mapping global health partnerships what they are, what
TRANSCRIPT
GHP Study Paper 1:
MAPPING GLOBAL HEALTH PARTNERSHIPS What they are, what they do and where they operate This paper forms part of the 2004 DFID Study: Global Health Partnerships: Assessing the Impact.
Cindy Carlson DFID Health Resource Centre 27 Old Street London EC1V 9HL Tel: +44 (0) 207 251 9555 Fax: +44 (0) 207 251 9552
The DFID Health Resource Centre (HRC) provides technical assistance and information to the British Government’s Department for International Development (DFID) and its partners in support of pro-poor health policies, financing and services. The HRC is based at IHSD's UK offices and managed by an international consortium of five organisations: Ifakara Health Research and Development Centre, Tanzania (IHRDC); Institute for Health Sector Development, UK (IHSD Limited); ICDDR,B - Centre for Health and Population Research, Bangladesh; Sharan, India; Swiss Centre for International Health (SCIH) of the Swiss Tropical Institute, Switzerland. This report was produced by the Health Resource Centre on behalf of the Department for International Development, and does not necessarily represent the views or the policy of DFID. Title: Mapping Global Health Partnerships Author: Cindy Carlson
DFID Health Resource Centre 27 Old Street London EC1V 9HL Tel: +44 (0) 20 7251 9555 Fax: +44 (0) 20 7251 9552
Table of Contents Acronym List ........................................................................................................... 1 Abbreviations .......................................................................................................... 3 1. Introduction ...................................................................................................... 4 2. Definition of a Global Health Partnership....................................................... 5 3. A Working Typology ........................................................................................ 6 4. Global Mapping of GHPS................................................................................. 7 5. Limitations........................................................................................................ 8 Appendix A – Global Health Partnerships – Basic Information ........................... 9 Appendix B: Global Health Partnerships – Mapping by Country Exercise ..... 27 Appendix C – DFID Interest .................................................................................. 55
Mapping Global Health Partnerships 1
DFID Health Resource Centre
ACRONYM LIST AAI Accelerating Access Initiative to HIV Care ACHAP African Comprehensive HIV/AIDS Partnerships AHPSR Alliance for Health Policy and Systems Research AMD Alliance for Microbicide Development AMP African Malaria Partnership (GSK) APOC African Program for Onchocerciasis Control CF Concept Foundation CICCR Consortium for Industrial Collaboration in
Contraceptive Research CVP Children’s Vaccine Program at PATH DPP Diflucan Partnership Program DNDi Drugs for Neglected Diseases Initiative DVP Dengue Vaccine Project EL-MDRTBP Eli Lilly Multi-Drug Resistance Tuberculosis
Partnership EMVI European Malaria Vaccine Initiative FIND Foundation for Innovative New Diagnostics GAEL Global Alliance to Eliminate Leprosy GAELF Global Alliance for the Elimination of Lymphatic
Filiariasis GAIN Global Alliance for Improved Nutrition GAVI Global Alliance for Vaccines and Immunization GBC Global Business Coalition on HIV/AIDS GCM Global Campaign for Microbicides GCWA Global Coalition on Women and AIDS GET 2020 WHO Alliance for the Global Elimination of Trachoma GFATM Global Fund to Fight AIDS, TB and Malaria GFUNC Gates Foundation/U. of North Carolina Partnership for
the Development of New Drugs GMAI Global Media AIDS Initiative GMP Global Microbicide Project GOARN Global Outbreak Alert and Response Network GPEI Global Polio Eradication Initiative GPHW Global Public-Private Partnership for Hand Washing
with Soap GRI Global Reporting Initiative GWEP Guinea Worm Eradication Program HACI Hope for African Children Initiative HATC HIV/AIDS Treatment Consortium (Clinton Foundation
AIDS Initiative) HHVI Human Hookworm Vaccine Initiative HIN Health InterNetwork HTVN HIV Vaccine Trials Network IAVI International AIDS Vaccine Initiative IDRI Infectious Disease Research Institute IOWH Infectious Disease Research Institute IPAAA International Partnership Against AIDS in Africa IPM International Partnership for Microbicides ITI International Trachoma Initiative JPMW Japanese Pharmaceutical, Ministry of Health, WHO
Malaria Drug Partnership
Mapping Global Health Partnerships 2
DFID Health Resource Centre
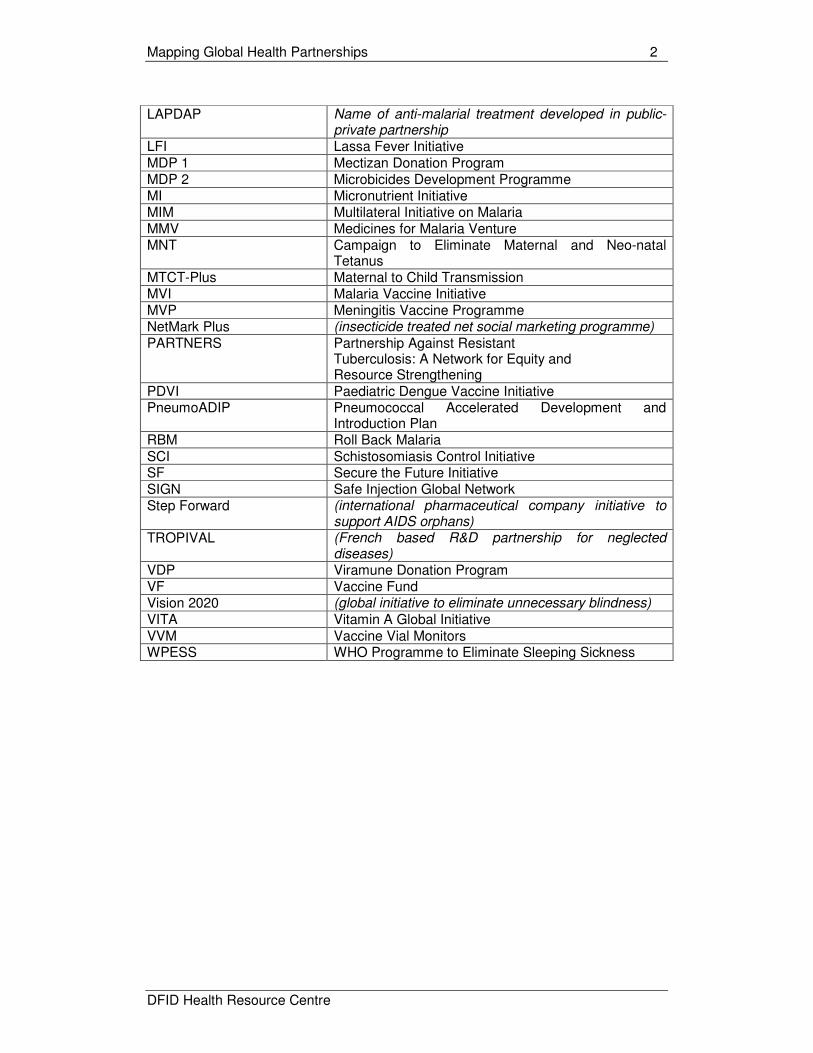
LAPDAP Name of anti-malarial treatment developed in public-
private partnership LFI Lassa Fever Initiative MDP 1 Mectizan Donation Program MDP 2 Microbicides Development Programme MI Micronutrient Initiative MIM Multilateral Initiative on Malaria MMV Medicines for Malaria Venture MNT Campaign to Eliminate Maternal and Neo-natal
Tetanus MTCT-Plus Maternal to Child Transmission MVI Malaria Vaccine Initiative MVP Meningitis Vaccine Programme NetMark Plus (insecticide treated net social marketing programme)
PARTNERS Partnership Against Resistant Tuberculosis: A Network for Equity and Resource Strengthening
PDVI Paediatric Dengue Vaccine Initiative PneumoADIP Pneumococcal Accelerated Development and
Introduction Plan RBM Roll Back Malaria SCI Schistosomiasis Control Initiative SF Secure the Future Initiative SIGN Safe Injection Global Network Step Forward (international pharmaceutical company initiative to
support AIDS orphans) TROPIVAL (French based R&D partnership for neglected
diseases) VDP Viramune Donation Program VF Vaccine Fund Vision 2020 (global initiative to eliminate unnecessary blindness)
VITA Vitamin A Global Initiative VVM Vaccine Vial Monitors WPESS WHO Programme to Eliminate Sleeping Sickness
Mapping Global Health Partnerships 3
DFID Health Resource Centre
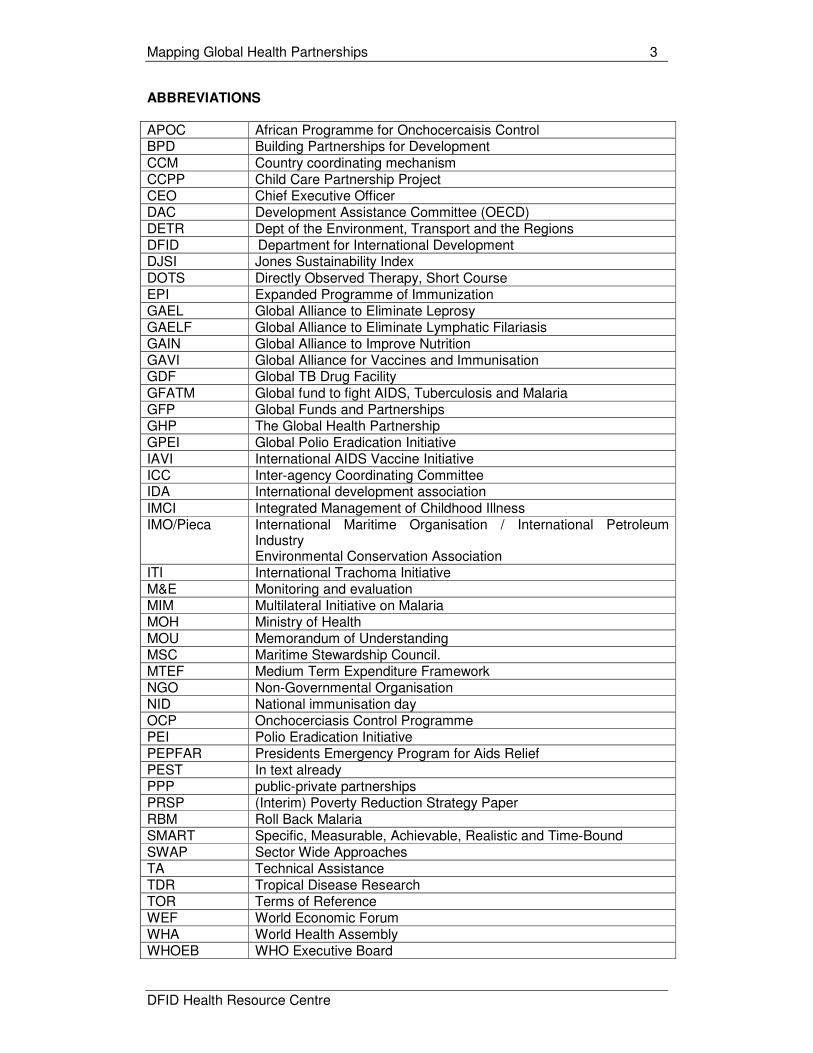
ABBREVIATIONS APOC African Programme for Onchocercaisis Control BPD Building Partnerships for Development CCM Country coordinating mechanism CCPP Child Care Partnership Project CEO Chief Executive Officer DAC Development Assistance Committee (OECD) DETR Dept of the Environment, Transport and the Regions DFID D Department for International Development DJSI Jones Sustainability Index DOTS Directly Observed Therapy, Short Course EPI Expanded Programme of Immunization GAEL Global Alliance to Eliminate Leprosy GAELF Global Alliance to Eliminate Lymphatic Filariasis GAIN Global Alliance to Improve Nutrition GAVI Global Alliance for Vaccines and Immunisation GDF Global TB Drug Facility GFATM Global fund to fight AIDS, Tuberculosis and Malaria GFP Global Funds and Partnerships GHP The Global Health Partnership GPEI Global Polio Eradication Initiative IAVI International AIDS Vaccine Initiative ICC Inter-agency Coordinating Committee IDA International development association IMCI Integrated Management of Childhood Illness IMO/Pieca International Maritime Organisation / International Petroleum
Industry Environmental Conservation Association
ITI International Trachoma Initiative M&E Monitoring and evaluation MIM Multilateral Initiative on Malaria MOH Ministry of Health MOU Memorandum of Understanding MSC Maritime Stewardship Council. MTEF Medium Term Expenditure Framework NGO Non-Governmental Organisation NID National immunisation day OCP Onchocerciasis Control Programme PEI Polio Eradication Initiative PEPFAR Presidents Emergency Program for Aids Relief PEST In text already PPP public-private partnerships PRSP (Interim) Poverty Reduction Strategy Paper RBM Roll Back Malaria SMART Specific, Measurable, Achievable, Realistic and Time-Bound SWAP Sector Wide Approaches TA Technical Assistance TDR Tropical Disease Research TOR Terms of Reference WEF World Economic Forum WHA World Health Assembly WHOEB WHO Executive Board

Mapping Global Health Partnerships 4
DFID Health Resource Centre
INTRODUCTION The purpose of mapping Global Health Partnerships (GHPs) is to provide a common understanding of what GHPs are, how they might be classified and how they operate. This paper explains the definition used by the project team in their work on ‘Assessing the Impact of GHPs’, outlines a classification system of GHPs to help with analysis of their impact and maps where GHPs are working globally.

Mapping Global Health Partnerships 5
DFID Health Resource Centre
1. DEFINITION OF A GLOBAL HEALTH PARTNERSHIP Previous work1 in this series defines the concept of Global Health Partnership in a broad manner:
Partnership: the key criterion is a collaborative relationship among multiple organisations in which risks and benefits are shared in pursuit of a shared goal. The focus is on more formal collaborative ventures and not exclusively on public-private partnerships, although these constitute the majority. Some important global health initiatives that are not partnerships per se, such as the World Bank’s MAP, are not included.
Health: The goal of the partnerships has to concern the redress of health problems of significance for the poor in low- and middle-income countries.
‘Global’ is interpreted to capture initiatives that extend across or transcend national boundaries. In this paper for example, APOC – the African Programme for Onchocerciasis Control – is included as a GHP addressing a neglected disease, though technically it operates only within Africa rather than globally. It forms the main operating component of the Global Partnership to Eliminate River Blindness.
The World Bank’s definition of global programs are those partnerships and related initiatives whose benefits cut across more than one region of the world, and in which the partners reach explicit agreements on objectives; agree to establish a new (formal or informal) organization; generate new products or services; and contribute dedicated resources to the program2. This is a tighter definition but can generally be applied to the GHPs covered in the study, other than the geographical limitation. See Appendix A for the full list of GHPs and their principal objectives.
1 Buse K., 2004. Global Health Partnerships: Mapping a shifting terrain. London: DFID Health Resource Centre.
2 Operations Evaluation Department, World Bank. The World Bank’s Approach to Global Programs: An Independent Evaluation. The World Bank, August 1, 2002.

Mapping Global Health Partnerships 6
DFID Health Resource Centre
2. A WORKING TYPOLOGY A number of typologies have been suggested for classifying the different GHPs (Tidewater 2003; Buse 2004). The project team considered each of these, attempting to classify nineteen GHPs of interest to DFID (see below) against these existing typologies. The classification exercise highlighted a number of problems with previous typologies.. In this study, the project team adopted a typology proposed by DFID with the following four categories to classify GHPs: • Research and Development: This includes GHPs that are involved in product
discovery and development of new therapies (vaccines, treatments etc.); • Technical assistance/service support: This includes GHPs that provide drug
donations, support improved service access and give technical assistance; • Advocacy (national and international levels): includes GHPs who advocate for
increased international and national response to specific diseases, who fund-raise for specific control programmes etc.
• Financing: includes GHPs who provide funds for specific programmes (not as donations).
GHPs have then been classified against this typology as to whether they have a primary or secondary role in these areas. See Appendix B for tables showing GHP classification. This classification is based on the stated objectives of each GHP, as well as an understanding of the modus operandi of each one.
Mapping Global Health Partnerships 7
DFID Health Resource Centre
3. GLOBAL MAPPING OF GHPS The project team also mapped where Global Health Partnerships provide support on a country by country basis, and analysed this against epidemiological and socio-economic information of these countries. The initial global mapping was done early in the project in order to inform decisions as to which countries to include in the country case study work. Key findings are that the strongest correlation for a high number of GHPs operating in a country is the region the country belongs to, with Africa having consistently the highest number of GHPs per country, followed by Asia (East, Southeast and Central). Eastern and Central European countries have the lowest number of GHPs. There appears to be a correlation between the per capita GDP and the number of GHPs operating in a country. In general, the lower the per capita GDP, the greater the number of GHPs, though this is inconsistent. There is a moderate correlation between the prevalence rate or case number of a disease and the presence of the relevant GHP, as would be expected. However, without looking at GFATM support on a country by country basis, it is impossible to assess whether appropriate levels of GFATM funding are being received by each of its three target diseases in each country where it is present, based on the epidemiology of the disease in that country, There is no apparent correlation between the number and type of GHPs operating in a country and:
- the type of government as measured on a scale of –10 (authoritarian) to +10 (fully democratic); or
- the percentage of spending on the health sector coming from the public purse.
Information from the full mapping exercise and analysis can be found in Appendix C.
Mapping Global Health Partnerships 8
DFID Health Resource Centre
4. LIMITATIONS The team encountered a number of constraints in trying to identify a useful typology as well as in mapping and analysing GHPs on a global level. These included the following: • While the list of GHPs is meant to be as exhaustive as possible, some are difficult
to identify and new ones are set up on a frequent basis. Also, there are definitional difficulties and some of the organisations included on the list in Appendix A may not fit with everyone’s interpretation of a GHP.
• GHPs are complex beasts and are not easily slotted into specific boxes on a table. Also, GHPs may change how they work depending on whether they are assessed at an international or national level. As such, the proposed classification found in Appendix B is open for further debate and discussion. For the purposes of this paper, it is their international ‘face’ that is being considered.
• The global mapping exercise focused primarily on those countries that appear to have the greatest number of active GHPs in-country. As such, not all countries have complete epidemiological or socio-economic information provided.
Mappin
g G
lobal H
ealth P
art
ners
hip
s
9
DF
ID H
ealth R
esourc
e C
entr
e
AP
PE
ND
IX A
– G
LO
BA
L H
EA
LT
H P
AR
TN
ER
SH
IPS
– B
AS
IC I
NF
OR
MA
TIO
N
Ac
ron
ym
M
issio
n,
Aim
s a
nd
/or
Ob
jecti
ves
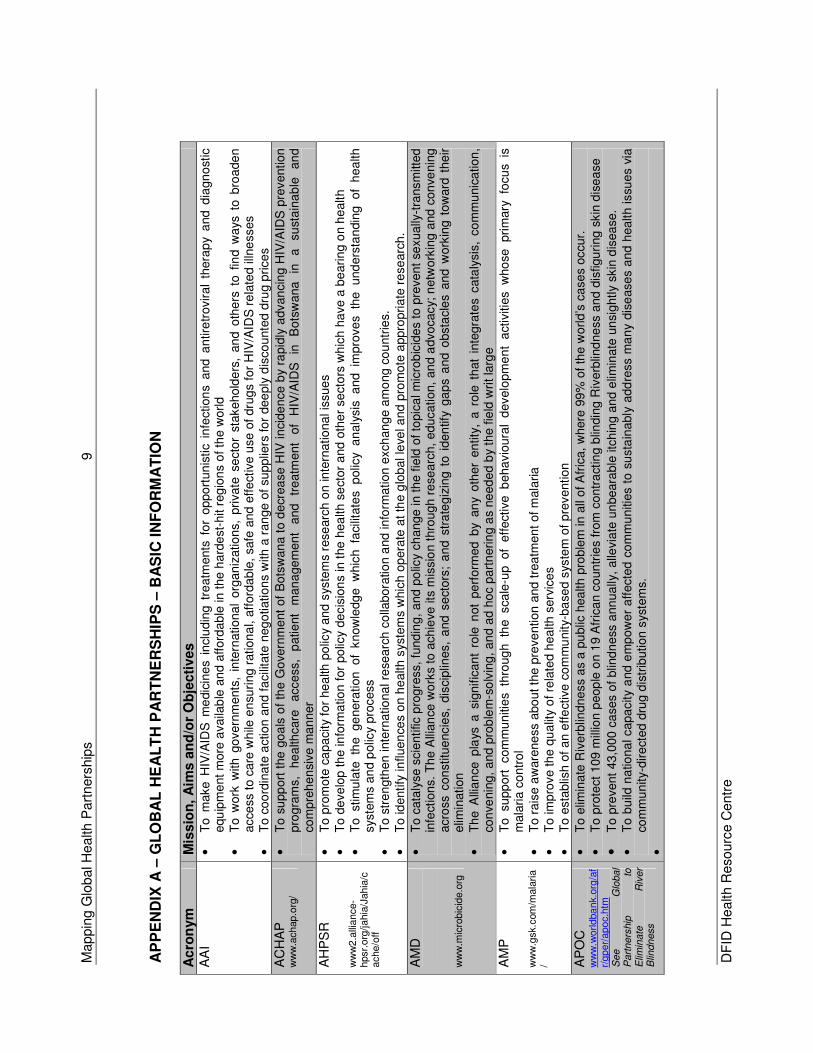
AA
I •
To m
ake
HIV
/AID
S m
edic
ine
s in
clu
din
g t
reatm
ents
fo
r oppo
rtun
istic
infe
ction
s and a
ntir
etr
ovir
al
thera
py
and d
iagn
ost
ic
equ
ipm
ent
more
availa
ble
an
d a
fford
ab
le in t
he
ha
rde
st-
hit r
eg
ion
s o
f th
e w
orld
•
To w
ork
with g
overn
ments
, in
tern
ationa
l org
an
izatio
ns,
pri
vate
se
cto
r st
akehold
ers
, an
d o
the
rs t
o f
ind w
ays
to b
roa
de
n
acce
ss t
o c
are
wh
ile e
nsu
ring r
ation
al,
aff
ord
ab
le,
safe
and
eff
ect
ive u
se o
f dru
gs f
or
HIV
/AID
S r
ela
ted illn
esses
•
To c
oo
rdin
ate
action
an
d fa
cili
tate
neg
otiation
s w
ith a
ran
ge
of
su
pplie
rs fo
r dee
ply
dis
co
unte
d d
rug p
rice
s
AC
HA
P
ww
w.a
chap.o
rg/
•
To s
upp
ort
the
go
als
of
the
Go
vern
me
nt
of
Bots
wan
a t
o d
ecr
ea
se
HIV
in
cid
en
ce b
y ra
pid
ly a
dvan
cin
g H
IV/A
IDS
pre
vention
pro
gra
ms,
he
alth
care
access,
patie
nt
man
age
men
t and
tre
atm
ent
of
HIV
/AID
S
in
Bots
wana
in
a
su
sta
ina
ble
an
d
com
pre
he
nsi
ve m
an
ner
AH
PS
R
ww
w2.a
lliance-
hpsr.
org
/jahia
/Jahia
/cache/o
ff
•
To p
rom
ote
ca
pa
city
for
he
alth
po
licy
an
d s
yste
ms r
ese
arc
h o
n in
tern
atio
na
l is
sue
s
•
To d
eve
lop t
he
info
rma
tion
for
po
licy
de
cis
ion
s in
the h
ea
lth s
ect
or
and
oth
er
se
cto
rs w
hic
h h
ave a
be
arin
g o
n h
ealth
•
To stim
ula
te th
e ge
nera
tion
of
know
ledg
e w
hic
h fa
cilit
ate
s p
olic
y a
naly
sis
a
nd im
pro
ve
s th
e und
ers
tan
din
g of
hea
lth
sys
tem
s a
nd p
olic
y pro
cess
•
To s
tre
ngth
en inte
rnatio
na
l re
sea
rch
co
llabora
tio
n a
nd info
rmation e
xch
an
ge a
mo
ng c
ou
ntr
ies.
•
To id
entify
in
fluen
ces o
n h
ealth
sys
tem
s w
hic
h o
pera
te a
t th
e g
lob
al le
vel a
nd
pro
mote
appro
pri
ate
re
se
arc
h.
AM
D
ww
w.m
icro
bic
ide.o
rg
•
To
cata
lyse
scie
ntific p
rogre
ss, fu
nd
ing
, a
nd
po
licy
ch
ange
in t
he f
ield
of to
pic
al m
icro
bic
ide
s t
o p
reven
t se
xually
-tra
nsm
itte
d
infe
ctio
ns.
Th
e A
llian
ce w
ork
s t
o a
ch
ieve
its
mis
sio
n t
hro
ugh r
ese
arc
h,
ed
ucation,
an
d a
dvo
cacy;
netw
ork
ing a
nd c
on
venin
g
acro
ss c
on
stitu
encie
s, d
iscip
lines,
and s
ect
ors
; a
nd s
tra
teg
izin
g t
o i
den
tify
ga
ps a
nd
obsta
cle
s a
nd
work
ing t
ow
ard
the
ir
elim
ination
•
Th
e A
llia
nce
pla
ys a
sig
nific
an
t ro
le n
ot
pe
rform
ed
by
an
y o
ther
en
tity
, a
ro
le t
hat
inte
gra
tes
cata
lysis
, co
mm
unic
ation
, co
nve
nin
g,
and p
rob
lem
-so
lvin
g, a
nd a
d h
oc p
art
nerin
g a
s ne
ed
ed b
y th
e f
ield
wri
t la
rge
AM
P
ww
w.g
sk.c
om
/mala
ria
/
•
To su
pp
ort
com
mu
niti
es
thro
ug
h th
e sca
le-u
p of
eff
ective b
eha
vio
ura
l d
evelo
pm
en
t a
ctiv
itie
s w
ho
se pri
mary
fo
cu
s is
m
ala
ria
co
ntr
ol
•
To r
ais
e a
ware
ne
ss
abo
ut th
e p
reve
ntion a
nd
tre
atm
en
t of m
ala
ria
•
To im
pro
ve th
e q
ua
lity
of re
late
d h
ea
lth s
erv
ice
s
•
To e
sta
blis
h o
f a
n e
ffe
ctiv
e c
om
mu
nity-
ba
sed
sys
tem
of p
revention
AP
OC
w
ww
.worldba
nk.o
rg/a
fr/
gper/
apoc.h
tm
See
Glo
bal
Part
ners
hip
to
E
limin
ate
R
iver
Blin
dness
•
To e
limin
ate
Riv
erb
lindne
ss
as a
pu
blic
hea
lth
pro
ble
m in
all
of A
fric
a,
where
99
% o
f th
e w
orld
’s c
ase
s occur.
•
To p
rote
ct
109
mill
ion p
eop
le o
n 1
9 A
fric
an c
oun
trie
s fro
m c
ontr
act
ing b
lindin
g R
iverb
lind
ne
ss
and
dis
figu
ring
skin
dis
ea
se
•
To p
revent
43,0
00
ca
ses o
f blin
dn
ess
ann
ua
lly,
alle
via
te u
nbeara
ble
itc
hin
g a
nd
elim
inate
un
sig
htly
skin
dis
ea
se.
•
To b
uild
na
tion
al capa
city
and e
mp
ow
er
aff
ecte
d c
om
mu
niti
es t
o s
usta
inably
add
ress m
an
y dis
ease
s a
nd h
ealth issu
es
via
co
mm
un
ity-
dire
cted d
rug d
istr
ibution s
yste
ms.
•
Mappin
g G
lobal H
ealth P
art
ners
hip
s
10
DF
ID H
ealth R
esourc
e C
entr
e
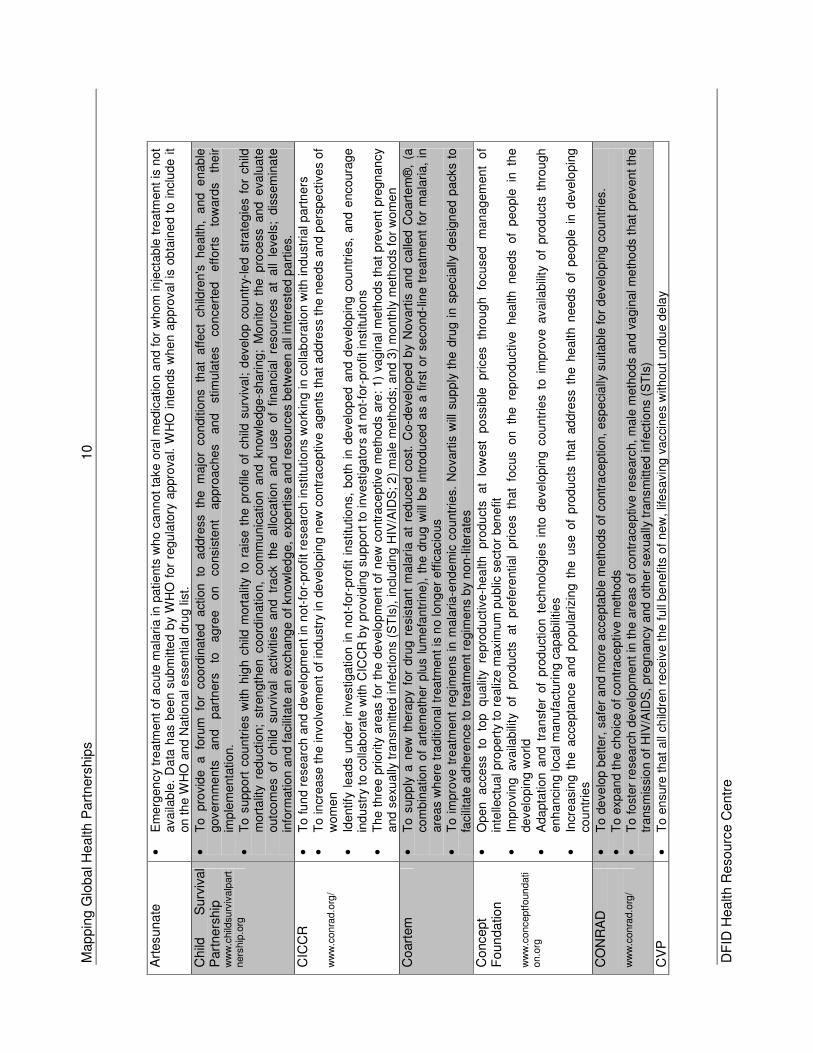
Art
esunate
•
Em
erg
en
cy
tre
atm
ent
of
acute
ma
lari
a in p
atie
nts
who
can
no
t ta
ke o
ral m
ed
icatio
n a
nd f
or
whom
in
ject
ab
le t
reatm
ent
is n
ot
ava
ilab
le.
Da
ta h
as b
ee
n s
ubm
itte
d b
y W
HO
for
regu
lato
ry a
ppro
val.
WH
O in
ten
ds
whe
n a
ppro
va
l is
ob
tain
ed t
o i
nclu
de i
t on t
he W
HO
and
Natio
na
l e
ssentia
l dru
g lis
t.
Child
S
urv
ival
Part
ners
hip
w
ww
.child
surv
ivalp
art
ners
hip
.org
•
To p
rovid
e a
foru
m fo
r coord
inate
d
act
ion
to
addre
ss th
e m
ajo
r co
nditio
ns
that
aff
ect
child
ren's
he
alth,
and e
nab
le
govern
me
nts
an
d
part
ners
to
a
gre
e
on
co
nsis
tent
appro
ache
s
an
d
stim
ula
tes
con
cert
ed
e
ffort
s
tow
ard
s th
eir
imp
lem
enta
tion.
•
To
supp
ort
cou
ntr
ies
with
hig
h c
hild
mort
alit
y to
rais
e t
he p
rofile
of
child
surv
iva
l; d
evelo
p c
ou
ntr
y-le
d s
tra
teg
ies f
or
child
m
ort
alit
y re
du
ctio
n;
str
en
gth
en
coord
inatio
n,
co
mm
un
ication an
d k
now
ledge-s
ha
ring;
Mo
nitor
the pro
cess
and
eva
luate
outc
om
es of
ch
ild surv
iva
l activi
tie
s and
tr
ack th
e a
lloca
tio
n a
nd
u
se of
fina
ncia
l re
so
urc
es at
all
leve
ls;
dis
sem
ina
te
info
rmation a
nd
fa
cilit
ate
an
exch
ang
e o
f kno
wle
dg
e,
expert
ise
and r
eso
urc
es b
etw
een a
ll in
tere
ste
d p
art
ies.
CIC
CR
w
ww
.conra
d.o
rg/
•
To f
un
d r
esearc
h a
nd d
eve
lopm
en
t in
not-
for-
pro
fit re
sea
rch
institu
tio
ns w
ork
ing in
colla
bora
tio
n w
ith in
du
stri
al p
art
ners
•
To in
crea
se t
he in
vo
lvem
en
t of
ind
ustr
y in
de
ve
lop
ing n
ew
con
tra
ceptive a
gents
th
at
addre
ss t
he n
ee
ds
and p
ers
pe
ctiv
es o
f w
om
en
•
Identify
le
ad
s u
nder
investiga
tion
in n
ot-
for-
pro
fit
institu
tions,
bo
th i
n d
evelo
ped
and d
evelo
pin
g c
ou
ntr
ies,
and
encoura
ge
ind
ustr
y to
colla
bo
rate
with
CIC
CR
by
pro
vid
ing
sup
port
to
in
ve
stig
ato
rs a
t no
t-fo
r-pro
fit in
stitu
tio
ns
•
Th
e t
hre
e p
rio
rity
are
as f
or
the d
eve
lop
men
t of
new
co
ntr
ace
ptive m
eth
od
s are
: 1)
vag
ina
l m
eth
od
s th
at
pre
ven
t pre
gn
an
cy
and
se
xually
tra
nsm
itte
d in
fectio
ns
(ST
Is),
in
clud
ing H
IV/A
IDS
; 2
) m
ale
me
tho
ds;
an
d 3
) m
onth
ly m
eth
od
s f
or
wo
me
n
Coart
em
•
To
supp
ly a
new
the
rap
y fo
r dru
g r
esis
tan
t m
ala
ria a
t re
du
ced
co
st. C
o-d
eve
lop
ed b
y N
ovart
is a
nd
calle
d C
oart
em
®,
(a
com
bin
atio
n o
f a
rte
meth
er
plu
s lu
me
fan
trin
e),
th
e d
rug w
ill b
e i
ntr
od
uced
as
a f
irst
or
se
co
nd-l
ine
tre
atm
ent
for
ma
lari
a,
in
are
as w
here
tra
ditio
nal tr
ea
tment
is n
o lo
ng
er
eff
icacio
us
•
To i
mpro
ve t
reatm
ent
reg
ime
ns
in m
ala
ria-e
nde
mic
co
untr
ies.
No
vart
is w
ill s
up
ply
th
e d
rug i
n s
pecia
lly d
esig
ned p
ack
s to
fa
cili
tate
ad
here
nce
to
tre
atm
ent re
gim
ens b
y n
on-litera
tes
Concept
Foundatio
n
ww
w.c
onceptf
oundati
on.o
rg
•
Open
a
cce
ss
to
top
qua
lity
repro
du
ctiv
e-h
ea
lth
pro
du
cts
a
t lo
west
po
ssib
le
prices
thro
ug
h
focused
man
ag
em
en
t o
f in
telle
ctu
al pro
pert
y to
realiz
e m
axim
um
pu
blic
se
ctor
ben
efit
•
Imp
rovin
g availa
bili
ty of
pro
ducts
at
pre
fere
ntial
pri
ces
that
focus on
th
e re
pro
ductive
hea
lth
ne
ed
s o
f p
eo
ple
in
th
e
develo
pin
g w
orld
•
Ada
pta
tio
n a
nd t
ran
sfer
of
pro
du
ctio
n t
ech
no
log
ies
into
de
ve
lopin
g c
oun
trie
s t
o i
mpro
ve a
vaila
bili
ty o
f pro
du
cts
thro
ugh
enh
ancin
g lo
cal m
an
ufa
ctu
ring c
ap
ab
ilitie
s
•
Incr
easin
g t
he a
cce
pta
nce
and p
op
ula
rizin
g t
he u
se o
f p
rod
ucts
that
addre
ss t
he
he
alth n
eed
s of
pe
op
le i
n d
eve
lopin
g
cou
ntr
ies
CO
NR
AD
w
ww
.conra
d.o
rg/
•
To d
eve
lop b
ett
er,
safe
r an
d m
ore
acce
pta
ble
me
tho
ds
of
contr
ace
ptio
n,
esp
eci
ally
su
ita
ble
fo
r d
eve
lop
ing c
ountr
ies.
•
To e
xp
an
d t
he c
ho
ice o
f co
ntr
aceptive m
eth
ods
•
To
fo
ste
r re
se
arc
h d
eve
lop
men
t in
th
e a
reas o
f co
ntr
ace
ptive r
ese
arc
h, m
ale
meth
od
s a
nd v
agin
al m
eth
ods t
hat p
revent
the
transm
issi
on o
f H
IV/A
IDS
, pre
gn
an
cy
and
oth
er
sexua
lly t
ran
sm
itted infe
ctio
ns (
ST
Is)
CV
P
•
To e
nsure
that
all
child
ren r
ece
ive t
he
full
be
nefits
of
new
, lif
esa
vin
g v
acci
ne
s w
ith
out
undu
e d
ela
y
Mappin
g G
lobal H
ealth P
art
ners
hip
s
11
DF
ID H
ealth R
esourc
e C
entr
e
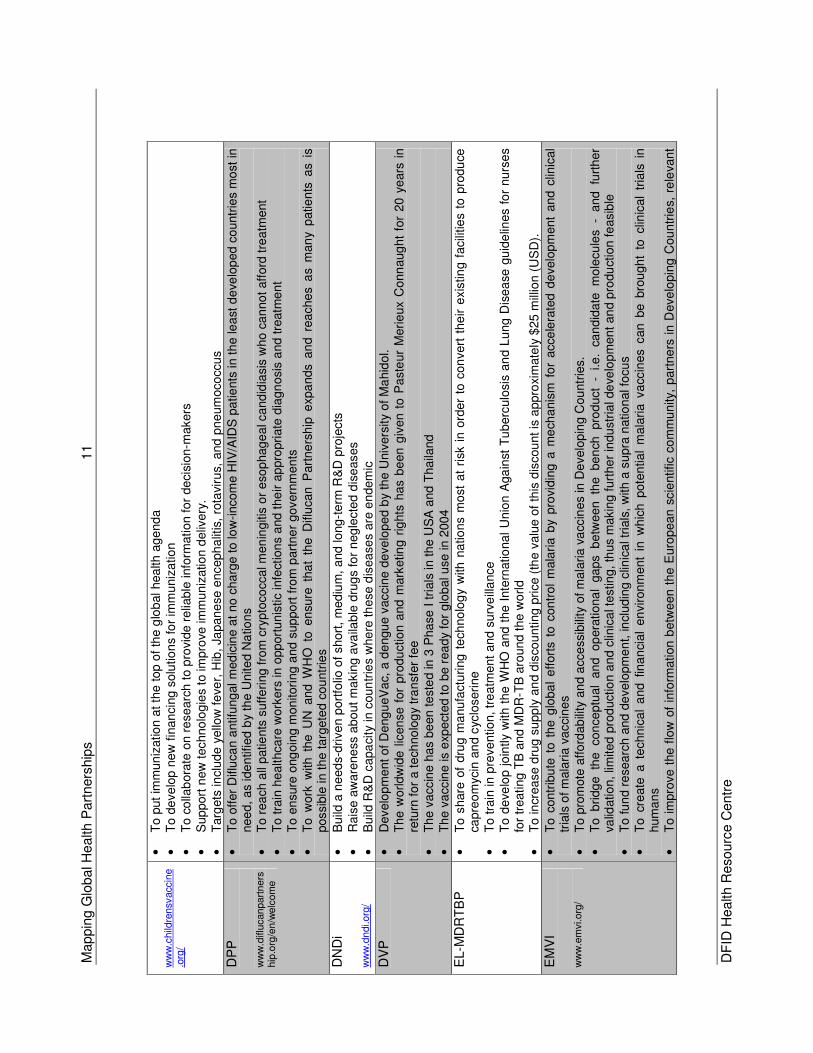
ww
w.c
hild
rensv
acc
ine
.org
/
•
To p
ut
imm
un
izatio
n a
t th
e t
op
of
the
glo
bal hea
lth a
ge
nd
a
•
To d
eve
lop n
ew
fin
an
cin
g s
olu
tio
ns
for
imm
uniz
atio
n
•
To c
olla
bora
te o
n r
ese
arc
h t
o p
rovid
e r
elia
ble
info
rmation f
or
de
cis
ion-m
akers
•
Sup
port
new
techno
log
ies
to im
pro
ve im
mun
izatio
n d
eliv
ery
. •
Targ
ets
in
clu
de
yello
w f
eve
r, H
ib,
Japan
ese e
nceph
alit
is,
rota
viru
s, a
nd
pn
eum
oco
ccu
s
DP
P
ww
w.d
iflu
canpart
ners
hip
.org
/en/w
elc
om
e
•
To
off
er
Diflu
ca
n a
ntifu
ng
al m
ed
icin
e a
t no
cha
rge
to lo
w-incom
e H
IV/A
IDS
pa
tie
nts
in t
he le
ast
de
velo
ped c
ountr
ies m
ost
in
nee
d, a
s ide
ntif
ied
by
the U
nite
d N
atio
ns
•
To r
ea
ch a
ll p
atie
nts
suffe
ring f
rom
cry
pto
co
cca
l men
ingitis
or
eso
phag
ea
l cand
idia
sis
who c
an
no
t aff
ord
tre
atm
ent
•
To t
rain
he
althca
re w
ork
ers
in o
pp
ort
un
istic
infe
ctio
ns a
nd t
he
ir a
ppro
pri
ate
dia
gn
osis
and
tre
atm
en
t •
To e
nsure
ong
oin
g m
on
itori
ng a
nd
sup
po
rt fro
m p
art
ne
r govern
men
ts
•
To w
ork
with t
he
UN
and
WH
O t
o e
nsu
re t
ha
t th
e D
iflu
can
Part
ne
rsh
ip e
xpa
nds a
nd r
ea
che
s a
s m
an
y p
atie
nts
as
is
possib
le in t
he targ
ete
d c
ou
ntr
ies
DN
Di
ww
w.d
ndi.org
/
•
Build
a n
eed
s-d
rive
n p
ort
folio
of short
, m
ed
ium
, a
nd lo
ng-t
erm
R&
D p
roje
cts
•
Rais
e a
wa
rene
ss a
bo
ut
ma
kin
g a
vaila
ble
dru
gs
for
neg
lecte
d d
ise
ases
•
Build
R&
D c
apa
city
in c
oun
trie
s w
he
re th
ese
dis
ea
se
s are
en
dem
ic
DV
P
•
Develo
pm
ent
of D
eng
ueV
ac,
a d
engu
e v
accin
e d
eve
lope
d b
y th
e U
niv
ers
ity
of
Ma
hid
ol.
•
Th
e w
orldw
ide l
icen
se f
or
pro
du
ctio
n a
nd
mark
etin
g r
ights
ha
s b
een g
iven t
o P
aste
ur
Meri
eux C
onn
aug
ht
for
20 y
ears
in
retu
rn for
a t
ech
no
log
y tr
an
sfer
fee
•
Th
e v
accin
e h
as
be
en
te
ste
d in
3 P
ha
se I
tri
als
in th
e U
SA
and
Tha
iland
•
Th
e v
accin
e is e
xpe
cted t
o b
e r
ea
dy
for
glo
bal u
se in 2
004
EL-M
DR
TB
P
•
To
share
of
dru
g m
anu
factu
ring
te
ch
no
log
y w
ith n
atio
ns m
ost
at
risk
in o
rder
to c
on
vert
the
ir e
xis
tin
g f
acili
tie
s to
pro
du
ce
capre
om
ycin
an
d c
yclo
seri
ne
•
To t
rain
in
pre
ve
ntio
n, tr
ea
tment
and
su
rve
illa
nce
•
To d
eve
lop jo
intly
with t
he W
HO
and
the I
nte
rnatio
na
l U
nio
n A
ga
inst
Tu
berc
ulo
sis
an
d L
ung D
ise
ase
gu
ide
lines
for
nu
rse
s fo
r tr
eating
TB
and
MD
R-T
B a
round
the w
orl
d
•
To in
crea
se
dru
g s
upp
ly a
nd d
isco
unting p
rice (
the v
alu
e o
f th
is d
iscou
nt is
appro
xim
ate
ly $
25
mill
ion (
US
D).
EM
VI
ww
w.e
mvi.o
rg/
•
To c
ontr
ibu
te t
o t
he g
loba
l e
ffort
s t
o c
on
tro
l m
ala
ria b
y pro
vid
ing a
me
cha
nis
m f
or
acce
lera
ted d
evelo
pm
ent
an
d c
linic
al
tria
ls o
f m
ala
ria v
acci
ne
s
•
To p
rom
ote
affo
rdab
ility
an
d a
cce
ssib
ility
of
ma
laria v
acc
ines
in D
evelo
pin
g C
ou
ntr
ies.
•
To b
ridg
e th
e con
ce
ptu
al
an
d op
era
tiona
l ga
ps b
etw
een th
e be
nch
pro
duct
- i.e
. ca
nd
ida
te m
ole
cu
les -
and fu
rth
er
valid
atio
n,
limited
pro
ductio
n a
nd c
linic
al t
estin
g, th
us
makin
g furt
he
r in
du
str
ial de
velo
pm
en
t an
d p
rodu
ctio
n f
easib
le
•
To f
un
d r
esearc
h a
nd d
eve
lopm
en
t, in
clud
ing c
linic
al tr
ials
, w
ith a
supra
natio
nal fo
cu
s
•
To
cre
ate
a t
echn
ica
l a
nd
fin
an
cia
l en
viron
ment
in w
hic
h p
ote
ntia
l m
ala
ria
va
ccin
es c
an b
e b
rou
gh
t to
clin
ical
tria
ls i
n
hum
an
s
•
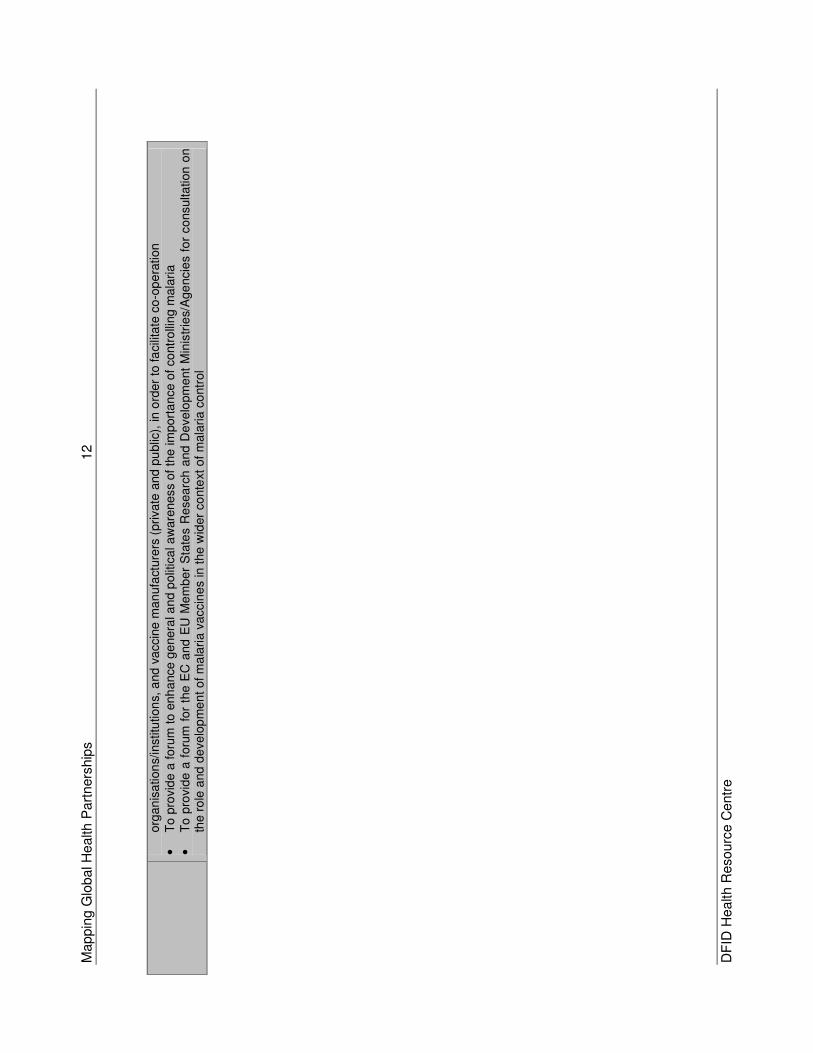
To i
mpro
ve
the f
low
of
info
rmation b
etw
een
th
e E
uro
pean
scie
ntific c
om
mu
nity,
part
ne
rs i
n D
eve
lopin
g C
ou
ntr
ies,
re
leva
nt
Mappin
g G
lobal H
ealth P
art
ners
hip
s
12
DF
ID H
ealth R
esourc
e C
entr
e
org
an
isa
tion
s/in
stitu
tion
s, a
nd v
accin
e m
an
ufa
cture
rs (
pri
vate
and
pu
blic
), in o
rder
to fa
cili
tate
co
-op
era
tion
•
To p
rovid
e a
fo
rum
to e
nh
ance
ge
nera
l an
d p
olit
ica
l a
ware
ness
of
the im
port
an
ce o
f co
ntr
olli
ng
mala
ria
•
To
pro
vid
e a
foru
m f
or
the E
C a
nd
EU
Me
mb
er
Sta
tes R
esearc
h a
nd
De
ve
lopm
ent
Min
istr
ies/
Age
ncie
s fo
r consulta
tion
on
th
e r
ole
and
de
ve
lop
me
nt o
f m
ala
ria v
accin
es
in t
he
wid
er
co
nte
xt o
f m
ala
ria
co
ntr
ol
Mappin
g G
lobal H
ealth P
art
ners
hip
s
13
DF
ID H
ealth R
esourc
e C
entr
e
FIN
D
ww
w.f
inddia
gnostics
.org
•
To a
cce
lera
te t
he d
eve
lop
ment, e
valu
ation,
an
d a
ppro
priate
use
of
hig
h-q
ua
lity
yet
aff
ord
able
dia
gn
ost
ic t
ools
fo
r in
fectio
us
dis
ea
ses
in d
eve
lop
ing c
ou
ntr
ies (
initia
l fo
cus o
n T
B)
•
To d
eve
lop d
iagn
ostic ap
pro
ache
s th
at
have
bee
n pro
ve
n in
pri
ncip
le an
d tr
ansfo
rm th
em
in
to effe
ctive p
rodu
cts,
in
part
ners
hip
with
acad
em
ia,
pub
lic a
nd p
riva
te r
esea
rch
institu
tes a
nd in
du
stry
•
To c
om
pa
re a
nd e
va
luate
th
ese
pro
du
cts
in
coord
ina
ted labora
tory
an
d fie
ld t
rials
•
To d
em
on
str
ate
th
e im
pa
ct
of th
ese im
pro
ved
too
ls o
n d
isea
se c
ontr
ol
GA
EL
ww
w.w
ho.int/le
p/
•
To m
ake a
con
cert
ed a
nd c
oord
inate
d e
ffo
rt t
o a
chie
ve t
he e
limin
atio
n o
f le
pro
sy
as a
pu
blic
he
alth p
rob
lem
fro
m e
very
end
em
ic c
ou
ntr
y, a
t th
e n
atio
nal le
vel b
y 2
005
•
To e
nsure
th
at
all
lepro
sy
patie
nts
, w
here
ver
the
y m
ay
live
, an
d h
ow
eve
r poo
r, h
ave f
ree a
nd e
qu
al
acce
ss
to t
he m
ost
modern
of
treatm
ent
ava
ilab
le
GA
ELF
w
ww
.fila
riasi
s.org
/
•
To r
edu
ce,
inte
rrup
t and
elim
inate
tra
nsm
issi
on
of
lym
pha
tic fila
riasis
•
To
red
uce,
alle
via
te a
nd
pre
ven
t m
orb
idity
(su
fferi
ng
and
dis
ab
ility
) in
affe
cte
d i
nd
ivid
ua
ls t
hro
ugh
th
e u
se o
f A
lbe
nd
azo
le,
pro
vid
e a
dew
orm
ing b
en
efit
to e
ndem
ic p
opu
latio
ns
•
To p
rovid
e s
tre
ngth
enin
g b
enefits
to t
he h
ea
lth
serv
ice
s
GA
IN
ww
w.g
ain
health.o
rg/
•
To s
up
port
foo
d f
ort
ific
atio
n a
nd o
ther
su
sta
inab
le n
utr
itio
n s
tra
teg
ies
in o
rde
r to
sa
ve liv
es a
nd im
pro
ve h
ealth
, pro
ductivity,
and
co
gnitiv
e f
un
ction
.
•
To im
pro
ve th
e m
icro
nu
trie
nt st
atu
s o
f in
div
idu
als
liv
ing in
de
ve
lop
ing
cou
ntr
ies
•
To
supp
ort
develo
pin
g c
ou
ntr
ies
in f
oo
d f
ort
ifica
tion e
ffo
rts,
un
de
rtake
n i
n t
he c
onte
xt
of
bro
ade
r m
icro
nutr
ien
t str
ate
gie
s,
that
will
re
duce
mic
ron
utr
ient
maln
utr
itio
n
in
de
velo
pin
g
co
un
trie
s,
pa
rtic
ula
rly
thro
ug
h
incr
eased
co
nsu
mptio
n
of
mic
ronu
trie
nt-
rich fo
od
s.
GA
TB
DD
w
ww
.tballi
ance.o
rg
•
To a
ccele
rate
th
e d
isco
very
and/o
r de
velo
pm
en
t o
f co
st-
eff
ect
ive n
ew
dru
gs
that:
1.
Sh
ort
en o
r si
mplif
y tr
ea
tmen
t of
TB
, 2
. P
rovid
e e
ffective
tre
atm
ent
of
mu
lti-d
rug-r
esis
tant
TB
, 3.
Imp
rove t
he t
rea
tme
nt
of
late
nt
TB
infe
ction
, an
d 4
. C
an
be m
ade
affo
rda
ble
an
d a
cce
ssib
le in T
B e
nd
em
ic c
oun
trie
s
GA
VI
•
Mis
sio
n: to
protect children of all nations and of all socioeconomic levels against vaccine-preventable diseases
• Improve access to sustainable immunization services
• Expand the use of all existing safe and cost-effective vaccines, and promote delivery of other appropriate
interventions at immunization contacts
• Support the national and international accelerated disease control targets for vaccine-preventable diseases
• Accelerate the development and introduction of new vaccines and technologies
• Accelerate R&D efforts for vaccines needed primarily in developing countries
• Make immunization coverage a centerpiece in international development efforts
Mappin
g G
lobal H
ealth P
art
ners
hip
s
14
DF
ID H
ealth R
esourc
e C
entr
e
GB
C
ww
w.b
usin
essfig
hts
ai
ds.o
rg/
•
Incr
ease
sig
nific
antly
the
num
be
r of
com
pa
nie
s co
mm
itte
d t
o t
ack
ling A
IDS
, a
nd t
o m
ake b
usin
ess a
va
lue
d p
art
ner
in t
he
glo
ba
l eff
ort
s aga
inst
the e
pid
em
ic
•
Imp
lem
entin
g p
reventio
n a
nd c
are
pro
gra
ms a
nd p
olic
ies for
em
plo
yee
s and im
media
te c
om
mu
nitie
s
•
Brin
gin
g b
usin
ess
core
str
ength
s o
f cre
ativity
an
d f
lexib
ility
to
im
pro
ve t
he
re
ach
an
d e
ffe
ctive
ne
ss
of
AID
S p
rogra
ms
•
Lea
ders
hip
an
d a
dvo
cacy
by
bu
sin
ess
le
ade
rs,
lob
byin
g f
or
gre
ate
r actio
n a
nd p
art
ners
hip
s w
ith g
ove
rnm
ents
an
d c
ivil
soci
eties
GC
M
ww
w.g
lobal-
cam
paig
n.o
rg/
•
Rais
e a
ware
ne
ss
and
mo
bili
ze p
olit
ica
l su
pport
fo
r in
cre
ase
d f
und
ing f
or
mic
rob
icid
e r
ese
arc
h,
fem
ale
cond
om
an
d c
erv
ical
barr
ier
meth
od
s
•
Cre
ate
a s
up
po
rtiv
e p
olic
y environ
men
t fo
r th
e t
imely
develo
pm
en
t, in
tro
du
ction
an
d u
se o
f n
ew
pre
ven
tio
n t
ech
no
log
ies
•
En
sure
tha
t a
s sc
ience p
rocee
ds,
the p
ub
lic inte
rest
is p
rote
cted a
nd t
he r
ights
and inte
rests
of
tria
l pa
rtic
ipan
ts,
use
rs,
an
d
com
mu
nitie
s a
re fu
lly r
epre
sen
ted a
nd
respe
cte
d
GC
WA
•
To a
ddre
ss t
he
in
cre
asin
g g
lob
al im
pa
ct
of
AID
S o
n w
om
en
an
d g
irls
•
To h
elp
meet
a s
eri
es o
f a
mbitio
us
inte
rnatio
na
l targ
ets
•
To s
up
port
the
wid
er
glo
ba
l A
IDS
re
spo
nse
•
To im
pro
ve p
reve
ntion f
or
wom
en a
nd
gir
ls
•
To a
ddre
ss s
evere
so
cie
tal and leg
al in
eq
uitie
s w
hic
h c
om
po
un
d th
e im
pa
ct
of
HIV
and
AID
S o
n w
om
en a
nd g
irls
•
To p
revent
HIV
in
fect
ion a
mong
gir
ls a
nd y
ou
ng w
om
en
•
To r
edu
ce v
iole
nce
ag
ain
st
wom
en
•
To p
rote
ct
the p
rop
ert
y and
inh
erita
nce r
ights
of
wom
en a
nd g
irls
•
To e
nsure
equ
al a
cce
ss b
y w
om
en
an
d g
irls
to
care
an
d tre
atm
en
t •
To s
up
port
im
pro
ved c
om
munity-
ba
sed c
are
, w
ith a
sp
ecia
l fo
cus o
n w
om
en
an
d g
irls
•
To p
rom
ote
acce
ss
to n
ew
pre
ven
tion o
ption
s f
or
wom
en,
inclu
din
g m
icro
bic
ides
•
To s
up
port
on-g
oin
g e
ffort
s tow
ard
s u
niv
ers
al e
du
catio
n f
or
girls
GE
T 2
020
ww
w.w
ho.int/pbd/tra
chom
a/p
ress
rel.htm
•
Glo
ba
l elim
ination
of
blin
din
g tra
cho
ma b
y 202
0
•
To
im
ple
me
nt
the
SA
FE
str
ate
gy
con
sis
ting
of
Surg
ery
, A
ntib
iotic t
rea
tmen
t, p
rom
otio
n o
f F
acia
l cle
an
line
ss a
nd
in
itia
tio
n o
f E
nvi
ronm
enta
l cha
nge
s t
o r
edu
ce t
he tra
nsm
issi
on
of
trach
om
a
•
To
co
mb
ine
the
ab
ove
com
po
ne
nts
w
ith
m
edic
al,
beha
vio
ura
l a
nd
en
viro
nm
en
tal
str
ate
gie
s th
rou
gh th
e
targ
eting
of
com
mu
nitie
s
•
To i
nclu
de s
anitary
infr
astr
uctu
re a
nd s
erv
ices,
lifesty
le a
nd
hea
lth r
ela
ted b
eh
avio
ura
l aspe
cts
in a
imin
g a
t a s
usta
ina
ble
and
lon
g lastin
g r
ed
uctio
n o
r elim
inatio
n o
f tr
ach
om
a
GF
AT
M
ww
w.t
heglo
balfund.o
r
•
To f
ina
nce
a d
ram
atic turn
-aro
un
d in t
he fig
ht
aga
inst
AID
S, tu
berc
ulo
sis
an
d m
ala
ria
•
To a
ttra
ct, m
an
ag
e a
nd d
isburs
e a
dd
itio
nal
mon
ies w
ith l
ess
bu
reau
cra
cy
for
recip
ient
co
untr
ies,
allo
win
g m
ore
effe
ctiv
e
Mappin
g G
lobal H
ealth P
art
ners
hip
s
15
DF
ID H
ealth R
esourc
e C
entr
e
g/e
n/
use
of
don
or
resourc
es, an
d few
er
tran
sa
ctio
n c
osts
fo
r a
ll •
To d
ire
ct
fin
an
cia
l re
sourc
es
wh
ere
th
ey
are
nee
de
d m
ost
an
d e
nsu
re th
at th
ey
are
use
d e
ffe
ctively
GF
UN
C
•
to d
eve
lop p
ote
nt,
safe
, ora
lly a
ctive a
nd e
co
nom
ical n
ew
dru
gs
to tre
at A
fric
an t
ryp
ano
so
mia
sis
an
d leis
hm
an
iasi
s
•
To c
arr
y ou
t P
ha
se I
I C
linic
al T
rials
of
the
in
itia
l d
rug
(D
B2
89)
for
Afr
ica
n try
pa
no
som
iasi
s
•
To
syn
the
sis,
scr
ee
n
an
d
de
ve
lop
se
con
d
genera
tion
com
po
und
s
rela
ted
to
D
B2
89
for
the
tre
atm
ent
of
Afr
ica
n
tryp
ano
som
iasi
s
•
To s
ynth
esiz
e,
scr
ee
n a
nd
de
velo
p n
ove
l co
mp
ound
s f
or
the t
reatm
ent
of
leis
hm
an
iasis
. S
tud
ies
by
the c
onsort
ium
ha
ve
alre
ad
y show
n tha
t com
po
unds s
tru
ctura
lly r
ela
ted
to D
B28
9 a
re a
ctive,
both
in v
ivo a
nd in v
itro
, a
gain
st
leis
hm
an
iasis
Glo
bal
Buru
li’s
Ulc
er
Initi
ative
w
ww
.who.int/g
tb-
buru
li/in
itia
tive/in
dex.h
tml
•
To a
dvo
cate
for
Bu
ruli
ulc
er
as
a h
ealth a
nd d
evelo
pm
en
tal pro
ble
m
•
To s
ee
k p
art
ne
rsh
ip for
con
trol a
nd r
ese
arc
h
•
To c
o-o
rdin
ate
glo
ba
l con
tro
l an
d r
ese
arc
h e
ffort
s.
Glo
bal
Part
ners
hip
to
E
limin
ate
R
iver
Blin
dness
ww
w.w
orldba
nk.o
rg/a
fr/
gper/
part
ners
hip
s.ht
m
•
To e
limin
ate
Riv
erb
lindne
ss
as a
pu
blic
hea
lth
pro
ble
m in
all
of A
fric
a,
where
99
% o
f th
e w
orld
’s c
ase
s occur.
N
B T
he G
lob
al
Pa
rtners
hip
is a
n u
mbre
lla t
erm
fo
r th
e O
ncho
cerc
iasi
s C
on
trol
Pro
gra
m (
OC
P)
an
d t
he A
fric
an P
rogra
m f
or
Onch
ocerc
iasi
s C
ontr
ol (A
PO
C).
Th
e O
CP
ra
n f
rom
1974
-200
2 in 1
1 W
est
Afr
ica
n c
ou
ntr
ies.
It h
alte
d t
ransm
issio
n a
nd
virtu
ally
elim
inate
d R
ive
rblin
dn
ess t
hro
ug
hou
t p
art
icip
atin
g c
ou
ntr
ies,
tho
ug
h o
pera
tio
ns c
ontinue
in f
ive S
pe
cia
l In
terv
en
tio
n Z
one
s.
For
curr
ent
op
era
tion
s,
see
AP
OC
abo
ve.
GM
AI
•
To a
ctiva
te m
edia
org
an
iza
tion
s t
o r
ea
ch
the
worl
d’s
peop
le –
esp
ecia
lly y
outh
- w
ith info
rmatio
n a
bout
how
to p
reve
nt
and
tr
eat
HIV
and t
o h
elp
com
ba
t A
IDS
-re
late
d s
tigm
a a
nd
dis
crim
inatio
n
GM
P
ww
w.c
onra
d.o
rg/
•
To s
peed t
he d
evelo
pm
en
t an
d t
est
ing o
f m
icro
bic
ides,
topic
al
app
lication
s co
nta
inin
g c
om
pou
nd
s th
at
dis
ab
le o
r b
lock
age
nts
ca
usin
g s
exua
lly tra
nsm
itte
d infe
ctio
ns
(ST
Is)
•
To a
llow
sys
tem
atic s
cre
en
ing o
f ca
ndid
ate
lea
ds
and
para
llel
testin
g o
f ca
nd
ida
te m
icro
bic
ide
s in
hum
an t
ria
ls i
n o
rder
to
acce
lera
te le
ad-t
ime
fro
m labo
rato
ry t
o th
e m
ark
et
GO
AR
N
ww
w.w
ho.int/csr/
outb
reakne
twork
/en
/
•
To c
ontr
ibute
to
wa
rds
glo
ba
l he
alth s
ecu
rity
•
To c
om
ba
t th
e in
tern
atio
nal spre
ad o
f ou
tbre
aks
•
To e
nsu
re t
ha
t ap
pro
pria
te te
chnic
al a
ssis
tance r
ea
ches a
ffe
cted
sta
tes r
apid
ly
•
To c
ontr
ibute
to long
-term
epid
em
ic p
repa
red
ness a
nd
ca
pa
city
build
ing
GP
EI
ww
w.p
olio
era
dic
atio
n.
org
/
•
Th
e g
oa
l is
to h
ave
inte
rrup
ted t
ransm
issio
n o
f w
ild p
olio
virus b
y en
d-2
00
4 a
nd t
o c
ert
ify
the w
orl
d p
olio
-fre
e in 2
00
8
•
To
con
duct
eff
ective a
nd
hig
h q
ua
lity
su
pple
me
nta
ry im
mu
niz
ation
activiti
es,
inclu
din
g n
ation
al im
mu
nis
atio
n d
ays
and m
op-
up c
am
pa
ign
s t
o inte
rru
pt
wild
po
lioviru
s tra
nsm
issio
n
•
To d
evelo
p a
nd s
ust
ain
ce
rtifi
cation
sta
nd
ard
su
rve
illa
nce
an
d l
abo
rato
ry s
yste
ms
that
can r
apid
ly i
dentify
po
lio-i
nfe
cte
d
Mappin
g G
lobal H
ealth P
art
ners
hip
s
16
DF
ID H
ealth R
esourc
e C
entr
e
are
as
•
To e
nsure
la
bo
rato
ry c
onta
inm
en
t of w
ild p
olio
viru
s st
ock
s •
To d
eve
lop a
con
sensus s
trate
gy
to s
top p
olio
im
mu
nis
atio
n a
fte
r cert
ific
ation o
f e
radic
atio
n
•
To u
se
po
lio e
radic
atio
n t
o s
tren
gth
en a
nd e
xpan
d r
outine im
mun
isation s
erv
ice
s
Mappin
g G
lobal H
ealth P
art
ners
hip
s
17
DF
ID H
ealth R
esourc
e C
entr
e
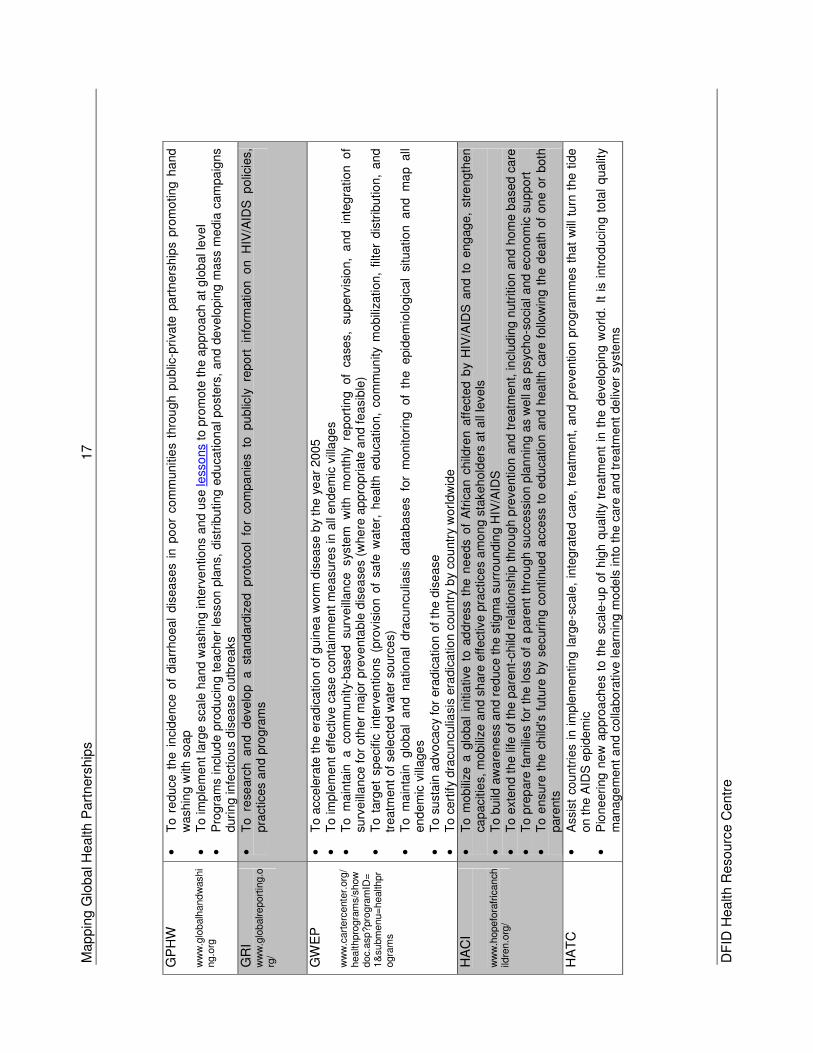
GP
HW
w
ww
.glo
balh
and
washi
ng.o
rg
•
To r
edu
ce t
he
in
cid
ence
of
dia
rrho
ea
l dis
ea
se
s in
po
or
co
mm
unitie
s th
rou
gh p
ub
lic-p
riva
te p
art
ners
hip
s p
rom
oting
ha
nd
w
ashin
g w
ith s
oap
•
To im
ple
me
nt
larg
e s
ca
le h
and w
ashin
g inte
rve
ntion
s a
nd u
se le
sso
ns
to p
rom
ote
th
e a
ppro
ach
at
glo
bal le
ve
l •
Pro
gra
ms inclu
de p
rodu
cin
g t
each
er
less
on
pla
ns,
dis
trib
uting
ed
ucation
al po
ste
rs,
and
de
ve
lopin
g m
ass m
edia
cam
pa
ign
s
duri
ng in
fect
iou
s d
isea
se o
utb
rea
ks
GR
I w
ww
.glo
balreport
ing.o
rg/
•
To re
searc
h a
nd d
eve
lop
a st
and
ard
ize
d pro
toco
l fo
r co
mpa
nie
s to
pu
blic
ly re
po
rt in
form
ation o
n H
IV/A
IDS
p
olic
ies,
pra
ctic
es a
nd p
rogra
ms
GW
EP
w
ww
.cart
erc
ente
r.org
/healthpro
gra
ms/s
how
doc.a
sp?pro
gra
mID
=1&
subm
enu=
health
pr
ogra
ms
•
To a
cce
lera
te t
he e
radic
ation o
f g
uin
ea w
orm
dis
ea
se b
y th
e y
ear
20
05
•
To im
ple
me
nt eff
ect
ive
case
conta
inm
en
t m
easu
res in
all
en
de
mic
vill
age
s
•
To m
ain
tain
a co
mm
unity-
base
d surv
eill
an
ce sys
tem
w
ith m
onth
ly re
port
ing
of
case
s,
sup
erv
isio
n,
and in
teg
ratio
n o
f su
rve
illa
nce
for
oth
er
majo
r pre
ve
nta
ble
dis
ea
ses (
whe
re a
pp
ropri
ate
an
d f
ea
sib
le)
•
To t
arg
et
spe
cific
inte
rven
tion
s (
pro
vis
ion o
f sa
fe w
ate
r, h
ealth e
du
cation,
co
mm
un
ity
mo
bili
zation,
filter
dis
trib
utio
n,
and
tr
eatm
ent
of
sele
cte
d w
ate
r so
urc
es)
•
To m
ain
tain
g
lob
al
an
d n
atio
na
l dra
cu
ncu
liasis
d
ata
ba
ses fo
r m
on
itori
ng
of
the epid
em
iolo
gic
al
situ
atio
n a
nd m
ap all
end
em
ic v
illage
s
•
To s
usta
in a
dvo
cacy
for
era
dic
atio
n o
f th
e d
ise
ase
•
To c
ert
ify
dra
cun
culia
sis
era
dic
atio
n c
oun
try
by
cou
ntr
y w
orl
dw
ide
HA
CI
ww
w.h
opefo
rafr
icanch
ildre
n.o
rg/
•
To m
ob
ilize
a g
loba
l in
itia
tive
to a
ddre
ss
the n
ee
ds o
f A
fric
an c
hild
ren a
ffect
ed b
y H
IV/A
IDS
an
d t
o e
ng
ag
e,
stre
ngth
en
ca
pacitie
s, m
ob
ilize
an
d s
hare
eff
ective p
ractice
s a
mo
ng s
takeh
old
ers
at
all
leve
ls
•
To b
uild
aw
are
ne
ss a
nd r
educe th
e s
tig
ma
surr
ound
ing H
IV/A
IDS
•
To e
xte
nd
th
e life
of
the
pa
rent-
child
re
lation
ship
th
rou
gh p
reve
ntion a
nd t
reatm
en
t, in
clu
din
g n
utr
itio
n a
nd h
om
e b
ased
care
•
To p
rep
are
fa
mili
es
for
the
loss
of
a p
are
nt
thro
ugh
su
cce
ssio
n p
lan
nin
g a
s w
ell
as p
syc
ho
-so
cial and e
cono
mic
su
ppo
rt
•
To e
nsure
the c
hild
's f
utu
re b
y securin
g c
ontinu
ed a
cce
ss
to e
du
catio
n a
nd h
ea
lth c
are
follo
win
g t
he d
eath
of
on
e o
r both
pare
nts
HA
TC
•
Assis
t co
untr
ies i
n i
mp
lem
en
ting l
arg
e-s
cale
, in
tegra
ted c
are
, tr
ea
tme
nt, a
nd
pre
ven
tion
pro
gra
mm
es t
ha
t w
ill t
urn
the t
ide
on t
he A
IDS
ep
ide
mic
•
Pio
ne
eri
ng n
ew
ap
pro
ach
es
to t
he s
cale
-up o
f h
igh
qualit
y tr
eatm
ent
in t
he d
evelo
pin
g w
orld.
It i
s i
ntr
od
ucin
g t
ota
l q
ua
lity
mana
ge
ment
an
d c
olla
bo
rative learn
ing
mo
de
ls in
to t
he c
are
an
d tre
atm
ent
de
live
r sys
tem
s
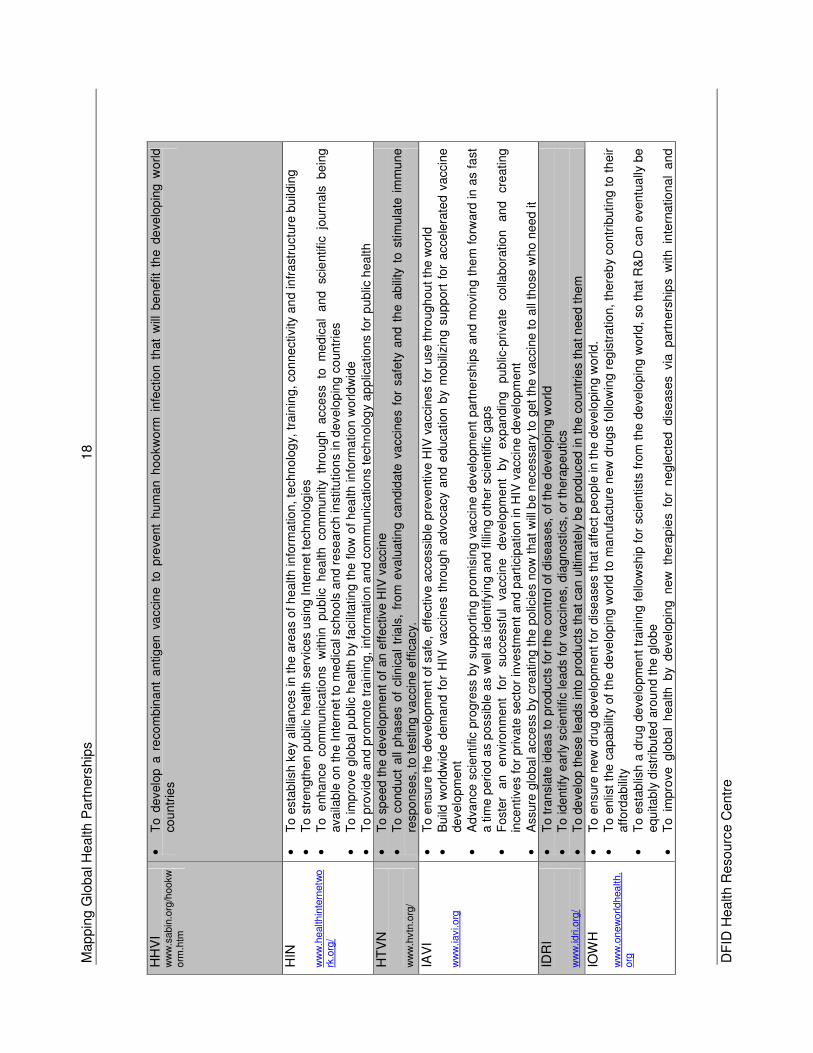
Mappin
g G
lobal H
ealth P
art
ners
hip
s
18
DF
ID H
ealth R
esourc
e C
entr
e
HH
VI
ww
w.s
abin
.org
/hookw
orm
.htm
•
To d
evelo
p a
re
com
bin
ant
antig
en v
acci
ne t
o p
reve
nt
hum
an h
oo
kw
orm
in
fectio
n t
hat
will
be
nefit
the d
eve
lop
ing w
orld
co
untr
ies
HIN
w
ww
.healthin
tern
etw
ork
.org
/
•
To e
sta
blis
h k
ey
alli
an
ces in
the
are
as
of h
ealth in
form
atio
n, te
chn
olo
gy,
tra
inin
g,
con
ne
ctivity
an
d in
fra
stru
ctu
re b
uild
ing
•
To s
tre
ngth
en p
ub
lic h
ea
lth s
erv
ice
s u
sing
Inte
rne
t te
chn
olo
gie
s
•
To e
nha
nce com
mun
icatio
ns
with
in pu
blic
h
ea
lth co
mm
unity
thro
ugh
acce
ss
to m
ed
ical
and
scie
ntif
ic jo
urn
als
b
ein
g
ava
ilab
le o
n th
e In
tern
et to
me
dic
al scho
ols
and r
ese
arc
h in
stitu
tion
s in
develo
pin
g c
ountr
ies
•
To im
pro
ve g
lobal pu
blic
he
alth
by
facili
tating t
he f
low
of hea
lth
in
form
atio
n w
orl
dw
ide
•
To p
rovid
e a
nd
pro
mote
tra
inin
g,
info
rma
tio
n a
nd c
om
mun
icatio
ns
tech
no
log
y a
pplic
atio
ns for
pu
blic
hea
lth
HT
VN
w
ww
.hvtn
.org
/
•
To s
pe
ed
th
e d
eve
lopm
ent
of
an
eff
ective H
IV v
acc
ine
•
To
cond
uct
all
pha
se
s o
f clin
ica
l tr
ials
, fr
om
eva
luatin
g c
and
idate
va
cci
ne
s f
or
safe
ty a
nd
th
e a
bili
ty t
o s
tim
ula
te i
mm
un
e
respo
nse
s, to
te
stin
g v
acci
ne e
ffic
acy.
IAV
I w
ww
.iavi.org
•
To e
nsure
the d
eve
lop
men
t of safe
, eff
ective a
cce
ssi
ble
pre
ventive H
IV v
accin
es f
or
use
thro
ugh
out
the w
orl
d
•
Build
wo
rldw
ide
dem
an
d f
or
HIV
va
ccin
es t
hro
ug
h a
dvo
ca
cy
and
edu
cation b
y m
ob
ilizin
g s
upport
for
acce
lera
ted v
accin
e
develo
pm
en
t •
Ad
van
ce s
cie
ntific p
rogre
ss b
y su
pp
ort
ing p
rom
isin
g v
acci
ne
develo
pm
ent
part
ne
rsh
ips
an
d m
ovin
g t
he
m f
orw
ard
in
as f
ast
a tim
e p
eri
od a
s p
ossib
le a
s w
ell
as
identify
ing a
nd
fill
ing o
the
r sc
ientif
ic g
ap
s •
Foste
r a
n
en
viro
nm
en
t fo
r su
cce
ssfu
l va
ccin
e
develo
pm
ent
by
exp
an
din
g
pu
blic
-pri
vate
colla
bora
tio
n
and
cre
ating
in
centive
s for
private
se
cto
r in
vestm
ent
an
d p
art
icip
atio
n in
HIV
va
ccin
e d
eve
lop
ment
•
Assure
glo
ba
l acce
ss b
y cr
eatin
g t
he p
olic
ies
now
tha
t w
ill b
e n
ece
ssary
to
get
the v
accin
e t
o a
ll th
ose
who n
eed
it
IDR
I w
ww
.idri.o
rg/
•
To t
ran
sla
te ide
as to
pro
du
cts
fo
r th
e c
on
trol of d
isea
ses,
of th
e d
evelo
pin
g w
orld
•
To id
entify
earl
y sci
en
tific
leads for
va
ccin
es,
dia
gn
ostics
, or
thera
peutics
•
To d
eve
lop t
he
se le
ad
s in
to p
rodu
cts
that
can
ulti
mate
ly b
e p
rod
uced in t
he
co
untr
ies th
at n
ee
d t
he
m
IOW
H
ww
w.o
new
orldhealth.
org
•
To e
nsure
new
dru
g d
eve
lopm
en
t fo
r dis
ea
ses
tha
t aff
ect
peo
ple
in th
e d
eve
lopin
g w
orld
. •
To e
nlis
t th
e c
apab
ility
of
the d
eve
lop
ing w
orl
d t
o m
an
ufa
cture
new
dru
gs
follo
win
g r
eg
istr
atio
n,
there
by
co
ntr
ibutin
g t
o t
heir
affo
rda
bili
ty
•
To e
sta
blis
h a
dru
g d
eve
lopm
en
t tr
ain
ing f
ello
wsh
ip f
or
scie
ntists
fro
m t
he d
eve
lopin
g w
orld,
so t
hat
R&
D c
an e
ventu
ally
be
equ
itab
ly d
istr
ibu
ted a
rou
nd t
he
glo
be
•
To
im
pro
ve glo
ba
l h
ea
lth b
y d
eve
lop
ing n
ew
th
era
pie
s fo
r n
egle
cte
d dis
eases via
part
ne
rsh
ips
with in
tern
atio
na
l a
nd
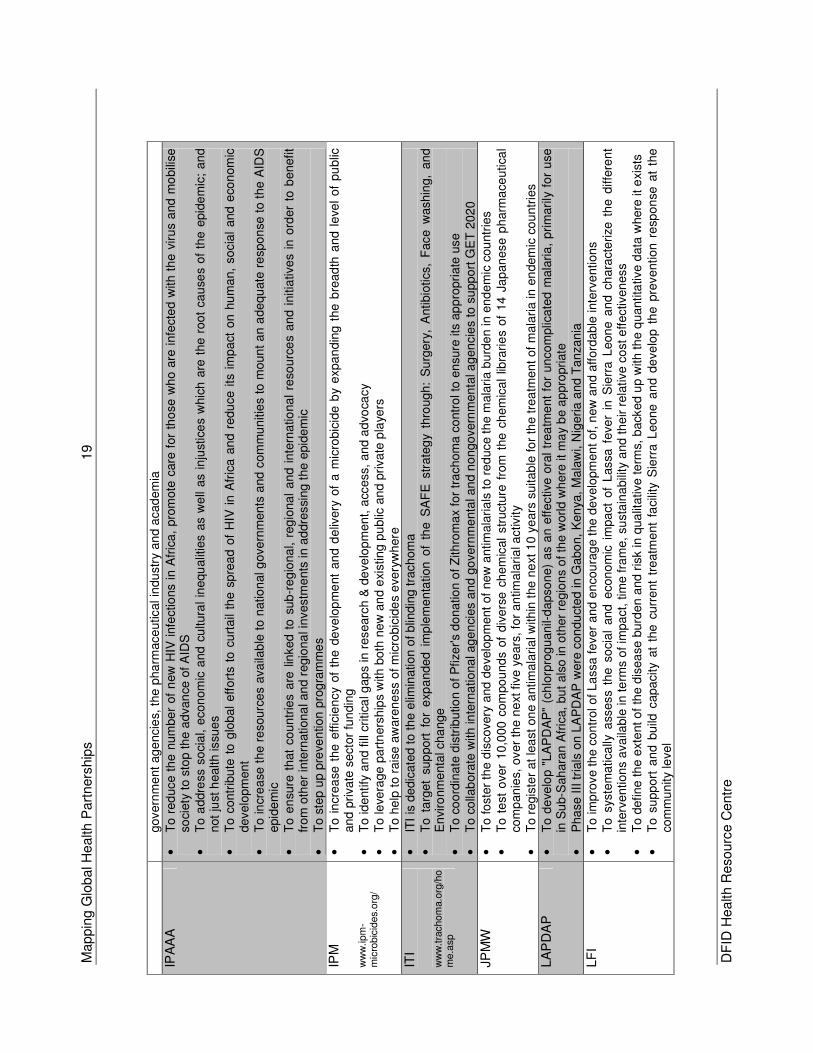
Mappin
g G
lobal H
ealth P
art
ners
hip
s
19
DF
ID H
ealth R
esourc
e C
entr
e
govern
me
nt
ag
encie
s, t
he p
ha
rmace
utical in
du
str
y an
d a
cad
em
ia
IPA
AA
•
To
red
uce t
he
num
be
r of
new
HIV
infe
ctio
ns i
n A
fric
a,
pro
mote
care
for
tho
se w
ho
are
infe
cte
d w
ith
th
e v
iru
s a
nd
mo
bili
se
soci
ety
to s
top th
e a
dvan
ce o
f A
IDS
•
To a
ddre
ss s
ocia
l, e
con
om
ic a
nd c
ultura
l in
equ
alit
ies a
s w
ell
as i
nju
stic
es
whic
h a
re t
he r
oo
t ca
use
s o
f th
e e
pid
em
ic;
an
d
not
just
health issu
es
•
To c
ontr
ibu
te t
o g
lob
al
eff
ort
s t
o c
urt
ail
the s
pre
ad
of
HIV
in A
fric
a a
nd r
edu
ce i
ts i
mp
act
on
hu
ma
n,
so
cia
l and e
con
om
ic
develo
pm
en
t
•
To in
cre
ase
the r
esourc
es a
va
ilab
le t
o n
atio
nal g
ove
rnm
ents
and
com
mu
nitie
s t
o m
oun
t a
n a
de
qu
ate
re
spo
nse
to t
he A
IDS
epid
em
ic
•
To e
nsu
re t
hat
co
un
trie
s a
re l
inked
to
sub
-re
gio
na
l, r
eg
iona
l a
nd i
nte
rna
tiona
l re
sou
rce
s a
nd i
nitia
tive
s in
ord
er
to b
enefit
from
oth
er
inte
rnationa
l an
d r
egio
na
l investm
ents
in a
ddre
ssi
ng t
he e
pid
em
ic
•
To s
tep u
p p
reve
ntion
pro
gra
mm
es
IPM
w
ww
.ipm
-m
icro
bic
ides.
org
/
•
To i
ncre
ase
the
effic
ien
cy
of
the d
eve
lop
me
nt
an
d d
eliv
ery
of
a m
icro
bic
ide b
y e
xpa
nd
ing t
he b
read
th a
nd l
eve
l o
f pu
blic
and
pri
vate
secto
r fu
ndin
g
•
To id
entify
an
d fill
cri
tica
l gap
s in
researc
h &
de
ve
lop
men
t, a
ccess,
an
d a
dvo
cacy
•
To le
vera
ge
pa
rtn
ers
hip
s w
ith b
oth
new
an
d e
xisting
pu
blic
an
d p
riva
te p
laye
rs
•
To h
elp
to
rais
e a
ware
ne
ss o
f m
icro
bic
ide
s e
very
wh
ere
ITI
ww
w.t
rachom
a.o
rg/h
om
e.a
sp
•
ITI
is d
edic
ate
d t
o t
he e
limin
atio
n o
f b
lindin
g tra
chom
a
•
To t
arg
et
sup
port
fo
r e
xpa
nded
im
ple
me
nta
tion
of
the S
AF
E s
trate
gy
thro
ug
h:
Su
rgery
, A
ntibio
tics,
Face w
ashin
g,
an
d
En
viro
nm
enta
l cha
nge
•
To c
oo
rdin
ate
dis
trib
utio
n o
f P
fize
r's d
ona
tio
n o
f Z
ith
rom
ax for
tra
ch
om
a c
ontr
ol to
en
sure
its
ap
pro
pri
ate
use
•
To c
olla
bora
te w
ith
inte
rna
tiona
l ag
en
cies a
nd g
overn
me
nta
l an
d n
ongo
vern
men
tal a
gen
cie
s to
su
pp
ort
GE
T 2
02
0
JP
MW
•
To f
oste
r th
e d
iscovery
and
de
velo
pm
ent
of
new
an
tim
ala
ria
ls t
o r
ed
uce th
e m
ala
ria
bu
rde
n in e
nd
em
ic c
ou
ntr
ies
•
To t
est
over
10,0
00 c
om
po
und
s o
f div
ers
e c
he
mic
al
str
uct
ure
fro
m t
he c
hem
ica
l lib
rari
es
of
14
Ja
pan
ese p
harm
ace
utica
l co
mp
an
ies,
over
the
ne
xt f
ive y
ears
, fo
r an
timala
ria
l activ
ity
•
To r
egis
ter
at
lea
st
on
e a
ntim
ala
ria
l with
in t
he n
ext 1
0 y
ears
suitab
le f
or
the
tre
atm
en
t of
mala
ria in
en
dem
ic c
ou
ntr
ies
LA
PD
AP
•
To
de
velo
p "
LA
PD
AP
" (c
hlo
rpro
gu
anil-
da
pso
ne)
as a
n e
ffective o
ral
trea
tme
nt
for
un
co
mplic
ate
d m
ala
ria
, p
rim
ari
ly f
or
use
in
Su
b-S
ah
ara
n A
fric
a,
bu
t als
o in o
ther
regio
ns o
f th
e w
orld
wh
ere
it m
ay
be a
ppro
priate
•
Pha
se I
II tri
als
on L
AP
DA
P w
ere
con
du
cted
in
Gabo
n,
Ken
ya,
Ma
law
i, N
igeri
a a
nd
Ta
nzan
ia
LF
I •
To im
pro
ve th
e c
on
trol of L
assa f
ever
an
d e
ncou
rag
e t
he d
evelo
pm
en
t of, n
ew
an
d a
fford
ab
le inte
rve
ntion
s
•
To s
yste
ma
tica
lly a
ssess
the s
ocia
l and
econ
om
ic i
mpa
ct
of
Lassa
feve
r in
Sie
rra
Leon
e a
nd c
hara
cte
rize
th
e d
iffe
ren
t in
terv
en
tion
s a
va
ilable
in te
rms
of im
pa
ct, t
ime f
ram
e,
su
sta
ina
bili
ty a
nd t
he
ir r
ela
tive c
ost e
ffectiven
ess
•
To d
efine
th
e e
xte
nt o
f th
e d
isea
se b
urd
en a
nd
ris
k in q
ua
litative t
erm
s, b
ack
ed u
p w
ith th
e q
uantita
tive d
ata
where
it e
xis
ts
•
To
su
pp
ort
an
d b
uild
capa
city
at
the
curr
ent
tre
atm
ent
facili
ty S
ierr
a L
eo
ne
an
d d
eve
lop
th
e p
revention
re
spo
nse
at
the
co
mm
un
ity
level
Mappin
g G
lobal H
ealth P
art
ners
hip
s
20
DF
ID H
ealth R
esourc
e C
entr
e
•
To id
entify
the
mo
st
cost
eff
ect
ive
inte
rven
tio
ns for
the c
on
trol of th
e d
ise
ase
•
To id
entify
part
ners
fo
r d
eve
lopin
g n
ew
inte
rven
tion
s
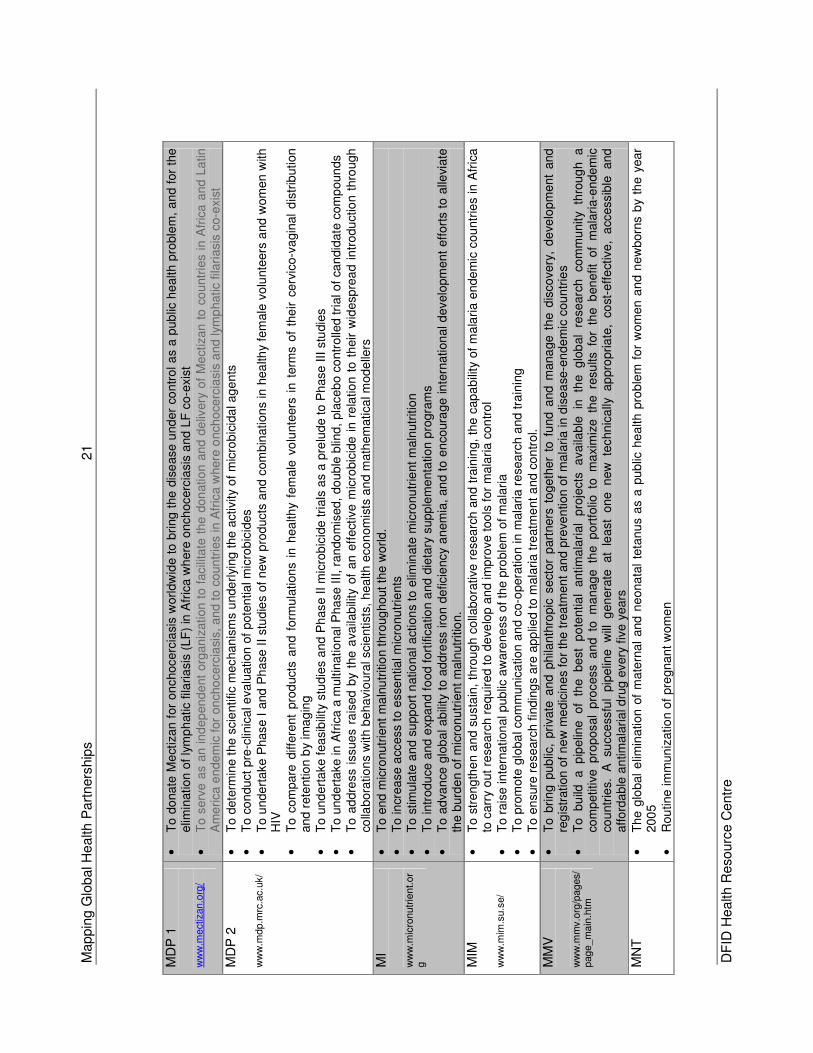
Mappin
g G
lobal H
ealth P
art
ners
hip
s
21
DF
ID H
ealth R
esourc
e C
entr
e
MD
P 1
w
ww
.mectiz
an.o
rg/
•
To d
onate
Me
ctiz
an
for
on
chocerc
iasi
s w
orldw
ide t
o b
ring
the d
ise
ase u
nd
er
con
tro
l a
s a
pub
lic h
ealth p
roble
m,
an
d f
or
the
elim
ination
of
lym
ph
atic f
ilaria
sis
(L
F)
in A
fric
a w
here
onch
ocerc
iasis
and L
F c
o-e
xis
t •
To
serv
e a
s an in
dep
en
de
nt
org
an
ization t
o f
acili
tate
the
don
atio
n a
nd
de
livery
of
Me
ctizan t
o c
ountr
ies in A
fric
a a
nd
La
tin
Am
eri
ca
en
de
mic
for
on
cho
cerc
iasi
s,
an
d t
o c
oun
trie
s in A
fric
a w
here
onch
oce
rcia
sis
and
lym
phatic
fila
riasis
co-e
xis
t
MD
P 2
w
ww
.mdp.m
rc.a
c.u
k/
•
To d
ete
rmin
e t
he s
cie
ntific m
echan
ism
s u
nde
rlyi
ng
the
activity
of
mic
rob
icid
al ag
en
ts
•
To c
on
du
ct
pre
-clin
ica
l eva
lua
tion
of
pote
ntia
l m
icro
bic
ides
•
To u
nde
rta
ke P
hase I
and P
ha
se I
I st
ud
ies
of
ne
w p
rod
ucts
and
com
bin
ation
s in h
ea
lthy
fem
ale
vo
lunte
ers
and w
om
en
with
H
IV
•
To c
om
pare
diff
ere
nt
pro
duct
s a
nd f
orm
ula
tion
s i
n h
ea
lth
y fe
male
vo
lunte
ers
in
term
s o
f th
eir
cerv
ico-v
agin
al
dis
trib
ution
and
rete
ntio
n b
y im
ag
ing
•
To u
nd
ert
ake f
ea
sib
ility
stu
die
s a
nd
Ph
ase II
mic
rob
icid
e tri
als
as a
pre
lud
e to
Ph
ase
III
stu
die
s
•
To u
nd
ert
ake in A
fric
a a
multin
atio
nal P
ha
se III
, ra
ndo
mis
ed,
do
ub
le b
lind
, pla
ceb
o c
ontr
olle
d tri
al o
f ca
ndid
ate
com
poun
ds
•
To a
ddre
ss
issue
s r
ais
ed b
y th
e a
vaila
bili
ty o
f an e
ffect
ive
mic
robic
ide
in r
ela
tio
n t
o t
heir w
idesp
rea
d i
ntr
odu
ctio
n t
hro
ugh
co
llabora
tio
ns
with b
eha
vio
ura
l scie
ntist
s, h
ea
lth e
co
nom
ists
an
d m
ath
em
atica
l mod
elle
rs
MI
ww
w.m
icro
nutr
ient.
or
g
•
To e
nd
mic
ronutr
ient
ma
lnu
triti
on thro
ug
ho
ut
the
worl
d.
•
To in
crea
se
acc
ess t
o e
sse
ntia
l m
icro
nu
trie
nts
•
To s
tim
ula
te a
nd s
upp
ort
natio
na
l a
ctio
ns to
elim
inate
mic
ronu
trie
nt m
aln
utr
itio
n
•
To intr
odu
ce a
nd
expa
nd
fo
od f
ort
ifica
tion a
nd d
ieta
ry s
upp
lem
enta
tion
pro
gra
ms
•
To a
dva
nce
glo
ba
l a
bili
ty t
o a
ddre
ss iro
n d
eficie
ncy
an
em
ia,
an
d t
o e
ncoura
ge in
tern
ation
al d
evelo
pm
en
t eff
ort
s t
o a
llevi
ate
th
e b
urd
en o
f m
icro
nutr
ien
t m
aln
utr
itio
n.
MIM
w
ww
.mim
.su.s
e/
•
To s
tren
gth
en a
nd s
usta
in,
thro
ug
h c
olla
bo
rative
re
sea
rch
an
d t
rain
ing,
the c
ap
ab
ility
of
ma
lari
a e
nde
mic
cou
ntr
ies in
Afr
ica
to
carr
y o
ut
researc
h r
equ
ired t
o d
eve
lop
an
d im
pro
ve t
oo
ls f
or
ma
lari
a c
on
tro
l •
To r
ais
e in
tern
ation
al pub
lic a
ware
ne
ss
of th
e p
roble
m o
f m
ala
ria
•
To p
rom
ote
glo
ba
l com
mun
ica
tion
an
d c
o-o
pera
tio
n in m
ala
ria
re
sea
rch
and tra
inin
g
•
To e
nsure
re
searc
h fin
din
gs a
re a
pp
lied t
o m
ala
ria t
reatm
ent
and c
on
trol.
MM
V
ww
w.m
mv.o
rg/p
ages/
page_m
ain
.htm
•
To b
rin
g p
ub
lic,
pri
vate
an
d p
hila
nth
ropic
sect
or
part
ners
to
geth
er
to f
und
and m
ana
ge t
he d
isco
very
, d
eve
lop
men
t and
re
gis
tration o
f n
ew
me
dic
ine
s fo
r th
e tre
atm
en
t an
d p
reve
ntion
of
ma
laria in d
ise
ase
-en
de
mic
cou
ntr
ies
•
To
b
uild
a p
ipelin
e o
f th
e
be
st
po
tentia
l antim
ala
rial
pro
jects
a
vaila
ble
in
th
e g
lob
al
researc
h
com
mu
nity
thro
ug
h
a
com
petitive
pro
posal
pro
cess a
nd to
m
anag
e th
e p
ort
folio
to
m
axim
ize
th
e re
su
lts fo
r th
e b
en
efit
of
mala
ria-e
nde
mic
co
untr
ies.
A su
cce
ssfu
l pip
elin
e w
ill g
en
era
te at
lea
st
one
n
ew
te
chn
ica
lly a
ppro
pria
te,
co
st-e
ffe
ctiv
e,
acc
essib
le and
affo
rda
ble
an
tim
ala
ria
l dru
g e
very
fiv
e y
ears
MN
T
•
Th
e g
lobal
elim
ina
tion
of
mate
rna
l and
ne
ona
tal
teta
nu
s a
s a
pub
lic h
ea
lth p
rob
lem
fo
r w
om
en
an
d n
ew
born
s b
y th
e y
ear
200
5
•
Rou
tine
im
mun
izatio
n o
f pre
gna
nt w
om
en
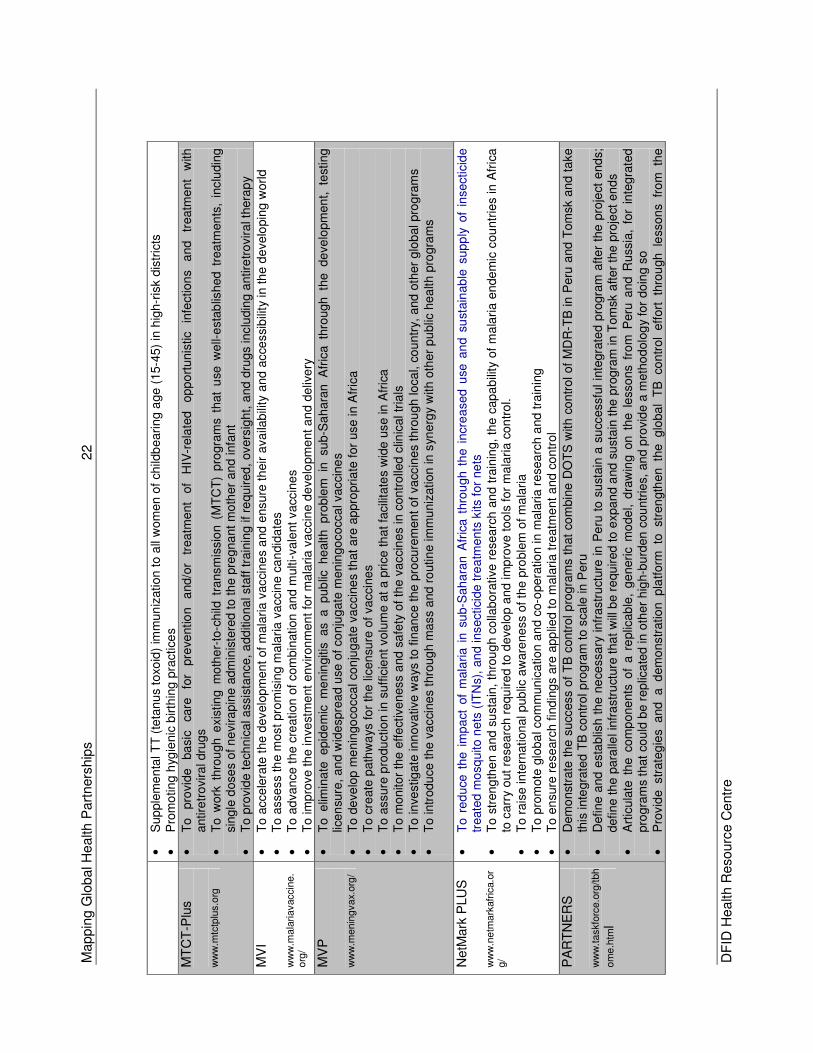
Mappin
g G
lobal H
ealth P
art
ners
hip
s
22
DF
ID H
ealth R
esourc
e C
entr
e
•
Sup
ple
me
nta
l T
T (
teta
nu
s to
xoid
) im
mun
ization t
o a
ll w
om
en
of
child
beari
ng a
ge (
15-4
5)
in h
igh-r
isk d
istr
icts
•
Pro
mo
tin
g h
ygie
nic
birth
ing
pra
ctice
s
MT
CT
-Plu
s
ww
w.m
tctp
lus.o
rg
•
To
pro
vid
e
ba
sic
ca
re
for
pre
ventio
n
and/o
r tr
ea
tment
of
HIV
-rela
ted
op
po
rtunis
tic
infe
ction
s
and
tr
eatm
ent
with
antire
tro
vira
l dru
gs
•
To
work
thro
ugh
exis
tin
g m
oth
er-
to-c
hild
tra
nsm
issio
n (
MT
CT
) p
rogra
ms
that
use
we
ll-e
sta
blis
hed
tre
atm
en
ts,
inclu
din
g
sing
le d
ose
s of n
evira
pin
e a
dm
inis
tere
d t
o t
he p
regna
nt
mo
ther
and infa
nt
•
To p
rovid
e t
ech
nic
al a
ssis
tance, a
dd
itio
na
l sta
ff tra
inin
g if re
qu
ired
, overs
igh
t, a
nd
dru
gs inclu
din
g a
ntire
tro
vir
al t
hera
py
MV
I
ww
w.m
ala
riavacci
ne.
org
/
•
To a
cce
lera
te t
he d
evelo
pm
en
t of
mala
ria v
acci
ne
s a
nd e
nsure
th
eir
ava
ilab
ility
and a
cce
ssi
bili
ty in th
e d
evelo
pin
g w
orl
d
•
To a
sse
ss
the m
ost pro
mis
ing m
ala
ria
va
ccin
e c
an
did
ate
s
•
To a
dvan
ce
th
e c
reation o
f com
bin
ation
an
d m
ulti-va
lent vaccin
es
•
To im
pro
ve th
e in
ve
stm
ent
environ
men
t fo
r m
ala
ria
va
ccin
e d
eve
lopm
ent a
nd d
eliv
ery
MV
P
ww
w.m
enin
gvax.
org
/
•
To e
limin
ate
epid
em
ic m
en
ingitis
as a
p
ub
lic h
ealth
pro
ble
m in
su
b-S
ah
ara
n A
fric
a th
rough
th
e de
ve
lopm
en
t, te
stin
g
licen
sure
, a
nd w
ide
spre
ad u
se o
f co
nju
gate
men
ingo
cocca
l vaccin
es
•
To d
eve
lop m
enin
go
cocca
l co
nju
gate
va
ccin
es
that
are
appro
pria
te f
or
use
in A
fric
a
•
To c
reate
path
wa
ys f
or
the
lic
en
sure
of
va
ccin
es
•
To a
ssure
pro
du
ctio
n in
suff
icie
nt
volu
me a
t a p
rice
th
at fa
cili
tate
s w
ide u
se in
Afr
ica
•
To m
onito
r th
e e
ffe
ctiv
en
ess
and s
afe
ty o
f th
e v
acci
ne
s in
contr
olle
d c
linic
al tr
ials
•
To in
vestig
ate
inn
ova
tive w
ays
to
fin
an
ce t
he
pro
cure
men
t of
va
ccin
es t
hro
ugh lo
ca
l, co
untr
y, a
nd
oth
er
glo
bal pro
gra
ms
•
To intr
odu
ce t
he v
acci
ne
s t
hro
ug
h m
ass
and
ro
utin
e im
mu
niz
ation
in s
yne
rgy
with o
ther
pu
blic
he
alth p
rogra
ms
NetM
ark
PLU
S
ww
w.n
etm
ark
afr
ica.o
rg/
•
To r
ed
uce
the
im
pa
ct o
f m
ala
ria i
n s
ub-S
ah
ara
n A
fric
a t
hro
ugh t
he i
ncre
ased
use
an
d s
ust
ain
ab
le s
up
ply
of
insecticid
e
treate
d m
osq
uito
ne
ts (
ITN
s),
an
d insectici
de
tre
atm
en
ts k
its f
or
ne
ts
•
To s
tren
gth
en a
nd s
usta
in,
thro
ug
h c
olla
bo
rative
re
sea
rch
an
d t
rain
ing,
the c
ap
ab
ility
of
ma
lari
a e
nde
mic
cou
ntr
ies in
Afr
ica
to
carr
y o
ut
researc
h r
equ
ired t
o d
eve
lop
an
d im
pro
ve t
oo
ls f
or
ma
lari
a c
on
tro
l. •
To r
ais
e in
tern
ation
al pub
lic a
ware
ne
ss
of th
e p
roble
m o
f m
ala
ria
•
To p
rom
ote
glo
ba
l com
mun
ica
tion
an
d c
o-o
pera
tio
n in m
ala
ria
re
sea
rch
and tra
inin
g
•
To e
nsure
re
searc
h fin
din
gs a
re a
pp
lied t
o m
ala
ria t
reatm
ent
and c
on
trol
PA
RT
NE
RS
w
ww
.taskfo
rce.o
rg/tbh
om
e.h
tml
•
Dem
onst
rate
th
e s
ucc
ess
of
TB
contr
ol p
rog
ram
s t
hat
com
bin
e D
OT
S w
ith c
on
trol of
MD
R-T
B in
Peru
and
Tom
sk a
nd t
ake
this
inte
gra
ted T
B c
ontr
ol p
rogra
m t
o s
cale
in
Peru
•
Define a
nd
esta
blis
h t
he
ne
cessa
ry infr
astr
uct
ure
in P
eru
to s
ust
ain
a s
ucc
essfu
l in
tegra
ted p
rogra
m a
fter
the
pro
ject
end
s;
define t
he p
ara
llel in
fra
str
uct
ure
tha
t w
ill b
e r
equ
ired t
o e
xpa
nd a
nd s
usta
in t
he
pro
gra
m in T
om
sk a
fter
the p
roje
ct e
nd
s •
Art
icu
late
th
e c
om
pone
nts
of
a r
eplic
ab
le,
ge
neri
c m
ode
l, d
raw
ing o
n t
he l
esso
ns f
rom
Peru
and
Russia
, fo
r in
teg
rate
d
pro
gra
ms t
hat
cou
ld b
e r
ep
lica
ted
in o
ther
hig
h-b
urd
en
cou
ntr
ies,
an
d p
rovid
e a
meth
od
olo
gy
for
do
ing s
o
•
Pro
vid
e str
ate
gie
s a
nd
a d
em
onstr
atio
n pla
tform
to
st
ren
gth
en th
e g
loba
l T
B co
ntr
ol
eff
ort
th
rou
gh le
sson
s fr
om
th
e
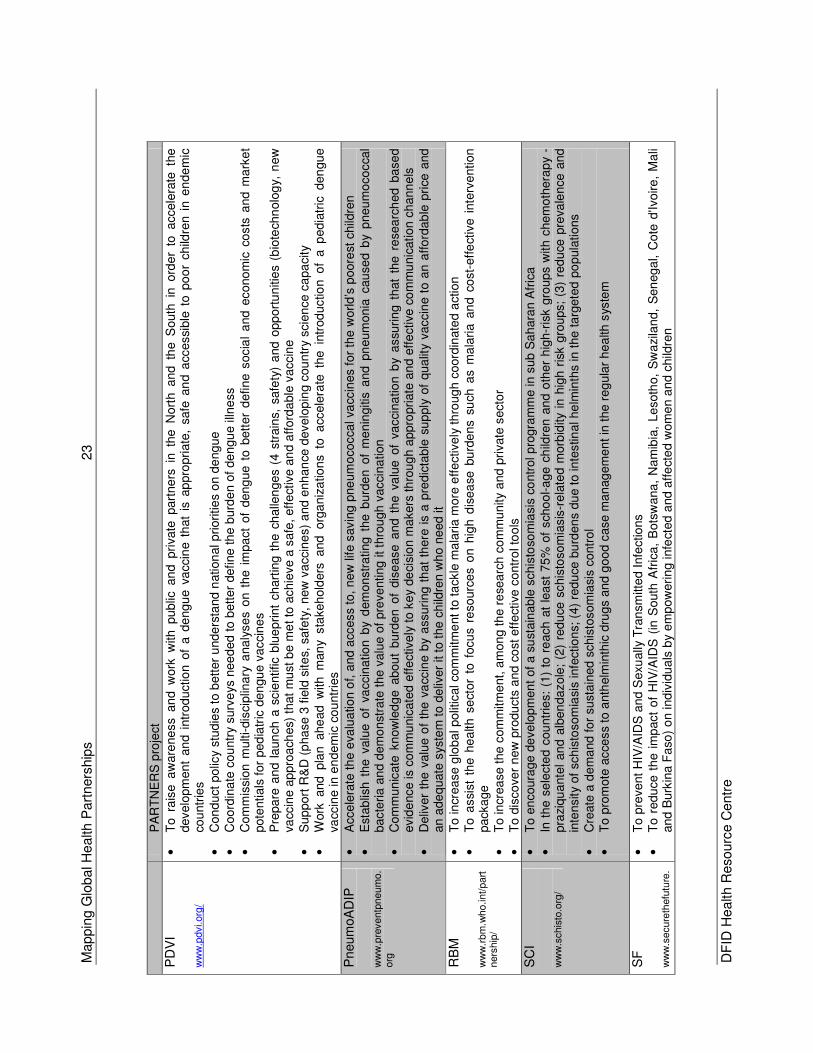
Mappin
g G
lobal H
ealth P
art
ners
hip
s
23
DF
ID H
ealth R
esourc
e C
entr
e
PA
RT
NE
RS
pro
ject
PD
VI
ww
w.p
dvi.org
/
•
To ra
ise a
ware
ne
ss
an
d w
ork
with public
an
d p
rivate
part
ne
rs in
th
e N
ort
h and th
e S
outh
in
ord
er
to accele
rate
the
develo
pm
en
t an
d i
ntr
od
uctio
n o
f a
de
ng
ue v
accin
e t
hat
is a
ppro
pri
ate
, safe
an
d a
ccessi
ble
to
po
or
ch
ildre
n i
n e
nde
mic
co
untr
ies
•
Con
duct
po
licy
stu
die
s t
o b
ett
er
unde
rsta
nd
nation
al p
rioritie
s o
n d
eng
ue
•
Coo
rdin
ate
cou
ntr
y surv
eys
nee
ded t
o b
ett
er
define
th
e b
urd
en o
f de
ngu
e illn
ess
•
Com
mis
sio
n m
ulti-dis
ciplin
ary
ana
lyse
s o
n t
he i
mpa
ct
of
den
gue
to b
ett
er
defin
e s
ocia
l a
nd e
cono
mic
co
sts
and
ma
rke
t pote
ntials
for
ped
iatr
ic d
en
gu
e v
acci
ne
s •
Pre
pa
re a
nd l
aun
ch a
scie
ntific b
lue
ch
art
ing
th
e c
halle
nge
s (
4 s
train
s,
safe
ty)
and o
pp
ort
un
itie
s (
bio
tech
nolo
gy,
new
va
ccin
e a
ppro
ach
es)
that
mu
st b
e m
et to
achie
ve a
safe
, eff
ect
ive
an
d a
fford
able
va
ccin
e
•
Sup
port
R&
D (
pha
se 3
fie
ld s
ite
s, s
afe
ty,
new
va
ccin
es)
and e
nh
an
ce d
evelo
pin
g c
ou
ntr
y scie
nce c
apa
city
•
Work
and pla
n ahe
ad w
ith
m
an
y sta
keh
old
ers
a
nd
org
aniz
atio
ns to
a
ccele
rate
th
e in
trod
uctio
n o
f a p
edia
tric
den
gu
e
vacc
ine in
en
de
mic
co
untr
ies
Pneum
oA
DIP
w
ww
.pre
ventp
neum
o.
org
•
Acce
lera
te t
he e
valu
atio
n o
f, a
nd a
ccess
to, n
ew
life
savin
g p
ne
um
ococca
l va
ccin
es f
or
the
world
’s p
oore
st c
hild
ren
•
Est
ab
lish
the
valu
e o
f va
ccin
atio
n b
y d
em
on
str
ating
the
burd
en o
f m
en
ingitis
and p
neum
on
ia c
au
se
d b
y p
neu
mo
co
cca
l bacte
ria
an
d d
em
on
stra
te t
he v
alu
e o
f pre
ve
nting it th
rou
gh
vacci
na
tion
•
Com
mun
icate
kn
ow
led
ge a
bou
t b
urd
en
of
dis
ease a
nd t
he v
alu
e o
f va
cci
na
tio
n b
y a
ssu
rin
g t
hat
the
re
sea
rch
ed b
ase
d
evid
ence is c
om
mu
nic
ate
d e
ffe
ctive
ly t
o k
ey
de
cisio
n m
akers
th
rou
gh a
ppro
priate
an
d e
ffe
ctive
co
mm
unic
ation c
hann
els
•
Deliv
er
the
valu
e o
f th
e v
acc
ine b
y a
ssuri
ng t
hat
there
is
a p
red
icta
ble
su
pply
of
qua
lity
vaccin
e t
o a
n a
ffo
rdab
le p
rice
and
an a
de
quate
sys
tem
to d
eliv
er
it t
o t
he c
hild
ren
wh
o n
eed it
RB
M
ww
w.r
bm
.who.int/part
ners
hip
/
•
To in
crea
se
glo
ba
l polit
ical co
mm
itm
ent to
ta
ckle
ma
lari
a m
ore
effe
ctive
ly th
roug
h c
oord
inate
d a
ction
•
To a
ssi
st
the h
ea
lth s
ect
or
to f
ocu
s re
so
urc
es o
n h
igh
dis
ea
se b
urd
en
s su
ch a
s m
ala
ria a
nd c
ost-
eff
ect
ive i
nte
rve
ntion
packa
ge
•
To in
crea
se
the
com
mitm
ent, a
mon
g th
e r
ese
arc
h c
om
mu
nity
and p
rivate
secto
r •
To d
isco
ver
new
pro
du
cts
and c
ost eff
ect
ive
co
ntr
ol to
ols
SC
I w
ww
.schis
to.o
rg/
•
To e
ncoura
ge d
eve
lop
men
t of a s
ust
ain
ab
le s
chis
toso
mia
sis
co
ntr
ol p
rogra
mm
e in
sub S
ah
ara
n A
fric
a
•
In t
he s
ele
cte
d c
ou
ntr
ies:
(1)
to r
each a
t le
ast
75
% o
f sch
oo
l-a
ge
ch
ildre
n a
nd o
ther
hig
h-r
isk g
roup
s w
ith c
hem
oth
era
py
- pra
ziqu
ante
l an
d a
lben
da
zole
; (2
) re
du
ce s
chis
toso
mia
sis
-re
late
d m
orb
idity
in h
igh r
isk g
roups;
(3)
red
uce
pre
vale
nce a
nd
in
tensity
of
sch
isto
som
iasi
s in
fectio
ns;
(4)
red
uce
bu
rden
s d
ue t
o in
testin
al he
lmin
ths in
the t
arg
ete
d p
op
ula
tions
•
Cre
ate
a d
em
and f
or
susta
ined s
chis
tosom
iasi
s c
ontr
ol
•
To p
rom
ote
acce
ss
to a
nth
elm
inth
ic d
rug
s a
nd g
oo
d c
ase
ma
nag
em
en
t in
the
re
gula
r h
ea
lth s
yste
m
SF
w
ww
.secure
thefu
ture
.
•
To p
revent
HIV
/AID
S a
nd
Sexu
ally
Tra
nsm
itte
d I
nfe
ctio
ns
•
To
redu
ce
th
e i
mp
act
of
HIV
/AID
S (
in S
outh
Afr
ica
, B
ots
wana
, N
am
ibia
, Le
soth
o,
Sw
azi
lan
d,
Sen
ega
l, C
ote
d'Iv
oire
, M
ali
and
Burk
ina F
aso
) o
n ind
ivid
ua
ls b
y e
mp
ow
eri
ng infe
cted a
nd a
ffe
cte
d w
om
en
an
d c
hild
ren
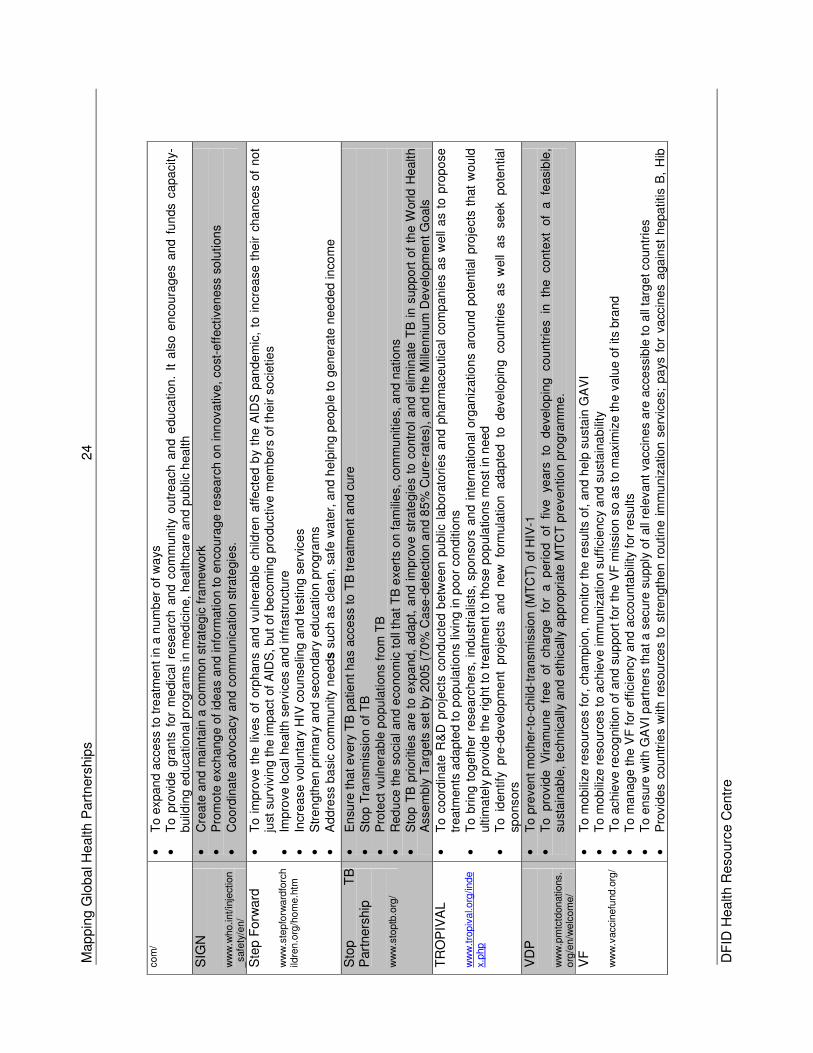
Mappin
g G
lobal H
ealth P
art
ners
hip
s
24
DF
ID H
ealth R
esourc
e C
entr
e
com
/ •
To e
xp
an
d a
cce
ss t
o tre
atm
en
t in
a n
um
ber
of
wa
ys
•
To
pro
vide
gra
nts
for
me
dic
al
rese
arc
h a
nd
com
mun
ity
ou
trea
ch
an
d e
du
cation
. It a
lso e
ncoura
ge
s a
nd
fu
nds c
apa
city-
build
ing
ed
uca
tion
al p
rogra
ms
in m
ed
icin
e,
hea
lth
care
and
pu
blic
hea
lth
SIG
N
ww
w.w
ho.int/in
ject
ion
_safe
ty/e
n/
•
Cre
ate
and m
ain
tain
a c
om
mon s
trate
gic
fra
me
work
•
Pro
mo
te e
xch
ang
e o
f id
ea
s a
nd info
rmatio
n to
en
cou
rage
re
sea
rch
on inn
ova
tive
, co
st-e
ffect
ive
ness s
olu
tion
s
•
Coo
rdin
ate
advocacy
and c
om
mun
ica
tio
n s
trate
gie
s.
Ste
p F
orw
ard
w
ww
.ste
pfo
rward
forc
hild
ren.o
rg/h
om
e.h
tm
•
To
im
pro
ve t
he
liv
es o
f orp
han
s a
nd v
uln
era
ble
ch
ildre
n a
ffe
cte
d b
y th
e A
IDS
pand
em
ic,
to i
ncre
ase
the
ir c
ha
nce
s o
f no
t ju
st s
urv
ivin
g th
e im
pa
ct
of
AID
S, b
ut of
be
com
ing
pro
ductive m
em
bers
of th
eir s
ocie
tie
s •
Imp
rove lo
cal he
alth s
erv
ices
and
infr
ast
ructu
re
•
Incr
ease
volu
nta
ry H
IV c
ou
nse
ling a
nd t
est
ing s
erv
ice
s •
Str
en
gth
en p
rim
ary
and
se
con
dary
ed
ucation p
rog
ram
s
•
Addre
ss b
asic
com
mu
nity
needs
such
as c
lean
, sa
fe w
ate
r, a
nd
help
ing p
eop
le t
o g
en
era
te n
ee
ded in
com
e
Sto
p
TB
P
art
ners
hip
w
ww
.sto
ptb
.org
/
•
En
sure
tha
t every
TB
patie
nt ha
s acce
ss
to T
B tre
atm
en
t a
nd
cure
•
Sto
p T
ran
smis
sion
of
TB
•
Pro
tect
vu
lnera
ble
po
pu
lations fro
m T
B
•
Red
uce
the s
ocia
l an
d e
co
nom
ic t
oll
tha
t T
B e
xert
s o
n f
am
ilie
s,
com
mu
nitie
s, a
nd
nation
s
•
Sto
p T
B p
riori
tie
s a
re t
o e
xpa
nd
, a
da
pt,
an
d i
mpro
ve s
trate
gie
s t
o c
ontr
ol a
nd e
limin
ate
TB
in
supp
ort
of
the W
orld H
ealth
Asse
mb
ly T
arg
ets
set
by
2005
(7
0%
Ca
se-d
ete
ction
an
d 8
5%
Cu
re-r
ate
s),
an
d th
e M
ille
nniu
m D
evelo
pm
en
t G
oals
TR
OP
IVA
L
ww
w.t
ropiv
al.o
rg/inde
x.php
•
To
coord
inate
R&
D p
roje
cts
con
du
cte
d b
etw
een
pu
blic
lab
ora
tori
es a
nd p
harm
ace
utica
l co
mp
an
ies a
s w
ell
as t
o p
rop
ose
treatm
ents
ada
pte
d t
o p
op
ula
tio
ns
livin
g in p
oo
r con
ditio
ns
•
To b
rin
g t
og
eth
er
rese
arc
hers
, in
du
str
ialis
ts,
spon
sors
an
d i
nte
rnation
al
org
an
izatio
ns
aro
und p
ote
ntial
pro
jects
that
wou
ld
ultim
ate
ly p
rovid
e the
rig
ht to
tre
atm
en
t to
tho
se p
op
ula
tion
s m
ost
in n
eed
•
To id
en
tify
pre
-de
velo
pm
ent
pro
ject
s an
d new
fo
rmula
tio
n ada
pte
d to
de
ve
lop
ing co
untr
ies a
s w
ell
as seek po
ten
tial
spo
nsors
VD
P
ww
w.p
mtc
tdonations.
org
/en/w
elc
om
e/
•
To p
revent
mo
the
r-to
-child
-tra
nsm
issi
on
(M
TC
T)
of H
IV-1
•
To p
rovid
e V
iram
un
e fr
ee
of
ch
arg
e fo
r a
p
eri
od o
f five
ye
ars
to
de
velo
pin
g cou
ntr
ies
in th
e conte
xt
of
a fe
asib
le,
sust
ain
able
, te
chn
ica
lly a
nd
eth
ically
app
ropri
ate
MT
CT
pre
ven
tion
pro
gra
mm
e.
VF
w
ww
.vacc
inefu
nd.o
rg/
•
To m
obili
ze r
eso
urc
es f
or,
ch
am
pio
n,
mo
nito
r th
e r
esu
lts
of, a
nd
he
lp s
usta
in G
AV
I
•
To m
obili
ze r
eso
urc
es t
o a
chie
ve im
mun
ization
suff
icie
ncy
and s
ust
ain
ab
ility
•
To a
ch
ieve r
eco
gnitio
n o
f a
nd s
up
port
fo
r th
e V
F m
issio
n s
o a
s to
maxim
ize th
e v
alu
e o
f its
bra
nd
•
To m
anag
e th
e V
F f
or
eff
icie
ncy
and a
cco
unta
bili
ty f
or
resu
lts
•
To e
nsure
with G
AV
I p
art
ners
th
at a
secure
sup
ply
of
all
rele
vant
va
cci
nes a
re a
cce
ssib
le t
o a
ll ta
rge
t coun
trie
s
•
Pro
vid
es
cou
ntr
ies
with
resourc
es t
o s
tren
gth
en r
outin
e i
mm
un
izatio
n s
erv
ice
s;
pa
ys f
or
va
ccin
es a
ga
inst
hepa
titis
B,
Hib
Mappin
g G
lobal H
ealth P
art
ners
hip
s
25
DF
ID H
ealth R
esourc
e C
entr
e
dis
ea
se a
nd
ye
llow
fe
ver,
and s
afe
in
jection m
ate
ria
ls
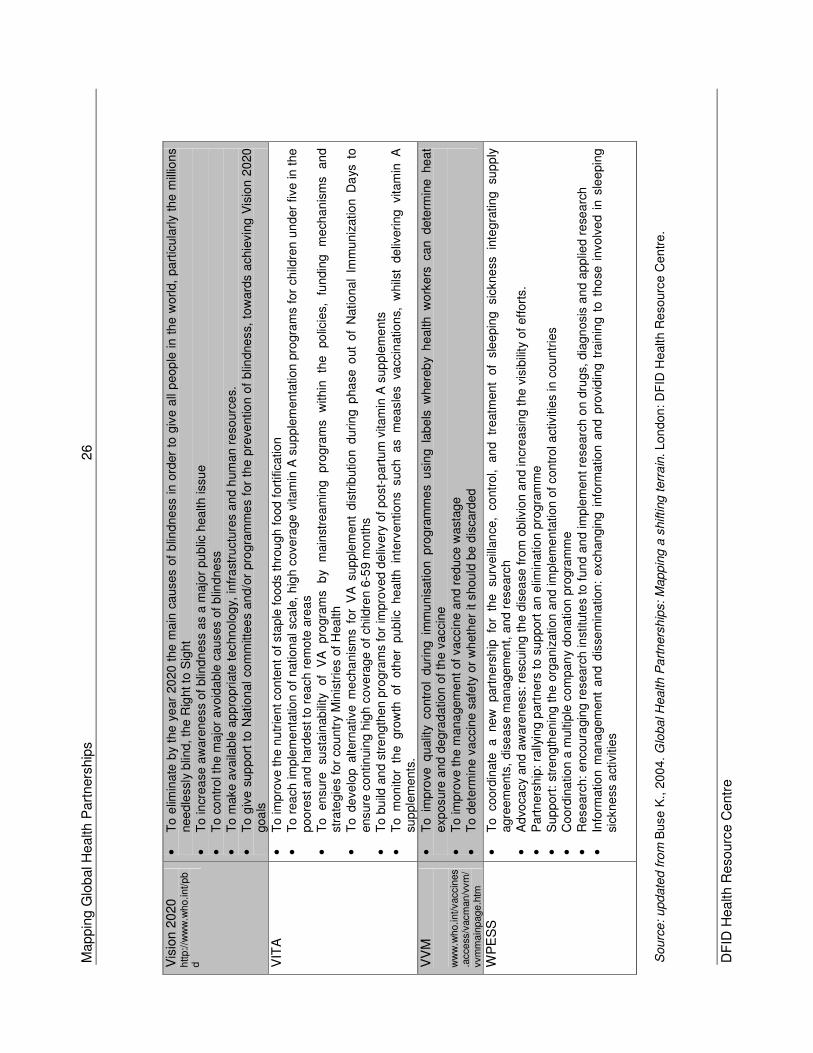
Mappin
g G
lobal H
ealth P
art
ners
hip
s
26
DF
ID H
ealth R
esourc
e C
entr
e
Vis
ion
2020
http://w
ww
.who.int/pb
d
•
To
elim
ina
te b
y th
e y
ear
20
20 t
he
ma
in c
auses o
f b
lind
ne
ss in
ord
er
to g
ive a
ll p
eop
le in
th
e w
orld,
pa
rtic
ula
rly
the
mill
ion
s
nee
dle
ssly
blin
d,
the
Rig
ht to
Sig
ht
•
To in
crea
se
aw
are
ne
ss
of
blin
dn
ess
as a
majo
r pu
blic
hea
lth issu
e
•
To c
on
tro
l th
e m
ajo
r avoid
able
ca
uses o
f b
lind
ne
ss
•
To m
ake a
vaila
ble
ap
pro
pri
ate
techno
log
y, infr
ast
ructu
res a
nd h
um
an r
eso
urc
es.
•
To
giv
e s
up
port
to N
ation
al co
mm
itte
es
and/o
r pro
gra
mm
es f
or
the p
reve
ntio
n o
f b
lindne
ss,
tow
ard
s a
chie
vin
g V
isio
n 2
020
goa
ls
VIT
A
•
To im
pro
ve th
e n
utr
ient
con
tent
of sta
ple
foo
ds t
hro
ugh
food
fort
ific
atio
n
•
To
rea
ch im
ple
me
nta
tio
n o
f nation
al sca
le,
hig
h c
ove
rage
vitam
in A
su
pp
lem
en
tation p
rogra
ms f
or
ch
ildre
n u
nder
five in
the
poo
rest a
nd
ha
rde
st
to r
each r
em
ote
are
as
•
To
en
sure
su
sta
inab
ility
of
VA
pro
gra
ms
by
main
stre
am
ing
pro
gra
ms
with
in
the
po
licie
s,
fundin
g
me
cha
nis
ms
an
d
stra
teg
ies
for
cou
ntr
y M
inis
trie
s o
f H
ea
lth
•
To d
eve
lop a
ltern
ative m
ech
anis
ms f
or
VA
supp
lem
en
t d
istr
ibutio
n d
urin
g p
ha
se o
ut
of
Natio
na
l Im
mu
niz
ation
Da
ys t
o
ensure
contin
uin
g h
igh
cove
rage
of
child
ren 6
-59 m
on
ths
•
To b
uild
an
d s
tre
ng
the
n p
rogra
ms for
impro
ved
de
livery
of
po
st-
part
um
vitam
in A
sup
ple
me
nts
•
To m
on
itor
the gro
wth
of
oth
er
pu
blic
h
ea
lth in
terv
ention
s such
as m
ea
sle
s va
ccin
atio
ns,
w
hils
t d
eliv
ering
vitam
in A
su
pple
me
nts
.
VV
M
ww
w.w
ho.int/vaccin
es
.acce
ss/v
acm
an/v
vm
/vvm
main
page.h
tm
•
To im
pro
ve q
ualit
y co
ntr
ol
duri
ng im
mu
nis
atio
n pro
gra
mm
es u
sin
g la
be
ls w
here
by
he
alth
wo
rke
rs c
an d
ete
rmin
e he
at
exp
osure
and
de
gra
datio
n o
f th
e v
accin
e
•
To im
pro
ve th
e m
ana
ge
me
nt
of
va
ccin
e a
nd r
ed
uce
wast
age
•
To d
ete
rmin
e v
accin
e s
afe
ty o
r w
heth
er
it s
hou
ld b
e d
iscard
ed
WP
ES
S
•
To
coord
inate
a
new
part
ne
rsh
ip fo
r th
e
surv
eill
an
ce,
co
ntr
ol, an
d tr
eatm
ent
of
sle
epin
g
sic
kne
ss
inte
gra
ting
sup
ply
agre
em
ents
, dis
ease m
ana
gem
ent,
an
d r
ese
arc
h
•
Ad
voca
cy
an
d a
ware
ne
ss:
resc
uin
g t
he d
isea
se fro
m o
bliv
ion
an
d in
cre
asi
ng
the v
isib
ility
of eff
ort
s.
•
Part
ners
hip
: ra
llyin
g p
art
ne
rs to s
upport
an e
limin
atio
n p
rog
ram
me
•
Sup
port
: st
ren
gth
en
ing t
he o
rga
niz
ation a
nd
im
ple
me
nta
tion o
f contr
ol a
ctivitie
s in
co
untr
ies
•
Coo
rdin
atio
n a
mu
ltip
le c
om
pan
y don
ation p
rogra
mm
e
•
Researc
h:
encoura
gin
g r
esearc
h in
stitu
tes
to f
un
d a
nd
imp
lem
en
t re
searc
h o
n d
rugs,
dia
gn
osis
an
d a
pplie
d r
ese
arc
h
•
Info
rmatio
n m
ana
gem
ent
and d
isse
min
ation
: exch
ang
ing
info
rmatio
n a
nd
pro
vid
ing t
rain
ing t
o t
ho
se i
nvo
lve
d i
n s
lee
pin
g
sickne
ss a
ctiv
itie
s
Sourc
e:
upd
ate
d f
rom
Buse
K.,
20
04. G
loba
l H
ealth P
art
ners
hip
s:
Map
pin
g a
shifting t
err
ain
. Lon
don
: D
FID
Health R
eso
urc
e C
en
tre
.
Mapping Global Health Partnerships 27
DFID Health Resource Centre
APPENDIX B: GLOBAL HEALTH PARTNERSHIPS – MAPPING BY COUNTRY EXERCISE Purpose To provide a global picture of where Global Health Partnerships provide support on a country by country basis, and with an overview of key country characteristics that might effect GHP support. Methodology The mapping exercise looked at a number of variables, which included:
• Global Health Partnerships • Country GDP per capita • Prevalence or cases of specific diseases of interest to target GHPs • Demographic characteristics • Poverty characteristics • Political characteristics • Health system characteristics, in terms of levels of financing.
These were then analysed by converting the table into a spreadsheet and sorting the data, using the number of GHPs as the independent variable, and all other factors as dependent variables. Full information was gathered for only a selection of countries in each region, focusing on those countries of greatest interest to DFID, as well as those with the largest number of GHPs providing support. Findings As far as the type of government is concerned, as measured on a scale of –10 (authoritarian) to +10 (fully democratic), there is no apparent correlation between the number and type of GHPs operating when looked at by type of government As far as public spending on health is concerned, there is no correlation between the percentage of spending on the health sector coming from the public purse and the number or type of GHPs operating in a country. There is a moderate correlation between the prevalence rate or case number of a disease and the presence of the relevant GHP, as would be expected. However, it is impossible to state whether GFATM is providing appropriate levels of funding for each of its three target diseases in each country where it is present, based on the epidemiology of the disease in that country, without looking at GFATM support on a country by country basis. There would appear to be a correlation between the per capita GDP and the number of GHPs operating in a country, though this is inconsistent. The strongest correlation is between the what region the country is part of and the number of GHPs operating in that country, with Africa having consistently the largest number of GHPs per country, followed by Asia (East, Southeast and Central). Eastern and Central European countries have the lowest number of GHPs.
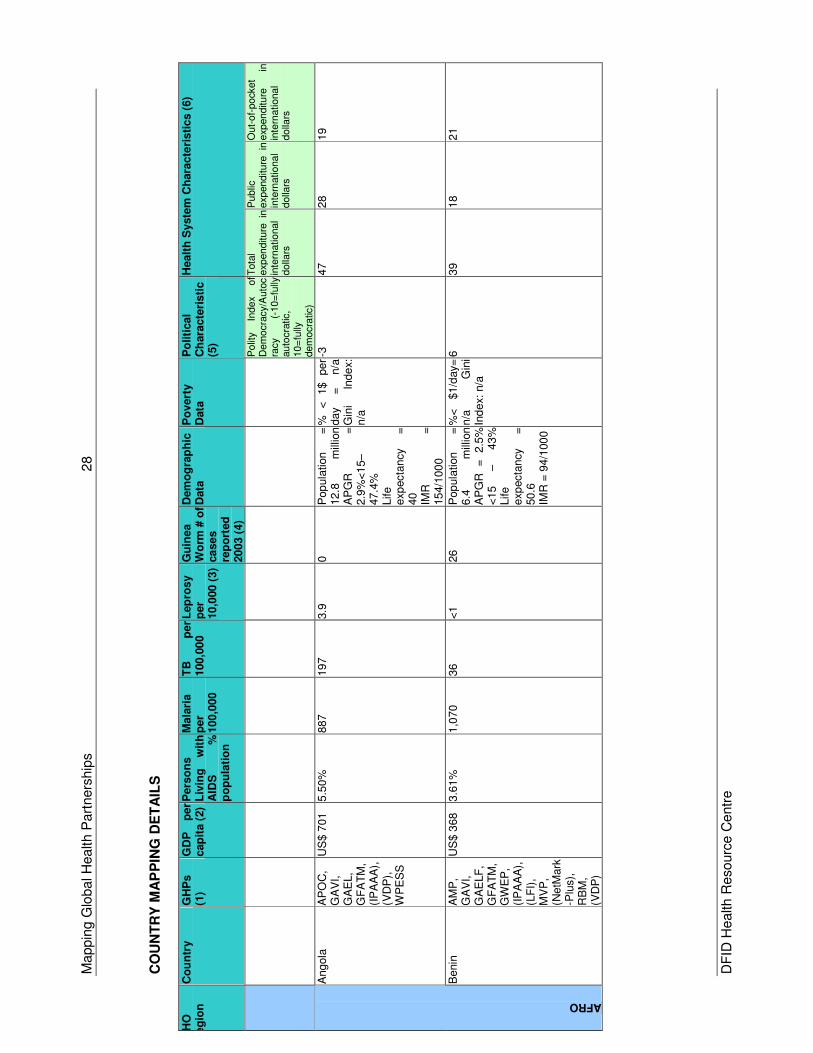
Mappin
g G
lobal H
ealth P
art
ners
hip
s
28
DF
ID H
ealth R
esourc
e C
entr
e
CO
UN
TR
Y M
AP
PIN
G D
ET
AIL
S
W
HO
R
eg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
P
olit
y In
dex
of
Dem
ocra
cy/
Auto
cra
cy
(-10=
fully
auto
cra
tic,
10=
fully
dem
ocra
tic)
Tota
l exp
enditure
in
in
tern
ational
dolla
rs
Public
exp
enditure
in
in
tern
ational
dolla
rs
Out-
of-
pock
et
exp
enditure
in
in
tern
ational
dolla
rs
Angola
A
PO
C,
GA
VI,
GA
EL,
GF
AT
M,
(IP
AA
A),
(V
DP
),
WP
ES
S
US
$ 7
01
5.5
0%
887
197
3.9
0
Pop
ula
tion
=
12.8
m
illio
n
A
PG
R
=
2.9
%<
15–
47.4
%
Life
exp
ecta
ncy
=
40
IM
R
=
15
4/1
00
0
%
<
1$
per
day
=
n/a
Gin
i In
de
x:
n/a
-3
47
28
19
AFRO
Benin
A
MP
, G
AV
I,
GA
ELF
, G
FA
TM
, G
WE
P,
(IP
AA
A),
(L
FI)
, M
VP
, (N
etM
ark
-Plu
s),
R
BM
, (V
DP
)
US
$ 3
68
3.6
1%
1,0
70
36
<1
26
Pop
ula
tion
=
6.4
m
illio
n
AP
GR
=
2.5
%
<15
–
43%
Life
exp
ecta
ncy
=
50.6
IMR
= 9
4/1
00
0
%<
$1/d
ay=
n/a
G
ini
Ind
ex:
n/a
6
39
18
21
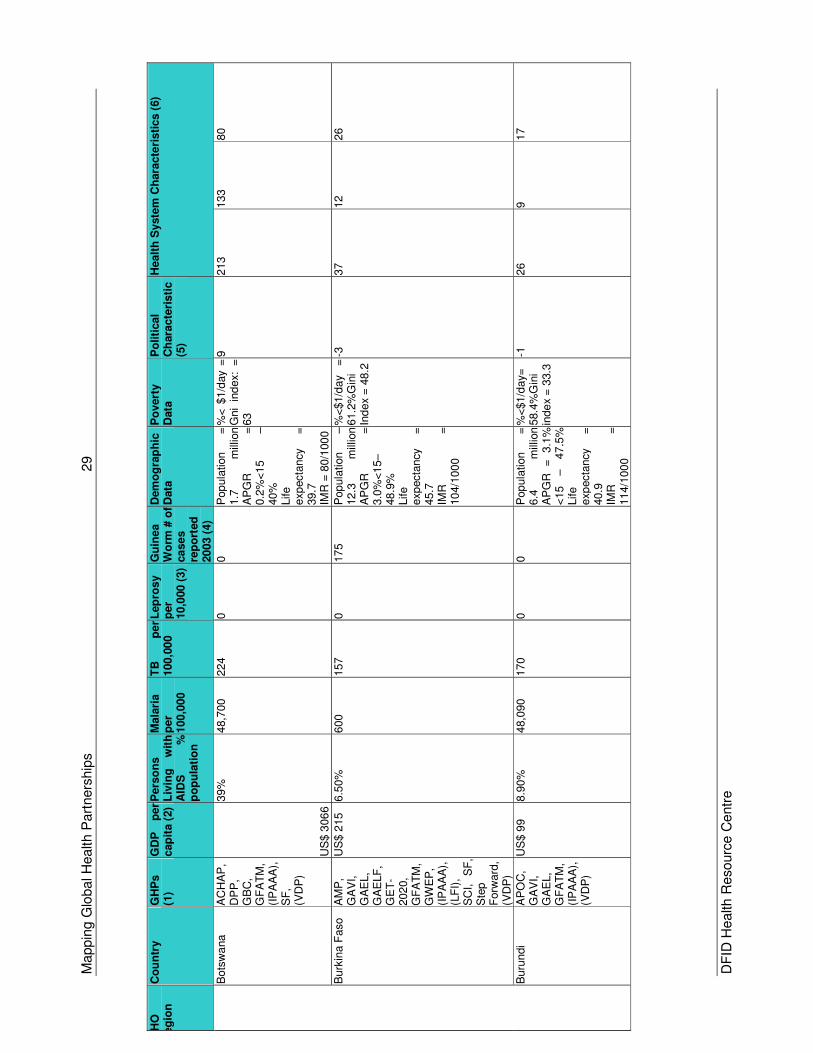
Mappin
g G
lobal H
ealth P
art
ners
hip
s
29
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Bots
wa
na
AC
HA
P,
DP
P,
GB
C,
GF
AT
M,
(IP
AA
A),
S
F,
(VD
P)
US
$ 3
06
6 3
9%
48,7
00
224
0
0
Pop
ula
tion
=
1.7
m
illio
n
AP
GR
=
0.2
%<
15
–
40%
Life
exp
ecta
ncy
=
39.7
IMR
= 8
0/1
00
0
%<
$1/d
ay =
G
ni
ind
ex:
=
63
9
213
133
80
Burk
ina F
aso
AM
P,
GA
VI,
GA
EL,
GA
ELF
, G
ET
-202
0,
GF
AT
M,
GW
EP
, (I
PA
AA
),
(LF
I),
SC
I,
SF
, S
tep
Forw
ard
, (V
DP
)
US
$ 2
15
6.5
0%
600
157
0
17
5
Pop
ula
tion
–
12.3
m
illio
n
AP
GR
=
3.0
%<
15–
48.9
%
Life
exp
ecta
ncy
=
45.7
IMR
=
10
4/1
00
0
%<
$1/d
ay
=
61.2
%G
ini
Ind
ex
= 4
8.2
-3
37
12
26
Buru
ndi
AP
OC
, G
AV
I,
GA
EL,
GF
AT
M,
(IP
AA
A),
(V
DP
)
US
$ 9
9
8.9
0%
48,0
90
170
0
0
Pop
ula
tion
=
6.4
m
illio
n
A
PG
R
=
3.1
%
<15
–
47.5
%
Life
exp
ecta
ncy
=
40.9
IM
R
=
11
4/1
00
0
%<
$1/d
ay=
58.4
%G
ini
inde
x =
33.3
-1
26
9
17
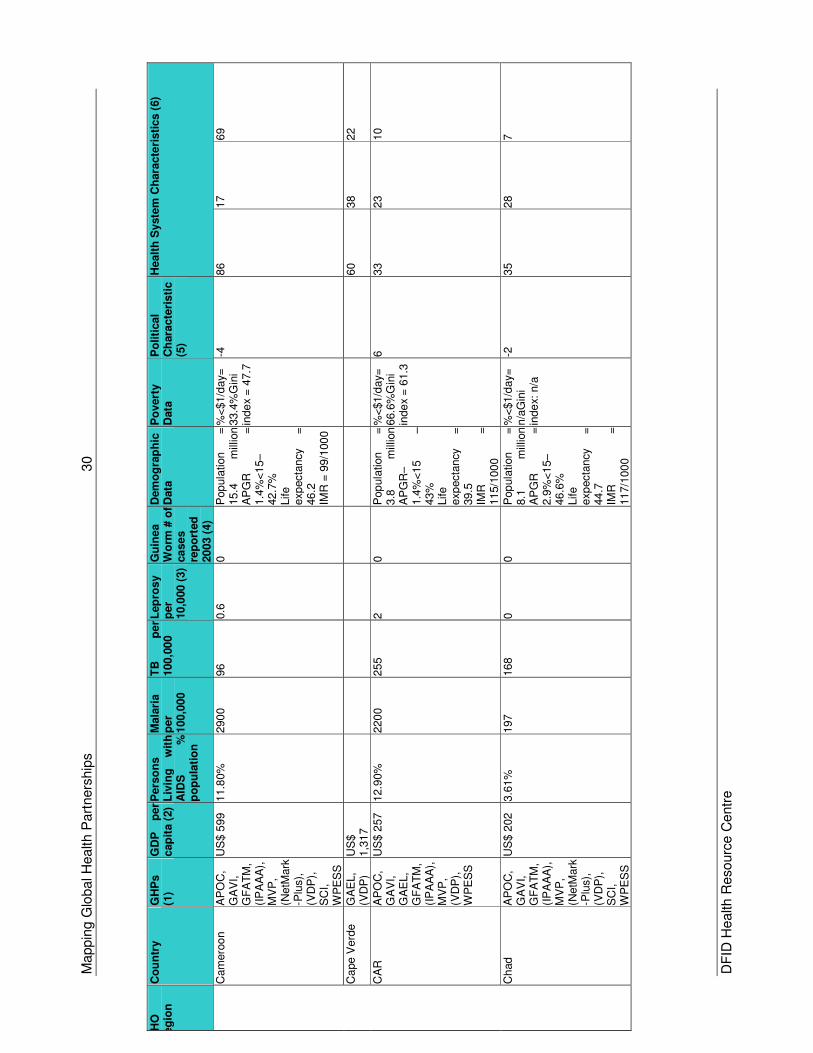
Mappin
g G
lobal H
ealth P
art
ners
hip
s
30
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Cam
ero
on
AP
OC
, G
AV
I,
GF
AT
M,
(IP
AA
A),
M
VP
, (N
etM
ark
-Plu
s),
(V
DP
),
SC
I,
WP
ES
S
US
$ 5
99
11.8
0%
290
0
96
0.6
0
Pop
ula
tion
=
15.4
m
illio
n
AP
GR
=
1.4
%<
15–
42.7
%
Life
exp
ecta
ncy
=
46.2
IMR
= 9
9/1
00
0
%<
$1/d
ay=
33.4
%G
ini
inde
x =
47.7
-4
86
17
69
Ca
pe V
erd
e
GA
EL,
(VD
P)
US
$
1,3
17
60
38
22
CA
R
AP
OC
, G
AV
I,
GA
EL,
GF
AT
M,
(IP
AA
A),
M
VP
, (V
DP
),
WP
ES
S
US
$ 2
57
12.9
0%
220
0
255
2
0
Pop
ula
tion
=
3.8
m
illio
n
AP
GR
–1.4
%<
15
–
43%
Life
exp
ecta
ncy
=
39.5
IM
R
=
11
5/1
00
0
%<
$1/d
ay=
66.6
%G
ini
inde
x =
61.3
6
33
23
10
Ch
ad
AP
OC
, G
AV
I,
GF
AT
M,
(IP
AA
A),
M
VP
, (N
etM
ark
-Plu
s),
(V
DP
),
SC
I,
WP
ES
S
US
$ 2
02
3.6
1%
197
168
0
0
Pop
ula
tion
=
8.1
m
illio
n
AP
GR
=
2.9
%<
15–
46.6
%
Life
exp
ecta
ncy
=
44.7
IM
R
=
11
7/1
00
0
%<
$1/d
ay=
n/a
Gin
i in
de
x: n
/a
-2
35
28
7
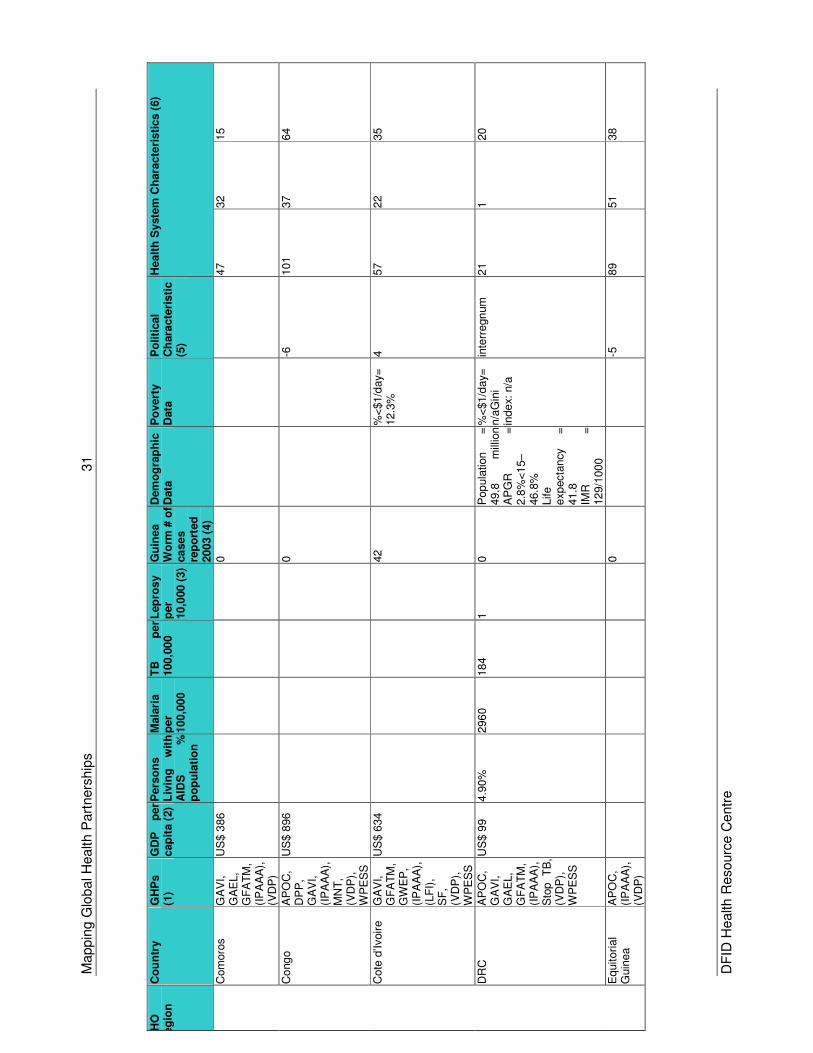
Mappin
g G
lobal H
ealth P
art
ners
hip
s
31
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Com
oro
s
GA
VI,
GA
EL,
GF
AT
M,
(IP
AA
A),
(V
DP
)
US
$ 3
86
0
47
32
15
Co
ng
o
AP
OC
, D
PP
, G
AV
I,
(IP
AA
A),
M
NT
, (V
DP
),
WP
ES
S
US
$ 8
96
0
-6
101
37
64
Cote
d’Ivoir
e
GA
VI,
GF
AT
M,
GW
EP
, (I
PA
AA
),
(LF
I),
SF
, (V
DP
),
WP
ES
S
US
$ 6
34
42
%
<$1/d
ay=
12.3
%
4
57
22
35
DR
C
AP
OC
, G
AV
I,
GA
EL,
GF
AT
M,
(IP
AA
A),
S
top
TB
,
(VD
P),
W
PE
SS
US
$ 9
9
4.9
0%
296
0
184
1
0
Pop
ula
tion
=
49.8
m
illio
n
A
PG
R
=
2.8
%<
15–
46.8
%
Life
exp
ecta
ncy
=
41.8
IMR
=
12
9/1
00
0
%<
$1/d
ay=
n/a
Gin
i in
de
x: n
/a
inte
rregn
um
21
1
20
Equitori
al
Guin
ea
AP
OC
, (I
PA
AA
),
(VD
P)
0
-5
89
51
38
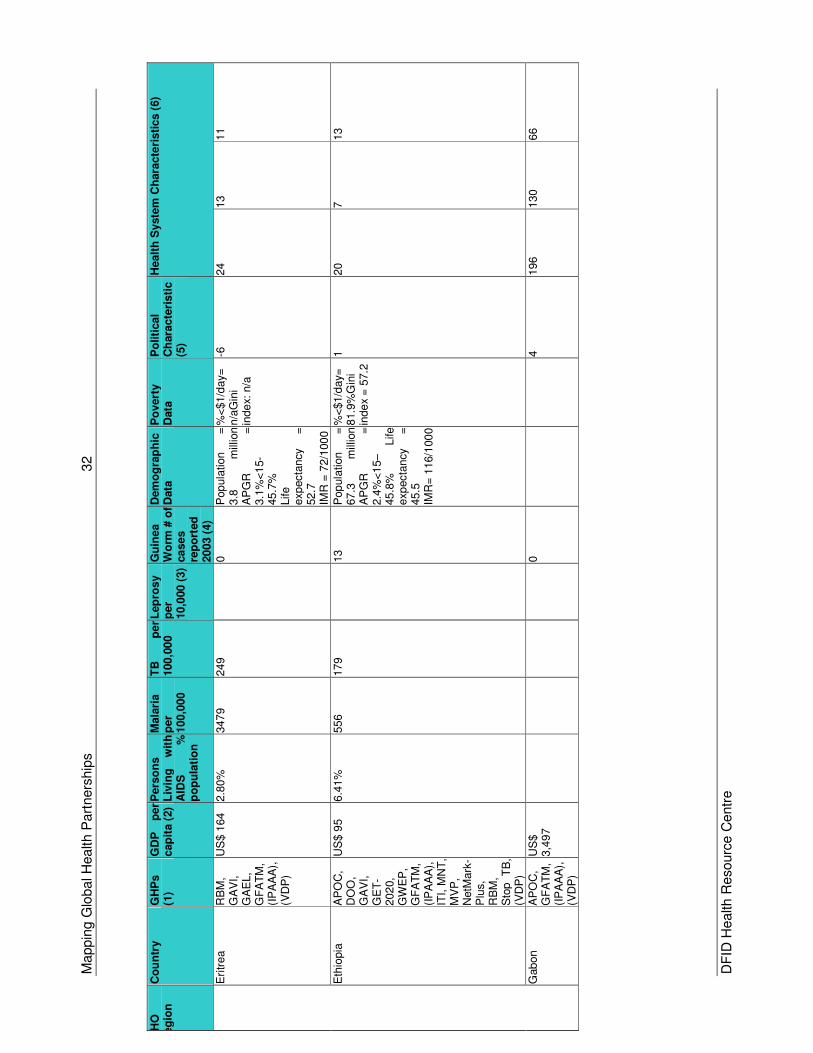
Mappin
g G
lobal H
ealth P
art
ners
hip
s
32
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Eri
trea
RB
M,
GA
VI,
GA
EL,
GF
AT
M,
(IP
AA
A),
(V
DP
)
US
$ 1
64
2.8
0%
347
9
249
0
Pop
ula
tion
=
3.8
m
illio
n
A
PG
R
=
3.1
%<
15-
45.7
%
Life
exp
ecta
ncy
=
52.7
IMR
= 7
2/1
00
0
%<
$1/d
ay=
n/a
Gin
i in
de
x: n
/a
-6
24
13
11
Eth
iopia
A
PO
C,
DO
O,
GA
VI,
GE
T-
202
0,
GW
EP
, G
FA
TM
, (I
PA
AA
),
ITI,
MN
T,
MV
P,
NetM
ark
-P
lus,
RB
M,
Sto
p
TB
, (V
DP
)
US
$ 9
5
6.4
1%
556
179
13
Pop
ula
tion
=
67.3
m
illio
n
A
PG
R
=
2.4
%<
15–
45.8
%
Life
exp
ecta
ncy
=
45.5
IM
R=
116/1
00
0 %
<$1/d
ay=
81.9
%G
ini
inde
x =
57.2
1
20
7
13
Gabon
AP
OC
, G
FA
TM
, (I
PA
AA
),
(VD
P)
US
$
3,4
97
0
4
196
130
66
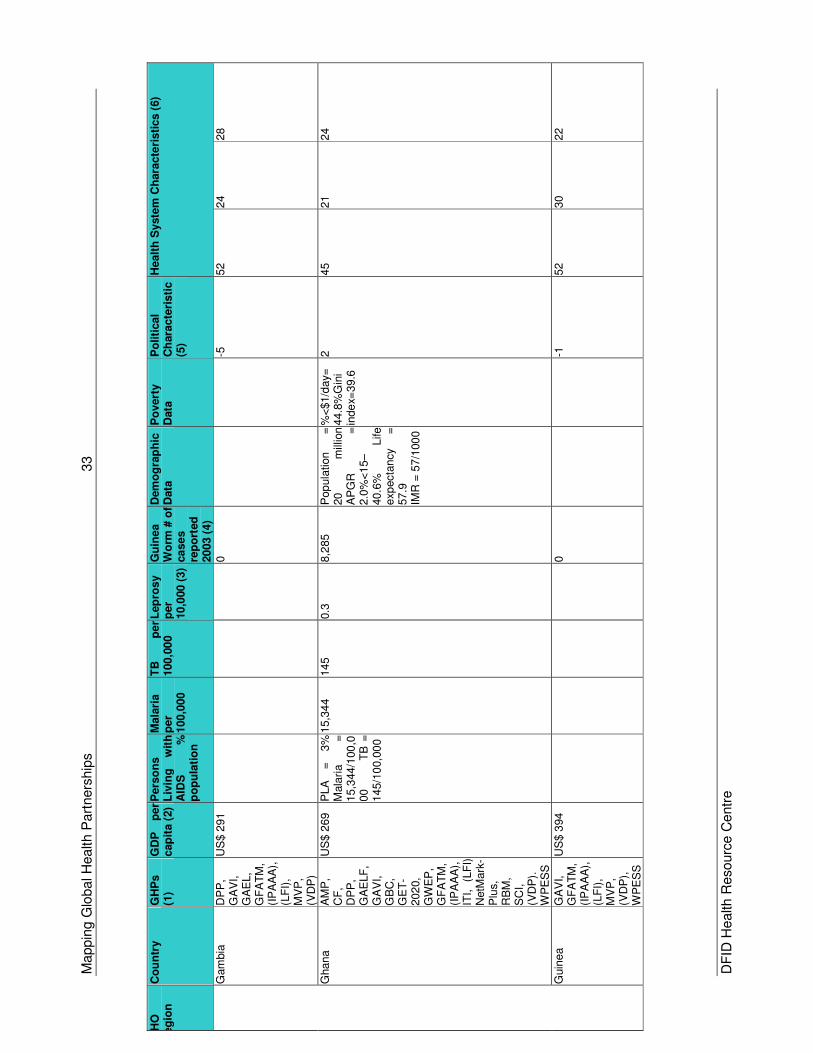
Mappin
g G
lobal H
ealth P
art
ners
hip
s
33
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Gam
bia
D
PP
, G
AV
I,
GA
EL,
GF
AT
M,
(IP
AA
A),
(L
FI)
, M
VP
, (V
DP
)
US
$ 2
91
0
-5
52
24
28
Ghana
AM
P,
CF
, D
PP
, G
AE
LF
, G
AV
I,
GB
C,
GE
T-
202
0,
GW
EP
, G
FA
TM
, (I
PA
AA
),
ITI,
(L
FI)
N
etM
ark
-P
lus,
RB
M,
SC
I,
(VD
P).
W
PE
SS
US
$ 2
69
PLA
=
3%
Mala
ria
=
15,3
44/1
00,0
00
TB
=
145/1
00,0
00
15,3
44
145
0.3
8,2
85
Pop
ula
tion
=
20
m
illio
n
AP
GR
=
2.0
%<
15–
40.6
%
Life
exp
ecta
ncy
=
57.9
IMR
= 5
7/1
00
0
%<
$1/d
ay=
44.8
%G
ini
inde
x=39.6
2
45
21
24
Guin
ea
GA
VI,
GF
AT
M,
(IP
AA
A),
(L
FI)
, M
VP
, (V
DP
),
WP
ES
S
US
$ 3
94
0
-1
52
30
22
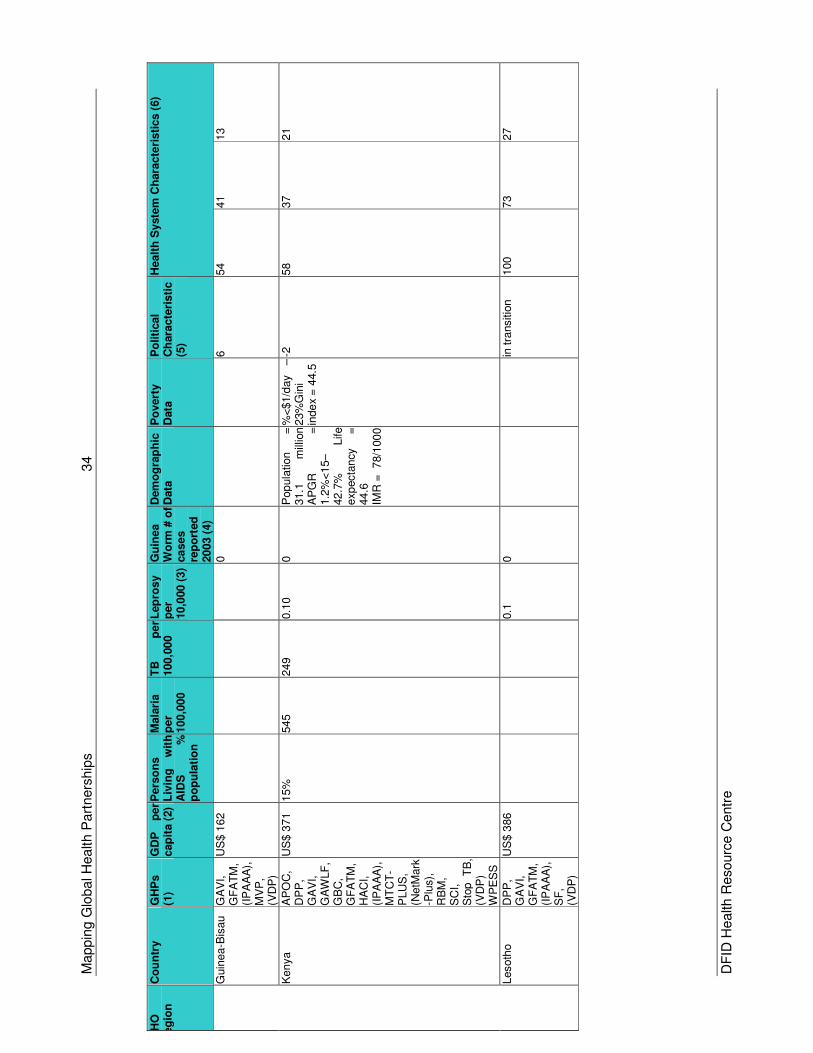
Mappin
g G
lobal H
ealth P
art
ners
hip
s
34
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Guin
ea-B
isau
GA
VI,
GF
AT
M,
(IP
AA
A),
M
VP
, (V
DP
)
US
$ 1
62
0
6
54
41
13
Kenya
AP
OC
, D
PP
, G
AV
I,
GA
WLF
, G
BC
, G
FA
TM
, H
AC
I,
(IP
AA
A),
M
TC
T-
PLU
S,
(NetM
ark
-Plu
s),
R
BM
, S
CI,
Sto
p
TB
, (V
DP
) W
PE
SS
US
$ 3
71
15%
545
249
0.1
0
0
Pop
ula
tion
=
31.1
m
illio
n
A
PG
R
=
1.2
%<
15–
42.7
%
Life
exp
ecta
ncy
=
44.6
IMR
= 78/1
00
0 %
<$1/d
ay
–
23%
Gin
i in
de
x =
44.5
-2
58
37
21
Lesoth
o
DP
P,
GA
VI,
GF
AT
M,
(IP
AA
A),
S
F,
(VD
P)
US
$ 3
86
0.1
0
in t
ransitio
n
100
73
27
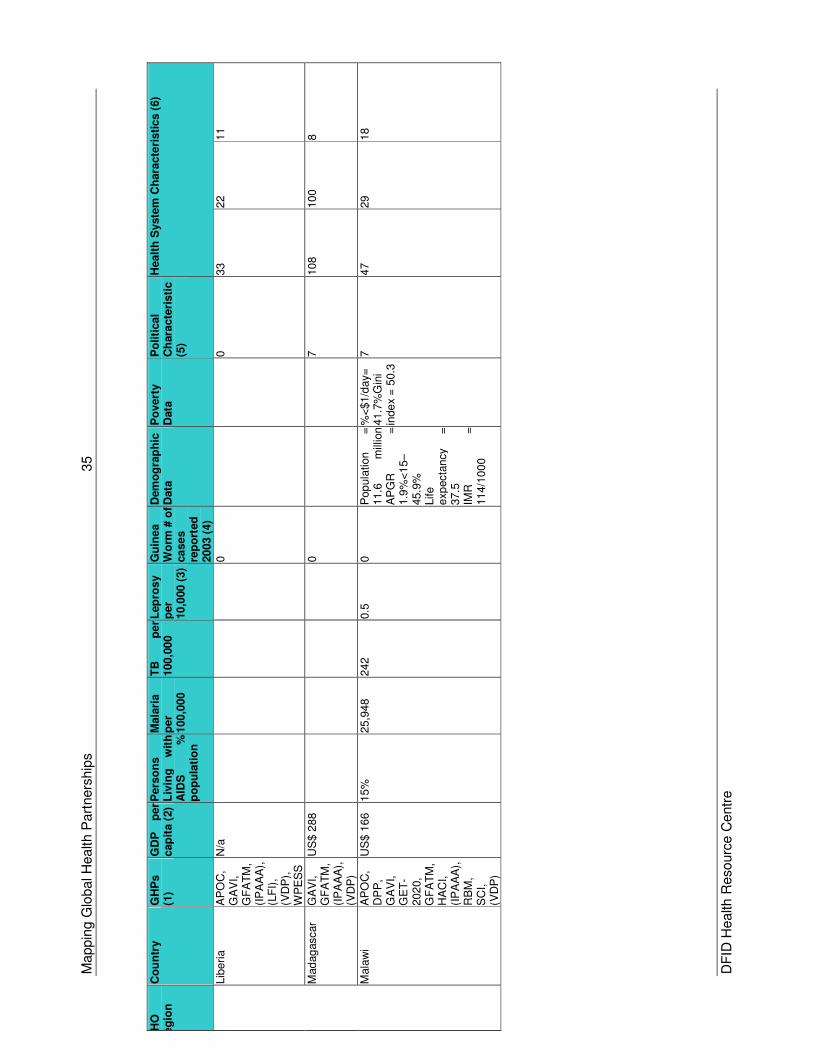
Mappin
g G
lobal H
ealth P
art
ners
hip
s
35
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Lib
eri
a
AP
OC
, G
AV
I,
GF
AT
M,
(IP
AA
A),
(L
FI)
, (V
DP
),
WP
ES
S
N/a
0
0
33
22
11
Mad
ag
ascar
GA
VI,
GF
AT
M,
(IP
AA
A),
(V
DP
)
US
$ 2
88
0
7
108
100
8
Mala
wi
AP
OC
, D
PP
, G
AV
I,
GE
T-
202
0,
GF
AT
M,
HA
CI,
(IP
AA
A),
R
BM
, S
CI,
(VD
P)
US
$ 1
66
15%
25,9
48
242
0.5
0
Pop
ula
tion
=
11.6
m
illio
n
AP
GR
=
1.9
%<
15–
45.9
%
Life
exp
ecta
ncy
=
37.5
IMR
=
11
4/1
00
0
%<
$1/d
ay=
41.7
%G
ini
inde
x =
50.3
7
47
29
18
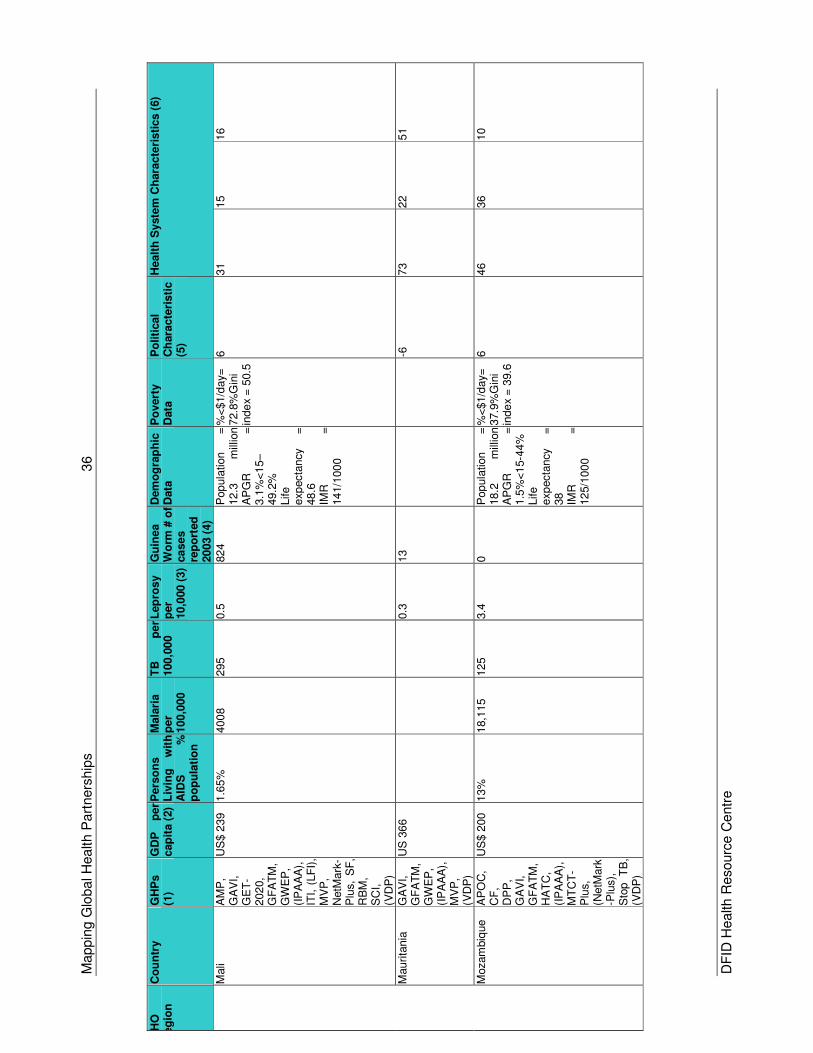
Mappin
g G
lobal H
ealth P
art
ners
hip
s
36
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Mali
AM
P,
GA
VI,
GE
T-
202
0,
GF
AT
M,
GW
EP
, (I
PA
AA
),
ITI,
(LF
I),
MV
P,
NetM
ark
-P
lus,
SF
, R
BM
, S
CI,
(VD
P)
US
$ 2
39
1.6
5%
400
8
295
0.5
82
4
Pop
ula
tion
=
12.3
m
illio
n
AP
GR
=
3.1
%<
15–
49.2
%
Life
exp
ecta
ncy
=
48.6
IMR
=
14
1/1
00
0
%<
$1/d
ay=
72.8
%G
ini
inde
x =
50.5
6
31
15
16
Mauri
tania
G
AV
I,
GF
AT
M,
GW
EP
, (I
PA
AA
),
MV
P,
(VD
P)
US
36
6
0.3
13
-6
73
22
51
Mozam
biq
ue
AP
OC
, C
F,
DP
P,
GA
VI,
GF
AT
M,
HA
TC
, (I
PA
AA
),
MT
CT
-P
lus,
(NetM
ark
-Plu
s),
S
top
TB
, (V
DP
)
US
$ 2
00
13%
18,1
15
125
3.4
0
Pop
ula
tion
=
18.2
m
illio
n
AP
GR
=
1.5
%<
15-4
4%
Life
exp
ecta
ncy
=
38
IMR
=
12
5/1
00
0
%<
$1/d
ay=
37.9
%G
ini
inde
x =
39.6
6
46
36
10
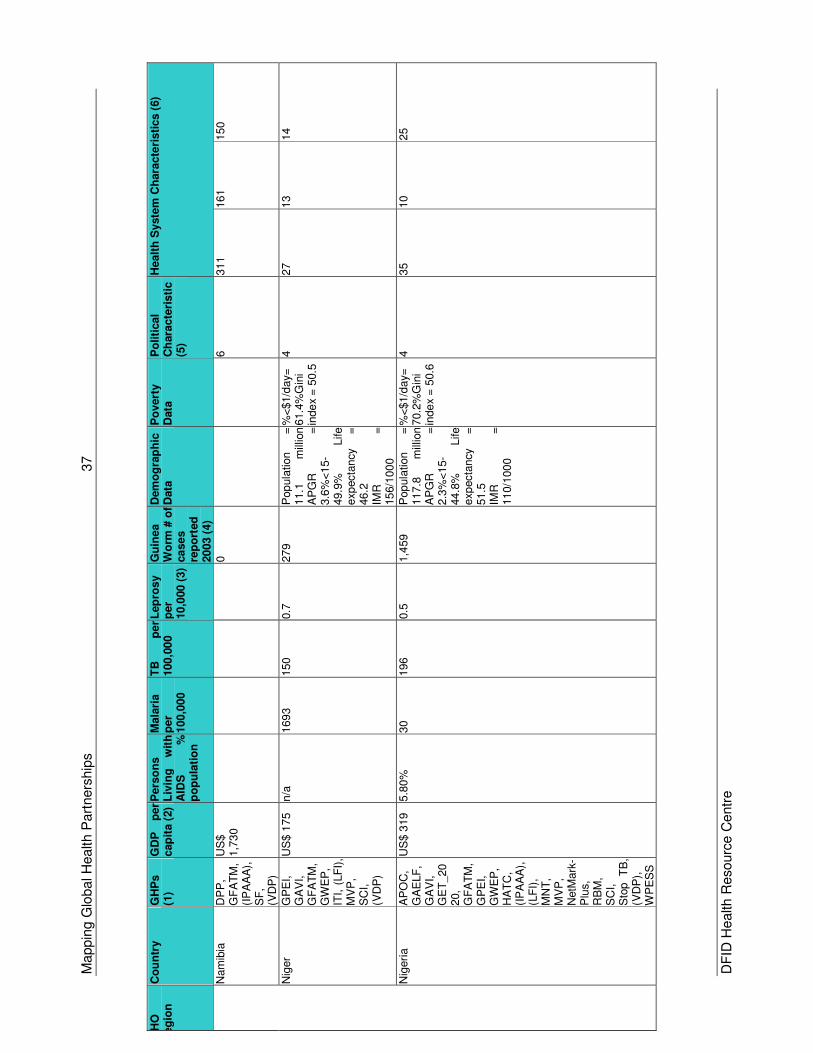
Mappin
g G
lobal H
ealth P
art
ners
hip
s
37
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Nam
ibia
D
PP
, G
FA
TM
, (I
PA
AA
),
SF
, (V
DP
)
US
$
1,7
30
0
6
311
161
150
Nig
er
GP
EI,
GA
VI,
GF
AT
M,
GW
EP
, IT
I, (
LF
I),
MV
P,
SC
I,
(VD
P)
US
$ 1
75
n/a
169
3
150
0.7
27
9
Pop
ula
tion
=
11.1
m
illio
n
AP
GR
=
3.6
%<
15-
49.9
%
Life
exp
ecta
ncy
=
46.2
IM
R
=
15
6/1
00
0
%<
$1/d
ay=
61.4
%G
ini
inde
x =
50.5
4
27
13
14
Nig
eri
a
AP
OC
, G
AE
LF
, G
AV
I,
GE
T_20
20,
GF
AT
M,
GP
EI,
GW
EP
, H
AT
C,
(IP
AA
A),
(L
FI)
, M
NT
, M
VP
, N
etM
ark
-P
lus,
RB
M,
SC
I,
Sto
p
TB
, (V
DP
),
WP
ES
S
US
$ 3
19
5.8
0%
30
196
0.5
1,4
59
Pop
ula
tion
=
11
7.8
m
illio
n
A
PG
R
=
2.3
%<
15-
44.8
%
Life
exp
ecta
ncy
=
51.5
IMR
=
11
0/1
00
0
%<
$1/d
ay=
70.2
%G
ini
inde
x =
50.6
4
35
10
25
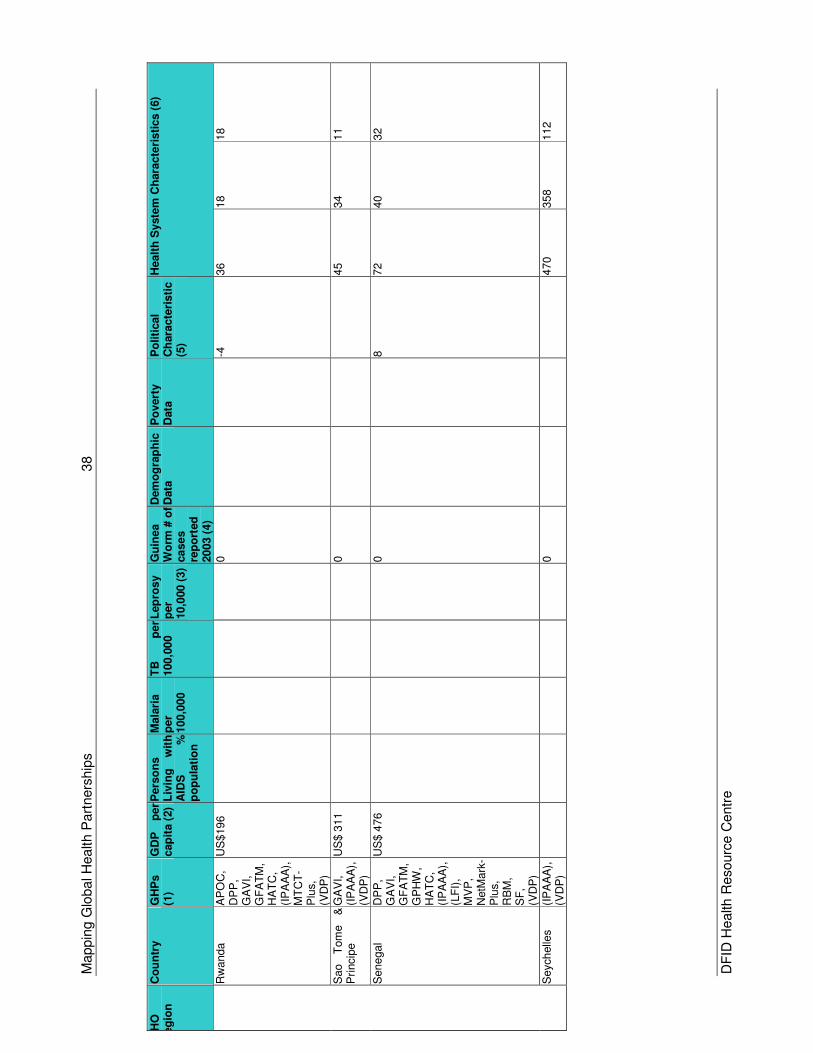
Mappin
g G
lobal H
ealth P
art
ners
hip
s
38
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Rw
anda
AP
OC
, D
PP
, G
AV
I,
GF
AT
M,
HA
TC
, (I
PA
AA
),
MT
CT
-P
lus,
(VD
P)
US
$19
6
0
-4
36
18
18
Sao
Tom
e
&
Pri
ncip
e
GA
VI,
(IP
AA
A),
(V
DP
)
US
$ 3
11
0
45
34
11
Sene
gal
DP
P,
GA
VI,
GF
AT
M,
GP
HW
, H
AT
C,
(IP
AA
A),
(L
FI)
, M
VP
, N
etM
ark
-P
lus,
RB
M,
SF
, (V
DP
)
US
$ 4
76
0
8
72
40
32
Seych
elle
s
(IP
AA
A),
(V
DP
)
0
470
358
112
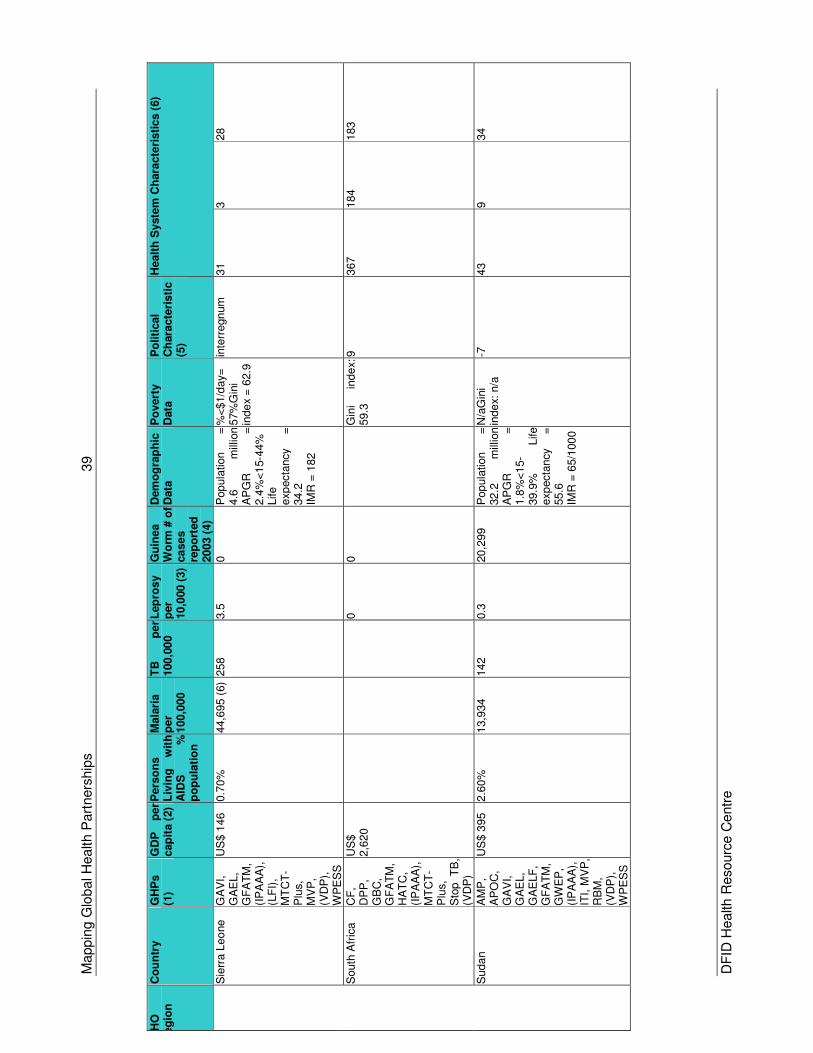
Mappin
g G
lobal H
ealth P
art
ners
hip
s
39
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Sie
rra L
eo
ne
GA
VI,
GA
EL,
GF
AT
M,
(IP
AA
A),
(L
FI)
, M
TC
T-
Plu
s,
MV
P,
(VD
P),
W
PE
SS
US
$ 1
46
0.7
0%
44,6
95 (
6)
258
3.5
0
Pop
ula
tion
=
4.6
m
illio
n
AP
GR
=
2.4
%<
15-4
4%
Life
exp
ecta
ncy
=
34.2
IMR
= 1
82
%<
$1/d
ay=
57%
Gin
i in
de
x =
62.9
inte
rregn
um
31
3
28
South
Afr
ica
CF
, D
PP
, G
BC
, G
FA
TM
, H
AT
C,
(IP
AA
A),
M
TC
T-
Plu
s,
Sto
p
TB
, (V
DP
)
US
$
2,6
20
0
0
G
ini
inde
x:
59.3
9
367
184
183
Suda
n
AM
P,
AP
OC
, G
AV
I,
GA
EL,
GA
ELF
, G
FA
TM
, G
WE
P,
(IP
AA
A),
IT
I, M
VP
, R
BM
, (V
DP
),
WP
ES
S
US
$ 3
95
2.6
0%
13,9
34
142
0.3
20,2
99
Pop
ula
tion
=
32.2
m
illio
n
AP
GR
=
1.8
%<
15-
39.9
%
Life
exp
ecta
ncy
=
55.6
IMR
= 6
5/1
00
0
N/a
Gin
i in
de
x: n
/a
-7
43
9
34
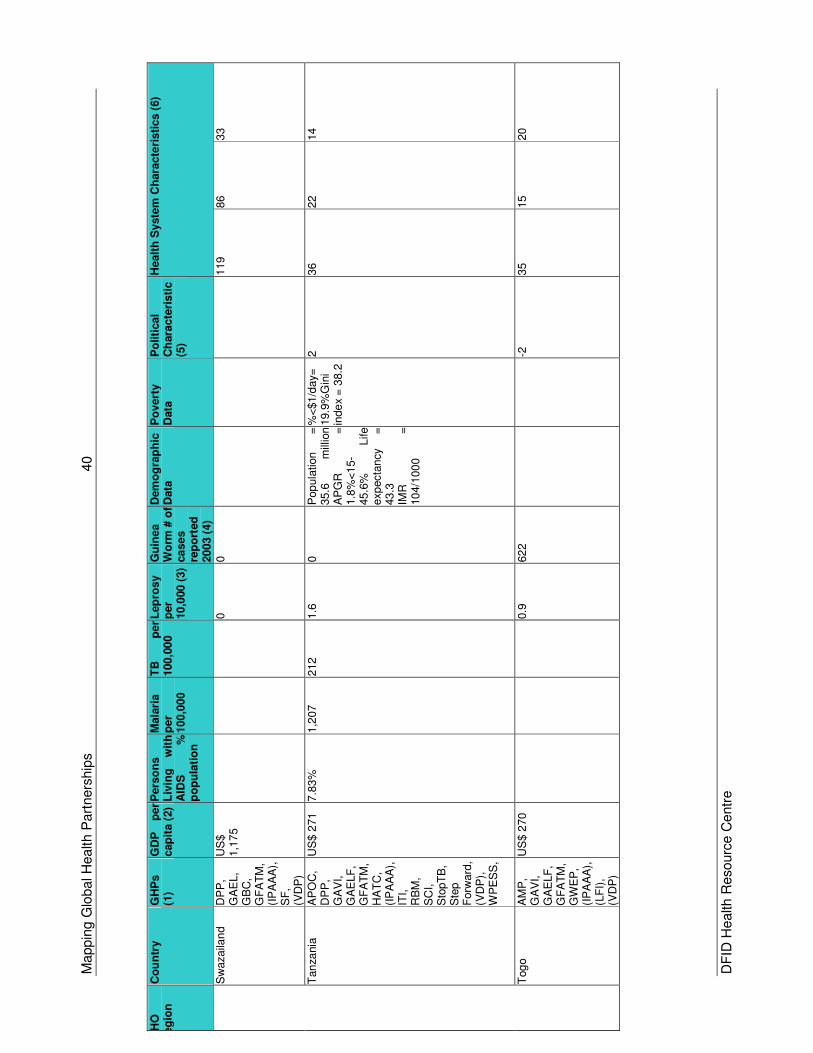
Mappin
g G
lobal H
ealth P
art
ners
hip
s
40
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Sw
azaila
nd
DP
P,
GA
EL,
GB
C,
GF
AT
M,
(IP
AA
A),
S
F,
(VD
P)
US
$
1,1
75
0
0
119
86
33
Tan
zania
A
PO
C,
DP
P,
GA
VI,
GA
ELF
, G
FA
TM
, H
AT
C,
(IP
AA
A),
IT
I,
RB
M,
SC
I,
Sto
pT
B,
Ste
p
Forw
ard
, (V
DP
),
WP
ES
S, U
S$ 2
71
7.8
3%
1,2
07
212
1.6
0
Pop
ula
tion
=
35.6
m
illio
n
AP
GR
=
1.8
%<
15-
45.6
%
Life
exp
ecta
ncy
=
43.3
IMR
=
10
4/1
00
0
%<
$1/d
ay=
19.9
%G
ini
inde
x =
38.2
2
36
22
14
Tog
o
AM
P,
GA
VI,
GA
ELF
, G
FA
TM
, G
WE
P,
(IP
AA
A),
(L
FI)
, (V
DP
)
US
$ 2
70
0.9
62
2
-2
35
15
20
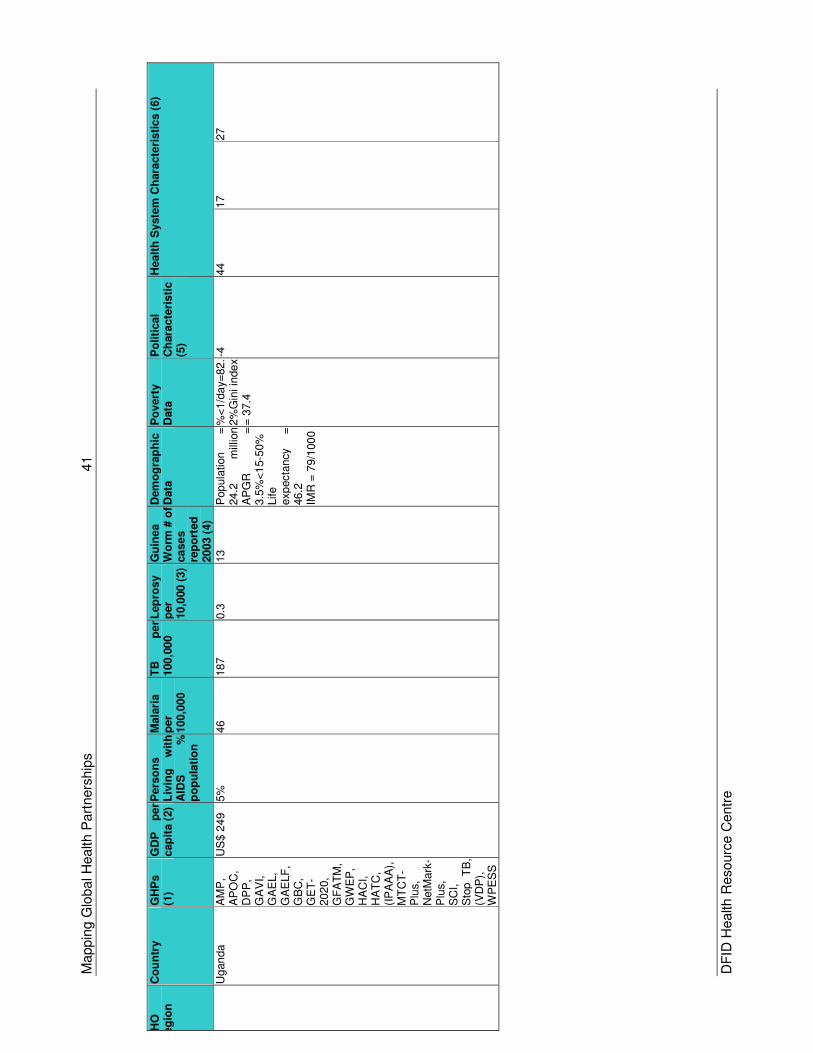
Mappin
g G
lobal H
ealth P
art
ners
hip
s
41
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
U
gan
da
AM
P,
AP
OC
, D
PP
, G
AV
I,
GA
EL,
GA
ELF
, G
BC
, G
ET
-202
0,
GF
AT
M,
GW
EP
, H
AC
I,
HA
TC
, (I
PA
AA
),
MT
CT
-P
lus,
NetM
ark
-P
lus,
SC
I,
Sto
p
TB
, (V
DP
),
WP
ES
S
US
$ 2
49
5%
46
187
0.3
13
Pop
ula
tion
=
24.2
m
illio
n
AP
GR
=
3.5
%<
15-5
0%
Life
exp
ecta
ncy
=
46.2
IMR
= 7
9/1
00
0
%<
1/d
ay=
82.
2%
Gin
i in
de
x
= 3
7.4
-4
44
17
27
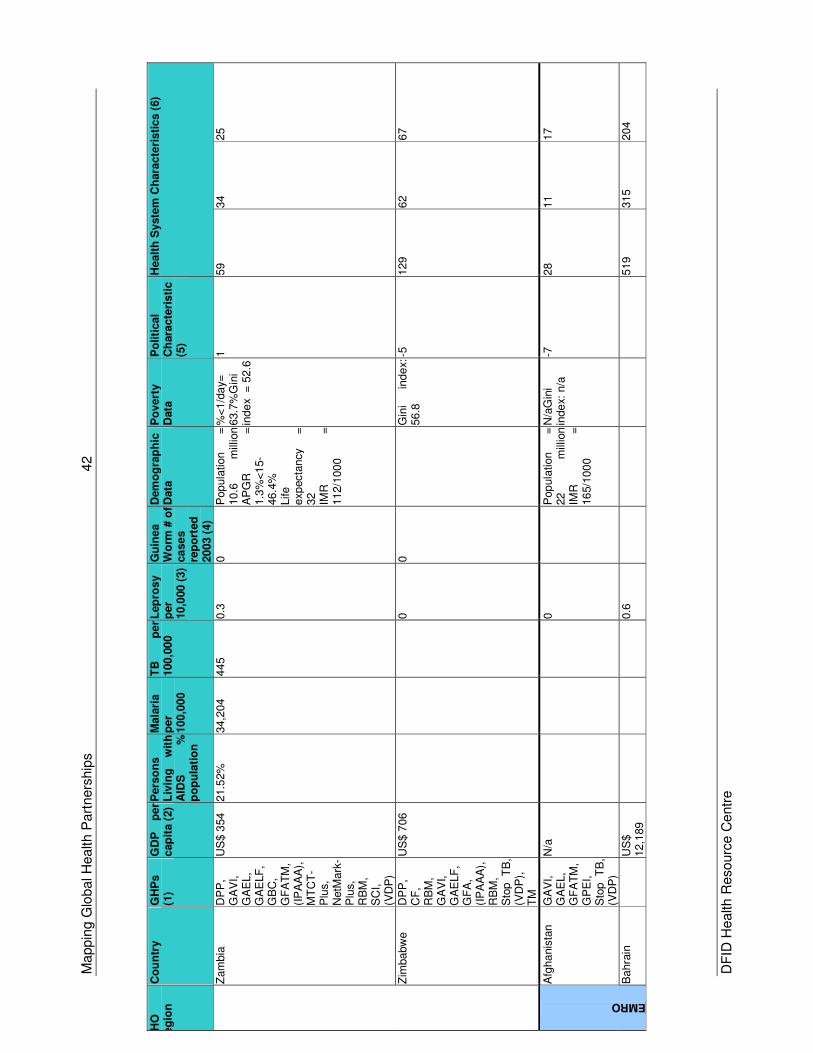
Mappin
g G
lobal H
ealth P
art
ners
hip
s
42
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Zam
bia
D
PP
, G
AV
I,
GA
EL,
GA
ELF
, G
BC
, G
FA
TM
, (I
PA
AA
),
MT
CT
-P
lus,
NetM
ark
-P
lus,
RB
M,
SC
I,
(VD
P)
US
$ 3
54
21.5
2%
34,2
04
445
0.3
0
Pop
ula
tion
=
10.6
m
illio
n
AP
GR
=
1.3
%<
15-
46.4
%
Life
exp
ecta
ncy
=
32
IM
R
=
11
2/1
00
0
%<
1/d
ay=
63.7
%G
ini
inde
x =
52.6
1
59
34
25
Zim
babw
e
DP
P,
CF
, R
BM
, G
AV
I,
GA
ELF
, G
FA
, (I
PA
AA
),
RB
M,
Sto
p
TB
, (V
DP
),
TM
US
$ 7
06
0
0
G
ini
inde
x:
56.8
-5
129
62
67
Afg
ha
nis
tan
GA
VI,
GA
EL,
GF
AT
M,
GP
EI,
Sto
p
TB
, (V
DP
)
N/a
0
P
op
ula
tion
=
22
m
illio
n
IMR
=
16
5/1
00
0
N/a
Gin
i in
de
x: n
/a
-7
28
11
17
EMRO
Bahra
in
U
S$
12,1
89
0.6
519
315
204
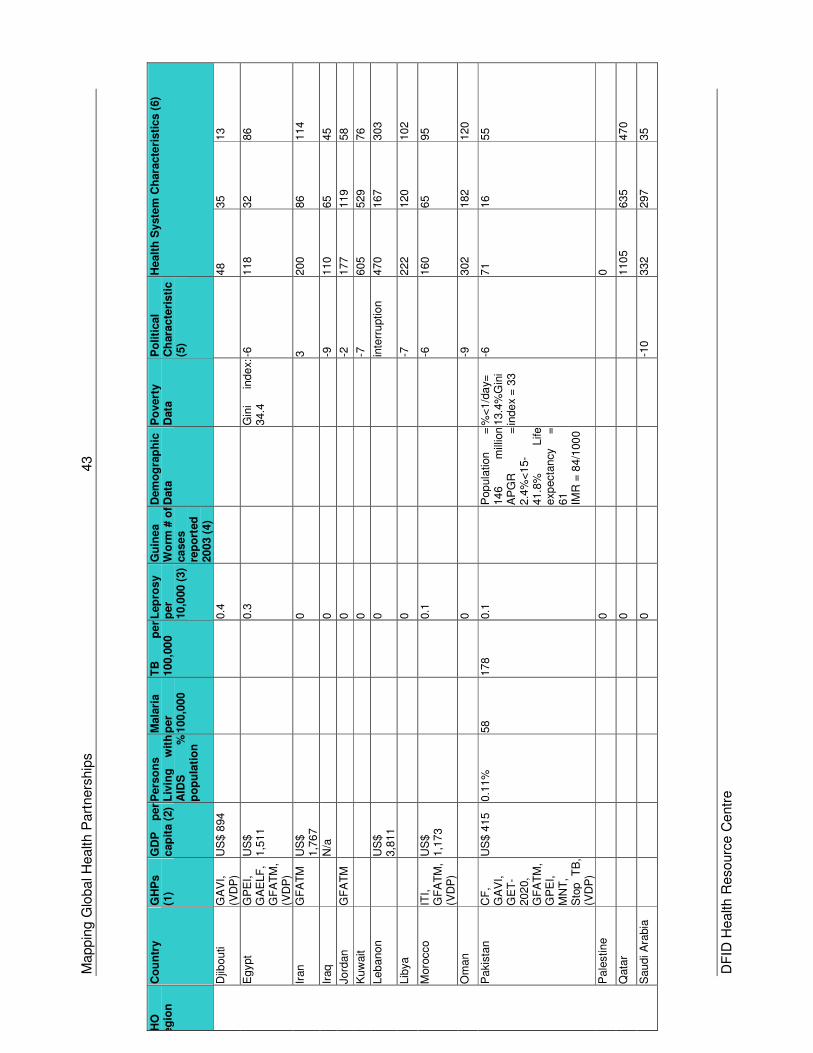
Mappin
g G
lobal H
ealth P
art
ners
hip
s
43
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Djib
outi
GA
VI,
(VD
P)
US
$ 8
94
0.4
48
35
13
Egypt
GP
EI,
GA
ELF
, G
FA
TM
, (V
DP
)
US
$
1,5
11
0.3
G
ini
inde
x:
34.4
-6
118
32
86
Iran
GF
AT
M
US
$
1,7
67
0
3
200
86
114
Iraq
N
/a
0
-9
110
65
45
Jord
an
GF
AT
M
0
-2
177
119
58
Kuw
ait
0
-7
605
529
76
Leb
anon
U
S$
3,8
11
0
in
terr
uption
470
167
303
Lib
ya
0
-7
222
120
102
Moro
cco
ITI,
G
FA
TM
, (V
DP
)
US
$
1,1
73
0.1
-6
160
65
95
Om
an
0
-9
302
182
120
Pakis
tan
CF
, G
AV
I,
GE
T-
202
0,
GF
AT
M,
GP
EI,
MN
T,
Sto
p
TB
, (V
DP
)
US
$ 4
15
0.1
1%
58
178
0.1
Pop
ula
tion
=
14
6
mill
ion
AP
GR
=
2.4
%<
15-
41.8
%
Life
exp
ecta
ncy
=
61
IMR
= 8
4/1
00
0
%<
1/d
ay=
13.4
%G
ini
inde
x =
33
-6
71
16
55
Pale
stine
0
0
Qata
r
0
110
5
635
470
Saudi A
rabia
0
-1
0
332
297
35
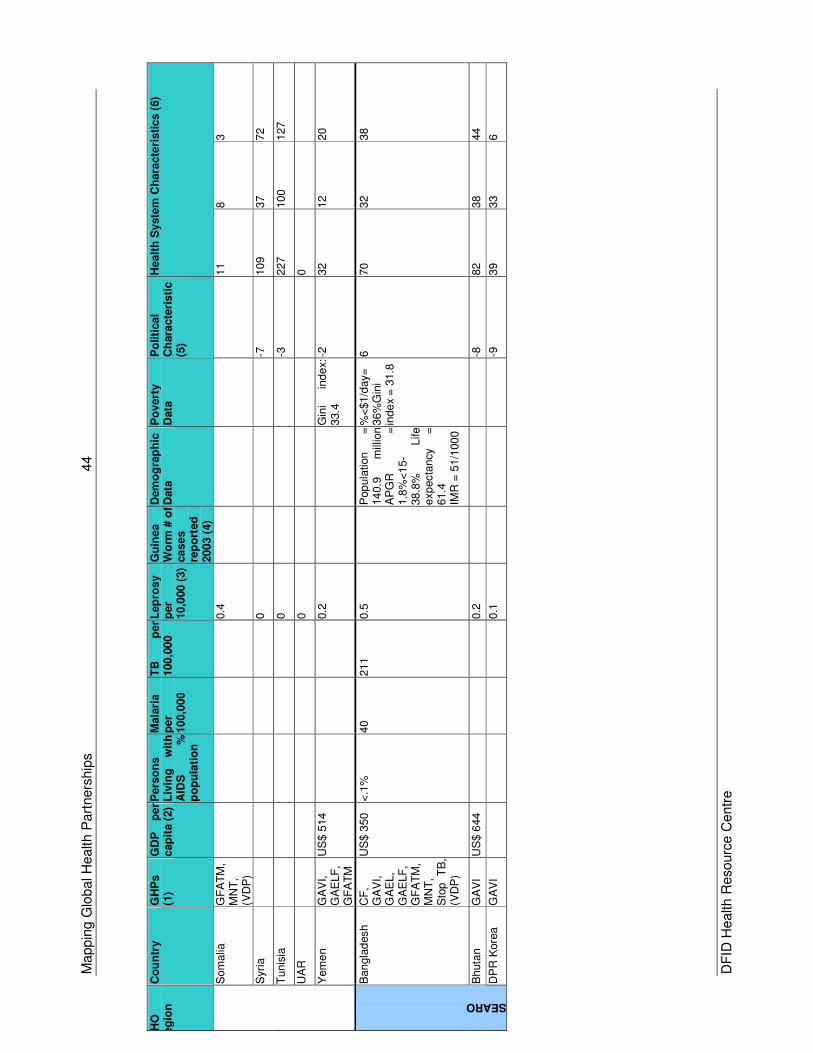
Mappin
g G
lobal H
ealth P
art
ners
hip
s
44
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Som
alia
G
FA
TM
, M
NT
, (V
DP
)
0.4
11
8
3
Syri
a
0
-7
109
37
72
Tunis
ia
0
-3
227
100
127
UA
R
0
0
Yem
en
GA
VI,
GA
ELF
, G
FA
TM
US
$ 5
14
0.2
G
ini
inde
x:
33.4
-2
32
12
20
Bangla
desh
CF
, G
AV
I,
GA
EL,
GA
ELF
, G
FA
TM
, M
NT
, S
top
TB
, (V
DP
)
US
$ 3
50
<.1
%
40
211
0.5
Pop
ula
tion
=
14
0.9
m
illio
n
AP
GR
=
1.8
%<
15-
38.8
%
Life
exp
ecta
ncy
=
61.4
IMR
= 5
1/1
00
0
%<
$1/d
ay=
36%
Gin
i in
de
x =
31.8
6
70
32
38
Bhuta
n
GA
VI
US
$ 6
44
0.2
-8
82
38
44
SEARO
DP
R K
ore
a
GA
VI
0.1
-9
39
33
6
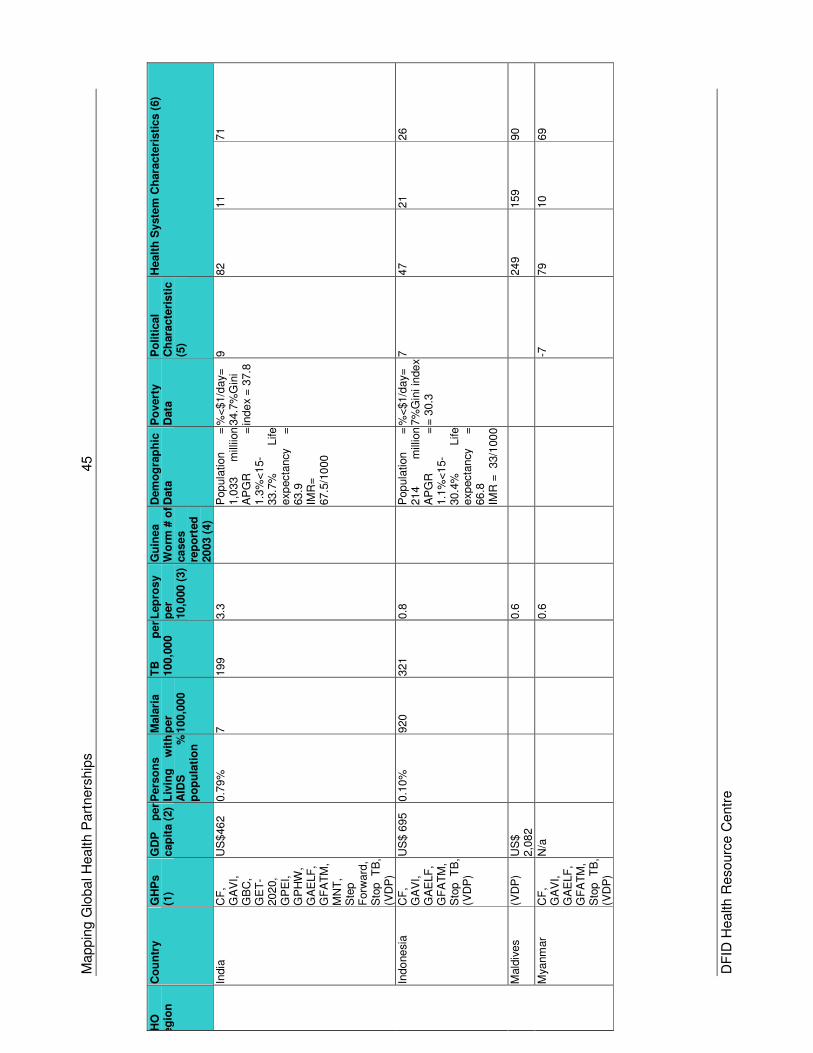
Mappin
g G
lobal H
ealth P
art
ners
hip
s
45
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
India
C
F,
GA
VI,
GB
C,
GE
T-
202
0,
GP
EI,
GP
HW
, G
AE
LF
, G
FA
TM
, M
NT
, S
tep
Forw
ard
, S
top
TB
, (V
DP
)
US
$46
2
0.7
9%
7
199
3.3
Pop
ula
tion
=
1,0
33
mill
iion
AP
GR
=
1.3
%<
15-
33.7
%
Life
exp
ecta
ncy
=
63.9
IM
R=
67.5
/10
00
%<
$1/d
ay=
34.7
%G
ini
inde
x =
37.8
9
82
11
71
Indo
nesia
C
F,
GA
VI,
GA
ELF
, G
FA
TM
, S
top
TB
, (V
DP
)
US
$ 6
95
0.1
0%
920
321
0.8
Pop
ula
tion
=
21
4
mill
ion
AP
GR
=
1.1
%<
15-
30.4
%
Life
exp
ecta
ncy
=
66.8
IMR
= 33/1
00
0 %
<$1/d
ay=
7%
Gin
i in
de
x
= 3
0.3
7
47
21
26
Mald
ives
(VD
P)
US
$
2,0
82
0.6
249
159
90
Mya
nm
ar
CF
, G
AV
I,
GA
ELF
, G
FA
TM
, S
top
TB
, (V
DP
)
N/a
0.6
-7
79
10
69
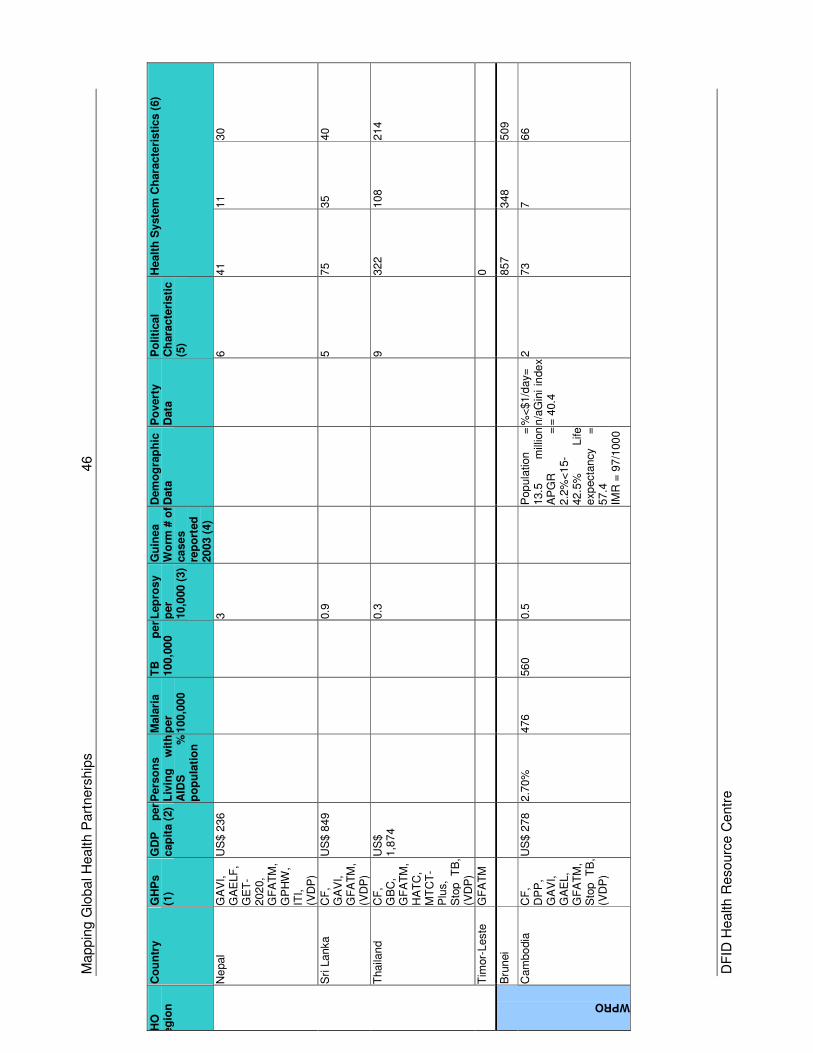
Mappin
g G
lobal H
ealth P
art
ners
hip
s
46
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Ne
pal
GA
VI,
GA
ELF
, G
ET
-202
0,
GF
AT
M,
GP
HW
, IT
I,
(VD
P)
US
$ 2
36
3
6
41
11
30
Sri
Lanka
CF
, G
AV
I,
GF
AT
M,
(VD
P)
US
$ 8
49
0.9
5
75
35
40
Thaila
nd
CF
, G
BC
, G
FA
TM
, H
AT
C,
MT
CT
-P
lus,
Sto
p
TB
, (V
DP
)
US
$
1,8
74
0.3
9
322
108
214
Tim
or-
Leste
G
FA
TM
0
Bru
nei
857
348
509
WPRO
Cam
bo
dia
C
F,
DP
P,
GA
VI,
GA
EL,
GF
AT
M,
Sto
p
TB
, (V
DP
)
US
$ 2
78
2.7
0%
476
560
0.5
Pop
ula
tion
=
13.5
m
illio
n
A
PG
R
=
2.2
%<
15-
42.5
%
Life
exp
ecta
ncy
=
57.4
IMR
= 9
7/1
00
0
%<
$1/d
ay=
n/a
Gin
i in
de
x
= 4
0.4
2
73
7
66
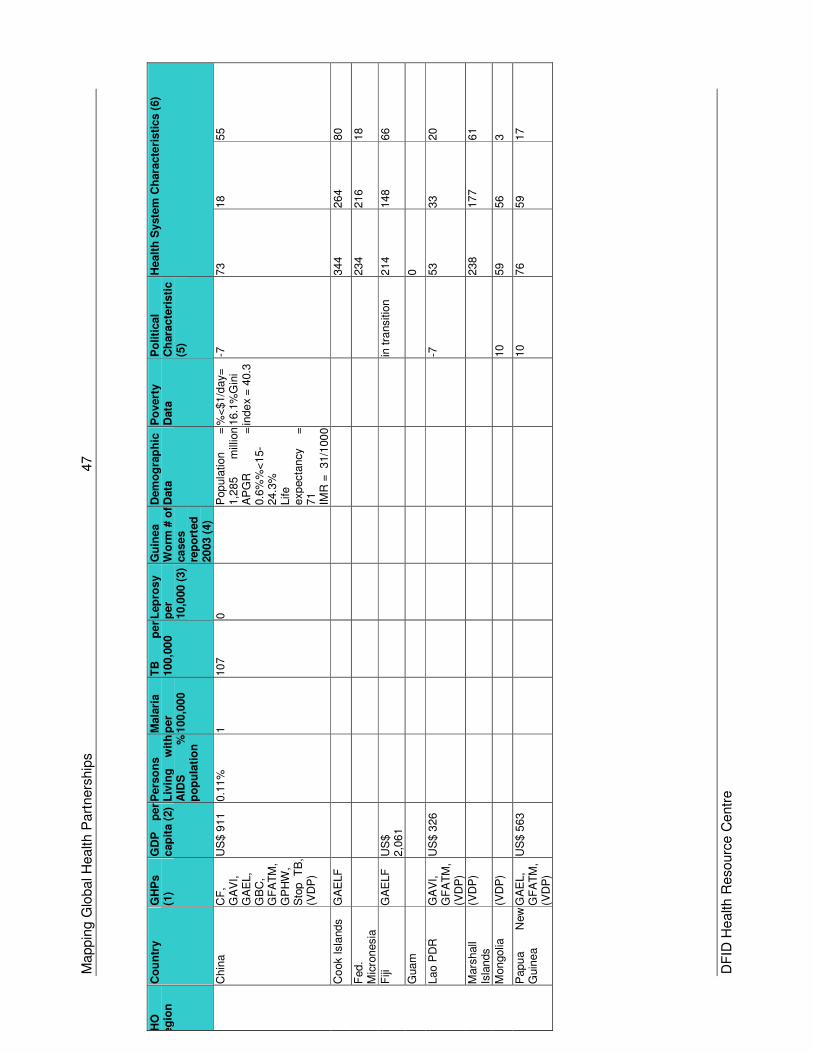
Mappin
g G
lobal H
ealth P
art
ners
hip
s
47
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Chin
a
CF
, G
AV
I,
GA
EL,
GB
C,
GF
AT
M,
GP
HW
, S
top
TB
, (V
DP
)
US
$ 9
11
0.1
1%
1
107
0
P
op
ula
tion
=
1,2
85
mill
ion
A
PG
R
=
0.6
%%
<1
5-
24.3
%
Life
exp
ecta
ncy
=
71
IM
R =
31/1
00
0 %
<$1/d
ay=
16.1
%G
ini
inde
x =
40.3
-7
73
18
55
Co
ok Isla
nds
GA
ELF
344
264
80
Fed.
Mic
ronesia
234
216
18
Fiji
G
AE
LF
U
S$
2,0
61
in
tra
nsitio
n
214
148
66
Guam
0
Lao P
DR
G
AV
I,
GF
AT
M,
(VD
P)
US
$ 3
26
-7
53
33
20
Mars
hall
Isla
nds
(VD
P)
238
177
61
Mon
golia
(V
DP
)
10
59
56
3
Papu
a
New
G
uin
ea
GA
EL,
GF
AT
M,
(VD
P)
US
$ 5
63
10
76
59
17
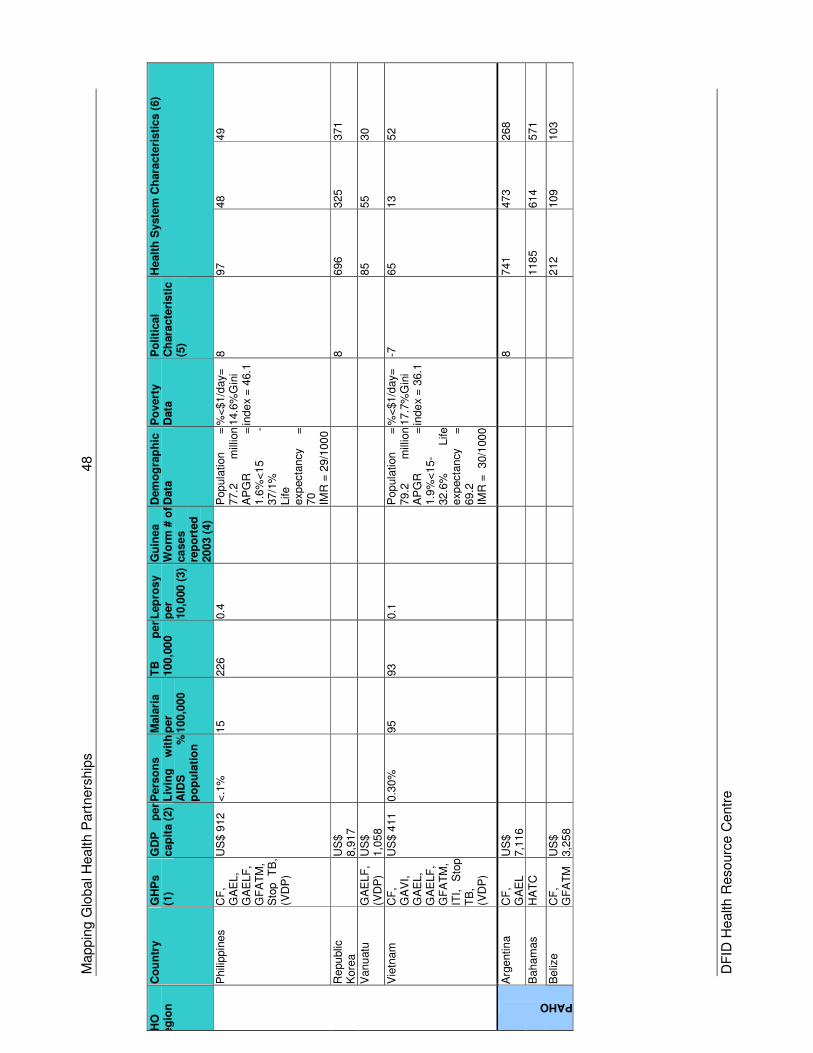
Mappin
g G
lobal H
ealth P
art
ners
hip
s
48
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Phili
ppin
es
CF
, G
AE
L,
GA
ELF
, G
FA
TM
, S
top
TB
, (V
DP
)
US
$ 9
12
<.1
%
15
226
0.4
Pop
ula
tion
=
77.2
m
illio
n
AP
GR
=
1.6
%<
15
-37/1
%
Life
exp
ecta
ncy
=
70
IMR
= 2
9/1
00
0
%<
$1/d
ay=
14.6
%G
ini
inde
x =
46.1
8
97
48
49
Re
pu
blic
K
ore
a
U
S$
8,9
17
8
696
325
371
Vanu
atu
G
AE
LF
, (V
DP
) U
S$
1,0
58
85
55
30
Vie
tnam
C
F,
GA
VI,
GA
EL,
GA
ELF
, G
FA
TM
, IT
I,
Sto
p
TB
, (V
DP
)
US
$ 4
11
0.3
0%
95
93
0.1
Pop
ula
tion
=
79.2
m
illio
n
AP
GR
=
1.9
%<
15-
32.6
%
Life
exp
ecta
ncy
=
69.2
IMR
= 30/1
00
0 %
<$1/d
ay=
17.7
%G
ini
inde
x =
36.1
-7
65
13
52
Arg
entin
a
CF
, G
AE
L
US
$
7,1
16
8
741
473
268
Baham
as
HA
TC
118
5
614
571
PAHO
Beliz
e
CF
, G
FA
TM
U
S$
3,2
58
212
109
103
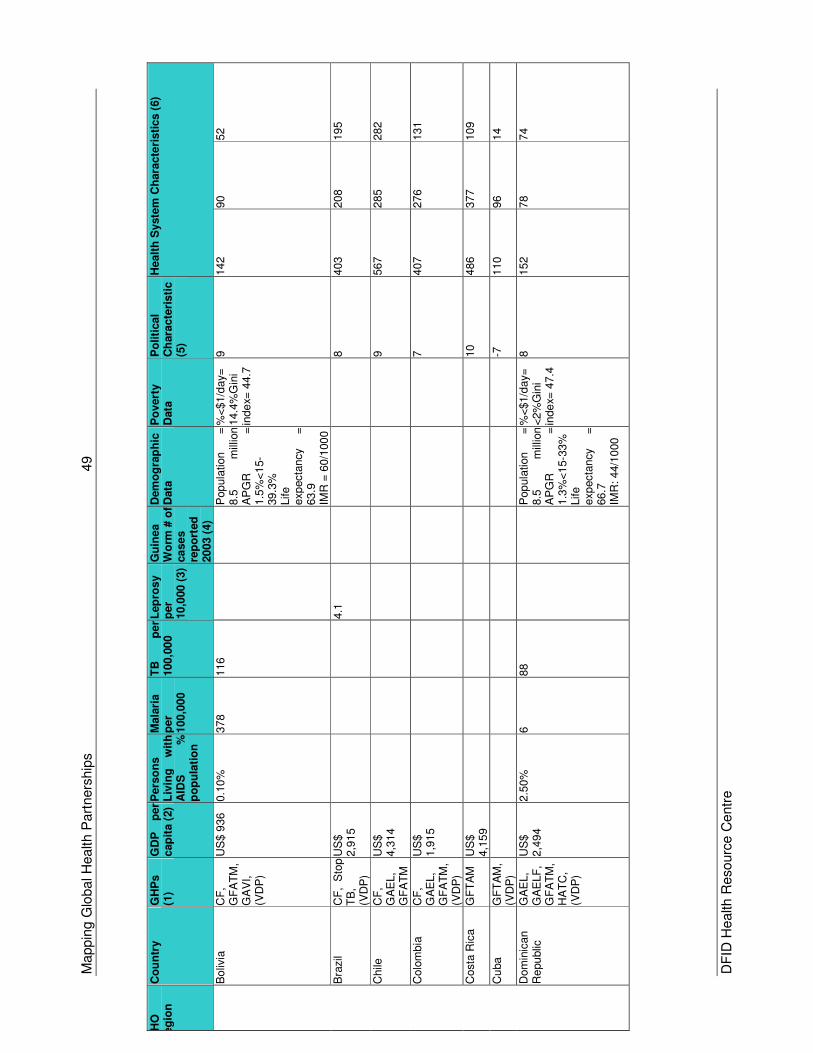
Mappin
g G
lobal H
ealth P
art
ners
hip
s
49
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Boliv
ia
CF
, G
FA
TM
, G
AV
I,
(VD
P)
US
$ 9
36
0.1
0%
378
116
Pop
ula
tion
=
8.5
m
illio
n
AP
GR
=
1.5
%<
15-
39.3
%
Life
exp
ecta
ncy
=
63.9
IMR
= 6
0/1
00
0
%<
$1/d
ay=
14.4
%G
ini
inde
x= 4
4.7
9
142
90
52
Bra
zil
CF
, S
top
TB
, (V
DP
)
US
$
2,9
15
4.1
8
403
208
195
Chile
C
F,
GA
EL,
GF
AT
M
US
$
4,3
14
9
567
285
282
Colo
mbia
C
F,
GA
EL,
GF
AT
M,
(VD
P)
US
$
1,9
15
7
407
276
131
Costa
Ric
a
GF
TA
M
US
$
4,1
59
10
486
377
109
Cu
ba
GF
TA
M,
(VD
P)
-7
110
96
14
Dom
inic
an
Re
pu
blic
G
AE
L,
GA
ELF
, G
FA
TM
, H
AT
C,
(VD
P)
US
$
2,4
94
2.5
0%
6
88
Pop
ula
tion
=
8.5
m
illio
n
A
PG
R
=
1.3
%<
15-3
3%
Life
exp
ecta
ncy
=
66.7
IMR
: 44/1
000
%<
$1/d
ay=
<
2%
Gin
i in
de
x= 4
7.4
8
152
78
74
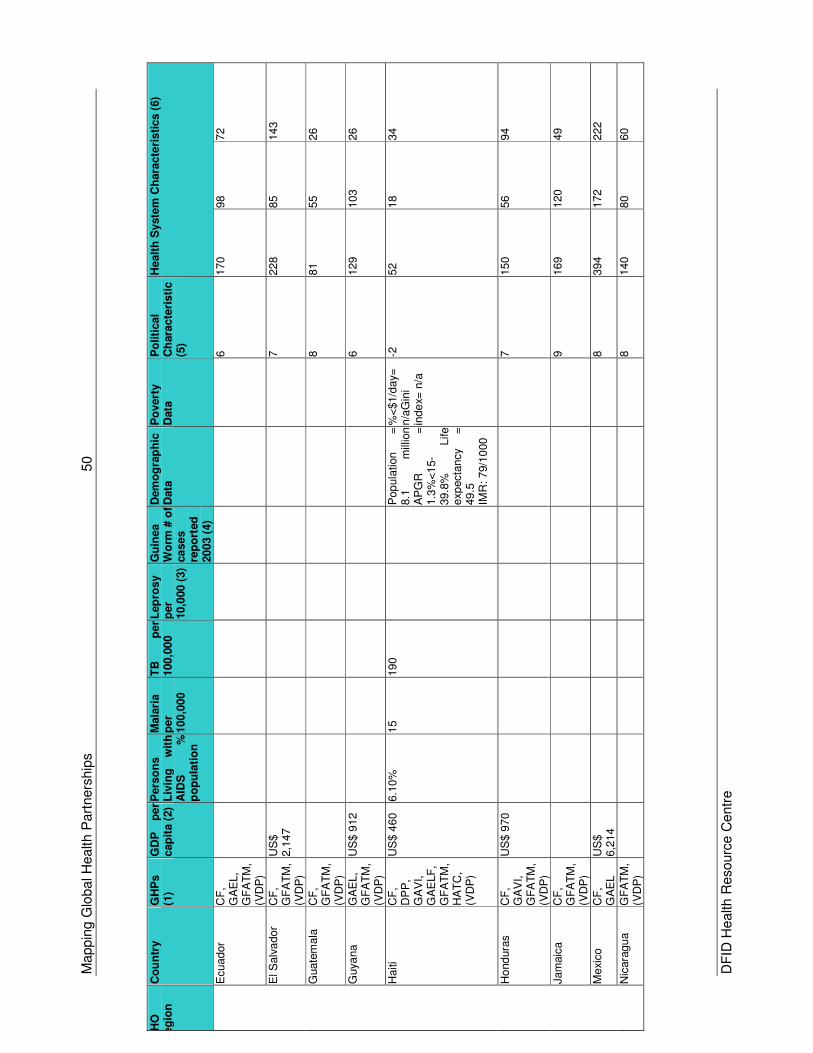
Mappin
g G
lobal H
ealth P
art
ners
hip
s
50
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Ecuador
CF
, G
AE
L,
GF
AT
M,
(VD
P)
6
170
98
72
El S
alv
ador
CF
, G
FA
TM
, (V
DP
)
US
$
2,1
47
7
228
85
143
Guate
mala
C
F,
GF
AT
M,
(VD
P)
8
81
55
26
Guya
na
GA
EL,
GF
AT
M,
(VD
P)
US
$ 9
12
6
129
103
26
Haiti
CF
, D
PP
, G
AV
I,
GA
ELF
, G
FA
TM
, H
AT
C,
(VD
P)
US
$ 4
60
6.1
0%
15
190
Pop
ula
tion
=
8.1
m
illio
n
AP
GR
=
1.3
%<
15-
39.8
%
Life
exp
ecta
ncy
=
49.5
IM
R: 79/1
000
%<
$1/d
ay=
n/a
Gin
i in
de
x= n
/a
-2
52
18
34
Ho
nd
ura
s
CF
, G
AV
I,
GF
AT
M,
(VD
P)
US
$ 9
70
7
150
56
94
Jam
aic
a
CF
, G
FA
TM
, (V
DP
)
9
169
120
49
Mexi
co
CF
, G
AE
L
US
$
6,2
14
8
394
172
222
Nic
ara
gua
GF
AT
M,
(VD
P)
8
140
80
60
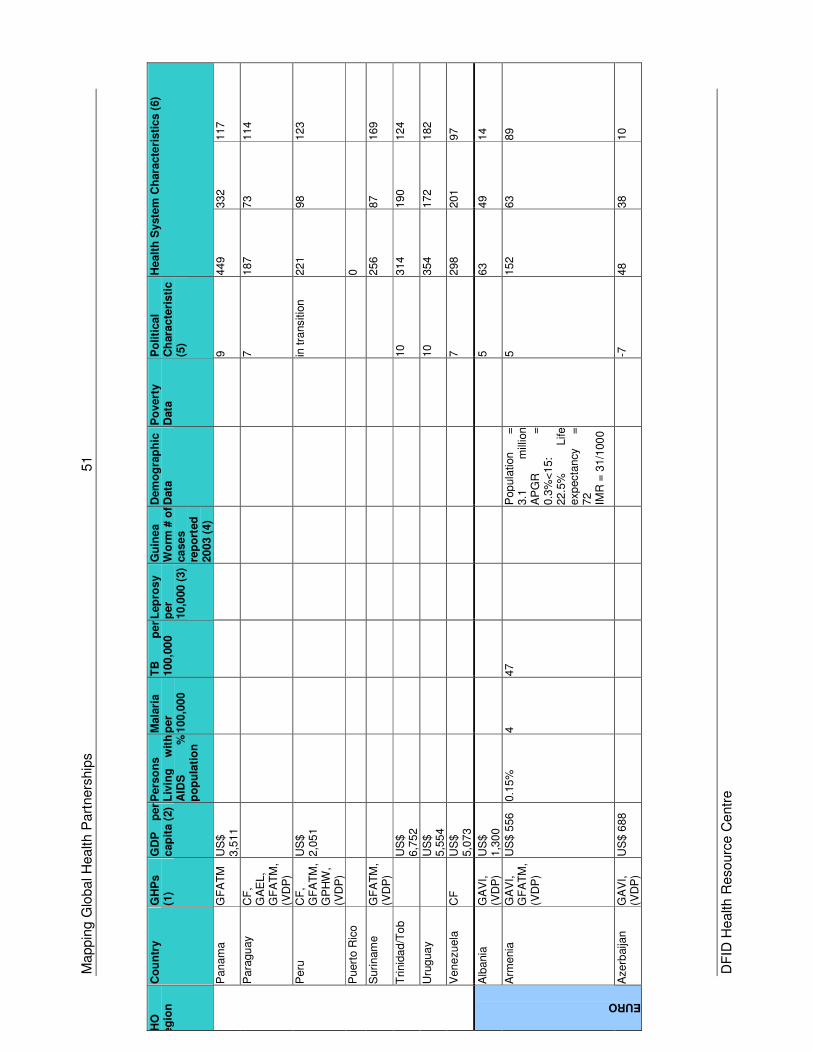
Mappin
g G
lobal H
ealth P
art
ners
hip
s
51
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Panam
a
GF
AT
M
US
$
3,5
11
9
449
332
117
Para
gu
ay
CF
, G
AE
L,
GF
AT
M,
(VD
P)
7
187
73
114
Peru
C
F,
GF
AT
M,
GP
HW
, (V
DP
)
US
$
2,0
51
in
tra
nsitio
n
221
98
123
Puert
o R
ico
0
Suri
nam
e
GF
AT
M,
(VD
P)
256
87
169
Trinid
ad/T
ob
U
S$
6,7
52
10
314
190
124
Uru
gua
y
US
$
5,5
54
10
354
172
182
Vene
zuela
C
F
US
$
5,0
73
7
298
201
97
Alb
ania
G
AV
I,
(VD
P)
US
$
1,3
00
5
63
49
14
Arm
enia
G
AV
I,
GF
AT
M,
(VD
P)
US
$ 5
56
0.1
5%
4
47
Pop
ula
tion
=
3.1
m
illio
n
AP
GR
=
0.3
%<
15:
22.5
%
Life
exp
ecta
ncy
=
72
IM
R =
31/1
00
0
5
152
63
89
EURO
Azerb
aija
n
GA
VI,
(VD
P)
US
$ 6
88
-7
48
38
10
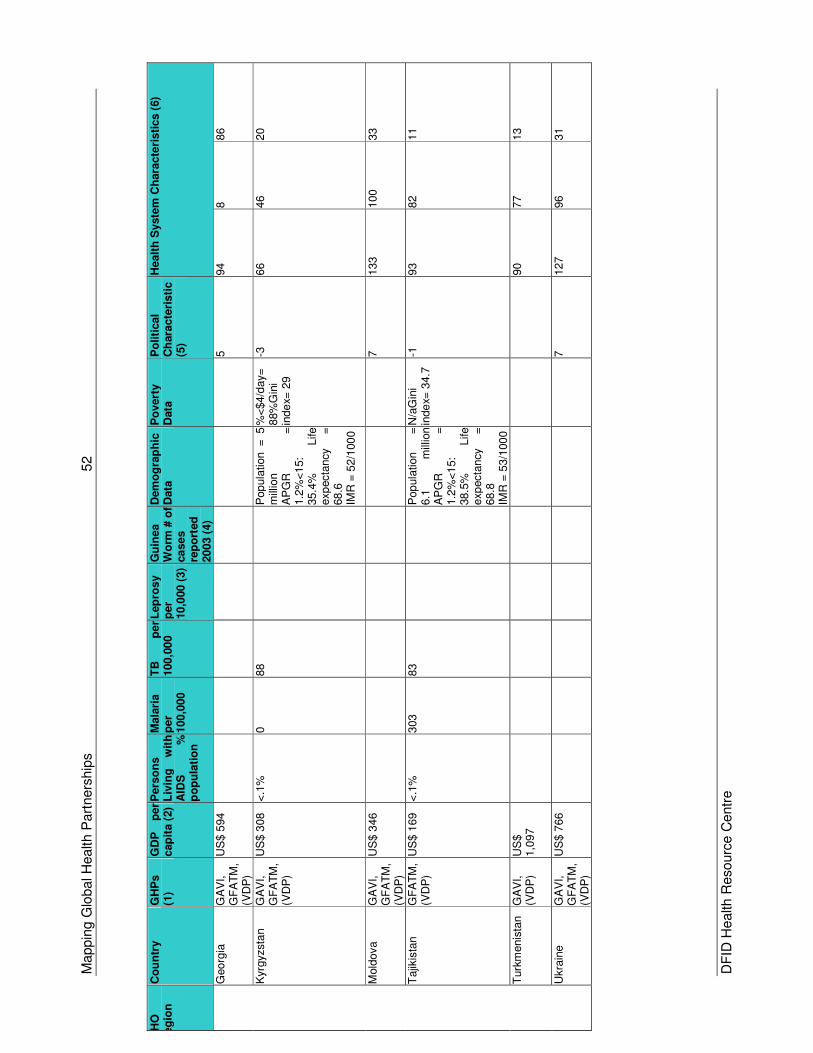
Mappin
g G
lobal H
ealth P
art
ners
hip
s
52
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Georg
ia
GA
VI,
GF
AT
M,
(VD
P)
US
$ 5
94
5
94
8
86
Kyrg
yzsta
n
GA
VI,
GF
AT
M,
(VD
P)
US
$ 3
08
<.1
%
0
88
Pop
ula
tion =
5
m
illio
n
AP
GR
=
1.2
%<
15:
35.4
%
Life
exp
ecta
ncy
=
68.6
IMR
= 5
2/1
00
0
%<
$4/d
ay=
88%
Gin
i in
de
x= 2
9
-3
66
46
20
Mold
ova
GA
VI,
GF
AT
M,
(VD
P)
US
$ 3
46
7
133
100
33
Tajik
ista
n
GF
AT
M,
(VD
P)
US
$ 1
69
<.1
%
303
83
Pop
ula
tion
=
6.1
m
illio
n
A
PG
R
=
1.2
%<
15:
38.5
%
Life
exp
ecta
ncy
=
68.8
IMR
= 5
3/1
00
0
N/a
Gin
i in
de
x= 3
4.7
-1
93
82
11
Turk
menis
tan
GA
VI,
(VD
P)
US
$
1,0
97
90
77
13
Ukra
ine
GA
VI,
GF
AT
M,
(VD
P)
US
$ 7
66
7
127
96
31
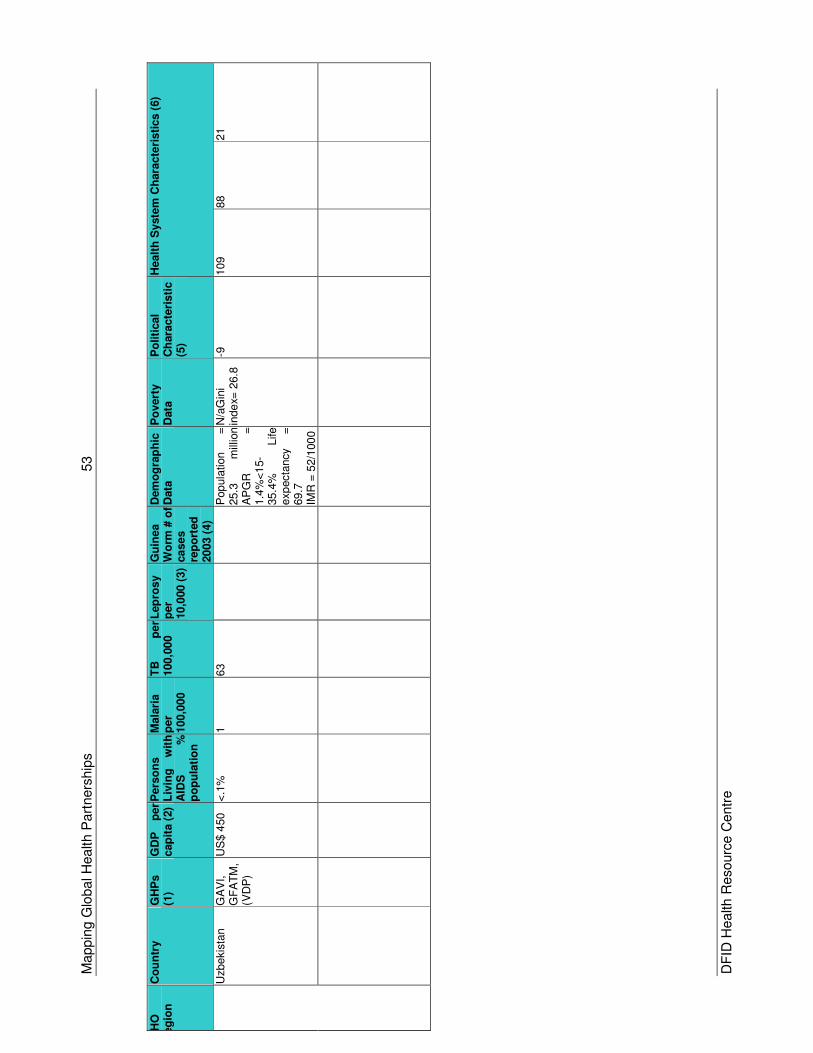
Mappin
g G
lobal H
ealth P
art
ners
hip
s
53
DF
ID H
ealth R
esourc
e C
entr
e
WH
O
Reg
ion
C
ou
ntr
y
GH
Ps
(1)
GD
P
per
cap
ita (
2)
Pers
on
s
Liv
ing
w
ith
A
IDS
%
p
op
ula
tio
n
Mala
ria
per
100,0
00
TB
p
er
100,0
00
Lep
rosy
per
10,0
00 (
3)
Gu
inea
Wo
rm #
of
ca
se
s
rep
ort
ed
20
03 (
4)
Dem
og
rap
hic
D
ata
P
overt
y
Data
P
oliti
cal
Ch
ara
cte
risti
c
(5)
Healt
h S
yste
m C
hara
cte
risti
cs (
6)
Uzbekis
tan
GA
VI,
GF
AT
M,
(VD
P)
US
$ 4
50
<.1
%
1
63
Pop
ula
tion
=
25.3
m
illio
n
AP
GR
=
1.4
%<
15-
35.4
%
Life
exp
ecta
ncy
=
69.7
IM
R =
52/1
00
0
N/a
Gin
i in
de
x= 2
6.8
-9
109
88
21
Mapping Global Health Partnerships 54
DFID Health Resource Centre
Key to GHP Mapping Tables *A GHP in brackets covers the country but does not necessarily operate in it at present (1) GHP information was provided from individual GHP websites. Therefore the
information is only as accurate and up to date as the websites are themselves. (2) All figures and definitions are from the UNDP’s Human Development Report
2003, unless otherwise stated.
GDP =.GDP converted to US dollars using the average official exchange rate reported by the International Monetary Fund. An alternative conversion factor is applied if the official exchange rate is judged to diverge by an exceptionally large margin from the rate effectively applied to transactions in foreign currencies and traded products. Epidemiological information: PLA = Estimated percentage of Adults between the ages of 15 and 45 living with AIDS at the end of the year. Malaria figures represent total number of cases report by the country to the WHO, divided by the total population and then multiplied by 100,000 to give a comparison rate. A similar calculation is made for TB (tuberculosis) to provide a TB case rate.
Demographic Data: All population figures are 2001 estimates. APGR = Annual Population Growth Rate – the APGRs presented here are the estimated ones for 2001-2015. %<15 is the Percentage of the Population aged less than 15 in 2001. Poverty data: Population below income poverty line - This is set of < US$ 1 per day for low and some medium income countries. For OECD, CIS and CCE countries this is set at a series of levels, including <US$ 4/day, or the national poverty line. A further indicator of the distribution of income is the Gini index. The Gini index is used to measure the extent to which income distribution between individuals and families in a country deviates from equal distribution. A ‘0’ represents perfect equality while ‘100’ represents perfect inequality. To put this into context, the Gini index for the Nordic countries is around 25. For the US it is 40.8, and for the UK it is 36.
(3) Leprosy prevalence: information was provided by ILEP (International Leprosy
Eradication Partners) 2002/2003 annual report, available on their website. (4) Guinea Worm cases: information was provided by the Guinea Worm Eradication
Programme’s website. (5) Political system: Measures of polity taken from EarthTrends 2003 report, which
provides information on the degree of democracy in individual countries. (EarthTrends Data Tables: Environmental Governance and Institutions)
(6) Health Systems information: Public v Private – based on data presented in the
World Health Report 2000 Table 8 – National Health Accounts (7) Sierra Leone malaria prevalence: Provided by the Statistics for Sierra Leone
website, relating to 2002 prevalence.
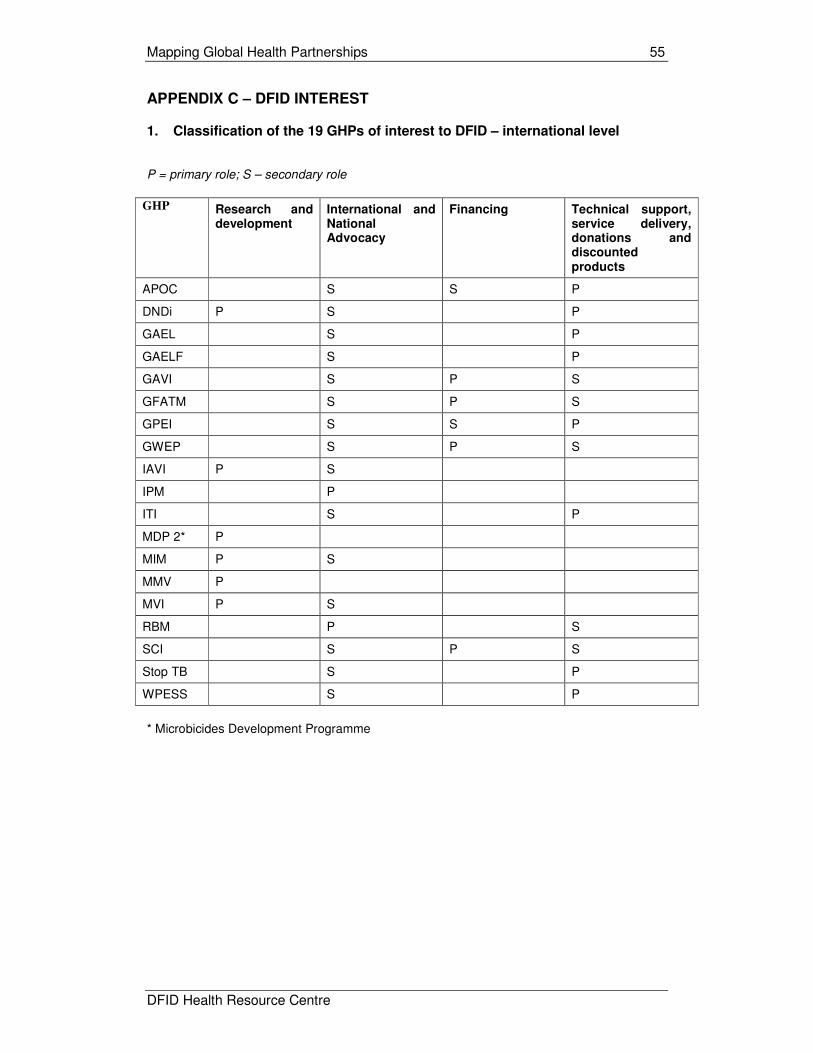
Mapping Global Health Partnerships 55
DFID Health Resource Centre
APPENDIX C – DFID INTEREST 1. Classification of the 19 GHPs of interest to DFID – international level P = primary role; S – secondary role
GHP Research and
development
International and National Advocacy
Financing Technical support, service delivery, donations and discounted products
APOC S S P
DNDi P S P
GAEL S P
GAELF S P
GAVI S P S
GFATM S P S
GPEI S S P
GWEP S P S
IAVI P S
IPM P
ITI S P
MDP 2* P
MIM P S
MMV P
MVI P S
RBM P S
SCI S P S
Stop TB S P
WPESS S P
* Microbicides Development Programme
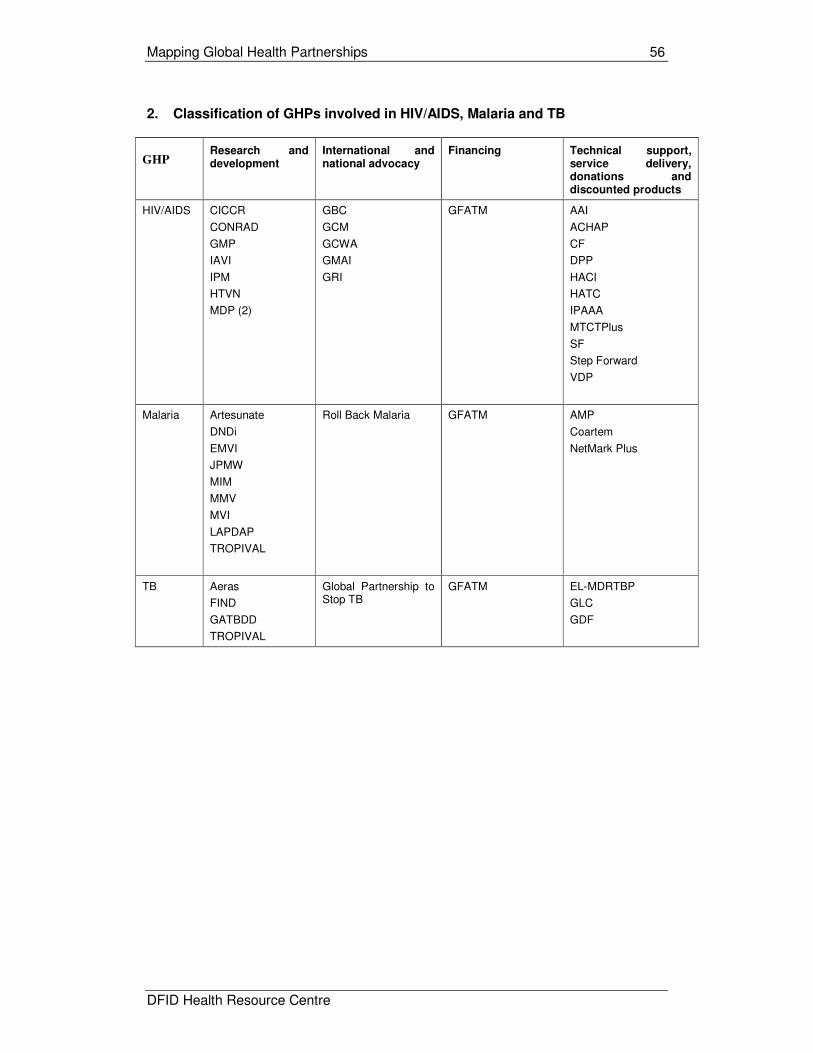
Mapping Global Health Partnerships 56
DFID Health Resource Centre
2. Classification of GHPs involved in HIV/AIDS, Malaria and TB
GHP Research and development
International and national advocacy
Financing Technical support, service delivery, donations and discounted products
HIV/AIDS CICCR
CONRAD
GMP
IAVI
IPM
HTVN
MDP (2)
GBC
GCM
GCWA
GMAI
GRI
GFATM AAI
ACHAP
CF
DPP
HACI
HATC
IPAAA
MTCTPlus
SF
Step Forward
VDP
Malaria Artesunate
DNDi
EMVI
JPMW
MIM
MMV
MVI
LAPDAP
TROPIVAL
Roll Back Malaria GFATM AMP
Coartem
NetMark Plus
TB Aeras
FIND
GATBDD
TROPIVAL
Global Partnership to Stop TB
GFATM EL-MDRTBP
GLC
GDF