measuring effects in the nordic context · measuring effects in the nordic context: transferability...
TRANSCRIPT

Measuring effects in the Nordic context:
Transferability of international programmes and the importance of local evaluation
Knut Sundell
Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU)
Photograph by The Sydney Justice & Police Museum

Implications
• We need to evaluate the effects of interventions
• We can evaluate with rigorous designs
• Culture/context probably moderate effects
• A well designed trial always teach us something
• Effectiveness is necessary – but not enough
Photograph by The Sydney Justice & Police Museum

Safe
Accessible
Effective
Cost
efficient
Acceptable
Equal
Quality

Photograph by The Sydney Justice & Police Museum
Safe ?

18 Motivating interview
18 ART
8 Repulse
3 12-stegsbehandling
3 Family therapy (ospecified)
2 Dialektisk beteendeterapi
2 Kriminalitet som livsval
2 Marte meo
1 TEACCH (Treatment of Education of Autistic and related communiction-handicapped Children)
1 Tejping
<1 Active parenting
Akupunktur
Antroposofisk behandling
Avslappning
Bekymringssamtal
Bildanalys
Bildterapi
CAP (Children Are People Too)
COPE (Community Parent Education program)
Community Reinforcement Training
Depression in swedish adolescents (DISA)
EMDR (Eye Movement Desensitisation and Reprocessing)
Funktionell familjeterapi
Gestaltterapi
Haschavvänjningsprogram
Hästterapi
Vägledande samtal
Komet
Lekterapi
Livsbok
Läkepedagogik
Lösninginriktad pedagogik
Massage
Mindfulness
Multisystemisk Miljöterapi
Parenting Young Children
Problembaserad skolutveckling
PMTO (Parent Management Training)
Psykodrama
Robo-memo
Rollspel
Trappan
Traumabehandling
Transaktionsanalys
Trestegsmodell
Youth at risk program (YAR)
Interventions in 250 institutions for children and youth (%)
Arbetssätt på HVB för barn och unga (Knut Sundell och Malin Hultman, Inspektionen för vård och omsorg, 2013-11-19)

Negative effects might be because:
• Harmful intervention (e.g., Lilienfeld, 2007)
• Ineffectiv intervention (e.g., psychodynamic therapy for treatment of autism)
• Malpractice – the intervention is not used appropriately (e.g., poor fidelity, low competence)
• Contraindikation – the interventions was used for the wrong population (Lowenkamp & Latessa, 2006)
Can talk harm?
Lilienfeld, S. O. (2007). Psychological treatments that cause harm. Perspectives on psychological science, 2, 53-70.
Michael Linden (2012). How to Define, Find and Classify Side Effects in Psychotherapy: From Unwanted Events to Adverse
Treatment Reactions. Clinical Psychology and Psychotherapy. DOI: 10.1002/cpp.1765
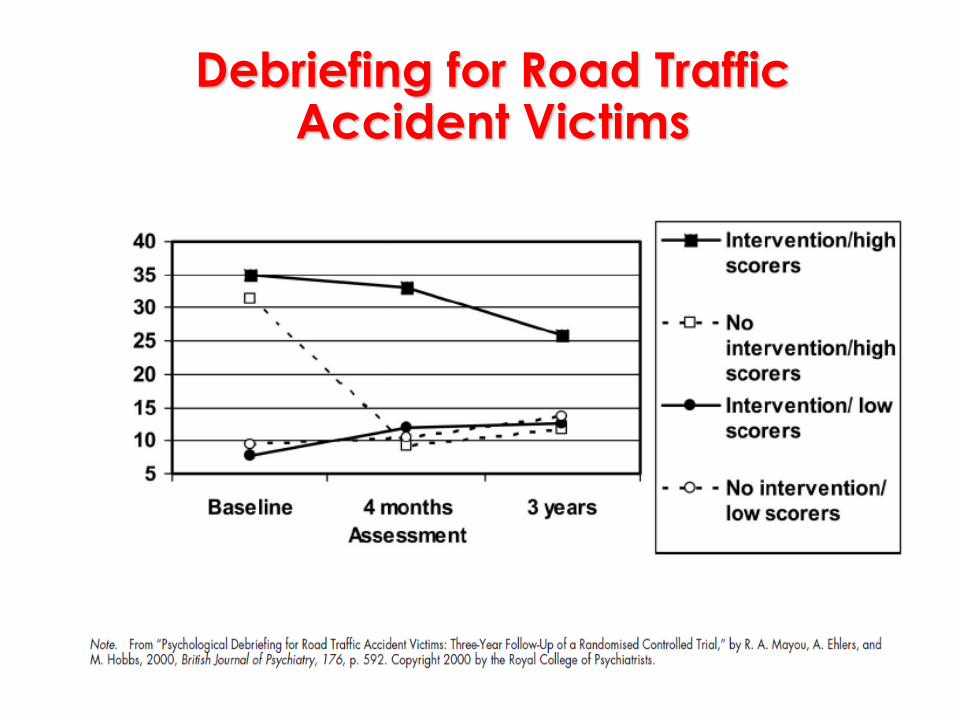
Debriefing for Road Traffic Accident Victims

Swedish research
Internet-based CBT for social anxiety (Boettcher et al, 2014)
• 14 % reported of unwanted effects (new symptoms, increased anxiety, et cetera)
• 7 % had enhanced problems between pre and post measurement
”Open survey” (Rozenthal & Carlbring, in prep)
• During one month 464 individuals could reported negative effects of psychoterapy (e.g., ”I became more anxious”; ”I didn’t understand the treatment”; ”My expectations was not met”)
• Longer therapies was associated with more negative effects

-40 -20 0 20 40 60 80
The Effectiveness of Correctional Rehabilitation: A Review of Systematic Reviews (Lipsey & Cullen, 2007)
Behavioral treatment (risk & needs) ……….. Family and parenting ……..……….………… Multidimensional treatment foster care …..
Interpersonal skills ………………………………
Individual counseling .…………………………
Victim-offender mediation .…….……………
Life skills ………...…………………………………
Multisystemic therapy …………………………
Aggression Replacement Training …….……
Victim-offender mediation ……..……………
Challenge programs ………………..…………
Milieu therapy ……………………..……………
Community supervision …….…………………
Group counseling .………………..……………
Psychodynamic therapy …..…………………
Vocational and employment programs …..
Boot camps ……………………….……….
Incarcaration, prison ….……………….
Scared straight …………………
Change in
recidivism %
Decreased risk Increased risk

Photograph by The Sydney Justice & Police Museum
The Swedish
MST-trial

The Swedish Trial
Started in 2004
MST vs Treatment-As-Usual (50/50)
Randomized controlled trial
27 local authorities / 6 MST-teams
Low attrition = 6 % (24 months)
Intention-to-treat (randomization intact)
Explicit inclusion criteria (Conduct Disorder)
Multiagent / multimethod assessment
Study of ”real life” (effectiveness)
No financial or other interests in MST

Participants
Conduct disordered youth
12 – 17 years
Exclusion criteria:
No motivated guardian
Sexual offending
Autism, acute psychosis, risk of suicide
The presence of the youth in the home posed a serious risk to the youth or to the
family

MST
Treatment As Usual
Pre- measure
7 month
follow-up
24 month
follow-up 60 month
follow-up
Rando-
misation Recruit-
ment
168 156
(93%)
149
(96%)
147
(94%)
155
(99%)

Child Behavior Checklist / Youth Self-Report (Achenbach,
1991a; 1991b)
Sense of Coherence (Antonovsky, 1987)
Self-Report Delinquency Scale (Elliott et al., 1983)
Alcohol Use Disorder Identification Test (Babor et al., 1992)
Drug Use Disorder Identification Test (Berman et al., 2005)
Pittsburgh Youth Study (Keenan et al., 995)
Social Competence with Peers Questionnaire (Spence,
1995)
Social Skills Ratings System (Gresham & Elliott, 1990)
Symptoms Checklist-90 (Derogatis & Cleary, 1997)
Parenting skills (Stattin,2004)
School attendance
Social services (case file review)
Police reports
Measures

0
20
40
60
80
0 7 24
MST
Trad
0
20
40
60
80
0 7 24
Self-reported
(YSR)
Parent
(CBCL)
Mental Health Problems

Antisocial behaviors (SRD)
0
0,5
1
1,5
2
0 7 24
MST
TAU

Arrested during the last 6 months (parent reports)
0
20
40
60
80
100
0 7 24
%
MST
TAU

0
2
4
6
8
10
0 7 24
MST
TAU
0
2
4
6
8
10
0 7 24
Drugs
(Dudit score)
Alcohol
(Audit score)
Substance abuse (scores)

0
0,5
1
1,5
2
0 7 24
MST
Trad
Mothers’ mental health (SCL-90)

Days in out-of-home care (Cumulative %)
0
20
40
60
80
100
0 7 24
%
MST
TAU

Days with services (Cumulative)
0
100
200
300
400
500
600
700
0 7 24
days
MST
TAU

Multisystemic Therapy (Sweden, Canada)
PATHS (Switzerland)
Multidimensional treatment Foster Care (UK)
Triple-P (Canada, Switzerland)
Strengthening Families Program 10-14 (Sweden)
Nurse Home Visiting (Germany)
Effekt (Örebro Prevention Program) (the Netherlands)
Multisystemic Therapy (Norway, the Netherlands, UK)
PATHS (UK)
Multidimensional treatment Foster Care (Sweden)
Triple-P (Germany, Hong Kong, Japan, Switzerland, USA)
Functional Family therapy (Sweden)
Incredible Years (UK, Canada, Norway; Sweden)
International RCTs of some family interventions on the Blueprint list

Photograph by The Sydney Justice & Police Museum
Why?

Possible reasons for
contradictory results?
1. Variations in research methodology
2. Poor cultural adaptation
3. Poor treatment adherence
4. Context moderate the effects
5. Conflict of interest bias
Sundell, K., Ferrer-Wreder, L., & Fraser, M. W. (2013). Going Global: A Model for Evaluating Empirically-Supported Family-Based Interventions in New Contexts. Evaluation & the Health Professions. Published online before print January 4, 2013, doi: 10.1177/0163278712469813

1 - Research methodology
Non-randomized trials produce lager d’s (e.g., Kunz et al., 2008)
Efficacy trials produce lager d’s (e.g., Curtis, et al., 2004; Emshoff, 2008;)
Passive control group produce lager d’s (e.g., Magill & Ray, 2009; Baldwin, et al., 2012)
“Treatment of the treated” approach to attrition produce lager d’s (e.g., Kunz, Vist & Oxman, 2008)
Shorter follow-up time, tighter inclusion criteria & measures on delinquency and substance abuse measures produce lager d’s

1 - Research methodology
A review of 13 MST RCTs (Andrée Löfholm et al., 2013)
• No two studies used the same research methodology
• The TAU condition included a wide variety of treatment alternatives
• A significant heterogeneity in effect sizes (83% of the variation was attributable to heterogeneity between studies)
A review of 24 RCTs of MST, FFT, BSFT, MFT (Baldwin et al., 2012)
• A significant heterogeneity in effect sizes
• Significant effects vs. TAU d = .21
vs. alternative treatment d =.26
vs. no active interventions d = .70

Interventions in the control group (n = 77)
17 Family therapy
14 Counseling youth
6 Counseling parent
12 Mentor
4 Institution care
6 Foster care
4 Substance abuse treatment
3 Aggression Replacement Training
2 Unspecified support youth
1 Structured open care treatment
1 Special education
7 Nothing

2 - Poor cultural adaptation
Distinction deep vs. surface structure (Resnicow et al., 2000)
• Deep structure – causal model, “theory of change”, mediators, risk factors
• Surface structure –make an EBI in tune with culturally linked aspects of participants’ life experience (e.g., program materials)
The issue is not weather to adapt a program or not – it is how to control the adaptation taking place (Resnicow et al., 2000)
Few program developers specify the core components of the intervention

3 - Poor treatment adherence
Data from the MST Institute
March 2003 to August 2009
2 948 TAMs / 973 families (87%) from 68 therapists in 10 teams
19 TAM items + post treatment youth outcomes as reported to MST Institute
Multilevel structural equation modeling
Andrée Löfholm, C., Eichas, K., & Sundell, K. (2014). The Swedish implementation of Multisystemic therapy for adolescents: does treatment
experience predict treatment adherence? Journal of Clinical Child & Adolescent Psychology. Published online before print March 20, 2014,
http://dx.doi.org/10.1080/15374416.2014.883926

70
75
80
85
90
95
1 2 3 4 5 6
2003 (7 team)
2005-6 (3 team)
TAM
Years
Treatment fidelity MST
Andrée Löfholm, C., Eichas, K., & Sundell, K. (2014). The Swedish implementation of Multisystemic therapy for adolescents: does treatment experience predict treatment adherence? Journal of Clinical Child & Adolescent Psychology, 43, 643-655.

87%
91%
94% 95%
60%
70%
80%
90%
100%
65 75 85 95
Po
st-T
rea
tme
nt
TAM
Living at Home
71%
76%
80%
84%
60%
70%
80%
90%
100%
65 75 85 95
Po
st-T
rea
tme
nt
TAM
In School or Work
26%
22%
19%
16%
0%
10%
20%
30%
40%
65 75 85 95
Po
st-T
rea
tme
nt
TAM
New Arrests-Male
13%
11% 9%
7%
0%
10%
20%
30%
40%
65 75 85 95
Po
st-T
rea
tme
nt
TAM
New Arrests-Female

Aggression Replacement Training in Sweden (Catrine Kaunitz och Anna Strandberg, 2009)
According to the manual:
– 3 modules: social skills, anger control, moral reasoning
– 3 lessons x 10 weeks (at least 20 lessons)
– Roll play, reinforcement and homework
Prevalence study 2006 + 2012
Repeated study of random sample of local authorities (N=102)

Aggression replacement Training (Kaunitz & Strandberg, 2009; Kaunitz in prep)
65%
88%
58%
25% 22%
50% 89%
39% 13% 9%
0
20
40
60
80
100
ART Role
play
etc
3
moduls
20+
lessons
All 3 ART Role
play
etc
3
moduls
20+
lessons
All 3
2006 2012
Kaunitz, C.& Strandberg, A. (2009). Aggression Replacement Training (ART) i Sverige- evidensbaserad socialtjänst i praktiken. Socionomens forskningssupplement, 26, 36-52. Kaunitz (in prep).

4 - Context moderates the effects
Context can be conceptualized in a variety of ways (e.g., Sussman et al., 2008)
The exact effects of cultural differences is widely acknowledged and poorly understood
Possible examples: • Prevalence of various risk factors (e.g., drug use, powerty)
• National policies on social services

Mental health (CBCL) change T-scores in
evaluations of MST (6-12 month follow-up)
0
4
8
12
Sundell et al
(2008)
Ogden &
Halliday-
Boykins
(2004)
Henggeler et
al (2006)
Henggeler et
al (2006) -
cont man
Rowland et al
(2005) -
external
Rowland et al
(2005) -
internal
MST TAU

Cannabis use (life-time)
males aged 15 (ter Bogt et al, 2006)
0
10
20
30
40
50
60
70
80
%
Cannabis use (life-time)
females aged 15 (ter Bogt et al, 2006)
0
10
20
30
40
50
60
70
80
%
Risk factors for cannabis use (von Sydow et al, 2002)
Availability of drugs
Peers’ drug use

5 - Conflict of Interest Bias
Conflict of interest is a threat to the validity of findings in evaluation research
The problem has increased because of a growth in international prevention firms
The label “evidence-based” is a major sales factor (but not protected)
This undermines the goal of providing policy-makers with the best evidence of what works
Eisner, M. (2009). No effects in independent prevention Trials: Can we reject the cynical view. Journal of Experimental Criminology, 5(2).

Advert or Research?

Advert or Research?

A Flourishing Prevention Industry
Triple P:
– Sold in 24 countries.
– 62,000 providers trained
USD 2000/provider training > 120 Mio (estimate)
– 6 million parent training courses sold
USD 250/parent training seminar > 1 500 Mio (estimate)
http://www.brighton-hove.gov.uk/downloads/bhcc/children/Matt_Sanders_Presentation.pdf

Effect Size by Financial COI Result
The findings suggest a small
nonsignificant effect for studies
without financial COI and a
large significant effect for
studies with financial COI
Eisner, M. P., & Humphreys, D. (2012). Measuring conflict of Interest in prevention and intervention research: A feasibility sudy. In T. Bliesener, A. Beelmann & M. Stemmler (Eds.), Antisocial behavior and crime: Contributions of developmental and evaluation research to prevention and intervention (pp. 165-180). Cambridge: Hogrefe.

Photograph by The Sydney Justice & Police Museum
Are interventions transportable?

• 4 interventions for reducing behavioural problems in children aged 3-10 (Incredible Years; Parent-Child Interaction Therapy; PMTO, Triple P)
• 14 RCTs + 3 non-randomised transported trials
• Tested in 10 countries in 5 regions
• Cohen’s d = .71 (comparable to those in the origin country)
• No association effect size x implementation factors, country-level policy or resource factors
• Stronger effect sizes in countries with more traditional values about family life and childrearing (Hong Kong, Costa Rica and Iran).
Gardner, F., Montgomery. P., & Knerr, E´W. (2015). Transporting Evidence-Based Parenting Programs for Child Problem Behavior (Age 3–10) Between Countries: Systematic Review
and Meta-Analysis. Journal of Clinical Child & Adolescent Psychology. DOI:10.1080/15374416.2015.1015134


• RCT: 4 interventions for reducing behavioural problems in children aged 3-12 (Incredible years, Cope, Connect,
Komet) vs. book on parent training / waiting list)
• 6 regions and 908 children (95% retrieved at 4 months)
• Self-referral
• Self-reporting (Eyeberg, SNAP-IV, PSOC, ARC, CGSQ, CES-D...)
• Acceptable fidelity
• All interventions were effective compared to the waiting list
Stattin, H., Enebrink, P., Özdemir, M., & Giannotta , F. (2015). A National Evaluation of Parenting Programs in Sweden: The Short-Term Effects Using an RCT Effectiveness Design. Journal of Consulting and Clinical Psychology. doi.org/10.1037/a0039328

All interventions were effective compared to the waitlist control

Photograph by The Sydney Justice & Police Museum
Effective compared to what?

116
17 25 0
25
50
75
100
125
150
175
Germany (N = 158)
96
32 11 0
25
50
75
100
125
150
175
Sweden (N = 139)
34% RCT
80% universal prevention
90% passive controls
100% child and youth
interventions
Based on the average
means of all outcomes in
the articles
89% RCT
12% universal prevention
30% passive controls
14% child and youth
interventions
Based on the primary
outcomes
Sundell, K., Beelmann, A., Hassan, H. & von Thiele Schwarz, U. (2015). Novel programs, international adoptions, or contextual adaptations? Meta-analytical results from
German and Swedish intervention research. Journal of Clinical Child & Adolescent Psychology. DOI: 10.1080/15374416.2015.1020540

Coding and analysis
Inter-coder agreement (3 broad categories) = 96.2% (German) and 92.8% (Swedish sample)
Calculation of effect sizes according to Lipsey and Wilson (2000)
Meta-analysis according to Hedges and Olkin (1985)
Because of significant heterogeneity, calculations = Random Effect Model
Controlled for study design (only RCT) and sample size (50+)

,22 ,10 ,16 ,19
0
0.25
0.5
0.75
1
Germany (N = 119)
.45
,27
,44 ,41
0
0.25
0.5
0.75
1
Sweden (N = 94)
Cohen’s d (Controlled for design and sample size)
Note – all groups were significant compared to
control

Tentative conclusion
Transported programs are
effective but should not be
implemented without
considering adaptation.

Photograph by The Sydney Justice & Police Museum
Can we trust controlled
research?

Publiced in a peer-review journal 1990-2014
Randomised or non-randomised with control group
Pre- and post measurement
Psychological or social intervention
Effects measured on client
Trends in methodological quality in Swedish controlled trials of psychological and social
interventions
Sundell, K., & Åhsberg, E. (in press). Trends in methodological quality in Swedish controlled trials of psychological and social interventions. Research on Social Work Practice

0
5
10
15
20
25
30
35
40
1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014
Trends in methodological quality in
Swedish trials (N = 302)
Sundell, K., & Åhsberg, E. (in press). Trends in methodological quality in Swedish controlled trials of psychological and social interventions. Research on Social Work Practice

140
90
25 14 11 11
5 6 0
20
40
60
80
100
120
140
160
Target area (N = 302)

0
20
40
60
80
100
90-99 00-04 05-09 10-14
Randomised (%)
0
20
40
60
80
100
90-99 00-04 05-09 10-14
Intent-to-treat (%)
0
20
40
60
80
100
90-99 00-04 05-09 10-14
Dropouts presented (%)
0
20
40
60
80
100
90-99 00-04 05-09 10-14
Significant effect (%)

4.33 6.04
6.98
9.09
0
4
8
12
16
1990-99 2000-04 2005-09 2010-14
Publication year (N=302)
Methodological quality index

Conclusions
Increased methodological quality, but still
not good-enough (single outcome trials
may be biased)
Only 51% of the interventions were effective
(reasonable theory is not enough)
RCTs was the standard – 85% (is doable and
should be used)

Implications
• We need to evaluate the effects of interventions
• We can evaluate with rigorous designs
• Culture/context probably moderate effects
• A well designed trial always teach us something
• Effectiveness is necessary – but not enough
Photograph by The Sydney Justice & Police Museum

Safe
Accessible
Effective
Cost
efficient
Acceptable
Equal
Quality