mcn audit report - · pdf filewest of scotland cancer network final – published breast...
TRANSCRIPT
West of Scotland Cancer Network Breast Cancer Managed Clinical Network
Audit Report Report of the 2011 Clinical Audit Data
Dr Ruth Adamson Consultant Pathologist MCN Clinical Lead Tom Kane MCN Manager Julie McMahon Information Officer
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 2
CONTENTS
EXECUTIVE SUMMARY 3
1. INTRODUCTION 8
2. BACKGROUND 8
2.1 NATIONAL CONTEXT 9
2.2 WEST OF SCOTLAND CONTEXT 9
3. METHODOLOGY 10
4. RESULTS AND ACTION REQUIRED 11
4.1 DATA QUALITY 11
4.2 PERFORMANCE AGAINST QIS STANDARDS 12
ACKNOWLEDGEMENT 32
ABBREVIATIONS 33
REFERENCES 34
APPENDIX I: NHS QIS STANDARDS CONSISTENTLY MET ACROSS WOS 35
APPENDIX II: RESPONDENTS 36
APPENDIX III-VI: NHS BOARD ACTION PLANS 37

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 3
Executive Summary
Introduction This report presents an assessment of performance of West of Scotland (WoS) Breast Cancer Services measured against NHS Quality Improvement Scotland (QIS) Clinical Standards for the management of breast cancer, using clinical audit data from the period January – December 2011. Where available, 2011 audit data has been presented alongside data from 2009 and 2010 to allow year-on-year comparison. During this period 2277 new cases of breast cancer were recorded within the WoS. The Managed Clinical Network (MCN) for breast cancer continues to support and develop the clinical service for these patients and at present there are eight breast clinics held across the region. The Network continues to benefit from enthusiastic engagement of a range of healthcare professionals across the WoS. Background Breast cancer is the most common cancer in women in Scotland with approximately 4500 new cases diagnosed annually. The incidence rate of breast cancer continues to rise with a 12% increase over the last decade. Breast cancer in men is very rare, accounting for less than 1% of all cancers in Scotland(1). In spite of the increase in incidence of breast cancer, mortality rates from breast cancer have decreased by over 19% over the last 10 years. Significant improvements have been achieved in long term survival with around 85% of women surviving 5 years based upon current Information Services Division (ISD) data(2). West of Scotland breast cancer services are organised around e igh t Mu l t id isc ip l i nary Team (MDT) Mee t ings serving 2.4 million people in four NHS Boards – NHS Ayrshire & Arran, NHS Forth Valley, NHS Greater Glasgow and Clyde and NHS Lanarkshire. Methodology Audit of breast cancer is long established in the WoS. Audit staff in each WoS NHS Board are responsible for collecting data on patients diagnosed by their service and entering the data on the electronic Cancer Audit Support Environment (eCASE) system. The data is then extracted from eCASE and analysed centrally by the West of Scotland Cancer Network (WoSCAN) Information Team. Analysis of the 2011 data, against the pre-determined NHS Quality Improvement Scotland (QIS) Clinical Standards, was undertaken to show the performance of each NHS Board and also produce a collated report which allows for full comparison of performance and activity across the region. Data relating to patients diagnosed between 1st January and 31st December 2011 was downloaded from eCASE on 5th September 2012 and the timescales agreed took into account the patient pathway to ensure that a complete treatment record was available for each case. Results The data was analysed against 29 core NHS QIS Standards (essential x 28 and *desirable x 1) relating to service delivery and the clinical management of breast cancer. Results for regional performance against the 29 Standards for 2011 are listed below; the values represent WoS figure and the range expressed as a percentage.

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 4
Standards consistently met by all WoS units Diagnosis 8a.1 - A minimum of 85% of breast cancer patients have a non-operative diagnosis (FNA/core biopsy/large volume biopsy). ( 98.0 [96.7-100.0]% ) Surgical Management 9a.1 - A minimum of 70% of all symptomatic breast cancers are surgically treated. (83.3 [70.3- 89.8]%) 9c.1 - A minimum of 5% of mastectomy patients have immediate breast reconstruction. ( 28.5 [8.7-38.8]% ) 9d.1 - A maximum of 10% of breast cancer patients with breast conservation have final excision margins of less than 1mm. ( 0.8 [0.0-2.6]% ) 9e.1 - A minimum of 90% of breast cancer patients having surgery for invasive tumours, undergo surgical staging of the axilla. ( 98.7 [95.6-100.0]% ) 9f.1 - A minimum of 75% of breast cancer patients undergoing surgical staging of the axilla for invasive tumours less than 15mm invasive tumour size (pathological diameter) have node sampling or a sentinel lymph node biopsy (SLNB) rather than axillary clearance. (Excluding patients who have undergone neoadjuvant treatment). ( 97.8 [76.9-100.0]% ) Pathology 10a.1 - A minimum of 90% of surgically treated invasive breast cancers have the tumour grade known and reported. ( 97.9 [95.8-100.0]% ) 10a.2 - A minimum of 90% of surgically treated breast cancers have the closest margin reported in mm from invasive tumour and in situ disease, where present.(99.0 [95.8-100.0]% ) 10a.3 - A minimum of 90% of surgically treated breast cancers have the whole tumour size reported in mm including invasive tumour and in situ disease, where present. (99.8 [99.4-100.0]% ) 10b.1 - A minimum of 90% of invasive breast cancers have the oestrogen receptor (ER) status measured and reported. ( 99.9 [99.5-100.0]% ) 10b.2 - A minimum of 90% of invasive cancers have human epidermal growth factor receptor 2 (HER2) tested and reported. ( 98.8 [96.3-100.0]% ) Oncological Management 11c.1 - A minimum of 90% of invasive breast cancer patients who are ER-positive or PR-positive, receive adjuvant treatment which includes hormonal therapy or ovarian ablation. (98.0 [92.7-100.0]% ) 11d.1 - A minimum of 85% of breast cancer patients less than 50 years at diagnosis who are node-positive, receive chemotherapy as part of the initial plan of treatment. (95.4 [87.5-100.0]%) 11d.2 - A minimum of 80% of breast cancer patients less than 70 years at diagnosis who are ER/PR-negative, node-positive, receive chemotherapy as part of the initial plan of treatment. (100 [100.0]% )

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 5
11e.1 - A minimum of 70% of breast cancer patients with HER2 positive or fluorescence in situ hybridisation (FISH) positive invasive cancer greater than 10 mm or node-positive, excluding T4 or inflammatory cancers, who have received chemotherapy, receive Trastuzumab. (95.5 [90.3 - 100.]% ) Standards not met or areas where variance is evident across WoS Referral 5a.1 - A minimum of 80% of patients referred to a symptomatic breast clinic, who are diagnosed with breast cancer, are seen within 28 days from the date of GP referral. ( 88.0 [44.0-98.2]% ) 5a.2* - A minimum of 80% of patients referred to a symptomatic breast clinic, who are diagnosed with breast cancer, are seen within 14 days from the date of GP referral. ( 53.8 [4.0-76.3]% ) Waiting Times 6a.1 - A minimum of 85% of breast cancer patients have a diagnosis within 14 days of first clinic visit (including image-guided needle biopsy). ( 94.8 [83.9-97.9]% ) 7a.1 - A minimum of 80% of breast cancer patients who require surgery as their first treatment, undergo surgery within 31 days of diagnosis. ( 68.1 [56.5-81.6]% ) 7a.2 - A minimum of 80% of breast cancer patients start primary or neoadjuvant chemotherapy within 31 days of diagnosis. ( 55.1 [27.3-83.3]% ) 7a.3 - A minimum of 80% of breast cancer patients start primary or neoadjuvant hormonal therapy within 31 days of diagnosis. ( 91.4 [71.4-100.0]% ) 7a.4 - A minimum of 70% of breast cancer patients start radiotherapy (adjuvant) within 42 days of final therapeutic operation/chemotherapy dose. ( 21.9 [14.9-35.7]% ) 7a.5 - A minimum of 80% of breast cancer patients start chemotherapy (adjuvant) within 42 days of final therapeutic operation. ( 68.1 [56.7-88.1]% ) 7a.6 - A minimum of 80% of all breast cancer patients receive first treatment within 62 days of GP referral. ( 82.9 [52.0.1-92.3]% ) Surgical Management 9b.1 - There is a minimum of 75% conservation rate of surgically treated small cancers less than 15mm whole tumour size (pathological diameter/invasive and in situ disease). (Excluding patients with multifocal disease and patients who have undergone neoadjuvant treatment).* (90.9 [33.3-96.7]% ) 9g.1 - A maximum of 10% of breast cancer patients undergoing unguided surgical staging or blue dye only guided sampling of the axilla have less than 4 lymph nodes removed. ( 4.7 [0.0-13.0]% )
* Caution should be given to interpretation as percentages are based on small numbers for some units.

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 6
Oncological Management 11a.1 - A minimum of 85% of breast cancer patients receive radiotherapy to the breast after conservation for invasive cancer (excluding breast cancer patients taking part in trials of radiotherapy treatment). ( 94.6 [83.9 -100.0]% ) 11b.1 - A minimum of 85% of breast cancer patients receive axillary radiotherapy or axillary clearance with nodal involvement (diagnosed by ultrasound/FNA, SLNB or sample). ( 97.7 [81.6-100.0]% ) Clinical Trials 12a.1 - A minimum of 5% of newly diagnosed breast cancer patients enter into peer reviewed clinical trials as part of their initial management. ( 4.6 [1.7-16.3]% ) Conclusions and Action Required The Breast Cancer MCN are encouraged that all units met 15 of the essential NHS QIS Standards, with results presented in this report demonstrating that patients with breast cancer in the WoS continue to receive a consistent high standard of care. Nonetheless, 1 desirable and 13 essential standards were not consistently achieved across all units. Each unit was asked to complete a performance summary report and document areas for improvement where essential standards were not met. Details of the respondents for each unit are detailed in Appendix II. To date, specific comments have been received from all units with the exception of Greater Glasgow. Moving forward, there is a need to establish more effective sign off and reporting processes with NHS Greater Glasgow and Clyde, taking account of the size and complexity of the organisation. Work to achieve this has been initiated. Reasons cited for variance in performance between units included consultant vacancies, surgical capacity, radiology resource and variable quality of data. Many of these issues are being addressed and it is anticipated that the positive impact of these changes will be evident in future audit analysis. As with previous years a number of standards not met relate to waiting times for different elements of the patient pathway. Again no unit met the target of 80% in standard 5a.2 relating to patients being seen within 14 days from the date of GP referral. Six units showed improvement in performance from 2010 which is encouraging. While overall reported performance against the national waiting times is good it is important to note such variances when all patients (urgent and non urgent referrals) are included in the analysis. It was observed that in all of the units the standard for starting radiotherapy within 42 days of final operation/chemotherapy was not met and it is recognised that this reflects the existing capacity issues experienced by the Beatson West of Scotland Cancer Centre (BWoSCC). An outline business case is currently being developed for a satellite radiotherapy facility within the west of Scotland. This new facility will provide additional radiotherapy capacity, improving access to radiotherapy treatment. Action Required
NHS Boards to assess their diagnostic capacity, taking cognisance of the increase in activity as a result of the Detect Cancer Early (DCE) initiative.
NHS Ayrshire & Arran should feed back the outcome of the review of cases not meeting Standard 7a.3 to the MCN Advisory Board and assess if further action is required.
NHS Boards to review oncology appointment booking process to minimise any delay in

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 7
commencing chemotherapy.
NHS Ayrshire & Arran should feed back the outcome of the review of cases not meeting Standard 9g.1 to the MCN Advisory Board and assess if further action is required.
The MCN will actively progress regional actions identified in this report and NHS Boards are asked to develop local Action/Improvement Plans in response to the findings presented in the report. Progress against these plans will be monitored by the MCN Advisory Board and reported to the Regional Cancer Advisory Group (RCAG) annually by Board Lead Cancer Clinicians and MCN Clinical Leads, as part of the regional audit governance process to enable RCAG to review and monitor regional improvement. This process is intended to deliver incremental and sustainable improvements in the quality of patient care. A summary of actions for each NHS Board has been included within the Action Plan templates in Appendices III -VI. Completed Action Plans should be returned to WoSCAN within two months of publication of this report.

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 8
1. Introduction This report assesses performance against NHS Quality Improvement Scotland (QIS) Standards of West of Scotland (WoS) breast cancer services, using the clinical audit data relating to patients diagnosed in the region in 2011. These audit data underpin much of the regional development/service improvement work of the Managed Clinical Network (MCN) and regular reporting of activity and performance is a fundamental requirement of an MCN to assure the quality of care delivered across the region. During this period 2277 new cases of breast cancer were recorded within the WoS. The MCN for breast cancer continues to support and develop the clinical service for these patients and at present there are eight breast cancer clinics held across the region. The Network continues to benefit from enthusiastic engagement of a range of healthcare professionals across the WoS.
2. Background Breast cancer services are organised around Mu l t id isc ip l inary Team (MDT) Meet ings serving 2.4 million people in four NHS Boards – NHS Ayrshire & Arran, NHS Forth Valley, NHS Greater Glasgow and Clyde and NHS Lanarkshire. From this population, each year approximately 2300 patients are newly diagnosed with breast cancer per annum (based on Cancer Registration data). There are two main routes of presentation i.e. symptomatic referrals to breast services or via the national screening programme. During 2011 services were configured as eight local MDTs. Table 1 lists the MDTs, the constituent hospitals and also the analysis group based on location of diagnosis which has been used to present results throughout the report.
Table 1: MDT configuration across the region
MDT Constituent Hospital Analysis Group
Ayrshire Ayr Hospital Crosshouse Hospital
Ayr XH
Forth Valley Forth Valley Royal Hospital FV
Lanarkshire Hairmyres Hospital Monklands District General Hospital Wishaw General Hospital
HM ML WS
Lanarkshire Hairmyres Hospital Monklands District General Hospital
HM ML
Greater Glasgow North East
Glasgow Royal Infirmary Stobhill Hospital
N&E Glasgow
Greater Glasgow South
Southern General Hospital Victoria Infirmary
SG
Greater Glasgow West
Western Infirmary WIG/GGH
Greater Glasgow Clyde
Royal Alexandra Hospital, Inverclyde Royal Hospital and Vale of Leven
Clyde

2.1 National Context
Breast cancer is the most common cancer in women in Scotland with approximately 4500 new cases diagnosed annually. The incidence rate of breast cancer continues to rise with a 12% increase over the last decade. Breast cancer in men is very rare, accounting for less than 1% of all cancers in Scotland(1). In spite of the increase in incidence of breast cancer, mortality rates from breast cancer have decreased by over 19% over the last 10 years. Significant improvements have been achieved in long term survival with around 85% of women surviving 5 years based upon current Information Services Division (ISD) data(2). Early detection of breast cancer through a national screening programme, improvements in diagnosis and staging of breast cancer and improved treatment interventions are all key factors in survival.
2.2 West of Scotland Context
The demographic profile of the WoS population is consistent with that of the whole of Scotland. As a result age distribution (Figure1) and deprivation category (Figure 2) of breast cancer patients does not vary significantly from the national perspective. Figure 1: Age Distribution of Breast Cancer Patients
0
50
100
150
200
250
300
350
400
450
500
550
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 >85
To
tal n
um
be
r of p
ati
en
ts
Age Range
2009 2010 2011
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 9

Figure 2: Distribution of Cases by Deprivation Category
0
50
100
150
200
250
300
350
400
450
500
550
600
SIMD 1 (Most Deprived)
2 3 4 SIMD 5 (Least Deprived)
No Match
To
tal n
um
be
r of p
ati
en
ts
Deprivation Category
3. Methodology The clinical audit data presented in this report was collected by clinical audit staff in each NHS Board in accordance with an agreed dataset and definitions. The data was recorded manually and entered locally into the electronic Cancer Audit Support Environment (eCASE): a secure centralised web-based database. Data relating to patients diagnosed between 1st January and 31st December 2011 was downloaded from eCASE at 2200 hrs on 5th September 2012. Cancer audit is a dynamic process with patient data continually being revised and updated as more information becomes available. This means that apparently comparable reports for the same time period and cancer site may produce slightly different figures if extracted at different times. Analysis was performed centrally for the region by the West of Scotland Cancer Network (WoSCAN) Information Team and the timescales agreed took into account the patient pathway to ensure that a complete treatment record was available for each case. Initial results of the analysis were provided to local NHS Boards to check for inaccuracies, inconsistencies or obvious gaps and a subsequent download taken upon which final analysis was carried out. The final data analysis was disseminated for NHS Board verification in line with the regional audit governance process to ensure that the data was an accurate representation of service in each area.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 10

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 11
4. Results and Action Required
4.1 Data Quality
Case ascertainment is a measure of data quality derived from comparing the number of new patients captured by the audit with the numbers recorded by the National Cancer Registry; as a proportion of the average number accrued over the most recently available 5 year period. Cancer Registry information is available some time after the year of interest as collection and verification of data is time intensive; it is for this reason that audit data cannot be compared directly to Cancer Registry data for the same year. Table 2 illustrates case ascertainment across the WoS NHS Boards. Cancer Registry data used to calculate case ascertainment for the 2011 cohort is the average of 2006 to 2010 (extracted in November 2012). Table 2: Case Ascertainment for Breast Cancer
Health Board
n
Cancer Registry
Average*
Percentage Estimated Case Ascertainment
Ayrshire & Arran 391 371 105.4
Forth Valley 178 158 112.6
Lanarkshire 349 296 117.9
Greater Glasgow and Clyde 1359 1374 98.9
Network Region Total 2277 2200 103.5
* The number of patients diagnosed each year will naturally vary therefore some NHS Boards may report case ascertainment above 100% and others below. Case ascertainment is intended to be an indication rather than an exact measure.

4.2 Performance Against QIS Standards
For the purposes of this report, those standards that have been consistently met across the WoS are listed in Appendix I. Acknowledging the continued hard work and efforts of all involved in breast cancer services in the WoS, this report focuses on those standards where regional variance exists. It is these therefore that are illustrated and expanded to help benchmark services, regionally and nationally, and give direction for local or regional action/improvement plans. Performance results for each of the standards not achieved are presented in both graphical format and the underlying data in tabular form. Data for 2011 and the results from the previous years (2009 and 2010) are given to enable comparative reporting. The data is presented as a series of bar charts. The majority of the results are displayed as a percentage of the overall number of cases. Blue dashed lines are included on charts to show the essential target and purple dashed lines to show the desirable target. Results: A total of 2277 new diagnoses of breast cancer were recorded by the MCN in the WoS during 2011. Figure 3 shows the distribution of cases across the analysis groups within the region. Figure 3: Distribution of Breast Cancer Cases within WoS
0
50
100
150
200
250
300
350
400
450
500
550
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
HM ML WS
Tota
l nu
mb
er o
f pat
ien
ts
Analysis Group
2009 2010 2011
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 12

Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 76 85 37 269 307 354 163 167 178 268 312 352 222 215 215 387 375 393
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 403 404 399 87 119 90 113 99 99 104 95 160 2092 2178 2277
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 13
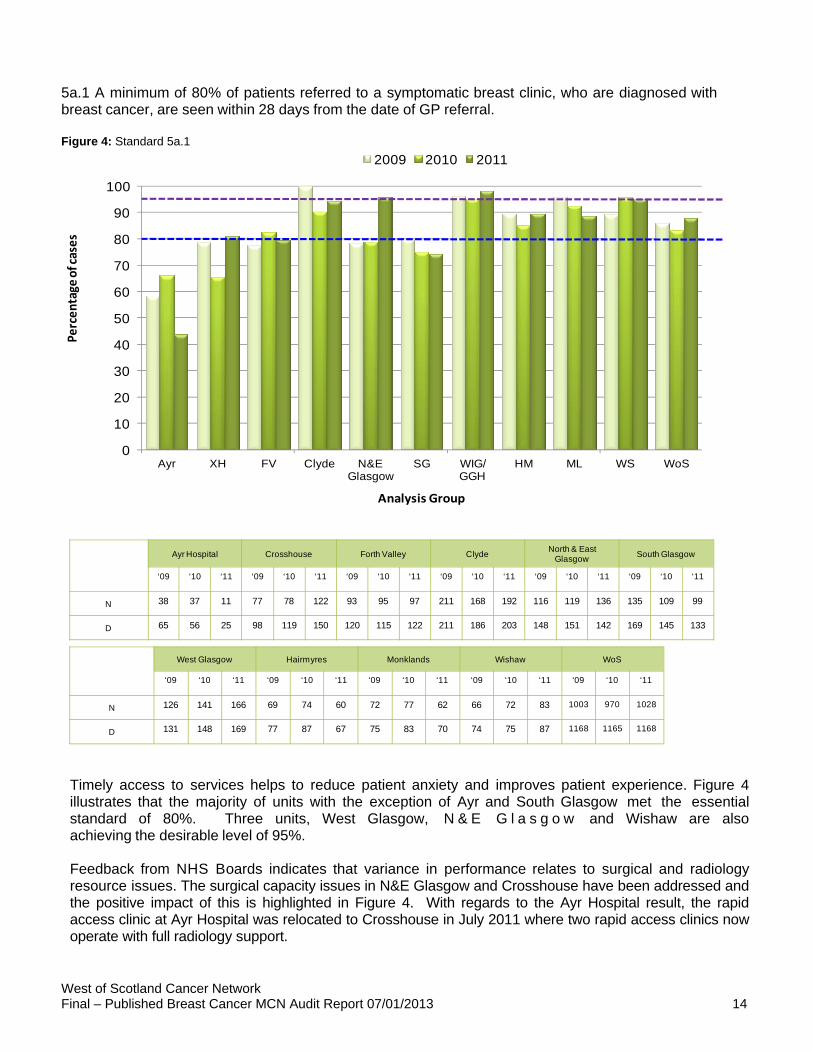
5a.1 A minimum of 80% of patients referred to a symptomatic breast clinic, who are diagnosed with breast cancer, are seen within 28 days from the date of GP referral. Figure 4: Standard 5a.1
0
10
20
30
40
50
60
70
80
90
100
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
HM ML WS WoS
Percentage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 38 37 11 77 78 122 93 95 97 211 168 192 116 119 136 135 109 99
D 65 56 25 98 119 150 120 115 122 211 186 203 148 151 142 169 145 133
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 126 141 166 69 74 60 72 77 62 66 72 83 1003 970 1028
D 131 148 169 77 87 67 75 83 70 74 75 87 1168 1165 1168
Timely access to services helps to reduce patient anxiety and improves patient experience. Figure 4 illustrates that the majority of units with the exception of Ayr and South Glasgow met the essential standard of 80%. Three units, West Glasgow, N & E G l a s g o w and Wishaw are also achieving the desirable level of 95%.
Feedback from NHS Boards indicates that variance in performance relates to surgical and radiology resource issues. The surgical capacity issues in N&E Glasgow and Crosshouse have been addressed and the positive impact of this is highlighted in Figure 4. With regards to the Ayr Hospital result, the rapid access clinic at Ayr Hospital was relocated to Crosshouse in July 2011 where two rapid access clinics now operate with full radiology support.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 14

5a.2 A minimum of 80% of patients referred to a symptomatic breast clinic, who are diagnosed with breast cancer, are seen within 14 days from the date of GP referral. Figure 5: Standard 5a.2
0
10
20
30
40
50
60
70
80
90
100
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
HM ML WS WoS
Percen
tage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 10 11 1 27 21 42 49 29 39 186 126 119 53 57 99 64 72 64
D 65 56 25 98 119 150 120 115 122 211 186 203 148 151 142 169 145 133
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 80 103 129 51 55 42 61 55 51 48 34 42 629 563 628
D 131 148 169 77 87 67 75 83 70 74 75 87 1168 1165 1168
Figure 5 above shows that no unit in the WoS met this desirable target. Three units showed a further decrease from 2010 results; however six units showed an increase in performance from 2010 to 2011. This improvement is encouraging and it is anticipated that this will continue. The implementation of the national Detect Cancer Early (DCE) initiative which aims to increase the detection of breast, colorectal and lung cancers at the first stage of disease by 25% is likely to impact further on performance against this standard. Feedback from NHS Forth Valley stated that they currently have a vacancy for a breast surgeon which has had an impact on waiting times. They have used an external breast surgeon to undertake additional clinics and a consultant is triaging all breast referrals with the aim of reducing waiting times. Action Required NHS Boards to assess their diagnostic capacity, taking cognisance of the increase in activity as a result of the DCE initiative.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 15

6a.1 A minimum of 85% of breast cancer patients have a diagnosis within 14 days of first clinic visit (including image-guided needle biopsy).
Figure 6: Standard 6a.1
0
10
20
30
40
50
60
70
80
90
100
AYR XH FV Clyde N&E Glasgow
SG WIG/GGH HM ML WS WoS
Percentage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 54 51 22 93 112 146 113 108 118 206 176 195 142 137 139 156 136 127
D 65 56 25 98 119 150 120 115 122 211 186 203 148 151 142 169 145 133
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 129 137 161 65 84 62 65 71 64 65 64 73 1088 1076 1107
D 131 148 169 77 87 67 75 83 70 74 75 87 1168 1165 1168
Figure 6 highlights that only Wishaw failed to meet the essential 85% target. Six units also met the desirable target of 95%.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 16

7a.1 A minimum of 80% of breast cancer patients who require surgery as their first treatment, undergo surgery within 31 days of diagnosis.
Figure 7: Standard 7a.1
0
10
20
30
40
50
60
70
80
90
100
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
HM ML WS WoS
Percentage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 32 30 13 154 178 218 80 70 78 171 175 181 83 81 103 196 135 132
D 44 50 23 197 227 267 108 112 122 193 211 243 164 154 155 306 295 313
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 304 258 246 40 60 32 64 46 39 55 45 85 1179 1078 1127
D 350 335 311 50 77 43 69 50 59 68 54 118 1549 1565 1654
As highlighted in Figure 7 only one unit met the essential target of 80% and no unit met the 95% desirable target. Six units show a decrease from the previous year.
On investigation it was evident that delays were the result of patient choice, unplanned periods of leave, surgeon availability, increased demand and onward referral for immediate breast reconstruction. Failure to meet the standard in Ayr Hospital may be due to a change between the retired and newly appointed surgeon. All cases will be reviewed via their clinical governance structure. Crosshouse Hospital met the essential standard of 80%. This was achieved by moving patients between surgeons and being flexible with available theatre times, though this may not be sustainable in the long term. In NHS Lanarkshire a review of operating theatre time is ongoing as part of the reconfiguration of services. In N&E Glasgow the addition of a new consultant has made a positive impact and it is anticipated that this will
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 17

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 18
continue. During 2010, the Scottish Government revised cancer waiting times targets. The new target stipulates that all patients diagnosed with cancer should commence treatment 31 days from the date of decision to treat. The National Breast Cancer dataset does not incorporate a field for ‘date of decision to treat’; therefore it is not possible to provide this result in this report. It should be noted that this pre-existing standard, the results of which are shown here, is measured from date of diagnosis which is earlier in the patient pathway than date of decision to treat.
The most current Cancer Waiting Times data demonstrates improvements during 2012 (Quarters 1-2) with the overall WoS result, and the majority of WoS NHS Boards consistently exceeding the 95% level for performance against the 31 day target from decision to treat to first cancer treatment. (4)

7a.2 A minimum of 80% of breast cancer patients start primary or neoadjuvant chemotherapy within 31 days of diagnosis. Figure 8: Standard 7a.2
0
10
20
30
40
50
60
70
80
90
100
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
HM ML WS WoS
Percen
tage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 4 14 2 19 21 10 6 7 10 11 17 23 4 8 6 7 7 7
D 6 16 3 29 23 15 7 8 12 16 33 38 11 13 9 12 13 21
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 10 9 14 8 6 3 12 12 6 8 7 5 89 108 86
D 11 13 27 12 11 11 14 14 11 8 9 9 126 153 156
Figure 8 indicates that only one unit met the essential target of 80%. Eight units also showed a decrease from the previous year’s results. This standard however pertains to small numbers where the omission of just one can have an impact on data appearance as can be seen by the Ayr Hospital result. Due to small numbers any comparison of percentages should be treated with caution. Again it should be noted that this pre-existing standard, the results of which are shown here, is measured from date of diagnosis which is earlier in the patient pathway than date of decision to treat which is used for national waiting times.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 19

7a.3 A minimum of 80% of breast cancer patients start primary or neoadjuvant hormonal therapy within 31 days of diagnosis. Figure 9: Standard 7a.3
0
10
20
30
40
50
60
70
80
90
100
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
HM ML WS WoS
Percentage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 16 13 5 27 37 47 32 35 27 39 34 47 25 26 26 42 42 39
D 19 17 7 28 38 52 34 35 31 41 38 47 33 28 30 50 45 41
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 27 17 27 11 22 23 18 23 21 22 16 15 259 265 277
D 30 20 33 13 22 24 20 23 22 22 18 16 290 284 303
Figure 9 indicates that only Ayr Hospital did not meet the essential standard of 80%. All cases failing to meet the standard will be reviewed by NHS Ayrshire & Arran breast service via their clinical governance structure. Four units Clyde, Monklands, Hairmyres and South Glasgow all met the desirable level of 95%. Action Required:
NHS Ayrshire & Arran should feed back the outcome of the review of cases not meeting Standard 7a.3 to the MCN Advisory Board and assess if further action is required.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 20

7a.4 A minimum of 70% of breast cancer patients start radiotherapy (adjuvant) within 42 days of final therapeutic operation/chemotherapy dose. Figure 10: Standard 7a.4
0
10
20
30
40
50
60
70
80
90
100
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
HM ML WS WoS
Percentage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 13 17 5 34 38 49 31 24 25 52 42 61 74 53 47 67 53 41
D 37 52 14 180 202 231 77 70 110 166 219 232 134 135 136 248 232 275
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 67 56 52 8 10 8 16 9 9 9 5 23 371 307 320
D 278 285 282 38 57 38 49 51 51 48 39 89 1255 1342 1458
As indicated by Figure 10 no units in the WoS met the essential target of 70%. Radiotherapy capacity still remains the single most critical regional issue. Significant work is ongoing to increase and maximise the use of existing radiotherapy capacity in the BWoSCC. This includes, for example, extended working days and the implementation of new technologies. Work is also underway to plan the development of a new satellite radiotherapy facility to serve the central belt population.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 21

7a.5 A minimum of 80% of breast cancer patients start chemotherapy (adjuvant) within 42 days of final therapeutic operation. Figure 11: Standard 7a.5
0
10
20
30
40
50
60
70
80
90
100
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
HM ML WS WoS
Percen
tage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 18 23 9 41 54 58 36 40 37 62 34 51 56 57 54 70 64 53
D 31 30 12 73 69 87 42 48 42 103 67 90 93 76 78 104 96 73
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 54 63 64 17 15 10 22 21 12 20 20 37 396 391 385
D 96 88 96 30 29 17 29 25 15 22 24 55 623 552 565
As demonstrated in Figure 11 only NHS Forth Valley and Monklands met the essential target of 80%. Improvement was noted in three units; however five units show a decrease on previous year’s figures.
Comments received from NHS Ayrshire & Arran stated that all patients requiring chemotherapy are now appointed to oncology clinics directly from MDT to minimise delays. A local review of case notes not meeting the standard will be carried out.†
Action Required:
NHS Boards to review oncology appointment booking process to minimise any delay in commencing chemotherapy.
† Further local review of audit data for standard 7a.5 for Crosshouse has amended the percentage to 69.04%
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 22

7a.6 A minimum of 80% of all breast cancer patients receive first treatment within 62 days of GP referral.
Figure 12: Standard 7a.6
0
10
20
30
40
50
60
70
80
90
100
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
HM ML WS WoS
Percentage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 46 37 13 85 94 127 101 94 95 204 158 181 113 103 125 138 99 88
D 68 56 25 102 119 150 119 114 121 208 184 202 154 148 141 170 144 132
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 128 130 156 65 73 54 65 69 58 61 71 65 1006 928 962
D 131 146 169 77 86 66 75 83 69 73 75 85 1177 1155 1160
Figure 12 highlights that the majority of units met the essential level of 80% of patients receiving first treatment within 62 days of GP referral. No units met the desirable level of 95%. Ayr, South Glasgow, Wishaw and Forth Valley (who just missed the 80% target) did not meet the essential target. The overall WoS result however shows a slight increase on 2010 results with 82.9% in 2011 being treated within 62 days of GP referral compared to 80.3% in 2010. Feedback from NHS Ayrshire & Arran indicates that the figures for Ayr Hospital may not reflect the current situation within the breast team and should be monitored locally for 2012.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 23

9b.1 - There is a minimum of 75% conservation rate of surgically treated small cancers less than 15mm whole tumour size (pathological diameter/invasive and in situ disease). (Excluding patients with multifocal disease and patients who have undergone neoadjuvant treatment). Figure 13: Standard 9b.1
0
10
20
30
40
50
60
70
80
90
100
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
HM ML WS WoS
Percentage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 0 3 1 65 72 90 13 16 17 23 55 55 23 27 15 93 91 118
D 4 3 3 76 86 99 16 19 19 27 59 63 30 32 22 101 96 122
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 106 105 97 2 12 9 11 4 7 2 3 9 338 388 418
D 112 111 103 3 12 11 12 5 8 5 3 10 386 426 460
As highlighted in Figure 13 all units with the exception of Ayr and N&E Glasgow met the essential target of 75%. Some results however pertain to small numbers where the omission of just one can have an impact on the numbers; therefore comparison of percentages should be treated with caution. Seven units also met the desirable standard of 85%.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 24

9g.1 A maximum of 10% of breast cancer patients undergo unguided surgical staging or blue dye only guided sampling of the axilla have less than 4 lymph nodes removed.
Figure 14: Standard 9g.1
0
2
4
6
8
10
12
14
16
18
20
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
ML HM WS WoS
Percentage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 2 3 3 2 3 4 6 4 2 1 2 0 2 0 1 1 0 2
D 50 64 23 184 176 86 92 59 43 60 55 40 63 51 33 255 78 44
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 2 1 0 5 2 0 2 2 0 3 6 8 26 23 20
D 246 117 50 45 37 20 68 30 11 70 42 79 1133 709 429
As highlighted in Figure 14 all units with the exception of Ayr met the essential target of 10% of patients having fewer than 4 nodes removed during axillary staging apart from those undergoing Sentinel Lymph Node Biopsy (SLNB).
Feedback received from NHS Ayrshire & Arran indicates that review of cases not meeting the standard will be carried out. Wishaw appear to have addressed previous resource issues and an improvement has been noted.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 25

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 26
Action Required:
NHS Ayrshire & Arran should feed back the outcome of the review of cases not meeting Standard 9g.1 to the MCN Advisory Board and assess if further action is required.

11a.1 A minimum of 85% of breast cancer patients receive radiotherapy to the breast after conservation for invasive cancer (excluding breast cancer patients taking part in trials of radiotherapy treatment).
Figure 15: Standard 11a.1
80
82
84
86
88
90
92
94
96
98
100
0 50 100 150 200
% R
ecei
vin
g P
ost
Op
Rad
ioth
erap
y
Number of Patients
Standard 11a.1
Average
2SD limits
3SD limits
Ayr
XH
Clyde
FV
ML
WS
HM
N&E Glasgow
West Glasgow
South Glasgow
Source:
QIS Standard
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 16 20 4 96 130 160 40 43 76 113 129 165 79 81 80 169 136 193
D 22 21 4 105 132 165 48 55 81 117 138 187 85 82 81 179 140 198
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 220 194 176 15 18 26 28 24 34 28 30 56 804 805 970
D 223 199 178 22 47 31 34 34 36 30 42 64 865 890 1025
Figure 15 shows the position of each NHS Board with the proportion of patients receiving radiotherapy after conservation surgery relative to the number of patients diagnosed in 2011 who received conservation surgery and demonstrates variation in the results of this standard across the region.
The broken lines represent the 95% (2 Standard Deviations) and 99.8% (3 Standard Deviations) control limits. NHS Boards that lie above the upper control limits have significantly better radiotherapy rates than the average.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 27
Nine of the units met the essential target of 85% with five of those units also achieving the desirable level

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 28
of 95%. Year on year improvement is noted in 8 units and although Hairmyres fell just short of the 85% essential target, significant improvement is noted from the previous year’s figure. ‡
‡ 2 cases from Hairmyres were recorded as having radiotherapy to the chest wall instead of to the breast. This has been amended locally and the result is now 28/31, 90.3%. One Wishaw case was also amended locally and the result is now 57/64, 89.1%.

11b.1 A minimum of 85% of breast cancer patients receive axillary radiotherapy or axillary clearance with nodal involvement (diagnosed by ultrasound/FNA, SLNB or sample). Figure 16: Standard 11b.1
0
10
20
30
40
50
60
70
80
90
100
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
ML HM WS WoS
To
tal n
um
be
r of p
ati
en
ts
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 18 28 11 53 56 62 43 43 53 82 80 75 73 72 57 79 80 67
D 19 28 11 59 56 64 52 44 53 86 80 75 74 72 57 82 81 68
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 91 78 109 24 33 20 33 27 24 24 25 40 520 522 518
D 92 81 109 36 34 20 34 28 24 26 26 49 560 530 530
Figure 16 indicates that only Wishaw failed to meet the essential target of 85%§. All other NHS boards met the desirable standard of 95%.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 29
§ 3 Wishaw cases have now been updated to reflect that they received radiotherapy to the axilla. 1 Wishaw case has been updated to being node negative (0/1 node) so should now be removed from the denominator. Results for Wishaw should now be 44/48 = 97.7%.

12a.1 A minimum of 5% of newly diagnosed breast cancer patients enter into peer reviewed clinical trials as part of their initial management.
Figure 17: Standard 12a.1
0
5
10
15
20
25
30
35
40
45
50
Ayr XH FV Clyde N&E Glasgow
SG WIG/ GGH
ML HM WS WoS
Percentage of cases
Analysis Group
2009 2010 2011
Ayr Hospital Crosshouse Forth Valley ClydeNorth & East
GlasgowSouth Glasgow
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 4 7 2 5 14 8 8 16 14 8 10 6 11 10 8 23 32 10
D 76 85 37 269 307 354 163 167 178 268 312 352 222 215 215 387 375 393
West Glasgow Hairmyres Monklands Wishaw WoS
‘09 ‘10 ‘11 ‘09 ‘10 ‘11 ’09 ‘10 ‘11 ‘09 ‘10 ‘11 ‘09 ‘10 ‘11
N 34 25 18 1 8 4 14 8 8 10 12 26 118 142 104
D 403 404 399 87 119 90 113 99 99 104 95 160 2092 2178 2277
Measurement of performance against this standard does not reflect the number of WoS breast cancer patients recruited into clinical trials after treatment has started or with metastatic disease. The availability of clinical trials for newly diagnosed patients has declined in recent years.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 30

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 31
5. Conclusions The Breast Cancer MCN are encouraged that the majority of units are achieving the NHS QIS Standards. The results presented in this report once again demonstrate that patients with breast cancer in the West of Scotland continue to receive a consistent high standard of care. We are encouraged by the progress which has been made over the last year and the network will progress the actions identified in this report in conjunction with local NHS Boards. While overall reported performance against the national waiting time target is good, notable variance in performance against QIS Standards relating to waiting times is observed when urgent and non urgent GP referrals are included in the analysis. This has highlighted a requirement for NHS Boards to assess their diagnostic capacity particularly in relation to the impact of the national DCE initiative which will feed through into 2013 and beyond. It was observed that in all of the units the standard for starting radiotherapy within 42 days of final operation/chemotherapy was not met and it is recognised that this reflects the existing capacity issues experienced by the BWoSCC. An outline business case is currently being developed for a satellite radiotherapy facility within the west of Scotland. This new facility will provide additional radiotherapy capacity, improving access to radiotherapy treatment. There are some actions required as a consequence of this assessment of performance against the agreed criteria, which relate to a continued commitment to data quality and service improvement. The MCN will actively take forward regional actions identified and NHS Boards are asked to develop local Action/Improvement Plans in response to the findings presented in the report. A summary of actions for each NHS Board has been included within the Action Plan templates in Appendices III – VI. Completed Action Plans should be returned to WoSCAN within two months of publication of this report. Progress against these plans will be monitored by the MCN Advisory Board and reported to the Regional Cancer Advisory Group (RCAG) annually by Board Lead Cancer Clinicians and MCN Clinical Leads, as part of the regional governance process to enable RCAG to review and monitor regional improvement.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 32
Acknowledgement This report has been prepared using clinical audit data provided by the following NHS Boards in the WoSCAN area: NHS Ayrshire & Arran NHS Forth Valley NHS Greater Glasgow and Clyde NHS Lanarkshire
We would like to thank all members and active participants in the cancer network for their continued support of the MCN, and the many hospitals that are committed to making the audit succeed. We also acknowledge the efforts of the clinical effectiveness staff, nurses, and other service users for their work in ensuring the data are available to enable analysis to take place each year. Without their considerable efforts this level of progress would not be possible.

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 33
Abbreviations
BWoSCC
Beatson West of Scotland Cancer Centre
CEF
Clinical Effectiveness Facilitator
CEPAS
Chemotherapy Electronic Prescribing and Administration System
DCE Detect Cancer Early
e-CASE
Electronic Cancer Audit Support Environment
ER
Oestrogen receptor
FNA
Fine Needle Aspiration
GP
General Practitioner
HER2
Human Epidermal growth factor Receptor
ISD
Information Services Division
MCN
Managed Clinical Network
MDT
Multidisciplinary Team
NHSGGC
NHS Greater Glasgow and Clyde
NHS QIS
NHS Quality Improvement Scotland
PR
Progesterone Receptor
RCAG
Regional Cancer Advisory Group
SLNB
Sentinel Lymph Node Biopsy
T4
Thyroid Hormone
WoS
West of Scotland
WoSCAN
West of Scotland Cancer Network

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 34
References List of references and useful websites for further information
1. Cancer in Scotland, October 2011
2. ISD, National Services Scotland, August 2010
3. http://www.isdscotland.org/Health-Topics/Waiting-Times/Publications/2012-09-25/2012-09-25-CWT-Report.pdf?17112368346

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 35
Appendix I
List of NHS QIS Standards consistently met across WoS Diagnosis
o 8a.1 - A minimum of 85% of breast cancer patients have a non-operative diagnosis (FNA/core biopsy/large volume biopsy.
Surgical Management
o 9a.1 - A minimum of 70% of all symptomatic breast cancers are surgically treated. o 9c.1 - A minimum of 5% of mastectomy patients have immediate breast reconstruction. o 9d.1 - A maximum of 10% of breast cancer patients with breast conservation have final excision
margins of less than 1mm. o 9e.1 - A minimum of 90% of breast cancer patients having surgery for invasive tumours, undergo
surgical staging of the axilla. o 9f.1 - A minimum of 75% of breast cancer patients undergoing surgical staging of the axilla for
invasive tumours less than 15mm invasive tumour size (pathological diameter) have node sampling or a sentinel lymph node biopsy (SLNB) rather than axillary clearance. (Excluding patients who have undergone neoadjuvant treatment).
Pathology
o 10a.1 - A minimum of 90% of surgically treated invasive breast cancers have the tumour grade known and reported.
o 10a.2 - A minimum of 90% of surgically treated breast cancers have the closest margin reported in mm from invasive tumour and in situ disease, where present.
o 10a.3 - A minimum of 90% of surgically treated breast cancers have the whole tumour size reported in mm including invasive tumour and in situ disease, where present.
o 10b.1 - A minimum of 90% of invasive breast cancers have the oestrogen receptor (ER) status measured and reported.
o 10b.2 - A minimum of 90% of invasive cancers have human epidermal growth factor receptor 2 (HER2) tested and reported.
Oncological Management
o 11c.1 - A minimum of 90% of invasive breast cancer patients who are ER-positive or PR-positive, receive adjuvant treatment which includes hormonal therapy or ovarian ablation.
o 11d.1 - A minimum of 85% of breast cancer patients less than 50 years at diagnosis who are node-positive, receive chemotherapy as part of the initial plan of treatment.
o 11d.2 - A minimum of 80% of breast cancer patients less than 70 years at diagnosis who are ER/PR-negative, node-positive, receive chemotherapy as part of the initial plan of treatment.
o 11e.1 - A minimum of 70% of breast cancer patients with HER2 positive or fluorescence in situ hybridisation (FISH) positive invasive cancer greater than 10 mm or node-positive, excluding T4 or inflammatory cancers, who have received chemotherapy, receive Trastuzumab.

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 36
Appendix II
Respondents
Lead Breast Clinician
MDT Sign Off Comments Submitted
Monzir Osman Ayrshire & Arran Yes Yes Michail Winkler Forth Valley Yes Yes Alison Lannigan Lanarkshire Yes Yes Douglas Hansell Greater Glasgow and Clyde Yes No

Appendix: NHS Board Action Plans A summary of actions for each NHS Board has been included within the Action Plan templates in Appendices III – VI. Completed Action Plans should be returned to WoSCAN within two months of publication of this report.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 Appendix

Appendix III
Action / Improvement Plan
Timescales No Action Required Health Board Action Taken Start End
Lead Progress/Action Status Status (see key)
Ensure actions mirror those detailed in Audit Report.
Detail specific actions that will be taken by the NHS Board.
Insertdate
Insertdate
Insert name of responsible lead for each specific action.
Provide detail of action in progress, change in practices, problems encountered or reasons why no action taken.
Insert No. from key above
1.
NHS Boards to assess their diagnostic capacity, taking cognisance of the increase in activity as a result of the Detect Cancer Early (DCE) initiative.
2. NHS Ayrshire & Arran should feed back the outcome of the review of cases not meeting Standard 7a.3 to the MCN Advisory Board and assess if further action is required.
3.
NHS Boards to review oncology appointment booking process to minimise any delay in commencing chemotherapy.
Health Board: NHS Ayrshire & Arran KEY (Status) Action Plan Lead: 1 Action fully implemented Date: 2 Action agreed but not yet implemented 3 No action taken (please state reason)
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 Appendix

Timescales No Action Required Health Board Action Taken Start End
Lead Progress/Action Status Status (see key)
4. NHS Ayrshire & Arran should feed back the outcome of the review of cases not meeting Standard 9g.1 to the MCN Advisory Board and assess if further action is required.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 Appendix

Appendix IV
Action / Improvement Plan
Health Board: NHS Forth Valley KEY (Status) Action Plan Lead: 1 Action fully implemented Date: 2 Action agreed but not yet implemented 3 No action taken (please state reason)
Timescales No Action Required Health Board Action Taken Start End
Lead Progress/Action Status Status (see key)
Ensure actions mirror those detailed in Audit Report.
Detail specific actions that will be taken by the NHS Board.
Insertdate
Insertdate
Insert name of responsible lead for each specific action.
Provide detail of action in progress, change in practices, problems encountered or reasons why no action taken.
Insert No. from key above
1.
NHS Boards to assess their diagnostic capacity, taking cognisance of the increase in activity as a result of the Detect Cancer Early (DCE) initiative.
2.
NHS Boards to review oncology appointment booking process to minimise any delay in commencing chemotherapy.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 Appendix

Appendix V
Action / Improvement Plan
Health Board: NHS Lanarkshire KEY (Status) Action Plan Lead: 1 Action fully implemented Date: 2 Action agreed but not yet implemented 3 No action taken (please state reason)
Timescales No Action Required Health Board Action Taken Start End
Lead Progress/Action Status Status (see key)
Ensure actions mirror those detailed in Audit Report.
Detail specific actions that will be taken by the NHS Board.
Insertdate
Insertdate
Insert name of responsible lead for each specific action.
Provide detail of action in progress, change in practices, problems encountered or reasons why no action taken.
Insert No. from key above
1.
NHS Boards to assess their diagnostic capacity, taking cognisance of the increase in activity as a result of the Detect Cancer Early (DCE) initiative.
2.
NHS Boards to review oncology appointment booking process to minimise any delay in commencing chemotherapy.
West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 Appendix

West of Scotland Cancer Network Final – Published Breast Cancer MCN Audit Report 07/01/2013 Appendix
Appendix VI
Action / Improvement Plan
Timescales No Action Required Health Board Action Taken Start End
Lead Progress/Action Status Status (see key)
Ensure actions mirror those detailed in Audit Report.
Detail specific actions that will be taken by the NHS Board.
Insertdate
Insertdate
Insert name of responsible lead for each specific action.
Provide detail of action in progress, change in practices, problems encountered or reasons why no action taken.
Insert No. from key above
1.
NHS Boards to assess their diagnostic capacity, taking cognisance of the increase in activity as a result of the Detect Cancer Early (DCE) initiative.
2.
NHS Boards to review oncology appointment booking process to minimise any delay in commencing chemotherapy.
Health Board: NHS Greater Glasgow and Clyde KEY (Status) Action Plan Lead: 1 Action fully implemented Date: 2 Action agreed but not yet implemented 3 No action taken (please state reason)