mapping interior environment and integrated health systems...
TRANSCRIPT
Mapping Interior Environment and
Integrated Health Systems Research
Using the Psychoneuroimmunological (PNI) Model
Mini Suresh BA, Dip.Int.Des
Principal Supervisor Associate Professor Dr. Jill Franz
Associate Supervisor
Dr. Dianne Smith
School of Design Faculty of Built Environment and Engineering
Queensland University of Technology
Submitted for:
Masters by Research February 2007

ii
Keywords
Interior environment, built environment, physical environment, design,
psychoneuroimmunology, health and wellbeing, mental wellbeing, physiological
wellbeing, integrative systems, person environment interrelationship, space, place.

iii
Abstract
This study maps research concerning person environment interrelationships with
health and wellbeing outcomes. The purpose of this study is to provide insights into
the inter-relationship between the built environment (BE) and human health and
wellbeing as it is conveyed in research literature. It particularly focuses on literature
that connects built environment, emotions, feelings, mind and body. This thesis
therefore provides a review of relevant literature on the physical environment, with a
focus on person environment (PE) relationship that may influence the person’s
psychological and physiological systems consequently affecting health and
wellbeing. Specifically, psychoneuroimmunology (PNI) is used to identify
dimensions of the BE which are significant for this study.
The understanding of PE interrelationships to health outcomes is achieved by
undertaking a transdisciplinary outlook. To conceptualise the ‘person’ as a whole and
the workings of the mind and human system PNI has been recognised as a main
platform. PNI is the study of mind-body relationships (Evans, et al, 2000), providing
a scientific framework which captures the understanding of the inter-relationship of
the mind to the neuroendocrine systems and the immune systems with the aim of
understanding the influence of the mind on eliciting as well as preventing illnesses.
The work was motivated by the need for better understanding of the human
interaction/transaction in an interior environment and their consequences on health.
An exploration of literature from both the environmental and health fields provided a
knowledge base upon which to develop an understanding of the interrelationship.
Research has demonstrated a link between the BE and wellbeing, however, this is
limited in its application and/or scope. For example, over the past years there has
been an increasing amount of research showing the possible influence of the
environment in reducing stress (Sommer & Oslen, 1980; Kaplan, 1983; O’Neill,
1991; Wapner & Demick, 2000; Parsons & Tassinary, 2002, Frumkin, 2006). In
addition, there is growing evidence that indicates there is a relationship between BE
and health including the psychological and physiological systems, in healthcare
environments (Ulrich & Zimring, 2004). However, while there is ample research in
the areas of environmental stressors and other determinants of the environment in

iv
contributing to health, less research has been undertaken in studying the impact of
the environment on health (Evans& McCoy, 1998). The potential of the environment
in contributing to the mental wellbeing of a person and how this could affect the
physical health therefore needs further investigation (Solomon, 1996).
The methodology followed was Coopers (1998) ‘research synthesis’ and the tool to
sort the domains and PE interrelationships was adapted from White’s (1989) ‘space
adjacency analysis’. The scope of this study was limited to explorations of literature
that inquired into PE relationships that fit into the primarily established ‘integrative
systems model’; a parameter that enabled categorisation of the literature into the
areas that related to the PNI framework.
The findings illustrate that the person is interrelated to the environment in several
ways and can be interpreted and explained in terms of various dimensions such as
the psychological, physical, social, and spatial dimensions. Furthermore,
empirical research indicates that the environment impacts on a person’s health and
wellbeing through psychological and physiological systems. PNI
acknowledges the interrelationship of the mind and body systems contributing to an
integrative systems model of human health and wellbeing.
As an outcome, the study has produced an analysis method and a navigation map of
the various literature domains related to PE interrelationships in terms of health and
wellbeing. This has been facilitated by the development of, a ‘PE integrative systems
model’. Apart from demonstrating the need for transdisciplinary research and
contributing to research methodology, the study also adds to the current design
knowledge base providing BE professionals and creators with a better understanding
of the health outcomes from PE interrelationships.

v
Table of Contents
Keywords…………………………………………………………………………ii Abstract…………………………………………………………………………..iii List of Tables …………………..………………………………………………..vii List of Figures…………………………………………………………………...viii Abbreviations……………………………………………………………………..ix Glossary………………………………………………………………………….. x Statement of Original Authorship……………………………………………..xiii Acknowledgements……………………………………………………………. .xiv
Chapter 1: Introduction...................................................................1
1.1 Background ................................................................................................... 1 1.2 Aims and objectives of the study .................................................................. 2 1.3 General approach of the study....................................................................... 5 1.4 Overview of the thesis................................................................................... 9 1.5 Conclusion .................................................................................................. 10
Chapter 2: Psychoneuroimmunology (PNI) ................................11
2.1 Introduction................................................................................................. 11 2.2 Defining PNI ............................................................................................... 14 2.3 Influence of the mind on physical health .................................................... 15 2.4 Summary ..................................................................................................... 19 Chapter 3: Methodology ...............................................................21
3.1 Introduction................................................................................................. 21 3.2 Establishing the context of the study .......................................................... 21 3.3 Overall mapping framework .......................................................................23 3.4 Methodological approach............................................................................ 26
3.4.1 Problem formulation ...........................................................27 3.4.2 Data collection ....................................................................28 3.4.3 Data evaluation....................................................................31 3.4.4 Data analysis and interpretation .........................................36 3.4.5 Presentation........................................................................42
3.5 Summary ..................................................................................................... 43 Chapter 4: Results .........................................................................44
4.1 Introduction................................................................................................. 44 4.2 PE inter-relationship.................................................................................... 47
4.2.1 The animate dimension ......................................................49 4.2.2 The inanimate dimension ...................................................51
4.3 The properties of place or space.................................................................. 52 4.4 Built Environment (BE) .............................................................................. 58

vi
Table of Contents (continued)
4.5 Results of review analysis........................................................................... 60
4.5.1 Consideration of integrated health ......................................60
4.6 Psychological dimensions of the PE relationship ....................................... 65
4.6.1 BE Research: Environmental psychology...........................70 4.6.2 BE Research: Design and architecture................................80 4.6.3 BE Research: Environmental health ..................................85 4.6.4 Health and medical research ..............................................85 4.6.5 Summary ............................................................................88
4.7 Physiological dimensions of the PE relationship........................................ 90
4.7.1 BE Research: Environmental psychology.........................95 4.7.2 BE Research: Design and architecture............................100 4.7.3 BE Research: Design and healthcare ...............................103 4.7.4 BE Research: Environmental health ...............................106 4.7.5 Health and medical research ...........................................107
4.8 The physical environment and integrated health and wellbeing.............. 108
4.8.1 Environmental psychology............................................110 4.8.2 Design and architecture.................................................115 4.8.3 Design and healthcare ...................................................117 4.8.4 Environmental health ....................................................119 4.8.5 Health and medical research .........................................121 4.8.6 Psychoneuroimmunology: PE interrelationships ..........122
4.9 Discussion of Implications of the review results .......................................... 132
4.9.1 Classification of the relationships linkages................... 133 4.9.2 Core recognized PE interrelationship ...........................135 4.9.3 Environmental factors emerging from the review ........138 4.10 Summary ...................................................................142
Chapter 5: Conclusion ................................................................143
5.1 Summary of study process .......................................................................144 5.2 Reflections on the research findings ......................................................... 146 5.3 Future recommendations........................................................................... 151
5.3.1 Application of current and future research (practice) .....152 5.3.2 Application of current and future research (education) ..153 5.3.3 Application of current and future research (research).....154
5.4 Conclusion ................................................................................................ 156
References ............................................................................................157
Appendices ...........................................................................................174

vii
List of Tables
Table 1 Method for classification of data into domains........................................ 24
Table 1.1 Classification of data into domains……………………………………...61
Table 2 Classification of PE relationships studies to health model ...................... 25
Table 3 Criteria for evaluation .............................................................................. 32
Table 4 Analysis pointers...................................................................................... 38
Table 5 Analysis levels ........................................................................................ 46
Table 6 Identified dimensions of PE + health and
well-being interrelationships.................................................................... 49
Table 7 Sensory modality and the absolute threshold ......................................... 93
Table 8 Personal and environmental factors in health and illness ...................... 112
Table 9 Design factors that affect health and well-being .................................. 116
Table 10 PNI domain and physical environmental considerations...................... 127
Table 11 Environmental dimensions relating
to human response and outcomes.......................................................... 139
Table 12 Information processing and outcomes model ....................................... 146
Table 1(a) Classification of data into domains P&E................................................. 65
Table 1(b) Classification of data into domain N&E and I&E................................... 90
Table 1(c) Classification of data into domain Integrated & E ................................ 108
Table 1(d) Classification of data into domain PNI&E............................................ 122
viii
List of Figures
Figure 1 Model for PE relationship to integrative health and well-being............... 6
Figure 2 Categorisation of BE and Design ............................................................. 7
Figure 3 Categorisation of PNI ............................................................................... 7
Figure 4 PNI Model ........................................................................................... 12
Figure 5 PNI process and health outcomes.......................................................... 13
Figure 6 PE Integrated Health Systems Model ....................................................22
Figure 7 Data matching........................................................................................ 39
Figure 8 Matrix 1 & 2 interrelationship tool……………………………….........41
Figure 9 Graphical representation of data found in the literature survey ............ 64
Figure 10 BE + Psychological systems interrelationship...................................... 66
Figure 11 Psychological dimension relevant to health and well-being.................. 89
Figure 12 BE + Physiological systems interrelationship ....................................... 91
Figure 13 BE + Integrated systems interrelationship........................................... 109
Figure 14 Personal characteristics influencing
environmental impact on the physiological system. ............................ 121
Figure 15 Sample relationships............................................................................ 133
Figure 16 PE Integrative Systems Flow Model: Health and well-being
outcomes from PE interrelationship………………………… ………..136

ix
List of Abbreviations P Person
E Environment
BE Built Environment
PE Person Environment
PNI Psychoneuroimmunology

x
Glossary
Built environment: is everything built without naturally being there in the first
place. “It encompasses all buildings, spaces and products that are created, or
modified, by people. It includes homes, schools, workplaces, parks/recreation areas,
greenways, business areas and transportation systems. It extends overhead in the
form of electric transmission lines, underground in the form of waste disposal sites
and subway trains, and across the country in the form of highways. It includes land-
use planning and policies that impact our communities in urban, rural and suburban
areas” (www.nih.gov, n.d.).
Person environment (PE) relationships: The relationship that the person (P) forms
with the environment (E) through interactions and transactions. “The built E is
physical, of particular materials and of particular appearance or style. We exist in
relationship with the physical E and with non-human and human entities” (Smith,
2000, p.287).
Person environment (PE) interrelationships: The relationships that the person as a
whole forms through the interactions and transactions with the environment in its
entirety. This interrelationship may affect the person on the whole mind-body
systems knowingly or unknowingly. This has been developed from the integrative
approach consisting of Person, Built Environment and health and wellbeing.
Environmental health: “The study of the influence of physical, biological,
chemical, and psychosocial factors on human health. Environmental health is
concerned with the influence of natural factors (e.g., climate), as well as those of
human origin (e.g., noise, the built environment). The field is broad and draws upon
research in many disciplines, such as molecular biology, toxicology, clinical
medicine, population genetics, epidemiology and public health. An emerging area of
importance is the application of genomics techniques to study gene-environment
interactions” (NIH, 2003, n.d.)

xi
Psychoneuroimmunology: The study of mind - body relationships. The
psychological system is interrelated to the neuroendocrine and immune systems, thus
influencing the physiological systems whenever the psychological system is
disrupted (Schedlowski & Tewes, 1996).
Psychological system: The system related to the brain and mind.
Physiological system: For this study it is related to the central nervous system,
endocrine system and the immune system of the body.
Nervous system: The nervous system can be called the controller of our responses.
“It receives information from the different sensory organs and then integrates them to
determine the responses to be made by the body (Guyton, 2000, p.512).
The nervous system consists of the “sensory input portion, the central nervous
system, and the motor output portion. The sensory receptors detect the state of the
body or the state of the surrounding” (Guyton, 2000, p.4). The central nervous
system (CNS) consists of the brain and the spinal cord. “The brain can store
information, generate thoughts, create ambition, and determine reactions that the
body performs in response to the sensations” (Guyton, 2000, p.4). The motor output
portion takes care of sending out “appropriate signals of the nervous system to carry
out one’s desires” (p.4). A large part of this is called ‘the autonomous nervous
system’ (ANS) as it operates on a subconscious level and controls many functions of
the internal organs (Guyton, 2000).
The endocrine system: The system “in which glands or specialized cells release into
the circulating blood, chemicals (hormones) that influence the functions of cells at
another location in the body” ( Guyton, 2000, p.836). In other words they
communicate with various part of the body through chemicals called the hormones.
The endocrine system which “regulates the metabolic functions of the body like
hormonal functions complements the nervous system which regulates mainly the
muscular and secretory activities of the body” (Guyton, 2000, p.836). “The
neuroendocrine system is the system in which neurons secrete substances

xii
(neurohormones) that reach the circulating blood and influence the functions of cells
at another location in the body” (Guyton, 2000, p.836).
Immune system: Immunity means “the state of being protected against a specific
disease” (Cohen, 2004, p.221). Our body protects us against alien matters. Some of
these defence mechanisms are non-specific and protects against any foreign intruders
such as “unbroken skin, bactericidal body secretions, reflexes such as coughing,
sneezing” (p.217) and so on. But specific attacks are carried out on diseased
organisms (Cohen, 2004). The immune system is able to differentiate between the
friend and the enemy and fights the adversary when necessary to protect the body
(Guyton, 2000).
Adrenaline/ Epinephrine: Epinephrine or more commonly known as adrenaline is a
“…a powerful stimulant produced by the adrenal gland and sympathetic nervous
system… activates the cardiovascular, respiratory, and other systems needed to meet
stress” (Cohen, 2004, p.231). These hormones are produced by the adrenal glands,
which produces several important hormones in response to emergencies and stress.
Though the nervous system also produces epinephrine and norepinephrine, they have
less acting time than those produced by the endocrine system (Guyton, 2000)
Sensory system: This “is our network for detecting stimuli from the internal and
external environments” (Guyton, 2000, p.501). The sensory systems controlled by
complex sensory organs that form the eye, ear, nose, tongue, and skin are vision,
hearing, olfactory senses, taste and tactile sense.

xiii
Statement of Original Authorship
1
2
3
4
5
6
7
8
9
10
11
“The work contained in this thesis has not been previously submitted for a degree or diploma at any other higher education institution. To the best of my knowledge and belief, the thesis contains no material previously published or written by another person except where due reference is made.”
Signature Date
xiv
12 Acknowledgements
First and foremost I would like to sincerely thank my principal supervisor, Associate
Prof. Dr. Jill Franz and my associate supervisor Senior Lecturer Dr. Dianne Smith.
Thank you Jill for enabling me to undertake this research, for encouraging me
through the process, guiding me and for the detailed feedback on my numerous
drafts. Thank you also for listening to my woes through this exciting journey and for
your advice, academic and personal. Thank you Dianne for being so adept at
unscrambling and consolidating my thoughts. Thank you also for your
encouragement and valuable feedback and encouragement on my draft thesis. I am
grateful to Dr. Renata Meuter (Senior Lecturer, The School of Psychology and
Counselling) for her valuable advice and feedback on psychoneuroimmunology.
There are various people who have supported and provided me with encouragement
through this process. I am grateful to QUT for the scholarship support during the
final stage of this project, especially Prof. Mahen Mahendran; Prof. Vesna Popovic,
for providing me with assistance; Dr. Anoma Kumarasuriyar for always willing to
cheer me up and keeping your door open to run for advice; Kellie Hinchy and Chris
Cook for always lending an ear to any student or technical problems. Thank you also
to my friends and colleagues in the Faculty of Built Environment and Engineering
for always being ready to help and keeping up the humour. I would especially like to
thank Rebekah Davis for stepping in during the last stage, helping and pushing me
on.
Finally, I owe a huge debt of gratitude to my family for their tolerance, support,
humour and encouragement throughout this journey. To Suri, my husband for always
giving my dreams colour and life, and for running this race with me. Thank you also
for shouldering many of my responsibilities without question. To my little ones,
Unni and Ammu who have always inspired me and always been a source of
encouragement to do my best. Thank you for patiently listening to my loud readings
and smilingly saying “great work…but we didn’t understand anything”. I love you
and I could not have done this with out the three of you…

1
Chapter 1
Introduction
1.1 Background
According to Rapoport (1990), the human body and the natural/built
environment (BE) are closely connected with each other by the simple fact
that a person is always in one place or the other, be it in natural settings or
human-made settings, and the human body reacts to a place consciously and
subconsciously all the time. Furthermore, the fact that people are
psychologically dependent on their social and physical surroundings for
their individual development and well-being is well-known (Ittelson, 1976).
Our physiological system and psychological system are not “separate and
distinct from our experiences in life” (Ray 2004, p.29).
Therefore physical environments and a person’s health are interconnected.
The “health promotiveness” of an environment “ultimately depends on its
capacity to support those health outcomes most desirable and important to
its members while eliminating or ameliorating those most clearly negative
and detrimental to individual and social well-being” (Stokols et al., 2003,
p.139 ). Studies on the properties of restorative environments in promoting
well-being (for example, Kaplan, 1995) indicate that the environment is
closely connected to the human being in terms of health and well-being. In
one of his early studies, Roger Ulrich (1984) – one of the pioneers in
promoting the concept that physical environments influence physiological
systems in relation to healthcare environments – found that the length of
stay in hospitals can be reduced by providing better physical surroundings.
This suggests that mental well-being is necessary for the physiological well-
being of a person and that the built environment (BE) may be responsible in
several ways. Most recently, Ulrich and colleagues (2004) undertook an
extensive literature review of the role of the physical environment in
hospital settings and found that many properties of the built environment

2
play a role in facilitating or weakening human response to illness, thus
promoting or harming health and well-being.
1.2 Aims and objectives of the study
As the previous references show, many properties of the built environment
are understood to have the potential to influence the health of a person
through the psychological and the physiological systems of the human body.
The purpose of this study is to map research literature to identify the various
ways in which the relationship between health and environment has been
considered in BE research. While the research highlighted in the previous
section implies to a holistic understanding of human health and well-being
and a relationship between this and the environment is required, it is not
always clear as to the extent or specific nature of this or to how the notions
of health, well-being, and environment are integrated and conceptualised.
In this investigation, ‘integrated health’ refers to the transactions between
the mental state and physical state resulting in either positive or negative
well-being. In the health context, this does not simply mean the absence of
illness. ‘Health’ according to the Constitution of World Health Organisation
(WHO) is defined as:
A state of complete physical, social and mental wellbeing, and not
merely the absence of disease or infirmity (WHO, 2001, p.6).
Integrative health for the purpose of this study is the embodiment of the
overall health systems of a person that contribute to health and well-being1
and to the outcome of illnessess. Therefore health and wellbeing is framed
in this study through the application of the psychoneuroimmunological
(PNI) concept which relates health and wellbeing to the psychological and
1 For this study, health and wellbeing (or human wellness) is understood in accordance with the psychoneuroimmunological model, that is, as the outcome of the psychological system influencing the physiological system.

3
physiological systems of the human body and their interaction. In addition,
the ‘environment’ refers here to the built environment, that is, everything
built without naturally being there in the first place.
Using an integrative approach, people and environments cannot be viewed
in isolation. The different aspects of the environment cannot be separated
from one another as they interact and transact within themselves, eliciting
different reactions from the person as s/he experiences place. In other
words, they cannot be “defined independent of the other” (Ittleson 1976,
p.56). Support for a more holistic understanding of environment continues
today as conveyed in a published report from Canada which states that:
“While considerable attention has been paid to the public-health-related
impact of air pollution, relatively little research has been done to understand
how other aspects of the built environment impact health” (The Medical
Letter, CDC & FDA, 2005, p.140).
Impetus for an integrated appreciation of health and environment is also
reflected in the emergence of a new area of personal experience, knowledge,
professional practice and research (Brown, 1996) labelled ‘environmental
health’. However, as Frumkin (2006) asserts, there is yet to be a developed
understanding of it. The National Environmental Health Strategy of
Australia defines the practice of environmental health as “ …covering the
assessment, correction, control and prevention of environmental factors that
can adversely affect health, as well as the enhancement of those aspects of
the environment that can improve human health” (1999, p. ?).
For interior designers, the way in which people interact with the
environment and vice versa is of personal concern. As Abercrombie (1990)
proposes, the designer should:
be attuned to that person’s tastes, habits, mental sensibilities, and
psychological susceptibilities…the designer must not forget the more
obvious fact that the person also has a body...our body is also the key
instrument in the art form of interior design…this three - dimensional
bulk, with all its weight, its size, its heat, its sensing devices, its

4
peculiar ways of moving and ways of folding, is ever- present when
an interior is being used, it is not only a shell enclosing mental
processes; the body is also a major physical reference by which those
mental processes judge their surroundings (p.164).
In recognition of the above, the motivation driving this study is to establish
whether researchers have made any concerted effort to recognise health
holistically, that is, to understand how various systems of the human body
are interrelated and how the well-being of a person as a whole is considered
in relation to the built environment and the various elements of which it is
comprised. There are also reasons beyond immediate interest for
undertaking such a study. Firstly, the increasingly complex and global
health impacts which we currently face demand a much broader knowledge
and skills base (Frumkin, 2005). Secondly, this can only be achieved
through collaborative partnerships that harness the combined knowledge
and skills of a wide range of professional networks with an interdisciplinary
and holistic approach to human health and the capability of the built
environment (Canter, 1982).
As we know, significant progress has been made in increasing life
expectancy. For the majority of individuals living in developed countries,
life expectancy has increased considerably, with the aging population
believed to exceed the younger population by 32% by 2050 in developed
countries (UN Press release, 2005). Australia expects an increase of 26% -
38% by 2051 (Australian Bureau of Statistics, 2005). This shows the
potential of science in fighting illnesses and diseases and providing cures
(Jasmin, 2000). The improvement in life expectancy is also the result of
better and improved healthcare facilities (Lundberg, 1998). In addition, a
concern for quality of life is mounting rapidly. People are more aware than
before of keeping healthy and achieving and maintaining quality of life
(QOL) for themselves and for those depending on them.
Two factors, then, appear to contribute to these outcomes regarding life
expectancy: (1) personal awareness of physical fitness, nutrition and the

5
importance of leading a healthy lifestyle and, (2) the provision of better
social and physical conditions, workplace health and safety measures,
healthy residential management support, ergonomics, air quality, aesthetics
(see Butler & Jasmin, 2000). In terms of the latter, however, little attention
appears to be given to environments providing people with better holistic
health and well-being by means of improved mental and/or emotional
wellbeing. This may be because some relationships with the built
environment and contribution towards certain illnesses are difficult to
ascertain (Hodgson, 2002).
Reviewing medical literature to develop an understanding of health and
well-being and the physical environment revealed very little research that
looked at the various systems of the body as an integrated entity. While
there is considerable research, for example, in relation to environmental
stressors and certain determinants of the environment (Sommer & Oslen,
1980; Kaplan, 1983; O’Neill, 1991; Wapner & Demick, 2000; Parsons &
Tassinary, 2002), there is less research carried out in studying the impact of
the environment on health in an integrative way (McCoy & Evans, 1998).
As noted by Solomon (1996), the potential of the environment in
contributing to the mental wellbeing of a person and how this could affect or
be related to physical/biological health, needs further investigation.
1.3 General approach of the study
One area of medical research that represents an attempt to understand
psychological and physiological systems as an integrated whole is
psychoneuroimmunology (PNI). PNI is the study of mind-body
relationships (Evans et al., 2000), considering the inter-relationship of the
mind to the neuroendocrine system and the immune system. It looks at all
the aspects of the human-body systems and their influence on each other.
In this study, which aims to map research literature dealing with health,
well-being, and environment from a designer’s perspective, PNI is used as a
6
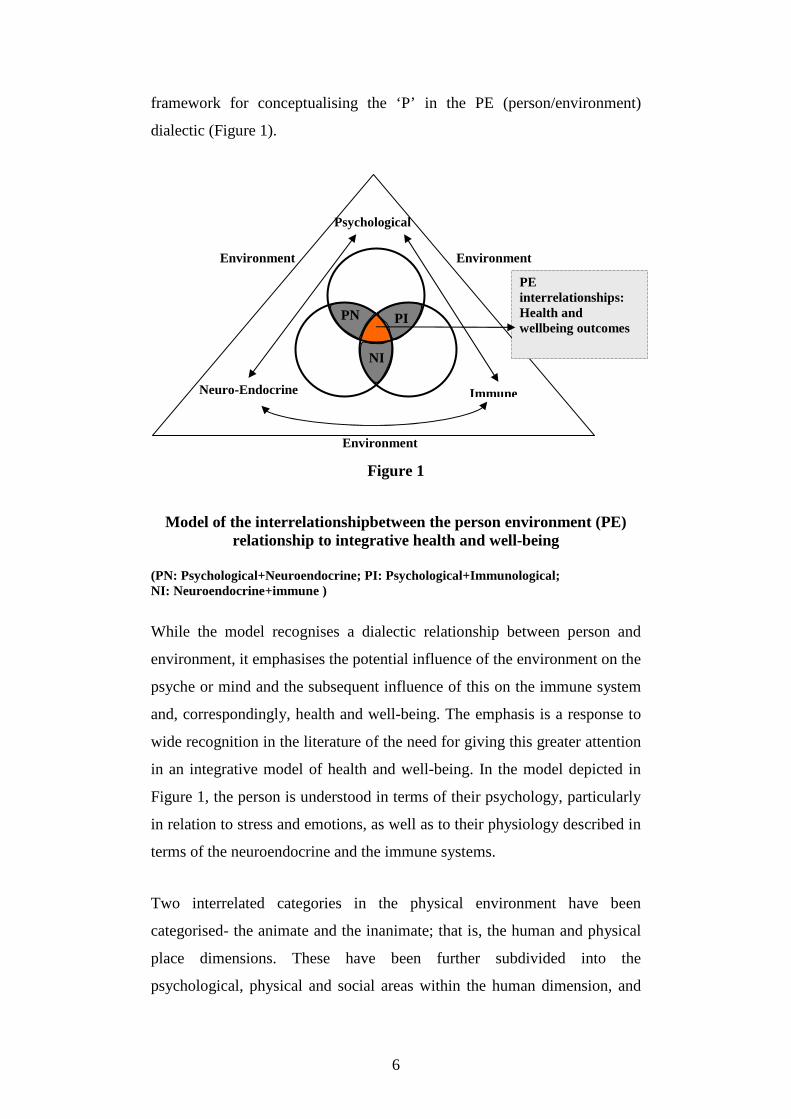
framework for conceptualising the ‘P’ in the PE (person/environment)
dialectic (Figure 1).
Figure 1
Model of the interrelationshipbetween the person environment (PE) relationship to integrative health and well-being
(PN: Psychological+Neuroendocrine; PI: Psychological+Immunological; NI: Neuroendocrine+immune )
While the model recognises a dialectic relationship between person and
environment, it emphasises the potential influence of the environment on the
psyche or mind and the subsequent influence of this on the immune system
and, correspondingly, health and well-being. The emphasis is a response to
wide recognition in the literature of the need for giving this greater attention
in an integrative model of health and well-being. In the model depicted in
Figure 1, the person is understood in terms of their psychology, particularly
in relation to stress and emotions, as well as to their physiology described in
terms of the neuroendocrine and the immune systems.
Two interrelated categories in the physical environment have been
categorised- the animate and the inanimate; that is, the human and physical
place dimensions. These have been further subdivided into the
psychological, physical and social areas within the human dimension, and
Environment
Environment
PE interrelationships: Health and wellbeing outcomes
PN
NI
PI
Environment
Psychological
Immune Neuro-Endocrine

7
Psychoneuroimmunology
Psychological
Physiological
Stress Emotions Neuroendocrine Immune
BE
Animate/ human
Inanimate/ Physical
Psychological Physical Social Elemental Spatial
elemental and spatial areas within the physical place dimension. This is
depicted in Figure 2.
Figure 2
Categorisation of Built Environment (BE)
PNI research has been categorised in terms of the psychological and the
physiological systems. In accordance with the PNI model, in this research
psychological has been subdivided into stress, emotions and psychological
well-being and the physiological systems into the neuroendocrine and the
immune systems as represented in Figure.3.
Figure 3 Categorisation of Psychoneuroimmunology (PNI)
The categorisation helps to identify specific features that establishes the
boundaries for the literature review and analysis. Th classification helps in
exploring only the direct areas that concern person environment
relationships that influence health and wellbeing outcomes. In general, the
study is directed by addressing several questions associated with the main
goal of mapping research of relevance to designers in order to develop a
more comprehensive understanding of the relationship between built
environment and holistic health and well-being. These are:

8
1) In what ways have health, environment, and their interrelationship been
conceptualised by researchers from a built environmental-design
perspective?
2) In what ways have health, environment and their interrelationship been
conceptualised by researchers from a medical-health perspective?
3) What research specifically addresses the relationship between the
physical environment and the mind? What are the implications of this
for the immune system and general health and well-being? What is the
nature of this research?
To organise the critique and map the research, the study used an adaptation
of Cooper’s (1998) method of synthesising literature and White’s (1986)
Space Adjacency Analysis technique. These are described in detail in a
following section of the thesis. Unlike many theses which include a
literature review of research contextually related to the study in question,
other than a brief literature review presented in this section, this thesis does
not. Rather, the literature comprises the data of this study, providing the
challenge and opportunity of examining the nature of the reviewing process
in order to achieve a methodologically rigorous outcome. Specific attention
was given to how the literature was critiqued as well as to how it was
presented, in order to best highlight the aspects of the PE relationship within
the integrative health and environment frameworks that were given
emphasis in the research.
Produced as a matrix, the mapping process reveals where the majority of
research has been focussed, in the process identifying potential areas for
future research. In addition, the matrix helps organise the research
undertaken, enabling designers to navigate their way through the
information. It invites designers to develop a more extensive awareness of
how the environment relates to the health of individuals, conveying in the
process the various areas of research where they can source relevant
information.

9
1.4 Overview of the thesis
In Chapter One of the study, the study’s aims and objectives are presented
against the background of research and call for a more integrated
appreciation of the person and health, the environment and their
interrelationship. The chapter also gives a brief description of the approach
adopted by the study as well as an overview of the structure of the thesis.
Chapter Two briefly explores psychoneuroimmunology (PNI) and seeks to
describe the interrelationship of the mind or the psychological systems to
the body systems or physiological systems.
Chapter Three explains the approach of the study, giving specific emphasis
to how the literature data are analysed, organised and presented to best
highlight the qualities of the research undertaken and the interrelationship of
the studies comprising the research.
Using the PNI/holistic health framework, Chapter Four examines theoretical
and empirical research undertaken in the general area of health and
medicine as well as research undertaken in the area of design and the built
environment. The outcome is a multifaceted picture of research highlighting
an array of PE and integrative health dimensions. This chapter is divided
into specific sections which identify categories related to human
psychological and physiological responses to person environment
relationships. They are further divided into sections in each of the categories
which look at different domains of built environment and health literature.
The implications of the picture of research presented in Chapter Four are
then explored and discussed in Chapter Five. Further research possibilities
are suggested, along with opportunities for interdisciplinarity,
multidisciplinarity, and transdisciplinarity. This chapter is also an
opportunity to reflect on the patterns of person environment inter/transaction
and the potential for the design of the built environment to more positively
engage with a person’s mental and emotional state, their physical health and
10
their well-being generally. It returns to the original research question and
reflects on the extent to which the capacity of the BE as a catalyst for health
and well-being is recognised in past and current research. Lastly, this
chapter also provides a brief conclusion to the thesis, summarising the
previous chapters. In the process it reiterates the main questions of the
thesis, the findings in relation to the questions and their implications for
future research and design practice.
1.5 Conclusion
Much of the literature on the relationship involving environment, health,
and wellbeing has focused on the role of the psychological systems or
physiological systems. The roles of the mind as a parameter in affecting the
physiological systems, and of the environment as a determinant or influence
are not well documented. This study attempts to document such research, in
addition to research that draws a relationship between various facets of the
person and the environment in the general context of holistic health and
well-being.
Although methods and theories used by researchers vary from study to
study, all agree that PE interaction is an inevitable part of human existence
and that the relationship between person and the environment has many
facets which – though they may be interpreted in different ways – are
overlapping and inter-connecting when person and environment are
conceptualised in an integrated sense. The following chapter describes the
approach taken in the study to analyse, organise and represent as a
meaningful whole, the work of these researchers.
11
Chapter 2
Psychoneuroimmunology (PNI)
(The Mind- Body Connection)
2.1 Introduction
As highlighted in the previous chapter, psychoneuroimmunology (PNI) is
central to this thesis and to its aim in the mapping of research that explores
the relationship between the built environment and the body’s health system
from an integrative perspective. In this chapter PNI will be explained in
some depth because it forms the basis of the framework or platform upon
which the methodology was developed. As an example of an integrative
systems model, it also enables the construct of the person (P) to be
understood more deeply and purposefully. In addition, it informed the
development of the model which emerged from this study and is described
in Chapter Four (see section.4.9.2/ Figure 16).
PNI is a field of science linking the psychological system to the
neuroendocrine and the immunological systems2 of the body. Its basic tenet
is that a person’s immunological response is affected by their psychological
wellbeing. If one’s psychological/emotional health is depressed, the
physical body could be more susceptible to illnesses. Accordingly, the
interactions between the psychological systems, the central nervous system
(CNS) and the neuro and endocrine systems are included as they also are
understood to affect the immunological systems of the body.
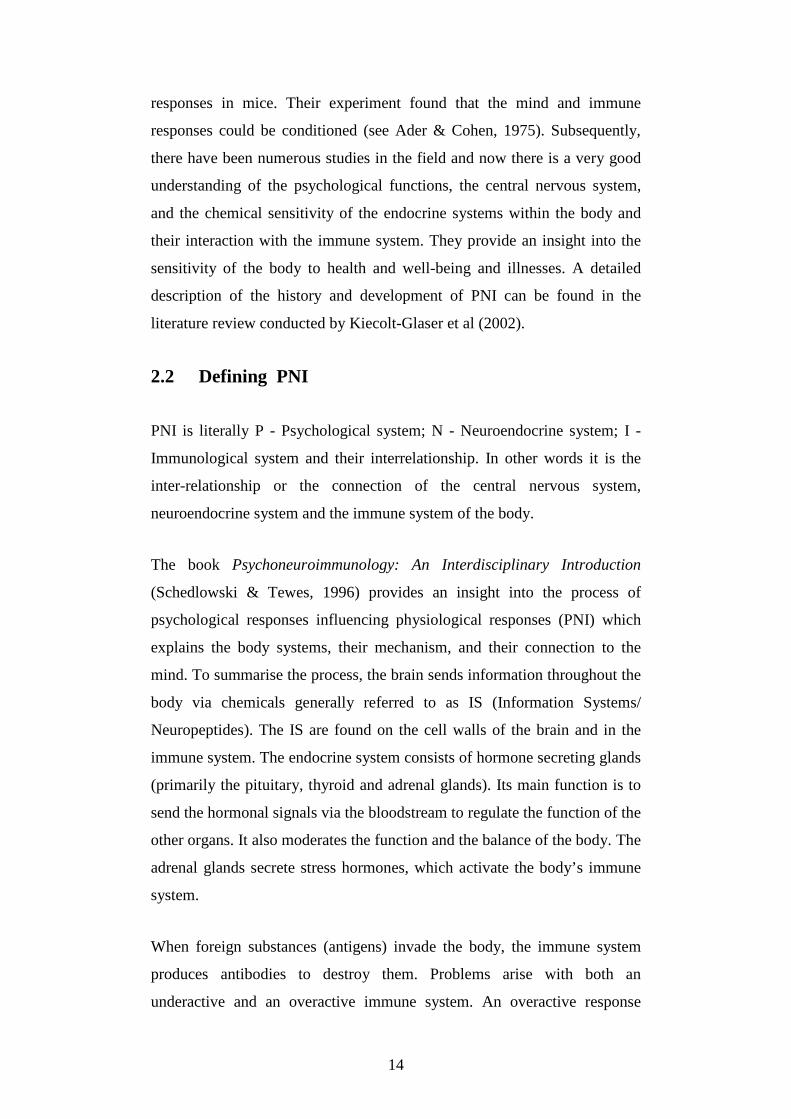
An increasing number of studies have documented the connection between
mind and the body (Figure 4) (Cousins, 1983; Ader et al., 1991; Hafen,
1996; Smith, 1998). For example, Evans et al. (2000) refers to a study
2 Definitions of key medical terms used in this chapter are provided in the glossary section at the end of this chapter.

12
conducted by Marucha et al (1998) on wound healing which compared
students healing time during vacation time versus examination time when
they were under duress. It was found that healing took 40% longer in
students when they were stressed during exam times.
Figure 4
PNI Model
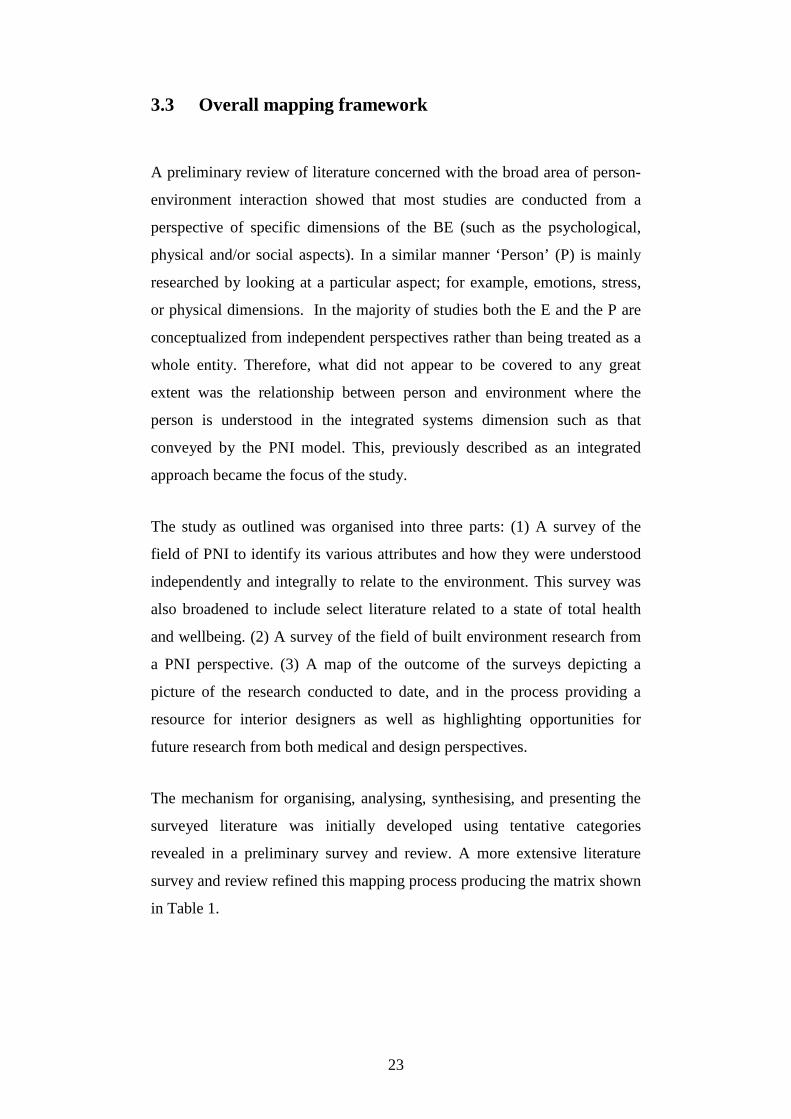
The process by which psychological, neuroendocrine and immune systems
are interconnected is believed to occur as follows (Figure 5). The central
nervous system (CNS), the neuroendocrine system and the immune system
of the body are linked to the mind through the chemical responses
associated with our emotions (positive or negative). For instance, the
experiences of stress can result in the production of an excess amount of
epinephrine (adrenaline), causing a chemical breakdown and resulting in
the internal weakening of the immune system, and an increased potential for
disease (Schedlowski & Tewes, 1996).
Neuroendocrine System
Immunological System
Psychological system
Affects overall health systems resulting in possible illness

13
Figure 5 PNI process and health outcomes
The study of the power of the mind on the body (or the physiological
systems) goes back more than forty years3 when Solomon and Moos (1964)
described how personality disorders affect the body. They brought to the
forefront the role of emotions in the pathogenesis of physical disease
associated with immunological dysfunction. Their paper on emotions,
immunity and disease dealt with evidence gathered through various studies
on different illnesses from arthritis to cancer. They cite the work of Leshan
and Worthington (1956, as cited in Solomon & Moos, 1964) who reported
that cancer could be caused by various factors including emotional factors
dealing with the loss of an important relationship and the suppression of
hostile feelings. They also speculated that there might be a relationship
between personality disorders and immune functions and suggested a
possible link between stress, emotions, immunological dysfunction and
mental state on one hand, and physical disease on the other.
Years later, the link between mind and physiological responses was
established by Ader and Cohen (1975) in their study of conditioned 3 The relationship between emotions and illness existed long before. This is the only study cited in this thesis that has been published before 1975-2006. The paper was considered significantly important to mention as it relates to the origin of PNI.
Emotions/ Psychological response produce an excess amount
of epinephrine
causes a chemical breakdown
results in internal weakening
increased potential for disease
central nervous system
neuro endocrine system
immune system
14
responses in mice. Their experiment found that the mind and immune
responses could be conditioned (see Ader & Cohen, 1975). Subsequently,
there have been numerous studies in the field and now there is a very good
understanding of the psychological functions, the central nervous system,
and the chemical sensitivity of the endocrine systems within the body and
their interaction with the immune system. They provide an insight into the
sensitivity of the body to health and well-being and illnesses. A detailed
description of the history and development of PNI can be found in the
literature review conducted by Kiecolt-Glaser et al (2002).
2.2 Defining PNI
PNI is literally P - Psychological system; N - Neuroendocrine system; I -
Immunological system and their interrelationship. In other words it is the
inter-relationship or the connection of the central nervous system,
neuroendocrine system and the immune system of the body.
The book Psychoneuroimmunology: An Interdisciplinary Introduction
(Schedlowski & Tewes, 1996) provides an insight into the process of
psychological responses influencing physiological responses (PNI) which
explains the body systems, their mechanism, and their connection to the
mind. To summarise the process, the brain sends information throughout the
body via chemicals generally referred to as IS (Information Systems/
Neuropeptides). The IS are found on the cell walls of the brain and in the
immune system. The endocrine system consists of hormone secreting glands
(primarily the pituitary, thyroid and adrenal glands). Its main function is to
send the hormonal signals via the bloodstream to regulate the function of the
other organs. It also moderates the function and the balance of the body. The
adrenal glands secrete stress hormones, which activate the body’s immune
system.
When foreign substances (antigens) invade the body, the immune system
produces antibodies to destroy them. Problems arise with both an
underactive and an overactive immune system. An overactive response

15
(autoimmune reaction) results when the immune system incorrectly
identifies part of the body as an enemy and attacks it. The immune cells or
lymphocytes (white blood cells) are produced in the long bones. Some of
these cells (stem cells) migrate to the thymus and multiply to T-Cells. The
thymus educates the T lymphocytes (or T Cells) to distinguish between self
and foreign proteins. To do so they either turn into T-Helper cells (CD4+)
that recognise antigens presented by MHC class 2+ and class 1+ cells and
thus lead to positive selection, or into cytotoxic T lymphocytes (CD8+) that
control the strength of the response and thus avoiding a negative selection.
Those lymphocytes remaining in the bone marrow mature to become B –
Cells. B-Cells ensure that the cells reacting against foreign antigens (for
example, toxins or viruses) survive and those reacting against self antigens
die. Some cells leave the thymus to circulate the body and protect the
system by fighting the antigens. This forms the basic mechanism of the
immune system.
2.3. Influence of the mind on physical health
There has been an increasing number of studies that document the
connection between the mind and the body where illnesses are shown to
have developed through mental stress and strain. Cancer, arthritis, asthma
and cardiac illnessess are only some of them. In the early 1960’s Solomon
and Moos (1967) referred to the findings of Leshan and Worthington (1956)
regarding mental illness/wellbeing as contributing the development of
cancer. Their findings identify factors like bereavement, inability to express
hostile emotions and feelings, unresolved tensions, and personal
disturbances prior to the development of a tumour. Solomon and Moos
(1964) studied the personality of over 5000 patients with rheumatoid
arthritis and came to the conclusion that most of them have common
personality traits. They are seen to be “self-sacrificing, masochistic, rigid,
moralistic, conforming, self-conscious, shy, inhibited, perfectionist, and
interested in activity” (Solomon & Moos, 1964, p. 659). There is also

16
evidence that fear or distress before surgery can slow down postoperative
recovery by delaying wound healing (Keicolt-Glaser et al., 1998).
‘Immune Dysregulation’ can be the influence of negative emotions leading
to “a spectrum of conditions [associated with] aging, cardiovascular
diseases, osteoporosis, arthritis, type 2 diabetes, certain cancers, frailty and
functional decline; production of proinflammatory cytokines” (Glaser et al.,
2002. p.16) and so on. A review including research literature from more
than 300 empirical studies identified that psychological stress affects the
immune system in human participants and it does so as a function of age
and disease (see Segerstrom & Miller, 2004). While psychological and
behavioral functions can affect the immune system, these effects can, in
turn, influence behavior patterns (Mair et al., 1994). This is explained in
detail in Klaizen Matter-Walstra’s (1999) paper on PNI.
Many studies have been conducted on animals which show immunological
responses to environmental conditions. For example, Riley et al. (1981)
studied the impact of environmental stress on tumour incidence in mice.
Three groups of mice with mammary tumours were studied; ‘parous’4 mice
and ‘non-parous’ mice were housed in open communal rooms and subjected
to daily activities and environmental stress such as cage cleaning, usual
dust, noise, drafts, and odours. The third group was housed in plastic cages
with bedding, providing ventilation and less thermal fluctuation. The low
stress residential conditions proved beneficial for the third group,
influencing their immunologic competence by sustaining ‘normal T cell
population’ (Riley et al., 1981). The implication that physical environments
can play a key role in reducing or eliciting stress (comfort levels, air quality,
light and so on) has also been recorded in research undertaken in the field of
environmental studies.
4 The word ‘parous’ means “Having given birth one or more times” (Medical Dictionary).

17
Stress is defined as:
A mentally or emotionally disruptive or upsetting condition occurring
in response to adverse external influences and capable of affecting
physical health, usually characterized by increased heart rate, a rise in
blood pressure, muscular tension, irritability, and depression (The
Free Medical Dictionary, n.d.).
Wellbeing, which is affected by responses to stress can be influenced by the
environment as a whole, either social or built. Not only are these responses
conscious or subconscious, they also can be positive and/or negative (Rice,
1987). When negative, stress which involves a state of “anxiety, fear, worry
or agitation” leads to “painful situations” (p.18) is usually known as
‘distress’. Positive, stress which is a response to pleasurable and satisfactory
situations “heightens awareness, increase mental alertness, and often leads
to superior cognitive and behavioural performances” (p.19) and is known as
‘eustress’ (Seyle, 1974 as cited by Rice, 1987).
There are many ‘sensual stresses’ that stay in the background – such as
urbanisation, crime, boredom, computer invasion, isolation of the aged,
drugs, alcohol and tobacco abuse, noise levels – affecting the health and
wellbeing of an individual adversely (Wheatly, 1994). Wheatly (1994) states
that stress contributes to “initiating, maintaining, and aggravating a number
of physical and mental disorders” (p.1); for example, the cardiovascular
system which is affected by many of the ‘habits’ incurred due to stress such
as smoking, alcohol consumption, caffeine, sleep disorders, sex, obesity,
character, heredity and race (Wheatly, 1994). Mental stress is further
activated by noise, crowding, other stress factors related to industrialisation
and urbanisation, and by emotions. Anxiety can handicap adaptive efforts
which try to suppress or repress uncontrollable emotional feelings leading to
psychological inadequacy. When constant, the result is anxiety and panic
disorders, mental impairment and other disassociation from reality (Sheehan
& Soto, 1987).

18
Wheatly (1994) has described in length the impacts of stress on various
physiological conditions. These include blood pressure, which may escalate
due to high levels of hypertension, certain psychiatric disorders such as
phobias and panic disorders, and depression arising from exposure to
prolonged chronic stress. Many infectious diseases and life threatening
illnesses like cancer can also manifest due to stress; for example, students
who faced failure or more disappointments in life were diagnosed as having
sore throats, and those with prolonged sadness with acute respiratory illness
(Wheatly, 1994). This is because people under stress are more susceptible to
the impairment of the immune system thereby potentially increasing their
vulnerability to infectious diseases. Recovery is also slower under stressful
conditions.
Stress is seen to initiate skin problems temporarily, while leading to
permanent and pathological problems after prolonged exposure. As the
biological reaction to stress is very complicated, the skin can react in a
number of ways (Wheatly, 1994). This may inadvertly lead to mental
unwellness as self esteem may be diminished as a result of the skin
disorders becoming a vicious circle. Other examples of negative impacts
due to stress are activation of PMS (premenstrual syndrome) which leads to
psychiatric problems like anxiety, tension, irritability and/or depression
(Wheatly, 1994). Physical problems like weight gain and headaches are also
possible (Wheatly, 1994).
Wheatly (1994) states that elderly people have increased susceptibility to
stress, especially those suffering isolation from the community, hearing and
sight problems, mental impairment, not being self sufficient, limited
mobility and lack of social contacts. The background sounds in the
surroundings they inhabit such as sounds of floor boards creaking, clocks
ticking, sound of the air on the windows and on the like may seem more
pronounced, leading to stress.
These are only some of the various implications of mental well-being
causing physical ailments (Wheatly, 1994). Stress can be said to be a

19
subconscious state of mind, which sometimes a person may not even be
aware of. Every person encounters stress in one way or other in life.
However, being aware of stress and its consequences and trying to prevent it
from the onset, would be key factors in preventing future illnesses.
2.4. Summary
The purpose of this chapter has been to show that the science of PNI
presents information about the interrelationship existing between the mind
and body systems. The studies referred to strongly support the notion that
illnesses are contractible and can be aggravated by psychosocial factors
responsible for stress. Though all diseases may not be based on emotions, a
growing number of experts believe that some diseases result from emotional
responses. For instance, a sense of loss of control over ones’ situation can
lead to a loss of normal functioning of the physiological system (Kiecolt-
Glaser et al., 2002). When something like this happens, our immune system
is weakened, making it easier to contract disease.
As the findings in PNI studies demonstrate, we cannot separate our
physiological systems from the mind which, in turn are internally tied to our
experiences with life. Experiences are a result of our interaction with the
external environment. As such, it makes sense to create environments that
are more conducive to health and well-being. The experiences in life are
individual and some of these are determined by the way an individual sees
the world, how a person can cope with stress or joy (Ray, 2004). It can be
said that an experience of the mind is psychological and not physiological.
The body initially responds to the signals reacts according to the signals sent
from the central nervous system including the brain without taking fantasy
or reality into account. This accounts for either positive or negative
responses with their corresponding physical effects on the individual (Ray,
2004). This perspective of health profits from the understandings of the
inter-relationships between the emotions/mind with the physiological part of
the body thus affecting health and well-being. Inquiries into PE
relationships would benefit from such understanding of person as a whole.

20
Keeping this in mind, we proceed to the next sections which describe the
study’s methodology and results.

21
Chapter 3
Methodology
3.1 Introduction
This chapter describes the approach taken in mapping research that deals
with the relationship between the built environment and the body’s systems
as defined by the PNI model. It commences by describing the temporal and
substantive parameters of the study as well as the theoretical framework
developed for conceptualising and situating the person (‘P’) and the
environment (‘E’) in a specific P/E dialectic. With this context in mind, the
chapter outlines the study’s general methodological approach, providing
specific information about how data (research literature) were collected,
analysed and organised.
3.2 Establishing the context of the study
In this study, the mapping of literature was generally restricted to studies
published between 1975 and 2006. There are three main reasons for this.
Firstly, there is the need to make the study relevant in a contemporary sense.
Secondly, it was around 1975 when there was a renewed interest by
researchers and designers regarding the relationship between people and
environment. Ittleson’s work published in 1975 is a prime example (refer to
Ittleson, 1975). Thirdly, the time frame provided for a manageable study
satisfying the expectations of a Master’s thesis.
With respect to the substantive parameters of the study these were
conceptualised in terms of the P/E dialect with an emphasis on the
relationship between the environment and how it affects the person in terms
of the psychological and physiological systems of the body. For this study,
this was described in terms of the primarily conceptualised PE Integrated

22
Health Systems5 Model (Figure 6). To define person (P) in this integrated
health systems context, the study used the PNI model (Figure 1) wherein the
mind, the neuroendocrine system and the immune system constitute the
major systems of the body in terms of an integrated understanding of health
and well-being. As previously described, the ‘E’ dimension was very
broadly viewed as everything built without naturally existing in the first
place. More specifically it incorporates animate and inanimate elements
most commonly managed through the design process by interior architects
and designers. Having said this, the study does not include literature that
relates specific aspects of the environment to specific elements of the body
such as the anthropometric relationship between environment and the
muscles and skeletal structure of the body. Instead this work deals chiefly
with the body in terms of the PNI systems. While this is recognised as a
limitation of the study, the study provides an opportunity to evaluate any
potential merits of PNI in broadening our understanding of the relationship
of the environment to health and well-being and, equally, of the
environment in challenging the value of PNI as representing P in the P/E
dialectic.
Figure 6 PE Integrated Health Systems Model
5 The title name for the model was suggested by my principal supervisor, Associate Professor Dr. Jill Franz.
Health Systems Environment
Mind Neuroendocrine Immune
PNI
Person BE
Inanimate Animate
23
3.3 Overall mapping framework
A preliminary review of literature concerned with the broad area of person-
environment interaction showed that most studies are conducted from a
perspective of specific dimensions of the BE (such as the psychological,
physical and/or social aspects). In a similar manner ‘Person’ (P) is mainly
researched by looking at a particular aspect; for example, emotions, stress,
or physical dimensions. In the majority of studies both the E and the P are
conceptualized from independent perspectives rather than being treated as a
whole entity. Therefore, what did not appear to be covered to any great
extent was the relationship between person and environment where the
person is understood in the integrated systems dimension such as that
conveyed by the PNI model. This, previously described as an integrated
approach became the focus of the study.
The study as outlined was organised into three parts: (1) A survey of the
field of PNI to identify its various attributes and how they were understood
independently and integrally to relate to the environment. This survey was
also broadened to include select literature related to a state of total health
and wellbeing. (2) A survey of the field of built environment research from
a PNI perspective. (3) A map of the outcome of the surveys depicting a
picture of the research conducted to date, and in the process providing a
resource for interior designers as well as highlighting opportunities for
future research from both medical and design perspectives.
The mechanism for organising, analysing, synthesising, and presenting the
surveyed literature was initially developed using tentative categories
revealed in a preliminary survey and review. A more extensive literature
survey and review refined this mapping process producing the matrix shown
in Table 1.
24
P&E (Psyche & Environment)
N&E (Neuroendocrine & Environment)
I &E (Immune & Environment)
Integrated Health and Environment
PNI (Psychoneuro- immunology & Environment)
BE Literature
Environmental Psychology
Design
Architecture
Design and healthcare
Envtironmental health
Health Literature
Healthcare
Health Psychology
Medical
Table 1
Method for classification of data into domains
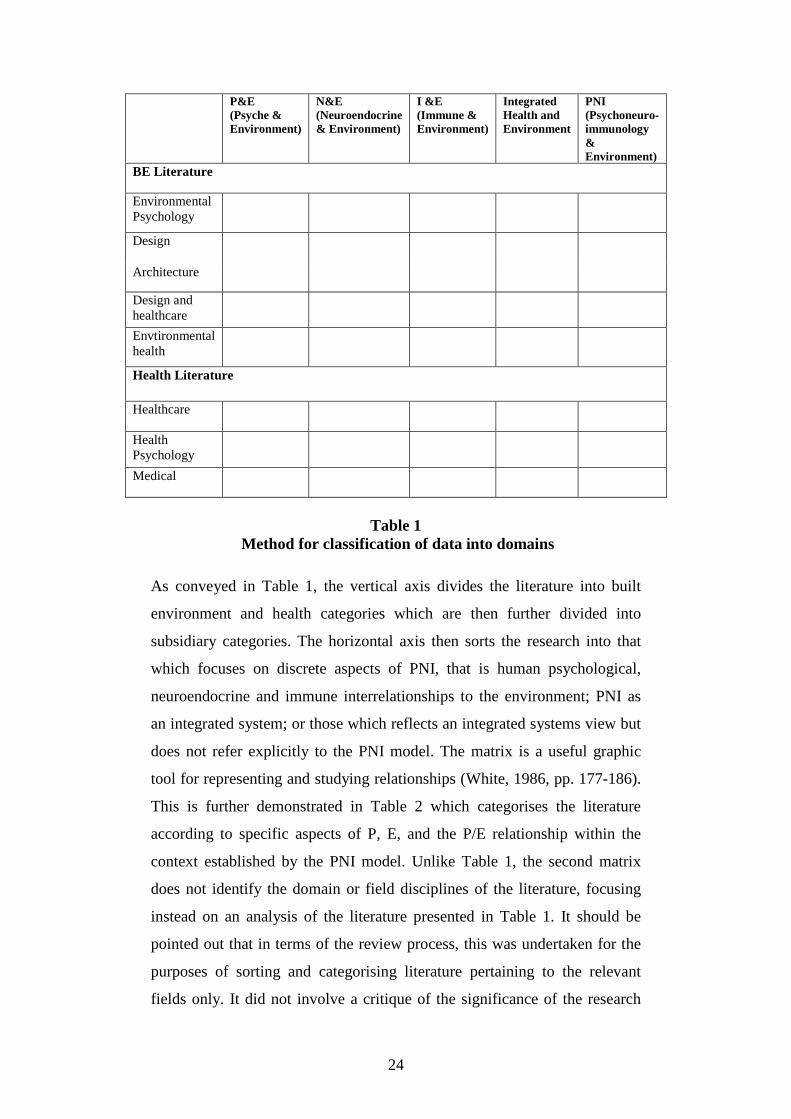
As conveyed in Table 1, the vertical axis divides the literature into built
environment and health categories which are then further divided into
subsidiary categories. The horizontal axis then sorts the research into that
which focuses on discrete aspects of PNI, that is human psychological,
neuroendocrine and immune interrelationships to the environment; PNI as
an integrated system; or those which reflects an integrated systems view but
does not refer explicitly to the PNI model. The matrix is a useful graphic
tool for representing and studying relationships (White, 1986, pp. 177-186).
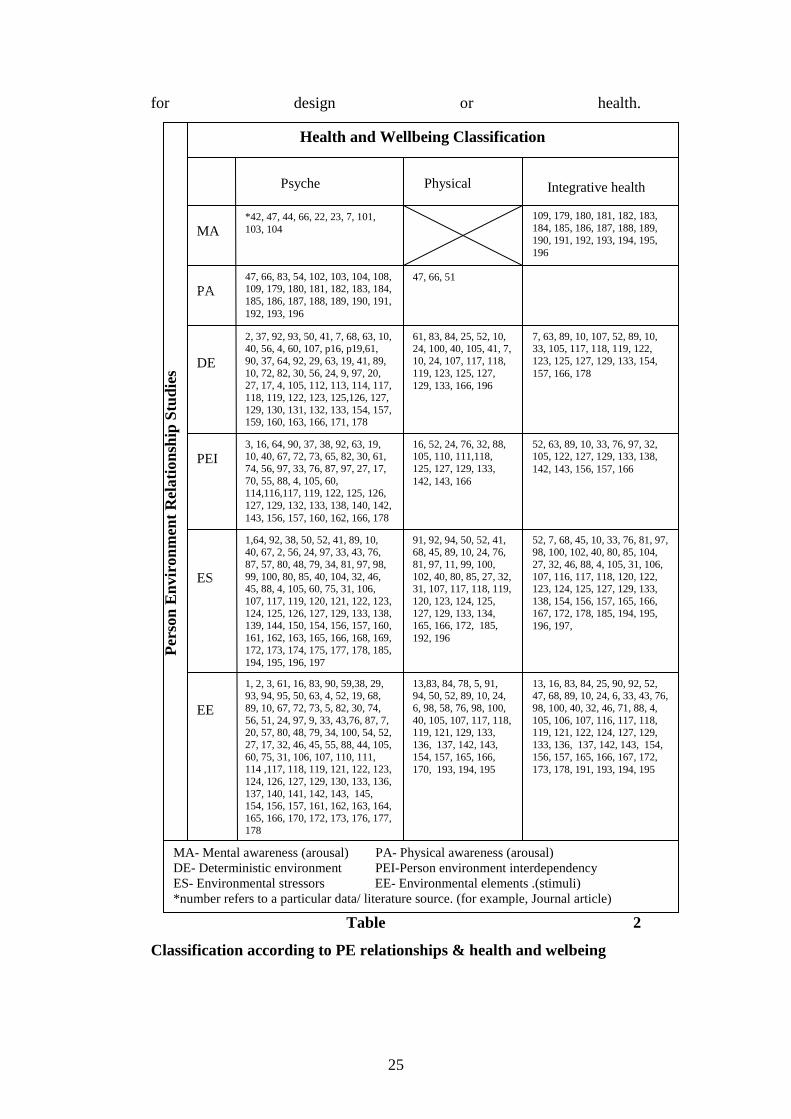
This is further demonstrated in Table 2 which categorises the literature
according to specific aspects of P, E, and the P/E relationship within the
context established by the PNI model. Unlike Table 1, the second matrix
does not identify the domain or field disciplines of the literature, focusing
instead on an analysis of the literature presented in Table 1. It should be
pointed out that in terms of the review process, this was undertaken for the
purposes of sorting and categorising literature pertaining to the relevant
fields only. It did not involve a critique of the significance of the research
25
for design or health.
Table 2
Classification according to PE relationships & health and welbeing
Psyche Physical Integrative health
MA
PA
DE
PEI
ES
EE
*42, 47, 44, 66, 22, 23, 7, 101, 103, 104
2, 37, 92, 93, 50, 41, 7, 68, 63, 10, 40, 56, 4, 60, 107, p16, p19,61, 90, 37, 64, 92, 29, 63, 19, 41, 89, 10, 72, 82, 30, 56, 24, 9, 97, 20, 27, 17, 4, 105, 112, 113, 114, 117, 118, 119, 122, 123, 125,126, 127, 129, 130, 131, 132, 133, 154, 157, 159, 160, 163, 166, 171, 178
3, 16, 64, 90, 37, 38, 92, 63, 19, 10, 40, 67, 72, 73, 65, 82, 30, 61, 74, 56, 97, 33, 76, 87, 97, 27, 17, 70, 55, 88, 4, 105, 60, 114,116,117, 119, 122, 125, 126, 127, 129, 132, 133, 138, 140, 142, 143, 156, 157, 160, 162, 166, 178
1,64, 92, 38, 50, 52, 41, 89, 10, 40, 67, 2, 56, 24, 97, 33, 43, 76, 87, 57, 80, 48, 79, 34, 81, 97, 98, 99, 100, 80, 85, 40, 104, 32, 46, 45, 88, 4, 105, 60, 75, 31, 106, 107, 117, 119, 120, 121, 122, 123, 124, 125, 126, 127, 129, 133, 138, 139, 144, 150, 154, 156, 157, 160, 161, 162, 163, 165, 166, 168, 169, 172, 173, 174, 175, 177, 178, 185, 194, 195, 196, 197
1, 2, 3, 61, 16, 83, 90, 59,38, 29, 93, 94, 95, 50, 63, 4, 52, 19, 68, 89, 10, 67, 72, 73, 5, 82, 30, 74, 56, 51, 24, 97, 9, 33, 43,76, 87, 7, 20, 57, 80, 48, 79, 34, 100, 54, 52, 27, 17, 32, 46, 45, 55, 88, 44, 105, 60, 75, 31, 106, 107, 110, 111, 114 ,117, 118, 119, 121, 122, 123, 124, 126, 127, 129, 130, 133, 136, 137, 140, 141, 142, 143, 145, 154, 156, 157, 161, 162, 163, 164, 165, 166, 170, 172, 173, 176, 177, 178
47, 66, 83, 54, 102, 103, 104, 108, 109, 179, 180, 181, 182, 183, 184, 185, 186, 187, 188, 189, 190, 191, 192, 193, 196
61, 83, 84, 25, 52, 10, 24, 100, 40, 105, 41, 7, 10, 24, 107, 117, 118, 119, 123, 125, 127, 129, 133, 166, 196
16, 52, 24, 76, 32, 88, 105, 110, 111,118, 125, 127, 129, 133, 142, 143, 166
91, 92, 94, 50, 52, 41, 68, 45, 89, 10, 24, 76, 81, 97, 11, 99, 100, 102, 40, 80, 85, 27, 32, 31, 107, 117, 118, 119, 120, 123, 124, 125, 127, 129, 133, 134, 165, 166, 172, 185, 192, 196
13,83, 84, 78, 5, 91, 94, 50, 52, 89, 10, 24, 6, 98, 58, 76, 98, 100, 40, 105, 107, 117, 118, 119, 121, 129, 133, 136, 137, 142, 143, 154, 157, 165, 166, 170, 193, 194, 195
7, 63, 89, 10, 107, 52, 89, 10, 33, 105, 117, 118, 119, 122, 123, 125, 127, 129, 133, 154, 157, 166, 178
52, 63, 89, 10, 33, 76, 97, 32, 105, 122, 127, 129, 133, 138, 142, 143, 156, 157, 166
52, 7, 68, 45, 10, 33, 76, 81, 97, 98, 100, 102, 40, 80, 85, 104, 27, 32, 46, 88, 4, 105, 31, 106, 107, 116, 117, 118, 120, 122, 123, 124, 125, 127, 129, 133, 138, 154, 156, 157, 165, 166, 167, 172, 178, 185, 194, 195, 196, 197,
13, 16, 83, 84, 25, 90, 92, 52, 47, 68, 89, 10, 24, 6, 33, 43, 76, 98, 100, 40, 32, 46, 71, 88, 4, 105, 106, 107, 116, 117, 118, 119, 121, 122, 124, 127, 129, 133, 136, 137, 142, 143, 154, 156, 157, 165, 166, 167, 172, 173, 178, 191, 193, 194, 195
47, 66, 51
109, 179, 180, 181, 182, 183, 184, 185, 186, 187, 188, 189, 190, 191, 192, 193, 194, 195, 196
Per
son
Env
ironm
ent R
elat
ions
hip
Stu
dies
Health and Wellbeing Classification
MA- Mental awareness (arousal) PA- Physical awareness (arousal) DE- Deterministic environment PEI-Person environment interdependency ES- Environmental stressors EE- Environmental elements .(stimuli) *number refers to a particular data/ literature source. (for example, Journal article)

26
3.4 Methodological approach
In surveying and reviewing the literature, the study was guided by an
integrating and synthesising approach described by Cooper (1989, 1998). As
Cooper (1998) points out, literature reviews can be undertaken for a variety
of reasons. Most typically they “...appear as detailed independent works or
as brief introductions to reports of new primary data” (p. 3). In terms of
their purpose, they can “...focus on empirical studies and seek to
summarisze past research by drawing overall conclusions from many
separate investigations that address related or identical hypotheses” or they
can “...present the theories offered to explain a particular phenomenon and
to compare them in breadth, internal consistency, and the nature of their
predictions” (Cooper, 1998, pp. 3-4). While adopting Cooper’s (1998)
method to identify literature, the literature review in this thesis is an
independent work that focuses on qualifying the characteristics of various
studies related to the topic of the thesis, integrating this through a
categorisation and mapping process.
While the qualifying process mentioned above involves a form of critique, it
is not a critique aimed at producing “...a decisive analysis of the quality of
the research” (Morrison, 1991, p. 20) or of extracting methodological
assumptions (Hart, 1998, p. 109). Not withstanding this, it still had to have
other features of a good critique as highlighted by Morrison (1991); that it,
it had to be “...objective, constructive, unbiased...” (p. 20). In other words, it
had to be cognisant of any threat to validity and set in place measures to
minimise this. Cooper and Hedges (1994) define a threat to validity as any
“plausible reason for false conclusions about the associations between a
class of treatments and a class of outcomes, about the casual nature of their
association, or about the generalization of their association” (p. 542). The
measures are incorporated into the following discussion of the various
stages of the study. The stages are an adaptation of the five stages of
research synthesis outlined by Cooper (1998). These are: problem

27
formulation; data collection or the literature search; data evaluation; analysis
and interpretation; and presentation of results (Cooper, 1998, p. 5).
3.4.1 Problem formulation
During problem formulation, conceptual and operational definitions are
considered to aid in distinguishing studies that are relevant to the review
(Cooper, 1982, 1998). The conceptual and operational parameters for this
study have been described in the previous sections. The term ‘conceptual’ as
used in this study relates for the most part to an integrated health system as
defined by the PNI model. The Tables presented in the previous section
convey the main ‘operational’ (categorisational) concepts and parameters. In
this sense, the conceptual definitions provide the operational constraints,
with some elementary concepts and parameters being established in order to
begin the search and consolidated during the main literature search stage.
Primary researchers establish operational definitions before their research
begins. However, in review research, the way that concepts are formulated
is evaluated for relevance as they are encountered during the search for
studies. It is not unusual for several different operational definitions to be
involved in a research review because of the individual ways the researchers
develop them (Cooper, 1998). In this respect, the study blends qualities of
both primary and review research as referred to by Cooper (1998).
Cooper (1989) also describes two possible threats to validity during problem
formulation. For instance, focusing on an overly narrow as well as
superficial set of operational definitions can be threats to validity. He
suggests that narrow definitions provide little information about whether a
finding may apply across a variety of situations. In this study, this could be
interpreted to mean that narrow definitions could prevent other relevant
research from being located. For this reason the PNI concept was extended
to include literature that related to the PNI concept from the holistic health
domain. Reviewers who use broad conceptual definitions or who believe
that several operations are relevant to the concept, have the opportunity to
reach more definite and robust conclusions. In addition, definitions

28
involving multiple operations serve to rule out alternative or confounding
conceptualizations of the findings (Cooper, 1989, 1998). Secondly, lack of
attention to study results in the review poses a threat to validity. For
example, if the categories established in the primary research were overly
broad – as could have been the case by including all literature in the holistic
health domain, – then the research operations are of questionable validity.
Reviewers who examine the operational details will produce more valid
review conclusions (Cooper, 1982, 1998).
3.4.2 Data collection
The next step of data collection involves locating research literature within
the initial parameters, using this to evaluate the parameters, adjusting the
parameters if necessary and then, within these parameters, completing the
collection of data. More specifically, the data collection stage involves:
determining the procedures to be used to find relevant data; determining the
sources of potentially relevant studies to examine; establishing a means of
dealing with differences in the research contained in sources of information,
and identifying and addressing sources of potential invalidity (Cooper,
1998, pp. 6-7).
According to Cooper (1989), locating studies “...involves making a choice
about the population of elements that will be the target of the study” (p. 8).
In this study, the target is published literature that refers in some way to a
relationship between P as defined by the PNI model and E the environment
in a context of relevance to interior design. In locating potential literature
for inclusion in the research synthesis, the study was informed by several
studies on literature searching. For Cooper (1998), there are informal as well
as formal channels for locating research.
In terms of the informal channel, this incorporates personal contact, personal
solicitation, traditional invisible college, electronic invisible college, and the
World Wide Web. In relation to personal contact, the study involved the
identification of literature from personal files, by talking to supervisors,
colleagues, librarians, and other contacts. Opportunities such as presenting

29
at Faculty seminars were actively sought to open up this channel as much as
possible. This process invariably led to the identification of other
individuals and groups who were then contacted (solicited), usually via
email. The opportunity to access invisible colleges was made possible
through such things as discussion lists. This was of some use in identifying
groups and individuals who were working on related research. The World
Wide Web by comparison was very effective but differentiation had to be
made between peer-reviewed material and other material that had not
undergone a refereed review process. Because formal channels have greater
demands in terms of quality, these were given preference over those
identified informally which had passed through specific quality checks. The
most common sources of material located through the formal channel as
highlighted by Cooper (1998) included conference papers, journal articles
(including electronic journal articles), and research reports. This was
augmented by the following sources identified by Rosenthal (1991): books;
published newsletters, magazines and newspapers; theses (including
doctoral, masters, and bachelors theses); and unpublished work including
reports, grant proposals, convention papers, films, cassette recordings and so
on.
The main goal in literature searching is to find all relevant literature. As this
is not practically possible, the goal then becomes one of widening the search
area as much as possible within explicitly recognised constraints. According
to Cooper (1982, 1989) the first threat to validity in the data-collection stage
is that the review probably will not be totally exhaustive. The second threat
is that the elements in the retrieved studies might not represent all the
elements of the identified target. For validity reasons, Cooper (1982, 1989)
recommends that reviewers access as many information sources as possible
to ensure that as many studies as possible are located. Correspondingly, it is
also important that the researcher doing the literature survey explains how
and why the studies were selected by specifying well- defined criteria for
inclusion and exclusion. Also in terms of reliability, “...the more exhaustive
a search, the more confident a synthesist can be that another synthesist using
similar, but perhaps not identical, sources of information will reach the same

30
conclusions” (Cooper, 1998. p. 76). In relations to this study, this would
mean the synthesist will produce similar results in terms of the
categorisation and classification.
The main library databases formed the initial internet based search. From
these readings, potential key words and phrases for search purposes were
identified such as psychoneuroimmunology, interior environment, design,
psychology, health, mental wellness, built environment, physical
wellness/illness, holistic health, and stress. These key words were used on
their own as well as in various combinations such as design psychology,
health and environment, mental well-being, physical well-being, health-care
design, holistic health and environment, built environment and holistic
wellbeing/mental health, and well-being/physiological health and well-
being. The process was managed by the Boolean operators featured as part
of each search engine. Boolean operators were central to restricting as well
as expanding the search. Adding boolean operators (AND/OR/NOT)
allowed retrieval of literature/data most relevant for the study.
Literature related to the topic was chiefly located in library catalogues,
databases (using the data base search engines), abstracting service and the
internet, using a range of search engines, including Google. Some sources of
relevance included: Proquest, MEDLINE (National Library of Medicine),
PsycINFO (American Psychological Association), EBSCO Host, and known
websites including the PNI (psychoneuroimmunological) Society website.
To expand the search beyond these sources, a process of reference tracking
and citation searching was employed. People with an interest in
environmental psychology and the health promotive capacity of
environments (such as Dr. Daniel Stokols of University of North Carolina)
were also contacted to help identify additional resources. The process
overall was informed by the experience and knowledge of the University’s
reference librarian. It overlapped a process of data evaluation described in
the following section.

31
3.4.3 Data evaluation
Cooper (1998) describes data evaluation as a process of deciding which of
the publications retrieved should be included in the review (p. 6). As such,
the process is one of making critical judgements about the quality of the
individual data points and determining if they describe too many factors
irrelevant to the problem of interest (Cooper, 1982, 1989; Cooper and
Hedges, 1994). In terms of the present study, the research literature was
required to satisfy two main criteria. Firstly, it had to acknowledge person /
environment relationship in a psychological or physiological sense, or in an
integrated psychological/physiological sense. Studies outside this – such as
those in built environment literature that took an economic point of view –
were excluded. Equally, PNI or medical/health literature had to recognise or
make reference to the built environment in relation to either P, N or I or in
the integrated sense. Those that looked exclusively at other medical aspects
of the human body were excluded. Secondly, the literature had to
conceptualise the environment in ‘interior’ environment terms or be relevant
to the design of interior environments in recognition of the aim and
contextual constraint established for this study.
In addition to Cooper’s work, this stage also followed principles described
by Miles and Huberman (1994) in relation to qualitative investigation for
‘categorizing and coding’ data. Using their frame-of-reference, the localities
were seen as the field for collecting data and the various pieces of literature
were the data collected to be reviewed and analysed. In their words, the
literature was evaluated by:
1) “Sorting and sifting through materials to identify similar phrases,
relationships between variables, patterns, themes, distinct differences
between subgroups, and common sequences” (Huberman, 1994. p. 9).
For this study, this involved identifying elements by which studies could
be compared and differentiated.
2) “Isolating these patterns and processes, commonalities and differences,
and taking them out to the field [research literature] in the next wave of

32
data collection” (Huberman, 1994. p. 9). In this study, this involved
using these elements in subsequent searching and sorting to check the
robustness of the elements and the emerging themes and categories.
3) Progressively “elaborating a small set of generalizations that cover the
consistencies and patterns discerned” (Huberman, 1994, p. 9). That is,
consolidating the categories and their differentiating qualities.
The elements (criteria) used to compare, differentiate and evaluate the
relevance of the literature are summarised in the following table (Table 3).
They are related to two phases as described by Cooper (1998, pp. 45-103).
The first phase provided the first basis of elimination/selection with those
satisfying the criteria undergoing further evaluation as outlined in Phase 2.
The criteria were applied at two levels: an initial scanning of abstracts and
content pages, and where necessary, a more detailed examination of the
content.
Phase 1
1. Publication language 2. Publication types 3. Author 4. Setting to which the studies referred 5. Participants 6. Research design and methodology 7. Phenomenon studied
Phase 2
8. Phenomenon studied 9. Discipline areas from which the study originated 10. Research circumstances 11. Other integrated systems
Table 3 Criteria for evaluation
Phase 1
i. Publication language:
• Only papers, articles, books, and other literature in the English
language were evaluated. Non-peer reviewed as well as peer-
reviewed literature were included.

33
ii. Publication types:
• The search was restricted to built environment, interior
environment, design, psychology, psychoneuroimmunology, and
health publications particularly relevant to PE relationships.
• From these discipline areas none of the publications were
excluded as long as they discussed a PE relationship.
• All publication formats were considered.
iii. Author:
• Author names were identified only after the initial (title)
screening.
• The title screening and abstract reading process revealed the
authors predominantly interested in the research areas that were
identified for the purpose of this study. Subsequently, some of
the prominent authors’ articles and books were looked at to
understand their study type (for example, Solomon, Ader,
Cohen, Keicolt-Glaser in relation to PNI and Stokols, Ittleson,
Gifford, Altman, Canter, Kaplan, Zeisel, Ulrich in built
environment and design). Additional works that had not been
picked up in the initial search were identified through citation
searches and retrieved for subsequent evaluation.
iv. Setting to which the studies referred:
• This involved an evaluation of the literature in terms of whether
it related to the environment and, if so, what type of
environment; and, further, what type of interior environment (for
example, residential, workplace, commercial, or healthcare
including hospital environment).
• Some studies that looked at the influence of the external
environment on people’s emotion and behaviour were included
because of their relevance for interior design (for example,
outside noise and its impact on people psychologically or
physiologically). Some aspects of external environments can also

34
be conceived of as relevant to internally and thus are considered
applicable for the purposes of this study.
v. Participants:
• Studies that considered the relationship between people and
environment were included. Studies involving animals were
generally not included. The exceptions were two studies that
involved animals and formed the basis for PNI research studies
related to humans. Conceptual studies related to P/E
interrelationship were included.
vi. Research design and methodology:
• Studies were not included or excluded according to their
methodology or research design because this was not relevant
within the context of this study.
• Those following qualitative and/or quantitative methods were
included.
vii. Phenomenon studied (nature of the content):
• The content of an article was the most important criterion used to
decide which studies would be included or excluded. As stated
previously, the substantive parameters of the study were
conceptualised in terms of the P/E dialect, with an emphasis on
the relationship between the environment and how it affects the
person in terms of the psychological and physiological systems
of the body. This was described in terms of the P/E Integrated
Health Systems Model which was generated for this study. To
encapsulate an appreciation of (P) in this PE integrated health
systems context, the study uses the PNI model wherein the mind,
the neuroendocrine system and the immune system constitute the
major systems of the body in terms of an integrated
understanding of health and well-being. With respect to the ‘E’
dimension, this is very broadly viewed as everything built

35
without naturally being there in the first place. More specifically,
it incorporates animate and inanimate elements most commonly
managed through the design process by interior designers. The
study does not include literature that relates specific aspects of
the environment to specific elements of the body. It deals chiefly
with the body in terms of the PNI systems.
Phase 2:
In accordance with the first criterion, studies looking at PE relationships
concerning health within the fields of PNI, design, built environment,
mental well-being, physical- wellbeing, and health were selected following
a broad range of the above mentioned categories in phase 1. The second
criterion for elimination and inclusion for analytical purposes was
developed from this by following Cooper’s (1998) directives to develop the
criteria according to the indications that the collected data revealed and the
specific needs of the research design and study.
Many of the database searches that brought up vast amounts of literature had
to be narrowed down by reading the abstracts in the initial stage and
choosing carefully the ones that had to be read completely and analysed. For
this purpose other criteria were applied to the literature in order to identify
them for analysis. After the initial information on the particular subject were
collected, studies were identified according to its essence - namely its
objectives, settings, method, participants, results, and conclusion loosely
based on the phenomenon under study or found, discipline areas, research
circumstances, and integrative health perspective. It was necessary for the
selected final documents for review to contain relevant information
according to preset standards. They had to include one of the required
categories mentioned in phase 2:
viii. Phenomenon studied:
• The application of this criterion is similar to that described as 7
in Phase 1. It provides an overlap between the two phases and a

36
further consolidation of the sorting according to the built
environment (and the person in terms of the PNI concept);
design and health; and PNI (and the built environment).
ix. Discipline areas and field of research from which the research
originated:
• While this was not mandatory in the initial stage, it was
considered to provide a relevant dimension for the analysis and
interpretation stage of the study and its presentation as a resource
for design.
x. Research circumstances:
• Some of the circumstances surrounding the production of the
research were examined (for example why, when, where, how,
and by and for whom the research was produced). In addition,
the underlying assumptions within the literature were
interrogated accordingly. This was mainly to develop an
understanding of the reviewed literature in relation to the PNI
concept.
xi. Other integrated systems:
• This criterion enabled the evaluation to incorporate a closer
examination of other related integrated health systems not
explicitly labelled as PNI. Examples include holistic health and
environmental health.
3.4.4 Data analysis and interpretation
As indicated previously, the study was organised into three parts: (1) review
of the field of PNI to identify its various attributes and how they were
understood independently and integrally to relate to the environment; (2)
review of the field of built environment research from a PNI perspective; (3)
mapping to produce a picture of the research conducted to date. In this
analysis stage, the literature in (1) and (2) was explored according to its
37
content as well as to the area of BE and PNI literature from which it
originated. With respect to content, the concern was for research that
explored human physical and psychological conditions in different
environments as framed by the PNI model and its P, N, and I constituents.
The assumption underlying the strategy to classify data into P, N and I
categories was that PNI represented the main systems of the body and that
this could be used as a basis for locating and categorising research that
related people and environment from a health and well-being perspective.
For example, the analysis was interested in descriptions about conditions in
the environment that influence physical health, that influence mental well-
being and that also recognise the integration of the various systems; for
example where conditions in the environment are understood to affect
mental wellbeing which is, in turn, understood to affect physical health.
These are listed in Table 4 under the general heading of ‘Analysis pointers’.
The analysis pointers acted as an analytical tool for identifying encouraging
patterns and meaning to emerge. Cooper (1998) states that “... data analysis
requires that decision rules be used, to distinguish systematic data patterns
from ‘noise’ or chance fluctuation ... the rules involve assumptions about
what noise looks like in the [target population] and what criteria must be
met before the existence of a pattern in the data is said to be reliable”
(p.104).

38
BE PNI
Influence of the BE on the mental well-being of a person
Influence of P, N, I on each other
Effect of the BE on the physical wellness
Influence of BE on P, N, I independently or integrally
BE influencing the health in an integrated sense
Dimensions of BE that influence P in the PNI context
Suggestions of human inter-relationships with the BE
Environmental elemental factors taken into consideration in relation to health factors
Health outcomes as a result of interaction/transaction with certain environmental stimuli
Dimensions of the BE other than design features that would result in negative/positive well-being
Table 4
Analysis pointers
During the initial analysis, any dimension under consideration was recorded.
For instance, if the researcher had looked at a part of psychological
dimension within the BE, this was considered as P in the PNI framework.
Here, it was noted that much of the literature was generated through what is
very broadly called environment-behaviour research. In terms of human
health, very little was found in design literature with the exception of design
and healthcare environments. Whilst there is a large amount of research that
indicates that the environment impacts on human health, these studies have
been conducted mainly in healthcare settings. Theoretically, however, they
may contribute generally to a better understanding of other physical
environment and person relationships within the broader area of integrated
health.
As well as a focus on content of the source paper and research domain (that
is BE or health domain), the analysis also differentiated between positive
and negative outcomes from the PE relationship. For instance, studies that
focused on the negative and positive aspects of psychological responses that

39
may influence or impair mental health/wellbeing of a person – such as stress
conditions due to certain variables in the environment that were seen to
generate better health outcomes – were identified for the purposes of the
study outcomes. For instance, a negative outcome in regard to the auditory
sense could be noise (such as continuous traffic noise, background noises)
rather than sound and the person as a result suffers stress. A positive
outcome in regard to auditory sense would be soothing sounds (music)
which may result in improvement in wellbeing.
It was thought that this differentiation would add another level of relevance
for the study’s use as a resource for designers’ and creators’ application.
Some positive and negative environmental impacts and their influence on
health and wellbeing are described in Chapter Four and are also represented
in table format at the end of the chapter (Table 10). The process was initially
undertaken comparing and correlating sets of data and how they were
interrelated (Figure 7).
Figure 7 Data matching
(Source: workbook, Suresh 2005)

40
Another tool which was central to the analysis as well as to its presentation
was the two-dimensional matrix. The matrix developed from adapting
White’s (1986) ‘space adjacency analysis’ was used to help develop6 an
understanding of PE relationship to integrated health and evaluate the
overlap of research from various disciplines. In architecture and design,
space adjacency analysis allows one to identify connections between one
space and another and juxtaposes places according to their significance and
requirement (White, 1986). “Space adjacency analysis is a pre-design study
tool that reveals the extent to which building spaces need to be located
adjacent to one another and the reasons for these required adjacencies.
Analysis leads to informed design decisions about the site plan, building
plan and section configurations, the routing of the circulation network that
connects the building spaces, and other planning judgements that ensure that
the clients organization will function smoothly and efficiently in the new
facility” (p.4).
The ‘space adjacency analysis’ underlines several methods that can be
followed according to necessity (see White, 1986). It is a diagramming
approach to make analysis for relationships possible and outlines the matrix
(45° and 90°) and bubble diagram methods among others. However, for this
research purpose, the 90° matrix was chosen and adapted to the demand of
the analysis as a possibility towards clarifying and representing the linkages.
The matrix, (see Tables 1 and 2) when horizontally and vertically
conceptualized, showed the number of studies done in various areas and the
distinct overlaps between P, N and I when looked at both separately and
integrally in health and BE research literature. White (1989) suggests that
“the 90° matrix is a useful tool for studying the relationship of any set of
things (side list) to any other set of things (top list)” (p. 32).
6 The idea was developed and adapted from the method used by Smith (2000) for her PhD study. As it is not mentioned in the thesis, the means for such a process emerged out of our discussions.

41
The ‘interrelationship tool’ (Figure 8) was developed to allow categorisation
of data in Tables 1 and 2. This enabled analysis and classificacation of data
into relevant domains and relationships through a sorting, matching and
categorization process. The classification revealed that PE relationships
were understood in similar ways across domains as well as they were spread
out according to their nature and characteristics. This is further described in
Chapter 4 through some examples.
As shown in Table 1, the matrix strategy allowed the literature to be sorted
in terms of the domains within which it was found, as well as how it linked
to various dimensions of the PNI model. Using numerical coding, each
reference could be categorised or/and, as in Table 1, represented in terms of
the quantity of publications drawn from in each domain. Out of the 197
sources/references/data selected as relevant for analysis, it was found that
only 43 came from design and architecture sources and these mainly focuses
on form and aesthetics. 111 references came from the environmental
psychology sources. Of these many are theory building with a few
empirically based; for example, studies conducted on wayfinding,
environmental control, and restorative environments. Another 48 studies
Figure 8
Matrix 1 & 2 interrelationship tool
Domain Matrix (reference: Table 1)
Relationship Matrix (reference: Table 2)

42
came from healthcare setting studies. The remainder fell into other areas
such as environmental health and health research encompassed by the PE
integrative systems category.
As conveyed in Table 2, the matrix also enabled particular types of
relationships, qualities of the environment and the person in the PNI context
to be classified, namely: 1. Person and environment as separate entities; 2.
Person and environment interrelated and interdependent; 3. Person exerting
a significant influence on the environment; and 4. Environment having a
major impact on the person.
Research in BE so far indicates that there are many facets of the BE that
impact on a person’s health which would be further described in the results
section. It is important to note here that the initial intention of this research
was to establish a link between PNI and BE through a literature review. For
this purpose, it was necessary to firstly classify the relationship theories
within person environment or PE research followed by research within
health and BE with the aim of understanding the links between PE
relationship to health.
The PE relationships revealed through literature in the BE and healthcare
design literature were then considered in terms of the PNI model to
determine the quality of health implications revealed and implications for
the person environment relationship. The PNI model in this study was
central to understanding human health in an integrated systems manner.
3.4.5 Presentation
The last step in the research synthesis process is reporting the study. This
step begins with the formal ‘public’ presentation of the research study, the
dissertation. Presentation of the research includes any form of oral or written
disbursement of the study process. For this thesis, presentation includes the
process of writing, followed by publication of the thesis. The first threat to
validity associated with report writing is the omission of details about how
the review was conducted (Cooper, 1989). An incomplete report reduces the

43
chances of replicating the review. The second threat to validity involves the
omission of evidence about elements and relationships from the primary
research studies that those researchers found important. Cooper. (1989) adds
that protecting the validity of the other four stages protects validity during
the report writing stage. Cooper (1998) defines four parts in the presentation
of the study, namely, the introduction, the method section, the results
section, and the discussion of the results.
3.5 Summary
The examination, exploration and interpretation of the diverse literature
provided the opportunity to categorise the nature of PE relationship to health
within an integrated systems health model as defined by PNI. The method
used for this study was a research review process adapted from Cooper
(1989, 1998). The five step procedure as described by Cooper (1989, 1998),
along with tools and analysis procedures described by White (1989),
provided the basis for analysis and interpretation. The outcome of this
process of analysis and interpretation is described in detail in the following
chapter.
44
Chapter 4
Results
Part 1
Outcomes of PE Interrelationship
Relating to Health and Wellbeing
4.1 Introduction
As described previously, this study was guided by an integrating and
synthesising approach developed by Cooper (1989, 1998). The five step
procedure described by Cooper (1998) provided a framework for conducting
the study. The steps involve: 1) problem formulation 2) data collection 3)
data evaluation 4) analysis and interpretation and 5) presentation of results.
This chapter describes the fifth step: the presentation of the results. In doing
this, use is made of the relationship and classification matrices, which as
well as identifying literature, also show how the studies responded and/or
linked to various dimensions of the PE Integrative Health Systems Models
(Figures 1 and 6).
As described in the introductory chapter, the purpose of this research was to
describe and explore the impact of the BE on health and wellbeing using
Cooper’s (1989, 1998) techniques of integrative research review and
synthesis. As suggested by Cooper (1998), an initial definition of health and
wellbeing was selected. This definition is based on the PNI principles of
conceptualising a person’s mental and physical well-being.
The research questions guiding this review concern the relationships that a
person forms with the physical environment and their contribution to
positive or negative health and well-being outcomes or, in other words, the

45
efficacy or inefficacy of the BE to health and wellbeing. The level of current
understanding regarding the outcomes of the environmental responses is
also investigated. This is explored in the BE and, to some extent, health
research literature. The second and third steps involve the description of the
procedure for selecting studies for research synthesis and determination of
the characteristics of each study selected. The fourth step addresses the
results of the analysis and is the subject of this chapter.
As the description of the integrative system approach pertaining to PE and
health inter-relationships ultimately exists in the logical and pragmatic
associations among theoretical approaches and conclusions, parts one and
two of this chapter undertake to investigate the understandings of PE
relationships in BE and health field literature. They also explore how
findings about the PE relationship principles can aid the linkages of PNI
framework and BE to encompass an integrative picture. Part One explores
specific concepts in the understanding of PE inter/transactions and the
interrelationships that may inform health and wellbeing outcomes. Part Two
looks at literature according to the classification of the PNI model: the P, N
and I categories.
In summary, it appears that most of the work in attempting to understand the
influence of the physical environment on health and well-being in humans
for the most part has focused on physiological and stress factors.
Environmental behavior research indicates that studies on PE relationships
have mainly focused on the psychological and social aspects of PE
interaction and transaction. Several key PE relationship dimensions have
been proposed as ways to understand and explain environmental behaviours,
responses and experiences, such as spatial use, environmental privacy and
control practices, other experiential behaviours, preventive health factors
connected to the environment (such as ‘sick building syndrome’),
importance of aesthetic qualities, and design for human physical activity
(see Zeisel, 2006; Bechtel & Churchman, 2002; Bell et al., 2001). The
concepts have sought to explain PE relationship as being a result of the
interaction/ transaction of a collection of factors. While a thorough review

46
of each of these dimensions of PE relationship is beyond the scope of this
thesis, the theoretical concepts as well as empirical research related to
psychological, social, and physiological aspects of PE relationship are
relevant as they support the argument that the BE and the emotional changes
they generate may be associated with instigating conditions related to poor
physical health and well-being. They are also selected because, as shown in
Table 5, they help describe the various attributes of an integrative health
systems model.
Level of Analysis
Psychological Psychoneuroimmunological Environmental
- general mental capacity - specific perceptual and cognitive skills - adaptive skills - hereditary and cultural makeup - situational control
- level of belief - mental capability - level of emotional distress - activity of neuroendocrine systems - impact on the immune systems - tendency to acquire illnesses
- environment that the person has grown up in - psychosociocultural factors that influence behaviours and place experience - elements within the environment that trigger negative and positive reactions - conducive parts of the environment that a person grows dependent on
Table 5 Analysis levels
PE relationship dimensions described in this part of the chapter are
separated into two categories for clarity. The two categories are (1) concepts
specifically about the human (animate) dimension of inter/transaction taking
place and (2) concepts about the physical space (inanimate) dimension.
These are then further categorised into psychological, social and
physiological for the animated category; and spatial and elemental for the
inanimate category (Table 6.). An additional categorisation process shows
other dimensions to these sub-categories. Examples of literature drawn from
design and architecture, healthcare settings, environmental psychology,
medical and health literature that is relevant to the integrated health system
focus of this thesis are also presented (Table 6, p.58).
Existing BE research that relates to health and well-being can be
conceptualised within the following five broad categories:

47
1. Studies that are concerned with the physical environment in the
psychological sense.
2. Studies that focus on the conditions of the physical environment
such as the physical elements, form, and characteristics of the built
environment.
3. Studies based on issues relating to the social relationships.
4. Studies that focus on specific fields of study or different types of the
physical environment, for example, residential, workplace, health-
care and so on.
5. Empirical research looking at specific relationships, occurrences and
outcomes from person environment connectivity and responses.
6. Empirical research that incorporates PE relationships in terms of the
person’s health and well-being.
4.2 The PE inter-relationship: Dimensions that relate to an
integrated health systems approach
Frumkin (2005) states that environmental health being dynamic in nature
encourages interdisciplinary as well as transdisciplinary research, rather
than trying to concentrate on one discipline to conceptualise relationship
between human-health and the environment. He also states that
environments have many different properties and functions allowing people
to interact and respond to them in “predictable ways” (p.xxxviii), providing
different dimensions ranging from being “alienating, disorienting, or even
sickening” to being “attractive, restorative, and even salubrious” (p.xxxviii).
Underlying this thesis is the premise that if we are to really understand the
consequence of person-environment relationship in relation to human health
and well-being, we need to regard the person and their psycho-physiological
systems in an integrated sense. In general, however, a person’s psycho-
physiological relationships with the BE, particularly emotional and mental
relationships and their influence on the physiological systems, are less

48
studied in physical environment research (Korpela &Ylen, 2005). As
Parsons & Tassinary (2002) state from the perspective of environmental
psychophysiology, “All psychological events have some physiological
referent - there is no entity called mind that is independent of the central
nervous system” (p. 174.). Some theories in environmental psychology like
those related to environmental stressors, restorative environments,
topographic cognition, environmental aesthetics, isolated environments, and
restricted environmental stimulation therapy, indirectly imply that
psychological events have some ‘physiological referent’ (Parsons &
Tassinary, 2002).
The discussion of the current status of research to be outlined in this chapter
will begin by looking at the various interdisciplinary areas of BE research
and health research in order to look at their distinctive dimensions. Human
mind-body relationships will then be discussed and linked to the
understanding of person as a whole in a relationship with a physical place.
Finally, given that we know little about the complex ways in which the
person and environment relationship inter/transact in an integrated health
sense, a case will be made for the development of a new integrative model.
The two primary dimensions of the PE relationship are P (person)
categorised in terms of the animate dimension and E (environment)
categorised in terms of the inanimate dimension. These encompass research
from environmental psychology/EBR, architecture and design (including
landscape), environmental health and healthcare settings.

49
Uunderlying characteristics influencing PE inter-relationship on health and
wellbeing *
Psychological Perception Cognition Responses Experiential knowledge Attitudes Arousal from stimuli
Ittleson, 1976; Stokols, 1978; Stokols & Altman, 1987; Wapner, 1987; Kaplan et al., 1988; Wapner & Demick, 2000; Bronfenbrenner, 1979; Gifford,1997; 2002; Kaplan, 1995; Altman, Rogoff, 1987.
Social Privacy Organisational structures Influences (acquired/ hereditary) Adaptation
Becker & Steele, 1995; Gifford, 1997; Bell et al, 2001; Wapner & Demick, 2000.
Animate
Physiological Risk factors Adaptation Personality Self – efficacy Objective/ subjective responses Belief system Physical limitations Sensation Arousal from stimuli
Anthony &Watkins, 2002; Parsons & Tassinary, 2002; Ulrich, 1989,1991, 2004; McCoy, 1997; Solomon, 1996; Parsons & Tassinary, 2002.
Spatial Facilities/ structure Form and function Access/ usage Safety Objective/subjective
Forrest, 1999; O’Neill, 1991; Stokols, 2000; Canter, 1997; Anthony & Watkins, 2002.
Inanimate Elemental Stimuli
Control Aesthetics Quality Usage Accessories Objects
Becker & Steele, 1995; Heerwagen,J. 1990; Ulrich, 1986; Ulrich et al, 2004; Prohansky & Fabian, 1986; Munroe, 2000; Clitheroe et al, 1998; Heerwagen, J. 1990.
Table 6
Identified dimensions of PE + health and well-being interrelationships (*sources mentioned are some examples only and not all are included)
4.2.1 The animate dimension (psychological, social, physiological)
Canter’s theory about place posits the notion that the experience of a person
in the environment is the sum total of the transactions between the

50
environment and the different levels of a person’s experience. These levels
are understood to involve “personal, social and cultural constituents of
person-place” (Canter, 1997, p.118). The specified dimensions in the
analysis categorisation evolve from similar theories associated with PE
experiences and relationships.
For this thesis, these constituents are described as psychological, social and
physiological related in turn to concepts such as environmental perception,
environmental cognition, stress and emotion, identifying environmental
stressors, person environment interdependency, environmental determinacy,
and environmental experiences and so on. These concepts originated chiefly
from environmental psychology, and while the field provides invaluable
insights to a person’s psychological responses and the environment
relationship, it does not directly identify the specific sources of any positive
and negative impacts on health and well-being within the environment.
Having said this, there is the potential for such links to be made by taking an
integrated health systems approach. This could be achieved by combining
knowledge from a number of different studies. For example, in EBR studies
a lack of control over the place a person inhabits may cause anxiety and
depression and an aversion to the place, all of which are psychological
outcomes of environmental perception and cognition (Gifford, 1997).
Healthcare environment studies indicate that such psychological responses
could elicit additional physiological disorders (Ulrich & Zimring, 2004).
Another example is the sociophysical environment and its relationship to
privacy. An open office plan can nurture as well as hinder a person’s
opportunity for interaction with other people, however this depends on how
they perceive the space (Evans & McCoy, 1998). Some responses from such
influences may generate negative responses causing anxiety. Studies
indicate that high levels of anxiety on a regular basis can be the cause of
certain physiological ailments (Schweitzer, et al., 2004).
51
4.2.2 The inanimate dimension (physical dimensions such as spatial and elemental)
The second dimension focuses on the physical elements within a space and
their relationship with/to form, layout, aesthetics and so on in terms of
sensual and physical impact. For example, furniture not ergonomically
considered can cause certain physical ailments such as neck and back pain
(Moffet et al., 2002). Open plan offices are related to headaches among
employees using them depending on their type of work (Stokols, 1998).
Further, the inability to change the circumstances – for instance not being
able to move furniture according to need or personal choice; not having
control over temperature settings – harms mental well-being which can
cause adverse health effects (Ray, 2004).
While the animate and inanimate dimensions which are mentioned in
existing studies may narrow the likely sources of the problem as direct or
indirect generators of negative health and wellbeing, and/or identify person
environment relationships in distinct contexts, they generally do not
implicate a specific source and its consequences on health and well-being.
The identified dimensions of the environment overlap when the person is
considered in his or her entirety. PNI provides a tool to better understand the
person as a whole. In addition, when linked to the BE relationships by
taking a transdisciplinary approach, a better understanding of the
interrelationships of environment with the person’s body systems and health
and wellbeing is possible.
In this thesis, the established PE relationship integrative systems model and
interrogation of the animate and inanimate dimensions of the BE according
to their domains provide the main basis for the approaches taken, such a
classification and categorisation. The dimensions have been categorised
under the assumption that they would inform health and wellbeing
relationships to the physical environment within the integrative systems
framework.

52
4.3 The properties of place or space and person environment relationships
To understand the properties of BE and PE inter/transaction, it is necessary
to construct an overview of current concepts and understandings in built
environment and design research that applies to the PE Integrative Systems
Model. This will help in providing an understanding of what built
environment is about, its scope of work, context of work, its relationship to
related disciplines, and an understanding of current design practice with
regards to human necessities, experiences, responses and relationships to the
physical environment. In the process, it will also demonstrate how different
approaches regard the environment (for example, the psychological, social,
behavioural constructs, and so on). The principles of PE relationships are
analysed using the PNI Integrated Systems Model, to gain understanding
and insight about health and wellbeing influenced by the BE.
The review of research identified various theories and conceptual models in
practice. Among them, in this thesis, we are only concerned about those
concepts and theoretical approaches that are necessary to understand the
person’s relationship with the environment influencing person’s health
psychologically or physiologically. Moore et al (2003) states that when
multiple levels are employed for analysis, the results lead to greater
understanding of PE relationships. Environmental research is then
concerned with “…the behavioral, emotional, and health outcomes of
people’s transactions with their everyday environments (called
settings)…which include residential, occupational, educational, recreational,
public, and virtual places” (Stokols & Clitheroe, 2005, p. 97).
To summarise the notion of environment in research literature, it means the
condition under which any person or thing lives or is developed; the sum
total of influences which modify and determine the development of life and
character. However, the term ‘human environment’ has evolved to embrace
not only the physical but also the psychological aspects of an environment
which includes the social, interactional, transactional, and organizational

53
aspects that might affect the mental health and wellbeing (Proshansky et al,
1976). Building codes and standards are compiled for design and
construction – in regard to air quality, building materials, water supply,
thermal requirements and so on – in order to improve the quality of the
physical environment (Lawrence, 2002). However, these codes need to also
address psychological and emotional aspects of the human being so that
they support health and wellbeing in the long run.
Bronfenbrenner (1979) identifies four levels of the “socioecological
environment” (p. 22). Firstly, he identifies the microsystem which includes
the environment that the person is affiliated with, for example the home.
Microsystems have certain physical, objective and material characteristics
with which the person associates. Secondly, he labels the mesosystem, that
is, environments which are the necessary settings in which the person works
and spends a constructive amount of time. Thirdly, he isolates the
exosystems which consist of the environments that may not be directly
associated with the individual but would affect the person indirectly. Lastly,
he identifies the macrosystem, which is associated with the system that
forms the social and cultural values and which influence the behaviour,
experiences and attitudes in people (Bronfenbrenner, 1979). This study’s
analysis is limited to relevant parts of the micro and the macro systems and
is concerned with only those aspects which are identified as being
interrelated to human health and well-being.
Canter (1997) states that if environmental psychology theories are to be
absorbed into the “heartland of architectural decision making” (p.109), an
understanding of what forms the experience of place where the aesthetic
elements stand out in connection with creative design is particularly
important (Canter, 1997). For this purpose, he points out the importance of
looking at the physical environment by exploring the designer’s view as
well as the researcher’s view. In exploring the designer’s view, it is
necessary to look at the different facets of place and “…the major facets of
designs that the designers manipulate” (p.110). Researchers mainly are
interested in the paradigms of the environment, that is, understanding what
54
they look at and how they look at it is important. Each environmental
understanding reveals different aspects (Canter, 1997) supporting the
relevance of understanding that the factors that characterise a place or
building also influence the human action and exoerience that occurs there.
Canter (1997, pp.110-112) cites the theory of Markus (1982, 1987) and
Saegert and Winkel (1990) to explain the different facets of a place that
influence the designer and suggest some research concepts.
According to these conceptions, the assumption is that designer’s influence
the PE relationship through (1) Function: the task and performance of a
place; (2) Form: the appearance of a place mainly comprising of the
structure and composition of the space and (3) Space: the whole place or
space occupied. These three aspects include only the spatial perspectives
which, in a broader sense, would identify and incorporate the user needs.
Canter (1997) further states that theories that explain PE inter/transaction
and relationship comprise: (1) Environmental adaptation: where the
individual copes with any environmental situation for psychological and
biological survival. The need for survival or comfort motivates their
adaptation capacities. Therefore, an individual’s cognitive capability is of
importance in order to determine environmental capacity; (2) Opportunity
structure: which focuses on the qualities of the environment and how it
could be manipulated to suit the person’s end. It is the “options for action
that the environment makes available and how a person can select or
manipulate settings to make possible those patterns of behaviour, or styles
of life to which they aspire” (p.112). (3) Sociocultural considerations: these
recognise that the environment has a direct connection between social
interactions of an individual. It goes beyond the immediate individual to the
social aspects of the environment. These aspects of the user’s and creator’s
influences indicate that the making of a place and its use are interrelated to
our experience and inter/transactions; designer, researcher and user
categories influence and manipulate each other in a multifaceted way
(Canter, 1997, p. 112).

55
Research in human environment relationships, reactions, and outcomes
reveals several dominant themes. They include psychological and
physiological factors, the effects of the physical environmental elements, the
effects of inter/transactions between humans and certain environmental
stimuli such as psychological and physiological arousal, emotional factors,
sensory awareness and finally the effect on these relationships on health
outcomes.
Many researchers suggest that human reaction and responses to the physical
environment may reflect heritage and cultural factors as well as personal
beliefs and adaptability (Bell et al, 2002). They also speculate that humans
respond to specific environments because of an inherent need, thus
conditioning the human response towards an unconscious preference for
particular settings (Kaplan & Kaplan, 1987; Ulrich, 1983). Other research
suggests that human responses to their surroundings or the place they come
in contact with are personal processes that vary according to many factors,
such as individual experiences, and social, cultural, and emotional
influences (Russel and Snodgrass, 1987; Rapoport, 1990; Canter, 1997).
Finally, an additional body of work focuses on the positive effects of human
well-being derived from direct experiences from the interaction and
transactions with the environments. These researchers examine topics such
as the health outcomes in healthcare settings, healing taking place in similar
settings, and the outcomes of environmental experiences that people come
across (Ulrich et al., 2006). One approach is the sensory awareness affecting
the healing and therapeutic processes. These also include restorative
environments. For instance, there have been numerous studies that show
people prefer natural landscapes over urban views when urban scenes lack
vegetation and water features (Kaplan, 1987; Ulrich, 1983; Korpela, 1991).
Most of these studies use rating scales showing response to visual stimuli,
such as slides or photographs of natural and urban scenes. Cognitive and
affective/emotional responses are assessed and rated.

56
From an integrative health perspective and considering the
psychophysiological outcomes from the environmental relationships
(Parsons & Tassinary, 2002), environmental preferences and restorative
environment theories may be the most dominant. Two of these are Kaplan’s
(1995) ‘attention restorations theory’ which follows a cognitive model, and
Ulrich’s (1983) ‘nature restoration theory’ which follows an ‘affective’ or
emotional model. The ‘attention restoration’ concept suggests that a rapid,
unconscious type of cognition may precede affect or emotion (Kaplan,
1987). Most of Kaplan’s research found that preferred places contained
features that influenced and encouraged the gathering of information and an
understanding of the elements as a person experiences space (Kaplan &
Kaplan, 1982; Kaplan, 1992). While the above mentioned model represents
the perceptive and the cognitive aspects of the PE relationship, the ‘affect
model’ emphasises human aesthetic, affective, emotional and physiological
responses to the physical settings or environments (Ulrich, 1981; 1983;
Ulrich, et al., 1991).
Ulrich (1983) believes that humans respond immediately, unconsciously,
emotionally and physiologically. These processes play a critical role in how
humans respond to the physical environment, its configurations and
elements. These concepts relate to the PE interrelationship integrative health
systems model, which is developed in this study from the PNI framework,
as precedence is given to the emergent human subjective and objective
reactions due to spatial inter/transactions. Furthermore, Pennebaker &
Brittingham (1982) state that certain environmental stimuli can elicit
physiological responses influenced by psychological responses. They state
that, when there is ‘external information’ (stimuli outside the human body),
the ‘internal sensation’ creates an awareness of it which is “directly related
to physiological change” (p.119), these perceptions evolving either
consciously or without deliberation. People may not be aware of the internal
physiological sensations unless it is something contradictory to everyday
encounters.

57
Emotional responses seem to be an innate phenomena and several
researchers propose that feelings are essentially precognitive or that
sensations occur before perception and cognition takes place (Ulrich, 1983).
Ulrich (1981) suggests that the cognitive process outcomes from the initial
emotional reaction are greatly influenced by cultural and personal
experiences and that the affective responses may be expressed as ‘neuro-
physiological’ activity. Exposures to everyday environments may elicit
various effects on human psychological and physiological systems (Ulrich,
1981; Ulrich et al., 1991; Ulrich et al., 2006). Ulrich’s experiments measure
the person’s physiological and psycho-physiological responses (such as
muscle tension, brain waves, heart rate and blood pressure) when
experiencing the physical environment. His results indicate that preferred
environments reduce anxiety and enhance recovery process and stress
responses (1981).
All these studies suggest that the environment consists of several stimuli
that influence the psychological and physiological responses in humans.
Although generalisations can be found within each area of research, it is still
helpful to identify general patterns crossing over environmental perceptions,
cognitive and emotional responses, preferences, cultural influences and
therapeutic and restorative qualities of the occupied space, to understand
their influences on health outcomes. It may well indicate that the results
found for one particular group may apply to other groups and that no single
study by itself can be conclusive. However, as numerous studies provide
similar understandings and concepts, they indicate that direct and indirect
effects may exist. Emotion featured repeatedly in the review, pointing out
that feelings play a role in human psychological and physiological responses
to place and that the physical environment can directly affect or alter
emotions.
In “recognition that the environment is a human creation, that the
environment is artefact…” (Ittleson, 1976, p. 56), this study accepts that
environments potentially have the power to influence the well-being of the
person or people occupying them because the environment (E) can affect
58
health and wellbeing as identified above. As built environment (BE) is
created, it is possible to encompass environmental properties that contribute
to the holistic health and well-being of a person.
With these underlying assumptions, this study adopts an all inclusive
outlook and does not adopt any bias towards any particular theoretical
concept. Before proceeding to Part Two, a brief description of the entity that
characterises ‘Built Environment’ is given.
4.4 Built Environment (BE)
According to Eberhard (2003),
Built environment is more than the buildings and design recorded in
history books. It is more than the special buildings and spaces
designed by architects and designers with significant reputations. It is
more than the visual images most people carry with them after
interaction with place… (n.d.).
Smith (2000) further notes, that P (person) and E (environment) in
relationship is part of environmental situation,
The built E is physical, of particular materials and of particular
appearance or style. The particular understanding of building or
interior E is unique for each individual. Our experiences of the world
are in relationship with the built E. We live these lives largely
unconcerned with what we are doing…at other times, we are aware of
the choices that we are making and we may struggle to make sense of
the situation or negotiate the potential outcomes…we live our lives as
part of a continuum and the built E bounds it in some way. We exist in
relationship with the physical E and with non-human and human
entities (p. 287).
Built environment, for the purpose of this study, consists of the spaces and
places that have been created by humans, for human activities; for now, we
will call the BE the ‘human oriented built environment’. “It includes places
59
where we were born, places where we went to school, where we were
treated for an illness, where we were entertained, where we worshipped,
where we work, and where we live the private part of our life called home
and numerous other areas that we visit during the course of life” (Eberhard,
2003). Stokols (2000), further, emphasises the necessity for understanding
and mapping this ‘human oriented environment’:
The application of theoretical strategies for mapping the context of
behaviour can be valuable, especially during the early stages of
research, as a tool for discovering the situational boundaries of
psychological phenomena, specifying the dimensions on which
diverse settings can be meaningfully compared, and estimating the
applied utility of our theories and policy recommendations before
these ideas and interventions are implemented in costly and
sometimes ineffective manner (p. 139).
The examination of research in BE that is concerned with health and
wellbeing reveals that it consists of a vast range of domains such as
architecture and design, interior architecture and design, landscape
architecture and design, healthcare design, environmental psychology, and
urban panning and design. The discipline of environmental health also
considers BE as among many of the environmental factors. Within the
domains, consideration is given to the interdisciplinary and transdisciplinary
connections including disciplinary connections with psychology, social
sciences, medicine, business, computer technology, public welfare, law and
ethics, and so on.
In this study, focus is given to the psychological, social, and medical aspects
as part of the transdisciplinary investigation of the PE relationship with
health. The following section will further identify the categories and
dimensions from within the areas of research explored, and the ways human
health is considered in the various disciplinary areas of BE and health
research.
60
Part 2
PE inter-relationships with health from domain perspectives
4.5 Results of the review analysis
As explained earlier, the studies were selected according to the criteria
established and described in the methodology chapter. The initial search of
data bases and monographs (using broad terms) yielded a total of 832
possible studies to be included in the review. A broad key word search was
implemented because specific keywords that pertain directly to health and
BE, produced only a limited number of studies. Following the evaluation
process previously described, 343 articles and monographs out of the 832
were selected for closer review. This process eliminated another 146 articles
for any of the following reasons: the article was not research based; the PE
relationship was not considered within the integrative systems parameters
even if implied in the abstract; or the study was not about the built
environment but only the general social environment.
In the end, the evaluation process produced 197 studies including journal
articles, monographs and dissertations. All 197 studies were numbered,
identified as belonging to various dimensions of BE and health research,
and sorted according to the matrix categories outlined previously (Tables 1
and 2).
4.5.1 Consideration of integrated health in BE and health research
This section presents findings that address the first two research questions.
These are:
1) In what ways have health, environment, and their inter-relationship been
conceptualised by researchers from an environment-design perspective; and
2) In what ways have health, environment, and their inter-relationship been
conceptualised by researchers from a medical-health perspective?
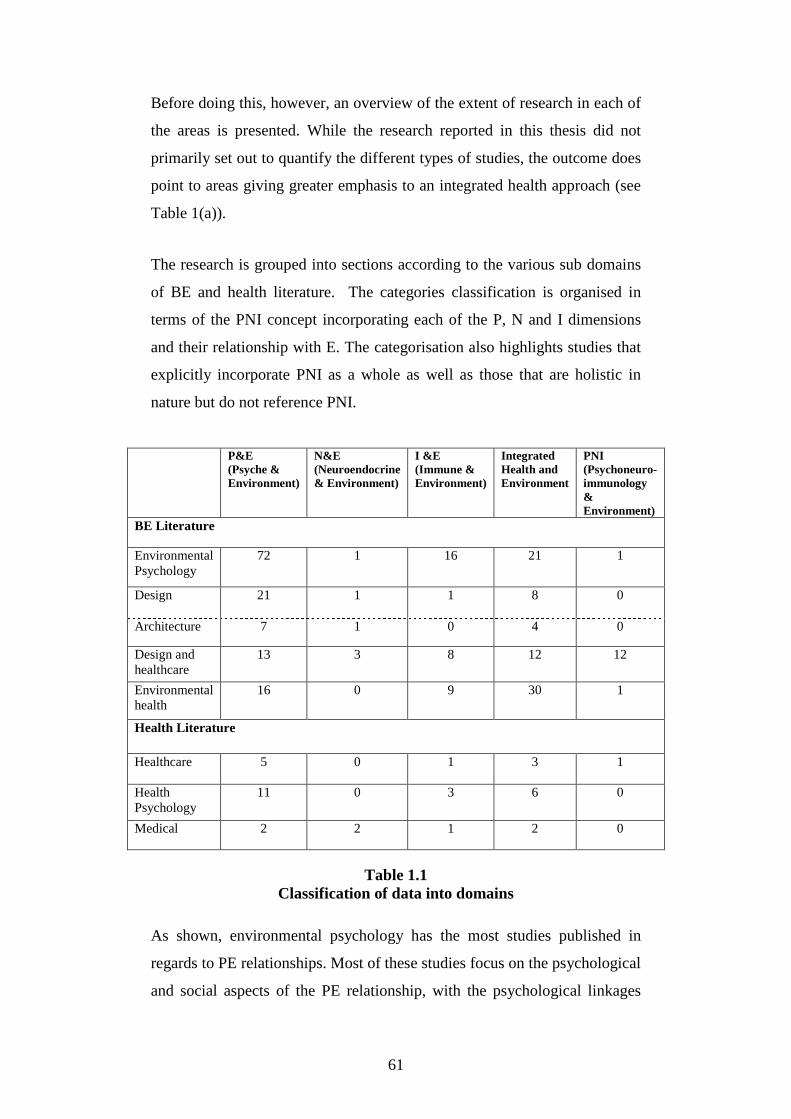
61
Before doing this, however, an overview of the extent of research in each of
the areas is presented. While the research reported in this thesis did not
primarily set out to quantify the different types of studies, the outcome does
point to areas giving greater emphasis to an integrated health approach (see
Table 1(a)).
The research is grouped into sections according to the various sub domains
of BE and health literature. The categories classification is organised in
terms of the PNI concept incorporating each of the P, N and I dimensions
and their relationship with E. The categorisation also highlights studies that
explicitly incorporate PNI as a whole as well as those that are holistic in
nature but do not reference PNI.
P&E (Psyche & Environment)
N&E (Neuroendocrine & Environment)
I &E (Immune & Environment)
Integrated Health and Environment
PNI (Psychoneuro- immunology & Environment)
BE Literature
Environmental Psychology
72
1 16 21 1
Design
21
1
1 8
0
Architecture 7 1 0 4 0
Design and healthcare
13 3 8 12 12
Environmental health
16 0 9 30 1
Health Literature
Healthcare 5 0
1
3
1
Health Psychology
11 0 3 6 0
Medical 2 2 1 2 0
Table 1.1
Classification of data into domains
As shown, environmental psychology has the most studies published in
regards to PE relationships. Most of these studies focus on the psychological
and social aspects of the PE relationship, with the psychological linkages

62
forming an important part of the PE/health relationship. In particular,
environmental psychology “is more broadly concerned with
conceptualizing, measuring, and evaluating complex environmental settings
such as buildings, neighbourhoods, and public spaces and the ways these
influence behaviour health, and well-being. Environmental psychologists
consider health to be more than the absence of illness or injury and, to
include both physical and psychological well-being, or wellness” (Stokols &
Clitheroe, 2005, p. 9).
By comparison, there are only a few studies in architecture and design that
focus on health and these are mainly concerned with the physical
environment as a source of stimuli, with the potential to inform an
integrated health approach. Health care studies, of course, focus more
directly on the setting and its relationships to health. As will be shown,
these studies are somewhat limited because they are mainly conducted in
environments with people already under duress, rather than in situations that
are of an everyday nature.
Environmental health is another area that is concerned with certain aspects
of health and the environment. As Table 1.1 shows, it considers health and
environments in a more integrated way or, in other words, more holistically.
Moving beyond climate and pollution, it now incorporates the broader issue
of environmental sustainability. As environmental sustainability is
simultaneously connected to BE, this is an important aspect to be considered
in regards to integrated health and wellbeing. A recent publication on
environmental health by Frumkin (2005) gives an overview of the
categories considered in the area of environmental research. Health
consequences relating to the environment are looked at both from macro and
micro levels, and in terms of global to local implications and inferences.
On the macro level, there are government initiations to help promote healthy
cities; these include dealing with environmental determinants such as
pollution, transportation, water and so on (Galea & Vlahov, 2006). Galea &
Vlahov (2006) note initiatives such as including ‘Moving to Opportunity for
63
Fair Housing (MTO)’ and the ‘Healthy Cities movement’ by the World
Health Organisation (WHO). The MTO program’s findings illustrate some
positive impacts on health and wellbeing when occupants were moved from
poverty stricken neighbourhoods to better neighbourhoods. They report less
“distress, depression, low anxiety levels and dependency problems” among
the occupants in the better housing conditions (Galea & Vlahov, 2006, p.
408). The project by WHO is on an international scale, encouraging national
and local governments to improve environmental conditions to improve the
existing environmental ‘determinants of health’ (Galea & Vlahov, 2006).
Through these examples, they state that it is important to identify urban
characteristics that impact health and argue that the urban level should be
identified on “multiple levels - features of population, the physical
environment, the social environment, and urban service provision - and to
determine how these characteristics interact to affect health and disease”
(Galea & Vlahov, 2006, p. 409).
On the micro level, building quality and its consequences for health are the
main areas of consideration. Hodgson (2006) states that ‘indoor
environment quality’, which is the base of ‘building related health’,
“presents a challenge to occupational and environmental health
professionals...first[ly] it involves exposures that cross over occupational
and nonoccupational settings. Second, little formal regulation exists.
Although recommended guide lines have been established by several
organizations these are nonenforcable guidelines, often lack a scientific
basis, and do not address a substantial number of important
pollutants...[b]uildings and indoor environments in general must be
examined to determine whether they were built and function as designed”
(p. 626).
Tickner (2006) suggests, in preventing future occurrences of diseases
(‘primordial prevention’), ‘action’ should be taken, based on what is
understood about the future and what is supposed to happen in the future (p.
853). He also states that “ Our capacity to identify adverse human health or
environmental effects is limited by the present state of scientific
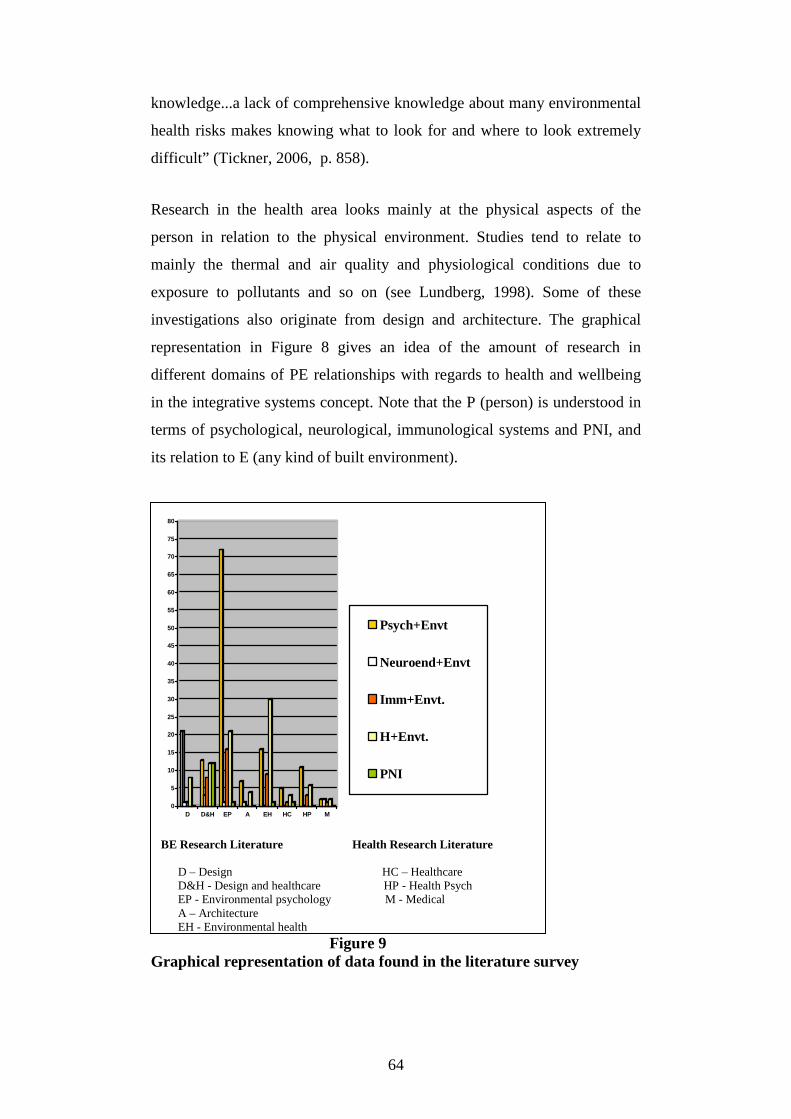
64
knowledge...a lack of comprehensive knowledge about many environmental
health risks makes knowing what to look for and where to look extremely
difficult” (Tickner, 2006, p. 858).
Research in the health area looks mainly at the physical aspects of the
person in relation to the physical environment. Studies tend to relate to
mainly the thermal and air quality and physiological conditions due to
exposure to pollutants and so on (see Lundberg, 1998). Some of these
investigations also originate from design and architecture. The graphical
representation in Figure 8 gives an idea of the amount of research in
different domains of PE relationships with regards to health and wellbeing
in the integrative systems concept. Note that the P (person) is understood in
terms of psychological, neurological, immunological systems and PNI, and
its relation to E (any kind of built environment).
0
5
10
15
20
25
30
35
40
45
50
55
60
65
70
75
80
D D&H EP A EH HC HP M
Psych+Envt
Neuroend+Envt
Imm+Envt.
H+Envt.
PNI
BE Research Literature Health Research Literature D – Design HC – Healthcare D&H - Design and healthcare HP - Health Psych EP - Environmental psychology M - Medical A – Architecture EH - Environmental health
Figure 9 Graphical representation of data found in the literature survey

65
In summary, Table 1.1 proposes that the major area of study involving the
environment in the health context is the psychological dimension. This
appears to be the case in built environment literature as well as health
literature. The table also shows a tendency towards relatively high number
of studies considering holistic health. The only area of note that explicitly
considers PNI or uses the term PNI is the design and healthcare area. Using
this as a background the discussion now turns to a description of the studies
which are representative of the various categories and of the nature of the
relationship between P and E. The location on the matrix (Table 1) of each
of the categories is indicated at the beginning of the relevant section. The
relevant domain being discussed in the section can be identified by the
highlighted segment. For example, the immediate following section
identifies research in the area of the psychological (P) dimension of person
environment (PE) relationship. Therefore, P&E is highlighted to reflect this
in Table 1(a). The rest of the sections are similarly identified and discussed
accordingly.
4.6 Psychological dimensions of the PE relationship
P&E
N&E
I&E
Integrated &E
PNI &E
BE Literature
Environmental Psychology
Design
Architecture
Design and healthcare
Environmental health
Health Literature
Healthcare
Health Psychology
Medical
Table 1(a) Classification of data into domain P &E

66
Psycho
Physio
BE
This section introduces the psychological dimensions that emerged from the
review relevant to research in BE as conveyed in Figure 10. These are
environmental perception, cognition, arousal, emotion and stress. A person
comprises different essential components that integrate to form a ‘whole’.
The brain and psychological experiences, the body and the physiological
systems, contribute to the ‘whole’. Environmental interrelationships with
the psychological system involve the external situations that the person
responds to. The resultant experiences include everything from the time a
person has contact with the environment through processes such as
perception and cognition (Altman & Rogoff, 1987; Gifford, 1997; Bell et
al., 2001). As the following discussion will show, most of the studies
reported are based on some understanding of this. The discussion also
explores the psychological reactions of emotion and stress and/or stressors.
Figure 10 BE + Psychological systems interrelationship
Perception and cognition
Where the environment is concerned, perception and cognition play a
significant part in the experience of place and space. These reactions are
related to one’s sensory appraisal of surrounding stimuli (Zimbardo &
Gerrig, 2002). Cultural background, character, personality, and
expectations combine with perception and cognition to define one’s
experiences (Gifford, 1997). Without being able to perceive or cogitate, the
person cannot interact or transact with the environment. In other words,
without perceptive and cognitive abilities, a person cannot experience the

67
environment. How a person perceives the environment is not always in a
conscious way, but mostly on an subconscious level, without essentially
being aware of the surroundings (Zimbardo & Gerrig, 2002).
Psychological studies exemplify perception as the interpretation of the
sensory feelings derived from stimulants that a person comes in contact with
(Zimbardo & Gerrig, 2002; Bell et al., 2001). Zimbardo & Gerrig (2002)
state that “The term perception refers to the overall process of apprehending
objects and events in the external environment- to sense them, understand
them, identify them, and prepare to react to them” (p.135). Studies such as
these regard cognition as the interpretation of a person’s perception or the
processing of that information in an intelligent way. Other studies however
use perception and cognition as overlapping meanings; perception can be
related to cognition in a more encompassing, holistic and iterative sense
(Bell et al., 2001). “It [cognition] integrates memory and experience with
the judgement of the present derived from perception to help us think about,
recognize, and organize the layout of an environment” (Bell et al., 2001, p.
95).
Arousal
Arousal is the reaction to certain stimuli within the environment. It can be
related to psychological or physiological outcomes. Physiologically, arousal
could be measured through the heart rate, blood pressure levels, sweating
conditions and so on. Psychologically, however, it is measured through the
‘neurophysiological’ reaction of the brain: “…arousal is a heightening of
brain activity by the arousal center of the brain known as the reticular
formation” (Bell et al., 2001, p. 103). Arousal could be negative or positive
and may arise from pleasant or unpleasant stimuli causing direct and
indirect behaviour changes (Bell et al., 2001).

68
Emotion
Human beings are constructively and sometimes unconstructively
emotional. Feelings can be the result of the social environment or of the
physical environment (Wapner, 1987; Levi, 1987).
Health literature refers to emotion as:
a relatively brief episode of coordinated brain, autonomic, and
behavioural change that facilitate a response to an external or internal
event of significance for the organism…feelings are the subjective
representation of emotions…they can reflect any or all of the
components that constitute emotion (Davidson et al., 2003, p. xiii).
Environmental literature refers to an emotional episode as:
An emotional episode is a gestalt that consists of component events,
including environmental, mental, physiological, and behavioural
changes…emotional response to an object depends on the level in the
hierarchy in which he or she categorizes it (Russel & Snodgrass,
1987, pp. 245-280).
Emotions range from negative emotions such as anger and pain to positive
emotions like joy and love. Natural factors like air, water and place play an
important role in the psychology of humans influencing such things as
moods, relationships, and memories (Frumkin, 2006). In exploring
environmental conditions that are related to emotional factors it is necessary
to look at ‘stressful’ conditions in the environment.
Stress
Stress is defined as
… the internal mental state of tension or arousal…interpretive,
emotive, defensive, and coping processes occurring inside the person.
69
Such processes may promote positive growth or produce mental strain
(Rice, 1987, p. 20)
The response to stress varies greatly between one individual and another.
Levi (1987) explains that interaction between person and the multi-faceted
environment in its all encompassing context, causes certain reactions,
resulting in stressful conditions affecting health. He says:
…the interaction between, or misfit of, environmental opportunities
and demands, and individual needs and abilities, and expectations,
elicit reactions. When the fit is bad, when needs are not being met, or
when abilities are over or under taxed, the organism reacts with
various pathogenic mechanisms …and in the presence or absence of
certain interacting variables, they may lead to precursors of disease
(Levi, 1987, pp. 9-14).
Responding to stress can result in one’s own destruction through
‘alcoholism, drug abuse, excess cigarette smoking, and obesity through
consuming food’ (Levi, 1987). Long term effects of ‘mismanaged stress’
can affect the society, home, work life, social life and relationships.
Knowles (1997) aptly says that most of us are born healthy and become sick
as a result of personal misbehaviours and environmental conditions
(‘environment’ refers to social environment here). In our society an
individual is sometimes expected to go on without showing any stress or
distress or any signs of weakness, often becoming more stressful as a result
of defiance. When an individual remains in a stressful condition for a long
time, it becomes difficult for the resistance to be maintained and this
weakens the resistance to disease (Rosenmann, 1994).
Henry & Grim (1990) state that “Our knowledge and technology have not
given adequate attention to man’s affective and moral form, or to his inner
self, character and aesthetic, or psychological needs and relationships to
mental and spiritual environment” (pp. 783-793). This relates to Dennehy’s
(2003) observation that our psychological characteristics are interdependent
of the surrounding environment (physical and social) in such a way that the

70
environment affects the ‘psyche’, and our ‘psyche’ determines our
involvement with nature.
In the next section, we continue this exploration of the psychological
dimension as it is understood in the various discipline domains.
4.6.1 BE Research - Environmental psychology
Environmental psychology regards the psychological aspects of
environment in terms of the person’s cognitive and emotional responses
from interacting and transacting with the environment. These include
everything that a person experiences when s/he encounters the physical
space/place, and involve perception and cognition of the surroundings;
subjective and factual absorption of percept’s; reacting to the degree of
understanding gained; consideration of action, immediate action and
reactive/considerate action (Gifford, 1997); and social aspects that influence
the mind.
Reactions to places are different from person to person because people are
diverse in character and likings, and vary accordingly in their responses to
place. For example, some people like the crowds, excitement and structuring
of urban environments, but others seem to prefer the quiet and calm
atmosphere of the countryside. Many factors affect the person when
choosing and liking a place. They include their heritage, cultural upbringing,
socioeconomic status, sense of belonging and worthiness: all these and
many other factors influence the experiences of place (Eyles, 1985;
Weinberg, 2001).
Places can evoke memories, arouse emotions, and excite passions (Walter,
1988; Lippard, 1997). This is further reinstated by an extensive review of
literature on clinical and environmental psychology undertaken by Anthony
and Watkins (2002) which reveals the importance of an interdisciplinary
approach. They state that one of the most noticeable examples of how
place/space or the physical environment affects human psychology would
be the effect and memory of place in trauma victims. Emotions are part of a
71
person and studies on trauma victims showed that they often associate a
place with traumatic happenings. Another place similar to one which in the
trauma took place is enough to remind them and could result in a phobic
reaction. In such a situation, the physical environment is seen as being a
stimulus that elicits a response. Both the environment and the human psyche
act together as “conditioned stimuli” (Anthony & Watkins, 2002, p.131), as
a result of the trauma. Such exposure elicits a reaction or response. The
sight, sound or smell of a traumatic environmental experience is enough to
trigger a negative reaction (Anthony & Watkins, 2002).
The physical environment stimulates certain elemental faculties of the
individual. Environmental factors have a positive or negative impact on the
person, depending on individual needs. This impact called the
‘environmental press’ was initially developed by Lawton (1975) to describe
environments for the elderly. A person interacts with the environment based
on the press an environment poses and the capacity he/she has to cope with
it. This depends on the level of dependency the person enforces on the
environment or the level of environment determinacy. If the environmental
demands are on a high or low level and if the person cannot cope with them,
negative emotions may be the resultant outcome. Positive feelings result
when the ‘press’ is within the coping limit of the individual (Lawton, 1975).
This theory can be viewed in terms of coping mechanisms described in
health and medical literature (see Rice, 1987; Williams, 1994).
Wong and Peacock (1994) have described three approaches to the study of
environmental impact on human well-being. These approaches focus on:
1. The objective characteristics of the environment such as noise,
temperature, air quality, and so on, mainly focusing on the physical
aspects of the environment;
2. Subjective response of the human being such as the “meaning and
significance of social and physical milieu in which they function”
(p.61); or

72
3. The meaning of interaction between the person and environment
incorporating the characteristics of the environment, and the
personality factors, needs, and competence of an individual.
Research on environmental stressors – mostly done in workplace
environments – points to noise, temperature levels, ventilation, exposure to
outdoor climatic conditions, vibration, lighting, hygiene, and crowding, as
affecting the wellbeing of individuals according to their age, gender, past
experiences, values, beliefs, values, cultural needs and character (Sutherland
et al., 1994). A paper presented at the APA Symposium (Anthony, 1998)
presents a review of various design issues that appear important in a
psychotherapist’s offices to influence the behaviour of visiting clients.
Features like location, image, degree of visibility, proximity to rest room,
privacy, easy - to - read clocks, entrances and exits, furniture, lighting,
views, plants, and artwork may cause irritation and worry in clients with
pre-existing conditions for better or for worse. There are many existing
studies that reveal the importance of place in clinical settings (Arneill &
Beaulieu, 2003).
Even if the environment is not agreeable to the person’s experience, it is the
way the person perceives the place and copes with the negative factors
which would eventually influence the physiological system (Rosenman,
1994). Not all factors in the environment can be called stressful in the
integrative sense. Certain environments such as beautiful landscapes,
comfortable homes and an aesthetic and user friendly workplace can be
benign and uplifting (Kaplan & Kaplan, 1990). While environments can
function as a
…moderator against the negative impact of stress…words like retreat,
haven, and sanctuary readily come to mind when we think about
places where we can find temporary refuge from the storms of life
(Wong & Peacock, 1994, p. 59).
These positive attributes (for example, extreme excitement and happiness)
contribute to the well-being of a person. Stress can originate from several
73
internal factors such as social and cognitive elements, as well as external
environmental elements. Findings from the study done with the elderly
suggest some important facts of environmental stress. They emphasise the
importance of taking the “psychological atmosphere” of the environment as
a very important consideration when designing for the elderly (Wong &
Peacock, 1994).
A pleasant environment significantly contributes to the wellbeing of the
people occupying it. Wong and Peacock (1994) used Lawton’s model to
measure “environmental press” on wellbeing and their study revealed that
people with higher IQ levels were more able to cope with adverse
environmental conditions than people with low IQ levels. Their study
indicated that environmental factors play an enormous role in mental
wellbeing. Elderly people of different demographics were studied for
mental health in relation to the environment and atmosphere they lived in
and it was determined that the (a) social atmosphere (co-inhabitants), (b)
activities that take place in a setting and (c) physical factors of an
environment such as the aesthetics, thermal, acoustic qualities and so on
influenced mental well-being by creating a happy atmosphere (Wong &
Peacock, 1994).
Another major area of study of relevance is ‘environmental control’, which
is understood in two ways. One understanding is where the person has
control over the environment; the other is where the environment has
control over the person. The feeling that the environment that is being
occupied can be controlled helps develop a confidence in the person
occupying it (Bell, et al., 2001). They cite Averill (1973) who explains
control as (a) ‘Behavioural control’ where it is possible to change our
behaviours according to the negative or positive environmental aspect; (b)
‘Cognitive control’ where we understand the consequences of a stressor or
environmental aspect (for example, the person tries to cognitively judge a
situation and takes the decision to view it so it looks less threatening); and
(c) ‘Decisional control’ is the person’s own choice where he/she has control
over the environmental aspect and can make a decision according to

74
preference. The perception of control is often significant in behaviour and
reactions (Bell et al., 2001, pp. 114-116). For instance, levels of noise affect
work performance less if they can be controlled according to individual
satisfaction (Cohen, et al., 1991). A traditional class room was redesigned
into a soft room with different adjustable lighting and furnishings by
Sommer and Olsen (1980). The changed environment increased the number
and participation of students in the class significantly when compared with
traditional classrooms. Students seemed to appreciate it more (Sommer &
Oslen, 1980, as cited in Wong et al., 1992). Seventeen years later when it
was further evaluated by Wong and colleagues to assess whether it still had
the same influence on students, they found that it produced the same results
(Wong et al., 1992).
Suedfeld (1987) researched various environmental extremes with different
people and gives many examples of diverse environmental situations. He
reports that external environmental factors that lead to mental stress can, in
turn, lead to extreme situations where a person makes wrong decisions as a
result of the exposure, resulting in accidents, suicides or other physical
conditions. Different situational aspects – as people involved in shipwrecks,
people in the army and so on – here studied and found that, when exposed to
conditions leading to stress, their behaviour changed dramatically. He
reports the suicide of a lone-yacht racer as a result of one such
environmental influence. This person’s mental stress as a result of cheating
in a race led him to commit suicide. Suedfeld (1987) reflects that the sailor’s
judgment could have been impaired as a result of in his long travel, resulting
in his making a wrong assessment. This is evidence of people being prone to
‘dramatic behavioural disturbances’ after prolonged exposure to extreme
environmental conditions. Some of these disturbances culminate in chronic
conditions such as ‘cabin fever’, a behaviour that manifests as a result of
being confined indoors due to extreme climatic conditions such as strong
winds, snow, extreme cold and so on. Another example is ‘cafard’, a form
of hysterical behaviour often culminating in homicide or suicide. This
condition is often found in soldiers confined to an outpost, enduring severe
75
environmental conditions like heat, sand storms, severe discipline, crowding
and frequent danger (Suedfeld, 1987).
The above mentioned conditions depends on the person, his/her mental and
emotional circumstances, personality factors and acquired or hereditary
influences. A person’s emotional experiences in the built environment
depends on the quality of space, the condition the person is in, the reason
the person is occupying the space and many other reasons. The environment
can serve as a stimulant of emotion. Some environments can provoke strong
emotional reactions compared with others. Moreover, it is important to note
that the environment can act as a stimulus also when a person is in a relaxed
state (Russell & Pratt, 1980) because relaxation invokes pleasure.
People experience and associate different emotions with diverse
environments. Research indicates that “when individuals encounter
environments that are too predictable and too controllable, they experience
those settings as boring and unchallenging” (Kaplan, 1983, pp. 311-322)
and that people prefer environments that offer opportunities for exploration
and for acquiring new information and skills (Kaplan, 1995). The
environment and person are interrelated in such a way that the action of the
person influences the environment and the environment influences the
action and behavior of the person (Bonnes & Bonaiuto, 2002). Thus, person
and environment are interdependent.
Human behaviour is considered to be the result of the physical environment;
hence, studying it by the response of the psyche to the environment
(Stokols, 1978) reveals the interactions and transaction between person and
environment. The space occupied is related to the reactions and behavior of
a person (Stokols & Altman, 1987).
In usual circumstances, a person is not aware and cannot recognise the
influence of the physical environment on his/her ‘behavior and experiences’
and it is through ‘objective analysis’ that this is revealed (Proshansky &
Fabian, 1986).

76
Wapner (1987), adopting a transactionalist point of view, states that many
aspects of the person and environment are mutually defining and an
ecological environment becomes psychologically relevant only through the
actions and experiences of the people living and acting in it (Wapner, 1987;
Wapner & Demick, 2000). In other words, people do not react to an
environment; they react to what they “perceive, think or feel” (Graumann,
2002, p. 99) in response to the environment; only when they experience the
physical environment and act upon it does the place acquire meaning.
Hence the place we live in is not only the space and spatial objects
that we act upon but inevitably the lifespace as acting and reacting on
us (Graumann, 2002, p.102).
The meaning of the various elements is achieved implicitly, by doing, not
by verbal communication. In other words:
…it is the shared performance that makes things signify something,
that makes lived space into an environment that can be experienced as
a special lifespace (Graumann, 2002, p.102).
The person acts according to the cues the environment provides, with the
environment bearing the impact of the person’s reaction. The physical
elements within the physical space play a large part in providing these cues.
The implication that the décor of a room suggests the occupant’s personality
and the way he/she would want the visitor to behave, exemplifies the
environment providing cues to the user; “whereby people judge or interpret
the social context or situation and act accordingly”(Rapoport, 1990, p. 57).
“It is the social situation that influences the people’s behavior, but it is the
environment that provides the cues” (Rapoport, 1990, p. 57). People act
differently in different settings and they react differently to various social
situations. “When the environmental code is known, behavior can easily be
made appropriate to the setting and the social situation to which it
corresponds” (Rapoport, 1990, p. 58). “People react towards objects and
people on the basis of the meaning which these have for them” (Rapoport,
1990, p. 59). Furthermore people interpret these meanings differently and

77
these interpretations plays a critical role in environmental interaction
(Rapoport, 1990). “Material objects first arouse a feeling that provides a
background for more specific images, which are then fitted to the material
and in the case of environments affective images play the major role in
decisions … and causing direct and indirect effects” (Rapoport, 1990, p.
60).
This is reinforced by Stokols and Montero (2002). They describe how, when
connecting to the environment, people try to “establish and maintain
meaningful psychological and social connections with the material world,
reflected in their strong emotional attachments to particular objects and
places…to optimize the degree of fit between environment and person”
(Stokols & Montero, 2002, pp. 661-675). Human beings have a tendency to
form an attachment to certain places through identification of the
surroundings, sometimes through the objects within the environment. These
places that they form an attachment with play a special part in developing a
self-identity. For example, in home environments, the bedroom is a key
space for “territorial and privacy conflict area”, followed by the bathroom,
kitchen and living area (Anthony, 1984).
These psychological factors also relate to the reaction of a person to the
physical attributes within an environment and how s/he looks at certain
elements. For example, a person’s perception of thermal quality and body
requirements differ in people according to individual demographics, mental
state of acceptance/denial and responses (Dorn, 1994). For example, when
some people find the air-conditioning just right, some may find it either too
warm or cold. In addition, there are also social and cognitive aspects to the
psychological dimensional attributes of spatial elements. Research implies
that organisational structures and stress free relationships in the habitats
form a better relationship with their surroundings. Dorn (1994) also argues
that there is a rising debate among researchers on the causes of ‘sick
building syndrome’. This syndrome, they argue, may be the result of the
actual physical elements of the environment or the result of the perception
and coping skills of people in that environment.

78
Studies undertaken on spatial organisation and workplace satisfaction
demonstrate the importance of the role of space allocation and organisation
in the satisfaction and performance of people in a workplace. They point to
a link between the social activities of people and the spatial organisation of
the physical environment which supports individual process as well as
fostering team communication and collaboration (McCoy, 2002).
Many studies suggest that places affect our performance as we work and
study and generally live. Some places promote our social skills and help us
connect with other people (see Oldenburg, 1989; 2000). Some environments
impact on and influence people’s mental well-being through their stressful
and emotional conditions. The capacity of restorative environments to
enhance health and well-being is widely acknowledged (Ulrich, et al., 1991;
Kaplan, 1995; Kaplan & Kaplan, 1989). Prime examples are studies of
people occupying windowless offices. It was found that the users of such
spaces tend to use more natural themes as decorative elements and they
incorporate more visual stimuli than people with offices having windows
(Heerwagen, 1990). Another study involving three groups of office workers
indicated that people having views of nature are more satisfied with their
work, having lower level of stress than people having views of buildings or
having no view at all (Kaplan, et al., 1988).
Another significant visual element in the physical environment is colour
which has the power to affect emotions ranging from calming and soothing,
exciting and stimulating, anxious and depressing (Mikellides, 1988). The
hues, values and intensity in colour stimulate certain moods and emotional
responses (Venolia, 1988; Kwallek & Lewis, 1990; Valdez & Mehrabian,
1994; Hemphill, 1996). Light is another visual factor that plays an important
role in psychological and physiological functioning. Gifford (1988) states
that lighting levels and room décor can influence interpersonal
communication, comfort, and arousal levels. The deprivation felt by people
who have no design details in their workplace lead to a number of
behavioral responses, resulting in less social interaction, complaints to
anxiety. This can eventually lead to the person quitting the organisation.

79
Spatial mapping for way finding is an area where a wide range of study has
been conducted and applied. It has been concluded that good signage
reduced the complexity of way finding for visitors and patients alike in
hospitals and many hospitals provide simple wayfinding maps in complex
buildings (O’Neill, 1991).
Mazumdar (1999) describes several potential areas of research including
technology, people and physical environment as to how people
accommodate their lifestyle and work for technology. Mazumdar (1992)
agrees that the emotions connected with the physical environment can be
intense. For example he describes ‘environmental deprivation’ as a
phenomenon where lesser quality elements replace essential environmental
elements affording a feeling of discontent (Mazumdar, 1992, p. 692). He
also makes the connection between productivity and emotional factors in the
workplace environment. He implies that the environment has become more
of a formal setting and that people accommodate their lifestyle and work for
technology. Anything can be accessed through the computer and, as a result,
communication among people has reduced. The potential areas of research
include: ‘the effect of culture on individual, physiological characteristics,
psyche, choice, preferences and cognition’, space and territory incorporating
social relations, environmental hazards, pollution and the emotions of
people when they shift to a new territory (Mazumdar, 1999).
Korpela’s (1991) study of the effect a favourite place plays on the
restorative functions of an individual found that people seek out their
favourite places when they have negative feelings. These places were seen
to help them calm down and help them bring their feelings and thoughts into
perspective and as a result help them to recover from bad moods,
establishing in turn that physical environments play a definite role in
regulating and controlling the mind. Francis & Cooper (1991) also studied
the type of places that an individual goes to when feeling low and depressed
and what these places do for the emotional well-being of the person. Good
views, water, vegetation and public settings were identified as enhancing the
moods of people, concluding that nature can reduce stress. Another study
80
conducted by Betchel & Korpela (1995) illustrates that spatial elements vary
in their emotional influences. Their study found that institutions can be the
most depressing as well as happiest places the participants had encountered.
Homes were mentioned as the second highest source of happiness.
4.6.2 BE Research - Design and architecture
Although the literature described in the previous section originates from
environmental psychology, many researchers have made reference in their
studies to architectural and interior dimensions. In design and architecture
research, the environmental elements and stressors on the psychological
well-being of the person using the place that have been identified are mainly
related to the senses and the emotions and feelings. The interdependency of
the person and environment is also an important aspect including such
things as privacy, control and territoriality factors. Mental well-being in an
environment may be related to the satisfaction that the person gets from
occupying a place.
Canter (1974) (as cited in Malnar & Vodvarka, 1992) categorises three
psychological factors that should be taken into consideration by designers.
These include understanding “activity requirements...what, when and how
people do things...and how they [the different activities] change over time;
relative values...determining design priorities based on finite resources;
environment behaviour relationships...the variables that influence human
behaviour” (p. 21). It is further stated that theoretical aspects are to be
incorporated within practice and application to create a ‘human
environment’ which requires “expertise of many people from diverse fields”
(p. 296). Several factors that are beneficial to the constructive activity of
designing a space are identified. These include:
• form, function and shape: the structural aspects which should be
looked at in terms of the user and why and how they intend to use a
space;
81
• organisation of space: which contains many ‘elements’ that give
meaning to the sensory aspects such as visualization and texture;
• ‘determinants of space’: differs relatively from person to person with
regards to socio-cultural and need aspects;
• conceptual constructs: pre-examined details in application;
• geometrical proportions: symmetry, scale, perspective and planning;
theoretical considerations;
• ‘systematic applications’: involving the sociocultural and aesthetic
considerations in implementation;
• types of spaces and buildings: their purpose and functionality and
• ‘human dimension’: physical, social, psychological, cultural
usability factors (see Malnar & Vodvarka, 1992 for a full
description).
In terms of psychology and design, the way a person experiences place may
be an important factor that helps us understand PE relationships. Lawton
(2001) suggests that, in order to understand the experiences of place, we
need to see interaction in consensual as well as objective and subjective
terms. People usually see to it that their personal needs and /or desires and
environmental resources are synchronised and this is associated with both
‘efficacious behaviour’ and favourable affective outcomes contributing to
their wellbeing which, Lawton states, represents the quality of life (QOL)
(Lawton, 1989). Though mainly concerned with geriatric studies, his
approach is based on the relationship between research and practice in the
same way as Lewin’s action research, and recognises that research findings
on people interaction with the environment are not readily applied in design
practice (Lawton, 2001).
Forrest (1999) and colleagues developed a set of assessment tools to
determine the satisfaction of a person occupying a place; these tools help in
evaluating the environmental qualities that a person believes cultivate
positive emotions. The tools help to create environments that are pleasing
for the occupants in terms of self-respect, privacy, social relationships, sense
of control and positiveness about the future. These three tools comprise the

82
developmental history of place, objects and favourite place. They help the
clients in recalling the places where they lived and the important events
occurring there, favourite objects they love, and their favourite places.
Understanding these, allows the designer to incorporate factors that pertain
to the satisfaction of the clients (Forrest, 1999).
The designer needs conceptual understanding, not only of design elements
such as form and structure or creative concepts. Design requires an
integration of the human aspects of the interior environment such as human
responses and behavior within the space. This is part due to
interrelationships between the spatial design and the physical environment
and how these affect human behavior in terms of interdependency and
determinism (Bell et al., 2001). This is further illustrated by Miller and
Schlitt (1985) in their concept of the ‘over designed’ and the ‘under
designed’ space. Their concept is that when ‘under designed’ space is
designed for comfort without being overbearing, the ‘over designed space’
is designed as a work of art, leaving little room for people to change it
according to their taste. This space has to be adapted to, which may prove to
be somewhat taxing for some people. The under designed space provides
comfort and optimal design features that allows the person to change it
according to individual liking, allowing the person have control on the
environment, whereas the over designed space controls the person (Miller &
Schlitt, 1985).
The implementation of Universal Design (UD) in specific environments also
relates to the design and creative process that take into account the outcomes
of some specific PE transactions that influence the behaviour and
experiences of people. The sociocultural as well as the elemental factors of
the physical space are taken into account when applying design principles.
The principles of UD demand that the products and environment are
equitable, flexible, simple and intuitive to use, and easy to perceive, tolerant
to error, require low physical effort, and are better sized and arranged to
accommodate all users (Danford, 2004).
83
Human senses are a significant aspect when interacting with the built
environment. People interact with a designed setting through the visual,
auditory, tactile, olfactory and kinaesthetic senses producing psychological
and physiological responses (Zeisel, 1981). There are some senses that we
cannot shut off even if we need to. Sense of smell is one of them. However,
no two individuals sense in the same way. Sensual perceptions and feelings
differ from individual to individual in many ways. Every individual creates
an awareness of the surroundings through the senses. Colour, a main factor
in visual sensing as well as giving identity to the environment, has been
reported to promote human adaptation to the environment and enhance
spatial form (Ching, 1996). The hues, values and intensity in colour provide
stimulation to certain moods and emotional responses (Venolia, 1988;
Kwallek & Lewis, 1990; Valdez & Mehrabian, 1994; Hemphill, 1996).
Most research done in work place environment settings show different
aspects of the physical place that are favourable or unfavourable for the
mental health and well-being of the occupants and people working in them.
This complements research on the importance of the social aspects of the
workplace settings (McCoy, 2002) in environmental psychology research.
The importance of workplace design for the benefits of individual needs and
organisational costs may be supported by the use of imagination in creating
a space where visual dimensions can also influence an individual’s self
satisfaction and feelings in an environment (Becker & Steele, 1995). Sound
is considered to be the most consistent stressor in office and workplace
environments, especially with the open office planning systems. Bad
acoustics are seen as reducing productivity in people working in such
offices (Tiernan, 2002). A study conducted on windowless offices found
that occupants who had no windows considered ‘space personalization’ as
more essential than doing something else to recompense for the lack of
windows (Biner et al., 1993).

84
4.6.2.0 BE Research: Design and healthcare
Many of the architecture and design factors detrimental to mental well-being
have been illustrated in the design and architecture section. In healthcare
design and architecture, visual elements (that influence the senses, privacy,
control and aesthetics) and social aspects (that foster relationships and
interaction) are regarded as being most crucial to health and well-being.
Also it is encouraging to note that the reference guide of the Coalition for
Health Environments Research (CHER) (2003) recognises the need for
understanding colour in healthcare environments, stating the importance of
sociocultural factors such as geographic location, systems, practices, culture,
age, condition, and personal experiences in people’s perception of colours.
Visual implications that positively affect the psychological system are also
seen to consequently affect the physiological systems, contributing to faster
recovery. This is further explained in the immune system section.
Privacy is also a main factor of the environment that people value most in
healthcare settings. This was further ascertained by a study that was
conducted on past patients in the Salford Royal Hospitals NHS Trust
(SRHT), Greater Manchester, UK (Douglas & Douglas, 2005). The study
consisted of distributing questionnaires to the previous patients in order to
understand their main concerns (whilst they were using the facility) and note
their suggestions for improvements. It was determined that the users’ main
concerns were limitation of private space around the bed area, indicating a
need for spaces to be supportive of privacy and dignity. They were of the
opinion that sustainable health-care environments should be considerate of
their health and recovery. According to the user, they visualised the
environments as having a home feel to it, being supportive of a normal
lifestyle and family functioning and being designed in such a way that they
would promote better user-friendliness and make transfers from one place to
the other easier (Douglas & Douglas, 2005).
85
4.6.3 BE Research: Environmental Health
The psychological dimension of the physical interior environment is a less
studied area in environmental health research. According to Frumkin
(2006), the physical, psychological, social, spiritual, and aesthetic outcomes
from the interactions with an environment can impact on health. He further
states that the perspectives of environmental health as understood today in
relation to mental wellbeing are:
• The environment contains several chemicals from which a ‘direct
toxic effect’ is experienced. They cause mild to harsh levels of
psychological and stressful impacts.
• People with ‘occupational or environmental illness issues’ are
experiencing stress, resulting in mental health conditions such as
depression.
• Many people show multiple symptoms from syndromes caused
by environmental exposures. These can be single or related.
• Nature is interlinked with our mental wellbeing by “contributing
to our spirituality and our sense of wholeness” (p.784).
He states that these perspectives have a multidisciplinary inquiry base which
would require interdisciplinary inquiry methods (Frumkin, 2006).
Mental well-being is influenced and affected by poor quality physical
environments, as indicated in a study on urban environments. The study
(Galea et al., 2005) found that people who inhabit places that are of
substandard quality are likely to be more depressed. The survey conducted
in New York is indicative of the properties of the BE in impacting mental
wellbeing (and even contributing to contracting mental illness) when people
are exposed to, and live in conditions that are below standard.
4.6.4 Health and Medical Research
The term ‘environment’ is understood by health professionals in terms of
the ‘social circle’ of the person; this includes their family, friends and

86
colleagues (Lundberg, 1998). Citing Chivian et al., Lundberg (1998) states
that “The physical environment, our habitat is the most important
determinant of human health” (p.6). The identified factors regarding
environment and health are ‘chemical pollution’, ‘ toxic exposures’,
‘climate change, heat, radiation’, ‘migration’, ‘stress’, ‘war’, ‘light’,
‘biological diversity’, ‘nature experience’, ‘sick building syndrome’, and
‘biophilia and biophobia’ (see Lundberg , 1998b). Studies on the physical
environment embrace the broader or the macro environment, and studies on
the micro environment are mainly restricted to the sick building syndrome
and their health related aspects, closely relating to the environmental
research domains. “Studies have mainly focused on pure physical/chemical
factors, while the mental/mind aspect of new age disorders has been
relegated to second place...there is ample opportunity to enhance our
understanding of environmental illness if we take a multidisciplinary
approach involving psychiatrists, psychologists, physicians, and industrial
hygienists” (Arnetz, 1998, p. 140).
Most of the literature in this category deals with the relationship between
physical setting and people with illnesses. With the exception of the benefits
of physical activities (such as walking, exercise), fewer studies involve
‘normal’ people.
For example, various studies have established the importance of the physical
environment in patients with mental illness. Many have supported the need
for a health favourable space to inhabit when sick as well as for overall
well-being (Williams, 1994). As described in the design and healthcare
section, researchers have identified the significance of informal
surroundings as opposed to institutional feel to positively support the mental
health of patients. Examples include the Planetree Model of health care and
the Pebble Project, Centre for Health Design.
The significance of the sensory organs interacting with the surroundings has
been found to be an important factor influencing health and wellbeing. For
example, sound has been recognised in health literature as being one of the
87
most stressful factors that is connected to the environment. Sound or noise
that originates from the external environment or within the interior
environment can be either stressful or beneficial. Even background hospital
noises were seen to affect the patients negatively (Ulrich & Zimring, 2005).
Music therapy used as part of the recovery process because of its properties
to calm and soothe people, has been found to be beneficial in alleviating
pain and stress in patients (Beck, 1999).
What a person does or thinks in a room depends on the moods and the
emotional state of the person. Mood and emotional feeling sometimes
impacts the decision a person makes about duration of stay in that place
(Rosenman, 1994). As within the other domains, research based on the
psychology of health has long recognised that we are exposed to many
elements that affect or arouse our senses on a day to day basis in a place.
Various studies have been conducted to determine the sensual feelings and
interaction of person within a place (Rosenman, 1994). Some of these have
found that emotions occur without the person being aware of them and
remain in our subconscious minds (Rosenman, 1994). Again we see links to
studies in environmental psychology; particularly those related to arousal,
occupational stress and the like.
Another fact is that the theories that emerge within the domain of
environmental psychology have originated from the theories that existed in
the medical area of psychology and, as EBR researchers consist of
psychologists and sociologists, many have similar theoretical
understandings and study designs. For example, the ‘environmental press’
theory identified in the environmental psychology section (Lawton, 1975) is
similar to the coping mechanisms that are identified in health and medical
literature (see Rice, 1987; Williams, 1994). Both identify similar
characteristics of the environment that produce stress in some people
depending on their personal traits.
Another aspect that has been recognised across discipline domains is
sensory response and PE interrelationship. For example, art and nature are

88
understood to contribute to the restorative capacity of place; odours trigger
memories of other places or experiences; smell is a proven therapeutic for
ailments as well as contributing to general wellbeing. Aroma therapists
claim that fragrances such as lemon, peppermint and basil lead to increased
alertness and energy, whereas lavender and cedar promote relaxation and
reduced tension after high-stress work periods (Iwasahi, 1992, as cited in
Pressly & Heesacker, 2001). Certain scents have been recognised to have
therapeutic benefits for a variety of physical conditions (Buckle, 1999).
4.6.5 Summary of results: Psychological dimensions of PE interrelationship to integrative systems approach
The above mentioned results indicate that research conducted in the
different domains has developed a sound theoretical and conceptual
understanding of the psychological effects of the physical environment.
When they are interrogated by the PNI concept of human mind-body
relationship and consider the person as whole an appreciation for the
integrated health system appears to be emerging. However, at present,
inquiry into person environment relationships and their influence upon
health and wellbeing remains limited.
As many studies conducted within the psychological dimension of PE
relationships indicate, the main approaches to the study of environmental
impact on human well-being focus on the objective characteristics of the
environment and the subjective response of the human being following PE
interaction and transaction. The impacts that stem from these influences are
explored on a singular or collective level and sometimes also on conditional
understandings that overlap (see Wong & Peacock, 1994; Bonnes &
Secchiaroli, 1995; Gifford, 1994; Stokols, 2006; Bell et al., 2002). Most
studies still only relate one dimension of P to the E and fail to explore the
additional impact on other dimensions or the ‘flow on’ effect to other
dimensions.

89
Singular
Collective
Interactional/ Transactional
R E L A T I O N S H I P
Objective
Subjective
P + E Overlap
Figure 11 Psychological dimension relevant to health and
well-being outcomes of analysis
Despite these studies, there seems to be a dearth of studies that specifically
look at the subsequent impact of place on the physiological system eliciting
or educing illnesses. This may be because there is no known framework that
integrates the human system in an integrative or holistic way. This thesis
argues that PNI is one such framework.

90
4.7 Physiological dimensions of the PE Relationship Person interacting/transacting with the environment: Relationship to the physiological system or the neuroendocrine and immune systems.
P&E
N&E
I&E
Integrated &E
PNI &E
BE Literature Environmental Psychology
Design
Architecture Design and healthcare
Environmental health
Health Literature
Healthcare Health Psychology
Medical
Table 1(b) Classification of data into domain N&E and I&E
As defined by World Health Organisation (WHO), health (physical well-
being) is “…a state of complete physical, mental and social wellbeing, not
merely the absence of diseases and infirmity” (WHO, 1984, p. 6).
Breslow (2000) states that health is prevention and curing of diseases, where
curing is done by doctors through treatment, and prevention is the
responsibility of the person, society or government (for individuals or the
population as a whole). Illnesses incorporate a variety of diseases such as
communicable diseases like tuberculosis, chicken pox, influenza,
pneumonia, as well as socially related problems such as malnutrition,
overwork, inadequate residential conditions, pollution of air and water and
so on. Chronic problems are mostly associated with the so called
‘improvements’ in society; for example, the luxuries that cause health
damage due to physical inactivity, excessive calorie consumption, smoking,
alcohol, drug abuse, to mention a few. The health damage caused includes
cardiovascular diseases, lung cancer, diabetes, and many other chronic

91
forms of diseases. Where treatment used to be the major specific approach,
now prevention is being given considerable importance (Breslow, 2000).
As described in Chapter Three dealing with PNI, the neuroendocrine and
immune systems are internally interrelated. Daruna (2004) states that
“…disease constitutes stress… psychosocial stress can increase the
probability of disease or exacerbate the manifestation of a disease
process…” (p. 134). For instance, WHO (2003) has identified cancer to be
one of the most life threatening diseases stating that the number of people
contracting the illness annually “is expected to rise from 10 million in 2000
to 15 million by 2020” (2003, n.d.). Indoor air pollution is one
environmental risk that concerns the interior environment that WHO (2006)
identifies as being a ‘lethal killer’ that plays a key role in developing lung
cancer, respiratory infections and chronic bronchitis and respiratory
diseases. Also recently identified as new hazards are “psychosocial
problems and sitting before the computer for long hours”. Additionally
“exposure to high levels of noise and dust, excess burdens of weight, and
toxic chemicals” are now recognized as serious workplace occupational
hazards to health (WHO, 2006, n.d.)). Cancer among others is one form of
illness that PNI acknowledges as sometimes emerging from psychosocial
stress issues (Daruna, 2004; Schedlowski & Tewes, 1999).
Figure 12 BE + Physiological systems interrelationship
Psych Physio
B E

92
This chapter is divided into specific sections which identify categories
related to human psychological and physiological responses to person
environment relationships as indicated in Figure 12 . Each section is further
divided according to categories which look at different domains of built
environment and health literature.
In research conducted on physical environment determinants, the sensory
organs and impacts on their function are of significance. This may be
because senses play an important role in a person’s psychological and
physiological systems. Without sensual ability, the acknowledgement of our
surroundings is impossible (Coon, 1991). Our sensory organs consist of the
sense of vision, hearing, smell, taste and touch which acts on the central
nervous system on different levels (Coon, 1991). There are some senses that
we cannot shut off even if we need to the sense of smell being one.
However, no two individuals respond to or detect stimuli in the same way
(Coon, 1991). Every individual creates an awareness of the surroundings
through their sensual capabilities. That people interact with a designed
setting according to five different dimensions namely visual, auditory,
tactile, olfactory and kinaesthetic is also recognised by Zeisel (1981).
‘Sensation’ is defined as the response caused by neurons (which process
sensory information) in the brain responding to a sensory organ, itself in
relationship with the environment (Coon, 1991). To better understand our
senses and surroundings, it is necessary to understand the acute sensory
dimension that exists between mind and physical system. Coon (1991) has
studied the minimum amount of physical energy necessary to produce a
sensation which is called the ‘absolute threshold’7through everyday
encounters involving the human senses. This is conveyed in Table 7.
7 This is studied in psychophysics which is “the study of the relationships between physical stimuli and the sensations they evoke in a human observer” and measures “the minimum amount of physical energy necessary to produce a sensation” called the “absolute threshold” (Coon, 1991, pp. 148- 150).

93
Sensory Modality Absolute Threshold
Vision Candle flame seen at 30 miles on a clear dark night .
Hearing Tick of a watch under quiet conditions at 20 feet.
Taste 1 teaspoon of sugar in 2 gallons of water.
Smell One drop perfume diffused into a three-room apartment.
Touch A bee’s wing falling on your cheek from 1 centimetre above.
Table 7 Sensory modality and the absolute threshold
(adapted from Coon, 1991. pp.148-150)
The senses are an important part of the physiological systems in enabling a
person to be aware of the surroundings and influenced by them. Following
is a brief overview of these senses.
• Sight is perhaps the most important sensory experience in the body.
While individual vision varies, it is generally sensitive enough to
detect even the smallest amount of light which the brain registers as
visual stimulations (Baron, 2001). The nature of light is central in
classification of colour.
• Sounds vary in frequencies from high to low and they can be
anywhere between desirable to undesirable (Bennet, 1977). Sounds
and noises are an integral and sometimes unavoidable part of our
life, thus being an important aspect of our everyday existence. These
sounds can be everyday sounds that we acknowledge and
background sounds that we do not acknowledge. The findings that
there is a trend towards premature hearing loss among young people,
supposedly caused by the every day facets of modern day living; for
instance, electronic gadgets which make life easier and enjoyable but
at the same time affect hearing through high degree sounds, causes
94
concern (ASHA Poll, 2006). These devices may enhance quality of
work and performance and everyday living, but prove to be
dangerous for our ears (Baron, 2001). Noise levels may differ from
individual to individual. For some, noise may provide respite from
boredom when doing routine tasks while, for others, it may interfere.
• Smell or the olfactory sense is referred to as the ‘chemical sense’ as
it is the response of the sense to some substance dissolved in air or
water (Coon, 1991). There are different receptors for specific odours
which identify pleasant smells as well as unpleasant odours (Coon,
1991). Certain smells and odours affect various psychological
functions, resulting in positive or negative reactions affecting mood,
cognition, perception, health, behaviour and physiological functions
(Martin, 1996).
• Taste is also said to be a chemical sense. Mostly, taste is associated
with smell as smells tend to facilitate taste (Baron, 2001). This is
why food loses its taste when one has a cold or similar infection.
Taste depends mainly on age, culture and the individual. However, it
could be agreed that taste provides one of the most common forms
of enjoyment. Though taste may not be directly relevant to this
study, it is still mentioned as being an important part of the
environment and psychosocial dimension of health.
• The tactile sense is influenced by warmth, cold, touch, pressure, pain
and so on sensed through the skin receptors (Coon, 1991; Baron,
2001). Research has shown the benefits of touch which can create a
positive effect on patients (Richards et al., 2000). It is significant in
physical environment studies as thermal quality, everyday furniture,
soft furnishing materials, floor coverings, walls and objects that a
person touches everyday, have an impact on tactile experiences, in
turn, influencing place experiences.

95
In addition to these five senses there are other essential sensory organs
related to the everyday experiences; for example, the somesthetic sense
which pertains to the sensations of the skin; kinaesthetic sense which is the
sense of the organs within the body (for example, the muscles, tendons, and
joints) and; the vestibular sense which relates to the sense of balance and
body position senses (Baron, 2001). These senses are responsible for what
the body feels, giving us the feeling of routiness in daily operations of the
body such as walking, sitting and so on. Another sense, the existential sense
is based on three levels of consciousness namely the conscious level,
preconscious level and the subconscious level. The subconscious mind is
aware of the conscious, whereas the conscious mind may not be aware of
the subconscious (Zimbardo & Gerrig, 2002; Proshansky and Fabian, 1986).
Each of our senses has its own capabilities which differ from those of other
living creatures. Each person senses in a unique way. It is our brains,
however, which seek, process, and make sense of information. The human
brain has the ability to select and organise this information into stable,
recognisable images of the surroundings which we interpret in terms of our
experiences and perceptions (Rosenzweig et al, 1999). Through these
perceptions and cognitive capabilities, we try to solve our initial natural
sensory experiences from a perspective of the circumstances, situation, and s
This following sections looks into research regarding PE relationships to the
neuroendocrine and immune systems pertaining to each domains. They are
described as separate sections under each domains.
4.7.1 BE Research: Environmental psychology
4.7.1.1 Environmental psychology and PE interrelationship to the neuroendocrine system
The review did not find many studies that relate specifically to the
neuroendocrine system and PE interrelationship. Zeisel’s (2006)
identification of the linkages between PE relationships and neuroscience in
design falls within the environmental behaviour but is further explored in

96
relation to design and architecture. Research indicates that the brain also
controls the behavioural aspects of people (Zeisel, 2006).
A study conducted by Spangenberg and colleagues (2005), suggested that
behavioural aspects of people are more positively affected in retail stores in
the presence of ambient scent and music together. These attributes
incorporated in the store, elicited a positive reaction of the senses and were
understood to encourage people to evaluate the store and its commodities in
a more positive way (Spangenberg et al, 2005). They identify that the
neurological response of the brain influences the sensual reactions as well.
4.7.1.2 Environmental psychology and PE interrelationship to the immune system
Psychophysiology attempts to understand human behaviour and recognises
the relationship between the psychological systems and their effect on the
physiological systems. Parsons and Tassinary (2002) look at the aspects of
the environment and state that “…environmental psychophysiology focuses
on organism-place transaction and physiological events” (p.173). They say
that physiological activities from psychological impacts of the environment
take place in different forms, one or many psychological impacts resulting
in one or two, or many physiological reactions (Parsons & Tassinary, 2002).
All psychological events have some physiological referent - there is
no entity called mind that is independent of the central nervous
system…Changes in psychological processes due to human-
environment transactions are presumed to be reflected in physiological
response systems (Parsons & Tassinary, 2002, p. 174 ).
Some theories in environmental psychology such as those concerning
environmental stressors, restorative environments, topographic cognition,
environmental aesthetics, isolated environments, restricted environmental
stimulation therapy, and so on have implied that psychological events have
some ‘physiological referent’ (Parsons & Tassinary, 2002). Parsons and
colleagues (1998) studied the relationships between place, emotional

97
changes and immune functions through an experiment conducted among
students on external environments requiring them to view nature videos
prior to being subjected to stress. The participants’ skin conductance,
electrodermal activity and heart rate were recorded concurrently when
exposed to environmental stress. The study revealed that the participants
showed greater immunity to subsequent stress after viewing nature scenes
(Parsons et al., 1998, p. 133)). This study had formerly established that the
physical environment plays a definite role in the impact of the physiological
system through the psychological system.
Anthony and Watkins (2002) point out from their review of clinical
literature that the physical environment is not often taken into consideration.
They state that the term ‘environment’ seemingly “denotes situational rather
than physical surroundings” (p.132). Their findings from the review indicate
that certain environmental stimulants elicit certain human systems disorders.
This aspect also was identified in workplace environment research
indicating that the social and organisational aspects of the work
environment consist of a variety of stressors that are associated with ill-
health, including “[M]ental and physical health symptoms ranging from
anxiety and depression to gastrointestinal and cardiovascular diseases”
(Jamison et al., 2004, p. 43). Findings from the analysis of literature
conducted in this study reinforce these findings.
Some of the elemental factors in the physical environment that are linked to
the physical health of a person are acoustics, ventilation, thermal quality,
lighting, air quality and so on. Many of these conditions are researched as
part of ‘sick building syndrome’ research which “…refers to the presence of
chronic symptoms associated with occupying a specific building. Such
symptoms often dissipate when the individual ceases occupancy for a period
of time” (Dorn, 1994, p.168). The symptoms typically relate to the physical
health of a person and the factors or elements in an environment that causes
them. The main factors identified in the physical environment affecting
health and wellbeing as part of the ‘sick building syndrome’ are, according
to Dorn (1994), “climatic affects (air quality), chemical pollutants (ozone

98
and formaldehyde), microbiological factors (bacteria and, mould), electrical
environment (electromagnetic fields caused by VDTs), psychological
factors (work relationships), organizational factors (job type), and
demographic factors (such as sex and age)” (p.169).
These elements then are present in a range of environments including work
environments. The chemical pollutants in the air can be an ever-present
threat to the human physical system. The “carbon dioxide” released by
occupants, “toxic substances” released from “smokers, water vapour,
microbial organisms, certain fabrics and furnishings release toxic substances
in the form of formaldehyde/organic and solvent vapours/dust and fibres”
are seen to affect the composition of air, possibly resulting in physical ill
health (Dorn, 1994, p. 170).
Microbiological factors are normally found in humidifiers and chillers or
duct works mainly because servicing and cleaning out of these systems is
usually not an easy process due to their inaccessibility. The bacteria and
viruses lead to a combined effect in harming the human physical systems
causing irritation to the respiratory system, affecting the eye causing
irritation and other allergic symptoms (Dorn, 1994). These elements, though
associated with the workplace environment can be attributed to other built
environments that we interact with every day such as our home, places we
relax in, shop in, and so on.
The elements referred to above can be considered as environmental
stressors. Several studies reveal that exposure to environmental stressors for
a period of time can lead to irregulations within the immune system causing
certain illnesses and diseases (Watkins & Fleshner, 1997; Schneiderman,
1982 as cited in Bell, et al, 2001). In other words, while exposure to some of
these stressors directly impacts on health, exposure to others can have
negative impacts on the physical well-being over an ensuing period of time.
‘Environmental Psychology 5th Ed.’ by Bell et al. (2001) is an excellent
source of information on research involving the physical environment and

99
human behaviour, incorporating the psychological as well as the
physiological aspects of a human being. Bell et al. (2001) indicate that one
of the influences affecting a person physiologically is ‘arousal’ as an
outcome of certain environmental stimuli. Physiologically, it is the result of
“heightening of brain activity which creates differences in the heart rate,
blood pressure, respiration rate, adrenalin secretion, and so on” (Bell et al.,
2001. p.103). Bell et al. (2001) cite various studies regarding environmental
arousal and behaviour. They use noise as an example of a phenomenon
which can create arousal and because of its effect on the brain can cause
behavioural change, including aggression. This, in turn, can affect other
systems in the body.
The five senses of the human body play a central role regarding the physical
environment’s impact on the physiological system. For example, when
exposed to certain colours, researchers have observed changes in blood
pressure, pulse rates, respiratory function, arousal levels, fatigue, and
depression (Ward, 1995). Another experiment involving workers and the
effect of smell is cited by Russel and Snodgrass (1987). The experiment
deals with the effect of the environment on the unconscious mind. They
explain how, in 1936, Winslow and Herrington exposed workers to the
odour of burnt dust. While not detectable by the workers the odour resulted
in the decline of appetite among the workers. This incidence is noteworthy
because the psychological change that occurs indicates that exposure to
some chemicals, even if not detected consciously, may change one’s mood
and can be the cause of certain physical conditions.
Correspondingly, there are other elements that are present in the air and
atmosphere that cannot be detected but that produce various physiological
and psychological conditions influencing a person’s mood. One such
element is temperature which has been shown to influence the mind, mood
and behaviour. Levels of heat sometimes provoke aggression or inhibit it if
the heat is high (Russel & Snodgrass, 1987). Noise, another potential health
hazard, can not only impair hearing but also sometimes affects people so
much that they become angry and aggressive (Bronzaft et al., 2000 as cited

100
in Bronzaft, 2002). Bronzaft (2002) further found that when exposed to
noise over a long period, people become depressed and acquire a helpless
feeling that they have no control over, and spend a lot of time either trying
to tolerate it or trying to avoid it. He further reports on a review (Evans &
Lepore, 1993, as cited in Bronzaft, 2002) of noise effects on children where
it was found “that residential noise delays early cognitive development and
that chronic noise exposure in classroom settings has been associated with
poorer reading” (p. 505).
Pennebaker and Brittingham (1982) recognise that certain environmental
stimuli can elicit physiological responses influenced by psychological
responses. They state that, when there is ‘external information’ (stimuli
outside the human body), the ‘internal sensation’ creates an awareness of it
which is “directly related to physiological change” (p.119); these
perceptions evolve consciously or without deliberation. People may not be
aware of the internal physiological sensations unless it is something
contradictory to everyday encounters.
4.7.2 BE Research: Design & architecture
4.7.2.1 Design & architecture and PE interrelationship to the neuroendocrine system
The neuroendocrine linkage of the PE relationship aspect is less researched
in this area although it is increasing acknowledgement now. Inquiries into
the relationships between neuroscience and architecture explore the
possibilities of linking architecture and neurology to develop a better
understanding of the human brain, mind and consequences. Neuroscience is
the study of mind and brain and how the brain processes what the mind does
or thinks (Eberhard, 2004). The brain processes emotional experience and
recalls it every time we enter the same setting. The Academy of
Neuroscience and Architecture is one such place where research is
conducted on brain and spatial issues. The academy hopes to find out the
actual workings of brain when a person enters a setting and how this activity
in the brain ‘changes people’s frame of mind’ (Eberhard, 2004). Research in
101
this area is indicative of the linkages between the workings of the brain and
the physical space/place. Place or space becomes significant to a person
only when s/he comes in contact with them. These contacts, big or small,
become the basis of experience of the physical environment. The
experiences subsequently contribute to several reactions within the human
mind and body. Eberhard (2003) refers to Damasio, stating that
“Place/space experience is recorded … [as] “dispositions” [which] record in
our brain a combination of sensory inputs, memories, emotions and any
related muscle memories. Just below the surface of consciousness, these
dispositions wait for the next experience with which they can be paired …
each time we enter the office in which we work, we are recalling a
dispositional record of our last visit - including any emotional experiences
we may have had. When we leave our office at the end of the day, our brain
creates a new dispositional record that updates the one we came with that
morning. The same happens when we drive or travel and when we enter the
places we live which we call our home” (Eberhard, 2003, n.d.).
Zeisel (2006) states that many ‘environment- related activities’ are related to
the workings of the brain; and to how we react to the surroundings and how
the mind and brain process information to do with the surroundings. He says
that while there is little known about the linkages between neurological
activities and environmental impact, researchers should “embrace
neuroscience tools as additions to our methodogical arsenal...if you
understand how people’s brains and minds develop and function in different
situations, and how they have evolved over time to respond to physical
environments, then environments designed to support these capabilities as
well as tasks, activities and user needs, will contribute to people’s quality of
life, creativity, and survival” (pp. 142-143). Zeisel identifies several ways in
which neuroscience can better inform design, including:
• explaining users’ needs, behaviour, attitude, and opinion
• informing psychological, sociological and anthropological
environment-behaviour knowledge research
• contributing to the development of user-need paradigms (p.143)

102
4.7.2.2 Design & architecture and PE interrelationship to the immune system
The studies that were conducted with regards to health and well-being and
the physical environment in the design and architecture area are generally
confined to the healthcare research settings. As a result, they are mainly
referred to in the relevant section in the thesis as well as in the
environmental psychology section.
An evaluation by researchers (Balanli et al., 2005) of the health
characteristics of a library building revealed some physical and social
determinants to health. They found that the physical properties such as
visual elements, acoustic levels, the level of cleanliness; spatial features;
thermal qualities; and social characteristics such as the spatial characteristics
of the interaction among users and lack of space for activities were
complicit in increasing stress levels. These, in turn, contribute to several
physiological complaints such as allergy, unhappiness, lethargy, general
discomfort, headaches, psychosomatic symptoms, fatigue and eye problems.
These problems were instrumental in fewer people using the library
precincts (Balanli et al., 2005).
A study conducted by Smith and Adkins (2005) to understand the shopping
experiences of people with impaired cognition capabilities indicates that
environmental cognition plays a significant role in people being able to
adapt within their surroundings. They identified appropriate signage and
layout as being important for place and product identification. It was found
that people with cognitive impairments often found the large spaces to be a
cause for complications, whereas smaller places helped them achieve their
goals. Smith and Adkins (2005) further state that creators of the physical
environment should take into consideration “…how environments are linked
to a person’s ability to understand and negotiate one’s surroundings, to
obtain one’s goals, to express one’s self as desired, and to maintain one’s
identity to a self established level at any time” (p. 16). Another study
revealed that certain environmental stimulants elicit several physiological

103
problems in cognitively impaired people including “dizziness, faintness and
disorientation”, making it difficult to perform simple daily activities
(Adkins et al., 2005, p. 11).
Another study conducted in a dental clinic showed that visual stimuli in the
spatial surroundings influence physiological functions in the visiting
patients (Heerwagen, 1990, as cited in Frumkin, 2006b). The researchers
placed a mural (depicting natural scenery) in the clinic on some days and
took it out on others. Patients visiting the clinic when the mural was there
were seen to have lower blood pressure levels and anxiety than the patients
visiting on the days the mural was not there.
4.7.3 BE Research: Design and healthcare
4.7.3.1 Design and healthcare and PE interrelationship to the neuroendocrine system
The review did not yield many studies that specifically looked at the
neuroendocrine systems, apart from a few studies that relate to the immune
system and which are described in the next section. There are studies that
look at the mental health area and its interrelationship with the environment.
These studies mainly relate to mental health facilities or studies regarding
people with mental health problems such as schizophrenia, dementia or
other neurological disorder. These studies were not explored and were
omitted from this review as they did not meet the criteria and guidelines of
the study. Studies that explore the cortisol levels and adrenaline levels are
included in the next section as they relate to the overall physiological
system in general.
4.7.3.2 Design and healthcare and PE interrelationship to the immune system
Many studies conducted in the healthcare settings area have indicated that
the immune system of the human being is affected by a variety of factors in
the physical environment. Inquiries into the specific areas of the human
physiological systems have mainly been carried out in studies based on

104
healthcare environment settings. For example, Ulrich’s (1984) study of the
benefits of views influencing the physical health aspect of individuals,
discovered that images that are visually pleasing benefit patients in
hospitals. Ulrich (1984) undertook a longitudinal study involving patients
recovering from surgery to understand the restorative capacities of hospital
environments and conducted a study within a 200 bed hospital. The existing
facility consisted of rooms where some patients faced a window with a
natural view of trees, while others faced a brick wall. For the study,
postoperative patients were assigned on a random basis one of the rooms.
The records of patients occupying each room were reviewed over a 10-year
period and it was found that patients with tree views had statistically
significantly shorter hospitalisations, less need for pain medications, and
fewer negative nurses' notes than patients with wall views. These results
suggest that views of trees have a beneficial effect and, together with other
evidence, support the notion that nature plays a considerable part in
restorative properties (Ulrich, 1984). As mentioned before, the role of nature
in restorative environments has been studied extensively and found to
positively impact on the mind in various studies conducted in environmental
behaviour research areas (see Betchel & Korpela, 1995; Kaplan, 1995).
Ulrich (1991, 1992) also suggests that control and privacy in the
environment is invaluable to speedy recovery possibilities in patients as well
as to the well-being of visitors and staff. He states that visible design
features and elements that the users could choose themselves are key aspects
in promoting wellness (Ulrich, 1991, 1992). He identified various elements
as contributing to faster recovery and well-being, stating that “poor design
[is linked] to anxiety, delirium, elevated blood pressure, increased need for
pain medication and longer hospital stays…[and] good design can reduce
stress and anxiety, lower blood pressure, improve postoperative courses,
reduce the need for pain medication, and shorten hospital stays” (Ulrich,
1992, p. 20).
Many hospitals today are implementing design principles that contribute to
the users’ wellbeing. There is extensive research undertaken in this area

105
with a high level of possibilities for application. The Planetree model of
healthcare is one such set of principles which takes a holistic view of the
patient’s mental, emotional, spiritual, social and physical needs, recognising
the importance of architecture and design as being an integral part of the
healing process of patients. It originated in San-Francisco in 1978 and has
since been adopted by many hospitals (Geoff, 1995).
The Planetree model acknowledges healthcare environments and settings
should be designed following principles that nurture both the body and the
spirit. They adopt the view that the senses of a human being should be given
utmost importance and reinforce the importance of surroundings in being
beneficial for the users (see Arneill & Beaulieu, 2003).
Unreceptive environments may be a cause of depleting energies thus
creating problems in the healing process (Geoff, 1995). The lack of privacy,
noise and staff disturbance worsens this situation (McCarthy, 2004).
Furthermore, a review of the literature conducted by Ulrich and Zimring
(2004) indicates that many studies have shown elements in the environment
as being connected to increasing hospital stays and longer recovery times.
For example, they state that the noise levels in most hospitals are too high
for two general reasons. Firstly, there are various pieces of hospital
equipment and fellow room-mates constantly producing noise. Secondly,
architectural and place dimensions such as the floors, walls, and ceilings
(which are usually hard) reflect sound rather than absorb it, causing the
sound to echo, overlap, and linger. Also, it is suggested that design features
that include private rooms with rooming-in accommodations for all patients;
creative use of artwork, music, light, and nature to create a more pleasant
and less stressful environment; shorter walking distances for patients and
families with seating along the way; and touch-screen information kiosks at
every main entrance, would help increase well-being for the users (Ulrich &
Zimring, 2004). All these factors point to health benefits for the person
using the surroundings.

106
4.7.4 BE Research: Environmental Health
4.7.4.1 Environmental Health and PE interrelationship to the neuroendocrine system
Studies concerned with the neuroendocrine systems are mainly concerned
with the external environments such as pollution, global warming and so on.
Therefore these were not included in the study set. However, some studies
that relate to the physiological system also regard the neuroendocrine
systems as being relevant. These studies are mentioned in the next section.
4.7.4.2 Environmental Health and PE interrelationship to the immune system
The causes of environmental health problems are no longer confined to any
singular aspect of the environment. Instead, there is increasing support for
the view that they result from the combined interactions of the social,
economic, and physical environment (McMichael, 2001).
Indoor air qualities, electrical factors, chemical exposures and so on, are
some of the factors identified by environmental health research that
adversely affect the health and physical systems (see Frumkin, 2006, for a
detailed report on the identified elements). For example, electric appliances
like the photocopier releases ozone if placed in a poorly ventilated place and
static electricity is also an element in affecting the physical system; it may
cause a syndrome called ‘electrical sensitivity’ which includes symptoms
like “headache, depression, muscular weakness, in-coordination, and even
blackouts” (Monro, 2000,n.d.). Some of the illnesses that result from such
exposures can take 3-10 years to be identified (Monro, 2000). Likewise, as
mentioned earlier, research on the effect of sound on psychological as well
as physiological systems reveals that sound influences anxiety, stress,
behaviour, pain, muscle tone, blood pressure, and heart rate (Standley, 1986;
Venolia, 1988; Wigram, 1995).
Inadequate housing has been seen to lead to various psychological
conditions as well as physiological conditions such as “depression, attention

107
deficit disorder, substance abuse, aggressive behaviour, asthma, heart
disease, and obesity” (Srnivasan, 2003, p.1448) and related complications.
4.7.5 Health and medical research: PE interrelationships to the neuroendocrine and immune systems
The majority of studies in this domain are conducted on physical activity
related to the physical environments and stress factors that emerge from
psychosocial issues within the settings. These are described in the healthcare
environmental setting section. The effect of the environmental elements on
the sensory system affecting certain physiological conditions is something
that has been widely acknowledged in all the domains analysed. Likewise
the domain of health psychology also recognises the effects of sound on the
psychological as well as physiological conditions (Standley, 1986; Venolia,
1988; Wigram, 1995).
Not only toxic materials but also environmental stressors can influence
emotions which, in turn, affect human health. The way one responds to
‘environmental stressors’ depends on the control one has on the
environment. Studies of animals have revealed that when they are in control
of the environment, they respond with aggressive activity, and when they
are in an uncontrollable situation they become defeated and withdrawn,
releasing cortisol (Henry & Grim, 1990, pp. 783-793). This applies to
human beings as well. It is also dependent on different types of personality.
Some people find it easy to cope with stressful conditions, while some do
not. Normally, however, a person’s interaction with their environment
depends on their experience of it, which, in turn, is dependent on their
perception and cognition of that environment.
Environmental stress has a direct influence on the physiological systems as
well. Stress is perceived by people in different ways. Rosenman cites
Seyle’s (Seyle, 1936) findings of the importance of cortisol and the fact that
humans respond differently depending on age, sex, genetics and various
other environmental factors. TABP (Type A Behaviour Pattern) is the
behaviour pattern of aggressive, hard driving and ambitious people who are

108
constantly compulsively striving to achieve goals incorporating power and
prestige. Studies show that people with TABP have a higher incidence of
cardiac dysfunction. Emotions like anger and anxiety can also cause
cardiovascular diseases as a result of affecting the cardiovascular function
(Rosenman, 1994). The environment, when not conducive to the person,
produces an excess level of cortisol in the human body, paving the way for
various physical ailments (Riley et al., 1981).
4.8 The physical environment and integrated health & well-being
P&E
N&E
I&E
Integrated &E
PNI &E
BE Literature Environmental Psychology
Design
Architecture Design and healthcare
Environmental health
Health Literature
Healthcare Health Psychology
Medical
Table 1(c) Classification of data into domain Integrated & E
As mentioned previously, a broader perspective of looking at health and
wellbeing outcomes from the interrelationships with the environment is
provided by the integrative systems model conceptualised in this study.
While the more conventional approaches to person-environment interaction
and its health hazards described earlier in this chapter, (for instance, sick
building syndrome) have been noted, psychosocial and cognitive
interactions may also be a direct result of broader dimensions. It is this
broader perspective – a perspective which explicitly acknowledges the
psychological, social and physical determinants of human health and the
state of the environment – and offers a much broader, environmental
interrelationship with health. In recognition of the key significance of this to

109
the future of BE health and its corresponding status as one of the guiding
principles of health and well-being of person, discussion of the concepts of
PE interrelationship to health and well-being outcomes (related to
psychological and physiological systems) is presented in the following
section.
Today, environmental health is being challenged to seek solutions to a range
of increasingly broad concerns. These include social, physical, cultural
dimensions of the environment (Frumkin, 2006). The psychological and
physical aspects of the environment mentioned in the previous sections are
interrelated and have a significant impact on human health and well-being.
Figure 13
BE + Integrated systems interrelationship
This section identifies components that are mainly identified in the research
domains that are directly concerned with the overall health and well-being
of a person, as opposed to the singular and overlapping aspects previously
identified. The health model is not discussed here as it is described in
Chapter Two. This section, therefore, looks at the influence of the physical
environment on the overall health system and identifies certain key aspects
that may be related to the environment in an integrative way. This is
illustrated in Figure 13.
Psycho Physio
BE
110
4.8.1 Environmental psychology: PE interrelationships to integrated health & well-being
Stokols (2000) states that, in understanding and creating health–promotive
environments, it is necessary to look at the “sociocultural and physical-
environment qualities of organisations, institutions, and community settings
that are especially health promotive” (p.135). This proposed unit of analysis
is called the ‘Wellness-promotive’ or the ‘Health-promotive environment’
and aims to look at the various “interdependencies that exist among
sociocultural, political, economic, spatial and technological features of
environmental settings, ranging from homes, neighbourhoods, workplaces,
and schools to regional and global environments that influence personal and
collective well-being” (p.135). Some features of the environment that
promote personal and collective well-being, which could form the requisites
of a health-promotive environment, are suggested, emphasising that to
understand environmental behavioural factors, it is important to first
understand the ‘key environmental resources or constraints’ (p.136) that
would be responsible for impacting on the users (Stokols, 2000).
Key issues of the physical and social factors that promote health and well-
being are identified by Stokols (2000). These include: installing physical
fitness facilities to encourage exercise regimens among the users of the area,
promoting injury resistant materials during construction; and avoiding using
toxic materials and sources of psychosocial stress like poor lighting and air
conditioning so as to reduce environmentally induced illness. As social and
physical settings are interrelated, the wellness gained through both are also
interrelated; for example, even if the physical settings are health promotive,
if the social atmosphere is not as good, the physical environment loses its
value and vice-versa. This suggests the necessity of understanding physical
place in terms of the value of the ‘physical’ as well as the ‘social’
interrelationship to understand the capacity of the environment to be a
catalyst for positive and negative impacts on health and well-being (Stokols,
2000).

111
Stokols (1992) has argued before that for environments to be ‘health-
promotive’, they should be sensitive to “physical health, mental and
emotional wellbeing, and social cohesion at organizational and community
levels” (p. 9). He further states that physical health should include design
that is ergonomically conscious, supportive of comfort levels, ‘injury
resistant’ and thus conducive to physiological health. Emotionally
supportive places should provide ‘controllability and predictability’
including aesthetic qualities and afford a ‘sense of personal competence’
with growth of creativity. The place should provide a system for social
support maintaining ‘high levels of social contacts’ and quality of life (pp.
7-10). He lists a variety of personal and environmental factors that relate to
health and illness (Table 8).

112
Table 8
Personal and environmental factors in health and illness
(Source: Stokols, 1992, p.13)
Psychosocial factors have been identified as connected to health and
wellbeing. Social dimensions of the physical environment have been
identified as having a broad range of purposes and contexts. Primarily, it is
useful to understand it as fostering and facilitating communication and
interaction with fellow human beings. Proshansky and colleagues (1983)
state that “Individual’s experience with particular places constitutes an

113
important part of their self-identity...Spatial proximity fosters social contacts
and friendship formation” (p. 62). They cite Festinger in relation to social
and environmental factors stating that “Involuntary relocation from a
familiar neighbourhood often provokes emotional distress and illness
symptoms among the dislocated individuals” (Festinger et al., 1950, as cited
in Proshansky et al., 1983, pp. 57-83).
Along with the psychological and physical elements of the social dimension,
the sociocultural aspects of an environment are also key factors in the
emotional and physical well-being of the people using these setting
(Stokols, 2000). The cultural factors depend on the personality and their
exposure to places and also on personal preferences. For example many
studies indicate that when the environment can be controlled it produces
beneficial results; the environment that is too predictive can be seen as
boring (Lawton, 1989). People are seen to prefer environments that allow
for growth and creativity (see Lawton, 1989; Gifford, 1997; Stokols, 2000).
Stokols (2000) further proposes that ‘controllability and predictability’ and
durability can be associated with contradictory health effects, (depending on
the magnitude of ‘moderate vs. excess levels of predictability’ and duration
which depends on the short-term or chronic exposure). Therefore, to gauge
the capacity of an environment to support health and wellness it is necessary
to specify relevant environmental dimensions and health outcomes and
differentiate between health outcomes in terms of their severity and
duration, and overall importance to members of the setting (Stokols, 2000).
Stokols and colleagues (2001), in their study of workplace health, state that
“Workplace health promotion combines behavioural and lifestyle change
strategies with those focusing on environmental restructuring and
enhancements...[which] include interventions aimed at improving the
ergonomic features and social climate of work settings and reducing levels
of noise, air pollution , and hazardous substances in those environments”
(p. 496). This type of environment consists of a variety of features that
affect the mental and physical condition of users which can be customised
by architectural and interior design intervention (Stokols, 1998). Stokols

114
(1998) looks at ‘workplace design and occupational health’ through a
review of research on workplace health and environmental design to show
the role of the environment on occupants’ well-being. He lists the following
potential determinants of health:
1. Physical enclosure of the work area positively relates to the
“employee satisfaction with the work environment and this to the
overall job satisfaction”.
2. Open plan offices are related to headaches among employees using
them, depending on their type of work and satisfactory experiences.
3. Presence of windows that ‘afford natural views’ provide satisfaction.
4. The ability to ‘personalize’ aesthetic situation, (for example, adding
pictures) improved satisfaction in employees or people using the
space.
5. Furniture and ergonomically fit surroundings also contribute to this
feeling of well-being including “reduced rates of eye strain and of
repetitive motion injuries and lower back pain”.
6. The ability to control the thermal power and acoustics and lighting
levels are also seen to provide better mental well-being and ‘lower
levels of stress’.
7. “Ambient environmental qualities such as levels of noise, speech,
privacy, social density, illumination and air quality” have been
“documents” to influence adverse effects on “stress levels and job
satisfaction”.
8. “Indirect lighting” has been seen to cause “less eyestrain” than the
“traditional down lighting”.
9. “Workers exposed to chilled air ventilation systems show higher
rates of upper respiratory problems and physical symptoms of ‘sick
building syndrome’ (Stokols, 1998m, pp. 19-22).
To have a better understanding of these phenomena, Stokols (1998) states
that future research on health and environmental design should include
consistent, multi-method strategies and include the recording of

115
environmental conditions, medical examinations, and physiological
measures.
4.8.2 Design and architecture: PE interrelationships to integrated health & well-being
Most research looks at overall human health and wellbeing and is conducted
in hospital settings. “Architecture is often recognized as an important tool in
attracting and retaining the best doctors and nurses, the most successful
HMOs and insurance plans, and the most patients. Consumer decisions are
based on cost, accessibility, quality of service, and quality of medical care.
An aesthetically pleasing facility is a key aspect of the perceived quality of
care” (Carr, 2003, n.d.).
Zeisel (2003) and colleagues looked at the relation between the
environmental design of a nursing home and psychological problems among
people living in the special care units of a nursing home. They studied the
incidence of aggression, agitation, social withdrawal, depression and
psychotic problems in regard to physical surroundings, medicines and care,
and found that certain physical environmental features were the key in
influencing behavioural conditions of the people in the study. It was found
that enhanced features improve the quality of life in people with
Alzheimer’s disease by improving behaviour and, subsequently, health
(Zeisel et al., 2003).
Though elemental features play an important role in changing behaviours
and altering health conditions positively or negatively, Aspinwall and
Staudinger (2003) identified certain environmental factors that impact on
human well-being as a result of the person’s ability to ‘fit’ into the
surroundings. They concluded that the positive and negative factors of an
environment that affect wellbeing can be measured through the
‘environmental fit’ between a person’s goals, activities, and surroundings.
However, this is dependent on the duration and exposure to positive and
negative environmental conditions. According to them, the environmental
conditions that could enhance or impact negatively on wellbeing include

116
several factors such as aesthetic quality, interior features, restorative
environments, social settings, high levels of noise, levels of privacy,
vehicular traffic, and natural and technological disasters. Some of the design
factors they mention are depicted in Table 9.
They state that ‘future theory development’ would benefit from looking at
concepts more related to the psychological and physiological understanding
of wellness on a more ‘subjective’ level (Aspinwall & Staudinger, 2003).
Table 9 Design factors that affect health and well-being
(Aspinwall & Staudinger, 2003)
The sensory influences (of which visual stimulations play an important role)
are an unavoidable element of the physical environment. Studies have
recorded the fact that not only our moods and emotional stability but also
117
certain physiological factors can be influenced by the different hues and
tones of colour. Colour can affect “appetite, hormones, muscle strength,
adrenaline production and blood pressure, [also] altering our perceptions of
space, weight, time, temperature and other aspects of the physical world”
(Recio, 2002, p.33). For example, white, when combined with a high level
of lighting can produce eyestrain causing ‘muscular imbalance and
nearsightedness’ (Recio, 2002, p. 33).
A review of research conducted on ‘counselling-relevant articles of the
surrounding environment’ (Pressly & Heesacker, 2001) found that certain
elements in the counselling environment affect the process of therapy. These
include sensory stimulants (such as colour, lighting, sound), objective
elements (such as artworks, plants), functional elements (such as furniture
and design elements) and thermal conditions. According to their findings,
the outcomes from these influences may be psychological (such as mental
stimulation, soothing qualities) or physiological (change in blood pressure,
pulse rate).
Evans and McCoy (1998) identify five dimensions of the physical
environment that may affect health and well-being. They state “building
design has the potential to cause stress and eventually affect human health”
(p. 92). They identify environmental stimulation, coherence, affordances,
control, and restorativeness as being conducive to avoiding stress.
The identified aspects of healthcare including hospital sections are discussed
in the following section.
4.8.3 Design and healthcare: PE interrelationships to integrated health & well-being
Environmental design factors have the potential to enhance the
physiological and psychological health of occupants in health care settings
and it is discerned that some of them are associated with decreases in
negative behaviour, increases in positive behaviour and change of attitude in

118
the staff and patients, depending on the type of environment inhabited and
the person using it (Gross et al., 1998).
Studies involving healthcare environments mostly concentrate on healing
process where the quality of the environments is seen to be relevant. Canter
and Canter’s (see 1979) early review of research on the subject ‘Designing
for therapeutic environments’ focused on diverse settings used for different
therapeutic purposes and explored how the physical environment can
influence the healing process. They identify sociocultural as well as spatial
elemental factors as being important when designing for the healing process.
Discussed below are a few empirical studies conducted to look at the
influence of the physical surroundings on occupants. They indicate that
many factors of the environment are singularly or collectively responsible
for the well-being of the inhabitants.
The study carried out on ‘multisensual’ environments illustrated that
environments designed for the senses have a positive effect on its occupants.
Though this involved people with dementia, it may be applicable to any
environment. The patients were studied in three different environments, the
“snoezelen room”8; a landscaped environment; and the usual living room. It
was found that patients using the living room and the garden became calm
and showed pleasure and their sense of wellbeing stayed with them after
leaving the room also. The ‘snoezelen room’ was seen to have ‘a power for
stress reduction’ in all users alike (such as the patients, caregivers, visitors)
producing a calm and comforting quality. On the other hand, the garden was
seen to provide a more active environment proving to be very therapeutic.
Though the study did not find evidence for either the garden or the
‘snozelen room’ being more beneficial than the living room, it was observed
that the ‘snoezelen room’ and the garden did give occupants more pleasure
than the common living room. However, the fact remains that, even if the
8 The ‘snozelen room’ which was particularly designed for the senses basically meant ‘multisensory environment’. The concept of the ‘snoezelen room’ has its beginning in the Haarendael Institute in Holland which “aims for pleasurable sensory experiences arranged to stimulate the primary senses in an atmosphere of trust and relaxation, without the need for intellectual activity” (p. 38).

119
place does not have any negative effects, the potential for it to have positive
effects should be explored (Cox et al., 2004, pp. 37-45).
Another study done on the facilities of the new and old units of the Barbara
Ann Karmanos Cancer Institute revealed that better surroundings influenced
the well-being of the patients using the new facilities. This was understood
by studying the use of pain medication by the patients, finding that there
was a decrease in the usage of pain medication which is self administered by
the patients using new facilities. Though they were the same patients who
used more medication in the old facilities, they felt a decreased need for
pain medication in the more pleasant surroundings of the new unit (Bilchik,
2002).
Other studies that may be relevant to the overall health and well-being of a
person are discussed in the neuroendocrine and immune section.
4.8.4 Environmental Health: PE interrelationships to integrated health & well-being
As mentioned earlier, the main identified interior environment properties
that influence health and well-being are indoor air quality and chemical
contaminants, these being the most studied area in environmental health that
concern the interior physical space. Indoor air quality, as identified by other
domains, is understood to affect psychological as well as physiological
systems (Frumkin, 2006). Research conducted on several factors of the air
quality (see Frumkin, 2006; Wargocki et al., 2002; IAP, 1994; Bearg, 1993)
indicates that poor air quality triggers certain allergic reactions, making
people lethargic and irritable. Air conditioners and air humidifiers are seen
to elicit “dry eyes and throat, congested or runny nose, itchy and watery
eyes, lethargy, headaches, respiratory complaints, chest tightness”
(Hodgson, 2006, p.627-632) and so on. Lack of ventilation has generated a
number of findings linking ventilation to ill-health. The influence of
naturally ventilated systems or mechanically ventilated systems in causing
health problems is still under speculation. Nevertheless, there is general
agreement that choosing building materials, furnishings, and cleaning agents

120
that minimize indoor emissions; designing and operating effective
ventilation systems; and maintaining air circulation and humidity at optimal
levels are all part of important design strategies to protect health and
wellbeing in occupants (Frumkin, 2006; Wargocki et al., 2002; IAP, 1994;
Bearg, 1993).
Workplace settings are also well-studied in this domain, concluding that the
quality of the workplace is important psychosocially as well as
physiologically. A comparative study conducted revealed that the effects of
a new building on employees when they were moved from the old facility
were related mainly to sensual perception. Many of the responses recorded
were on the social level. However, lack of control of the temperature of the
space occupied was seen to be a cause of stress for some (Neuner & Seidel,
2006).
Frumkin (2006) identifies four perspectives of environmental health as
understood today in relation to health and wellbeing. He states that:
• There are ‘direct toxic effects’ from some chemicals. They cause
mild to harsh levels of psychological and stressful impacts;
• People with ‘occupational or environmental illness’ issues are
susceptible to contracting stress, resulting in mental health
conditions such as depression and further complications;
• Many people show multiple symptoms from overlapping syndromes
caused by environmental exposure;
• Nature is linked with wellbeing as it contributes to our sense of
‘wholeness and spirituality’ (p. 782).
These perspectives as outlined, according to Frumkin (2006) constitute a
multidisciplinary enquiry base which demand interdisciplinary enquiry
methods.
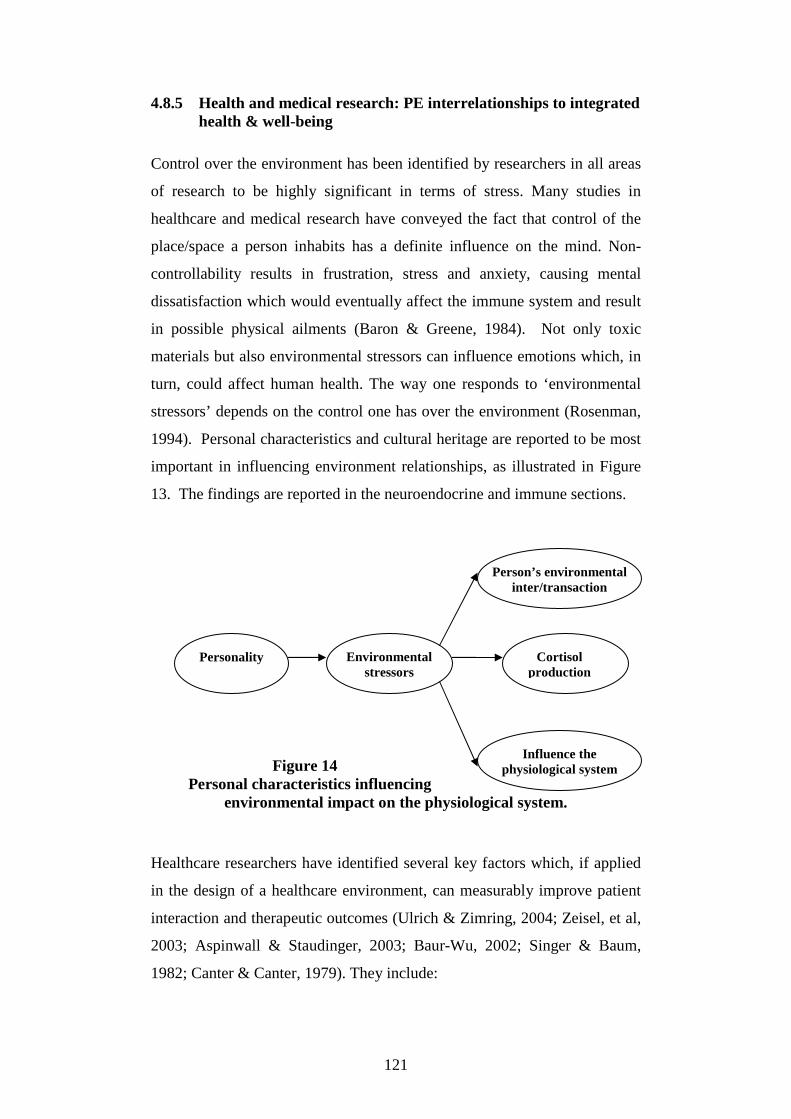
121
Personality Environmental stressors
Person’s environmental inter/transaction
Cortisol production
Influence the physiological system
4.8.5 Health and medical research: PE interrelationships to integrated health & well-being
Control over the environment has been identified by researchers in all areas
of research to be highly significant in terms of stress. Many studies in
healthcare and medical research have conveyed the fact that control of the
place/space a person inhabits has a definite influence on the mind. Non-
controllability results in frustration, stress and anxiety, causing mental
dissatisfaction which would eventually affect the immune system and result
in possible physical ailments (Baron & Greene, 1984). Not only toxic
materials but also environmental stressors can influence emotions which, in
turn, could affect human health. The way one responds to ‘environmental
stressors’ depends on the control one has over the environment (Rosenman,
1994). Personal characteristics and cultural heritage are reported to be most
important in influencing environment relationships, as illustrated in Figure
13. The findings are reported in the neuroendocrine and immune sections.
Figure 14 Personal characteristics influencing
environmental impact on the physiological system.
Healthcare researchers have identified several key factors which, if applied
in the design of a healthcare environment, can measurably improve patient
interaction and therapeutic outcomes (Ulrich & Zimring, 2004; Zeisel, et al,
2003; Aspinwall & Staudinger, 2003; Baur-Wu, 2002; Singer & Baum,
1982; Canter & Canter, 1979). They include:
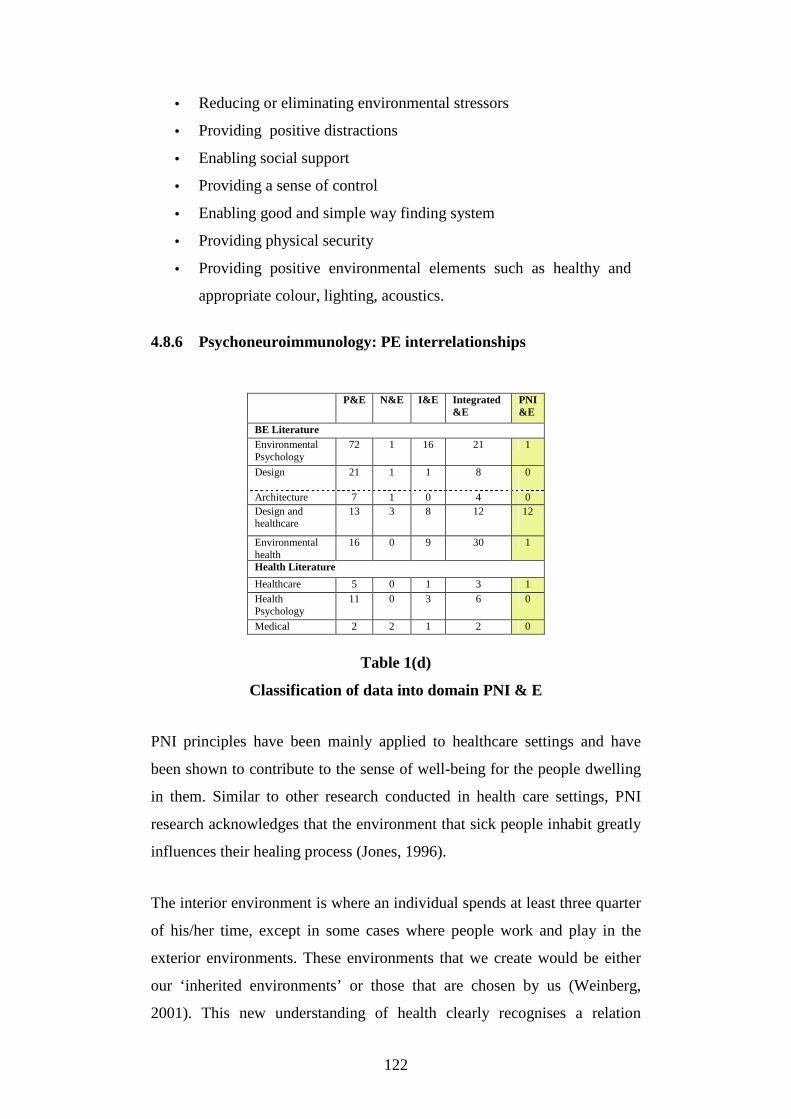
122
• Reducing or eliminating environmental stressors
• Providing positive distractions
• Enabling social support
• Providing a sense of control
• Enabling good and simple way finding system
• Providing physical security
• Providing positive environmental elements such as healthy and
appropriate colour, lighting, acoustics.
4.8.6 Psychoneuroimmunology: PE interrelationships
P&E
N&E
I&E
Integrated &E
PNI &E
BE Literature Environmental Psychology
72
1 16 21 1
Design 21
1
1 8
0
Architecture 7 1 0 4 0 Design and healthcare
13 3 8 12 12
Environmental health
16 0 9 30 1
Health Literature
Healthcare 5 0
1
3
1 Health
Psychology
11 0 3 6 0
Medical 2 2 1 2 0
Table 1(d)
Classification of data into domain PNI & E
PNI principles have been mainly applied to healthcare settings and have
been shown to contribute to the sense of well-being for the people dwelling
in them. Similar to other research conducted in health care settings, PNI
research acknowledges that the environment that sick people inhabit greatly
influences their healing process (Jones, 1996).
The interior environment is where an individual spends at least three quarter
of his/her time, except in some cases where people work and play in the
exterior environments. These environments that we create would be either
our ‘inherited environments’ or those that are chosen by us (Weinberg,
2001). This new understanding of health clearly recognises a relation

123
between the emotions or mind and the physical part of the body and their
interrelationship with the built environment. It is recognised by all domains
alike that experiences in life are based on individual perceptions and some
of these are determined by the way an individual sees the world, and how a
person can cope with stress or joy. All these perceptions are made in an
environment, be it external or internal, as we inhabit a place all the time
(Ray, 2004). It may be said that experiences of the mind are psychological
and not physical; however, as the mind is connected to the brain, the body
reacts according to the signals sent from the brain without taking fantasy or
reality into account. This culminates in either positive or negative resulting
in being either good or bad for the person involved (Ray, 2004).
The sensual impact of the environment on the person is probably the main
area of study in this domain. Baur-Wu (2002) states that the value of the
role of the senses can be understood better by applying the principles of PNI
to the five important senses of the body namely sight, smell, hearing, taste
and touch. These can be manipulated to achieve betterment for the human
body; creating an environment and therapy based on the sensory organs
which forms an important part in the healing process. The brain and the
senses are linked in such a way that “The cerebral cortex, the thinking part
of the brain and the limbic system, the emotional part of the brain,
communicate with one another and other parts of the body (that is, the
hypothalamus and the sympathetic and parasympathetic nervous systems).
Control and modification of thoughts and perceptions can affect emotions
and bodily functions” (p. 244). When the senses are affected, they
invariably affect the neuroendocrine and immune systems. Some factors and
linkages that Bauer-Wu (2002) points out regarding the sensory organs that
could influence the healing process in therapeutic and favourable
environments, are:
• Smell affects the olfactory nerve connections to the ‘limbic
structures’ (p. 243) which play a significant role in emotion and
memory. This is why certain smells influences the emotion and

124
are regarded as having therapeutic benefits in oncology therapy,
relieving anxiety, insomnia, nausea and so on.
• Sight is affected through stimulation of the optic nerve and also
affects the way a person feels. Rooms with visual stimuli like
colour, murals and so on can enhance the perception of patients
and carers.
• Music therapy is seen to help reduce cancer related anxiety, pain
and nausea.
Control over facilities is another factor that is agreed to be important in
impacting on the psychological, neuroendocrine and immune systems. For
example, having no control over aspects of the surroundings such as noise
levels, and lighting, is seen to affect mental well-being, resulting in
problems such as depression. This, in turn, affects blood pressure levels and
other conditions by adversely affecting the immune system functioning
(Jones, 1996).
Gappell (1992), an interior design practitioner, presented a paper in a
healthcare symposium on the possibilities of applying PNI and its principles
in design practice, suggesting that an environment can stimulate the senses
by influencing the enhancement of human perception of the environment.
The main approaches include sensory applications. Gappell, though, has a
misconception of the discipline of PNI as Cohen (1999) points out in
relation to an advertising article appearing in a newspaper on Gappell’s
practice:
“…if such an education [‘therapeutic intervention of mind-body medicine’] is
necessary, consider a recent advertising supplement to a newspaper (Democrat and
Chronicle newspaper, 1997) that featured an article on how homes may be
therapeutic for mind and body. I don’t disagree with that proposition, but I am
annoyed by the fact that in that article, psychoneuroimmunology was described “as
the art and science of designing interiors to enhance well-being, creativity, and
performance” (Cohen, 1999. p. ii).

125
The misconception of PNI aside, Gappell understood the potential of PNI to
inform better design and health and wellbeing and notes that designing
according to the responses of the senses generates better health and
wellbeing (Gappell, 1992).
The application of research findings has proven beneficial to the users of the
space as demonstrated by the ‘The Medical Investigation of
Neurodevelopmental Disorders’ (the M.I.N.D) institute. They applied
research findings to the space that manages children diagnosed with autism.
The finding that bright colours and patterns over stimulated children with
autism were taken into consideration and the facility was designed using
soothing colours and textures. It proved to be very beneficial for the
children being treated there, soothing them and helping them to calm down
(Henderson et al., 2004).
Siekkienen (2003) reports on a study concerned with measuring the
‘ecopsychological’ effects upon residents of the Puget Sound region. The
inhabitants of this place lived near an airport that produced a lot of noise due
to the air traffic. Their observations recorded various problems such as
cardiovascular problems, and other health impacts including SAD (Seasonal
Affective Disorder) syndrome due to noise pollution. The weather in the
region was also seen to influence the occupants, leading to depression,
anxiety, irritation and so on (Siekkienen, 2003).
As Solomon (1996) further reflects, “just as PNI is helping establish
necessary new models of health, disease and the body itself, perhaps it can
establish, on the basis of evidence, the nature of healing environments”
(Solomon, 1996, p. 83). His paper deals with responses to environmental
design through the understanding of psychoneuroimmunology.
Theoretically, psychoanalysis proposes that, when anger and aggression are
turned inwards, they can lead to depression which causes lower immunity.
Sometimes, something as simple as sleep deprivation can cause lower
immunity (Solomon, 1996). While health care environments which support
the immune system are very important, Solomon (1996) emphasises the

126
need for more PNI research in regard to physical environments, identifying
the following factors pertaining to the BE that help to enhance the immune
system by reducing stress:
• social support, activity and associations
• the development of a good attitude and optimism, which have been
found to be beneficial
• noise controllability, as noise levels lower immune levels
• control of surroundings, as they affect a person’s well-being
• sleep comfort as sleep deprivation causes lower immunity
• controlling feelings of hopelessness and helplessness
• dealing with surrounding smells which have emotion-eliciting power
and can evoke positive or negative emotions which are
immunosuppressants
• opportunities for exercise and
• means and activities for emotional expression which tends to
enhance immunity
• enhancing comfort levels of people visiting patients by providing a
good surrounding.
Following is a table (Table 10) that identifies some select PNI studies in
medical areas as well as areas that look into physical environmental
features. This is a representative sample and not all studies are included.
These are some important papers and monographs (or book extracts) that
may be of relevance to understand the human systems. Other literature in
various domains are included in the appendix section for reference.

127
PNI Domain and Physical Environmental Considerations* No.
Article Author Year Source Phenomenon Consideration of the physical environment
1.
Emotions, immunity and diseases: a speculative theoretical integration
Solomon & Moos 1964 Archives of General Psychiatry, pp. 657-674
Role of emotions in the pathogenesis of physical disease associated with immunological dysfunction Dealt with evidence gathered through various studies on different illnesses from arthritis to cancer.
Nil
2. Psychoneuroimmunology: Past, present and future
Kiecolt – Glaser & Glaser
1989. Health psychology, 8(6): pp. 677-682
Provides a brief overview of the history and current status of behavioural immunology research
Nil
3. Psychological influences on surgical recovery. Perspectives from psychoneuroimmunology
Kiecolt –Glaser et.al 1998 American Psychologist, .Nov. Vol. 53(11): pp.1209-1218
Stress and wound healing. Mental well-being that influences physical functioning
Nil
4. Mind Immunity and Health: The science of psychoneuroimmunology
Evans; Hucklebridge & Chow
2000. Mind Immunity and Health: The science of Psychoneuroimmunology (Book part)
Mental well-being influencing physical well-being, immune functions, stress and cancer.
Nil
5. Psychoneuroimmunology: Psychological influences on immune function and health
Keicolt-Glaser; McGuire; Roble & Glaser
2002 Journal of consulting & Clinical Psychology Jun Vol 70 (3): pp.537-547.
“Immune Dysregulation” can be the influence of negative emotions leading to “a spectrum of conditions” and illnesses
Nil
6. Psychoneuroimmunology: The interface between behaviour, brain and immunity
Mair; Watkins & Fleshner
1994 American Psychologist Dec. Vol. 49 (12) : pp. 1004-1071
While the psychological and behavioral functions can affect the immune system, these effects can in turn influence
Nil
127

128
behaviour patterns.
7. Body and Mind Klaizen Matter-Walstra
1999 http://www.cranial.co.nz/pni_definition.html
A model of PNI is presented Strong emotional and mind consequences pointed out The problem in PNI research is also acknowledged here stating that “individual internal thinking or feelings” cannot be measured, though many experiments on cancer patients have shown positive results
Nil
8. How the mind hurts and heals the body
Ray 2004 American Psychologist, Vol.59, No.1,: pp. 29-40
Our physiological system and psychological system are not separate and distinct from our experiences in life Explains mind-body relationships Belief affects the brain and thus the immune system
Environmental perceptions matter What people believe are their coping skills that count.
9. Psychoneuroimmunologic Factors in Neoplasia: Studies in Animals
Riley; Fitzmaurice & Spackman
1981 In Psychoneuroimmunology, Robert Ader (ED) (Book extract)
Psychological functioning affecting the physiological system
Study on mice in stressfull and non-stressfull conditions of the environment Environmental aspects are studied in respect of immunological functioning
10. Psychoneuroimmunology: An Interdisciplinary Introduction
Schedlowski, & Tewes ( Eds)
1996 Psychoneuroimmunology: An Interdisciplinary Introduction (Book part)
The functioning of the physical systems The mechanism of PNI
Nil
11. Environmental enrichment in mice decreases anxiety,
Benaroya- Milshtein; Hollander; Apter;
2004
European journal of Neuroscience, Vol.20,
Psychological functioning affecting the physiological
Environmental conditions also affect immunologic
128

129
attenuates stress responses and enhances natural killer cell activity
Kukulansky; Raz; Wilf; Yaniv & Pick
pp.1341-1347 system competence as highlighted in studies done on mice
12. Environments that support healing
Jones, Beth Frankowski
1996 ISdesigNET: Magazine, July/Aug
Having no control over the environment is seen to affect the physical system leading to negative mental well-being such as depression and also affecting blood pressure levels. It also adversely affects the immune system functioning. All these factors are seen to be slowing the recovery process
The environment that people are in when sick greatly contributes to the healing process Some factors that are identified here are ‘sense of control’ where the patients would be able to control the surroundings in terms of noise levels, lighting, and so on.
13. Quantum determinism versus indeterminism: Resolving the self-empowerment paradox
Weinberg 2001 The wellness support program URL:http://www.wellness.org.za/html/articles/a-versus.html
Responses of the individual through inherited consciousness Perception of individuals
The interior environment is where an individual spends at least three fourths of his/her time, except in some cases where people work and play in the exterior environments. These environments that we create would be either our ‘inherited environments’ or those that are chosen by us.
14. The Unconscious, Archetypes and the Environment
Dennehy 2003 Ecopsychology: A group project for psychoneuroimmunology by Casey Dennehy, Michael Brown, Dan Siekkinen
The conscious and the unconscious psyche
The environment makes a person who he/she is and ‘if this environment is ignored we may as well be ignoring much of what makes the ‘individual’
15. The Psyche of Psychoneuroimmunology
Brown 2003 In Ecopsychology: A group project for psychoneuroimmunology
Conscious mind, stress Psyche affecting the immune system functioning
Environment and individual perception and their relationship. Goal of
129

130
by Casey Dennehy, Michael Brown, Dan Siekkinen http://academic.evergreen.edu/curricular/pni/ecopsychology.htm
ecopsychology
16. Ecopsychological effects upon residents of the Puget Sound region
Dan Siekkienen 2003 In Ecopsychology: A group project for psychoneuroimmunology by Casey Dennehy, Michael Brown, Dan Siekkinen http://academic.evergreen.edu/curricular/pni/ecopsychology.htm
Natural factors like air, water and place play an important role in the psychology of human moods, relationships, memories, and so on
Environmental factors in Puget Sound region and their residents were studied. Sick building syndrome SAD Syndrome and noise was observed Illnesses like cardiovascular symptoms observed
17. Physiological responses to environmental design: understanding psychoneuroimmunology (PNI) and its application for healthcare
Solomon 1996 Symposium on Healthcare Design. Journal of Healthcare Design. Vol 8, 79-83
Stress influencing immune systems
States some environmental factors relating to PNI. Importance of environmental research in PNI is emphasised
18. Psychoneuroimmunology Part II: Mind-Body Interventions
Bauer-Wu, Susan M 2002 Clinical Journal Of Oncology Nursing July/Aug Vol. 6 No. 4
PNI provides the scientific foundation of several integrative therapies Sensory, cognitive, expressive, and physical aspects that influence the mental well-being in turn affecting the physical well-being
Providing sensory stimuli in the environment helps influence healing
19. Design technology: psychoneuroimmunology.
Gappell 1992 Journal of health care design. Proceedings from the Symposium on Healthcare Design Symposium on Healthcare Design. Vol.4, Pp. 127-
PNI and its principles put to practise in the environment can stimulate the senses influencing the enhancement of human perception of the environment.
Environmental factors and PNI principles applied to lighting, colour and so on
130
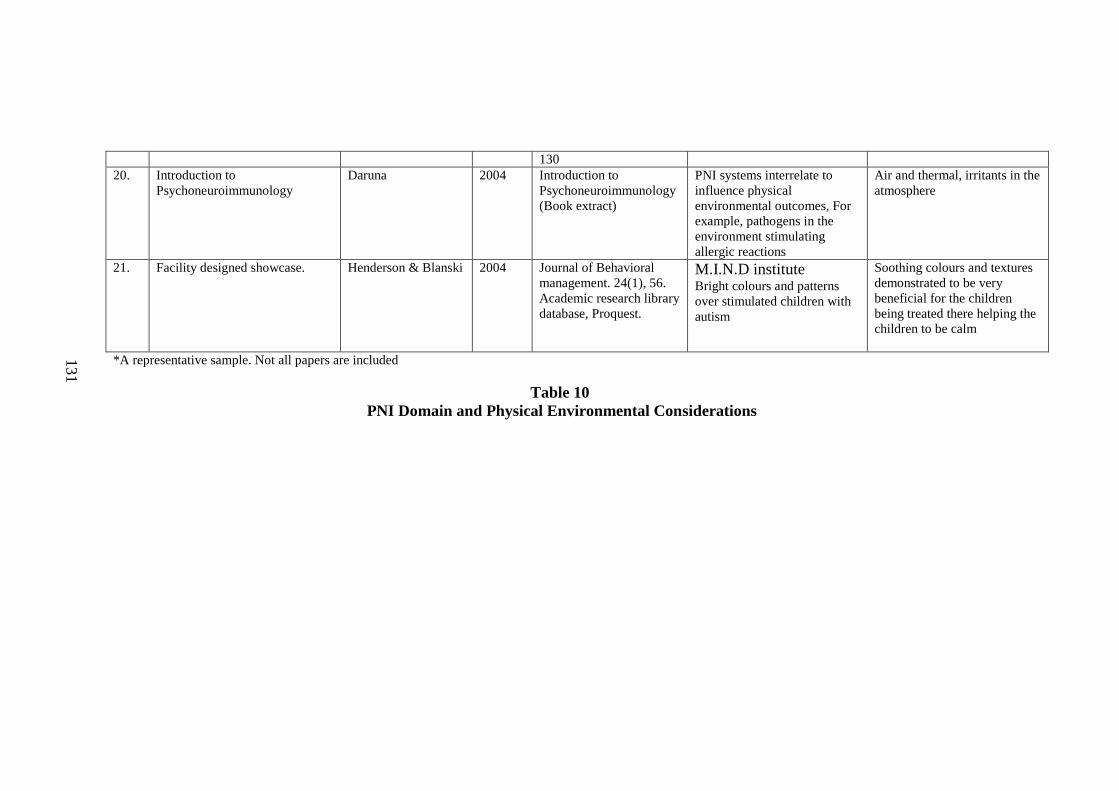
131
130 20. Introduction to
Psychoneuroimmunology Daruna 2004 Introduction to
Psychoneuroimmunology (Book extract)
PNI systems interrelate to influence physical environmental outcomes, For example, pathogens in the environment stimulating allergic reactions
Air and thermal, irritants in the atmosphere
21. Facility designed showcase. Henderson & Blanski 2004 Journal of Behavioral management. 24(1), 56. Academic research library database, Proquest.
M.I.N.D institute Bright colours and patterns over stimulated children with autism
Soothing colours and textures demonstrated to be very beneficial for the children being treated there helping the children to be calm
*A representative sample. Not all papers are included
Table 10 PNI Domain and Physical Environmental Considerations
131
132
4.9 Discussion of Implications of the review results
From this analysis of the literature on health and well-being influenced by the
physical environment, several patterns have emerged as listed below:
• Firstly, the literature can be found in books, journals and websites across
different domains. This makes it difficult for someone searching for a
related topic in one domain to identify aspects reported in other domains.
• Secondly, a large body of literature has focused on identifying a set of
environmental characteristics and attributes associated with the impact on
people, such as specific environmental features causing stressors (Russel
& Snodgrass, 1987; Evans & McCoy, 1997; Kaplan, 1995; Ulrich, 1986,;
Rosenman, 1994; Schedlowski &Tewes, 1999; Bell et al., 2001). These
studies have examined spatial characteristics ranging from psychological,
physiological and social aspects to the measurement of certain elements
and stimulants (Stokols, 2000; Gifford, 1997; Kaplan, 1995; Bell et al.,
2001; Canter, 1997; Heerwagen, 1990; Rappoport, 1990; Altman &
Rogoff, 1987).
• Thirdly, researchers have demonstrated that a set of core environmental
characteristics, including, sensual perceptions, spatial elements,
sociocultural elements, personal characteristics and modes of adaptation
can relate positively or negatively to a person’s health and wellbeing
across a variety of domains studied (Frumkin, 2006; Ulrich & Zimring,
2004; Zeisel, 2003; Parsons & Tassinary, 2002; Solomon, 1996; Dorn,
1996).
• Fourthly, understandings of environmental human experiences and
responses within the domains overlap or cross over.
• Fifthly, while there are considerable conceptual understandings of PE
relationships in various dimensions, most empirical work that directly

133
concerns health and wellbeing have been either conducted in healthcare
settings or regarding stress.
• Lastly, a number of researchers have looked at design and human
response factors, but very few have systematically looked at specific
outcomes of negative wellbeing and subjective responses.
4.9.1 Classification of the Relationships Linkages
Concept linkages
Eg. stress, arousal
theories
Empirical findings
Eg. control, privacy,
stressors
Spatial response
linkages
Response recognition
Figure 15 Sample relationships
The conceptual and empirical understandings from the domains revealed linkages
which are shown in Figure 15. Given the complex and indirect nature of these
connections, it was relatively difficult to depict the relationships. As a result the
identifier tool as illustrated in Chapter 3 on Methods (Figure 8) was used to
classify the health and well-being interrelationship to the physical environment
and health research domains. The matrices (Tables 1 and 2) were used to indicate
that there is an overlap within the domains on the understanding of the outcome of
health and well-being and PE inter-relationships as illustrated in Figure 8. The
current understandings of these interrelationships have been described in the
previous section.
Perhaps some of the most important findings linking the environment to human
health and wellbeing come from studies in environmental psychology, healthcare

134
environment design and ‘sick building syndrome’ research. As discussed earlier,
the degree of environmental ‘fit’ and the ability of the environment to provide
beneficial elements is highly related to the occurrences of physiological symptoms
(Parsons et al, 1998); empirical evidence of positive health factors (Cox et al.,
2004); control of immune regulations (Ulrich, 1986); cortisol production (Riley et
al, 1992); depression (Galea & Vlahov, 2006); work related stress (Stokols, 2000);
‘attention restoration theory’ (cognitive model) (Kaplan, 1995); and ‘nature
restoration theory’ (‘affect’ model) (Ulrich, 1983). They show that, when the
environment and person act on each other in a consistent and equivalent way, the
level of positive impact on health and wellbeing increases, as opposed to
situations and places where the person have little or no control.
In response to the above mentioned empirical and conceptual research in support
of the PE integrative system model, we can see the environment as having three
major influential characteristics. Firstly, it contains various stimuli which are
potentially a source of negative or positive health outcomes; secondly, the stimuli
can act as triggers in eliciting responses; and, finally, the environment can act on
the person’s individual characteristics in terms of adaptive responses and belief
processes. People’s perception and their beliefs are usually a turning point in their
experience of place. A person perceives a place as soon as s/he encounters a
setting. The outcome influences many other activities that subsequently take place
within the physical environment. The findings demonstrate that emotionally
satisfying surroundings give a positive outcome of anticipation of, and reaction to,
the events that are to take place inside the human body.
Most empirical studies directly related to health and well-being conducted in
healthcare facilities have produced some excellent results as seen in the
‘Planetree’ model of healthcare and the ‘Pebble Projects’. Ulrich’s (1986) findings
prompted the healthcare industry to undergo a massive development, keeping the
users and providers in mind. Hospitals under the Planetree model can be seen as
enhanced user friendly environments which speed the healing functions of the
person. For a further review on healthcare environment research refer to Ulrich et

135
al (2004). Their work provides a thorough understanding of the studies and
findings produced in this research domain.
4.9.2 Core recognised PE interrelationship relating to integrative system approach
Some of the key dimensions of research studies that relate to the integrative
approach to health and well-being are presented in the model below (Figure 16).
The ‘PE Integrative Systems Flow Model’ model depicts the stages of
inter/transaction that a person goes through when in contact with the physical
environment. They are developed from the results that emerged from the review
analysis and show overlaps and crossovers across the domains. The model follows
the PE Integrative systems model according to the PNI framework showing the
flow of responses and reactions in influencing health and wellbeing outcomes.
These interrelationships when in conflict with responses culminate in the
development of various negative health outcomes. Subsequently, positive
interrelationships may be responsible in maintaining better health and wellbeing
outcomes.
The model presents some of the core recognised characteristics of PE
interrelationships in the various domains and their overlap in the research
understandings. It demonstrates the integration of conceptual, theoretical and
empirical findings and understandings that are of relevance to an integrated
picture of environment acting on the human systems. It starts with the impact
from physical environmental stimuli and ends with the outcomes of human
responses. The information derived from the environmental stimuli is processed
by the human systems, and transformed through perceptual and cognitive analysis
into psychological and physiological outcomes relating to health.

136
Psychophysiological Stimulants
Human response Stimulants
Environmental determinants
Sensory response
Sensation
Senses
Perceptual analysis
Cognitive analysis
Health Research
BE Research
Human cognition Human perception
Environmental perception
Environmental cognition
Stage 1 – Sensory awareness (+ or -)
Psychophysiological Stimulants
Human response Stimulants
Physiological responses
Adrenaline /cortisol production
Physiological arousal/ internal activity
Sweating Fatigue Breathing
Health Research
BE Research
Physiological outcome Physiological evidence
Physical arousal symptoms
• Blood pressure • Heart rate • Pulse rate • Respiratory
level • Sal ivory levels
Physiological outcome
Reaction (eg. arousal)
• Assessment • Emotional & behavioral attitudes • Place attachment • Privacy • Control • Aesthetics • Stressors • Hygiene/Cleanliness • Territoriality • Sociocultural issues • Adaptiveness
Conceptual frameworks/empirical findings Health Research
BE Research
Conceptual frameworks/empirical findings Environmental responses from inter/transactional experience
Psychophysiological Responses
Outcome (eg. Stress/anxiety)
Emotions Feelings ‘Fight - flight syndrome’
Stage 2 – Psychological outcome (+ or -)
Stage 3 – Physiological Outcome (+ or -)

137
Figure 16 PE Integrative Systems Flow Model:
Health and well-being outcomes from PE interrelationship
The four stages – depicted in the model (Figure 16) range from environmental
awareness and stimuli to health outcomes – integrate the different levels of
understanding regarding human psychophysiological processes and environment
inter/transactions in the various domains, demonstrating the overlaps and
linkages. This PE integrative health system approach is the process by which PE
interrelationships that influence and improve health and wellbeing is understood.
The integrative system application to design would act as a tool to facilitate
positive health and wellbeing outcomes.
Environmental stimuli influence human body systems in several ways. These
interactions may lead to positive or negative wellbeing. Research in health as well
as built environment while describing them differently appears to understand them
in similar ways. Stage 1 depicts the sensory awareness of a person when s/he
enters a place/space. A person perceives and cogitates with the help of the sensory
systems (Rosenzweig et al., 1999). This is followed by Stage 2 where the
perception and cognition of the surroundings elicit several emotional responses
and reactions. Stage 3 brings forth the physiological responses that occur as a
result of the psychological reactions. Any number of reactions can emerge leading
to Stage 4 and influencing health and wellbeing. These stages together form the
Health Research
Health outcomes
Stage 4 – Health Outcomes (+ or -)
• Cardiac problems • Cancer • Blood pressure disturbances • Mental health • Sleep disturbances • Allergic reactions • Respiratory infections • Skin problems • Behavior issues • Chronic illness

138
sequence of human responses that may be the outcomes of person environment
interrelationships in respect to health and wellbeing.
4.9.3 Environmental factors emerging from the review
Some of the factors that have emerged from the review with respect to
environmental influences are illustrated and described in the table (Table 11)
below. They have been categorised in the various sections according to the model
above (Figure 16). They consist of sensory, perceptual and cognitive responses.
These responses are then described in terms of environmental stimulants,
experiences, arousals, process, and outcomes with select examples. These
outcomes emerged through the review of environmental and health domains.
The table describes some examples of positive and negative stimuli in the built
environment and how they can contribute to health outcomes. They are also
classified into positive and negative human responses as well as some positive and
negative outcomes. The responses are categorised into psychological or emotional
responses and some physiological outcomes evolving from them.
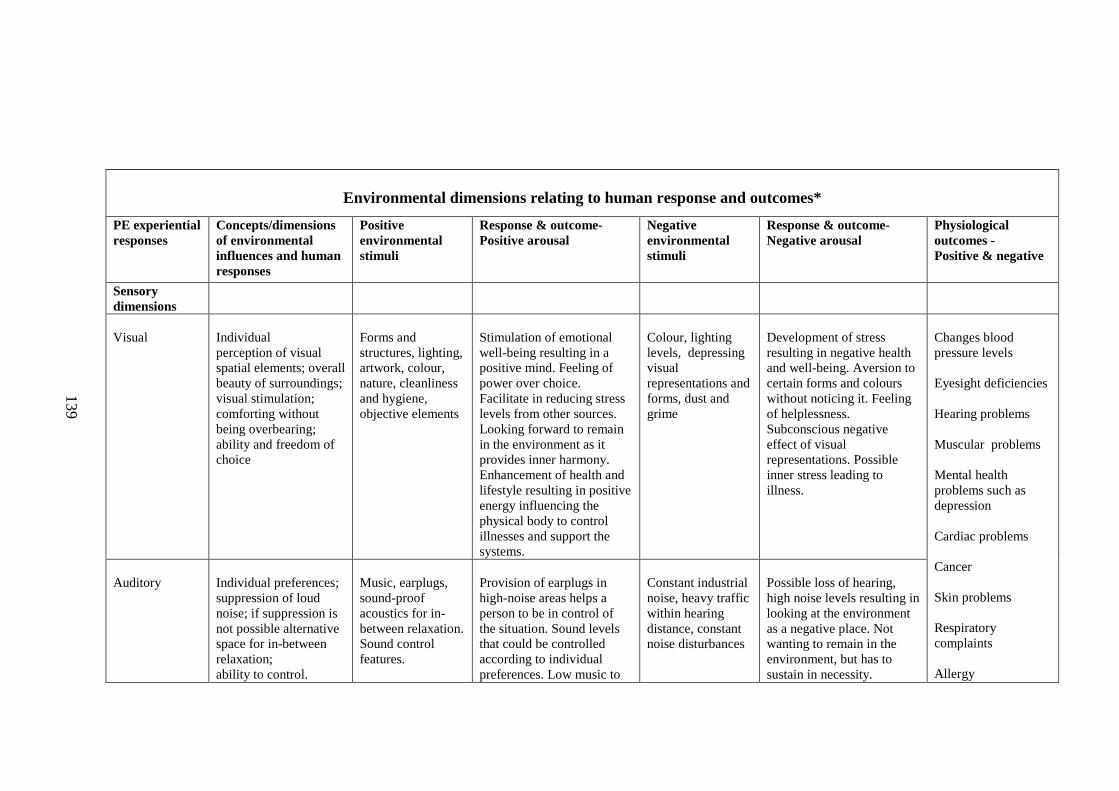
139
Environmental dimensions relating to human response and outcomes*
PE experiential responses
Concepts/dimensions of environmental influences and human responses
Positive environmental stimuli
Response & outcome- Positive arousal
Negative environmental stimuli
Response & outcome- Negative arousal
Physiological outcomes - Positive & negative
Sensory dimensions
Visual
Individual perception of visual spatial elements; overall beauty of surroundings; visual stimulation; comforting without being overbearing; ability and freedom of choice
Forms and structures, lighting, artwork, colour, nature, cleanliness and hygiene, objective elements
Stimulation of emotional well-being resulting in a positive mind. Feeling of power over choice. Facilitate in reducing stress levels from other sources. Looking forward to remain in the environment as it provides inner harmony. Enhancement of health and lifestyle resulting in positive energy influencing the physical body to control illnesses and support the systems.
Colour, lighting levels, depressing visual representations and forms, dust and grime
Development of stress resulting in negative health and well-being. Aversion to certain forms and colours without noticing it. Feeling of helplessness. Subconscious negative effect of visual representations. Possible inner stress leading to illness.
Auditory
Individual preferences; suppression of loud noise; if suppression is not possible alternative space for in-between relaxation; ability to control.
Music, earplugs, sound-proof acoustics for in- between relaxation. Sound control features.
Provision of earplugs in high-noise areas helps a person to be in control of the situation. Sound levels that could be controlled according to individual preferences. Low music to
Constant industrial noise, heavy traffic within hearing distance, constant noise disturbances
Possible loss of hearing, high noise levels resulting in looking at the environment as a negative place. Not wanting to remain in the environment, but has to sustain in necessity.
Changes blood pressure levels Eyesight deficiencies Hearing problems Muscular problems Mental health problems such as depression Cardiac problems Cancer Skin problems Respiratory complaints Allergy
139

140
stimulate creative thinking according to preferences. Contributing to positive mental wellness resulting in overall health and well-being.
Developing stress due to this resulting in possible health conditions affecting overall well-being. Feeling of helplessness. Factors affecting cognitive growth.
Olfactory
Individual sensitivity, air cleansing facilities, provision of light aromatic smells. Controllable smells/aroma according to individual preferences; control over premises. Exposure to constant odour.
Aroma, low-key scents. Provision of air purifiers and deodorants in toilets and key areas or on individual basis in workplaces. Usage of perfumed paints in places identified as high negative hazard smell areas
Good aromatic smells helps in energising the senses and creating positive emotions resulting in enhancing overall health and well-being. Influences the mind supporting wellness in an overall form.
Bad odour, constant strong smells from chemicals etc.
Bad odour produces stress and resentment of the surroundings results in negative emotional states. Some constant strong smells over long periods can affect the sense of smell. Perceiving smells subconsciously results in distress further ensuing negative health conditions.
Tactile
Individual preferences; soft edged tables and chairs, furnishing fabrics according to standard of usage (e.g. Some fabrics cause dampness and friction during prolonged usage) Touch sensitive furniture, walls and space. Temperature control (thermal quality). Risk free flooring and surfaces
Edges moulded for comfort to prevent injury from prolonged use. High usage areas to be designed according to user (individual or group) preferences. Touch supportive surfaces. Free of allergens.
Comfortable surroundings and furniture according to user preferences and control stimulates physical and emotional well- being. Sense of positive touch helps in enhancing sense of the environment.
Hard edges, rough and splintery surfaces, irregular grouting of tiles, irregular surface preparations, factors beyond control, subjective reaction, subconscious facilitation.
Possible injury from surface visible and non-visible abrasion. Aversion to surroundings due to constant usage of uncomfortable space and furniture resulting in negative health outcomes. Temperature uncontrollability resulting in uncomfortable conditions. Ergonomically unsound furniture resulting in long-term negative health outcomes. Subjective
Chronic problems such as asthma, backache etc. Obesity Deficiencies Sweating properties Injuries Physical resistances
140
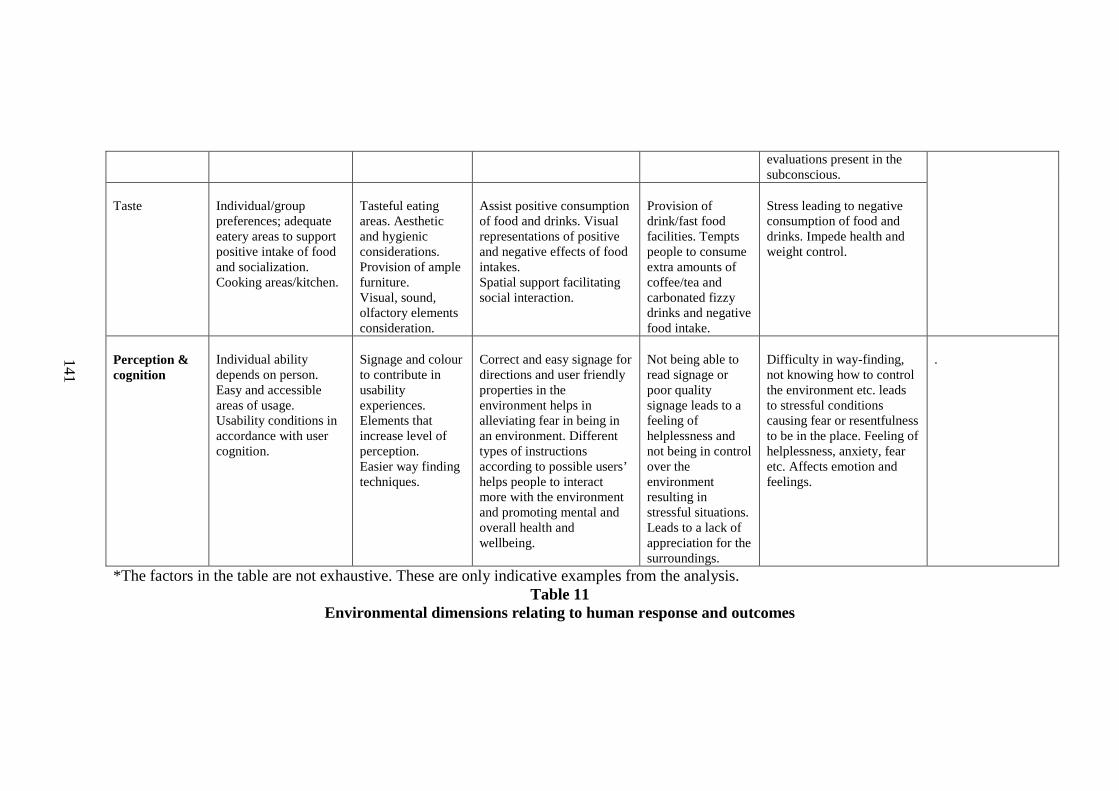
141
evaluations present in the subconscious.
Taste
Individual/group preferences; adequate eatery areas to support positive intake of food and socialization. Cooking areas/kitchen.
Tasteful eating areas. Aesthetic and hygienic considerations. Provision of ample furniture. Visual, sound, olfactory elements consideration.
Assist positive consumption of food and drinks. Visual representations of positive and negative effects of food intakes. Spatial support facilitating social interaction.
Provision of drink/fast food facilities. Tempts people to consume extra amounts of coffee/tea and carbonated fizzy drinks and negative food intake.
Stress leading to negative consumption of food and drinks. Impede health and weight control.
Perception & cognition
Individual ability depends on person. Easy and accessible areas of usage. Usability conditions in accordance with user cognition.
Signage and colour to contribute in usability experiences. Elements that increase level of perception. Easier way finding techniques.
Correct and easy signage for directions and user friendly properties in the environment helps in alleviating fear in being in an environment. Different types of instructions according to possible users’ helps people to interact more with the environment and promoting mental and overall health and wellbeing.
Not being able to read signage or poor quality signage leads to a feeling of helplessness and not being in control over the environment resulting in stressful situations. Leads to a lack of appreciation for the surroundings.
Difficulty in way-finding, not knowing how to control the environment etc. leads to stressful conditions causing fear or resentfulness to be in the place. Feeling of helplessness, anxiety, fear etc. Affects emotion and feelings.
.
*The factors in the table are not exhaustive. These are only indicative examples from the analysis. Table 11
Environmental dimensions relating to human response and outcomes
141

142
4.10 Summary
In summary, this analysis derived and produced the results from the review using
the five step method devised by Cooper (1987). The linking of the
interrelationships between domains occurs through a transdisciplinary framework.
The outcome produced results that show overlaps within the domains and
demonstrated the potential for an interdisciplinary, transdisciplinary and
multidisciplinary framework to understand PE interrelationship to health and
wellbeing.
Exploration of research literature in the area of built environment and design and
health indicates that the physical environment is an important component of the
multidimensional aspects of a human being. While much research on the health
aspects of person-environment interaction focuses on psychological aspects and
stress, social interaction, environmental elements and factors for example toxins,
air quality and so on, little attention has been paid to the role of the physical
environment that influences the mental wellness contributing to the longitudinal
effects on the holistic health of a person. A reflection of the research is further
portrayed in the next chapter.
143
Chapter 5
Conclusion
The preceding chapters of this thesis discussed:
• The understanding of health and wellbeing in selected domains (Chapter
4)
• The interrelationships between the physical environment dimensions and
the human psychological and physiological systems (Chapter 4)
• Psychoneuroimmunology as a platform for research in these areas
(Chapter 2)
• A methodology to fit the purpose of this study (Chapter 3)
Chapter One of the dissertation presented the aims and objectives of the study
against the background of research that revealed the need for a more integrated
appreciation of the person and health, the environment, and their
interrelationships. The chapter also gave a brief description of the approach
adopted for the study as well as an overview of the structure of the thesis.
Chapter Two briefly introduced psychoneuroimmunology (PNI) which served as a
platform to categorise the aspects of the person relevant to this study. In this
study, the person (P), as part of the person environment (PE) relationship is
conceptualised in terms of an interrelationship of the mind (psychological
systems) to the body systems (physiological systems).
Chapter Three explained the approach of the study, giving specific emphasis to
how the data (in the form of literature) were analysed, organised and presented to
best highlight existing research studies undertaken and their interrelationship.
Using the PNI/integrative system framework, Chapter Four examined theoretical
and empirical research undertaken in the general area of health and medicine, as
well as research undertaken in the area of design and built environment. The

144
outcome as seen in this chapter is a multifaceted picture of the existing research,
highlighting an array of PE relationships and integrative health dimensions and
outcomes. This chapter also discusses some implications of the findings.
As a conclusion, this chapter (Chapter 5) is a brief reflection on the study
described in this thesis. It provides further recommendations and possibilities for
its application to practice, education and research. It also highlights the need for a
transdisciplinary approach to the field of health and built environment in order to
capture a deeper understanding of the interrelationships and outcomes. In order to
gain an holistic understanding of health and environment interdependency, this
chapter also reflects on the patterns of person environment inter/transactions;
relationships they form which influence health outcomes and the potential for the
design of the built environment to more positively engage with a person’s mental
and emotional state, their physical health, and their well-being generally. It returns
to the original research question and reflects on the extent to which the capacity of
the BE as a catalyst for health and well-being is recognised in past and current
research. Lastly, this chapter also provides a brief conclusion to the thesis,
summarising the previous chapters, and in the process, reiterating the main
questions of the thesis, the findings in relation to the questions, and their
implications for future research and design practice.
5.1 Summary of study process
As mentioned earlier the methodology described in Chapter Three was adapted for
this study’s purpose. In addition, there was a need to develop specific methods for
interrelationship studies that reflect multi and transdisciplinarity in approach and
understanding. The study process outlined below is a contribution towards this
end.
The important features presented in this thesis are summarised in Table 12. There
are 6 stages - (I) to (VI) - that illustrate these features; the process which captures

145
the health and well-being dimensions of the physical environment developed from
research that addresses PE relationships. Each level represents a general (I & II)
or specific task (III-VI) that this study involved and discussed in previous
chapters. Collectively it provides an approach for researchers and designers
working in this area.
The ‘interrelationship tool’ used to categorise and classify data also serves to
demonstrate the process used to arrive at a conclusion drawn from emerging
concepts gathered from earlier processes involved in this research approach.
Specific tasks in the different stages are represented by miniature versions of a
figure used to illustrate either a mind map, concept map or a map designed to
stimulate a decision for the particular task that was explained in the body of this
thesis. ‘Process’ represents the order of processing information that emerged from
the data/research literature. The information is processed by a series of analytical
methods to determine the inter-relationship linkages.
The outcome constitutes maps of relevant data sources which can be accessed
from the short reference list in the appendices section and correspondingly from
the thesis reference section. The number of studies corresponding to each of the
key domains and interrelationships – Tables 1.1 comprising literature domains
and Table 2 interrelationship studies – is represented. The map therefore provides
a reference tool that enables researchers and designers to access the breadth of
knowledge available in relation to the built environment and health and wellbeing
in an integrated and systematic manner.
One of the other outcomes of this research was the process of the study or the
method designed to study the complex interrelationships in different domains
through a transdisciplinary approach. The process as illustrated in Table 12 related
to the technique by which the data were categorised and classified. It allowed the
study to identify specific issues and relationships existing between domains while
being able to study existing interrelationship as well as pointing out possible
interrelationships.

146
Stages Process Tools Outcome 1 PE Relationships Literature recognition
Database search Selection of analysis data
II Relationship recognition o Conceptual
Propositions
(Fig 7 )
Relationship mapping
III Sifting and assigning - Object tool
(Table 2)
Finding order Planning Classification
IV Literature classification - Comparison
(Table.1.1 )
Domain Identification
V Domain linkages –interelationship tool o Identification o Overlaps
(Fig.15 )
Recognition of interrelationships and overlaps
VI Similarities and interrelationships o PE inter/transactional
process o Health process
(Fig.16 )
Pattern recognition Model development
Table 12 Information processing and outcomes model
5.2 Reflections on the research findings
The aim of this study was to identify properties of the physical environment that
influence health outcomes as a result of PE interrelationships. The study was able
to explore and identify specific literature that looked at this aspect of the built
environment as well as demonstrate how the research could inform human health
and wellbeing when classified in an integrative systems model. The outcomes of
Figure. . Matrix 1 & 2 interrelationship relationship
Domain Matrix
Relationship Matrix
2122Medical
6311Health Psych.
1315Healthcare
HEALTH Lit.
130 9 16Envt. health
41 7Architecture
1 21 16 1 72Envt. Psychology
12128 313Design and healthcare
81121 Design
BE Lit.
PNI(PsychoneuroImmunology)
Integrated health
I &E(Immune &Environment)
N&E(Neuro & Environment)
P&E(Psycho & Environment)
2122Medical
6311Health Psych.
1315Healthcare
HEALTH Lit.
130 9 16Envt. health
41 7Architecture
1 21 16 1 72Envt. Psychology
12128 313Design and healthcare
81121 Design
BE Lit.
PNI(PsychoneuroImmunology)
Integrated health
I &E(Immune &Environment)
N&E(Neuro & Environment)
P&E(Psycho & Environment)
Psyche Physical
HH
MW
PW
DE
PEI
ES
CE
42, 47, 44, 66, 22, 23, 7, 101, 103, 104
2, 37, 92, 93, 50, 41, 7, 68, 63, 10, 40, 56, 4, 60, 107, p16, p19,61, 90, 37, 64, 92, 29, 63, 19, 41, 89, 10, 72, 82, 30, 56, 24, 9, 97, 20, 27, 17, 4, 105,
3, 16, 64, 90, 37, 38, 92, 63, 19, 10, 40, 67, 72, 73, 65, 82, 30, 61, 74, 56, 97, 33, 76, 87, 97, 27, 17, 70, 55, 88, 4, 105, 60, 114,116,117, 119
1,64, 92, 38, 50, 52, 41, 89, 10, 40, 67, 2, 56, 24, 97, 33, 43, 76, 87, 57, 80, 48, 79, 34, 81, 97, 98, 99, 100, 80, 85, 40, 104, 32,
1, 2, 3, 61, 16, 83, 90, 59,38, 29, 93, 94, 95, 50, 63, 4, 52, 19, 68, 89, 10, 67, 72, 73, 5, 82, 30, 74, 56, 51, 24, 97, 9, 33, 43,76, 87, 7, 20, 57, 80, 48, 79, 34, 100, 54, 52,
47, 66, 83, 54, 102, 103, 104, p1, p2, p3, p4, p5, p6, p7, p8, p9, p10, p11, p12, p13, p14, p15, p19, 108,109,
61, 83, 84, 25, 52, 10, 24, 100, 40, 105, 41, 7, 10, 24, 107, p19
16, 52, 24, 76, 32, 88, 105, 110, 111,118,
91, 92, 94, 50, 52, 41, 68, 45, 89, 10, 24, 76, 81, 97, 11, 99, 100, 102, 40, 80,
13,83, 84, 78, 5, 91, 94, 50, 52, 89, 10, 24, 6, 98, 58, 76, 98, 100, 40, 105, 107, 117, 118, 119, p15, p16, p17
7, 63, 89, 10, 107, 52, 89, 10, 33, 105
52, 63, 89, 10, 33, 76, 97, 32, 105
52, 7, 68, 45, 10, 33, 76, 81, 97, 98, 100, 102, 40, 80, 85, 104, 27, 32, 46, 88, 4, 105, 31, 106, 107, p7, p16,
13, 16, 83, 84, 25, 90, 92, 52, 47, 68, 89, 10, 24, 6, 33, 43, 76, 98, 100, 40, 32, 46, 71, 88, 4, 105, 106, 107, p13, p15, p16, p17, 116
47, 66, 51
P1, p2, p3, p4, p5, p6, p7, p8, p9, p10, p11, p12, p13, p14, p15, p16, p18, p19,109
Pe
rson
Env
iro
nme
nt R
ela
tions
hip
Stu
die
s
Health and wellbeing class ification
Fig. C lass ification of PE relationships st udies to hea lth model
Psychophysiological Stimulants
Human response Stimulants
Physiological responses
Adrenaline /cortisolproduction
Physiological arousal/ internal act ivity
Sweating,
Fatigue
Breathing
Health
Research
BE
Research
Physiological outcomePhysiological evidence
Physical arousal symptoms
Blood pressure
Heart rate
Pulse rate
Respiratory level
Sal ivory levels
Physiological outcome
Psychophysiological Stimulants
Human response Stimulants
Physiological responses
Adrenaline /cortisolproduction
Physiological arousal/ internal act ivity
Sweating,
Fatigue
Breathing
Health
Research
BE
Research
Physiological outcomePhysiological evidence
Physical arousal symptoms
Blood pressure
Heart rate
Pulse rate
Respiratory level
Sal ivory levels
Physiological outcome
Health
Research Health outcomes
Cardiac problems
Cancer
Blood pressure disturbances
Mental health
Sleep disturbances
Allegic reactions
Respiratory infections
Skin problems
Behavior issues
Chronic i llness
Health
Research Health outcomes
Cardiac problems
Cancer
Blood pressure disturbances
Mental health
Sleep disturbances
Allegic reactions
Respiratory infections
Skin problems
Behavior issues
Chronic i llness
Psychophysiological
Stimulants
Human response
Stimulants
Environmental determinants
Sensory response
Sensation
Senses
Perceptual analysis
Cognitive analysis
Health
Research
BE
Research
Human cognitionHuman perception
Environmental perception
Environmental cognition
Psychophysiological
Stimulants
Human response
Stimulants
Environmental determinants
Sensory response
Sensation
Senses
Perceptual analysis
Cognitive analysis
Health
Research
BE
Research
Human cognitionHuman perception
Environmental perception
Environmental cognition
Reaction
(eg. arousal)
Assessment
Emotional & Behavioral Attitudes
Place attachment
Privacy
Control
Aesthetics
Stressors
Hygiene/Cleanliness
Territoria lity
Sociocultural issues
Adaptiveness
Conceptual frameworks/empirical findingsHealth
Research
BE
Research
Conceptual frameworks/empirical findings Environmental responses from inter/transactional experience
Psychophysiological Responses
Outcome
(eg. Stress/anxiety)
Emotion
Feelings
‘Fight - flight syndrome’
Reaction
(eg. arousal)
Assessment
Emotional & Behavioral Attitudes
Place attachment
Privacy
Control
Aesthetics
Stressors
Hygiene/Cleanliness
Territoria lity
Sociocultural issues
Adaptiveness
Conceptual frameworks/empirical findingsHealth
Research
BE
Research
Conceptual frameworks/empirical findings Environmental responses from inter/transactional experience
Psychophysiological Responses
Outcome
(eg. Stress/anxiety)
Emotion
Feelings
‘Fight - flight syndrome’

147
the study are: (1) a methodological framework: the study process used Cooper’s
(1998) method and further developed it to include tools adapted from White
(1987) to find and map relationship linkages; (2) a framework/map of research
sources that identify outcomes of PE interrelationships to health and wellbeing.
The outcomes are graphically conveyed in Table 1, 1.1, 2, and Figure 16; (3) the
potential to develop transdisciplinary frameworks (Figure 16).
Health and wellbeing linkages
The healthcare environment researchers (such as Ulrich, 1986, 1989, 1991; Ulrich
et al., 2006) identify elements that improve quality of care, and recognise that
healing occurs more rapidly when people are exposed to conducive surroundings.
Research in this area also proposes that the immune system is indeed affected by
mental wellness. Collectively these understandings are the foundation of this
study.
An awareness of the benefits to health from responsive environments generated a
movement to reforming aspects of the healthcare industry and inspiring programs
such as the ‘Pebble Project’ and ‘Planetree’ health care system. The increased
complexity of determining the effect of space/place on the human psychological
and physiological systems requires multidisciplinary and/or interdisciplinary
inquiry methods. While research on physical environments associated with health
and wellbeing mainly concentrate on the overall functionality of the body – such
as influences and benefits of place in exercise, anthropometrics, environmental
qualities (thermal, air quality and so on) – there is less research concerning the
environmental influences on the physiological (the immune system functionality)
and PNI systems functionality (psychological systems acting on the
physiological systems and vice versa) which are responsible for health and well-
being.
As noted in the second chapter, it is reasonable to expect that the environmental
influences of health (psycho/neuroendocrine/immune systems) can be recognised
by analysing the studies conducted on different factors of the physical
148
environments. Psychological satisfaction and wellbeing are essential because they
serve to control the physiological systems of the body, aid the ability of the body
to maintain better health and wellbeing, and perhaps most importantly, improve
quality of life in individuals. Therefore, the purpose of this study was to describe
and evaluate current understandings of environmental factors impacting on health
and wellbeing from the PNI perspective. With that purpose in mind, only findings
directly related to the PNI model were addressed. The PNI model helped to
conceptualise ‘P’ (person) as well as analyse the conceptual understandings and
research directly and indirectly related to health and wellbeing as a result of PE
relationships.
PE Relationship research
The thesis reviews studies about human wellbeing from 1975 to 2006,
representing psychological and physiological wellbeing in conjunction with the
physical environment. The method was essentially designed and adapted from
Cooper (1998). The tools for sorting and analysing were further adapted from
White (1986).
Studies in different domains existing in environmental and health research were
explored. The selected studies primarily incorporated the characteristics of the
physical environment in PE relationships. In the late 1970s to mid 1990s more
environmental researchers were studying the different dimensions and impacts of
the physical environment on a person’s experiences and responses and building on
the work of other studies in the process (Proshansky et al., 1976; Bronfenbrenner,
1979; Proshansky & Fabian, 1986; Altman & Rogoff, 1987; Gifford, 1987;
Stokols &Altman, 1987; Rappoport, 1990; Proceedings of 11th and 12th EDRA
Conferences, 1991, 1995; Kaplan & Kaplan, 1989, 1995; Gifford, 1996; Canter,
1997). Around this time psychoneuroimmunology also came into existence and
revealed that the physiological system responds to the psychological system (Ader
& Cohen, 1975; Cousins, 1983; Ader et al, 1991; Mair et al, 1994; Schedlowski &
Tewes, 1996).

149
Associated with the importance of PE relationships are different dimensions of the
person as well as the physical characteristics of the environment. The
psychological dimensions of the PE relationship were identified in the research
synthesis as an important issue in health and wellbeing, in keeping with the PNI
framework. As a primary human response that influences the physiological
system, the person is capable of subjective and objective interpretations and
reactions. While this area is well represented in the BE domain, it seems its
impact on the physiological system and consequently on health is not well
recognised, perhaps because of the lack of a theoretical framework. Although the
general area is under study in the environmental psychophysiology domain, a
detailed and integrated understanding of health and wellbeing is yet to be
conveyed in a tangible way.
This seems illogical as it has long been conceptualised and supported by a body of
empirical findings that human responses to the physical environment impact on
the psychological system. The healthcare settings research domain reveals this and
has generated sufficient evidence of better physical healing possibilities from
environmental influences; psychological, social and physical. However, not many
of these studies have been extended to other areas of environmental research such
as workplace, residential, institutional and social settings. The increased
importance of environmental influences - such as control, privacy, spatial aspects,
sensual awareness, being able to direct perceptive and cognitive capacities; and
being able to facilitate social interaction at all environmental levels - documented
throughout the review is notable. While the review did not encounter many studies
that directly documented the interrelationship of PE inter/transaction to the PNI
model, the studies explored provide evidence that the dimensions of the PE inter-
relationship to specific dimensions of the health model are well documented,
although not in a direct way.
Also notable among the study outcomes is the role of stress in PE
inter/transaction. This phenomenon was seen to span almost all domains and
classifications. This was expected to be the case in all the domain studies, but the
fact that there is overlap within the classification in relation to physiological

150
responses is notable. For instance, environmental behaviour research documents
many elements – such as noise, lighting, and so on – as being environmental
stressors (Gifford, 1996; Bell et al., 2001) and it also recognises environmental
stressors as being major culprits in developing many conditions such as blood
pressure inconsistencies (Bell et al., 2001; Dorn, 1994). Healthcare research also
recognises lighting, noise and so on as being responsible for disrupting mental
wellbeing and generating physiological responses (Ulrich et al., 2004). However,
this can be expected because exposure to stressful events and surroundings is not
confined to any particular type of environment. On the other hand, environmental
and health research both identify such exposures as well known influences of
health and wellbeing. These are also recognisable as environmental
characteristics. There seems to be a dearth of studies that recognise that
environmental stress impacts on the immune systems thereby in the process
affecting health and wellbeing.
The disciplines concerned with the built environment (BE) have traditionally
attempted to be inclusive of a wide range of interests in the physical environment
and human relationships, as well as behaviours and activities taking place in the
environment. Although elements of physical and human BE can be studied in
isolation, any approach that focuses on the connections between humans and their
environments contributes to the development of a holistic, integrated perspective
for PE inter-relationship to health research. The theories of psychological and
biological relationships in built environment research that have been discussed in
the previous chapters provide the basis for such an approach. BE researchers
adopting this approach make the important connection between physical and
human environments to determine their influences on health and well-being.
These psychological dimensions of human behaviour in BE would benefit from
studies of the environmental information important for decision making in design,
as well as from how the information is attained and used to develop health
responsive environments.

151
5.3 Future recommendations
From the current review of the research in the areas identified, it is apparent that,
even in light of the limitation to the existing research, further significance should
be given to the physical environment and its impact on person’s integrative
systems such as PNI, to address human health outcomes of person environment
inter/transactions. This can be done by:
• Further research into aspects relating the PE interrelationship with
health, well-being, and illnesses
• Providing spaces and places that influence overall health and well-
being positively and thereby reduce the risk of illness
• Managing the social outcomes and the social impact of aesthetic
aspects of the physical environment through design.
• Establishing situations where human and environment co-existence is
supportive of each other through design
• Preserving human health by providing positive environmental
influence
The complexity of the PE interrelationship with health lies in the fact that a
response to mental wellbeing due to environmental influences may or may not
begin within the microenvironment. There may be a variety of factors that are
reasons for the trigger and generation of wellbeing or illness. These may be
subjective rather than objective and recognisable. As a result, identification of
minor triggers that develop into major issues may need to be identified in the first
instance.
Essentially, the numbers of possible forms of influences and/or relationships
between PE inter/transactions are quite large as identified in the review. However,
by following the method identified through this research and summarised (Table
12) one could potentially gain significant insights into the most relevant
influences. These may then be able to be defined so that they can be addressed as
152
part of dealing with the complexity of the field and situation. The understandings
can subsequently be applied to specific areas of design practice and inquiry in PE
interrelationships.
5.3.1. Application of current and future research and technology for
practitioners
Along with current technology, practitioners would benefit by applying possible
research findings to the design process. Practitioners dealing with design and
other areas of BE need to be aware of the dynamic process of research. While, in
practice, it is pertinent to use and apply the latest technology, it is not always as
popular for practitioners to browse through databases for current research
understandings that could be applied to practice. This could be because of the time
required since the sources are scattered across domains, thus making
complicating. As demonstrated in this review, many studies are indirectly
connected and are located in diverse domains such as design, architecture,
healthcare, environmental psychology, environmental health and related
medical/health fields.
Nevertheless, it may prove worthwhile to keep abreast of the current
understandings – especially in health and wellbeing – as many of the studies
indicate a definite link between health and well-being in relation to various
situations and environments. Constant review during designing (creation) and
constructing (production) processes is desirable. As Franz (1997) points out, it is
the designer’s responsibility to develop: “…a greater awareness of the potential of
design to extend understanding and prepare people for intrinsically meaningful
interaction...in addition to being a friend and collaborator, the designer is a
facilitator, mediator, and articulator, proposing and creating the conditions
understood to encourage and support meaningful interaction between the client
and the environment” (p.163). Only if the designer is aware of the benefits that
the environments can provide for a better life, will there be created supportive and
positively responsive environments.

153
In summary design should:
• Support appropriate inter/transactions in the sensual, emotional,
psychological and physiological sense to benefit, that is, improve the
quality of PE interrelationships
• Be able to facilitate the synchronicity of human psychological and
physiological capacities
• Provide the potential to sustain positive and avoid negative outcomes
• Consider the psychological and physiological outcomes of design on
users and their usage impacts.
“The designer needs to care deeply for a design’s uses even when those users are
anonymous and for a design’s effects” (Abercrombie, 1990, p.165).
5.3.2 Application of current and future research and technology for
education
Educational institutions should also keep in mind the transdisciplinarity of all
areas of application and give further importance to research and education in such
areas by collaborating across a number of disciplinary faculties. Design students
could therefore be provided in the very least with basic knowledge about the user
health model so that creativity embraces the application of the knowledge of the
human dimension to their work. Other than a handful of programs such as
environmental health, public health, and environmental psychology (which
concentrates on the health aspects related to the physical environment),
architecture and design disciplines do not necessarily look at these integrative
elements of applied design for human health. In the future, these directions will
have to be acknowledged. As proposed in this thesis, they should be a necessary
part of the operational framework becoming a part of the designer’s tacit and
taken for granted mode of practice. Central to this is the need for students to be
aware of the possibilities and the benefit of applying such knowledge because, in
the end, design is about supporting human interaction as well as it can.

154
5.3.3 Application of current and future research and technology for
research
Further recommendations for research related to physical environment, health and
wellbeing include two main aspects; firstly, there is a need for further research on
methodology for undertaking transdisciplinary and multidisciplinary research,
especially when looking at inter-relationships (as seen in this thesis). Secondly,
future research directions and recommendations include:
• Inquiry into specific physical environmental and design elements that
contribute to establishing a favourable environment to support a
positive psychophysiological relationship of the human body
• Exploring the extent to which designers can produce a positive
environment where distress and the potential for illness and disease
are minimised
• More extensive research concerning the role of the interior
environment in contributing to illness and disease
• Establishing a more detailed understanding of the various ways in
which people interact with the environment and vice versa in the
context of health and well-being
• Further exploring the benefit of applied linkages between PNI and the
physical environment in practice
• Development of ways in which the physical environment can be
evaluated for emotional capacities (along with other environmental
capacity measurements such as air quality) which may become a part
of government public policies
• More research into illnesses caused by environmental impact on
emotional wellbeing and consequences for the neuroendocrine and
immune systems
• Research synthesis of other specific areas of health and the human
body providing more insight into environmentally generated illnesses
155
supplemented with more detailed studies in the specific system areas to
produce a more in-depth understandingof PE relationships
• Undertaking case studies on pre occupancy and post occupancy levels
of psychological outcomes correlating with physiological outcomes;
• Additional case studies to investigate specific environmental situations
including pre-environmental influences on a person’s integrative or
PNI systems within a particular environment type.
Lastly, from the review of existing research, it has been highlighted that there are
many areas that have been studied producing findings that indicate human
relationships within the physical environment contribute to psychological and
physiological outcomes. This substantiates the need for a model for designers to
work with in creating not only an aesthetically pleasing but also health responsive
environmental settings. A framework of specific PE interrelationships for
application – on case by case basis – could be created and adapted depending on
the design requirements and outcome anticipated. The criteria could be modified
and matched as per the environmental elements recommendations. For instance, if
we take into consideration a space, the sensory, emotional, and physiological
capabilities can be checked against each spatial element such as visual (for
example, lighting and color), acoustics, tactile, perceptive/ cognitive, user
comfort, social interactive levels and so on (refer to Figure 16). The stages
mentioned in the model are interrelated to the environmental psychological and
physiological formulas corresponding to stimuli and arousal factors. These stimuli
can be from animate or inanimate factors present which impact on psychological
or physiological arousal. Such criteria assessment would help to potentially
identify and evaluate a positive or negative health strategy for design process and
application.

156
5.4 In conclusion
This review of existing literature in select areas of BE and health indicates that
many elements in the physical surroundings affect the person either favorably or
adversely in regard to health and wellbeing when understood in terms of the
integrative systems or the PNI system. Further research is necessary to find out
the specific influential elements that may be present in the physical environment
that impact on the outcomes of PE inter/transactions. Application of the current
findings will help in developing a future health responsive design approach for
application in practice and research.
Design factors in a space may be classified and categorised into specific user
interactions that correlate with the stages described in the ‘integrative health
systems flow model’ (Figure 16). The factors singularly or collectively may or
may not contribute to the responses and reactions stated. Once they have been
coordinated, design may contribute in eliciting positive wellbeing in users.
Finally, as George Nelson states “The humane environment is not a slogan; it is a
mystery which can only be penetrated by humane people” (quoted in
Abercrombie, 1990, p.165).

157
References Abercrombie, S. 1990. A Philosophy of Interior Design. New York: Harper &
Row.
Ader, R., & Cohen, N. 1975. Behaviourally conditioned immunosuppression. Psychomatic Medicine, 37 (4): pp. 3-340.
Ader, R.; Felten, D.L.; & Cohen, N. 1991. Psychoneuroimmunology 2nd Ed.
Academic Press, San Diego.
Adkins, B; Smith, D. J; Barnett, K & Grant, E. 2005. Public Space as ‘Context’ in Assistive Information and Communication Technologies for People with Cognitive Impairment. Information, Communication and Society, 9(3):pp. 355-372.
Altman , I., Rogoff, B.1987. World views in psychology: Trait, interactional,
orgasmic, and transactional perspectives. In Handbook of environmental psychology. Daniel Stokols and Irwin Altman (Eds). New York: Wiley.
Anthony, K. H. & Watkins, N.J. 2002. Exploring Pathology: Relationships
between Clinical and Environmental Psychology. In Handbook of Environmental Psychology, Robert B. Betchel and Arza Churchman (Eds). New York: Wiley
Anthony, K.H. 1998. Designing psychotherapists’ offices: Reflections of an environment-behaviour researcher. Conference Proceedings, American Psychological Association Convention, San Francisco.
Anthony, K.H. 1984. The role of the family in family conflict. In The challenge of
diversity: Proceedings of the 15th annual EDRA conference. Donna Duerk and David Campbell (Eds). Washington, DC: EDRA.
Arneill, B & Frasca-Beaulieu, K. 2003. Putting patients first: Designing and
practicing Patient- centered care. Susan .B. Frampton, Laura Gilpin and Patrick.A.Charmel (Eds). San Francisco: Jossey-Bass.
ASHA Poll, 2006. American Speech-Language-Hearing Association Survey
exposes Troublesome Hearing Loss Trends. URL: http://www.hearinglossweb.com/Medical/Causes/nihl/asha.htm. Accessed 16/04/2006
Arnetz, B.B. 1998. Environmental Illness: Multiple Chemical Sensitivity, Sick Building Syndrome, Electric and Magnetic Field Disease. In The Environment and Mental Health: A Guide for Clinicians. Ante Lundberg (Ed). Lawrence Erlbaum Associates, Inc., Publishers, London.

158
Aspinwall, L.G. & Staudinger, U.M. (Eds). 2003. A Psychology of human strengths: fundamental questions and future directions for a positive psychology. Published by American Psychological Association.
Washington, DC; London Australian population growth. URL:
http://www.abs.gov.au/ausstats/[email protected]/e8ae5488b598839cca25682000131612/0cd69ef8568dec8eca2568a900139392!OpenDocument . Accessed 18/01/2006.
Balanli, A; Ozturk, A; Karabiber, Z; Unver, R; Gedik, G; Yavuz, G; Vural, V.
2005. An examination and evaluation of YTU library and documentation building in terms of building biology. Building and Environment. 41(8): pp. 1079-1098.
Bardana, E.J. 2001. Indoor pollution and its impact on respiratory health. Ann Allergy Asthma Immunology. 87(3): pp.33-40.
Baron, J.H. & Greene, L.1984. Art in hospitals. British Medical Journal. 289:
pp.1731-1737. Baron, R. A. 2001. Psychology (5th Ed). Boston: Allyn and Bacon. Bauer-Wu, S. M. 2002. Psychoneuroimmunology Part II: Mind-Body
Interventions. Clinical Journal of Oncology Nursing. July/Aug 6(4).
Baum, A & Singer, J. E, 1982. Advances in Environmental Psychology (Vol.4) In Environment and Health. Andrew Baum & Jerome. E. Singer (Eds.). Lawrence Erlbaum Associates, Inc.
Bearg, D.W. 1993. Indoor Air Quality and HVAC Systems. Boca Raton, Fla :
Lewis Publishers.
Beck, S.L.1999. The therapeutic use of music for cancer- related pain. Oncology Nursing Forum. 18:1327-1337.
Becker, F. & Steele, F. 1995. Workplace by Design: mapping the high-
performance workscape. San Francisco: Jossey-Bass.
Bell, P.A.; Greene, T.C.; Fisher, J.D.; & Baum, A (Eds). 2001. Theories of Environment-Behaviour Relationships (5th ed.). pp. 98-135. Harcourt College Publishers.
Bennet, C. 1977. Spaces for people: Human factors in design. Englewood Cliffs, NJ: Prentice-Hall.
Betchel, R. B & Korpela, K. M. 1995. Most Happy and Most Depressing Places :
A Finnish- U.S. Comparison. In Handbook of Environmental Psychology, Jack L. Nasar; Peg Grannis & Kazunori Hanyu (Eds).

159
Bilchik, G.S. 2002. A better place to heal. Health forum journal. 45(4): pp.10-15. Biner, P. M; Butler D. L.; Lovegrove, T. E; & Burns, R.L, 1993. Windowlessness
in the workplace : A reexamination of the compensation hypothesis. Journal of Environment and Behavior. 25(2), 205.
Bronfenbrenner, U. 1979. The ecology of human development. Cambridge, MA: Harvard University Press.
Bronzaft, A.L, 2002. Noise Pollution: A hazard to Physical and Mental Well- being. In Hand book of Environmental Psychology, Robert B.Bechtel and Arza Churchman (Eds)
Brown, V.A. 1996. Double or Nothing. The Essential Connection between Human and Environmental Health. Health, Wellbeing and survival into the twenty-First Century. Nature and Society Forum. June 1996.
Bonnes, M & Secchiaroli, G, 1995. Environmental Psychology: A psycho-social introduction. Sage publications.
Bonnes, M & Bonaiuto, M. 2002. Environmental Psychology: From spatial-
physical environment to sustainable development. p. 28. In Hand book of Environmental Psychology, Robert B.Bechtel and Arza Churchman (Eds). New York: Wiley.
Breslow, L. 2000. The societal context of diseases prevention and wellness promotion. In Promoting human wellness – New frontiers for research, practice and policy. Daniel Stokols (ed.). University of California Press.
Buckle, J. 1999. Use of aromatherapy as a complementary treatment for chronic
pain. Alternative Therapies in health and medicine. 5(5): 42-51.
Butler, R.N & Jasmin, C, 2000. Longevity and quality of life: Opportunities and challenges. Proceedings of the Congress Worldwide Revolution in Longevity and Quality of life. Robert N. Butler and Claude Jasmin (Eds). Kluwer Academic/ Plenum Publishers, New York.
Canter, D. 1982. Psychology and environmental design. In Psychology in practice, S.Canter and D.Canter (Eds). London: Wiley.
Canter, D. 1997. The Facets of Place. p.109. Advances in Environment, Behavior, and Design. Towards the integration of theory, Methods, Research, and Utilization. Volume 4, Moore, G.T & Marans, R.W (Eds). Kluwer Academic/ Plenum Publishers, New York.
Carr, R. F. 2003. Health Care Facilities. URL: http://www.wbdg.org/design/health_care.php Accessed: 28/02/2005
160
Centre for Health Design, 2005. http://www.healthdesign.org/ Accessed: 17/01/2006
Ching, F. 1996. Architecture: Form, space and order. New York: Van Nostrand Reinhold.
Clitheroe, C.; Stokols, D & Zmuidzinas, M. 1998. Conceptualizing the context of
environment and behaviour. Journal of Environmental Psychology. 18: pp. 103-112.
Coalition for Health Environments Research (CHER) (2003). Color in Healthcare
Environments: A Monograph Reference Guide. Cohen, B. J. 2004. Medical Terminology: and illustrated guide. Barbara Janson
Cohen (4th Ed.). Lippincott Williams & Wilkins. Cohen, S., Evans, G., Stokols, D., & Krantz,D.1991. Behavior, Health and
Environmental Stress. New York : Plenum Press. Colarelli, C.J. & Seigel, S.1966. An adventure in innovation. Princeton, NJ Cousins, N. 1983. The healing heart. New York: Avon books. Coon, D. 1991. Essentials of Psychology (5th Ed.) Cooper, H.M. 1989. Integrating research: A guide for literature reviews (2nd Ed.)
Sage Publications: Newbury Park, CA. Cooper, H.M., & Hedges, L.V. 1994. The handbook of research synthesis.
Sage Publications: New York. Cooper, H. M. 1998. Synthesizing Research: A guide to literature reviews (3rd
Ed). Thousand Oaks, CA: Sage Publications.
Cox, H., Burns, I., Savage, S. 2004. Multisensory Environments for leisure: Promoting well-being in nursery home residents with dementia. Journal of Gerontological Nursing, 30(2), 37-45.
Danford, G.S, 2004. The performance prediction model. In Design with spirit.
Proceedings of the 35th Annual Conference of the Environmental Design Research Association. Dwight Miller & James A. Wise (Eds.). Albuquerque, New Mexico, June 2-6. Edmond, Okla: Environmental Design Research Association Publication.
Daruna, J. H, 2004. Introduction to Psychoneuroimmunology. Elsevier Academic
Press.

161
Davidson, R, J., Scherer, K.R., Goldsmith, H.H. 2003. Introduction. In Hand book of Affective Sciences. Richard. J. Davidson.; Klaus R. Scherer.; & H.Hill Goldsmith (Eds). Oxford University Press.
Dennehy, C. 2003. Ecopsychology: The unconscious Archetypes and the environment. In Ecopsychology: A group project for psychoneuroimmunology. By Casey Dennehy, Michael Brown, Dan Siekkinen.URL: http://academic.evergreen.edu/curricular/pni/ecopsychology.htm Accessed: 11/08/2004.
Dorn, L. 1994. Stress, Health and the Office Environment. In Human Stress and
the environment. Environmental topics (vol 5).Philadelphia: Gordon and Breach Science Publishers.
Douglas, C. H. & Douglas, M.R. 2005. Patient-centred improvements in health-care built environments: perspectives and design indicators. Health Expectations: An International Journal of Public Participation in Health Care and Health Policy. Sep 8(3), Pp. 264-276.
Eberhard, J, 2004. Neuroscience and Architecture: The new frontier. In Design with spirit. Proceedings of the 35th Annual Conference of the Environmental Design Research Association. Dwight Miller & James A. Wise (Eds.). Albuquerque, New Mexico, June 2-6. Edmond, Okla: Environmental Design Research Association Publication.
Eberhard, J. P. 2003. Science studies how architecture affects the brain: Architects, neuroscientists get together for research. URL: http://www.djc.com/news/ae/11151117.html Accessed: 12/03/2005
Environment Health Council of Australia. enHealth Council. URL:http://enhealth.nphp.gov.au/council/pubs/ecpub.htm Accessed: 23/07/2005
Evans, G.W & McCoy, J. M. 1998. When Buildings Don’t Work: The Role of Architecture in Human Health. Journal of Environmental Psychology. 18: pp. 85- 94.
Evans, P.; Hucklebridge, F.; & Chow, A. 2000. Mind Immunity and Health: The science of Psychoneuroimmunology. Free Association Books: London/ New York.
Eyles J. 1985. Senses of Place. Silverbrook Press: Warrington, England. Fink, A, 2005. Conducting Research literature reviews: From internet to paper
(2nd Ed).Thousand Oaks, California: Sage Publications
162
Forrest, C. 1999. Using design psychology to foster psychological growth and change: A case study in the design of a psychotherapist’s office. In The power of imagination: Proceedings of the 30th annual Conference of the Environmental Design Research Association: Orlando, Florida, June 2-6, (pp.278). Thorbjoern Mann (Ed.). Edmond, Okla: The Association Publication.
Francis, C & Cooper, 1991. Places People Take their Problems. In Healthy environments: Proceedings of the 22nd annual conference of the Environmental Design Research Association, Oaxtepec, Morelos, Mexico, March 12-15. Javier Urbina-Soria, Patricia Ortega-Andeane & Robert Bechtel (Eds). Oklahoma City : EDRA Publication.
Franz, J.M, 1997. A Phenomenographic Study of Design in the Interior Design
Context. PhD. Dissertation. Queensland University of Technology.
Frumkin, H, 2005. Nature Contact: A Health Benefit. In Environmental Health: From Global to Local. Howard Frumkin (Eds.). John Wiley & sons, Inc.
Frumkin, H, 2005b. Health, Equity, and the Built Environment. Environmental Health Perspectives. May , Vol.113 Issue 5, pp A290-291.
Frumkin, H, (Eds) 2005. Environmental Health: From Global to Local. Howard Frumkin (Eds.). John Wiley & sons, Inc.
Galea, S., Ahern, J., Rudenstine, S., Wallace, Z., Vlahov, D. 2005. Urban built
environment and depression: a multilevel analysis. Journal of Epidemiology and Community Health. Oct 59(10), Pp. 822-827.
Galea, S, & Vlahov, D, 2006. Urbanization.In Environmental Health: from Global
to Local. Howard Frumkin (Ed). John Wiley & Sons.
Gearon, C. J. 2002. Hospitals and health networks. Chicago: Health and medical Journal. 76(10).
Geoff, D, 1995. Human Interest. The Journal for Healthcare Design & Development. 26(8): p.35. Academic Search Elite.
Gifford, R. 1988. Light, décor arousal, comfort, and communication. Journal of Environmental Psychology. 8: pp.177-189.
Gifford, R. 1996. Environmental Perception and Cognition. In Environmental
psychology: principles and practices. Robert Gifford (2nd Ed). Boston: Allyn & Bacon,
Graumann, C. F. 2002. The Phenomenological Approach to People-Environment Studies. In Hand book of Environmental Psychology. Robert B. Bechtel and Arza Churchman (Eds). New York: Wiley.
Gross, R.; Sasson, Y.; Zarhy, M.; & Zohar, J. 1998. Healing Environment in

163
psychiatric hospital design. General Hospital Psychiatry. 20: 108-114. Guyton, A. C, 2000. Textbook of medical physiology. Arthur C.Guyton &
John.E.Hall (10th Ed). W.B.Saunders Company. Hafen, B.Q.; Karren, K.J; Frandsen,K.J; & Lee, S.N, 1996. Mind –Body Health.
The effect of attitudes, emotions and relationships. Allyn and Bacon Massachusetts.
Hart, C. 1998. Doing a literature review: releasing the social science research imagination. London: Sage Publications.
Heerwagen, J. 1990. The psychological aspects of windows and window design.
In Coming of age: Proceedings of the twenty – first annual Conference of the Environmental Design Research Association, Champaign-Urbana, Illinois, April 6-9. pp.269-280. Robert I. Selby et al. (Eds). Edmond, Oklahoma City: EDRA Publication.
Hemphill, M. 1996. A note on adults’ color-emotions associations. Journal of Genetic Psychology. 157: pp. 275-278.
Hendren, R., Blanski, B. 2004. Facility designed showcase. Journal of Behavioral management. 24(1): p.56. Academic research library database, Proquest.
Henry, J.P and Grim, C.E. 1990. “Psychosocial mechanisms of primary
hypertension”. J. Hyperten. (8): pp. 783-793
Hodgson, M. J, 2006. Indoor Air. In Environmental Health: from Global to Local. Howard Frumkin (Ed). John Wiley & Sons.
Hodgson M. 2002. Indoor environmental exposures and symptoms. Environ Health Perspective.110 (4): pp. 663-667.
IAP, Indoor Air Pollution: An Introduction for Health Professionals. 1994.
Washington, DC: US Environmental Protection Agency. EPA publication. Ittelson, W.H., Proshansky, H.H., Rivlin, L.G & Winkel,G. 1974. An introduction
to environmental psychology . New York: Holt, Rinehart and Winston. Ittleson, W.H. 1976. In Environmental Psychology: People and their settings, 2nd
Edition. Proshansky, H.M., Ittleson, W. H., Rivlin, L.G. (Eds). Ittleson, W.H. 1976. Environmental perception and contemporary perceptual
theory. In Environmental Psychology: People and their settings (2nd ed). Proshansky, H.M., Ittleson, W. H., Rivlin, L.G. (Eds)
164
Jamison, C.S., Wallace, M., Jamison, P.L. 2004. Contemporary Work Characteristics, Stress and Ill Health. American Journal of Human Biology. 16: pp. 43-56.
Jasmin, C. 2000. A Malthusian Revolution. In Longevity and quality of life: Opportunities and challenges. Proceedings of the Congress Worldwide Revolution in Longevity and Quality of life. Robert N. Butler and Claude Jasmin (Eds). Kluwer Academic/ Plenum Publishers, New York.
Jones, B. F.1996. Environments that Support Healing. ISDesigNET Jul/Aug issue. Kaplan, S. 1983. A model of person-environment compatibility. Environment and
Behavior. (15): pp. 311-322.
Kaplan, S. 1987. Aesthetics, affect and cognition: Environmental preference from an evolutionary perspective. Environment and Behavior, 19, 3-32.
Kaplan, S., Talbot, J., Kalan, R. 1988. Coping with daily hassles: The impact of
nearby nature on the work environment. Proj.Rep. U.S.Forest Service , North Central Forest Experiment Station, Urban Forestry Unit Cooperative Agreement 23-85-08. Washington DC: US .Govt. Printing Office
Kaplan, R., & Kaplan, S. 1989. The Experience of Nature: A Psychological Perspective. Cambridge University Press: New York.
Kaplan, S. 1995. The restorative benefits of nature. Towards an integrative framework. Journal of environmental psychology. (15): pp. 169-185.
Kiecolt-Glaser, J. K.; Page,G.G.; Marucha, P.T., MacCallum, R.C., Glaser, R. 1998. Psychological influences on surgical recovery: perspectives from psychoneuroimmunology. American Psychologist .Nov. 53(11), Pp. 1209-1218.
Kiecolt-Glaser, J.K.; McGuire, L.; Robles, T.F.; & Glaser, R. 2002. Psychoneuroimmunology and Psychosomatic Medicine: Back to the Future. Psychosomatic Medicine. 64: pp.15-28.
Knowles, J.H. 1997. Doing better and feeling worse: Health in the United States. New York, Norton
Korpela, K, 1991. Are Favorite Places Restorative Environments? In Healthy environments. Proceedings of the twenty-second annual conference of the Environmental Design Research Association, Oaxtepec, Morelos, Mexico, March 12-15. Javier Urbina-Soria; Patricia Ortega-Andeane; & Robert Bechtel (Eds).
165
Korpela, K. M. & Ylen, M. 2005. Perceived health is associated with visiting natural favourite places in the vicinity. Health & Place. pp. 1-14 (In Press).
Kwallek, N., Lewis, C.M. 1990. Effects of environmental colours on males and females: A red or white or green office. Applied Ergonomics. 21: pp. 275-278.
Lawrence, R. J. 2002. Healthy residential environments. In Hand Book of Environmental Psychology. Robert .B. Bechtel and Arza Churchman (Eds.). New York: Wiley.
Lawton, M.P. 1975. Competence, environmental press, and the adaptation of older people. In Theory development in environment and aging. P. G. Windley & G. Ernest (Eds.). Washington, DC: Gerontological Society.
Lawton, M.P. 1989. Social structure and aging: Psychological processes. LEA Publishers, Hillsdale, NJ.
Lawton, M.P., Moss, M., Hoffman, C., Kleban, M.H., Ruckdeschel, K., & Winter. L. 2001. Valuation of life: a concept and a scale. Journal of Aging and Health. 13(1): pp. 3-31.
Levi, L. 1987. Definitition and the conceptual aspects of health in relation to work: Psychosocial factors at work and their relation to health. In R. Kalimo, M.A. El-Batawi and C.L. Cooper. (Eds). Geneva, WHO.
Lippard LR.1997. The Lure of the Local: Senses of Place in a Multicentered Society. New York, NY: New Press.
Lipowski, Z.J. 1986. What does the word ‘psychosomatic’ really mean? A historical and semantic inquiry. In The psychosomatic approach: contemporary practise and wholeperson care. M.J.Christie & P.G.Mellet (Eds). New York: John Wiley and Sons.
Lundberg, A. 1998. Environmental change and human health. In The environment and mental health: a guide for clinicians. Ante Lundberg (Ed.). Lawrence Erlbaum Associates, Inc., Publishers, London.
Lundberg, A. 1998b. The Environment and Mental Health: A Guide for Clinicians. Ante Lundberg (Ed). Lawrence Erlbaum Associates, Inc., Publishers, London.
Mair, S.F.; Watkins, L.R.; & Fleshner, M.1994. Psychoneuroimmunology: The Interface between behavior, brain and immunity. 49 (12): pp.1004-1071.
Malnar, J. M & Vodvarka, F. 1992. The Interior Dimension: A Theoretical Approach to Enclosed Space. Van Nostrand Reinhold , New York.
166
Martin, G. 1996. Olfactory remediation: Current evidence and possible applications. Social Science and Medicine. 43: pp. 247-254.
Matter-Walstra, K.1999. Body and Mind. URL: http://www.cranial.co.nz/pni_definition.html Accessed: 12/08/2004
Mazumdar, Sanjoy, 1992. Sir please do not take away my cubicle: The phenomenon of environmental deprivation. Environment and Behavior. 24(6): 691-722.
Mazumdar, Sanjoy, 1999. Environmental Design Research. In The power of imagination: Proceedings of the 30th annual Conference of the Environmental Design Research Association: Orlando, Florida, June 2-6, Thorbjoern Mann (Ed.). Edmond, Okla: The Association Publication.
McCarthy, M. 2004. Healthy Design. The Lancet. London: 7(364): pp. 405-407. Proquest.
McMichael, A.J. 2001. Human Frontiers, Environments and Disease: Past Patterns Uncertain Futures. Cambridge University Press, Cambridge.
McCoy, J. M. 2002. Work Environments.p.447. Hand Book of Environmental Psychology. Robert B.Bechtel & Arza Churchman (Eds.). New York: Wiley
McCoy, J.M., and Evans, G.W. 1998. When buildings don’t work: the role of architecture in human health. Journal of Environmental Psychology. 18: 85-94.
Medical Letter on the CDC & FDA. 2005. Public Health: Community planning impacts public health. Jun 19: p.140.
Miller, S and Schlitt, J.K. 1985. Interior Space: Design concepts and needs. Praeger Publishers.
Miles, M. B & Huberman, M. A. 1994. Qualitative Data Analysis and: an expanded source book (2nd Ed). Sage Publications, Inc.
Millicent, G. 1992. Design technology: psychoneuroimmunology. Journal of health care design. Proceedings from the Symposium on HealthcareDesign Symposium on Healthcare Design. 4: pp. 127-130.
Mikellides, B. 1988. Looking back to the future. Proceedings of the tenth bienal
conference of the International Association for the Study of People and their Physical Surroundings. Delft. The Netherlands, July 5-8. Herbert van Hoogdalem et al. (Eds). Delft University Press.

167
Moffet, H; Hagberg, M; Hansson- Risberg, E; Karlqvist, L, 2002. Influence of laptop computer design and working position on physical exposure variables. Journal of Clinical Biomechanics. (17): pp. 368-375.
Monro, J. 2000. Electromagnetic screening as a protection from telephone
frequencies and effects on heart rate variability. 18th Annual International Symposium on Man and His Environment. June 8-11. Dallas, Texas.
Moore, K. D.; Van Haitsma, K.; Curyo K.; & Sapestein, N. 2003. A pragmatic environmental psychology: A metatheoretical inquiry into the work of M.Powell Lawton. Journal of Environmental Psychology. 23(4):pp. 471-482.
Morrison, P. 1991. Critiquing research. Surgical Nurse 6(1): pp. 20-22. National Institute of Health, 2003. URL: http://www.nlm.nih.gov/tsd/acquisitions/cdm/subjects33.html Accessed 19/07/2005.
Neuner, N & Seidel, H, 2006. Adaptation of office workers to a new building –Impaired well-being as part of the sick-building-syndrome. International Journal of Hygiene and Environmental Health. (In Press)
Oldenburg, R.1989.The Great Good Place: Cafes, Coffee Shops, Community Centers, Beauty Parlors, General Stores, Bars, Hangouts and How They Get You Through the Day. New York, NY: Paragon House.
Oldenburg, R. 2000. Celebrating the Third Place: Inspiring Stones about the "Great Good Places" at the Heart of Our Communities. New York, NY: Marlowe & Co.
O’Neill, M.J. 1991. Effects of signage and floor plan configuration on way finding accuracy. Environment and Behavior. 23: pp. 553-574.
Parsons, R & Tassinary, L.G. 2002. Environmental Psychophysiology. In Handbook of Environmental Psychology. Robert Betchel and Arza Churchman (Eds). John Wiley & Sons, Inc., New York.
Parsons, R.; Tassinary, L.G.; Ulrich, R. S.; Hebel, M.R.; & Grossman-Alexander, M. 1998. The View From The Road: Implications for Stress Recovery and Immunization. Journal of Environmental Psychology. 18: pp. 113-139. Academic Press.
Pennebaker, J.W. & Brittingham, G.L. 1982. Environmental and sensory cues affecting the perception of physical symptoms. In Advances in environmental psychology, Volume 4. A. Baum and L. Singer (Eds.). Hillside, NJ: L. Erlbaum Associates.
168
Pressly & Heesacker, 2001. The physical environment and counseling: A review of theory and research. Journal of Counselling and Development: Jcd. 79(2): pp. 148-160.
Proshansky, H.M.; Fabian, A.K.; & Kaminoff, R. 1983. Place identity: Physical world socialization of the self. Journal of environmental psychology. 3, 57-83.
Prohansky, H.M.; Ittleson, W. H; & Rivlin, L.G. (Eds). 1976. Environmental Psychology: People and their settings. (2nd Ed.). New York: Holt, Rinehart and Winston.
Proshansky, H. M. 1976. Research Methods in Environmental Psychology. Environmental perception and contemporary perceptual theory. In Environmental Psychology: People and their settings (2nd Ed). Harold M. Proshansky; William H. Ittelson; & Leanne G. Rivlin (Eds)
Proshansky, H. and Fabian, A.1986. Psychological aspects of the quality of urban life. In The quality of Urban Life. D.Frick (Ed.). Berlin: Walter de Grutyter.
Recio, B, (2002). The power of Colour. American Spa, 6(3). ABI/INFORM Trade and Industry Database. Proquest.
Rapoport, A. 1990. The meaning of the built Environment: A nonverbal communication approach. The university of Arizona press.
Ray, O. 2004. How the Mind Hurts and the Heals the Body. American Psychologist. (59)1: pp. 29-40.
Richards, K.C., Gibson, R., & Overton –McCoy, A.L. 2000. Effects of massage in acute and critical care. AACN Clinical Issues. 11: pp. 77-96.
Riley, V., Fitzmaurice, M.A., & Spackman, D.H.1981.Psychoneuroimmunologic Factors in Neoplasia: Studies in Animals. In Psychoneuroimmunology. Robert Ader (Ed). New York : Academic Press.
Rosch, E, 2002. Principles of categorization. In Foundations of Cognitive Psychology: core readings. Daniel .J. Levitin (Eds). A Bradford book, The MIT Press, Cambridge.
Rosenman, R. H. 1994. Human Stress and the environment. Environmental topics, (vol.5). J. Rose (Eds). Philadelphia: Gordon and Breach Science Publishers
Rosenzweig, M. R.; Leiman, A. L.; Breedlove, S. M, 1999. Biological Psychology: An Introduction to Behvioral, Cognitive, and Clinical Neuroscience(2nd ed.). Sinauer Associates, Inc.

169
Russell, J.A., & Pratt, G. 1980. A description of the affective quality attributed to environments. Journal of personality and Social Psychology. 38 (3): pp. 11-22
Russell, J.A. & Snodgrass, J, 1987. Emotion and the environment. In Handbook of Environmental psychology. Daniel Stokols & Irwin Altman (Eds). New York: Wiley.
Schedlowski, M & Tewes, U ( Eds). 1996. Psychoneuroimmunology: An Interdisciplinary Introduction. Kluwer Academic. Plenum Publishers.
Segerstrom, S.C. and Miller, G.E. 2004. Psychological stress and the human immune system: A Metaanalytic study of 30 years of inquiry. Psychological Bulletin. (130) 4: pp. 601-630.
Seidel, J & Kelle, U, 1995.Computer-Aided Qualitative Data Analysis: Theory, Methods and Practice. Udo Kelle (Eds). London: SAGE.
Sheehan, D.V. and Soto, S. 1987. Diagnosis and treatment of pathological anxiety. Stress Med.3: pp. 21-32.
Siekkienen, D. 2003. Ecopsychological effects upon residents of the Puget Sound Region. In Ecopsychology: A group project for psychoneuroimmunology by Casey Dennehy, Michael Brown, Dan Siekkinen. URL: http://academic.evergreen.edu/curricular/pni/ecopsychology.htm.) Accessed: 11/08/2004.
Smith, A .P. 1998. The power of thought to heal: An ontology of personal faith. Claremont Graduate University.
Smith, D. J, 2000. Architectural Experience: A composition of Viewpoints. PhD. Dissertation. Queensland University of Technology.
Smith, D. J & Adkins, B, 2005. Making Place: Issues Involved When Designing For The Cognitively Impaired (Unpublished).
Smith, D. J & Adkins, B, 2005. The Environmental Experience of Shopping With the Cognitive Impairment (Unpublished).
Solomon, G .F and Moos, R., 1964. Emotions, immunity and diseases: A speculative theoretical integration. Archives of General Psychiatry.11 (6): pp. 657-674.
Solomon, G. F., (1996). Physiological responses to environmental design: Understanding psychoneuroimmunology (PNI) and its application for healthcare. Journal Of Healthcare Design. (8): p.83. Symposium on Healthcare Design
Sommer, R, & Oslen, H. H. 1980. The soft classroom. Environment and Behavior. (12): 3-16.
170
Spangenberg, E. R., Grohmann, B., and Sprott, D. E. 2005. It's beginning to smell (and sound) a lot like Christmas: the interactive effects of ambient scent and music in a retail setting. Journal of Business Research. 58(11), 1583-1589.
Srinivasan, S., O’Fallon, L., & Dearry, A, 2003. Creating Healthy Communities, Healthy Homes, Healthy People : Initiating a Research Agenda on the Built Environment and Public Health. American Journal of Public Health. Washington: Sep, 93(9): pp. 1446- 1452.
Standley, J. 1986. Music Research in medical/dental treatment: Metaanalysis and clinical applications. Journal of Music Therapy. 23, 56-122.
Stokols, D., & Clitheroe, C. 2005. Environmental Psychology. In Environmental Health: Global to Local. Howard Frumkin (Ed). John Wiley & sons, Inc.
Stokols, D. 2003. The Ecology of Human Strengths. In A psychology of human strengths: fundamental questions and future directions for a positive psychology. Lisa G. Aspinwall and Ursula M. Staudinger (Eds.). Washington, DC, London: American Psychological Association.
Stokols, D., & Montero, M., 2002. Towards an Environmental Psychology of the Internet. In Hand book of Environmental Psychology. Robert B.Bechtel and Arza Churchman (Eds). New York: Wiley.
Stokols, D; McMahan, S; & Philip, K, 2001. Workplace health promotion in small businesses. In Health Promotion in the workplace (3rd Ed). M. O’Donnell (Ed). Albany, New York: Delmar Publishers, INC.
Stokols, D. 2000. Creating health promotive environments: implications for theory and research. Promoting Human Wellness: New Frontiers for Research, Practice, and Policy. Daniel Stokols and Margaret Schneider Jamner (Eds.). Berkeley, California, London : University of California Press.
Stokols, D, 1998. Environmental Design. Psychosocial and Organizational Factors. In Encyclopedia of Occupational Health and Safety. 4th Edition. Jeanne Mager Stellman (Eds). International Labour Office Geneva.
Stokols, D. 1992. Establishing and Maintaining Healthy Environments: Towards a Social Ecology of Health Promotion. American Psychologist. 47(1): pp. 6-22.
Stokols, D & Altman, I. 1987. Handbook of Environmental Psychology. New York: Wiley.
Stokols, D. 1978. Environmental Psychology. Annual Review of Psychology. (29): pp. 253-295.
171
Stokols, D, 1977. Perspectives of environment and behaviour. Plenum press: New York.
Suedfeld, P. 1987. Extreme and Unusual Environments . Handbook of environmental psychology. Daniel Stokols and Irwin Altman (Eds). New York: Wiley
Sutherland, V. J. and Cooper, C. L. 1994. Stress in the Work Environment. In Human Stress and the environment. Environmental topics- vol 5. J. Rose (Ed). Philadelphia: Gordon and Breach Science Publishers.
Taylor, S.T., Bogdan, R.1998. Introduction to qualitative research methods: A guidebook and resource( 3rd Ed.). John Wiley and sons, Inc.
Tiernan, C. 2002. Designing Workspaces for Higher Productivity. Journal of Occupational Health & Safety. 71(9): pp.192-195.
The Free Medical Dictionary by Farlex. URL:http://medical-dictionary.thefreedictionary.com/parous Accessed: 03/10/2005
Ulrich, R. S. 1981. Natural versus urban scenes: Some psychophysiological effects. Environment and Behavior. 13: pp. 523-556.
Ulrich, R. S. 1983. Aesthetic and Affective Response to Natural Environment. In Behavior and the natural environment. Irwin Altman & Joachim F. Wohlwill (eds),. New York: Plenum Press.
Ulrich, R.S. 1984. View through a window may influence recovery from surgery. Science. 224: pp. 420-421.
Ulrich, R.S., Simons, R.F., Losito, B.D., Fiorito, E., Miles, M.A., Zelson, M. 1991. Stress recovery during exposure to natural and urban environments. Journal of Environmental Psychology. 11: pp. 201-230.
Ulrich, R. S, 1992. Effects of interior design on wellness: theory and recent scientific research, Journal of Health Care Interior Design. pp. 97–109.
Urlich, R. S. 1992. How Design Impacts Wellness. The Healthcare Forum Journal. San Fransisco: Sep/Oct 35(5): pp. 20-26.
Urlich, R. S.; Zimring, C.; Quan, X.; Joseph,A.; & Choudhary, R. 2004. The role of the physical environment in the hospital of the 21st century. The Center for Health Design.URL: http://www.healthdesign.org/research/reports/pdfs/role_physical_env.pdf
UN Press release, (2005). URL: http://www.un.org/News/Press/docs/2005/pop918.doc.htm . Accessed 18/01/2006.
172
Valdez, P., and Mehrabian, A. 1994. Effects of colour on emotions. Journal of Experimental Psychology. 123: pp. 394-409.
Venolia, C. 1988. Healing environments. Berkeley, CA: Celestial Arts.
Walter EV. 1988. Placeways: A Theory of the Human Environment. Chapel Hill, NC: University of North Carolina Press.
Ward, G. 1995. Colors and employee stress reduction. Supervision. 56: 3-5.
Wargocki, P., Sundell, J., Bischof, W. 2002. Ventilation and health in non-industrial indoor environments: report from a European multidisciplinary scientific consensus meeting (EUROVEN). Indoor Air. 12: pp.113-128
Wapner, 1987. A holistic developmental, system-oriented environmental psychology: some beginnings. Handbook of environmental psychology. Daniel Stokols & Irwin Altman (Eds). New York : Wiley.
Wapner, S., Demick , J. 2000. Assumptions, methods and research problems of the holistic, developmental, system – oriented perspective. In Theoretical perspectives in environment-behavior research: Underlying assumptions, research problems, and methodologies. S.Wapner, J.Demick, T, Yamamoto, & H. Minami (Eds.). New York: Kluwer Academic/Plenum Press.
Weinberg, I. 2001. Quantum Determinism Versus Indeterminism: Resolving the Self-empowerment Paradox. URL: http://www.wellness.org.za/html/articles/a-versus.html Accessed: 22/03/2005.
Wheatly, D. 1994. Medical implications of stress. Human stress and the environment. In Environmental topics- vol 5. J.Rose (Ed). Philadelphia: Gordon and Breach Science Publishers.
White, E. T. 1986. Space Adjacency Analysis. Diagramming Information for Architectural Design. Architectural Media LTD. Tucson
World Health Organization, 2006. Indoor air pollution and health. URL: http://www.who.int/mediacentre/factsheets/fs292/en/index.html Accessed: 12/04/2006
World Health Organization, 2006. Information package on environmental and occupational health. URL: http://www.who.int/occupational_health/publications/occuphealthinfo/en/index.html Accessed: 12/04/2006
World Health Organization, 2003. Global Strategy on Diet, Physical Activities and Health. URL: http://www.who.int/dietphysicalactivity/media/en/gsfs_cancer.pdf Accessed: 02/07/2005

173
World Health Organization, 2001. Health impact assessment as part of strategic enviornmental assessment. C.H.Breeze and K.Lock (Eds). URL. http://www.euro.who.int/document/e74634.pdf
World Health Organization. WHO, 1984. Health promotion: A discussion document on the concept and principles. Health Promotion. 1: pp. 73-76
World Health Organization WHO: URL: http://www.who.int/phe/en/ Accessed: 12/04/2006
Wigram, T. 1995. The psychological and physiological effects of low frequency sound and music. Music Therapy Perspectives. 13: pp. 16-23.
Williams, S. M, 1994. Environment and mental health. John Wiley & Sons Ltd.: New York.
Wong, C.Y.; Sommer, R.; & Cook, R. 1992. The soft classroom 17 years later. Journal of environmental Psychology. 12: pp. 337- 343.
Wong, P.T.P., and Peacock, E. J. 1994. Environment, Stress and Aging. In Human Stress and the environment. Environmental topics- vol 5. Philadelphia : Gordon and Breach Science Publishers.
Zeisel, J, 2006.Inquiry by Design: Environment/Behavior/Neuroscience in Architecture, Interiors, Landscape and Planning. W.W.Norton & Company: New York.
Zeisel, J.1981. Inquiry by Design: tools for environment-behavior research. Brooks/ Cole Publishing Company.
Zeisel, J., Silverstein, N. M., Hyde, J., Levkoff, S. et al. 2003. Environmental correlates to behavioural health outcomes in Alzheimer’s special care units. The Gerontologists. 43 (5): pp. 695-711. Academic Research library database.
Zimbardo, P. G & Gerrig, R. J., 2002. Perception. In Foundations of cognitive psychology: core readings. Daniel .J. Levitin (Eds). The MIT Press, Cambridge.

0
Appendices
176

1
Appendix 1 List of Sources related to the numbers in Table 2 1. Anthony & Watkins, 2002 2. Anthony, 1998 3. Anthony, 1984 4. Aspinwall & Staudinger (EdS), 2003 5. Australian Bureau of Statistics, 2006 6. Bardana, 2001 7. Baron & Greene, 1984 8. N/A 9. Becker & Steele, 1995 10. Bell et al., 2001 11. Bennet, 1977 12. Bronfenbrenner, 1979 13. Brown, 1996 14. Arneill & Frasca-Beaulieu, 2003 15. Bonnes & Bonaiuto, 2002 16. Canter, 1982 17. Canter, 1997 18. Proshansky et al., 1983 19. Dennehy, 2003 20. Ching, 1996 21. Malnar & Vodvarka, 1992 22. Coon, 1991 23. Coon, 1991 24. Dorn, 1994 25. enHealth Council, 2005 26. Williams, 1998. 27. Altman & Rogoff, 1987 28. Forrest, 1999 29. Gifford, 1997 30. Graumann, 2002 31. Geoff, 1995 32. Gross et al., 1998 33. Heerwagen, 1990 34. Hemphill, 1996 35. Ittelson et al., 1974 36. Ittleson, 1976 37. N/A 38. N/A 39. N/A 40. Russel & Snodgrass, 1987 41. Henry &.Grim, 1990 42. N/A 43. Kaplan et al., 1988 44. Kaplan, 1983 45. Kaplan & Kaplan, 1990 46. Kaplan, 1995 47. Knowles, 1997 48. Kwallek & Lewis, 1990
49. Lawrence, 2002 50. Lawton, 1975 51. Breslow, 2000 52. Levi, 1987 53. Lundberg, 1998 54. Martin, 1996 55. McMichael, 2001 56. Miller & Schlitt, 1985 57. Mikellides, 1988 58. Monro, 2000 59. Moore et al., 2003 60. O’Neill, 1991 61. Rapoport, 1990 62. Parsons & Tassinary, 2002 63. Wong & Peacock, 1994 64. Proshansky, 1976 65. Proshansky & Fabian, 1986 66. Rosenman, 1994 67. Russell & Pratt, 1980 68. Sutherland & Cooper, 1994 69. Standley, 1986 70. Stokols, 1977 71. Stokols, 2000 72. Stokols, 1978 73. Stokols, & Altman, 1987 74. Stokols, & Montero, 2002 75. Sommer, & Oslen, 1980 76. Ulrich, 1984 77. Ulrich et al., 1991 78. UN Press release, 2005 79. Valdez & Mehrabian, 1994 80. Venolia, 1988 81. Ward, 1995 82. Wapner & Demick, 2000 83. WHO, 1984 84. WHO: URL: http://www.who.int/phe/en/ 85. Wigram, 1995 86. Wong et al., 1992 87. Zeisel, 1981 88. Zeisel et.al 2003 89. Suedfeld, 1987 90. Prohansky et.al., 1976 91. Lawrence, 2002 92. Cohen et al., 1991 95. Wong & Peacock, 1994 96. Russell & Pratt, 1980 97. Gifford, 1988

2
98. Indoor Air Pollution, 1994 99. Beck, 1999 100. Siekkienen, 2003 101. N/A 102. Buckle, 1999 103. Richards & Overton –McCoy, 2000 104. Bauer-Wu, 2002 105. Parsons & Tassinary, 2002 106. McCarthy, 2004 107. Urlich et al., 2004 108. Wheatly, 1994 109. Sheehan & Soto, 1987 110. Oldenburg, 1989 111. Oldenburg, 2000 112. Walter, 1988 113. Lippard, 1997 114. Eyles, 1985 115. Galea et al., 2005 116. Eberhard, 2003 117. Smith & Adkins, 2005 118. Smith & Adkins, 2005 119. Adkins et al., 2005 120. Jamison et al., 2004. 121. Hodgson, 2002. 122. Stokols & Clitheroe, 2005 123. Bearg, 1993 124. Wargocki et al., 2002 125. Russell & Snodgrass, 1987 126. Lawton, 1989 127. Arneill & Frasca-Beaulieu, 2003 128. N/A 129. Ulrich et al., 1991 130. N/A 131. Tiernan, 2002 132. N/A 133. Frumkin, 2005 134. Baron, 2001 135. N/A 136. CHER, 2003 137. Spangenberg et al., 2005 138. Segerstrom & Miller, 2004 139. Lawton, 2001
140. Gifford, 2002 141. Carr, 2003 142. Cox et al., 2004 143. Bilchik, 2002 144. Douglas & Douglas, 2005 145. Srinivasan et al., 2003 146. Frumkin, 2003 147. N/A 148. N/A 149. N/A 150. Frumkin, 2005b 151. Medical Letter on the CDC & FDA, 2005 152. N/A 153. N/A 154. Evans & McCoy, 1998 155. McCoy, 2002 156. Korpela & Ylen, 2005 157. Bell et al., 2001b 158. Bell et al., 2001c 159. Mazumdar, 1992 160. Mazumdar, 1999 161. Stokols et al., 2001 162. Korpela, 1991 163. Francis & Cooper, 1991 164. Dabford, 2004 165. Parsons et al., 1998 166. Ulrich R.S. 1992 167. Lundberg, 1998b 168. Balani et al., 2005 169. Moffet et al., 2002 170. Zeisel, 2006 171. Neuner, N, 2006 172. Evan & McCoy, 1998 173. Baum & Singer, 1982 174. Bronzaft, 2002 175. Recio, 2002 176. Pressly &Heesacker, 2001 177. Biner et al., 1993 178. Betchel & Korpela, 1995

Appendix 2 Paper submitted for Smart Systems 2005, Postgraduate Research Conference. 15
December 2005.
Suresh, M; Franz, J; & Smith, D, 2005. Holistic Health and Interior Environment:
Using the Psychoneuroimmunogical Model to Map Person-Environment Research
in Design. In Smart Systems 2005 Conference Proceedings. R. Goh & N.R. Ward
(Eds.). Queensland University of Technology.

1
Mini Suresh1, Jill Franz2, Dianne Smith3
Holistic Health and Interior Environment: Using the Psychoneuroimmunogical
Model to Map Person-Environment Research in Design.
Abstract: This paper focuses on the relationship between the holistic health of a human being and the interior environment as it is conveyed in research literature. The study described here particularly focuses on literature that connects environment, emotions, feelings, mind and body. Central to this work is the PNI (psychoneuroimmunology) model which proposes that a person’s psychological health is internally related to their neurological system and immunological systems. The study is underpinned by an interest in the relationship between these systems and the built environment. Its purpose is to establish the extent to which the built environment has been considered by research today in PNI and vice versa. This is achieved by further exploring the two subjects and looking at the possibilities of establishing a relationship between the two fields in order identify how PNI could contribute to Design. This is understood by examining the field of PNI and person-environment research in design. As an outcome, the project aims to produce a framework for further research and application. Keywords: Interior environment, Built environment, Holistic health, Psychoneuroimmunology, Design, Influence, Mental wellbeing Introduction: The purpose of this paper is to provide insights into the relationship between interior environments and holistic health. Over the past years there has been an increasing amount of research showing the possible influence of the environment in reducing stress [1-5].This is far more evident in healthcare environment investigations. However the potential of the environment in contributing to the mental wellbeing of a person and how this could affect the physical health needs further investigation. Towards this end, the study explores the field of Psychoneuroimmunology (PNI), further examining it to find a relationship with person-environment research in design and environment. Forming a relationship between PNI and the environment and designing with regard to PNI principles will help professionals to create an environment that will enhance health and wellbeing. For this there needs to be a basic understanding of PNI and its workings. There also needs to be an understanding of research undertaken in the design fields in relation to the built environment.
1 Student (Masters’ By Research), Mini Suresh, School of Design, Queensland University of Technology 2 Associate Professor, Dr. Jill Franz, School of Design, Queensland University of technology 3 Senior Lecturer, Dr.Dianne Smith, School of Design, Queensland University of Technology

2
Our physiological system and psychological system are not separate and distinct from our experiences in life. According to Rappoport (1990) the human body and the natural/ built environment are closely connected with each other by the simple fact that a person is always in one place or the other, be it in natural settings or human-made settings. The awareness of a particular place to a person depends on the reason the person is occupying the space [6]. For example, using a garden setting can be very different to a day in an office setting. This can further be subdivided into encounters that a person has with the place. The outlook of a jogger would differ from that of a person using the garden space for leisure. A casual visitor to an office will perceive the space differently from an employee using the space, whereas, an employer would have a different view from that of an employee. The human body reacts to a place consciously and subconsciously every time, all the time. The fact that people are psychologically dependent on their social and physical surroundings for their individual development and well-being is well-known [7]. Psychoneuroimmunology (PNI) PNI is the study of the interactions of the mind with the neuro and endocrine systems affecting the immunological systems of the body. An increasing number of studies have documented the connection between mind and the body (Fig.1) [For example, 8, 9, 10, &11]. The central nervous system, the neuroendocrine system and the immune system of the body are linked to the mind through the chemical connections involving our emotions (positive or negative) and the regulatory systems of the endocrine and immune systems through the central nervous system. Therefore, stressful emotions can produce an excess amount of epinephrine (Adrenaline) to be stored. This causes a chemical breakdown, resulting in the internal weakening of the immune system and an increased potential for disease [12].
Fig. 1. PNI Model Also research has supported the fact that many illnesses can be developed through mental stress and strain. Negative emotions lead to ‘immune dysregulation’ leading to physical conditions associated with “aging, cardiovascular diseases, osteoporosis, arthritis, type 2 diabetes, certain cancers, and frailty and functional decline; production of proinflammatory cytokines” and so on
Neuroendocrine System
Immunological System
Mind
Affects overall health systems resulting in possible illness

3
[13]. Solomon and Moos reports early research done by Leshan and Worthington (1956) regarding mental illness/wellbeing as a source for acquiring cancer is reported where some factors in personality traits like bereavement, inability to express hostile emotions and feelings, unresolved tensions, and personal disturbances are experienced prior to the development of tumor [14]. They studied the personality of over 5000 patients with rheumatoid arthritis and came to the conclusion that most of them have common personality traits [14]. Studies on wound healing and post-operative condition reports evidence of slow recovery following stress or fear [15 &16]. Environmental conditions also affect immunologic competence as highlighted in studies done on mice [17 &18]. Riley and colleagues studied the impact of environmental stress on three groups of mice in different environmental conditions. The low stress residential conditions proved beneficial for one group, influencing their immunologic competence contributing to the alteration of tumor incidence [17]. It indicates that apart from physical health being attributed to mental wellness, the implication that environment can play a key role in the reduction of stress where comfort levels, air quality, light and so on can influence in reducing reduced stress levels resulting in physical well-being. Therefore, environmental factors influencing mental wellbeing further contribute to the physical systems ability to alleviate illnesses. Dimensions of the built/interior environment to holistic health The importance of the environment in contributing to stress has long been recognised in environmental, social, and biological sciences. It is well- known that various factors in the environment triggers physical as well as psychological changes in the human body [19-24]. The environment consists of a set of ‘stimuli’ and people behave in response to this and adapt to it becoming more systematic and interdisciplinary in nature [25]. People usually see to it that their personal needs and /or desires and environmental resources are synchronised and this is associated with both “efficacious behavior” and favorable affective outcomes contributing to their wellbeing representing the QOL (quality of life) [26]. The ability to control the physical surroundings is further seen to influence in reducing the negative effects of stress impacting on overall health [27]. Studies done on spatial organization and workplace satisfaction demonstrates the importance of the role of space allocation and organization in the satisfaction and performance of people in a workplace. It also shows the link between the social activities of people within the organization highlighting that spatial organization of the physical environment supports individual process as well as team communication and collaboration [28]. In addition, individual needs and organizational costs are supported by use of imagination in creating a space where visual dimensions can also influence an individuals’ self satisfaction and feelings in an environment [29]. Environments also have restorative effects during times of stress thereby influencing wellbeing. For example people occupying windowless offices tend to use more of nature themes as decorative elements and they incorporate more visual stimuli than people with offices having windows [30]. Another study involving three groups of office workers indicates that people

4
having views of nature are more satisfied with their work having lower level of stress than people having views of buildings or having no view at all [31]. Views may further influence the physical health aspect of individuals and be of benefit as discovered from a study involving patients recovering from surgery. It was found that patient recovery is faster when they have views of nature through their windows than those who overlook the parking lot resulting in shorter hospital stays [32]. However, how a person perceives the environment is not always in a conscious way. Most of the time it occurs at an unconscious level, that is, without being aware of the surroundings. At times minimal attention is directed to the immediate surroundings which accounts for ‘environmental numbness’ in people resulting in causing minor or major problems such as stress [33] Environmental perception is also influenced by various factors like personality and characteristics, sex, age and education, culture, physical features of a setting, familiarity of the setting etc. [33]. The space occupied is relevant to the reactions and behavior of a person [34] which forms the experience gained from the events that take place. Thus, environment and person is interrelated in such a way that the action of the person influences the environment and the environment influence the action and behavior of the person [35]. People do not react to an environment as such, but they react to what they feel or think about the environment and only when it is experienced or acted upon does a space or place acquire meaning [36]. This influences a person on how they perceive the environment. Certain environmental cues like the décor provide a perception in the mind of a person on the personality of people occupying the space influencing the way they act in it. This could be seen as the environment causing an ‘direct and indirect effect’ in influencing the behavior of a person [6]. People often react differently in different situations, or in different settings due to the basis on which they perceive the place [6]. Furthermore people interpret these meanings differently and these interpretations play a critical role in environmental interaction [6]. It is interesting to note that certain environments foster social contacts and an individuals interactions with particular places influence the formation of their self-identity. For example the influence of the environment is so great that sometimes even relocation from a familiar place often produces distress resulting in negative health symptoms [37 & 38]. When trying to make a connection or in forming a relationship with the environment people try to “establish and maintain meaningful psychological and social connections with the material world, reflected in their strong emotional attachments to particular objects and places” [39]. As environments differ in their negative and positive health outcomes, the health promotiveness of an environment “ultimately depends on its capacity to support those health outcomes most desirable and important to its members while eliminating or ameliorating those most clearly negative and detrimental to individual and social well-being” [40]. Stokols suggests that “environmentally based health promotion programs must distinguish between the immediate and potential capacity of a particular setting, or organization, or community to promote health among its members” [40].

5
The potential of PNI dimensions for the built/interior environment As Solomon points out “just as PNI is helping establish necessary new models of health, disease and the body itself, perhaps it can establish, on the basis of evidence, the nature of healing environments” [41]. The interior environment is where an individual spends at least three fourth of his/her time, except in some cases where people work and play in the exterior environments. These environments that we create would be either our ‘inherited environments’ or that those are chosen by us [42]. In establishing a relationship between PNI and the environment, there are several elements that would help in creating a space/place for a person that would enhance health and wellbeing [3, 6, 21, 29, 30, 41, 43, 44, 45, 46]. Some dimensions that could contribute to the wellbeing of a person are: a.) When designing for a group or individual, several characteristics and dimensions could be altered to fit individual preferences. This involves careful scrutiny of individual/group preferences and usages. b.) Sensory experiences that a person derives from the environment are a strong element to take into consideration. Designing for sensory wellbeing influencing the overall health is as important as aesthetics and beauty of a place or space. c.) Usage and usability of environments differs from user to user on an individual basis and only with designer-user interaction could this be ascertained d.) For increasing health and wellbeing from individual to individual basis the interaction of the environment and how a person and environment adapts to each other should also be a priority to focus on. e.) Personal preferences and controllability of an environment plays an important part in maintaining health and wellbeing. f.) The factors that help to “modify a person’s immunological response to a stressor” such as social support, attitude and optimism have been found to be beneficial g.) Individual gender, age and personal attitudes, preferences and personality character should be taken into consideration where possible. h.) The demand of the environment could be real or perceived, few or many, and simple or complex. Adding to the fact that it is not the coping skills that counts, but the coping skills those the individual believe he/she has is of more importance. Studies on healthcare environments mostly concentrate on healing process where the quality of the environments is seen to be affecting healing process. A study done on multisensual environment showed that environments designed for the senses have a positive effect on its occupants. Though this study was done on people with dementia, it may be applicable to any environment. The patients were studied in three different environments – the “snoezelen room” (which was particularly designed for the senses – multisensory environment), a landscaped environment and the usual living room. It was found that patients using the room and the garden became calm and showed pleasure and the wellbeing stayed with them after leaving the room also. The snoezelen room had “a power for stress reduction” to all users alike - the patients, caregivers, visitors and so on in a calm and comforting manner. Whereas, the garden provided a more active environment proving to be therapeutic. Though the study did not find evidence for

6
one environment being more beneficial than the living room, it was observed that the ‘snoezelen room’ and the garden did give occupants more pleasure than the common living room. But the fact remains that even if the place does not have any negative effects they do have positive effects [47]. Research in health care environments proves that the quality of environment can speed or ‘retard’ healing. The planetree model adapted in healthcare environments is holistic in focusing on the patients’ mental, emotional, spiritual, social and physical needs recognizing the importance of architecture and interior design in the healing process [48]. A study done on the facilities of the new and old units of the Barbara Ann Karmanos Cancer Institute showed decrease in the usage of pain medication which is self administered by the patients using new facilities. Though they were the same patients who used more medication in the old facilities they feel the decrease in pain prescription in the more pleasant surroundings of the new unit [49] Conclusion This paper has directed an insight to the possibilities of applying PNI principles to design. Combining these two disciplines would provide a broader understanding of the environmental aspects in creating healthy environments for healthy living. Exploring research in the areas of PNI and built environment and design has shown that there is an overlap with in the broader dimensions. The physical environment is an important component of the multidimensional aspects of a human being. There are several elements in the environment that contribute to the well-being of a person. These elements are perceived by the individual in a conscious and subconscious manner. However, the environment plays a definite role in the health and well-being through the mind of a person. Through sensitive and careful space planning and designing using the key aspects that contributes to mental wellbeing, a less stressful environment can be created to influence the holistic well-being of the person occupying it. This point to a new direction, in focusing on the capacity of the built environment in influencing the holistic health of a person through emotional wellbeing. Further, it would provide an understanding of design principles for application to create an environment which would have properties to alleviate negative health hazards to an extent. References 1. Sommer,R & Oslen,H (1980). The soft classroom . Environment and Behavior, 12, 3-16 ; Wong , C.Y., Sommer,R., & Cook, R., (1992). The soft classroom 17 years later. Journal of environmental Psychology, 12, 337- 343 . 2. Kaplan, S, (1983). A model of person-environment compatibility. Environment and Behavior, 15,311-322. 3. O’Neill, M.J. (1991). Effects of signage and floor plan configuration on way finding accuracy. Environment and Behavior, 23, 553-574. 4. Wapner,S., Demick , J. (2000). Theoretical perspectives in environment-behavior

7
research: Underlying assumptions, research problems, and methodologies (pp.7- 19). S.Wapner, J.Demick, T,Yamamoto,&H.Minami(Eds.).New York : Kluwer Academic/Plenum Press. 5. Parsons, R & Tassinary, L.G (2002).Hand Book of Environmental Psychology. Pp.172-190. Robert B.Bechtel & Arza Churchman (Ed) 6. Rappoport, A. (1990). The meaning of the built Environment: A nonverbal communication approach. The university of Arizona press. 7.Ittelson,W.H; Proshansky,H.H; Rivlin,L.G; Winkel,G (1974).An introduction to environmental psychology. New York: Holt, Rinehart and Winston. 8. Norman Cousins, (1983). The healing heart. New York:Avon books. 9. Ader, R., Felten, D.L., & Cohen, N. (1991). Psychoneuroimmunology 2nd Ed. Academic Press ,San Diego. 10. Hafen, B.Q.; Karren, K.J; Frandsen,K.J; Lee, S.N, (1996). Mind –Body Health. The effect of attitudes, emotions and relationships. Allyn and Bacon Massachusetts.. 11. Smith, A .P (1998). The power of thought to heal: An ontology of personal faith. Claremont Graduate University. 12. Schedlowski, M & Tewes, U ( Ed)(1996) Psychoneuroimmunology: An Interdisciplinary Introduction. Kluwer Academic. Plenum Publishers. 13. Glaser, K.J; K; McGuire, L; Robles, T, F.; Glaser, R,(2002). Psychoneuroimmunology: Psychological influences on immune function and health.70 (3)537-547. Journal of consulting & Clinical Psychology. 14. Solomon, G. F; Moos, R,(1964). Emotions, immunity and diseases: A speculative theoretical integration .11(6) pp. 657-674. Archives of General Psychiatry. ( Leshan, L.L & Worthington, R.E (1956) Personality as Factor in Pathogenesis of Cancer; Review of literature ,Brit Journal of Medical Psychology 29:49) 15. Keicolt-Glaser, et al, (1998). American Psychologist .Nov. Vol. 53(11) 1209-1218. 16. Evans, P; Hucklebridge, F; Angela Chow, (2000). Mind Immunity and Health: The science of Psychoneuroimmunology. 17. Riley,V.V; M.A.Fitzmaurice,M.A; Spackman, D,(1981). Psychoneuroimmunologic Factors in Neoplasia: Studies in Animals. Psychoneuroimmunology, Robert Ader (ED).Academic Press, INC. 18. Benaroya- Milshtein, N; Hollander, N; Apter, A; Kukulansky,T; Raz. N; Wilf, A; Yaniv, I; Pick C.G, (2004) Environmental enrichment in mice decreases anxiety, attenuates stress responses and enhances natural killer cell activity. European journal of Neuroscience, Vol.20, pp.1341-1347 19. Williams, S.M (1994). Environment and mental health. John Wiley & Sons, New York 20. Ray. H.Rosenman. (1994). Human Stress and the environment. Environmental topics- Vol. 5. 21. Gifford, Robert, (1996). Environmental Psychology: Principles and practices. Robert Gifford (2nd Ed). 22. Cohen,S; Evans,G; Stokols, D & Krantz,D, (1991). Behavior, health and Environmental Stress. New York: Plenum Press. 23. Anthony, K.H.,(1998). Designing psychotherapists’ offices: Reflections of an environment-behavior researcher. Paper presented at the American Psychological Association Convention, San Francisco. 24. A. Russel, J.A & Snodgrass, J, (1987). Handbook of environmental psychology. pp.245- 280. Daniel Stokols and Irwin Altman (Ed)

8
25. Altman, I & Rogoff, B, (1987). World views in psychology: Trait, interactional, orgasmic, and transactional perspectives. PP – 7- 40. Handbook of environmental psychology. Daniel Stokols and Irwin Altman (Ed) 26. Lawton, M.P, (1989). Social structure and aging: Psychological processes. LEA Publishers, Hillsdale, NJ 27. Ulrich, R.S, (1992). How Design Impacts Wellness. The healthcare Forum Journal. San Francisco: Sep/ Oct 35(5). 28. McCoy, J. M, (2002).Work Environments.p.447. Hand Book of Environmental Psychology. Robert B.Bechtel and Arza Churchman (ED) 29. Becker, F.& Steele, F.(1995). Workplace by Design: mapping the high-performance workscape. SanFrancisco: Jossey-Bass. 30. Heerwagen, J, (1990). The psychological aspects of windows and window design. Coming of age: Proceedings of the twenty – first annual EDRA Conference. Pp.269-280). Edmond, O K: EDRA. 31. Kaplan, S; Talbot, J; Kalan, R, (1988). Coping with daily hassles: The impact of nearby nature on the work environment .Proj.Rep., U.S.Forest Service , North Central Forest Experiment Station, Urban Forestry Unit Cooperative Agreement 23-85-08. Washington DC: US .Govt. Printing Office. 32. Ulrich, R.S, (1984).View through a window may influence recovery from surgery. Science 224, 420-421. 33. Gifford, R, (1996). Environmental Psychology: Principles and practices. Robert Gifford (2nd Ed). p.16 34. Stokols, D., Altman, I, (1987). Handbook of Environmental Psychology. New York: Wiley press. 35. Bonnes, M & Bonaiuto, M, (2002). Environmental Psychology: From spatial-physical environment to sustainable development. P. 28. Hand book of Environmental Psychology. Robert B.Bechtel and Arza Churchman (EDs) 36. Graumann, C. F, (2002). The Phenomenological Approach to People-Environment Studies. Hand book of Environmental Psychology. Robert B.Bechtel and Arza Churchman (EDs). 37. Festinger, L.; Schachter,S.; Back,K. (1950). Social Pressures in informal groups. NewYork: Harper. 38. Proshansky, H.M.; Fabian, A.K; Kaminoff, R, (1983). Place identity: Physical world socialization of the self. Journal of environmental psychology.Vol.3, 57-83. 39. Stokols, D & Montero, M. (2002) Towards an Environmental Psychology of the Internet. p.666. Hand book of Environmental Psychology, Robert B.Bechtel and Arza Churchman (EDs) 40. Stokols, D; Grzywacz, J.G ; McMahan, S; Philips, K, (2003). Increasing the health promotive capacity of human environments. American journal of health promotion, 18 (9). 41. Solomon,G.F., (1996). Physiological responses to environmental design: understanding psychoneuroimmunology (PNI) and its application for healthcare. Journal Of Healthcare Design. Vol.8, p.83. Symposium on Healthcare Design 42. Weinberg, I (2001) Quantum Determinism Versus Indeterminism: Resolving the Self- empowerment Paradox URL: http://www.wellness.org.za/html/articles/a-versus.html 43. Lisa.G.Aspinwall and Ursula.M.Staudinger (Ed), (2003). A Psychology of human strengths: fundamental questions and future directions for a positive psychology. Published by American Psychological Association.).
9
44. Baron, R.A, (2001). Psychology 5th edition. 45. Gifford, R, (2002). Making a difference: Some ways Environmentsl Psychology has improved the world. Pp 323-333. Hand book of environmental psychology. Robert B.Bechtel and Arza Churchman ) 46. Oakley, R, (2004). American Psychologist .59/1, Pp29-40. 47. Cox, H; Burns, I; Savage, S, (2004). Multisensory Environments for leisure: Promoting well- being in nursery home residents with dementia. Journal of Gerontological Nursing, 30(2), 37-45. 48. Gearon, C. J, (2002) Hospitals and health networks. Chicago: Health and medical journal 76(10). 49. Bilchik, G.S (2002).A better place to heal. Health forum journal. 45(4), Pp.10-15.

10