measuring harm reduction: the effects of needle and syringe exchange programs and methadone...
DESCRIPTION
Ernest Drucker, Peter Lurie*, Alex Wodakt† and Philip Alcabes.*AIDS 1998, 12 (suppl A):S217-5230*"Minimizing the epidemic spread of an infectious disease requires that we carefully examine data on the effectiveness of all interventions believed to reduce transmission. For AIDS, the absence of an effective vaccine and the continued high cost and still undetermined long-term efficacy of antiviral medications dictate a focus on preventing HIV infection - our only available tool to slow the global pandemic [1]. While the effect of combination therapies (using the new protease drugs) on viral load suggests that competent and ongoing medical care for people with HIV/AIDS will reduce their infectivity, the high cost of this approach means it has no public health consequence outside the developed world."TRANSCRIPT

Measuring harm reduction: the effects of needle and syringe exchange programs and methadone
maintenance on the ecology of HIV
Ernest Drucker, Peter Lurie*, Alex Wodakt† and Philip Alcabes*
AIDS 1998, 12 (suppl A):S217-5230
Keywords: Harm reduction, injecting drug use, HIV transmission, methadone maintenance, needle and syringe exchange
A public health approach Minimizing the epidemic spread of an infectious disease requires that we carefully examine data on the effectiveness of all interventions believed to reduce transmission. For AIDS, the absence of an effective vaccine and the continued high cost and still undetermined long-term efficacy of antiviral medications dictate a focus on preventing HIV infection - our only available tool to slow the global pandemic [1]. While the effect of combination therapies (using the new protease drugs) on viral load suggests that competent and ongoing medical care for people with HIV/AIDS will reduce their infectivity, the high cost of this approach means it has no public health consequence outside the developed world. Interrupting transmission of HIV means reducing the susceptibility of the uninfected by controlling the quantity and characteristics of contact with all infectious vectors. But the complex social and behavioral ecology associated with the spread of HIV in human populations makes this very difficult, involving us in some of the most intimate (and often proscribed) areas of personal life: sexuality and drug use. Nonetheless, in order to slow the spread of AIDS, we must examine all available measures for reducing those risks that are associated with the transmission of HIV And, as is always the case in public health, we must pay the closest attention and give the highest (priority to those factors that account for the greatest proportion of incident infections and are most amenable to changes that reduce transmission. Illicit drug use, particularly injecting drug use (IDU), qualifies on both counts it is a potent risk factor for transmission of HIV (as well as for hepatitis and other infectious diseases) and is, we believe, accessible to risk reduction by a number of social and behavioral interventions currently available to us. Drug use and AIDS The overall importance of nonmedical (illicit) drug use for the AIDS pandemic lies in its global prevalence, rapid growth, and central role in igniting regional outbreaks of HIV infection. There are now an estimated 3.4-5.5 million injecting drug users in 120 countries [1], one part of a larger population who constitute the illicit drug market for heroin (8-10 million persons), cocaine (30--40 million), and amphetamines (at least 30 million) .While not all illicit drug use involves injection (for example, cannabis), the practice of IDU has expanded rapidly in the 17 years since AIDS was first identified in 1981, emerging in scores of nations with no prior history of IDU many of which are ill-equipped to restrict drug use in their populations. The prevalence of IDU and the severity of its risks for HIV transmission are fueled by (and fuel) poverty, social dislocation, and political instability. Finally, the rapid expansion of international drug markets creates a profitable criminal `economy' that undermines and corrupts key institutions of civil societies, including those responsible for addressing the public health problems associated with drug use and addiction [2]. IDU has proven itself capable of igniting the regional spread of HIV infection in both developed and developing societies with astonishing speed. This pattern was first evident in poor urban populations in the USA and Europe, but is now also seen in Asia, Africa, and Latin America [3]. From the Montefiore Medical Center/Albert Einstein College of Medicine and the Lindesmith Center, New York, USA, the *University of
California, San Francisco and University of Michigan, Ann Arbor, Michigan, USA, the 'New York University School of Medicine, New York, USA and 'St Vincent's Hospital, Sydney, Australia.
Sponsorship: This work was supported by NIDA under awards DA 09-712 (P.L. and E.D.), R01 DA 11324-01 (E.D.),the Lindesmith Center/The Open Society Institute (E.D.) and the New York University CFAR under NIAID award P30 A127742 (PA.).
Requests for reprints to: Dr Ernest Drucker, Department of Epidemiology and Social Medicine, Montefiore Medical Center, 111 East 210th Street, Bronx, NY 10467, USA.
© Lippincott-Raven Publishers ISBN 1-41284-040-5 ISSN 1350-2840S217
Drug control policies and health risk International drug control strategies and regimes based almost exclusively on prohibition (in other words, on the use of criminal penalties to regulate the sale and use of certain drugs) appear to have been unsuccessful in containing IDU
geographically [3]. In the years of epidemic HIV spread (since the 1970s), despite massively increased interdiction and drug enforcement activities, worldwide heroin and cocaine production have tripled [1], with comparable increases in the prevalence of IDU and addiction. In addition, prohibitive drug policies also affect patterns of drug use in ways that increase individual and public health risk. The necessarily clandestine life of the (criminal) addict fosters several specific patterns of behavior known to increase HIV transmission, most important among these the sharing of scarce injection equipment and increased sex work to get money for drugs. Stigmatizing and marginalizing the drug user also acts as a barrier to access to medical and social services, isolating the drug user from education, prevention, and drug treatment that might ameliorate AIDS and other health risks (for example, overdose). In this context of rapidly expanding drug markets and the growing prevalence of drug use worldwide, the major test of the public health efficacy of specific AIDS prevention measures is, therefore, not their impact on the prevalence of drug use per se (which is a function of drug policies and markets) but, rather, their effect on the transmission risk associated with continued and possibly increased drug use within the current environment, in other words in the context of drug policies based on absolute prohibition. Application of the communicable disease model From a communicable disease standpoint, AIDS in the drug-using population is a vector-borne epidemic, with the needle and syringe serving as the `vector' responsible for transmission of the biologic agent of infection, HIV AIDS control must take into account a social ecology that includes the interaction of drug users with injection equipment (and with drug policies) in ways that determine patterns of drug use and of risk [4]. Clearly, there also can be other modes of HIV transmission in this population, notably sexual and (in countries that cannot protect the blood supply) by transfusion. However, the salient role of the syringe in mediating transmission, the potentially higher transmission potential in MISSING TEXT injection equipment (as opposed to most sexual contact), and the generally higher volume of contact through needles and syringes for addicts (who inject at least once and often many times per day, every day) demand attending to this `vector' in designing intervention strategies for restricting the spread of infection in this population. Public-health practice for limiting communicable disease has long experience in control of arthropod vectors for malaria, yellow fever, dengue, and other diseases. And, although some preventive interventions focus on wholesale ecological change to halt disease spread (for example, draining swamps), the majority rely on one of four broad classes of intervention: immunization, vector elimination, biologic vector control, and personal protection. Immunization, which exists for other vector-borne diseases, is currently unavailable for HIV, and we are still years (at least) away from the earliest possible large-scale vaccine intervention. Vector elimination was embraced as a drug control policy long before AIDS, in the form of `drug paraphernalia' laws. These were based on the (misguided) belief that criminal sanctions would eliminate or severely restrict needles and syringes and thereby limit IDU This policy's disregard for the social ecology of the `vector' and the motivation of its host caused it to backfire as a disease control strategy, forcing users to share injecting equipment more frequently [4]. In some areas of the USA this policy drove IDU into the now-infamous `shooting galleries,' where the spread of HIV was accelerated [5]. Under the circumstance outlined above, the total elimination of the critical vectors of IDU (injecting equipment and addictive drugs) do not seem plausible goals for public-health actions Biologic vector control generally recognizes the complex interactions among vector, pathogen, and host, and seeks to shift the ecological balance by introducing variants of the vector (for example, new species of mosquitoes that will not carry malaria) in hopes that they will outcompete the transmissive vector and take over its ecological niche. The initial use of bleach to sterilize syringes, while raising awareness of risk and creating the vehicle for the first outreach and peer-Ied AIDS prevention programs for IDU in the USA [6], was found to be only partly effective, in part because (like vector elimination) it failed to adequately account for the social circumstance in which IDU occurred and the difficulties this posed for interuse cleaning of injecting equipment [7]. These efforts. however, paved the way for the introduction of sterilesterile injecting equipment in ways that displace contaminated equipment and significantly alter the risk environment of IDU, acting as an effective form of biologic vector control [8]. Personal protection is a common strategy for prevention MISSING TEXT mosquito netting against malaria. yellow fever, or dengue) and sexually transmitted diseases (STD; including condoms to prevent HIV transmission). This model can be applied easily to understanding and modifying risks associated with the ecology of IDU, even within societies that criminalize drug use and injection equipment.The medical provision to addicts of forms of opioid drugs that do not require injection (for example, oral methadone in a maintenance regimen) or sterile injectable drugs and equipment (for example,
heroin maintenance) can eliminate exposure to HIV for the individual drug user in treatment. The more accessible these substitute drugs are and the greater the proportion of addicts using them, the greater the protection they will confer on the entire population of users and their secondary contacts. Evaluating the evidence In the next section of this paper we compile and review the evidence on the public-health impact of two such interventions for interrupting HIV transmission among IDU: needle and syringe exchange programs (NSEP) and methadone maintenance treatment. We summarize the findings and methods of this body of research and update earlier assessments of their impact on AIDS risk factors. A methodological note: in public health, it is often neither feasible nor ethical to conduct strictly randomized controlled trials of interventions. In the midst of an epidemic, such as AIDS, circumstances may preclude the strict control of all collateral risk factors and the illicit nature of drug use impedes the collection of complete and timely data to assess efforts to reduce risks associated with an ever-changing social and behavioral environment in which most illicit drug use occurs. But these limitations do not exempt us from making our best efforts to protect public health or from using existing evidence to inform our actions. By employing a publichealth analvsis of the circumstances of IDU and transmission of HIV (as above), we take advantage of ecological associations, observational studies, and `natural experiments' which point the way towards the best available measures to blunt the epidemic's force. In addressing these same concerns, the report of the USA National Academy of Sciences' Institute of Medicine on the efficacy of NSEP [8] (pages 200-202) weighed both the `traditional approach' (to the preponderance of evidence) and an 'alternative approach' (to the patterns of evidence), concluding that to reject NSEP, based on limitations of the design of single studies, ignores both the preponderance and pattern of the evidence and `is both poor scientific judgment and bad public health policy'. The Institute argued `that the improbability of being able to carry out the definitive study ... does not necessarily preclude the possibility of making confident scientific judgments' and (citing the admonition of the biostatistician A. Bradford Hill in a 1965 address to the Royal Society of Medicine) that `incomplete' scientific evidence `does not confer upon us a freedom to ignore the knowledge we already have, or to postpone the action that it appears to demand'. It is this approach that guides our review and interpretation of the current evidence, and that has (fortunately) guided public-health officials and community-health advocates throughout the world, who have acted based on assessing the relative impact of available interventions and chosen to mount substantial national NSEP and methadone treatment to reduce HIV risk. Indeed, most of the AIDS prevention measures in force today (for example, counseling, promotion of condom use) were begun and had substantial effects long before any controlled trials had demonstrated their efficacy. Needle and syringe exchange NSEP are one of the hallmarks of public-health innovation for AIDS prevention among IDU. These programs not only provide sterile injecting equipment to active IDU, they also offer sex education and prevention materials, referrals to medical care, legal and social services, and drug treatment. And, by reducing the marginalization of drug users, they increase the likelihood that IDU who continue to use drugs will do so more safely. The specific biologic action of NSEP (as a form of vector control) is to reduce the time that needles and syringes spend in circulation; the less time that potentially contaminated injecting equipment circulates among drug users, the fewer individuals it has a chance to `share' and the less chance it has of being contaminated and of being used thereafter by an uninfected user [9]. Ideally, each syringe would be in circulation only long enough to be used by a single person a single time (as the USA Centers for Disease Control recommends [10]) with the potential for eliminating syringe-mediated HIV transmission altogether. The NSEP accomplishes this diminution in syringe lifetime in two ways. First, its volume-related circulation effect is to increase the total number of syringes and needles available in a given time. Since NSEP do not recruit nonusers, the total number of users does not change and the NSEP increases the number of syringes per capita, driving used syringes out of circulation. Second, NSEP increase the rate at which syringes and needles are removed from circulation or, equivalently, reduce the average circulation time of each syringe and needle by physically removing used syringes from circulation, the essence of the `exchange.' This also helps eliminate used syringes in the environment, reducing the risk of inadvertent needlesticks of nonusers.

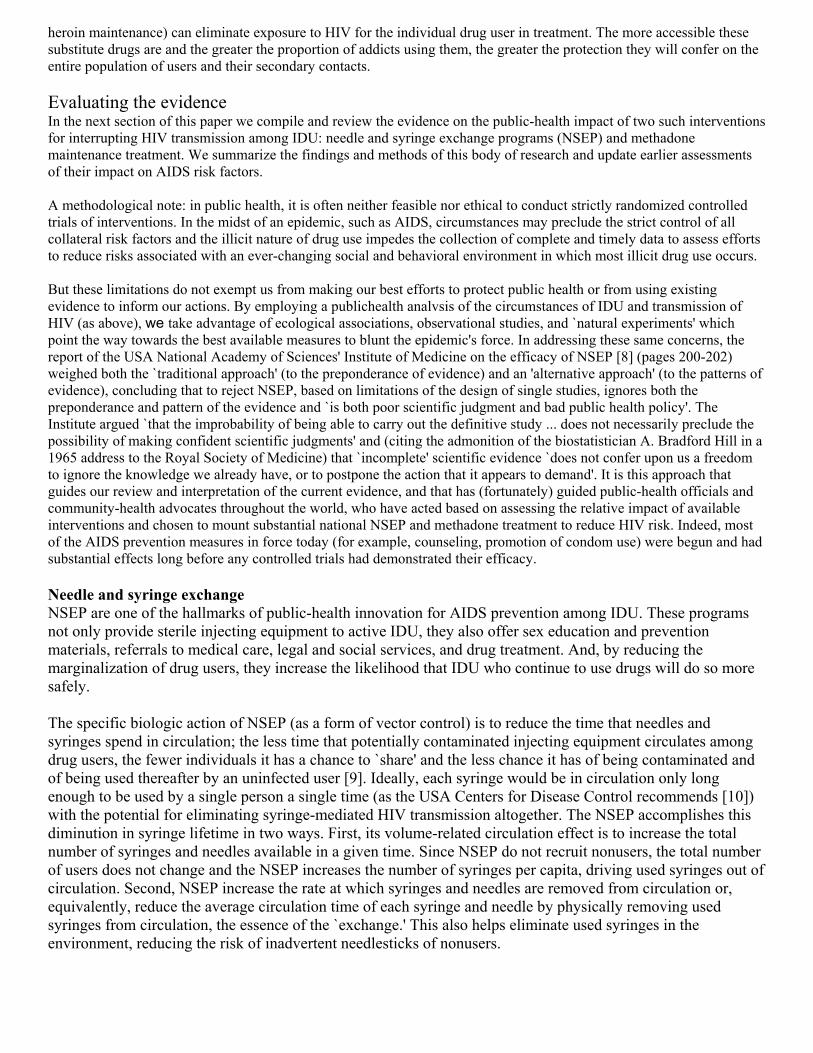
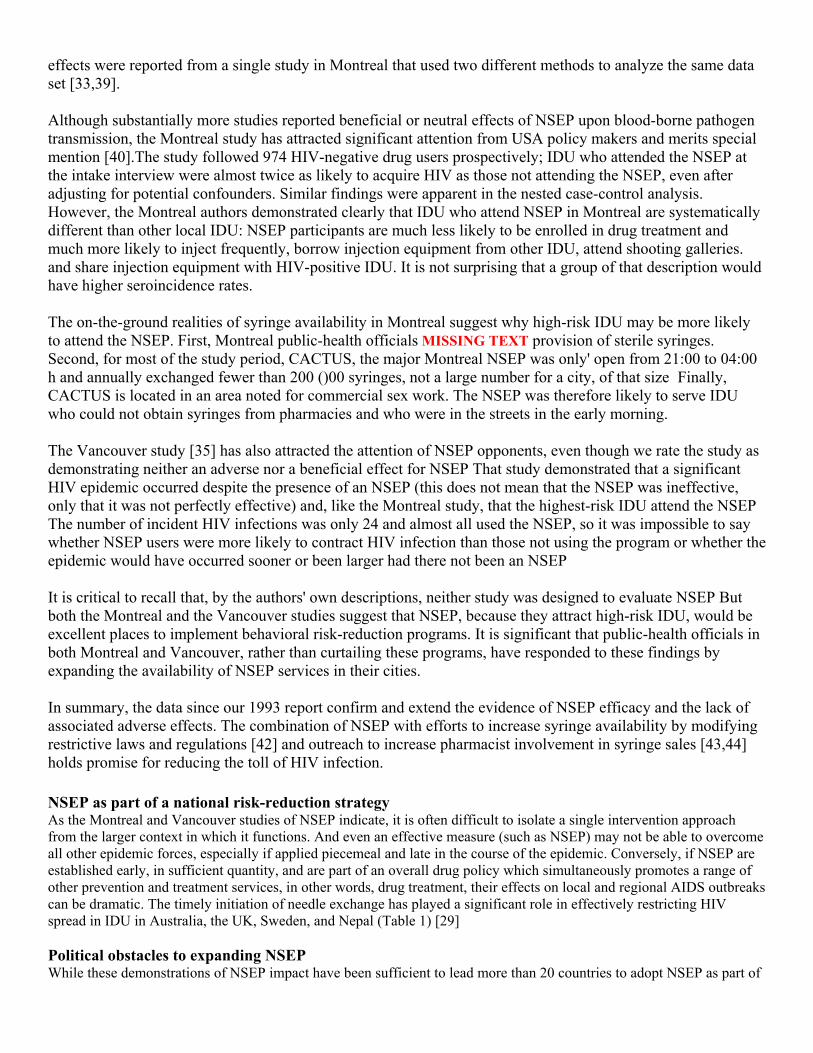
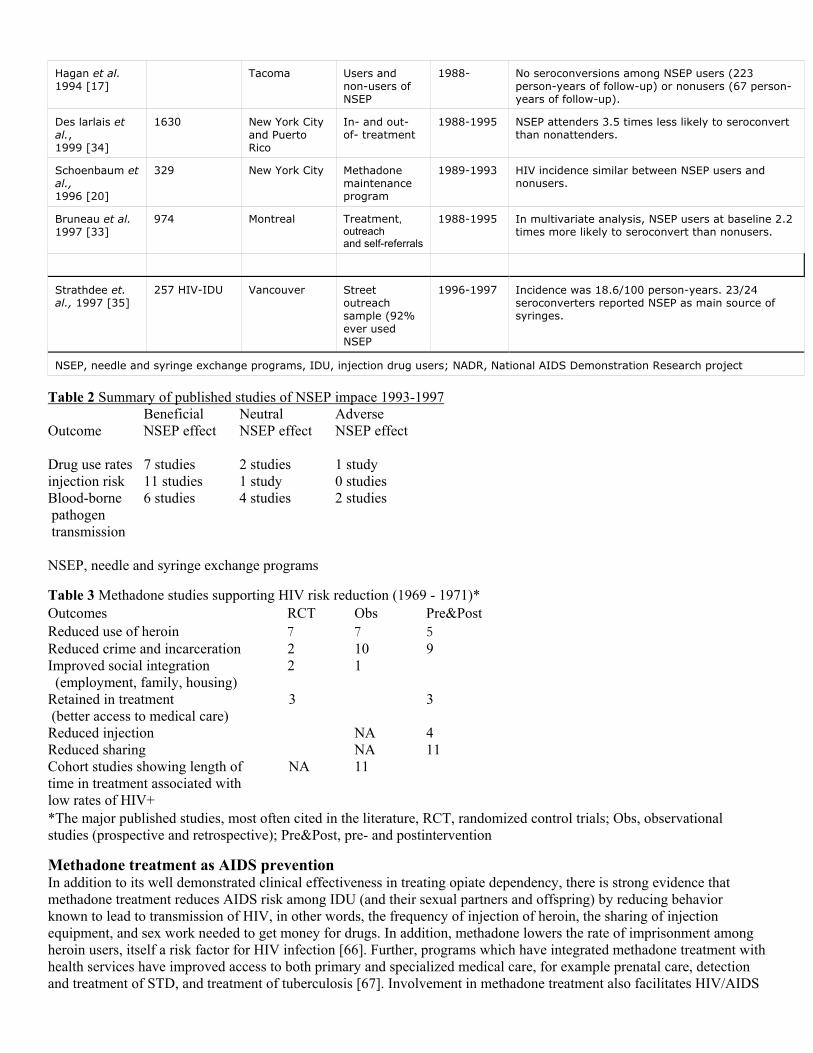
In 1993, one of the present authors was part of a group of researchers who summarized all studies, published and unpublished, then available on the efficacy of NSEP [11]. That review concluded that it was likely that NSEP would reduce HIV incidence and that there was no evidence that NSEP were associated with increases in IDU or community levels of drug use. Since that time, two dozen articles that assess the public health impact of NSEP have been published; in this report we summarize their results. We conducted a computerized literature review using the keyword `needle exchange' for English language articles published from 1993 through to the end of 1997. We examined the references in articles identified by our literature search and contacted NSEP experts to identify additional articles. Books with articles on NSEP were also included, but abstracts from conferences were not. Articles that were only available in abstract form at the time of our previous report were included if they presented at least some new data. We included only articles that addressed the impact of NSEP upon drug use rates, injection-risk behaviors, hepatitis and HIV (Table 1) [12-35]. Serial cross-sectional studies addressing the impact of NSEP upon the IDU community were included as this a key question about the effect of NSEP Otherwise cross-sectional studies were excluded, as they cannot address trends over time and serial cross-sectional studies of particular cities were included only if the data for NSEP participants and nonparticipants were analyzed separately. All changes reported are statistically significant at P < 0.05. If there was more than one statistically significant finding, representative findings are reported. Some studies appear more than once in Table 1 because they addressed more than one outcome or used more than one analytic approach; each is considered a separate study. Studies of cost-effectiveness, changes in sexual risk behavior (there were few of these), and the impact upon referrals to drug treatment were not included. We assumed that successful publication was a rough proxy for quality and did not use a quality scale as in our previous report. We identified a total of 24 articles that have been published since our previous report. The impact of NSEP on drug use rates was addressed in 10 articles, on injection risk behaviors in 12 articles, on hepatitis B and C in one article, and on HIV in 11 articles. The studies were generally of a higher quality than those available in 1993 with a wider range of evaluation designs. In particular, ecological and case-control designs were more common, and prospective studies of HIV incidence had greater statistical power and were therefore analyzed using more sophisticated methods than was possible with the small prospective studies that were available in 1993. Control groups were more often used in the studies measuring NSEP impact upon injection risk behaviors and blood-borne pathogen transmission. Half of the studies were conducted in the USA. The results of the studies are summarized in Table 2 with the different study designs combined. Of the 10 studies MISSING TEXT rates, four serial cross-sectional studies examined the impact of NSEP on drug use rates in the IDU community and the remaining six assessed NSEP impact on drug injection rates of IDU using the NSEP Some studies used mean IDU age to investigate whether young people had begun injecting as a result of the NSEP Seven studies reported reductions in measures of drug use, two reported no change, and one an adverse effect associated with NSEP The latter finding, in a drug treatment cohort, was a greater decline in the percentage of IDU who never used the NSEP and who continued to inject, compared to IDU who ever used the NSEP This observation has been made once before [36], and likely represents self-selection: IDU who expected to continue injecting drugs may have been more likely to select NSEP use. In any event, the number of studies with beneficial or neutral effects of NSEP upon drug use measures greatly exceeds this single study. Eleven out of 12 studies examining injection risk behaviors reported improvements, generally decreases in syringe sharing rates. None showed an increase in injection risk behavior. By comparison, in our 1993 study [37],16 out of 23 studies showed a beneficial NSEP effect, six showed a mixed or neutral effect, and one showed an adverse effect (which was not apparent in subsequent studies [38]). Of the 12 studies examining the impact of NSEP upon blood-borne infections, six reported beneficial effects for NSEP, four reported neither a beneficial nor an adverse effect, and two reported an adverse effect. The adverse
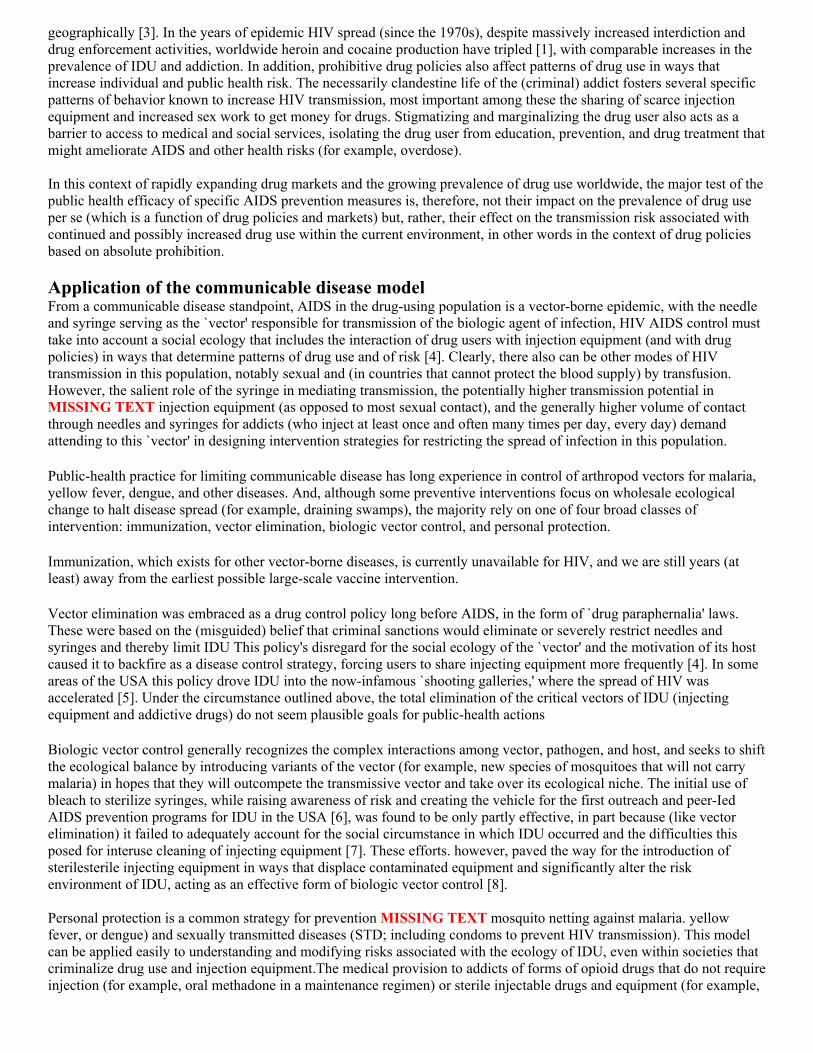
effects were reported from a single study in Montreal that used two different methods to analyze the same data set [33,39]. Although substantially more studies reported beneficial or neutral effects of NSEP upon blood-borne pathogen transmission, the Montreal study has attracted significant attention from USA policy makers and merits special mention [40].The study followed 974 HIV-negative drug users prospectively; IDU who attended the NSEP at the intake interview were almost twice as likely to acquire HIV as those not attending the NSEP, even after adjusting for potential confounders. Similar findings were apparent in the nested case-control analysis. However, the Montreal authors demonstrated clearly that IDU who attend NSEP in Montreal are systematically different than other local IDU: NSEP participants are much less likely to be enrolled in drug treatment and much more likely to inject frequently, borrow injection equipment from other IDU, attend shooting galleries. and share injection equipment with HIV-positive IDU. It is not surprising that a group of that description would have higher seroincidence rates. The on-the-ground realities of syringe availability in Montreal suggest why high-risk IDU may be more likely to attend the NSEP. First, Montreal public-health officials MISSING TEXT provision of sterile syringes. Second, for most of the study period, CACTUS, the major Montreal NSEP was only' open from 21:00 to 04:00 h and annually exchanged fewer than 200 ()00 syringes, not a large number for a city, of that size Finally, CACTUS is located in an area noted for commercial sex work. The NSEP was therefore likely to serve IDU who could not obtain syringes from pharmacies and who were in the streets in the early morning. The Vancouver study [35] has also attracted the attention of NSEP opponents, even though we rate the study as demonstrating neither an adverse nor a beneficial effect for NSEP That study demonstrated that a significant HIV epidemic occurred despite the presence of an NSEP (this does not mean that the NSEP was ineffective, only that it was not perfectly effective) and, like the Montreal study, that the highest-risk IDU attend the NSEP The number of incident HIV infections was only 24 and almost all used the NSEP, so it was impossible to say whether NSEP users were more likely to contract HIV infection than those not using the program or whether the epidemic would have occurred sooner or been larger had there not been an NSEP It is critical to recall that, by the authors' own descriptions, neither study was designed to evaluate NSEP But both the Montreal and the Vancouver studies suggest that NSEP, because they attract high-risk IDU, would be excellent places to implement behavioral risk-reduction programs. It is significant that public-health officials in both Montreal and Vancouver, rather than curtailing these programs, have responded to these findings by expanding the availability of NSEP services in their cities. In summary, the data since our 1993 report confirm and extend the evidence of NSEP efficacy and the lack of associated adverse effects. The combination of NSEP with efforts to increase syringe availability by modifying restrictive laws and regulations [42] and outreach to increase pharmacist involvement in syringe sales [43,44] holds promise for reducing the toll of HIV infection. NSEP as part of a national risk-reduction strategy As the Montreal and Vancouver studies of NSEP indicate, it is often difficult to isolate a single intervention approach from the larger context in which it functions. And even an effective measure (such as NSEP) may not be able to overcome all other epidemic forces, especially if applied piecemeal and late in the course of the epidemic. Conversely, if NSEP are established early, in sufficient quantity, and are part of an overall drug policy which simultaneously promotes a range of other prevention and treatment services, in other words, drug treatment, their effects on local and regional AIDS outbreaks can be dramatic. The timely initiation of needle exchange has played a significant role in effectively restricting HIV spread in IDU in Australia, the UK, Sweden, and Nepal (Table 1) [29] Political obstacles to expanding NSEP While these demonstrations of NSEP impact have been sufficient to lead more than 20 countries to adopt NSEP as part of

their national AIDS prevention strategy, USA Federal health authorities have been unyielding in their opposition to NSEP [29]. At the time of writing, the USA still bans the use of Federal funds for NSEP despite the many USA studies demonstrating their safety and efficacy, and the clear and repeated recommendations of two National AIDS Commissions, the National Academy of Science's Institute of Medicine, and leading USA government experts calling for Federal support of NSEP Further, the USA appears to have some influence in sustaining hostility to NSEP in other countries (Russia, Sweden). This USA national policy is a landmark failure of public health in the USA: one study [31] found that expanded provision of NSEP in the USA (with over one million injectors) would have prevented 10,000 to 20,000 HIV infections in the past decade. Methadone Substitution treatment or maintenance pharmacotherapy using methadone is today the most sought after and effective form of treatment for opiate addiction [45]. Because methadone is a long-acting opiate whose dosage can be stabilized, it is well suited to daily administration and has proven effective in the elimination of narcotic craving, a driving force behind continued heroin use [46]. And, because it can be administered orally, methadone dramatically reduces heroin injecting frequency and, with it, associated risks for HIV and other blood-borne pathogens (Table 3). Methadone treatment effectiveness The clinical effectiveness of methadone is most commonly measured by its retention of patients in care and by reductions in heroin use as well as improvements in social outcomes, for example, employment, family integration, and reduced arrests and incarceration for criminal offenses [47]. Both randomized trials and observational studies (Table 4) [5,48-59] have determined that methadone maintenance retains patients at levels two to four times that of other treatment modalities (in other words, >75%, 12-month retention) [60], and the longer patients remain in treatment, the better the results, for example, for those in treatment more than 24 months, methadone reduces the use of heroin to levels below 15% of those in the period immediately before treatment [61]. Conversely, even among those who have greatly reduced their heroin use while in methadone treatment, over 80% relapse to heroin use when they leave treatment [62]. The most basic public-health benefit of methadone treatment can be seen in the reduction of mortality rates among IDU who remain in treatment, observed in randomized clinical trials [63], and later follow-up [64], and, most recently, in population data from Australia documenting that the (nonHIV-related) mortality rate of patients in methadone treatment was 25% that of drug users not in treatment [65]. Table 1. Studies of needle and syringe exchange program effectiveness published since 1993
Reference Number Location Recruitment Year of Study
Summary of Findings
Studies of changes in drug use rates Serial cross-sectional studies
Walters et al. 1994 [12]
5644 San Francisco Drug detox and street recruited
1986-1992 Percent using NSEP at least 25 times in previous year increased from 14% in 1989 to 28% in 1992. Number of daily injections decreased from 1.9 in 1987 to 0.7 in 1992. Mean age increased from 36 years in 1987 to 42 in 1992.
Hunter et al., 1995 [13}
"500/year London In- and out- of- treatment IDU
1990-1993 Percent using NSEP as main syringe source increased from 37% to 50%. Mean age rose from 28 to 32 years. Percent injecting daily remained stable.
Peak et al., 1995 {14]
59-200/year Kathmandu IDU at NSEP 1991-1994 Number of injections per month decreased from median of 21 to 15.
Des Jarlais et al., 1994 [15]
1115 New York City Detox program 1984 1990-1992
Mean IDU age increased from 32 years to 36 years. Number of cocaine injections per month declined from 55 to 43 as injection frequency of other drugs remained stable.
Fennema el al., 1997 [16]
"200/year Amsterdam Street recruited IDU
1990, 1993 1996
Duration of drug injection increased from 10 years to 14 years. Mean age increased from 28 years to 37 years. Decrease in percent injecting ? twice a day from 74%, to 56%,.
Retrospective cohort studies

Hunter et al., 1994 [17]
426 Tacoma IDU at NSEP 1988- Number of injections per month remained stable
Paone et. al., 1994 [18]
1752 New York City IDU at NSEP
1992-1993
Numbinjectmontdeclinfrom
Prospective cohort studies
Oliver et al., 1994 [19]
77 frequent NSFP users and 355 NADR clients
Portland NSEP and outreach clients
1989-1991 Change in percentage of IDU reporting injecting now similar in NSEP users and NADR clients.
Schoenbaum et al., 1996 [20]
329 New York City Methadone main-tenance program
1989-1993 61 % relative decline in proportion of non-NSEP users continuing to inject versus 14% relative decline in those ever using the NSEP.
Vlahov et al., 1997 [21]
221 Baltimore IDU at NSEP 1994-1995 Percent injecting at least daily decreased from 97% at baseline to 77% at 6 months. Number of injections per clay decreased from 5.7 at baseline to 4.2 at 6 months.
Studies of changes in injection risk behaviors
Serial cross-sectional studies
Walters et al., 1994 [12]
5644 San Francisco Drug detox and street recruited
1986-1992 Percent using NSEP at least 25 times in previous year increased from 14% in 1989 to 28% in 1992. Decrease in sharing from 66%, in 1987 to 36% in 1992 for full study population. In multivariate analysis, greater use of NSEP associated with less sharing.
Hankins et al., 1994 [22]
Montreal IDU at NSEP Lending of needles decreased from 31% at opening of NSEP to 20%,. Bleach use increase from 30%, at opening of NSEP to 62%.
van Ameijden et al., 1994 [23]
616 Amsterdam In- and out-of- t 1986-1992 In multivariate analysis, current NSEP use associated with reduction in reuse of syringes.
Peak et al., 1995 [14]
59-200/year Kathmandu IDU at NSEP 1991-1994 Number of times syringes shared per month declined from 13 to 8.
Retrospective cohort studies
Frischer and Elliot, 1993 [24]
503 Glasgow IDU using and not using NSEP
1990 In multivariate analysis, NSEP users had made more harm reduction changes than nonusers.
Keene el al 1993 [25]
328 Wales IDU using and not using NSEP
1990-1991 NSEP users and nonusers had similar rates of ever sharing syringes, but 18"6, of users shared syringes in past year compared to 52% of nonusers.
Hagan et al., 1993 [17]
426 Tacoma IDU at NSEP 1988- 64º/<, relative reduction in percent injecting with at least one used syringe per month. 67% relative reduction in percent passing on used syringe al least once per month.

Paone et al., 1994 [18]
1752 New York City IDU at NSEP 1992-1993 Injection with previously used syringes declined from 12%, of the time to 4%. Percent injecting with previously used syringes declined from 22% to 6%.
Hahn et.al. 1997 [26]
141 San Francisco IDU in drug treatment
1989-1990 Number of sharing partners declined equally in IDU who ever and never used NSEP
Prospective cohort studies
Oliver et al., 1994 [19]
77 frequent NSEP users and 355 NADR clients
Portland NSEP and outreach clients
1989-1991 Greater reductions in percentage reporting reuse of syringes and throwing away syringes in NSEP clients than in NADR clients.
Schoenbaum et al., 1996 [20]
329 New York City Methadone maintenance program
1989-1993 Needle sharing declined more among IDU ever using the NSEP than among nonNSEP users
Vlahov et al., 1997 [21]
221 Baltimore IDU at NSEP 1994-1995 Per cent using someone elses’ syringe in previous 6 months decreased from 22% at baseline to 8%, at 6 months follow-up. Per cent giving syringe to friend in previous 6 months declined from 27% at baseline to 12% at 6 months follow-up. Number of injections per syringe declined from 12.8% at baseline to 3.6% at 6 months follow-up.
Studies of Hepatitis B and C
Case-control studies
Hagan et al. 1995 [27]
28 IDU with hepatitisB and 20 with hepatitis C
Tacoma IDU using health department services
1991-1993 For hepatitis B, ever use of NSEP associated with adjusted odds ratio of 5.5. For hepatitis C, 'ever use of NSEP associated with adjusted odds ratio of 7.3
Studies of HIV
Ecological studies
Des larlais et al., 1999 [34]
>7300 Worldwide IDU in five cities with stable seroprevalence
1984-1993 Cities with consistently low seroprevalence had all made efforts to provide sterile injection equipment.
Hurley et a1., 1997 [29]
332 892 IDU Worldwide IDU in 81 cities (75% of IDU in treatment)
1984-1994 HIV seroprevalence declined 5.8% per year in 29 cities with NSEP and increased 5.9% per year in cities without NSEP.
Mathematical modeling studies
Kaplan et al. 1994 [30]
New Haven 1990-1992 HIV prevalence in NSEP syringes returned decreased from over 69% to under 45% This decrease not explained by changes in client demographics.
Lurie and Drucker 1997 [31]
USA 1987-2000 Up to 9666 HIV infections could have been prevented by NSEP by 1995. Will cost $244 million to treat those infections.
Case-control studies
Patrick et al, 1997 [32]
89 cases 192 controls
Vancouver Referrals, outreach, self-referral
1994 In multivariate analysis, no relationship between frequency of NSEP use and HIV seroconversion
Bruneau et al. 1997 [33]
88 cases 320 controls
Montreal Treatment, outreach and self-referrals
1988-1995 In nested case-control analysis, exclusive NSEP users 6.5 times as likely to seroconvert.
Prospective cohort studies
Hagan et al. 1994 [17]
Tacoma Users and non-users of NSEP
1988- No seroconversions among NSEP users (223 person-years of follow-up) or nonusers (67 person-years of follow-up).
Des larlais et al., 1999 [34]
1630 New York City and Puerto Rico
In- and out-of- treatment
1988-1995 NSEP attenders 3.5 times less likely to seroconvert than nonattenders.
Schoenbaum et al., 1996 [20]
329 New York City Methadone maintenance program
1989-1993 HIV incidence similar between NSEP users and nonusers.
Bruneau et al. 1997 [33]
974 Montreal Treatment, outreach and self-referrals
1988-1995 In multivariate analysis, NSEP users at baseline 2.2 times more likely to seroconvert than nonusers.
Strathdee et. al., 1997 [35]
257 HIV-IDU Vancouver Street outreach sample (92% ever used NSEP
1996-1997 Incidence was 18.6/100 person-years. 23/24 seroconverters reported NSEP as main source of syringes.
NSEP, needle and syringe exchange programs, IDU, injection drug users; NADR, National AIDS Demonstration Research project
Table 2 Summary of published studies of NSEP impace 1993-1997 Beneficial Neutral Adverse Outcome NSEP effect NSEP effect NSEP effect Drug use rates 7 studies 2 studies 1 study injection risk 11 studies 1 study 0 studies Blood-borne 6 studies 4 studies 2 studies pathogen transmission NSEP, needle and syringe exchange programs T able 3 Methadone studies supporting HIV risk reduction (1969 - 1971)* O utcomes RCT Obs Pre&Post Reduced use of heroin 7 7 5 Reduced crime and incarceration 2 10 9 Improved social integration 2 1 (employment, family, housing) Retained in treatment 3 3 (better access to medical care) Reduced injection NA 4 Reduced sharing NA 11 Cohort studies showing length of NA 11 time in treatment associated with l ow rates of HIV+ *The major published studies, most often cited in the literature, RCT, randomized control trials; Obs, observational studies (prospective and retrospective); Pre&Post, pre- and postintervention Methadone treatment as AIDS prevention In addition to its well demonstrated clinical effectiveness in treating opiate dependency, there is strong evidence that methadone treatment reduces AIDS risk among IDU (and their sexual partners and offspring) by reducing behavior known to lead to transmission of HIV, in other words, the frequency of injection of heroin, the sharing of injection equipment, and sex work needed to get money for drugs. In addition, methadone lowers the rate of imprisonment among heroin users, itself a risk factor for HIV infection [66]. Further, programs which have integrated methadone treatment with health services have improved access to both primary and specialized medical care, for example prenatal care, detection and treatment of STD, and treatment of tuberculosis [67]. Involvement in methadone treatment also facilitates HIV/AIDS

screening programs and medical care, and helps adherence to the new antiviral combination therapies. Table 3 shows a summary of these effects from the major studies on methadone published between 1969 and 1997, documenting each specific area of methadone treatment's impact relevant to HIV risk reduction, by type of outcome.
Enrollment and retention in treatment and HIV Retention in methadone treatment varies as a function of program characteristics [68] and dose [69], but length of time in treatment is generally associated with lower rates of HIV, especially if treatment is initiated early in the course of the local epidemic of HIV among IDU [5]. A striking example of this effect can be seen in the virtual absence of HIV infection among IDU admitted for methadone treatment in New York City prior to 1978 [49] and lower HIV rates among those with more time undergoing methadone treatment [70], a finding confirmed by subsequent studies in the USA, Europe, and Austraha. Most studies of methadone are observational (random assignment to methadone being ethically inconsistent with the evidence of its efficacy), and involve self selection into methadone treatment (or the choice to leave it). One early study that did involve random assignment among applicants to a limited-capacity methadone program began in Sweden in the early years of AIDS, and found that only 3% of those admitted before 1983 were HIV-positive. However, 16% of those subsequently admitted (between 1984 and 1986) and 57% of those admitted after 1987 tested positive for HIV [64]. Further, among those HIV-negative individuals admitted since 1984, no seroconversions occurred in 3-4 years of follow-up. Low-threshold methadone programs and those employing general practitioners have proven effective in attracting more marginal IDU to longer term methadone treatment, but are more difficult to assess regarding reduced HIV rates [23,71,72]. Reduced intravenous drug use Early observational studies of methadone patients compared to active heroin users [73] found 80-90% reductions in daily heroin use among those in treatment. The two most comprehensive prospective studies of continued IDU among USA methadone patients, the Three Cities Study by Ball and Ross [62] (1991) and The Treatment Outcome Evaluation Study (TOPS) [74], both found sharp reductions of injecting heroin within weeks of entering treatment and steady reductions in the level of IDU as a function of time in treatment (in TOPS by 77% among those in treatment > l 8 months). Sufficient methadone dose (6()-100 mg) is a critical factor in predicting reduced IDU and concurrent cocaine use often predicts higher injecting; and sharing rates [55,75]. In prisons which provide methadone. similar positive results have been observed, with reduced injecting both during incarceration and afterwards [76-78]. Reduced sharing of injecting equipment Sharing of injecting equipment is generally related to the frequency of IDU, which is almost universally reduced by methadone treatment. Concurrent use of cocaine and shooting galleries, however, increases the likelihood of sharing as it does among drug users with the most marginalized social circumstances (for example, homelessness [79]). However, cocaine use is lowered when higher doses of methadone are used and is inversely correlated with longer time in treatment and withdrawal from the drug culture. In jails and prisons, the role of methadone is especially significant for HIV risk because of the almost universal sharing of (contraband) injection equipment, and the high background prevalence rates of HIV among incarcerated IDU [80], who commonly constitute 50% of prison populations in the USA and Europe.
Table 4. Studies on methadone treatment effectiveness published since 1987.
Author Year Place Study No. of Subjects Outcome
Moss et. al., [48]
1994 San Francisco, USA Observational 2531 heterosexual intravenous drug users (681 HIV-negative initially)
HIV seroconversion rate 1.9'% ppy. Risk behaviour reduction over 5 years: intravenous cocaine 18%, shooting gallery 13% proportion with more than 5 sex partners 15% Methadone highly protective (less than 1 year methadone hazard ratio for seroconversion = 2.7: P = 0.02). Stable attendance at methadone maintenance was highly protective: the seroconversion rate in subjects with one year or more in methadone was 1% ppy.

Novick et. al., [49]
1990 New York, USA Retrospective review
58 long-term, socially rehabilitated methadone-maintained, pre-treatment 10.3 +/- 1.7 years heroin injecting
0/58 (0%) HIV-positive: 53/58 (91%) at least one HBV marker.
Vanichseni et. al., [50]
1991 Bangkok, Thailand Controlled trial (methadone maintenance, 45 day methadone detoxification)
240 male heroin addicts with at least Six prior detoxification treatment episodes
Methadone maintenance clients more likely to complete 45 days treatment (P <0.0001); less likely to have used heroin during treatment (P < 0.0002); less likely to have used heroin on the 45th day of treatment (P <0.000007)
Ball et. al., [51]
1988 Six programs in three cities in eastern USA
Observational 633 males were interviewed initially (113 new admissions and 520 already in treatment for at least 6 months). A year later 388 remained in treatment and 107 had left treatment during the previous year
Of the 388 patients still in treatment, 36% had not injected again after the first month of treatment; an additional 22% had not injected in the past year and a further 13% had not injected for a period of between 1 and 11 months. The remaining 29%, had injected in the past month. Overall, 71% had not injected in the last month with similar results for sharing (both numbers of sharers and frequency of sharing).
Metzger et. al., [52]
1993 Philadelphia, USA
Observational 152 in-treatment, 103 out-of-treatment from same neighborhood as methadone maintenance unit
At baseline 10% of methadone maintained group and 16% of out-of-treatment group HIV-positive. Over 18 months, 3.5% of methadone maintained subjects and 22% of those out-of-treatment initially HIV-negative seroconverted. Out-oftreatment subjects injected drugs, shared needles, visited shooting galleries, and practised unsafe sex at significantly higher rates than in-treatment subjects.
Stark and Muller [53]
1993 Berlin, Germany Cross-sectional, multisite sampling
472 Current borrowing of syringes was associated with younger age, shorter history of intravenous drug use, negative HIV serostatus and nonparticipation in methadone maintenance program.
Schoenbaum et. al., [5]
1990 New York, USA Observational 452 patients in methadone treatment
HIV infection associated with more injections per month, higher percentage of injections with used needles, more injections with cocaine per month, higher percentage of injections with needles shared with strangers or acquaintances.
Marmor et. al., [54]
1987 New York, USA Observational 308 hospital-based methadone maintenance or drug detoxification, Manhattan, New York City
50.7% HIV-positive. HIV infection associated with more frequent drug injection, higher proportion of injections in shooting galleries, male to male sex.

Chaisson et. al., [55]
1989 San Francisco, USA Observational 633 heterosexual intravenous drug users
HIV infection associated with intravenous cocaine use, drug use in shooting galleries, sharing of drug injection equipment. Multivariate analysis found black race, daily cocaine injection by blacks and Hispanics, all other cocaine injection, heavy drug use prior to entry into methadone treatment by blacks and use of drugs in shooting galleries were independent predictors of HIV infection. Methadone associated with substantial reduction in heroin use and some reduction in cocaine use.
Brown et. al., [56]
1989 New York, USA Multisite,cross-sectional
454 patients in methadone maintenance
Frequent use of intravenous drugs, duration of drug use, and duration of drug treatment enrolment were significantly associated with HIV infection and complications.
Williams et. al., [57]
1992 New Haven, CT, USA Observational 56 patients in continuous methadone maintenance treatment, 42 with interrupted methadone treatment
Subjects in continuous treatment reported less needle sharing, fewer needle sharing partners, fewer sexual partners and were more likely to be women.
Selwyn et. al., [58]
1987 New York, USA Cross-sectional 261 intravenous drug users either in methadone maintenance treatment or a large detention facility in NYC
Continued needle sharing behaviour associated with detention facility site and lower scores on age knowledge questionnaire. Reduced needle sharing among methadone maintained and subjects with greater knowledge about AIDS.
Serpelloni et. al., [59]
1994 Verona, Italy Nested case-control study
40 cases (seroconverters), 40 controls (HIV-negative injecting drug users).
HIV seroconversion associated with number of cycles of treatment, daily dose and time out of treatment (univariate analysis). Daily dose (linear effect) and time out of treatment most important risk factors (multivariate analysis). Risk of HIV infection increased 1.5 times for every 3 months spent out of treatment.
ppy, Per person-years; HBV, hepatitis B virus Reduced sex work Drug treatment is often found to be less effective in reducing sexual risk behavior than injecting or sharing [81], in part because female IDU may use condoms with sexual customers, but not with their regular partners who are more likely also to be IDU and HIV-positive [82]. However, retention in methadone treatment is associated with reduced arrest rates for women for prostitution, a marker for higher HIV risk. And some studies [83] indicate that, for those who continue to inject, participation in methadone treatment is associated with greater use of NSEP, which provide condoms and other social supports favoring reduced sexual risks. Reduced arrests/incarceration and the role of methadone in prisons In the earliest demonstration of effects on criminal behavior, the growth of New York City's methadone treatment capacity (in the 1970s) from 20 000 to 34 000 patients corresponded with 25 000 fewer drug arrests [84]. A 90% reduction in drug imprisonment in Hong Kong also followed initiation of a low-threshold methadone program [85]. It is the potential to expand methadone treatment in jails and prisons, however, that offers the greatest promise for HIV reduction [55] because IDU continues in these settings, albeit at lower levels of use but with far fewer syringes and greater likelihood of sharing. Furthermore, because drug users spend so much of their careers incarcerated and because relapse

frequently occurs shortly after release, they are particularly vulnerable populations for HIV infection and are prime candidates for methadone to begin during incarceration and to be continued post release New forms of methadone treatment In the face of the HIV epidemic, many countries have developed low-threshold approaches which expand the availability of methadone treatment, for example, the Netherlands' Methadone Bus and Beth Israel's interim program in New York City. Most significantly, the rapid expansion of office-based methadone within general medical practice has become the norm in many countries [86-88], and allowed some countries to expand rapidly the availability of methadone treatment (for example, in Australia, tenfold increase in 10 years) and help avert the growth of HIV prevalence among IDU [89,90]. Methadone is also now being incorporated within some residential therapeutic communities [91]. In addition, a longer-lasting version of methadone (LRAM) is now being used to reduce the frequency of dosing (and costs) and to alleviate concerns about dispensing take-home doses of potentially dangerous narcotics. International differences in access to methadone The number of methadone treatment places is a critical determinant of its potential public health (or population) impact. Worldwide, there are dramatic differences in the availability of methadone treatment: from <10 in France and Belgium to 80 in Denmark per 100 000 population [92]. Availability is 45 per 100 000 in the USA, but, with 115 000 patients in care, 10 states still have no methadone treatment [93]. While some countries (such as the Netherlands) have provided a wide range of drug treatment options (including methadone) that reach over 75% of the IDU population, fewer than 15% of the 2 000 000 opiate addicts in the USA and Europe today have access to methadone. In eastern Europe and most of Asia, these proportions are far lower [94]. Expansion of methadone is still limited by widespread medical misunderstanding of methadone treatment and (often) very deep-seated hostility to the concept of ,substitution' treatment for opiate dependency. Thus, in Germany, until very recently, doctors were barred by law from using methadone (some were even imprisoned for prescribing it) and methadone is still in only limited use, mainly for patients with HIV infection. In Belgium, there were only a few hundred patients on methadone treatment until 1992, when the general physicians' union successfully mounted a legal challenge to psychiatric restraints on its use [84]. France (with >50 000 IDU) had only 50 patients in methadone treatment as late as 1993, when the medical human-rights communities and a powerful social and health insurance organization successfully fought a resistant psychiatric profession to institute methadone treatment as a national public-health program within general medicine [95]. In the USA, where it was first developed and adopted on a massive scale, however, methadone has lost ground. Throughout the two decades of the AIDS epidemic among IDU in the USA, there has been no real expansion of the methadone maintenance treatment program in the USA and, in some states, severe limits are placed on time in publicly financed treatment, doses are subtherapeutic, and large fees are charged for private programs [96]. Strong prejudice against methadone continues in the (generally) abstinence-oriented USA drug treatment world. Beyond methadone Methadone is not the only drug substitution option available to medical practitioners. Faced with severe restrictions on methadone prescribing, German physicians developed a system of maintenance using oral codeine, with over 35 000 patients in treatment. Results have been positive. French general practitioners are prescribing buprenorphine in far greater numbers (30 000 patients) than they do methadone. These new developments are pushing the boundaries of addiction treatment within medical practice and offering significant therapeutic advantages over the current narrow spectrum of available pharmacotherapies, along with the prospect of including more patients in care and effecting decisive reductions in the spread of HIV Most significantly, in 1995, the Swiss began a landmark program of injectable heroin maintenance for longer-term addicts who had previously failed in treatment with methadone [97]. The 1200 patients included can visit any of 20 clinic sites throughout Switzerland up to three times a day, to inject pharmaceutical heroin under medical supervision. The preliminary evaluation by the Swiss Federal Health Ministry (with over 1800 person-years of data) indicates that 1-year retention in treatment is >80%, sharp reductions have occurred in arrests and criminal activity, and there is greater involvement with non-drug using family and friends, all while injecting a median of 400 mg of heroin each day.

Conclusion: harm reduction These two public health strategies, NSEP and maintenance pharmacotherapy for opiate dependency (especially methadone), are among our best available response to the AIDS epidemic in drug users. Both build on established public-health principles of disease control, acting on one or more elements of the complex ecology of HIV among drug injectors to reduce transmission. These elements include the vector-control approach mentioned above, separation of the potential host (the user) from the vector (in other words, needles and syringes), and reducing the susceptibility of opiate dependent drug users through making safer alternative forms of opiates more accessible through medical services. The common goal of these efforts is `harm reduction'; not ending drug use, but reducing the population morbidity and mortality rates associated with HIV [98-101]. This approach to IDU and AIDS prevention is clearly along the lines of the steps taken to deal with other dangerous drugs, for example, alcohol. In countries that tolerate and regulate alcohol use (rather than prohibiting it) harm-reduction strategies now include standard unit labeling, availability of low-alcohol beverages, designated driver programs, and coordinated national media campaigns, backed up by road testing for blood alcohol level with strict enforcement. National Harm Reduction Drug Strategies for all drugs (licit and illicit) can be seen today in many countries [102]. These strategies have proven effective in stopping or slowing the spread of AIDS in quite different societies (for example, the UK, Australia, Nepal, Thailand, and parts of the USA). Today, however, instead of instituting more harm reduction services and working for social improvement that might prevent drug abuse (for example, jobs, housing, healthcare, and schools), many nations continue building prisons, and most addicts spend more time in prison than in treatment. In the USA, which leads the world in the rate of incarceration of its citizens (most of it associated with the prosecution of drug users), over 3.5 million Americans are in the control of the criminal justice system and 1.5 million behind bars, including 35% of all young African-American men [103]. These national programs of massive prosecution and incarceration of addicts further destabilize exactly those communities most vulnerable to drugs and AIDS, destroying social capital, and damaging many social and civic institutions vital both to order and to public health. In public health, we seek pragmatic solutions which produce demonstrable and reproducible results, measured in reduced rates of morbidity and mortality. In the case of AIDS, because of the large populations and many societies at risk, the stakes are very high. The uneven burden of HIV infection and AIDS faithfully reiterates all of our social, economic, and political tensions and inequalities. How could it be otherwise' As the rapid globalization of the economy proceeds unchecked in much of the world, by restraining social welfare policies and uprooting large populations it creates a lethal ecology of poverty, social dislocation, and despair [104,105] from which, predictably, many people seek escape in drugs. And, just as predictably, others will seek to profit from the physical dependency that these drugs engender. So it will take more than sterile needles and methadone to stop the AIDS epidemic associated with drug use. But while we (literally) await the millennium and AIDS continues to spread, we have a clear obligation to employ the best public-health tools available to protect the millions of people affected. Acknowledgement The authors wish to thank Alicia Knowles. Ann Arbor, Michigan, for her assistance.

1.Mann J, Tarantola D: AIDS In The World 11. New York: Oxford; 1996. 2. Drucker E: Harm reduction: a public health
strategy. Curr issues Public Health 1995, 1:64-70.
3. Ball A, Des Jarlais D, et al.: Multi-Center Study on Drug Injecting and Risk of HIV Infection. Geneva: WHO; 1991.
4. Grund JPC, Stern LS, Kaplan CD, Adriaans NFP, Drucker E: Drug use contexts and HIV-consequences: the effect of drug policy on patterns of everyday drug use in Rotterdam and the Bronx. Br ] Addiction 1992, 87:41-52.
5. Schoenbaum EE, Hartel D, Selwyn PA, et al.: Risk factors for human immunodeficiency virus infection in intravenous drug users. N Engl J Med 1989, 321:874-879.
6. Watters JK: Historical perspective on the use of bleach in HIV/ AIDS prevention. J Acquir Immun Defic Syndr 1994, 7:743-747.
7. Haverkos HW, Jones ST: HIV, drug-use paraphernalia, and bleach. J Acquir Immune Defic Syndr 1994, 7:741-742.
8. Normand J, Vlahov D, Moses L (eds): Preventing HIV Transmission. The Role of Sterile Needles and Bleach. Washington: National Research Council, IOM National Academic Press; 1995.
9. Kaplan EH: Probability models of needle exchange. Operations Res 1995, 43:558-569.
10. US Public Health Service: HIV Prevention Bulletin: Medical Advice For Persons Who Inject Illicit Drugs. Atlanta: US Public Health Service; 1997.
11. Lurie P, Reingold AL, Bowser B, et al.: The Public Health Impact of Needle Exchange Programs in the United States and Abroad. San Francisco: University of California; 1993.
12. Watters JK, Estilo MJ, Clark GL, Lorvick J: Syringe and needle exchange as HIV/AIDS prevention for injection drug users. JAMA 1994, 271:115-120.
13. Hunter GM, Donoghoe MC, Stimson GV, Rhodes T, Chalmers CP: Changes in the injecting risk behaviour of injecting drug users in London, 1990-1993. AIDS 1995, 9:493-501.
14. Peak A, Rana S, Maharjan SH, Jolley D, Crofts N: Declining risk for HIV among injecting drug users in Kathmandu, Nepal: the impact of a harm-reduction programme. AIDS 1995, 9:10671070.
15. Des Jarlais DC, Friedman SR, Sotheran JL, et al.: Continuity and change within an HIV epidemic: injecting drug users in New York City, 1984 through 1992. )AMA 1994, 271:121-127.
16. Fennema JSA, Wiessing LG, Coutinho RA, van den Hoek A, Houweling H, van Ameijden EJC: Trends in injection drug use in a city with harm reduction. In: HIV infection among drugusers and the potential for heterosexual spread. Edited by Fennema H. Wageningen: Ponsen and Looijen BV; 1997:51-62.
17. Hagan H, Des Jarlais DC, Friedman SR, Purchase D: Risk for human immunodeficiency virus and hepatitis B virus in users of the Tacoma syringe exchange program. In: Proceedings: Workshop on Needle Exchange and Bleach Distribution Programs. Washington: National Academy Press; 1994:24-34.
18. Paone D, Des Jarlais DC, Caloir 5, Freedman P, Ness 1, Friedman SR: New York City syringe exchange: an overview. In: Proceedings: Workshop on Needle Exchange and Bleach Distribution Programs. National Academy Press, Washington, 1994:47-63.
19. Oliver K, Maynard H, Friedman SR, Des Jarlais DC: Behavioral and community impact of the Portland syringe exchange program. in: Proceedings:' Workshop on Needle Exchange and Bleach Distribution Programs. National Academy Press, Washington, 1994:35-46.
20. Schoenbaum EE, Hartel DM, Gourevitch MN: Needle exchange use among a cohort of injecting drug users. AIDS 1996,10:17291734.
21. Vlahov D, Junge B, Brookmeyer R: Reductions in high-risk drug use behaviours among participants in the Baltimore needle exchange program. J Acquir Immune Defic Syndr Hum Retrovir 1997, 16:400-406.
22. Hankins C, Gendron S, Bruneau 1, Roy E: Evaluating Montreal's needle exchange CACTUS-Montreal. In: Proceedings:
23. van Ameijden EJC, van den Hoek JAR, Coutinho RA: Injecting risk behavior among drug users in
Amsterdam., 1986 to 1992, and its relationship to AIDS prevention programs. Am J Public Health 1994, 84:275-281
24. Frischer M, Elliot L: Discriminating needle exchange attenders from non-attenders. Addiction 1993, 88:681-687.
25. Keene J, Stimson GV, Jones S, Parry-Langdon N: Evaluation of syringe-exchange for HIV prevention among injecting drug users in rural and urban areas of Wales. Addiction 1993, 88:10631070.
26 Hahn JA, Vranizan KM, Moss AR: Who uses needle exchange? A study of injection drug users in treatment in San Francisco, 1989-90. J Acquir Immune Defic Syndr Hum Retrovir 1997, 15:157164.
27. Hagan H, Des Jarlais DC, Friedman SR, Purchase D, Alter MJ: Reduced risk of hepatitis B and hepatitis C among injection drug users in the Tacoma syringe exchange program. Am J Public Health 1995, 85:1531-1537.
28. Des Jarlais DC, Hagan H, Friedman SR, et al.: Maintaining low HIV seroprevalence in populations of injecting drug users. JAMA 1995, 274:1226-1231.
29. Hurley SF, Jolley DJ, Kaldor JM: Effectiveness of needle-exchange programmes for prevention of HIV infection. Lancet 1997, 349: 1797-1800.
30. Kaplan EH, Khoshnood D, Heimer R. A decline in HIV infected needles returned to New Haven's needle exchange program: client shift or needle exchange? Am J Public Health 1994, 84:1991-1994.


31. Lurie P, Drucker E: An opportunity lost: HIV infections associated with lack of a national needle-exchange programme in the USA. Lancet 1997, 349:604-608.
32. Patrick DM, Strathdee SA, Archibald CP, et al.: Determinants of HIV seroconversion in injection drug users during a period of rising prevalence in Vancouver. Int J STD AIDS 1997, 8:437445.
33. Bruneau J, Lamothe F, Franco E, et al.: High rates of HIV infection among injection drug users participating in needle exchange programs in Montreal: results of a cohort study. Am J Epidemiol 1997, 146:994-1002.
34. Des Jarlais DC, Marmor M, Paone D, et al.: HIV incidence among injecting drug users in New York City syringe-exchange programmes. Lancet 1996, 348:987-991.
35. Strathdee SA, Patrick DM, Currie SL, et al.: Needle exchange is not enough: lessons from the Vancouver injecting drug use study. AIDS 1997, 11:1`59-1`65.
36. Dolan K, Donoghoe M, Jones S, Stimson G: A cohort study of syringe exchange clients and other drug injectors in England, 1989 to 1990. London: Centre for Research on Drugs and Health Behaviour; 1991.
37. Kahn JG: Do NEPs affect rates of HIV drug and/or sex risk behaviors? In: The public health impact of needle exchange programs in the United States and abroad. Edited by Lurie P, Reingold AL, Bowser B, et al. San Francisco: University of California; 1993:403-427.
38. Klee H, Morris J: The role of needle exchange in modifying sharing behaviour: cross-study comparisons 1989-1993. Addiction 1995, 990:1635-1645.
39. Bruneau J, Franco E, Lamothe F: Assessing harm reduction strategies: the dilemma of observational studies. Am J Epidemiol 1997, 146:1007-1010.
40. Lurie P: Le mystere de Montreal. Am J Epidemiol 1997, 146: 1003-1006.
41. Lurie P, Jones TS, Foley J: A sterile syringe for every drug user injection: how many injections take place annually and how might pharmacists contribute to syringe distribution? J Acquir Immune Defic Syndr Hum Retrovir 1998, in press.
42. Gostin LO, Lazzarini Z, Jones TS, Flaherty K: Prevention of HIV/ AIDS and other blood-borne diseases among injection drug users: a national survey on the regulation of syringes and needles. JAMA 1997, 277:53-62.
43. Valleroy LA, Weinstein B, Jones TS, Groseclose SL, Rolfs RT, Kassler WJ: Impact of increased legal access to needles and syringes on community pharmacies' needle and syringe sales- Connecticut, 1992-1993. J Acquir Immune Defic Syndr Hum Retrovir 1995, 10:73-81.
44. Groseclose SL, Weinstein B, Jones TS, Valleroy LA, Fehrs L), Kassler WJ: Impact of increased legal access to needles and syringes on practices of injecting-drug users and police officers Connecticut, 1992-1993. J Acquir Immune Defic Syndr Hum Retrovir 1995, 10:82-89.
45. Ward J, Mattick R, Hall W: Key Issues In Methadone Treatment. Randwick, Australia: University of NSW Press; 1992.
46. Dole VP, Nyswander M: Methadone maintenance treatment: a ten-year perspective. ]AMA 1976, 235:80-84.
47. Drucker E: From morphine to methadone. In: Harm Reduction: Policy and Practice. Edited by Inciardi J, Harrison L. Thousand Oaks, CA: Sage; 1998:in press.
48. Moss AR, Vranizan K, Gorter R, Bacchetti P, Watters J, Osmond D: HIV seroconversion in intravenous drug users in San Francisco, 1985-1990. AIDS 1994, 8:223-231.
49. Novick DM, Joseph H, Croxson TS, et al.: Absence of antibody to human immunodeficiency virus in long-term, socially rehabilitated methadone maintenance patients. Arch Intern Med 1990, 150:97-99.
50. Vanichseni S, Wongsuwan B, Choopanya K, Wongpanich K: A controlled trial of methadone maintenance in a population of intravenous drug users in Bangkok: implications for prevention of HIV lnt J Addictions 1991, 26:1313-1320.
51. Ball JC, Lange WR, Myers CP, Friedman SR: Reducing the risk of AIDS through methadone maintenance treatment. J Health Soc Behav 1988, 29:214-226.
52. Metzger DS, Woody GE, McLellan AT, et al.: Human immunodeficiency virus seroconversion among intravenous drug users in- and out-of-treatment: an 18-month prospective follow-up. J Acquir Immun Defic Syndr 1993, 6:1049-1056.
53. Stark K, Muller R: HIV prevalence and risk behaviour in injecting drug users in Berlin. Foren Sci Int 1993, 62:73-81.
54. Marmor M, Des Jarlais DC, Cohen H, et al.: Risk factors for infection with human immunodeficiency virus among intravenous drug abusers in New York City. AIDS 1987, 1:39-44.
55. Chaisson RE, Bacchetti P, Osmond D, Brodie B, Sande MA, Moss AR: Cocaine use and HIV infection in intravenous drug users in San Francisco. ]AMA 1989, 261:561-565.
56. Brown LS Jr, Chu A, Nemoto T, Ajuluchukwu D, Primm BJ: Human immunodeficiency virus infection in a cohort of intravenous drug users in New York City. Demographic, behavioral, and clinical features. NY State J Med 1989, 89:506-510.
57. Williams AB, McNelly EA, Williams AE, D'Aquila RT: Methadone maintenance treatment and HIV type 1 seroconversion among injecting drug users. AIDS Care 1992, 4:35-41.
58. Selwyn PA, Feiner C, Cox CP, Lipshutz C, Cohen RL: Knowledge about AIDS and high-risk behavior among intravenous drug users in New York City. AIDS 1987, 1:247-254.
59. Serpelloni G, Carried MP, Rezza G, Morganti S, Gomma M, Binkin N: Methadone treatment as a determinant of HIV risk reduction among injecting drug users: a nested case-control study. AIDS Care 1994, 6:215-220.

60. Hubbard RL, Marsden ME, Rachal JV, Harwood HJ, Cavanaugh ER, Ginzberg HM: Drug Abuse Treatment: A National Study of Effectiveness. Chapel Hill, NC: University of North Carolina Press; 1989.
61. Gerstein DR, Hendrick HJ: Treating Drug Problems. Vol. 1. Washington: National Academy Press; 1990.
62. Ball JC, Ross A: The Effectiveness of Methadone Maintenance Treatment: Patients, Programs, Services and Outcome. New York: Springer-Verlag; 1991.
63. Gunne L-M, Gronbladh L: The Swedish methadone maintenance program: a controlled study. Drug Alcohol Dependence 1981, 24:31-37.
64. Blix O, Gronbladh L: AIDS and IV heroin addicts: the preventive effect of methadone in Sweden. 4th international Conference on AIDS. Stockholm, 1988.
65. Hall W: Australia's Methadone Program. Randwick, Australia: National Drug and Alcohol Research Center ARC; 1997.
66. Dolan K, Wodak A, Hall W, Gaughwin M, Rae F: HIV risk behaviour before during and after imprisonment in New South Wales Addiction Res 1997, 4:151-160.
67. Herman M, Gourevitch MN: Integrating primary care and methadone maintenance treatment: Implementation issues. ] Addict Dis 1997, 16:91-102.
68 General Accounting Office: Methadone Maintenance: Some Treatment Programs Are Not Effective; Greater Federal Oversight Needed. Washington: US General Accounting Office; 1990 (GAO/HRD-90-1041.
69. D'Aunno T, Vaughn TE: Variations in methadone practice. /AMA 1992, 267:253-258.
70. Abdul-Quader AS, Friedman SR, Des Jarlais D, Marmor MM, Maslansky R, Bartelme S: Methadone maintenance and behaviour bv intravenous drug users that can transmit HIV. Contemporary Drug Problems 1987, 14:425-434.
71. Yancovitz SR, Des Jarlais DC, Peyser NP, et al.: A randomized trial of an interim methadone maintenance clinic. Am J Public Health 1991, 81:1185-1191.
72. Buning E, van Brussel GHA, van Santen GW: The 'Methadone by Bus' Project in Amsterdam. Br J Addictions 1990, 85:12471250.
73. Anglin MD, McGlothin WH: Outcome of narcotic addict treatment in California. In: Drug Abuse Treatment Evaluation: Strategies, Progress and Prospects. Edited by Timms FM, Ludford JP. Maryland: National Institute on Drug Abuse; 1984 INIDA Research Monograph, 511.
74. Hubbard RL, Rachal JV, Craddock SG, Cavanaugh ER, Treatment Outcome Prospective Study (TOPS): Client characteristics and behaviours before, during and after treatment. In: Drug Abuse Treatment Evaluation: Strategies, Progress and Prospects. Edited by Timms FM, Ludford JP. Maryland: National Institute on Drug Abuse; 1984 INIDA Research Monograph, 51].
75 Hartel DM Schoenbaum EE et al : Patterns of
76. Dolan K, Wodak A: An international review of methadone in prisons. Addiction Res 1996, 4:85-97.
77. Wale S, Gorta A: Pre-Release Methadone Program. Sydney: NSW Department of Corrective Services; 1987 [Research Publication No. 11.
78. Gorta A: Monitoring The NSW Methadone Program 1986-1997. Sydney: NSW Department of Corrective Services; 1987 [Research Publication No. 2].
79. Klee H, Faugier J, Hayes C, Boulton T, Morris J: AIDS-related risk behaviour, polydrug use and temazepam. Br J Addiction 1990, 85:1125-1132.
80. Hall W, Ward J, Mattick RE: Methadone maintenance in prisons: the NSW experience. Drug Alcohol Rev 1993, 12:193-203. 81. Donoghoe MC: Sex, HIV and injecting drug users. Br J Addict 1992, 87:405-416.
82. Van den HoekA, van Haastrecht HJ, Coutinho RA: Heterosexual behavior of intravenous drug users in Amsterdam: implications for the AIDS epidemic. AIDS 1990, 4:449-453.
83. Hartgers C, van den HoekA, Krijnen P, Coutinho RA: HIV prevalence and risk behaviors among injecting drug users who participate in' low-threshold' methadone programs in Amsterdam. Am J Public Health 1992, 82:547-551.
84. Joseph H: The criminal justice system and opiate addiction: a historical perspective. In: Compulsory Treatment of Drug Abuse: Research and Clinical Practice. Edited by Leukefeld CG, Tims FM. Maryland: National Institute on Drug Abuse; 1984:106-125 INIDA research monograph 861.
85. Newman RG, Whitehill WB:Double-blind comparison of methadone and placebo maintenance treatments of narcotic addicts in Hong Kong. Lancet 1979,ii:485-488.
86. Strang J, Farrell M (eds): Heroin Addiction and Drug Policy. Oxford; 1994.
87. Reisinger M, Picard E: Methadone in Belgium: physicians gaining therapeutic freedom. Addiction Res 1996, 3:369-371.
88. Carpentier J: La Toxicomanie a L'Heroine en Medecine Generale. Paris: Ellipses; 1994.
89. Wodak A: HIV infection and IDU in Australia: responding to a crisis. J Drug Issues 1992, 22:549-562.
90. Stimson G: AIDS and IDU in the UK. 1988-1993. The policy response and prevention of the epidemic. 1995.
91 Introduction of Methadone into a therapeutic Community in Leicester UK, 1997.
92. Farrell M: Methadone in the European Community. Brussels: EU; 1996.
93. Parrino MW (ed): State Methadone Treatment Guidelines. Center for Substance Abuse Treatment, Substance Abuse and Mental Health Administration. Rockville: US Public Health Service; 1993 (publication SMA 93-1991].
94. Grund JP: Harm reduction and Methadone Treatment in Eastern Europe. Open Society Institute; 1997
95. Exclusion: Report on Tri Ville Paris Conference, 1992. In: Les Temps Modernes, No. 567; 1993

96. Rosenbaum M, Murphy S, Beck ): Money for methadone. 1 Psychoactive Drugs 1987, 19:13-19.
97. Uchtenhagen A, Gutzwiller F, Dohler-Mikola A (eds): Program For Medical Prescription of Narcotics. Interim Report. Zurich: University of Zurich; 1996.
98. Nadelmann E, McNeely I. Drucker E: Harm reduction: an international perspective. In: Substance Abuse: A comprehensive Textbook. Edited by Lowinson IH, Ruiz P. Millman RB. Langrod ). New York: Wiley; 1997.
99. O'Hare P, Matthews A, Buning E, Drucker E (eds): The Reduction of Drug Related Harm. London: Routledge; 1994.
100. Heather N, Wodak A, Nadelmann E. O'Hare I' (eds): Harm Reduction: From Faith to Science. London: Whurr; 1996.
101. Erickson PG, Riley D, Cheung E (eds): Harm Reduction: A New Direction For Drug; Policy and Programs. Toronto: University of Toronto: 1997.
102. Nadelmann E: Common Sense Drug Policies. Foreign Affairs; 1998.
103. Mauer M: Report on Drug Incarcerations in the US. Washington: The Sentencing Project; 1996.
104. Lurie P, Hintzen P, Lowe RA: Socioeconomic obstacles to HIV prevention and treatment in developing countries: the roles of the International Monetary Fund and the World Bank. AIDS 1995, 9:539-546.
105.. Drucker E: Epidemic in the war zone: AIDS and community survival in New York City. Int I Health Services 1990. 20:601615.