masseter muscle fatigue in implant supported pros the tics
TRANSCRIPT

8/6/2019 Masseter Muscle Fatigue in Implant Supported Pros the Tics
http://slidepdf.com/reader/full/masseter-muscle-fatigue-in-implant-supported-pros-the-tics 1/6
S E C T I O N E D I T O R
M a s s e t e r m u s c l e f a t i g u e b e f o r e a n d a f t e r r e h a b i l i ta t i o n w i t hi m p l a n t - s u p p o r t e d p r o s t h e s e s
R . J a c o b s , D D S , P h D , a D . v a n S t e e n b e r g h e , M D , P h D , b a n dI . N a e r t , D D S , P h D c
Faculty of Medicine, Catholic University of Leuven, Leuven, Belgium
To e s t a b l i s h w h e t h e r d i f f e r e n t i m p l a n t - s u p p o r t e d p r o s t h e t i c r e c o n s t r u c t i o n si n f l u e n c e j a w m u s c l e r e s i s t a n c e t o c l e n c h i n g e f f o r t s , s u s t a i n e d s u b m a x i m a l ( 5 0 % )c l e n c h i n g w a s p e r f o r m e d i n t w o g r o u p s o f p a t i e n t s w h o w e r e e d e n t u l o u s i n o n e o rb o t h j a w s . O n e g r o u p c o n s i s t e d o f p a t i e n t s w h o w e r e r e h a b i l i t a t e d b y m e a n s o f a no v e r d e n t u r e o n t w o t o f o u r im p l a n t s c o n n e c t e d b y a b a r ; t h e o t h e r g r o u p c o n s i s t e do f p a t i e n t s w h o w e r e r e h a b i l i t a t e d w i t h a n i m p l a n t - s u p p o r t e d f i x e d p r o s t h e s i s o nf o u r to s e v e n i m p l a n t s i n e i t h e r t h e m a x i l l a o r t h e m a n d i b l e . R e s u l t s i n d i c a t e d t h a ta f t e r r e h a b i l i t a t i o n w i t h i m p l a n t - s u p p o r t e d f i x e d r e c o n s t r u c t i o n s , t h e m y o e l e c t r i co u t p u t l e v e l i n c r e a s e d o v e r t i m e , w h i c h w a s p a r a l l e l t o a h i g h e r b i t e f o r c e l e v e l .F o r t h e o t h e r g r o u p, s u c h a t i m e - d e p e n d e n t c h a n g e i n e l e c t r o m y o g r a p h i c a m p l i t u d ed i d n o t oc c u r . O n t h e o t h e r h a n d , p o w e r s p e c t r u m a n a l y s i s r e v e a l e d a s i g n i f i c a n td o w n w a r d s h i f t o f t h e m e a n p o w e r f r e q u e n c y d u r i n g s u s t a i n e d c l e n c h i n g a f t e rr e h a b i l i t a t i o n w i t h i m p l a n t - s u p p o r t e d o v e r d e n t u r e s b u t n o t w i t h i m p l a n t - s u p p o r t e df i x e d p r o s t h e s e s . T h e a b s e n c e o f a s p e c t r a l s h i f t i n t h e l a t t e r g r o u p p r o b a b l ye x p r e s s e d a f e a r o f b i t i n g t o o h a r d a n d f r a c t u r i n g t h e p r o s t h e s i s . ( J PRO STHET D EN T1 9 9 5 ; 7 3 : 2 8 4 - 9 . )
It has been assumed that implant-supported pros-theses lead to an impr ovement of masticatory muscle per-formance. 1 One para meter of muscle performance is fatigueresistance during sustained clenching. In a cross-sectionalstudy on different types of rehabilitation, fatigue occurredin patients with natural teeth, complete dentures, and im-plant- suppor ted overdentures, but fatigue was not presentin patients with fixed prostheses on implants. The absenceof fatigue in patients with fixed prostheses probablyreflected a fear of biting too hard and fracturing th e pros-thesis because of the absence of periodontal feedback. 2 Inthis follow-up study, the occurrence of change in fatigueresistance after installation of implants was investigated.
Muscle fatigue has been defined in different ways andhas led to different hypotheses about the underlyingmechanisms. 3-6 Time-d ependent changes in both myoelec-tric signal amplitude and spectral parameters may be ap-plied to monit or deterioration of muscle performance. 6 Forjaw muscles, the surface electromyogram (EMG) analyzed
Sponsored by the National Fund for Scientific Research (NFWOBelgium).
aResearch Assistant, NFWO, Department of Periodontology (lab-oratory of Oral Physiology).
bprofessor, Department of Periodontology, The P-I Br~nemarkChair in Osseointegration.
cprofessor, Department of Prosthetic Dentistry.Copyright | 1995 by The Editorial Council of THE JOURNAL OF
PROSTHETIC DENTISTRY.0022-3913/95/$3.00 + 0. 10/1/61130
by means of power spectrum analysis indicates that thepower shifts to lower frequencies when the subject ismaintaining a const ant clenching level. 7 The median fre-quency (mean power frequency, MPF) is one of the mostreliable spectral parame ters to analyze such shifts. 7 TheMPF is related to the bite force level. Lower MPF valuesare usually observed at higher bite force levels, ss~ Dent urewearers develop a reduced bite force compared with tha t ofsubjects with natu ral dentitions . 11 After r ehabili tationwith osseointegrated implant-supported prostheses, biteforce increases. I, 12-14 It could there fore be hypothesizedthat the increased bite force levels for implant-suppo rtedprostheses involve decreased MPF values.
This study investigated resistance to fatigue and shiftsin the power spectrum of the masseter muscle during asustained submaxi mal (50 %) clenching effort before andafter rehabilitation with osseointegrated implants. Thisinvestigation determined whet her masseter muscle fatiguewas depende nt on the type of the prosthetic super structuresupported by implants.
M AT E R I A L A N D M E T H O D S
S u b j e c t s
Seventeen women participated in the experiment (TableI). All subjects denied having any known heart disease orhypertension, which might make c onstant clenching effortunsafe because of the muscle heart reflex) 5 They gave in-formed consent and ethical committee approval was ob-tained.
2 8 4 T H E J O U R N A L O F P R O S T H E T I C D E N T I S T R Y V O L U M E 7 3 N U M B E R 3

8/6/2019 Masseter Muscle Fatigue in Implant Supported Pros the Tics
http://slidepdf.com/reader/full/masseter-muscle-fatigue-in-implant-supported-pros-the-tics 2/6
JACOBS, VAN STEENBERGHE, AND NAERT THE JOURNAL OF PROSTHETIC DENTISTRY
Table I. Patient groups
A g e (yr)N o . o f p a t i e n t s M e a n y e a r s o f
G r o u p ( a ll w o m e n ) M e a n ( S D ) R a n g e D e n t i t i o n e d e n t u l i s m(SD)
ODi 10 56 (8) 40-68 Over dent ure on impl ants 14 (13)
FFPi 7 50 (10) 34-62 Fixed prosthesis on implants 13 (8)
Before implant installation all patients were edentulousin at least one jaw and wore a complete dentur e for morethan 10 years (Table 1). The edentulous period before im-plant installation rang ed from 0 to 32 years (mean 14 years,standa rd deviation [SD] 13) for the overdenture su pportedby implan ts (ODi) group and 1 to 26 years (mean 13 years,SD 8) for the fixed implant-supported prosthesis (FFPi)group.
Test group ODi consisted of 10 patients whose agesranged from 40 to 68 years (mean age 56 years, SD 8) at en-try into the study. Seven of them h ad been rehabilitated bymeans of two osseointegrated implants connected by astr aigh t bar, s~:rictly parallel w ith the hinge axis of themandible suppor ting a denture in the lower jaw. Thus t heoverdenture was tissue-supported in the molar areas. Thethree others had been rehabilitated by means of fourosseointegrated implants connected by a ba r in the maxilla.The antagonistic jaw had natural teeth (n = 3) or carrieda complete denture (n = 7). Test group FFPi consisted ofseven patients whose ages ranged from 34 to 62 years (meanage 50 years, SD 10) at ent ry into the study. The y had beenrehabilitated by means of four to seven osseointegratedimplants supporting a full fixed prosthesis in either theupper or lower jaw opposing natural t eeth (n 4) or a com-plete denture (n 3).
For rehabilitation of the edentulous jaw with implant-supported prostheses, principles for occlusion and articu-lation did not differ from the conventional prosthodonticrules propo sed by Beyron. 16 Simult aneous bilateral cont actin centric relation was always present.
In both test groups, the experiments were done beforeimplant installation and 1 or 2 years after rehabilitationwith the present prostheses to avoid jaw muscle activityvariations caused by initial adaptati on to the prosthesis. 17
E x p e r i m e n t a l p r o c e d u r e
The subjects were seated upright in a dental chair withthe head leaning against the headrest. T he masseteric my-oelectric activity was recorded bilaterally by means of bi-polar surface tin/lead electrodes (Dantec Medical and Sci-entific Equipment, Skovlunde, Denmark) placed in paral-lel to the muscle fibers of the superficial masseter muscle.The electrode centers were 2 cm apart. To ensure repro-ducible placement of the electrodes at future recordings inthe subjects, a grid with horizontal and oblique intersect-ing lines was used. is A horizontal line was aligned with the
alar-tragus line, and the oblique intersecting line was po-sitioned parallel to the muscle fibers of the superficialmasseter muscle. The center of the upper electrode wasplaced 2 cm below the intersection, and the center of thesecond electrode was located on the same line 2 cm belowthis.
The skin was cleaned with ethyl alcohol and the pat ientwas grounded with a grounding electrode soaked in salinesolution (Dantec Medical and Scientific Equipment). Ateach follow-up session, t he maxima l EMG amplitude(EMGmax) when clenching bilatera lly was determined dur-ing an encouraged maximal clenching effort. Thereafterpatients had to develop an isometric contraction of the jawelevator muscles at 50% of EMGmax (50% maximum vol-unta ry contraction [MVC]) by clenching bilaterally. Visualfeedback by means of an oscilloscope screen showing theraw EMG amplitude allowed them to maintain a constantamplitude level until exhaustion appeared. Th e investiga-tor observed the experiments and gave the necessary feed-back to maintain the proper raw EMG level. Correctionsrarely had to be made, and when deviations occurred theywere always smaller than 10 ttV. Subjects clenched at theselected level for as long as possible until fatigue or painprevented them from further clenching (endurance time).The longest sustained contraction time was 5 minutes.Subjective perception of fatigue or pain was recorded. Inthis study, n o force meter was used that would inevitablylead to a bite rise. EMG feedback seemed appropriate tomeasure force output because of the existence of a linearrelationship between integrated surface EMG of the mas-seter and submaximal isometri c muscle force. 19, 20
D a t a c o l l e c t io n
During the clenching effort, 1/2-second runs of the mas-seter activity were recorded at the start and the end of thesustained contraction. The EMG was amplified with abandwidth from 20 to 1000 Hz. An on-line frequency anal-ysis was done in the 0 to 500 Hz frequency range by aDantec Counterpoint electromyograph (Dantec Medicaland Scientific Equipment) with a sampling frequency of204.8 kHz. It generated the power spectral densit y functionand the power spectra for each 1/2-second run.
Muscle fatigue is reflected by the time course of severalmyoelectric signal variables. I n this study, two paramet erswere chosen for data analysis. The peak -to-peak amplitudeand the MPF of all EMG signals were computed by the
MARCH 1995 28 5
8/6/2019 Masseter Muscle Fatigue in Implant Supported Pros the Tics
http://slidepdf.com/reader/full/masseter-muscle-fatigue-in-implant-supported-pros-the-tics 3/6
T H E J O U R N A L O F P R O S T H E T I C D E N T I S T R Y J A C O B S , VAN S T E E N B E R G H E , A N D N A E R T
350
3OO
(D
09 2500I . , .
o.m
g 200O~
"1:3
150E
@ 100
U.I
50
mB e B l =
before implants
ear after implants
2 years after implants
0overdenture on implants fixed prosthesis on implants
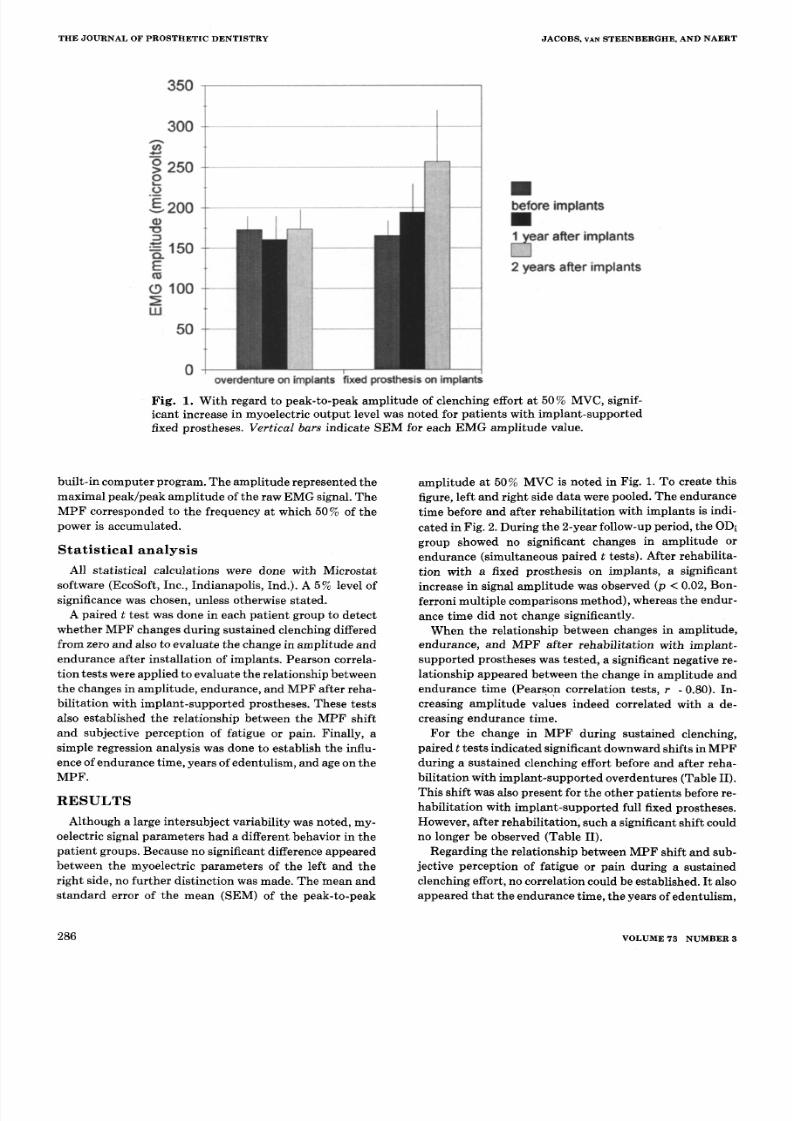
Fig . 1. With regard to peak -to-p eak ampli tud e of Clenching effort at 50 % MVC, signif-icant increase in myoelec t r ic output level was noted for pa t ien ts w i th implan t -suppo r tedfixed prostheses. Vertical bars indica te SEM for each EMG ampl i tude va lue .
bui l t - in computer program. The ampl i tude represented themax ima l peak /peak ampl i t ude o f t he r aw EMG s ignal . TheMP F corresponded to the f requency a t which 50 % of thepower i s accumula ted .
S t a t i s t i c a l a n a l y s i s
All stat ist ical calculations were done with Micros ta tsoftware (EcoSoft , Inc. , Indianap olis , Ind.) . A 5% level ofsignificance was chosen, unless otherwise stated.
A pai red t tes t w as done in each pa t ient group to de tec twhether MP F changes dur ing sus ta ined c lenching d i fferedfrom zero and a lso to evalua te the change in ampl i tude andendurance af te r ins ta l la t ion of implants . Pearson correla-t ion tes ts were appl ied to evalua te the re la t ionship be tweenthe changes in ampl i tude , endurance , and MP F a f ter reha-bi l i ta t ion wi th implant -suppor ted pros theses . These tes tsa lso es tabl i shed the re la t ionship be tween the MPF shi f tand subjective perception of fat igue or pain. Finally, asimple regression analysis was done to establish the influ-ence of endurance t ime, years of edentu l i sm, and age on theM P F.
R E S U LT S
Although a la rge in tersubjec t var iabi l i ty was noted , my-oelec tr ic s ignal parame ters h ad a d i fferent behavior in thepatient groups. Because no significant difference appearedbetween the myoelec t r ic param eters of the le f t and ther ight s ide , no fur ther d is t inc t ion was made. The mean ands tanda rd er ror of the mean (SEM) of the peak- to-p eak
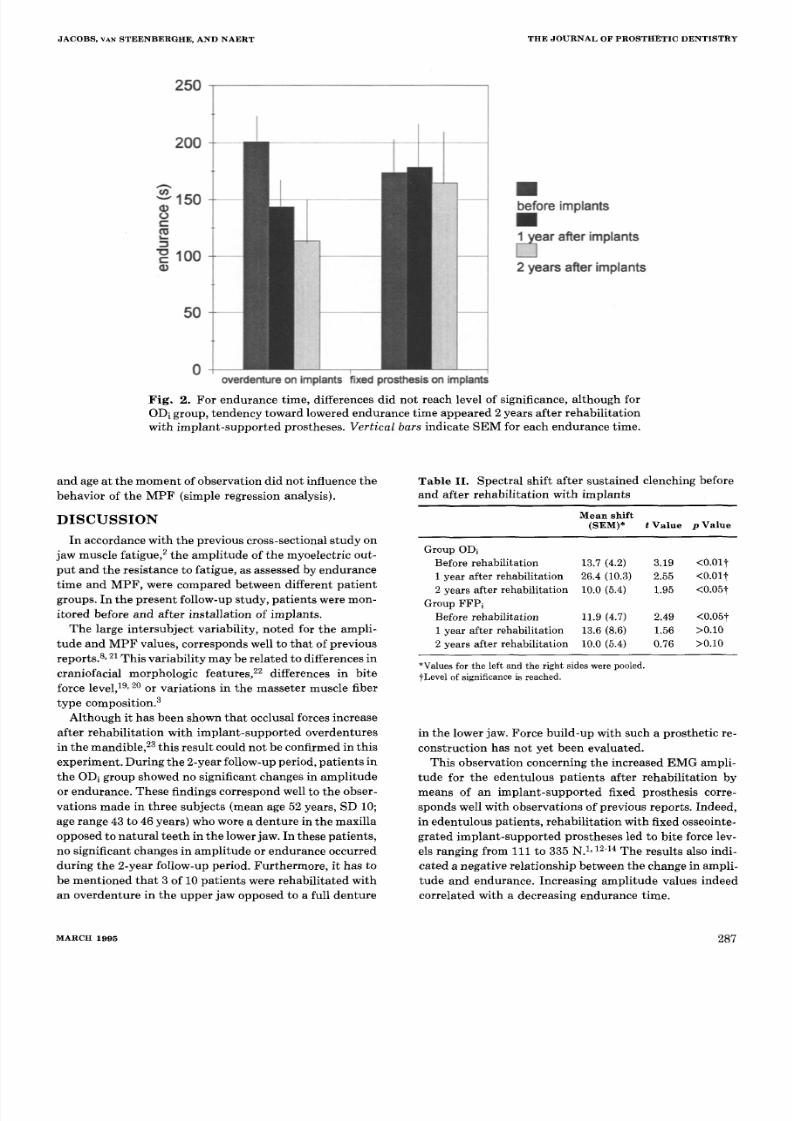
amp litud e at 50 % MV C is noted in Fig. 1. To create thisfigure, left and righ t side data were pooled. The end urancet ime before and af te r rehabi l i ta t ion wi th implants i s indi-
cated in Fig. 2. During the 2-year follow-up period, the ODigroup showed no s igni f icant changes in ampl i tude orendurance (s imul taneous pa i red t tes t s ) . Af ter rehabi l i ta -t ion with a f ixed prosthesis on implants, a significantincrease in signal amplitude was observed (p < 0.02, Bon-fer roni mul t ip le compar isons method) , whereas the endur-ance t ime did not change significantly.
When the re la t ionship be tween changes in ampl i tude ,endurance , and MPF af ter rehabi l i ta t ion wi th implant -supported prostheses was tested, a significant negative re-la t ionship appeared be tw een the change in ampl i tude andendu rance t im e (Pearson correlat ion tests , r -0.80). In-creas ing ampl i tude va lues indeed corre la ted wi th a de-creasing endurance t ime.
For the change in MPF dur ing sus ta ined c lenching,paired t tests indicated significant downw ard shifts in MP Fdur ing a sus ta ined c lenching effor t before and af te r reha-bi l i ta t ion wi th implan t -suppo r ted overdentures (Table I I ) .This sh i f t was a lso present for the o ther pa t ien ts before re-habi l i ta t ion wi th implan t -supp or ted fu ll f ixed prostheses .Howev er, after rehabil i ta t ion, su ch a significant shift couldno longer be observed (Table I I ) .
Regarding the re la t ionship be tween MPF shi f t and sub-jec t ive percept ion of fa t igue or pa in dur ing a sus ta inedclenching effort , no correlat io n could be established. I t alsoappeared t ha t the endurance t ime, the years of edentu l ism,
286 V O L U M E 7 3 N U M B E R 3
8/6/2019 Masseter Muscle Fatigue in Implant Supported Pros the Tics
http://slidepdf.com/reader/full/masseter-muscle-fatigue-in-implant-supported-pros-the-tics 4/6
J A C O B S , VAN S T E E N B E R G H E , A N D N A E RT T H E J O U R N A L O F P R O S T H E T I C D E N T I S T RY
250
200
(D"- " 15 000r -
= 1 0 00
50
0
Bbefore implants
e a r after implants
2 years after implants
overdenture on implants fixed prosthesis on implants
Fi g, 2. For endurance time, differences did not reach level of significance, although forODi group, tendency to ward lowered endurance time appeared 2 years after rehabilitationwith implant-supported prostheses. Vertical bars indicate SEM for each endurance time.
and age at the moment of observation did not influence thebehavior of the MPF (simple regression analysis).
D I S C U S S I O N
In accordance with the previous cross-sectional study onjaw muscle fatigue, 2 the amplitude of the myoelectric out-put and the resistance to fatigue, as assessed by endurancetime and MPF, were compared between different patientgroups. In the pr esent follow-up study, patients were mon-itored before and after installation of implants.
The large intersubject variability, noted for the ampli-tude and M PF values, corresponds well to that of previousreports.S, 21 This variabi lity may be r elated to differences incraniofacial morpho logic features, 22 differences in biteforce level, 19, 20 or va riat ions in the masseter muscle fibertype composition. 3
Although it has been shown that occlusal forces increaseafter rehabilitation with implant-supported overdenturesin the mandible , 23 this result could not be confirmed in thisexperiment. During t he 2-year follow-up period, patients inthe ODi group showed no significant changes in amplitudeor endurance. These findings correspond well to the obser-vations made in three subjects (mean age 52 years, SD 10;age range 43 to 46 years) who wore a dentur e in the maxillaopposed to natural teeth in the lower jaw. In these patients,no significant changes in amplitude or endurance occurredduring the 2-year follow-up period. Furthermore, it has tobe mentioned th at 3 of 10 patients were rehabilitated withan overdentur e in the up per jaw opposed to a full denture
Table I I. Spectral shift after sustained clenching beforeand after rehabilitation with implants
M e a n s h i f t
( S E M ) * t Va l u e p Va l u e
Group ODiBefore rehabilitation 13.7 (4.2) 3.19 <0.011 year after rehabilitation 26.4 (10.3) 2.55 <0.01t2 years after rehabilitation 10.0 (5.4) 1.95 <0.05#
Group FFPiBefore rehabilitation 11.9 (4.7) 2. 49 <0.05#1 year after rehabilitation 13.6 (8.6) 1.56 >0 .102 years after rehabilitation 10.0 (5.4) 0. 76 >0.10
*Va lues fo r t he l e f t and t he r i gh t s i d e s we re po o l ed .tLeve l o f s i g n i f i cance is r e ached .
in the lower jaw. Force build-up with such a prosthetic re-construction has not yet been evaluated.
This observation concerning the increased EMG ampli-tude for the edentulous patients after rehabilitation bymeans of an implant-supported fixed prosthesis corre-sponds well with observations of previous reports. Indeed,in edentulous patients, rehabilitation with fixed osseointe-grated impla nt-suppo rted prostheses led to bite force lev-els ranging f rom 111 to 335 N. 1,12-14 The results also indi-cated a negative relationship between the change in ampli-tude and endurance. Increasing amplitude values indeedcorrelated with a decreasing endurance time.
M A R C H 1 9 9 5 2 8 7

8/6/2019 Masseter Muscle Fatigue in Implant Supported Pros the Tics
http://slidepdf.com/reader/full/masseter-muscle-fatigue-in-implant-supported-pros-the-tics 5/6
T HE JOU RNA L OF PROSTHE TI C DE N T I S TRY JACOBS, VAN STEENBERGHE, AND NAERT
A n o t h e r a p p r o a c h t o e v a l u a t i n g m a s s e te r m u s c l e p e rf o r-m a n c e i s m o n i t o r i n g f a ti g u e p h e n o m e n a t h a t a p p e a r d u r -i n g s u s t a i n e d c l e n c h i n g e f f o r t s . D u r i n g s u s t a i n e d c l e n c h -i n g, a s i g n if i c a n t d o w n w a r d s h i f t o f t h e M P F p a r a m e t e ro c c u r r e d , w h i c h c a n b e r e l a t e d t o f a t i g u e . 7 ,1 0, 21 A f t e r r e h a -b i l i ta t i o n i n t h e i m p l a n t - s u p p o r t e d f ix e d p r o s t h e si s g r o u p ,
h o w e v e r , s u c h a s h i f t c o u ld n o t b e e s t a b l i s h e d . T h e l a t t e rf i n d i n g c o u ld e v e n t u a l l y b e r e l a t e d t o t h e l o w e r E M G l e v -e l s n o t i c e d d u r i n g s u b m a x i m a l c l e n c h in g . T h e f o r c e s d e -v e l o p e d a r e k n o w n t o b e lo w e r t h a n t h o s e t h a t o c c u r d u r -i n g c he w i n g , w h i c h p r o b a b l y e x p r e s s e s t h e f e a r o f c a u s i n gd a m a g e t o t h e i m p l a n t s o r t h e p r o s t h e t i c r e c o n s t r u c t i o nd u r i n g t h e e x p e r i m e n t a l c o n d i t i o n s . 24
I n t h i s s tu d y, t h e r e p o r t e d v a l u e s fo r e n d u r a n c e t i m ew e r e s o m e w h a t h i g h e r t h a n t h o s e r e p o r t e d f o r n a t u r a ld e n t i t i o n s , 25 b u t n o s i g n i f i c a n t d i f f e r e n c e i n e n d u r a n c et i m e c o u l d b e e s t a b l i s h e d b e t w e e n t h e p a t i e n t g r o u p s o rw i t h i n o n e g r o u p a f t e r r e h a b i l i t a t i o n w i t h i m p l a n t s . T h e
a c t u a l e x p e r i m e n t a l s e t u p , w h i c h i n v o l v e d r e g u l a r v e r b a le n c o u r a g e m e n t s , m a y h a v e e n h a n c e d t h e e n d u r a n c e t im e .I n a d d i t i o n , s o m e d i f f ic u l ti e s w e r e e n c o u n t e r e d i n m o t i v a t -i n g p a t i e n t s t o e x e r t r e a l m a x i m a l o u t p u t s . A f e a r o f f r a c -t u r e o f i m p l a n t s o r p r o s t h e s e s w a s s o m e t i m e s e x p r e s s e d .T h e e n d u r a n c e t i m e d u r i n g i s o m e t r i c c o n t r a c t i o n s i s r e -l a t e d t o t h e f i b e r t y p e c o m p o s i t i o n o f t h e m u s c l e . 26 L o w e rc l e n c h i n g f o r c e s i n v o lv e f a t i g u e - r e s i s t a n t t y p e I f i b e r s a n da r e a l s o a s s o c i a t e d w i t h a l o n g e n d u r a n c e t i m e s T h u s t h el o n g e r e n d u r a n c e t i m e o b s e r v e d i n t h i s s t u d y c o u l d a l so b ee x p l a i n e d b y t h e l o w e r c l e n c h i n g l e v e ls e x e r te d . T h e l i m -i t i n g f a c t o r t o t h e s u s t a i n e d c l e n c h i n g e f f o r t w a s s o m e w h a t
d i f f e r e n t b e t w e e n t h e p a t i e n t g r o u p s . B e fo r e r e h a b i l i t a t i o nw i t h i m p l a n t s , s o m e p a t i e n t s r e p o r t e d m u s c l e f a t i g u e( 1 0 % ) o r p a i n c a u s e d b y p r e s s u r e o f t h e d e n t u r e o n t h em u c o s a ( 2 0 % ) a s t h e l i m i t i n g f a c t o r s o f t h e i r c l e n c h i n g e f -f o r t . T h e o t h e r p a t i e n t s h a d n e i t h e r p a i n n o r f a t i g u e d u r -i n g c l en c h i n g . A f t e r r e h a b i l i t a t i o n , p a t i e n t s i n t h e O D ig r o u p d i d n o t p e r c e i v e g r e a t l y d i f f e r e n t s e n s a t i o n s : 6 0 %n o t e d n o p a i n , 2 0 % h a d m u s c l e fa t i g u e , a n d 2 0 % c o n t i n -u e d t o r e p o r t p r e s s u re o f t h e o p p o s i n g d e n t u r e o n t h e m u -c o s a. I n c o n t r a s t , p a t i e n t s i n t h e F F P i g r o u p r e p o r t e d m u s -
c l e f a t ig u e ( 4 2 .8 % ) o r fe a r o f c l e n c h i n g a n y f u r t h e r ( 2 8. 6 % )a s l i m i t i n g f a c to r s o f t h e s u s t a i n e d c l e n c h i n g e f fo r t . T h e
r e h a b i l i t a t io n o f e d e n t u l o u s p a t i e n t s b y m e a n s o f i m p l a n t -s u p p o r t e d f i x e d p r o s t h e s e s i n v o l v e s a n i m m e d i a t e l o a dt r a n s fe r t h r o u g h t h e i m p l a n t s t o t h e j aw b o n e i n s t e a d o f an e g a t i v e p e r i o d o n t a l f e e d b a c k , w h i c h i s a s s o c i a t e d w i t h i n -c r e a s e d b i t e f o r c e l e v el s c o m p a r e d w i t h t h o s e o f d e n t u r ew e a r e r s . I , 12-14 D u r i n g t h e s u s t a i n e d s u b m a x i m a l c l e n c h i n ge f f o rt , th e s e p a t i e n t s d e v e l o p l o w e r b i t e f o rc e s , e x p r e s s in gt h e i r f e a r o f c a u s i n g d a m a g e t o t h e i m p l a n t s o r t h ep r o s t h e t i c r e c o n s t r u c t i o n . 24 D e n t u r e s , o n t h e o t h e r h a n d ,a r e t i s s u e - s u p p o r t e d a n d d u r i n g s u s t a i n e d c l e n c h in g ac o m p r e s s i o n o f t h e s o f t t i s s u e s i s i n v o l v e d , w h i c h s t i m u -l a t e s th e p e r i o d o n t a l m e c h a n o r e c e p t o r s i n t h e g i n g i v a o fb o t h u p p e r a n d l o w e r j a w. T h u s i t m a y n o t b e s u r p r i s i n g
t h a t s e v e ra l p a t i e n t s w i t h a m a n d i b u l a r o v e r d e n t u r e o p -p o s i n g a f u l l d e n t u r e r e p o r t e d p a i n i n t h e a n t e r i o r m a x i l -l a r y r e g io n i n s t e a d o f m a s s e t e r m u s c l e p a i n .
C l i n ic a l ly , i t w a s o b s e r v e d t h a t a f t e r r e h a b i l i t a t i o n w i t hi m p l a n t - s u p p o r t e d o v e r d e n t u r e s n o r e a l c h a n g e s a p p e a r e di n t h e p a r a m e t e r s t h a t m o n i t o r e d m a s s e t e r m u s c le f a ti g ue .
O n t h e o t h e r h a n d , a f t e r r e h a b i l i t a t io n w i th i m p l a n t - s u p -p o r t e d f i x e d p r o s t h e s e s , p a t i e n t s e x h i b i t e d a n i n c r e a s e dE M G a m p l i t u d e d u r i n g a b r i e f c l e n c h i n g e f fo r t. N e v e r t h e -l e ss , d u r i n g s u s t a i n e d s u b m a x i m a l c l e n c h i n g , a s p e c t r a ls h i f t t h a t m o n i t o r e d f a t i g u e r e m a i n e d a b s e n t , w h i c h m i g h ti n d i c a t e t h e p a t i e n t s ' f e a r o f c l e n c h i n g t o o h a r d a n d f r ac -t u r i n g t h e p r o s t h e t i c r e c o n s t r u c t i o n .
C O N C L U S I O N S
T h e l i m i t e d s a m p l e s iz e d o e s n o t a l l o w o ne t o d r a w a n yd e f i n i t iv e c o n c lu s i o n s , b u t o b s e r v a t i o n s f r o m t h i s s t u d y a r ei m p o r t a n t w i t h r e g a r d t o m a s s e t e r m u s c l e b e h a v i o r a f t e r
r e h a b i l i t a t i o n w i t h i m p l a n t s .1 . S p e c t r a l a n a l y s i s o f f er s q u a n t i t a t i v e i n f o r m a t i o na b o u t m a s t i c a t o r y p e r f o r m a n c e o f p a t i e n t s r e h a b i l i t a t e d o rn o t r e h a b i l i t a t e d b y m e a n s o f o s s e o i n t e g r a t e d im p l a n t s .
2 . A f t e r r e h a b i l i t a t i o n w i t h i m p l a n t - s u p p o r t e d o v e r d e n -t u r e s n o r e a l c h a n g e s a p p e a r e d i n t h e p a r a m e t e r s t h a tm o n i t o r e d m a s s e t e r m u s c l e f a ti g u e . A s ig n i f i c an t d o w n -w a r d s h i f t o f t h e s p e c t r a l p a r a m e t e r s f o r p a t i e n t s w i t h a no v e r d e n t u r e o n i m p l a n t s w a s r e la t e d t o th e p h e n o m e n o n o ff a t i g u e .
3 . I n p a t i e n t s w i t h i m p l a n t - s u p p o r t e d f i x e d p r o s t h e s e sn o s u c h s h i f t o c c u r s , a n d t h e y e x p r e s s e d a f e a r o f p o s s i b l y
b i t i n g to o h a r d a n d f r a c t u r i n g t h e p r o s t h e t i c r e c o n s t r u c -t i o n .
R E F E R E N C E S
1. H araldson T, CarlssonGE. Bite forceand oral function n patients withosseointegrated oral im plants. Scand J Den t Res 1977;85:200-8.
2. Jacobs R, van Steenbergh eD. Ma sseter muscle atigueduring sustainedclenching n sub jects with completedentures, implant-supportedpros-these s, and n atura l teeth . J PROSTHETDENT 1993;69:305-13.
3. P erson RS, Kud ina LP. Cross-correlationof electromyograms howinginterference patterns. Electroencephalogr Clin Neurophysiol 1968;25:58-68.
4. L indstr6m L, Magn usson R, Peters6n I. Mu scular fatigue and actionpotential condu ction velocitychanges studied w ith frequency analysisof EM G signals. Electromyography1970;10:341-56.
5. Daw son MJ, G adian DG, Wilkie DR. Mus cular fatigue nvestigatedbyphosphorus nuclear mag netic resonance. Nature 1978;274:861-6.
6. Merletti R, Lo Conte LR, OrizioC. Indices of muscle atigue.J Electro-myo gr Kine siol 1991;1:20-33.
7. Palla S, Ash MM. Powe r spectral analysisof h e surfaceelectromyogramof h uman jaw muscles during fatigue. A rch Oral Biol 1981;26:547-53.
8. Duxbury AJ, Hughes DF, Clark DE. Pow er spectral distribution of themasseter electromyogram from surface electrodes. J Or al Rehabil1976;2:333-9.
9. Palla S, Ash MM . Effect of bite forceon the powerspectrum of the sur-face electromyogramof human jaw muscles.ArchO ral Bio11981;26:287-95.
10. Clark GT , Carter MC, Beemsterbo erPL. Analysisof electromyographicsignals n hum an jaw closingmusc les at v arious isometric orce levels.Arc h Oral B iol 1988;33:833-7.
11. HelkimoE, Carlsson GE, H elkimoM. Bite force and state o f dentition.Acta Odo ntol S can d 1977;35:297-303.
288 VOLUME 7 3 NUM B ER 3

8/6/2019 Masseter Muscle Fatigue in Implant Supported Pros the Tics
http://slidepdf.com/reader/full/masseter-muscle-fatigue-in-implant-supported-pros-the-tics 6/6
J A C O B S , VAN S T E E N B E R G H E , A N D N A E R T T H E J O U R N A L O F P R O S T H E T I C D E N T I S T R Y
12. Lind quis t LW, Carlsson GE. Changes in mast icato ry muscle functio n incomplete dent ure wea rers after i nserti on of bridges on osseointegratedimp lan ts in the lower jaw. Adv Biomaterials 1982;4:151-5.
13. Cart A, Laney WR. Maximu m occlusal force levels in patient s with os-seointegrated oral implant prost heses and pat ient s with complete den-tures. Int J Oral Maxillofac Implants 1987;2:101-8.
14. Falk H, Laurell L, Lundgr en D. Occlusal force patt ern in dentit ions withmandibular implant- supported fixed cantilever prostheses occluded
with complete den tures. I nt J Oral Maxillofac Im plan ts 1989;4:55-62.15. P etro JK , Hollande r AP, Bouma n LN. Ins tan tan eou s cardiac acceler-ation in man induced by a volun tary muscle contraction. J Appl Phys-iol 1970;29:794-8.
16. Beyron H. Occlusion: point of significance in plannin g restorative pro -cedures. J PROSTHET DENT 1973;30:641-52.
17. Tallgre n A, Holden S, Lang BR, Ash MM. Jaw mus cle activity in com-plet e den tur e wearers: a longitudinal electromyographic study. J PROS-THET DENT 1980;44:123-32.
18. Murr ay GM, Klineberg IJ. A standardiz ed sy stem for evoking reflexesin human jaw elevator muscles. J Oral Rehabil 1984;11:361-72.
19. van Steenber ghe D, De Vries JH, Hollan der AP. Resistance of aw-clos-ing muscles to fatigue duri ng repetitive maxima l voluntary clenchingefforts in man. Arch Oral Biol 1978;23:697-70L
20. Hagb erg C, Agerberg G, Hagberg M. Regression analysis o f electromyo-graphic activity of mastic atory muscles versus bite force. Scand J Den tRes 1985;93:396-402.
21. L indstr 6m L, Hellsing G. Massete r muscle fatigue in man objectivelyquantified by analysis ofmyoelectric signals. Arch Oral Bio11983;28:297-301.
22. M~tller E. The chewing appar atus: a n electromyographic study of theaction of mastication an d its correlation to facial morphology [Thesis,Univer sity of Copenhagen]. Acta Physiol Scan d 1966;69(Suppl):l-229.
23. Ha ralds on T, Jemt T, St/flblad P~,, Lekholm U. Oral functio n in sub-jects with overdentu res suppor ted by osseointegrated implants. Sca ndJ Dent Res 1988;96:235-42.
24. Hara ldson T, Ingervall B. Muscle functio n during chewing and swal-lowing in patien ts with osseointegrated oral impl ant bridges: an
electromyographic stud y. Acta Odontol Scand 1979;37:207-16.25. Lyons MF, Baxendale RH. A prelimi nary electromyographic study ofbite force and jaw-closing muscle fatigue in human subjects withadvanced too th wear. J Oral Rehabil 1990;17:311-8.
26. Petrof sky JS, Lind AR. Isometri c enduran ce in fast and slow musclesin the cat. Am J Physiol (Cell Physiol) 1979;236:C185-91.
27. Ringq uist M. A histochemical stud y of temporal muscle fibers in den-ture wearers and subjects with natural dentition. Scand J Dent Res1974;82:333-55.
Reprint requests to:DR. D. VAN STEENBERGHEDEPARTMENT OF PERIODONTOLOGYFACULTY OF MEDICINECATHOLIC UNIVERSITY OF LEUVENCAPUCIJNENVOER 73000 LEUVENBELGIUM
Av a i l a b i l i t y o f JO UR NA L B a c k I s s u e s
A s a s e rv i ce t o ou r subs c r i be r s , c o p i e s o f b a c k i s su e s o f THE JOURNAL O F PRO STHETICD E NT IS TRY f o r t h e p r e c e d i n g 5 y e a r s a r e m a i n t a i n e d a n d a r e a v a i l a b l e f o r p u r c h a s e f r o mt h e p u b l i s h e r , M o s b y, a t a c o s t o f $ 9 .0 0 p e r i s s u e . T h e f o l l o w i n g q u a n t i t y d i s c o u n t s a r ea v a i l a b l e : 2 5% o f f o n q u a n t i t i e s o f 12 t o 2 3, a n d o n e t h i r d o f f o n q u a n t i t i e s o f 24 o r m o r e .P l e a s e w r i t e t o M o s b y, S u b s c r i p t i o n S e r v i c e s , 11 8 3 0 We s t l i n e I n d u s t r i a l D r i v e , S t . L o u i s ,M O 6 3 146 -3318 , o r c a l l ( 800 )453 -4 351 o r ( 314 )45 3 - 4351 f o r i n f o r m a t io n o n ava i l a b i l i t y o fp a r t i c u l a r i s su e s . I f u n a v a i l a b l e f r o m t h e p u b l i s h e r , p h o t o c o p i e s o f c o m p l e t e i s s ue s a r ea v a i l a b l e f r o m U n i v e r s i t y M i c r o f i l m s I n t e r n a t i o n a l , 3 0 0 N . Z e e b R d . , A n n A r b o r , M I48106, (313)761-4700.
M A R C H 1 9 9 5 2 8 9