measuring maternal mortality: the potential of health data
TRANSCRIPT
Health Information Systems Knowledge Hub 2009
Measuring maternal mortality: the potential of
health facility data
• Principles for using facility data• Advantages and limitations of facility data
• Data requirements
• Data quality assessment and adjustment
• Methods to improve data completeness and quality
• Technical resources• Country examples

Definitions
Maternal death: “death of a woman while pregnant or within
42 days of termination of pregnancy…from any cause related
to the pregnancy or its management, but not from accidental
or incidental causes”
(ICD‐10)
Direct –
obstetric
Indirect – existing conditions aggravated by pregnancy
or its management
Incidental –
unrelated to pregnancy
Certain maternal deaths hard to identify (abortion‐related)
Distinction indirect and incidental causes unclear, subjective
Pregnancy‐related
death: death during pregnancy or within
42 days of termination of pregnancy, irrespective of cause

The data sources that identify “true”
maternal deaths require medical
determination of cause
Maternal deaths (cause of death definition)
Civil registration with medical certification
National and subnational demographic
surveillance with verbal autopsy
Health facility reports
Pregnancy‐related deaths (time of death definition)
Household surveys with sibling history
Censuses and household surveys with direct
measurement of household deaths–

Health facility records & Health Management Information Systems (HMIS)
• Health information system (HIS) data on deaths are generated from health facilities including hospitals
and health centres by medical professionals.
• Facilities compile statistics on maternal deaths and births and report these to the central level.
• HIS data are generally available, in some form, in most settings. However, quality can be variable os of
limited usefulness.
• Many facility deaths missed
• Poor quality or unavailability of medical records
• Poor death certification by physicians• Incomplete reporting by facilities,
especially private sector
• Cannot link maternal and infant outcomes
• Delays in compilation and analysis
• Biased estimates all women deliver in health facilities
Limitations of facility‐based HMIS data

Strengths of facility‐based HMIS data• Continuously available• In principle, all deaths are medically
certified
• Can measure “true”
maternal deaths and their causes
• By‐product of patient management
• Starting point for audits and case reviews to evaluate quality of care
and identify locally relevant avoidable factors.

Tapping the potential of facility data
• Currently, facility data are not used by agencies and academics for compiling global
maternal mortality estimates
• But they are widely used in countries because they are locally generated and continuously
available
• Methods are needed to improve data quality and increase the reliability and rustworthiness
of facility data

Total maternal deaths (hospital and community)
Maternal deaths reported bypublic & private sector
Maternal deaths on obgynand specialist wards
Maternal deaths reported by HMIS
Reasons for weakness of routine HMIS reporting
Maternal deaths reported by HMIS
Are all maternal deaths captured in routine HMIS reporting?


HMIS & facility reporting of maternal deaths
• What proportion of facilities are captured in HMIS?
• Are main referral hospitals included in the HMIS?• Do facilities report all facility deaths, on all
wards? • What is the accuracy of cause of death
certification and coding? • Are patient records adequately maintained? • How efficient is data transfer to central level?• Is there a way to deal with selection biases, for
example, poorest, most remote populations missed?

Maternal deaths reported by HMIS
Maternal deaths reported bypublic & private sector
Are all facilities reporting to the HMIS?


Maternal deaths reported by HMIS
Are all facility deaths being reported through the HMIS?
Maternal deaths reported bypublic & private sector
Maternal deaths on all wards

Improving identification of all maternal deaths in facilities
RAPID
A tool to review hospital records for all
deaths of women aged 15‐49 years
Information is extracted from registers and case notes and number of maternal deaths is then compared with that obtained
through the routine reporting system for the same period.
www.immpact‐international.org/toolkit

Non maternal deaths
Unclassified
Register review
Maternal deaths
Case notes review
Case notes unavailable
Maternal deaths
Non maternal deaths UnclassifiedUnclassifiedUnclassified

Non maternal deaths 78 (12%)
Unclassified 453 (68%)
Register review666 deaths f 15‐49
Maternal deaths 135
(20%)
Case notes found 262 (68%)
Case notes unavailable 191
(42%)
Maternal deaths 20 (8%)
Non maternal deaths 1 (0.4%)
Unclassified 241 (92%)
Unclassified 241(92%)
Unclassified 241 (92%)
Indonesia studyQomariyah et al 2009

Category Number %
Deaths in women of reproductive age 666 100
Maternal deaths identified through
facility registers 135 20.3
Maternal deaths identified from review
of case notes 20 3.0
Total maternal deaths 155 23.3
Non maternal deaths 79 11.9
Case notes missing 191 28.7
Case notes inadequate to identify causes
of death241 36.2
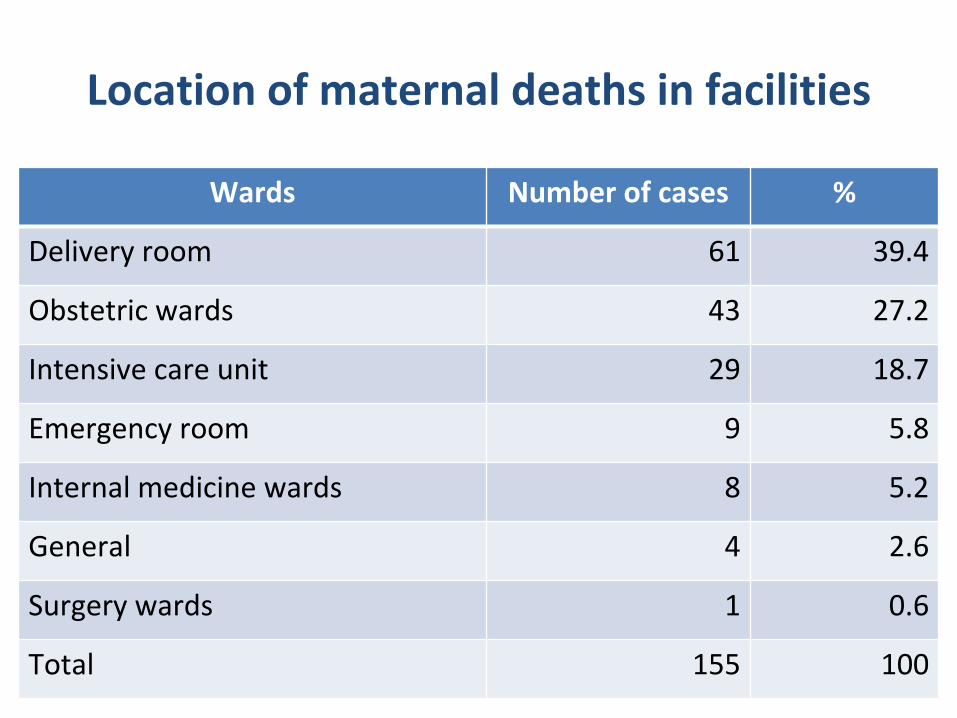
Location of maternal deaths in facilities
Wards Number of cases %
Delivery room 61 39.4
Obstetric wards 43 27.2
Intensive care unit 29 18.7
Emergency room 9 5.8
Internal medicine wards 8 5.2
General 4 2.6
Surgery wards 1 0.6
Total 155 100

Total maternal deaths (hospital and community)
Hospital maternal deaths, public & private sector
Maternal deaths on obgynand specialist wards
Maternal deaths reported by HMIS
Identifying maternal deaths in communities

Reconciling facility data and community reporting (capture‐recapture)
Referralhospital
22 deaths: only 2 in HMIS
26 total maternal deaths:
Identification of duplicates
Healthcentres
0 deaths
Village leaders
15 deaths:3 additional
Survey,Surveillance
5 deaths:
Source: Olsen et al (2002) Tanzania
Hospital under‐reporting 20% (3/15)

What proportion of maternal deaths occurs at home?
• Pattern of causes among home deaths varies
according to local epidemiological, social and
health system context
• Adjust facility estimates using % of home deaths from household surveys or
DSS

Options for identifying home deaths
• Birth and death registration, sample registration
• Reproductive age mortality studies suing multiple sources
• Key informant reporting• www.immpact‐international.org/toolkit
• www.maternal‐mortality‐measurement.org

Key informants
• Community health workers
• Traditional birth attendants (TBAs) • Health care providers • Village leaders • Religious leaders• Teachers • Political cadres • Cemetery official, workers
• Coffin makers

Can we use routine HMIS reports from health facilities for monitoring?
Yes …. IF• The HMIS covers all facilities or there can be
adjustment for underreporting• All facility deaths on all wards are captured• There is a assessment of quality of HMIS reporting on
maternal health indicators• Studies are conducted to assess patterns of non‐
facility deaths• Facility deaths are used as the starting point for case
reviews to identify avoidable factors• There is reconciliation with other sources of
data
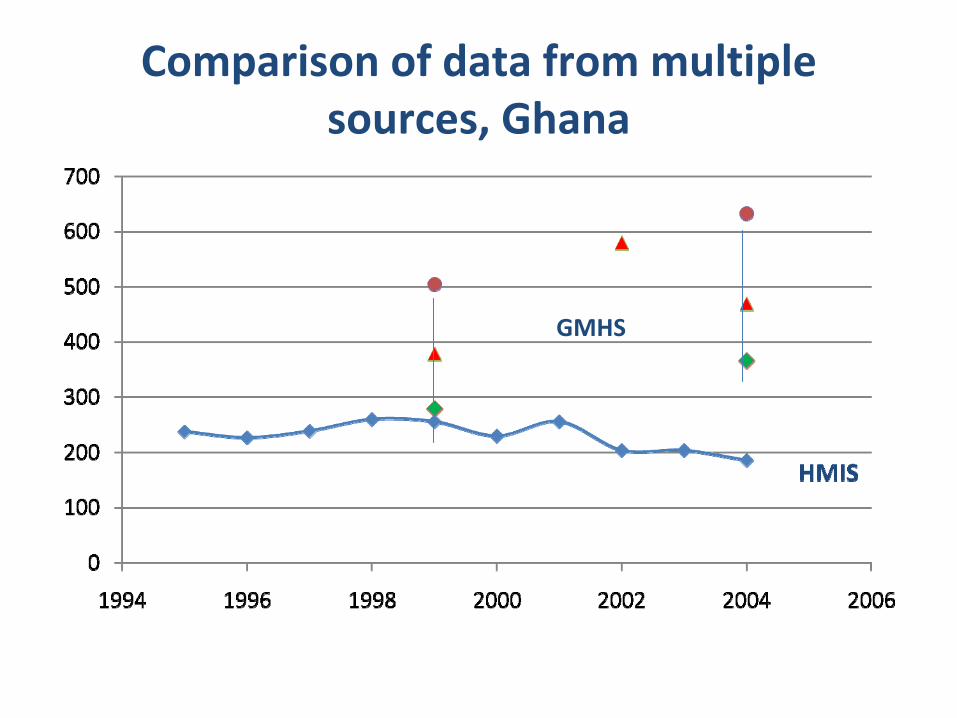
Comparison of data from multiple sources, Ghana
GMHS

Spreadsheet
Evaluating routine HMIS data

Country strategies for improving maternal mortality data
Increase primary data collection using a menu of measurement options:
• Improve quality of facility data, ensuring all maternal deaths captured
• Be more critical of available data and prepared to correct and adjust if needed
• Use facility reported deaths as starting point for audits and confidential enquiries
• Strengthen civil/sample registration and medical certification and coding of deaths
• Make use of multiple sources and mixed methods (surveys, census, facility, incomplete registration, sample registration)
Technical resources
http://www.maternal‐mortality‐ measurement.org/MMMResource _ToolBox.html

Major categories of MMR data sources
• Civil/sample registration
with medical certification or
verbal autopsy• Household surveys• Demographic surveillance• Census
• Facility reporting• Health management
information systems (HMIS)
Population-based estimates
Facility-based estimates

Source Strengths Limitations
Civil/sample
registration with
cause of death
Complete/Representative;Continuous
Not available in developing
countries;
Census Complete count of
events; Occasional; bias, over/under
reporting
Household
surveysRepresentative
population
sample;
Occasional; wide confidence
intervals; do not produce local
area estimates; challenge of
identifying pregnancy‐related
deaths
Facility health
management
information
system
Ongoing; country
owned; timely
reporting; cause‐
specific
Not representative; not all
women deliver in health
facilities; not all facilities report;
not all deaths detected; record‐
keeping;