.815-825.
Klevens, R. et al., 2007. Estimating Health Care-Associated Infections and Deaths in U.S. Hospitals, 2002. Public Health Reports, 22, pp.160-166.
Konchar, M. & Sanvido, V., 1998. Comparison of U.S. Project Delivery Systems. Journal of Construction Engineering and Management, 124(6), pp.435-444.
Korkmaz, S., 2005. High Performance Building Project Delivery. In Mindbend Research Symposium. The Pennsylvania State University.
Korkmaz, S., Horman, M., Riley, D., et al., 2010. Influence of Project Delivery Methods on Achieving Sustainable High Performance Buildings: Report on Case Studies,
Korkmaz, S., Horman, M.J. & Riley, D., 2010. Piloting Evaluation Metrics for Sustainable, High Performance Building Project Delivery. Journal of Construction Engineering and Management, 131(1).
Kozlowski, D., 2004. When Talk is Cheaper: Integrated Design And Better Buildings. FacilitiesNet. Available at: http://www.facilitiesnet.com/bom/article.asp?id=2138 [Accessed April 2, 2010].
Ling, F. et al., 2004. Predicting Performance of Design-Build and Design-Bid-Build Projects. Journal of Construction Engineering and Management, 130(1), pp.75-83.
Molenaar, K. et al., 2009. Sustainable, High Performance Projects and Project Delivery Methods: A State of Practice Report,
Pyzdek, T. & Keller, P., 2010. The Six Sigma Handbook 3rd ed., New York: McGraw-Hill.
Rahman, M. & Kumaraswamy, M., 2008. Relational Contracting and Teambuilding: Assessing Potential Contractual and Non-contractual Incentives. Journal of Management in Engineering, 24(1), pp.48-63.
Riley, D., Diller, B. & Kerr, D., 2005. Effects of Delivery Systems on Change Order Size and Frequency in Mechanical Construction. Journal of Construction Engineering and Management, 131(9), pp.953-962.

96
Riley, D., Sanvido, V., et al., 2005. Lean and Green: The Role of Design-Build Mechanical Competencies in the Design and Construction of Green Buildings. In Construction Research Congress. San Diego, CA, pp. 1-8.
Shooter, S. et al., 2000. A Model for the Flow of Design Information in Product Development. Engineering with Computers, 16(December), pp.178-194.
Tommelein, I.D. & Ballard, G., 1997. Coordinating Specialists, Berkeley, CA: University of California.
U.S. Bureau of Labor Statistics, 2008. Census of Fatal Occupational Injuries, 2008.
U.S. Department of Energy, 2003. Commercial Buildings Energy Consuption Survey (CBECS).
Yin, R.K., 2003. Case Study Research: Design and Methods 3rd ed., Sage Publications Inc.
Zhang, L. & Chen, W., 2010. The Analysis of Liability Risk Allocation for Integrated Project Delivery. In 2nd International Conference on Information Science and Engineering. Hangzhou, China, pp. 3204-3207.

97
APPENDIX A
Glossary of Terms
Building system-level: Contracted design, engineering and construction scope for a specific
functional building system, such as mechanical, electrical or façade. The building system may
be installed by one or more contractors, employing a single trade or multiple tradesmen. For
example, a contractor responsible for the building mechanical system may require several
trades, including: pipefitters, mechanics, sheet metal fabricators and installers, insulators and
control technicians.
Control variable: Describes the external environment and defining qualities of the project scope,
including: project type, intended building use, building size, geographic location, project
complexity, availability of skilled or qualified contractors, local regulations, legal constraints,
building system characteristics and sustainable features. Control variables are assumed to
remain constant during the design and construction of the project.
Dependent variable: Expressed at both the project and building system-level, dependent variables
are measurable outcomes including: cost, schedule, quality, safety and sustainability
performance. The values of these variables are frequently expressed as metrics, created from
measured in-process data on a specific project.
Independent variable: Describes the delivery decisions and team composition for the project,
including: organizational structure, contract type, procurement strategy, owner commitment,
team commitment and team characteristics. For the purpose of this research, independent
variables are synonymous with the term “project attributes” and are unaffected by variations in
other variables.
Project-level: Contracted architectural design, engineering and construction scope for the overall
project organizational level, excluding owner-specific costs such as land, financing, planning
and feasibility studies, consultants or inspectors, overhead and owner-furnished equipment.

98
APPENDIX B
Sample Semi-Structured Interview Questions
Assessing “Owner Commitment”, “Team Characteristics” and “Team Commitment” variables:
Owner Commitment
Who introduced the “green” concept to the project? When was it introduced?
What was the reason for pursuing “green” objectives?
How important were “green” goals for the project? How were they communicated to the
project team?
Was “green” contractually or verbally mandated?
Team Characteristics
How experienced is the team with similar projects?
Have you worked together with members of the team on previous projects?
How capable was the owner’s representative?
Was the owner able to adequately define scope?
Was the owner able to make decisions?
Was the team generally compatible?
How was information shared between parties? Was information only available to the
individuals responsible for that trade’s work?
Was the team located in a common office or separated?
Team Commitment
How did the team respond to the identification and resolution of problems? Was there a
culture of blame evident?
How would you describe the focus of the team? How did the team work to complete project
objectives?
Did working as a team improve the cost and time predictability of the project?
How flexible was the team in response to shifting workloads? Were new team members
added as necessary and less effective members removed?
Were all team members treated equally?
Were the comments or suggestions of team members valued and considered? How was
feedback provided?

99
APPENDIX C
Summary of Independent Project Variables for Case A and B
Project Attribute Case A Evidence
Contractor Contract Type Lump Sum • Contract value for design-build team and mechanical contractor
set fixed priced at contract award
Project Delivery Method Design-Build • CM/GC joint venture with design-build architect and
subcontractors as partners during RFP process
Contractor Procurement Best Value
• RFP issued on owner’s solicitation website as 2-phase design-build package
• Competitively procured and negotiated with qualified design-build teams
Contractor Design Integration High
• Mechanical contractor involved at 10% MEP design, 30% architectural design
• Responsible for energy performance, system design and installation
Owner Commitment High
• Vision statement issued with RFP to contractors • Mandated performance:
1) "…meet a minimum of "Certified" in the US Green Building Councils (USGBC) 'Leadership in Energy and Environmental Design (LEED) Rating System version 2.2'."
2) "...conform to the latest edition of ASHRAE Standard 90.1-2004... In addition...the Energy Policy Act of 2005 requires … designs achieve energy consumption levels 30% below the ASHRAE 90.1 baseline building."
3) “Green” promoted through owner program section Sustainable Design and distributed with RFP, dated 1-year prior to construction start.
• Emphasizes key sustainable principles: 1) "Reduce the total cost of ownership of the facility using a
whole building, life-cycle approach."
2) “Provide integrated sustainable design strategies and features to minimize energy consumption.”
Owner had some difficulty interpreting end-user feedback during the design process, resulted in scope ambiguities. Example: Owner provided CM/GC with an end-user request to change a “Waiting Room” into a “Reading Room”, but provided no further information on the desired scope modifications.
Team Commitment High
• Award fee program: “Unearned fee will not carry over into subsequent fee periods.”
• Liquidated damages: “…the following amounts for each calendar day of delay until the work is completed or accepted…”

100
• Mechanical contractor contractually responsible for performance of HAVC systems.
• Predictable project schedule enabled owner to request an early turnover of Buildings A and B. According to CM/GC, the early completion of structural trades and wall close-ins created 4 to 6-weeks of float passed to owner.
• Consistently strong team atmosphere, with the following observations: 1) Mechanical and other contractors wanted to attend safety
and coordination meetings 2) CM/GC meeting leaders went around the table, asking each
contractor to offer any recommendations or concerns for upcoming work (safety, sequence, etc.)
3) Construction incidents resulted in investigation, rather than finger-pointing. Example: Heat from muffler ignited combustible material during emergency generator testing. Meetings called to understand the cause of fire (fire-rated plywood used as substrate too close to generator muffler) and determine solution. Within 2-days of incident, mechanical contractor worked with design-build architect to revise the wall penetration detail, despite having only minimal responsibility for the fire.
4) Numerous visits from CM/GC team to mechanical contractor’s construction trailer to discuss design and commissioning issues.
Team Characteristics High
• Mechanical contractor superintendents are experienced with clean rooms and pharmaceuticals, but not explicitly hospital facilities. Owner staff is mixed in exposure to healthcare projects and was assembled internally after issuance of the RFP. CM/GC and design-build architect both have previous hospital experiences, but less with publically funded projects.
• Observed team interactions and instances of integration: 1) Universal use of “Constructware” software for document
management, which provided access to submittals, RFIs, change notices and drawing packages to all team members.
2) Mechanical contractor worked previously with members of the CM/GC management staff and electrical contractors.
3) Trailers connected via boardwalks, but not shared between parties. Design-build architect and mechanical contractor engineer have offices onsite to respond quickly to design questions.

101
4) Mechanical contractor is not invited to bi-weekly owner progress meetings; CM/GC prefers a single voice or point of contact with owner. However, owner is comfortable working 1-on-1 with mechanical contractor, often appearing to value mechanical contractor’s opinion over the GC/CM (ex: Commissioning Meeting 7/15/2010).

102
Project Attribute Case B Evidence
Contractor Contract Type Cost Plus Fee
• Owner describes contract as “fixed price with a ceiling, paid on a cost-reimbursable basis”
• Ceiling price is bid, not stipulated. Owner and successful contractor negotiate a firm fixed price typically around 85% design completion.
• Very similar to cost-plus fee, but lacking the incentive structure found in typical publically funded cost-plus projects
Project Delivery Method CM at Risk
• A version of design-build-build with early contractor involvement • Attempt to gain fast tracking and contractor benefits of CMR and
design-build deliveries, without relinquishing owner control of either architect or CM/GC contracts
Contractor Procurement Best Value • Bids solicited via website, owner considered price and non-price
factors before selecting contractor.
Contractor Design Integration Medium • Mechanical contractor contacted for periodic design assist
meetings, starting at 25% MEP design.
Owner Commitment Low
• No vision or mission statement distributed with RFP to contractor.
• Sustainability guidelines presented in RFP: 1) “As a LEED project, the selection and use of materials and
finishes that will contribute to LEED points will be very important.”
2) “The inclusion of appropriate materials and their use in this project is a critical element that has already begun.”
3) “In order to minimize the building’s energy consumption and comply with the LEED certification criteria, various energy conservation techniques will be used or further evaluated during the design.”
• “Green” introduced to architect during conceptual design (resulted in deliberate material selection, rain catchment system, etc.) and conveyed to contractors though RFP documents.
• LEED was heavily emphasized to architect, but specific owner requests limited potential for energy efficiency and cost savings. Examples: Using VAV systems in pressurized spaces (not energy efficient) and locating VAV boxes in hallways to reduce patient room noise (added cost for ceiling coordination).
• CM/GC noted that owner typically behaved as list-makers and box checkers, very rigid and slow to make decisions, often relying the designer, engineer or specifications for guidance. Example: During MEP management meeting, 3 outstanding change orders were identified—2 awaiting owner funding approval and 1 awaiting owner direction to proceed.

103
Team Commitment Low
• No contract incentive clauses or award fee program. However, liquidated damages are specified for exceeding the completion deadline.
• Contractual responsibility for design resides only with architect. Constructability or efficiency improvements to HVAC systems from mechanical contractor can be accepted or rejected at owner’s discretion.
• Low cost and schedule predictability, as demonstrated by the following: 1) Three efforts by owner to establish the ceiling price or
convert cost-plus contracts into lump sum. Attempts were performed at 6-8 month intervals.
2) Unmet design milestones, resulting in fractured design packages issued to keep pace with overlapping construction activities. The original schedule identified 9 drawing packages, which quickly grew to 200+ CDs and 800+ ASIs.
• Inconsistent team atmosphere, with the following observations: 1) Mechanical and electrical contractor field staff dread the
weekly MEP management meetings, which are not viewed as unproductive (minor issues exaggerated, milestone dates stressed without feasibility checks, etc.). However, the general (non-MEP specific) meetings are led by different CM/GC staff and are viewed more favorably by contractors.
2) Construction conflicts and design issues tend to linger “open” for long periods before reaching resolution. Often, trades continue working without design answers, which requires rework. Example: Owner added roof hatches to stairwell in Building A, which was noted as a conflict with the location of planned sprinkler standpipe and fan coil cooling unit. Despite this issue, sprinkler and drywall trades installed their work in the stairwell. An RFI with proposed relocation of the fan coil unit was issued. As of data collection, the conflict is still considered “open” and pending approval from architect.
3) Contractors are frustrated with progress of design, the lack of information to finish their work.
Team Characteristics High
• First CMR project for many owner staff, a combination of approximately 20% public employees and 80% outside contractors for consulting services. Due to the volume of projects currently underway, owner staff experienced with large healthcare or commercial projects is spread thin. Additionally, the predominantly civil-minded culture has difficulty adapting to military construction.

104
• CM/GC has previous experience with hospital and clean room projects. Architect has completed several healthcare facilities under a Design-Bid-Build delivery, having only minimal experience with the CMR schedule.
• CM/GC, subcontractors and owner have separate trailer complexes onsite. Architect visits jobsite weekly to perform contract administration (CA) work, but is otherwise only onsite as needed or requested to solve a field conflict.

105
APPENDIX D
Diagram for Relating Outcomes of Improved Predictability on Case A and B
Cost
Pred
ictab
ility:
Pote
ntial
Cau
sal R
elatio
nship
s
Impr
oved
cost
pred
ictab
ility
Team
Tool
s
Proc
ess
Ow
ner a
bilit
y to
defin
e sc
ope
earl
ier i
n de
sign
, mak
ing
few
er r
evis
ions
dur
ing
cons
truc
tion.
Com
plet
enes
s of o
wne
r pr
ogra
m a
nd
desi
gn a
t sta
rt o
f con
stru
ctio
n.
Team
und
erst
andi
ng o
f ow
ner’
s co
st
goal
s and
com
mitm
ent t
o va
lue.
Cha
nge r
isk
plac
ed w
ith c
ontr
acto
r, us
ing
com
bina
tion
of lu
mp
sum
con
trac
t te
rms
and
cont
ract
or d
esig
n re
spon
sibi
lity.

106
Sche
dule
Pred
ictab
ility:
Pote
ntial
Cau
sal R
elatio
nship
s
Impr
oved
sche
dule
pred
ictab
ility
Team
Tool
s
Proc
ess
Aw
ard-
fee i
ncen
tive
prog
ram
, whi
ch r
ewar
ded
cont
ract
or
addi
tiona
l fee
for m
eetin
g de
sign
del
iver
able
dea
dlin
es
and
spec
ific
cons
truc
tion
perf
orm
ance
cri
teri
a.C
ontr
acto
r inp
ut o
n th
e co
nten
t of
desi
gn d
eliv
erab
les,
crea
ting
flow
&
pull
duri
ng c
onst
ruct
ion.
Tim
elin
ess o
f ow
ner
deci
sion
-mak
ing,
due
to le
ss
repr
esen
tatio
n.U
se o
f onl
ine
docu
men
t m
anag
emen
t sof
twar
e fo
r sh
arin
g al
l dra
win
gs, R
FIs
& s
ubm
ittal
s
Des
ign
sche
dule
inte
gral
with
co
nstr
uctio
n sc
hedu
le a
nd
man
aged
by
cont
ract
or.