mc namara analysis
TRANSCRIPT

GOOD MORNING

McNAMARA ANALYSIS
WHY ANOTHER ANALYSIS? Most of the analyses available conceived during
the period (1940 to 1970) when significant alterations in craniofacial structural relationships were thought impossible.
Clinical orthodontics has seen the advent of numerous orthognathic surgery procedures which allow three-dimensional repositioning of almost every bony structure in the facial region and of functional appliance therapy which presents new possibilities in the treatment of skeletal discrepancies.

• Therefore, a need was arisen for a method of cephalometric analysis that is sensitive not only to the position of the teeth within a given bone but also to the relationship of the jaw elements and cranial base structures one to another.
• This analysis represents an effort to relate teeth to teeth, teeth to jaws, each jaw to the other, and the jaws to the cranial base.

INTRODUCTIONDr James. A. McNamara, described a method of cephalometric analysis which is used in the evaluation and treatment planning of orthodontic and orthognathic surgery patients.
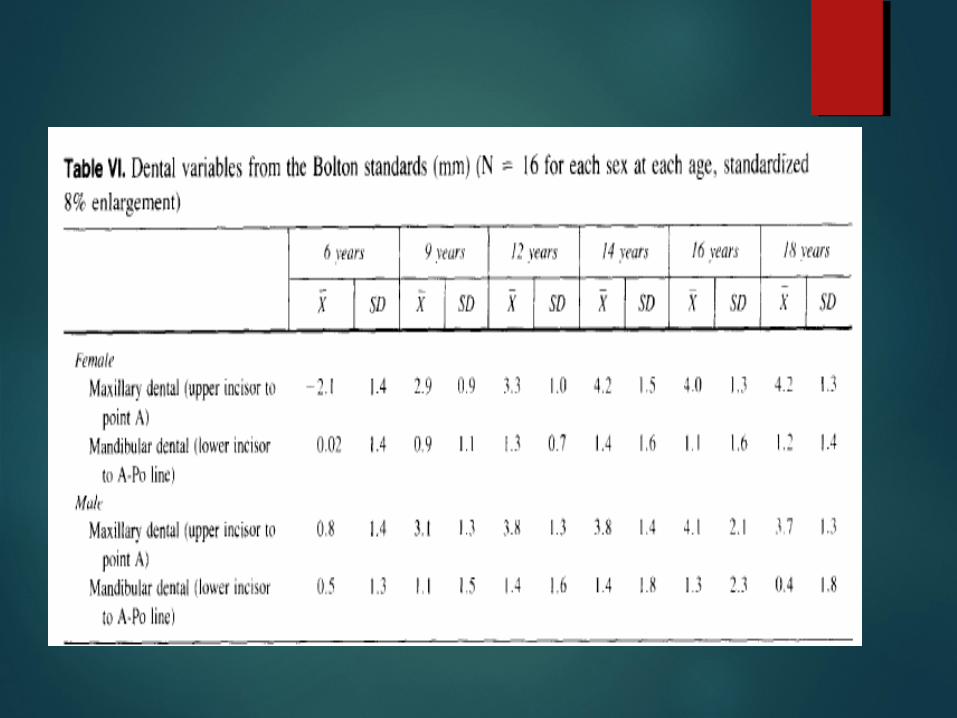
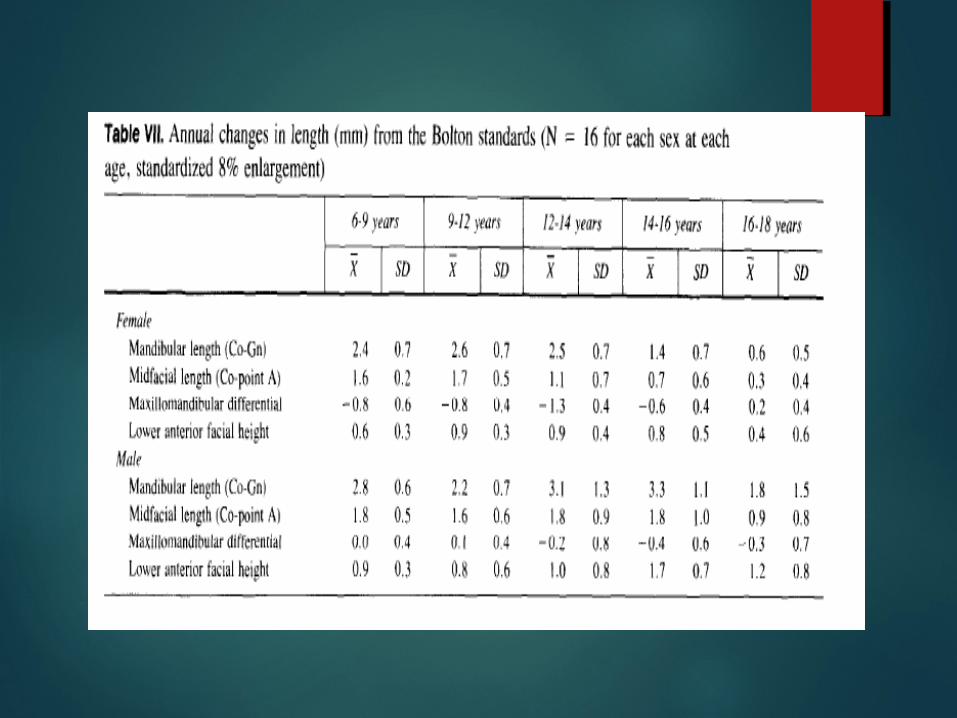
Standards for this analysis were derived from 3 sources:1.Selected values from the group of untreated children from Burlington research centre.2. Lateral cephalograms of children comprising Bolton standards.3. 111 Young adults from Ann Arbor, Michigan, having good to excellent facial and dental configuration. (Female- 26 yrs 8 mon, Male- 30 yrs 9 mon)
s
po
Ba
Co
Or
N
ANSA
Ptm
MeGnPog
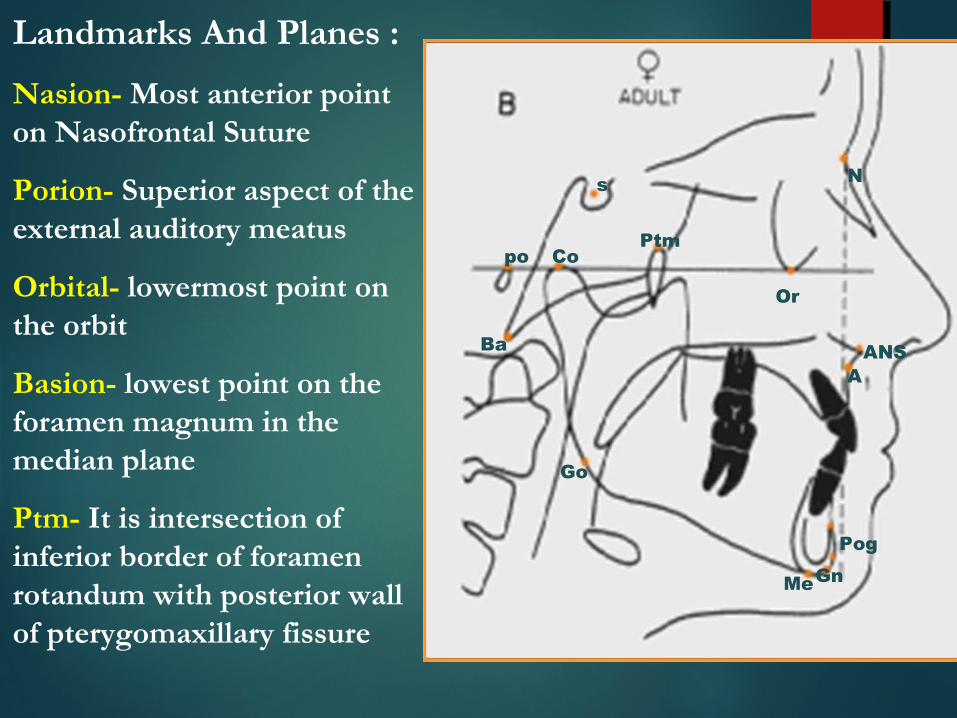
Landmarks And Planes :
Nasion- Most anterior point on Nasofrontal Suture
Porion- Superior aspect of the external auditory meatus
Orbital- lowermost point on the orbit
Basion- lowest point on the foramen magnum in the median plane
Ptm- It is intersection of inferior border of foramen rotandum with posterior wall of pterygomaxillary fissure
Go

s
po
Ba
Co
Or
N
ANSA
Ptm
MeGnPog
Landmarks And Planes :
ANS- Tip of the bony anterior nasal spine
Point A- Deepest point on the curved bony outline ( subspinale )
Pogonion- Most anterior point on the bony chin
Menton- Lowest point on the outline of the symphysis
Gonion- Constructed by intersection of the lines tangent to the posterior margin of the ascending ramus & the lower border
Go

s
po
Ba
Co
Or
N
ANSA
Ptm
MeGnPog
Landmarks And Planes :
Gnathion- Constructed by intersecting a line drawn perpendicularly to the line connecting Me and Pog
Condylion- Most posterosuperior point on the outline of the condyle
Go

Planes and measurements used for : For skeletal study:
1. Nasion perpendicular (mcnamara’s line or vertical):
from nasion to chin perpendicular to Frankfort plane.
2. Linear distance from point A to nasion perpendicular:
relates maxilla to cranial base.

3. Point pogonion to nasion perpendicular: Relates mandibular symphysis to cranial base.4. Maxillary length: (midfacial length) measures distance from condylion to point A.

5. Mandibular length: from condylion to anatomic gnathion.
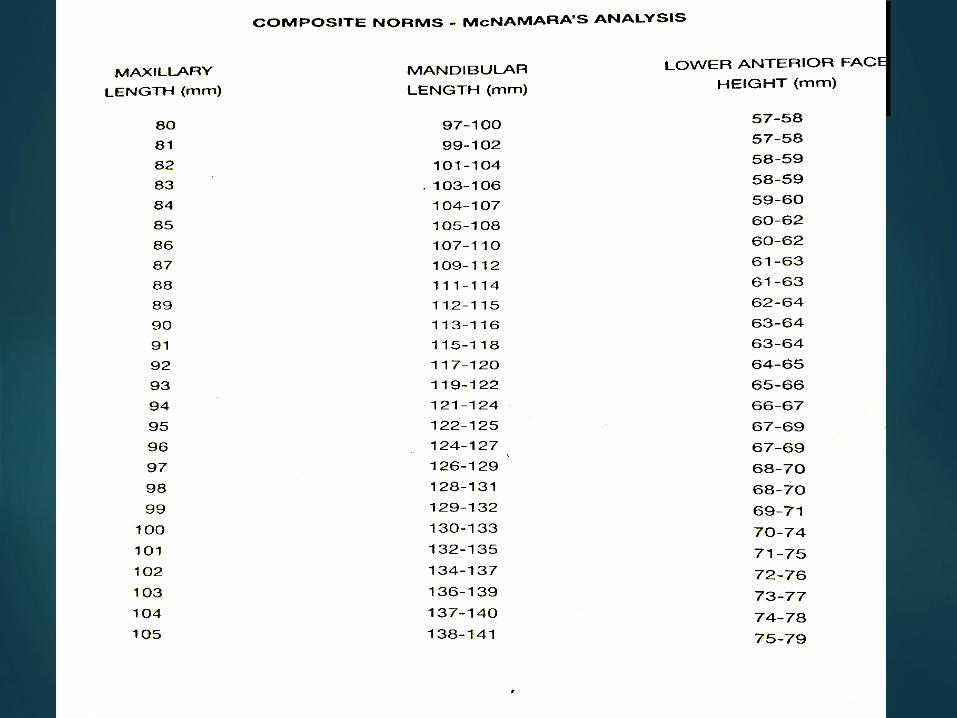
There is geometric relationship between midfacial and mandibular lengths. Any given midfacial length corresponds to given mandibular length.
6. Lower anterior facial height: from anterior nasal spine to menton.

Mcnamara divided craniofacial complex into 5 major sections:
Maxilla to Cranial base
Maxilla to Mandible
Mandible to Cranial base
Dentition
Airway

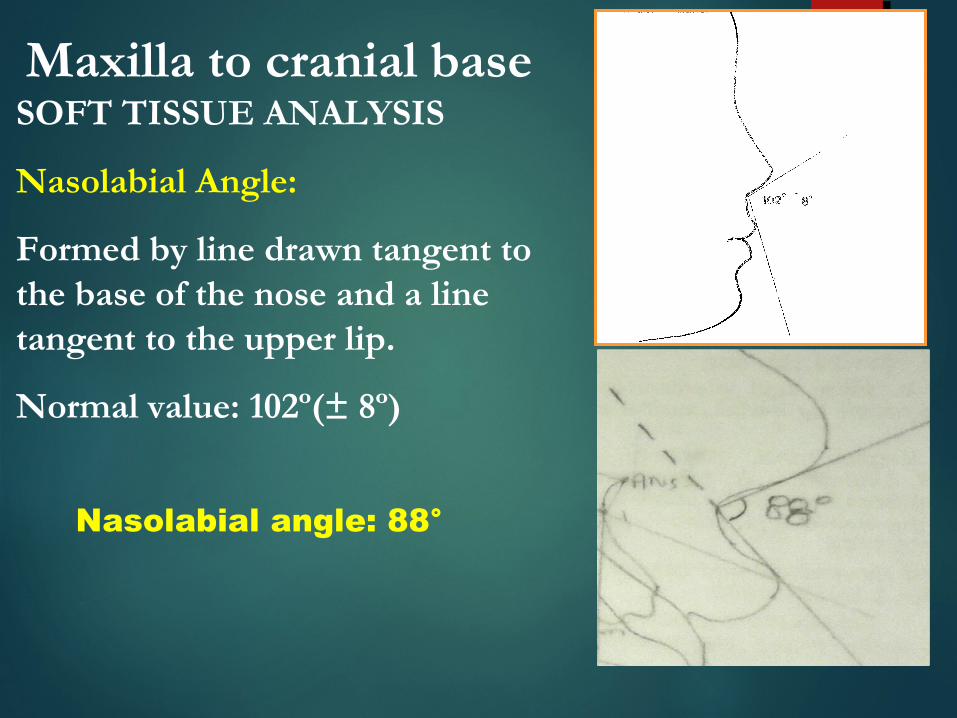
Maxilla to cranial baseSOFT TISSUE ANALYSIS
Nasolabial Angle:
Formed by line drawn tangent to the base of the nose and a line tangent to the upper lip.
Normal value: 102º(± 8º)
Nasolabial angle: 88°

Cant of the upper lip
It should be slightly forward to form an angle of about –
In women 14° ± 8°In men 8° ± 8°
N Perpendicular
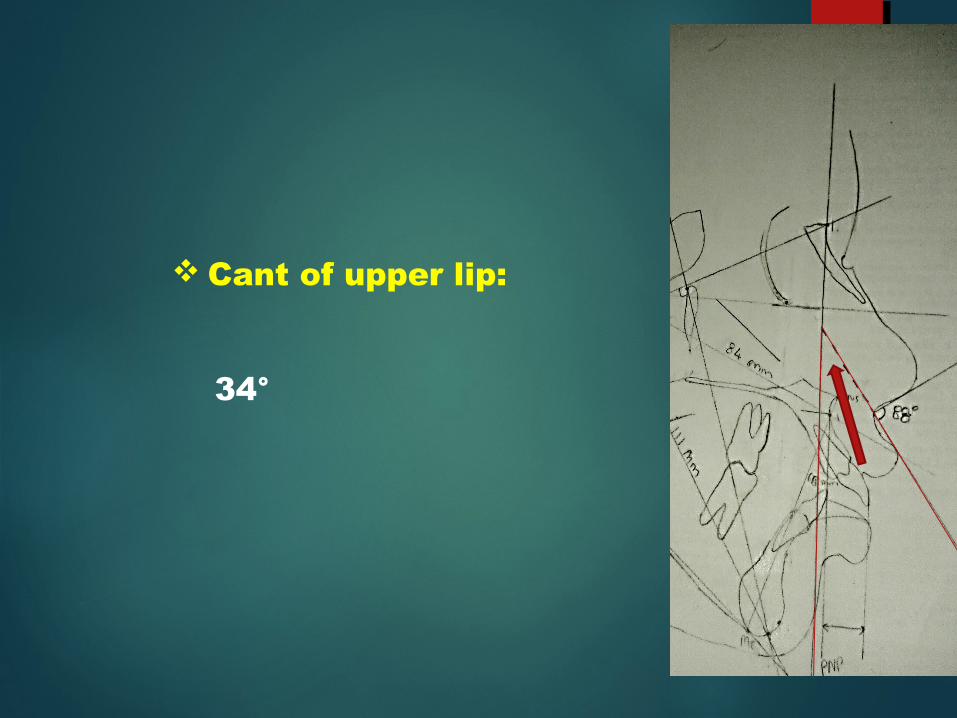
Cant of upper lip:
34°
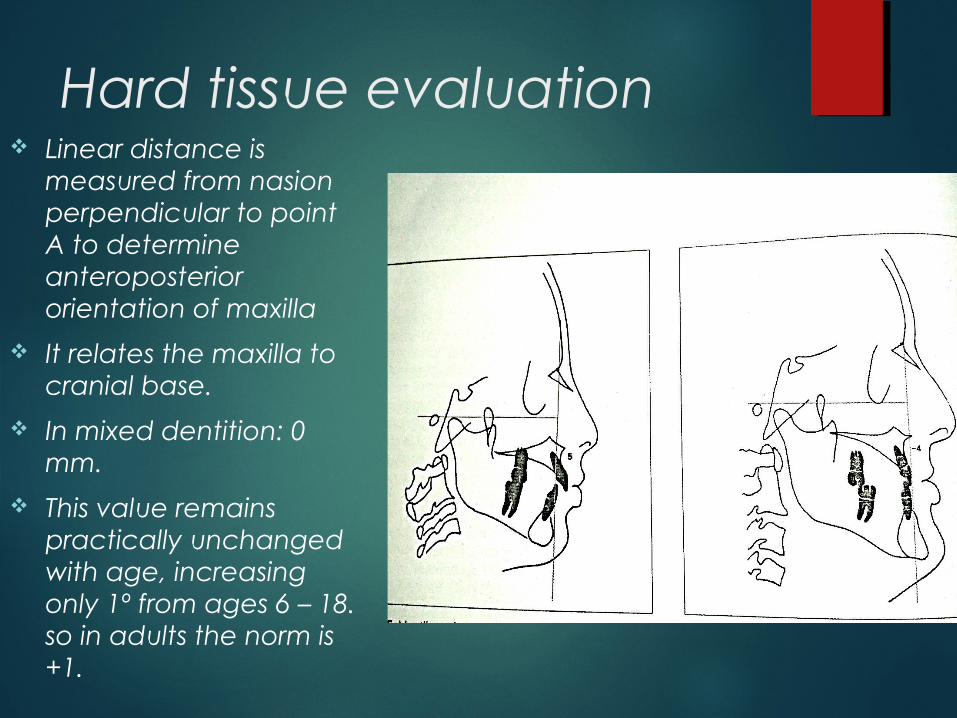
Hard tissue evaluation Linear distance is
measured from nasion perpendicular to point A to determine anteroposterior orientation of maxilla
It relates the maxilla to cranial base.
In mixed dentition: 0 mm.
This value remains practically unchanged with age, increasing only 1º from ages 6 – 18. so in adults the norm is +1.
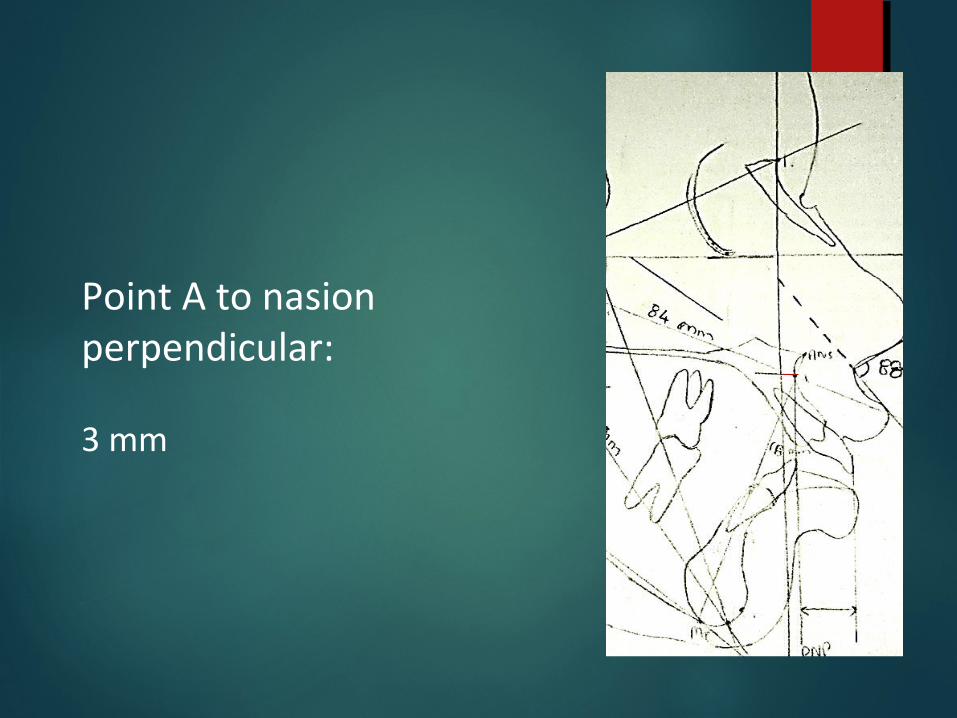
Point A to nasion perpendicular:
3 mm
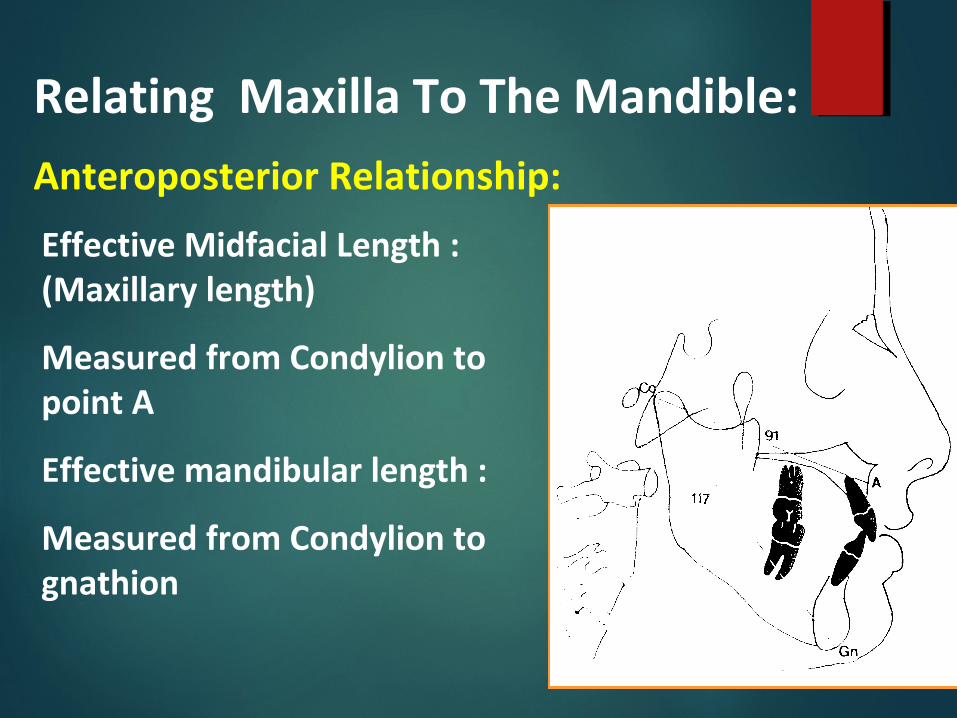
Relating Maxilla To The Mandible:
Anteroposterior Relationship:
Effective Midfacial Length : (Maxillary length)
Measured from Condylion to point A
Effective mandibular length :
Measured from Condylion to gnathion
Any given effective midfacial length corresponds to a given effective mandibular length
Mandibular length – Midfacial length =
Maxillomandibular differential
Effective lengths are not age or sex related but are related only to size of component parts. Thus the terms ued are-• Mixed dentition - Small • Adult female - Medium• Adult male – Large.
Thus “small”, “medium” and “large” are the preffered terms when describing these facial relationship.

Small : 20 mm to 23 mm Medium : 25 to 27 mm
Large : 30 to 33 mm

Midfacial length: (Co – Point A)
84 mm.
•So according to macnamara measurements mandibular length should be between 104- 107 mm and lower anterior face height should be 58- 59 mm for this case. • But in this case mandibular length – 111 mm lower anterior face height – 68 mm•Maxillomandibular differential = 111- 84 = 27 mm
VERTICAL RELATIONSHIP
Vertical maxillary excess can cause a downward and backward rotation of mandible resulting in an increase in lower anterior face height.
Vertical maxillary dentoalveolar deficiency will cause mandible to rotate upward and forward so reducing LAFH.
An increase or decrease in the lower anterior face height can have a profound effect on the horizontal relationship of the maxilla and mandible

Vertical Relationship :
Lower Anterior Face Height :
Measured from ANS to
menton
Increases with age and is correlated With effective midfacial length
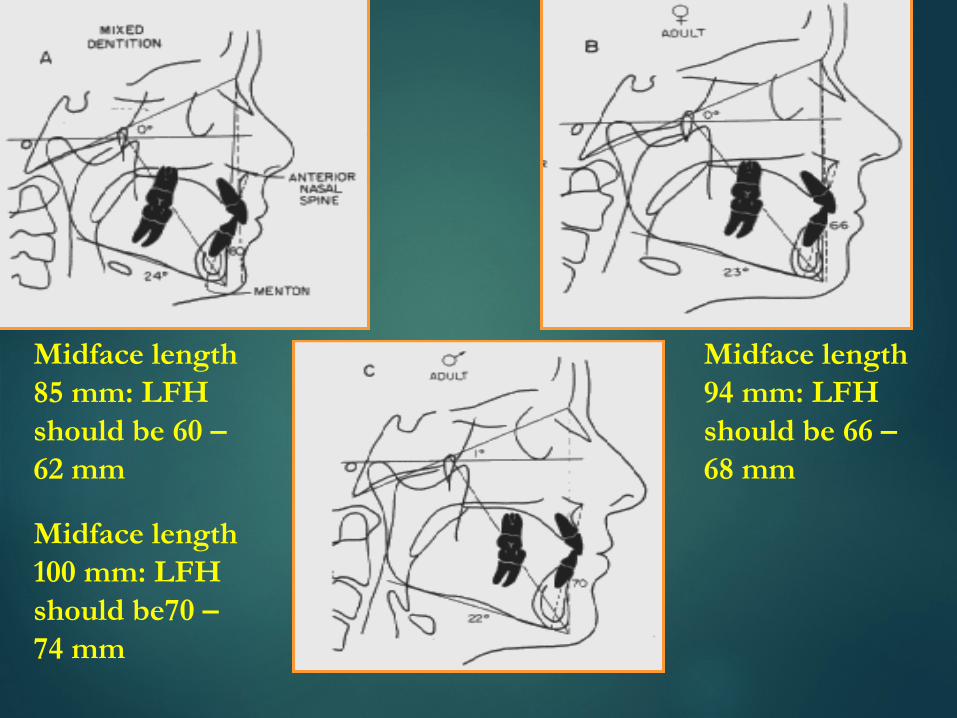
Midface length 85 mm: LFH should be 60 – 62 mm
Midface length 94 mm: LFH should be 66 – 68 mm
Midface length 100 mm: LFH should be70 – 74 mm
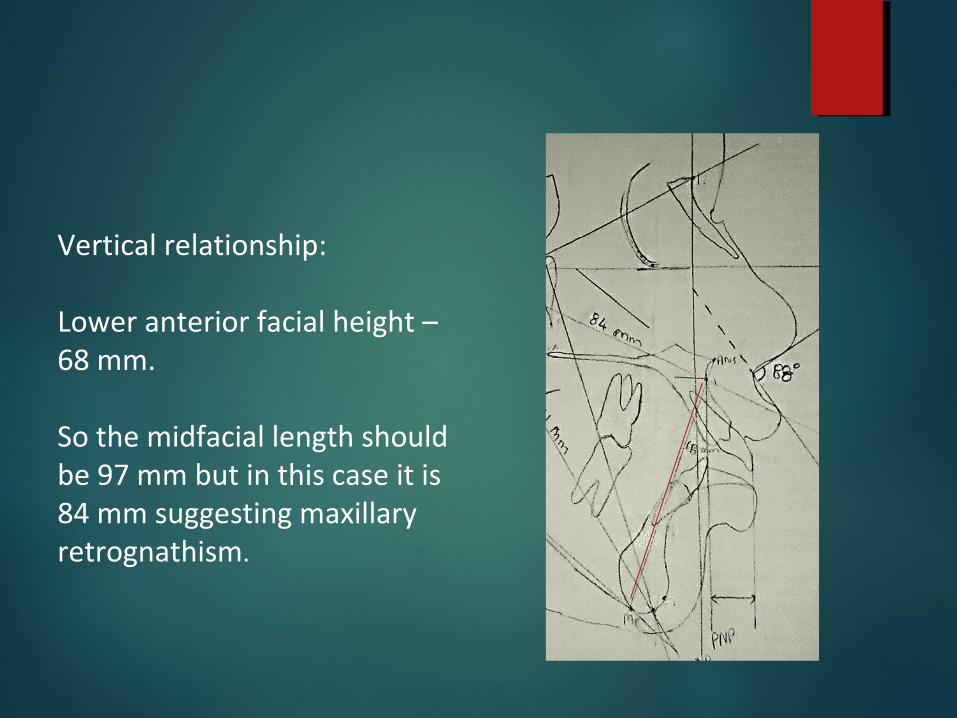
Vertical relationship:
Lower anterior facial height – 68 mm.
So the midfacial length should be 97 mm but in this case it is 84 mm suggesting maxillary retrognathism.
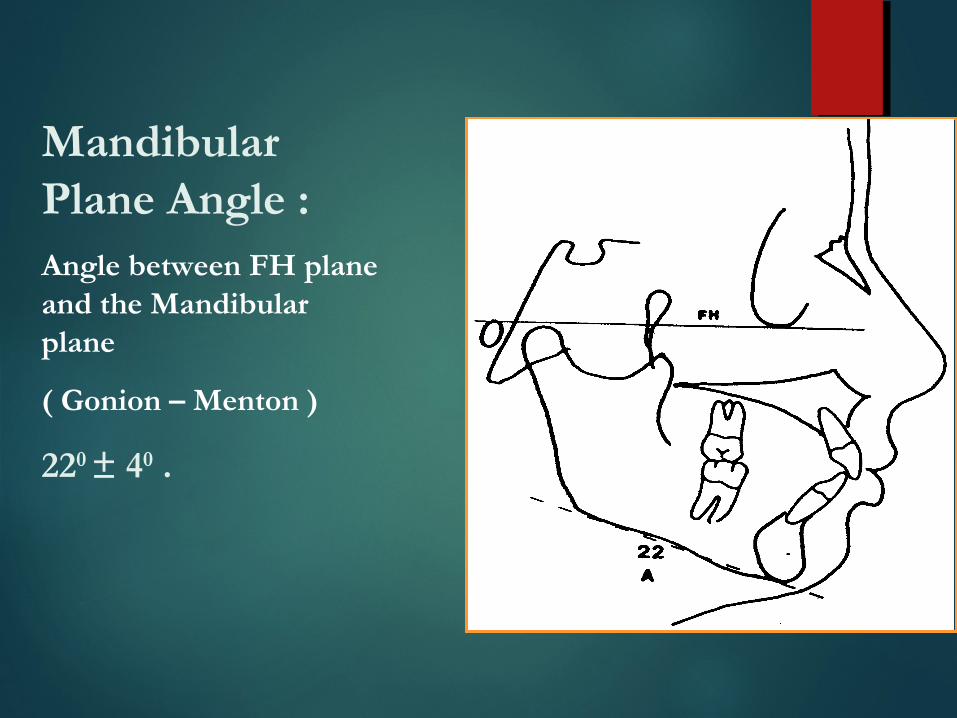
Mandibular Plane Angle :Angle between FH plane and the Mandibular plane
( Gonion – Menton )
220 ± 40 .

Mandibular plane angle:
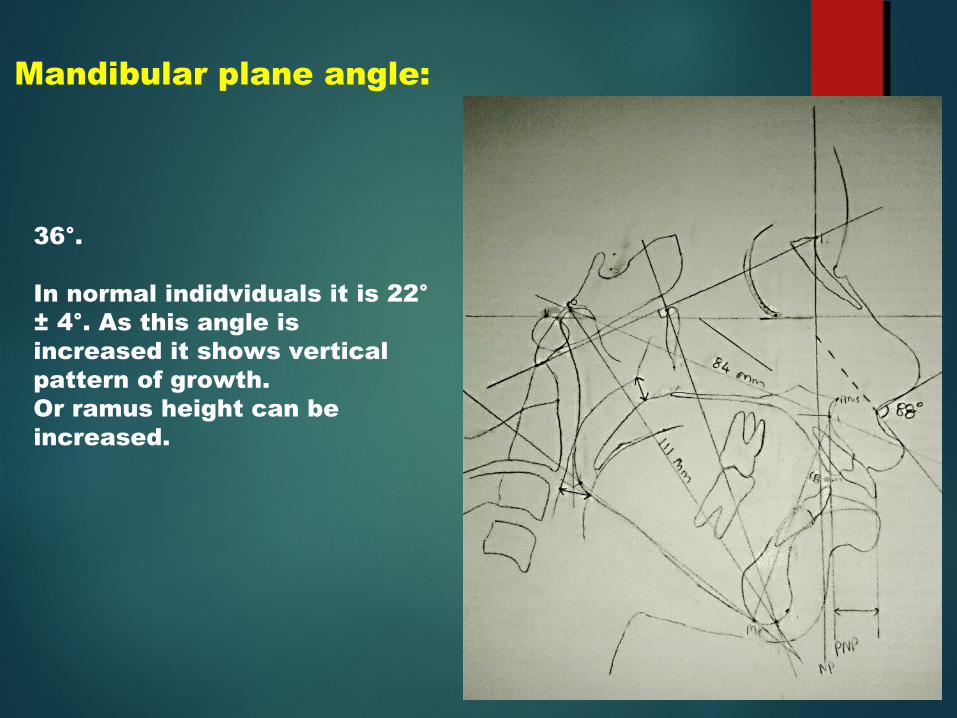
36°.
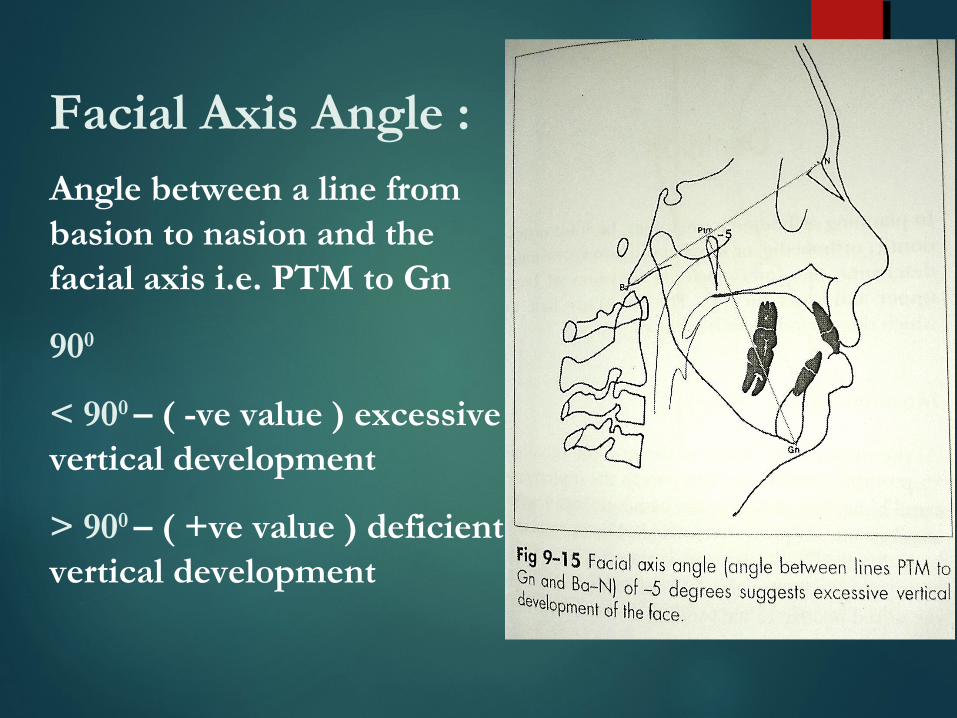
Facial Axis Angle :Angle between a line from basion to nasion and the facial axis i.e. PTM to Gn
900
< 900 – ( -ve value ) excessive vertical development
> 900 – ( +ve value ) deficient vertical development

Facial axis angle
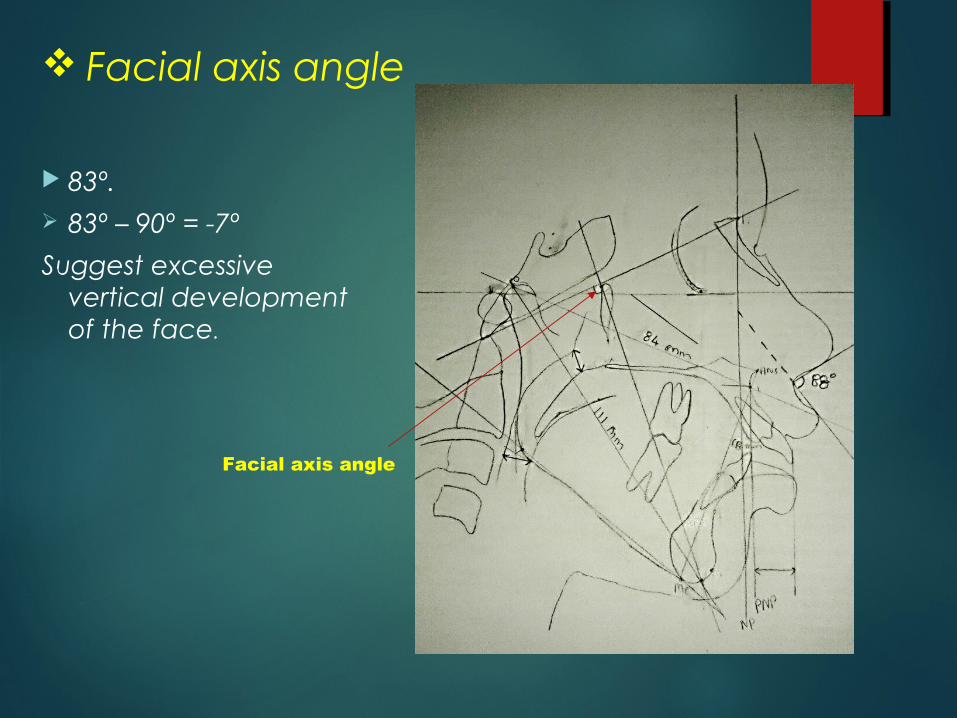
83º. 83º – 90º = -7º
Suggest excessive vertical development of the face.
Facial axis angle

Relating Mandible To The Cranial BaseDistance from Pog to the nasion Perpendicular.
In mixed dentition: 6-8 mm posterior to nasion perpendicular, but moves forward during growth.
In adult women: 4-0 mm behind nasion peprndicular line.
Adult men2 mm behind to approximately 2 mm forward of nasion perpendicular line.

Relating mandible to cranial base
Distance from pogonion to nasion perpendicular :
1o mm.

Dentition
In planning orthodontic treatment one must determine the anteroposterior position of the upper and lower incisors.
So the position of incisors in relation to basal bone must be determined

Relating upper Incisor to Maxilla :To measure position of maxillary incisor in relation to its apical base - a vertical line is drawn through point A parallel to nasion perpendicular.
Distance from point A to facial surface of incisor is measured.
It should be 4-6 mm

Vertical position :
The incisal edge of the upper incisor lies 2 – 3 mm below the upper lip at rest
Vertical position of the upper lip is best determined at the time of clinical examination

Maxillary incisor position:
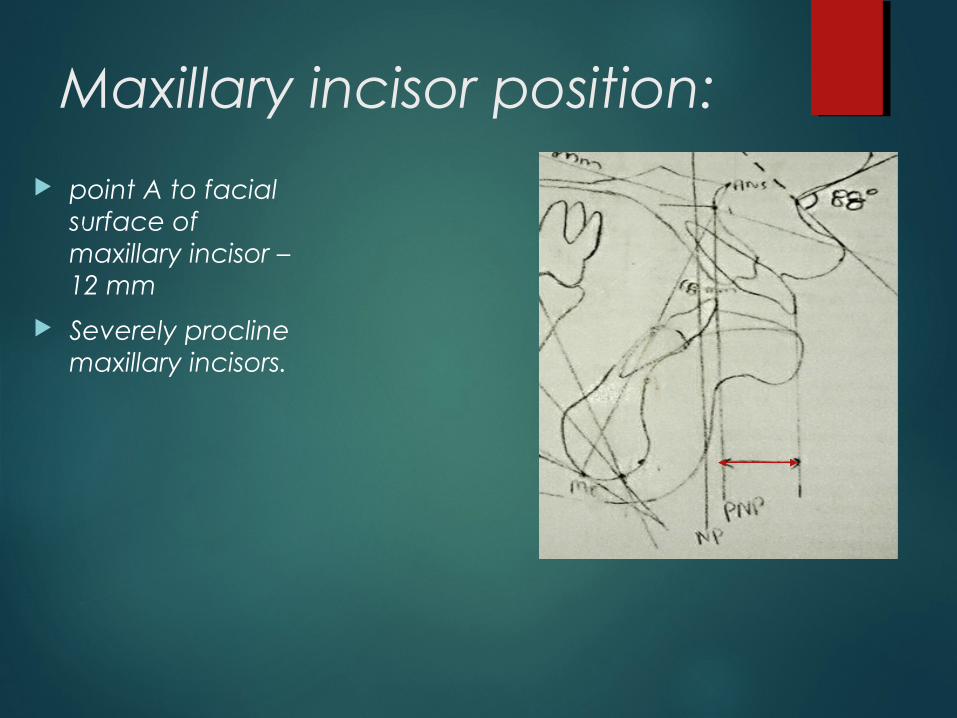
point A to facial surface of maxillary incisor – 12 mm
Severely procline maxillary incisors.

Relating Lower Incisor To Mandible :
Anteroposterior position :Measurement between the edge of the lower incisor to the A – Pog line
Normal : 1 mm to 3 mmA
Pog

Mandibular incisor position
Distance measured from edge of mandibular incisor to point A pogonion line-
5 mm

Assessment of vertical position of lower incisor:
• If the curve of spee is excessive, a decision must be made wheather the lower incisors should be intruded or molars erupted.
• Determining factor is the lower anterior facial height.
• If the lower anterior facial height is normal or excessive the lower incisor should be intruded.
• If the lower anterior facial height is deficient then the lower incisor should be extruded or buccal segments further erupted.

Airway :
Upper pharynx
Width is measured from a point on the posterior outline of the soft palate to the closest point on the posterior pharyngeal wall
Average : 15 - 20 mm

Airway :
Lower pharynx
Width is measured from intersection of the posterior border of tongue and the inferior border of the mandible to the closest point on the posterior pharyngeal wall
Average : 10 – 12 mm
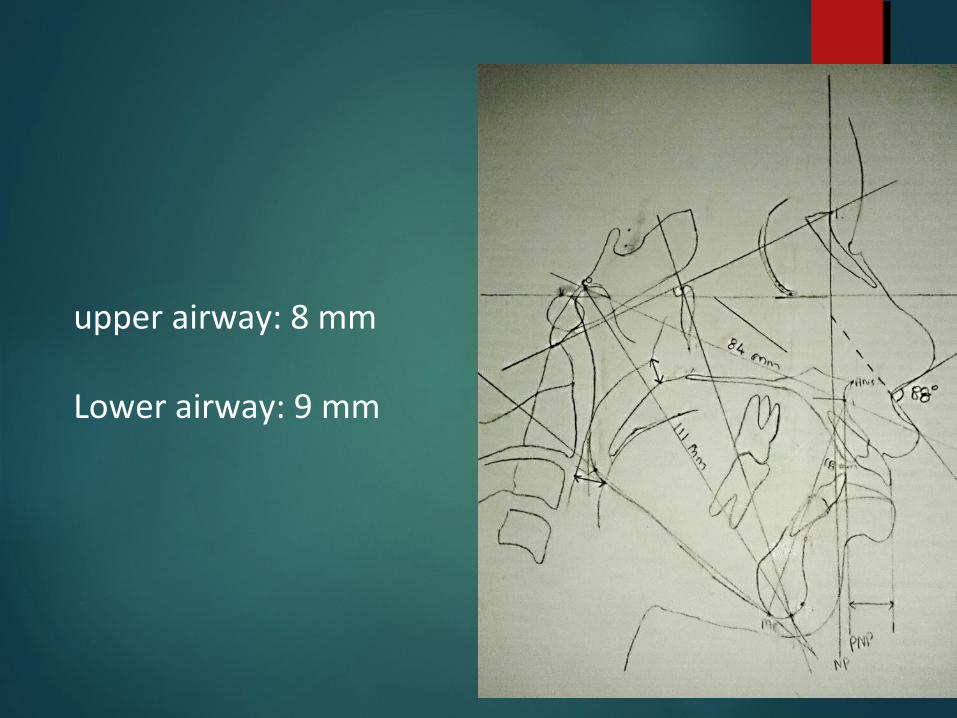
upper airway: 8 mm
Lower airway: 9 mm

Case discussion

Relating maxilla to cranial base:Soft tissue evaluation:Nasolabial angle: 88° (102° ±8°) Cant of upper lip: 35°(14°±8°)
Hard tissue evaluation:Midfacial length(co to point A): 84 mm mandibular length shoulb be between 104- 107 mm and lower anterior face height should be 58- 59 mm. In this case mandibular length – 111 mm lower anterior face height – 68 mm
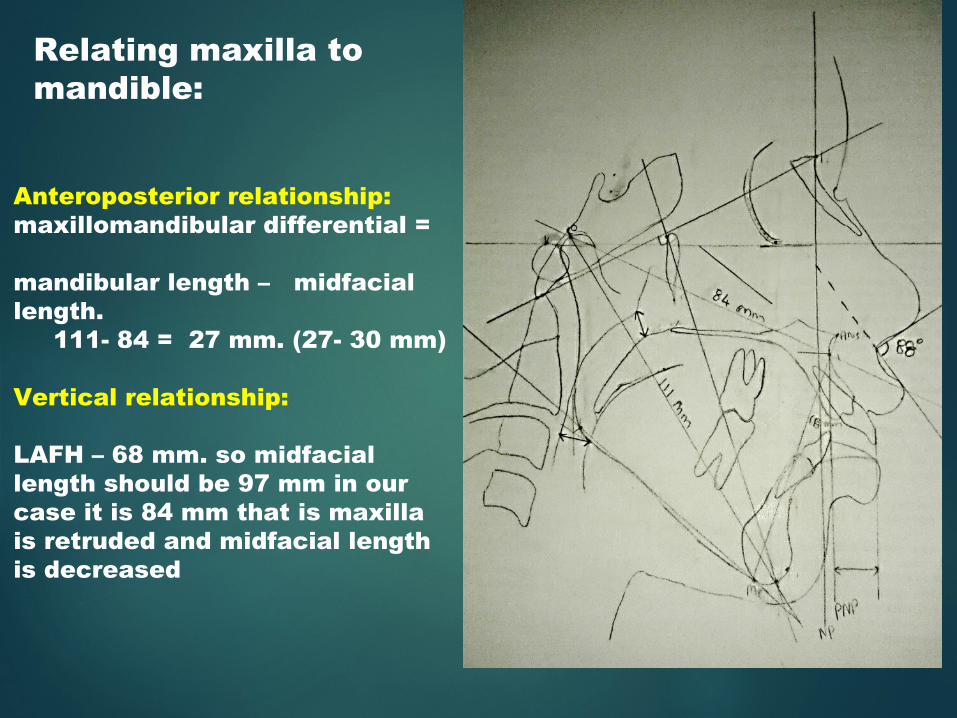
Relating maxilla to mandible:
Anteroposterior relationship:maxillomandibular differential = mandibular length – midfacial length. 111- 84 = 27 mm. (27- 30 mm)
Vertical relationship:
LAFH – 68 mm. so midfacial length should be 97 mm in our case it is 84 mm that is maxilla is retruded and midfacial length is decreased
36°.
In normal indidviduals it is 22° ± 4°. As this angle is increased it shows vertical pattern of growth.Or ramus height can be increased.
Mandibular plane angle:
Facial axis angle
83º. 83º – 90º = -7º
Suggest excessive vertical development of the face.
Facial axis angle

Relating mandible to cranial base
Distance from pogonion to nasion perpendicular :
1o mm therefore the mandible is retruded.
Maxillary incisor position:
point A to facial surface of maxillary incisor – 12 mm
Severely procline maxillary incisors.

Relating Lower Incisor To Mandible :
Anteroposterior position :Measurement between the edge of the lower incisor to the A – Pog line
Normal : 1 mm to 3 mmA
Pog

Mandibular incisor position
Distance measured from edge of mandibular incisor to point A pogonion line-
5 mm

upper airway: 8 mm
Lower airway: 9 mm
So the findings shows that patient have:
•Upper incisors proclined.
•Midfacial lemgth is less.
•Lower anterior facial height is increased.
•Mandible is growing more vertically and downwards.
•Airway space is reduced suggestive of breathing impairment.

Advantages :
Linear measurements rather than angles
Provides guidelines with respect to normally occurring growth increments
The method is more sensitive to the vertical changes
Easily explained to non specialist and lay persons such as patients and parents
It analyzes the interarch relationshipin the vertical planeas well as the sagittal, integrating gthem into single unit.

ARTICLE
A method of cephalometric evaluation.-James A. McNamara, Jr., D.D.S., Ph.D. Ann Arbor. Mich.
This method represents an effert to relate teeth to teeth, teeth to jaws, each jaw to the other and jaws to the cranial base.
This method of cephalometric analysis is conventional in nature in that it consists of a predetermined set of measurements of angles and distances applied to each cephalometric tracing.
This method of cephalometric analysis is useful in the diagnosis and treatment planning of the individual patient when the values derived from the tracing of the patient’s initial head film are compared to established norms. Therefore, composite normative standards based on three cephalometric samples are provided.
Samples for study
1. First sample contained normative data derived from lateral cephalograms of childrens comprising
Bolton standards.
2. Selected values from a group of normal children
from Burlington orthodontic research centre.
3. The third group considered is the Ann Arbor
sample of 111 young adults with good to facial
configuration.

•The average age of the females in the sample was 26 years 8 months, while the average age of the males was 30 years 9 months at the time the cephalogram was taken.

DISCUSSION
• This method depends primarily upon linear measurements rather than angles, so that treatment planning (particularly treatment planning for the orthognathic surgery patient) is made easier.
• This method of analysis is more sensitive to vertical changes than is an analysis which relies on the ANB angle, such as that of Steiner.
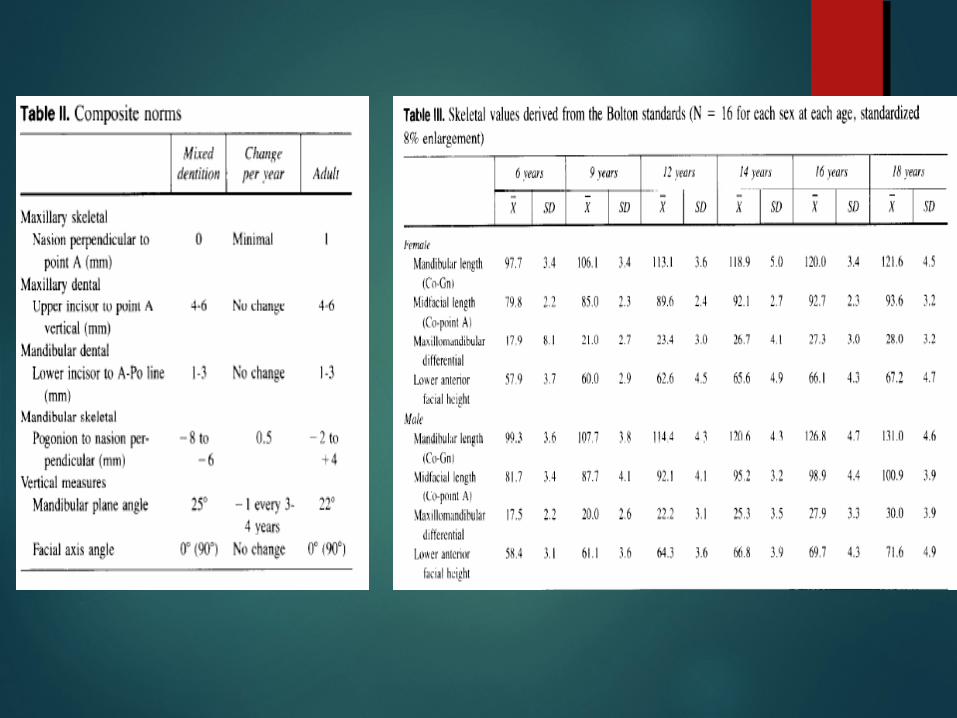
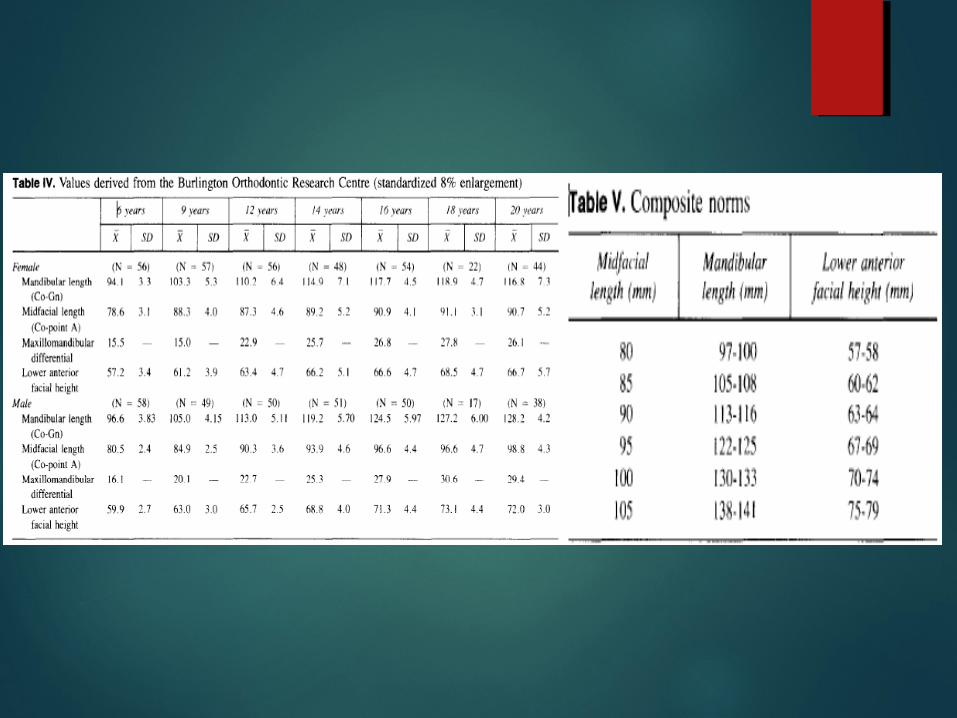
• This analytical procedure provides guidelines with respect to normally occurring growth increments. Therefore, the norms derived from the Bolton standards, the Burlington sample, and the Ann Arbor sample and the composite norms presented in this article can be used to evaluate treatment results.
• The principles of this analysis are easily explained to nonspecialists and to lay persons such as patients and parents.

RELATED ARTICLE
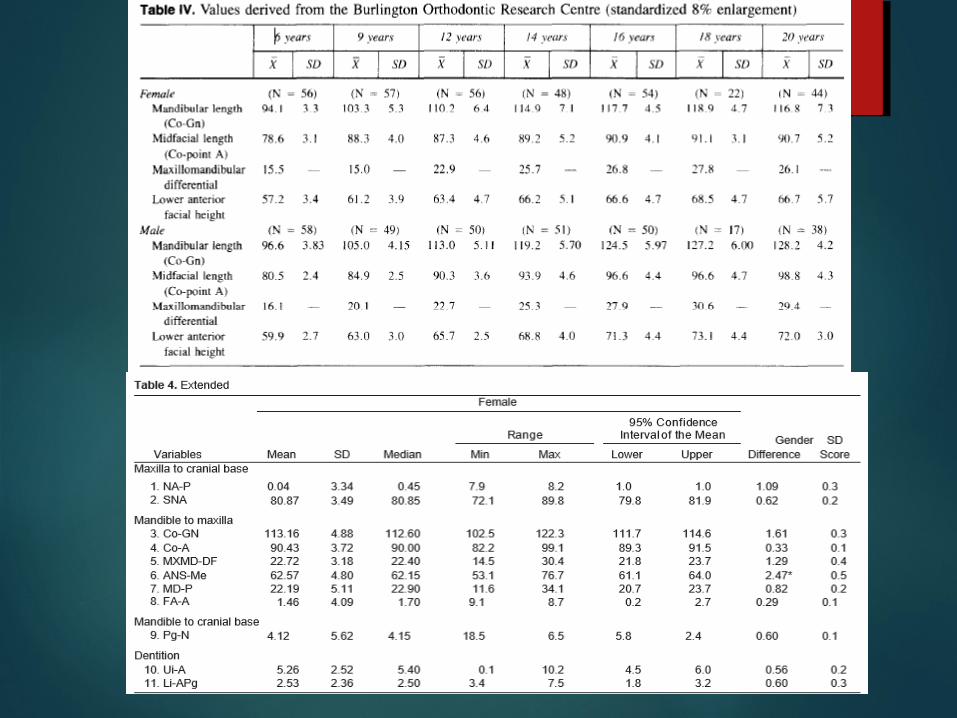
Chinese Norms of McNamara’s Cephalometric Analysis-John Wua; Urban Ha¨ggb; A. Bakr M. Rabiec

Objective:
To establish cephalometric norms of McNamara’s analysis in young Chinese and compare them to those of a matched young Caucasian sample.
Materials and Methods:
The material comprised lateral cephalometric radiographs of a random sample of 200 male and 205 female 12-year-old southern Chinese children, and an additional sample of 43 male and 43 female 12-year-old British Caucasian children in Hong Kong. The radiographs were digitized twice with the CASSOS program.
• McNamara’s analysis combines the anterior reference plane (a plane perpendicular to the Frankfurt horizontal through the nasion) described by Burstone et al and a description of the length of the jaws and their relationship as given by Harvold.
• This specific innovative cephalometric analysis was introduced because ‘‘a need had arisen for a method of cephalometric analysis that is sensitive not only to the position of teeth within a given bone, but also to the relationship of jaw elements and cranial base structures one to another.’’
This approach makes the actual analysis most suitable for diagnosis, treatment planning, and treatment evaluation, not only of conventional orthodontic patients, but also for patients with skeletal discrepancies who are candidates for dentofacial orthopedics and orthognathic surgery
This study establishes norms for young chinese children.






Discussion This study established norms for McNamara analysis5
in southern Chinese, separate for gender.
The study was based on a large sample of 12 year old children that was representative of its original population.
In the study, the cephalograms were measured twice and averaged figures were used.
These repeated measurements reduced the error of landmark identification, and duplicate measurements were sufficient for a comparison of the two groups.
Consequently, the means and standard deviations of the 11 cephalometric variables investigated in this study should be considered as representative for 12- year-old Chinese.

Results:
The results showed that there were statistically significant gender differences for six out of the 11 cephalometric variables in the Chinese, but for only one variable in the Caucasians. The size of the statistically significant gender differences varied from 0.3 to 0.4 on SD scores. There were statistically significant ethnic differences for eight variables in males and seven variables in females. The size of the observed statistically significant ethnic differences varied from 1.8 to 1.6 on SD scores.
CONCLUSIONS
• It would be preferable to use specific Chinese norms, separate for gender, because a comparison has revealed statistically significant differences in most variables between males and females and between Chinese and Caucasians

REFRENCE:
Orthodontics and orthognathic surgery diagnosis and planning by Jorge Gregoret.
Radiographic cephalometry by Alexander Jacobson
An original article by Mcnamara.
