many faces of tb · • travelled toto pipi 44 yearsyears agoago. 50 yomanwithman with diabetes •...
TRANSCRIPT

ManyfacesofTB:D i t t TB S i l G id 3Drug‐resistantTBSurvivalGuidev3
P B L Ch G S h t L TP. Barry, L. Chen, G. Schecter, L. TrueCurry International TB Center/CTCAApril 20, 2016

Real caseRealcasePractical
Walk throughNew Survival Guide

50 yomanwith diabetes50yomanwithdiabetes
• Philippines to US late 1990’sPhilippines to US late 1990 s• Hemoptysis x several weeks• Works in bankingWorks in banking• Tobacco hx• Travelled to PI 4 years ago• Travelled to PI 4 years ago

50 yomanwith diabetes50yomanwithdiabetes
• Philippines to US late 1990’sPhilippines to US late 1990 s• Hemoptysis x several weeks• Works in bankingWorks in banking• Tobacco hx• Travelled to PI 4 years ago• Travelled to PI 4 years ago
Let’s talk about risk factors…

TBRatebyDiabetes,Age,andNativityCalifornia 2010–2012California,2010 2012(Personsaged≥18)
80
100
0,00
0
Diabetes No Diabetes
60
te per 100
20
40
Case Rat
018‐44 45‐64 65‐74 75+ 18‐44 45‐64 65‐74 75+
United States or Canada Foreign‐born
5Demlow et al, BMC Public Health 2015Sources: Denominator: 2011‐2012 California Health Interview Survey | Numerator: CA TB Registry
What is the added value of NAAT?WhatistheaddedvalueofNAAT?• For AFB smear (–):
• 50‐70% of smear –/culture + cases will be + by NAAT start treatment (earlier)
• If NAAT (–), the likelihood of TB lower( ),• Release from isolation earlier (2 Xpert results finds all smear +)
• Still start treatment if suspicion is high• Still start treatment if suspicion is high• For AFB smear (+):
• NAAT can confirm TB quicklyNAAT can confirm TB quickly • If NAAT negative, prevent falsely diagnosing TB(likely NTM if inhibitors are ruled out and result repeated)repeated)
Luetkemeyer Clin Infect Dis 2016 6

XpertMTB/RIFTestPerformanced h lComparedwithCulture,U.S.patients
S i i i S ifi iSensitivity Specificity
1 X t 2 X t1 Xpert 2 Xperts
Smear (+) 96.7% 100%Smear (+) 96.7%(59/61)
100%(62/62)
99.2%Smear (–) 59.3% 71.4%Smear (–) 59.3%
(16/27)71.4%
(20/28)
Luetkemeyer Clin Infect Dis 2016 7
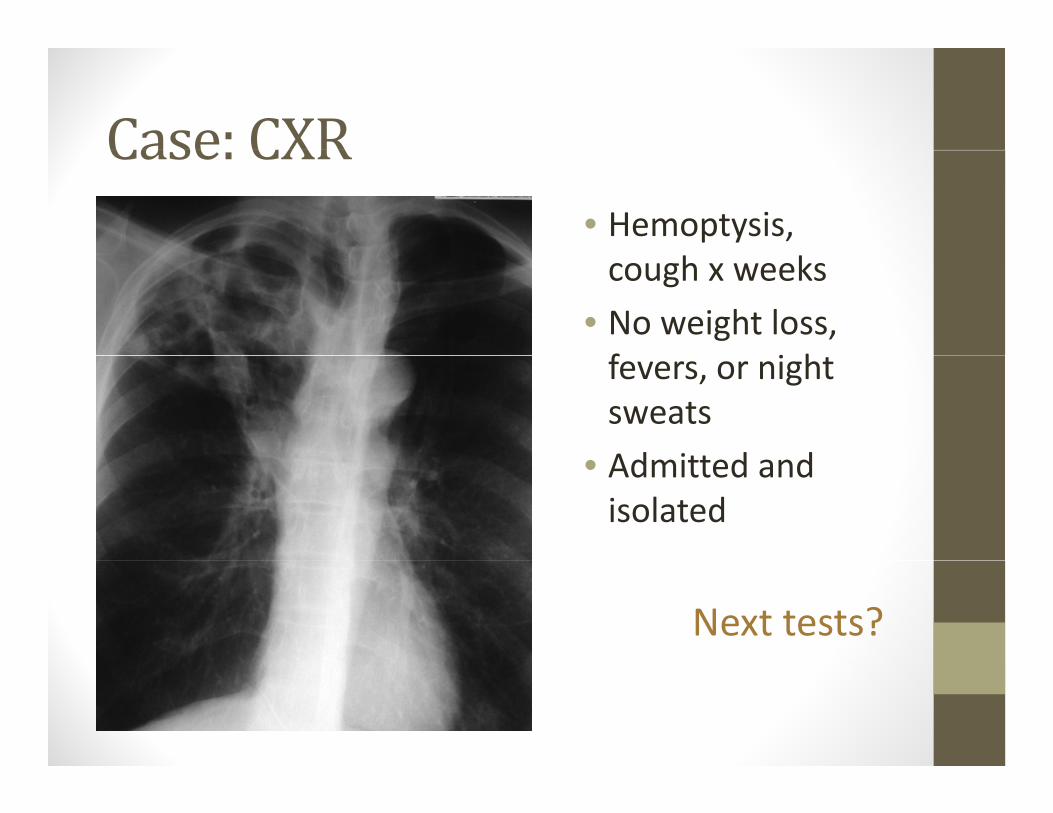
Case: CXRCase:CXR• Hemoptysis, cough x weeks
• No weight loss, f i hfevers, or night sweatsAd itt d d• Admitted and isolated
Next tests?

Initial diagnostic testsInitialdiagnostictests• Smear positive x3 (cultures sent)p ( )
• Xpert MTB/RIF:Xpert MTB/RIF: • Positive for Mtb and RIF resistance
BenefitsofMolecularTestsforDrugResistance
d d i d i f i• Reduced time to detection of resistance• Time from empiric (first‐line) treatment to MDR treatment 40 days less (median)treatment 40 days less (median)
• Less transmission• Less acquired resistance while DSTs pendingq p g• Less ineffective LTBI treatment given to contacts
Banerjee et al, J Clin Micro, 2010 10

Xpert PerformanceRifampinResistanceP l d di i i i• Pooled median sensitivity: • 95% (95% CrI: 90, 97)
• Pooled median specificity: • 98% (95% CrI: 97, 99)
Steingart 2014 Cochrane Review (http://tbevidence.org/wp‐content/uploads/2014/01/Steingart‐Cochrane‐Library‐Updated‐Xpert‐SR.pdf) 11

Chapter 3, page 53

Xpert Probes: Coverage of rpoBXpertProbes:CoverageofrpoB
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
Codon#
Most common Most common isilent mutation
(514 TTT)resistance
mutation (531 TTG)
Location of silent mutation Location of missense mutation

NumberandProportionMDRTBbyCountry/Region of Origin CA2009 2013Country/RegionofOrigin,CA2009–2013
Country/Region No. %Former Soviet Republics 8 14.5pLaos 5 4.3Korea, North and South 11 4.1Burma 2 3.4India 10 2.6Central America 9 2.2Peru 1 2.0Ethiopia 1 1.9Vietnam 17 1.9Philippines 25 1.6Kampuchea 2 1.4China (incl Taiwan) 7 1.2Mexico 16 0.8
• Countries with >50 cases tested for MDR
United States 8 0.5
14

NumberandProportionMDRTBbyCountry/Region of Origin CA2009 2013Country/RegionofOrigin,CA2009–2013
Country/Region No. %PPV
(99% spec)PPV
(98% spec)Former Soviet Republics 8 14.5 94% 89%Laos 5 4.3 81% 68%Korea, North and South 11 4.1 80% 67%B 2 3 4 77% 63%Burma 2 3.4 77% 63%India 10 2.6 72% 56%Central America 9 2.2 68% 52%P 1 2 0 66% 50%Peru 1 2.0 66% 50%Ethiopia 1 1.9 65% 48%Vietnam 17 1.9 65% 48%Philippines 25 1 6 61% 44%Philippines 25 1.6 61% 44%Kampuchea 2 1.4 57% 41%China (incl Taiwan) 7 1.2 54% 37%Mexico 16 0 8 44% 28%
• Countries with >50 cases tested for MDR
Mexico 16 0.8 44% 28%United States 8 0.5 33% 20%
15

MDRTBCasesbyCountry/RegionofOrigind Y i h US CA2009 2013andYearsintheUS,CA2009‐2013
Total <= 2 years
Country/RegionMDR TB cases
in USNo. (%)
>2 years in USNo. (%)
All Countries (excl US)* 123 29 (3.3) 93 (1.5)
Former Soviet Republics 8 3 (33.3) 5 (10.9)
Vietnam* 17 8 (7.1) 8 (1.1)
China (incl Taiwan)* 7 4 (6.4) 3 (0.6)China (incl Taiwan) 7 4 (6.4) 3 (0.6)
Philippines* 25 7 (3.6) 18 (1.4)
Central America 9 2 (3.5) 7 (2.1)
I di 10 2 (2 2) 8 (2 9)India 10 2 (2.2) 8 (2.9)
All Other Countries 20 3 (1.7) 17 (1.9)
Mexico 16 0 (0.0) 16 (0.9)
Korea, North and South 11 0 (0.0) 11 (4.5)
16* Difference is statistically significant.

Increased Risk forMDR‐TB?IncreasedRiskforMDR TB?• Foreign‐born patients from countries or groups with high prevalence of MDR• In California: Hmong refugees Tibetan ancestry
f f Immigrants from former USSR, Laos, Burma, Korea, Peru, Central America, India Recent immigrants (e g within 2 years) especially Recent immigrants (e.g., within 2 years) especially from China, Vietnam, Philippines

Increased Risk forMDR‐TBIncreasedRiskforMDR TB• History of previous TB treatment, particularly if tif recent
• Poor response to standard 4‐drug treatment
Culture remains (+) after 2 months treatment
• Known exposure to MDR TB case• Known exposure to MDR‐TB case
• HIV (+) Higher incidence of Rifampin mono‐resistance

Chapter 3, page 48

Initial diagnostic testsInitialdiagnostictests• Smear positive x3 (cultures sent)p ( )
• Xpert MTB/RIF:Xpert MTB/RIF: • Positive for Mtb and RIF resistance
• PSQ: • rpoBmutationrpoBmutation• No gyrA, rrs, inhA, or katG

MolecularTestingforRifampin(rpoB)• Rifampin cornerstone of TB treatment
• Resistance requires a longer duration of therapy• Rif resistance without INH resistance rare~90% (114 of 129) Rif resistant cases MDR (California, 2011‐2015)90% (114 of 129) Rif resistant cases MDR (California, 2011 2015)
MDR Rif mono RMDR Rif mono R
0% 20% 40% 60% 80% 100%
Rif resistance ≈ MDR
0% 20% 40% 60% 80% 100%
Basic steps: Choosing a regimenBasicsteps:Choosingaregimen
• Decision: Begin empiric MDR regimen
• Ask for help: Expert consultation
• Empiric (expanded) regimen for MDR:• 4 first‐line + FQ + injectable(+ consider additional second‐line drug)
• This case (Xpert, then PSQ results)?

Howmany drugs forMDR?HowmanydrugsforMDR?Goal: “4‐6 likely effective drugs Goa : 6 e y e ect e d ugs
(and optimally at least 5)”
• Recent studies suggest better outcomes with atRecent studies suggest better outcomes with at least 5 drugs
• Expert input:Expert input: • Consider more if extensive disease and/or
resistance• Four may be sufficient with limited disease
and/or limited resistance[WHO 2011 “ t l t 4 lik l ff ti d ”]• [WHO 2011 – “at least 4 likely effective drugs”]

BuildinganIndividualizedRegimenfor
Use any One of One of
MDR‐TB
STEP 1 Useanyavailable
Oneofthese
Oneofthese
First‐line Fluoro‐ Injectable
STEP1BeginwithanyFi t li t st e
drugsuo o
quinolonesjectab eagents
Pyrazinamide Levofloxacin Amikacin
First‐lineagentstowhichtheisolateis
ibly
Ethambutol Moxifloxacin Capreomycin
Kanamycin1
susceptible
Addafluoroquinolone
Streptomycin2fluoroquinoloneandaninjectabledrugbasedonsusceptibilities 1. Not available in U.S. susceptibilities
2. SM: use only if not previously used and if documented susceptibility

BuildinganIndividualizedRegimenfor
Use any One of One of
MDR‐TB
STEP 1 Useanyavailable
Oneofthese
Oneofthese
First‐line Fluoro‐ Injectable
STEP1
Thiscase: st edrugs
uo oquinolones
jectab eagents
Pyrazinamide Levofloxacin Amikacin✔ ✔✔✔ (INH) y
Ethambutol Moxifloxacin Capreomycin
Kanamycin1✔
( )
Streptomycin2
1. Not available in U.S. 2. SM: use only if not previously used and if documented
susceptibility

B ildi R i f MDR TB ( )
Pi k f th
BuildingaRegimenforMDR‐TB(2)
Pickoneormoreofthese
Oralsecond‐linedrugsAddsecond‐line
STEP2
CycloserineEthionamide
drugsuntilyouhave4‐6drugs(optimallyat least 5) to which Ethionamide
PASLinezolid3
atleast5)towhichtheisolateissusceptible(andpreferably which ✔preferablywhichhavenotbeenusedtotreatthepatient
i l )3. Although considered a third-line drug, many experts now use LZD as apreviously) many experts now use LZD as a second-line drug option

Building a Regimen forMDR TB (3)BuildingaRegimenforMDR‐TB(3)
Consideruseofthese
Third‐linedrugsIftherearenot4‐6
STEP3g
BedaquilineDelamanid4
Meropenem/Clavulanate
drugsavailableintheabovecategories, Delamanid
ClofazimineImipenem
Amoxicillin/ClavulanateClarithromycin
g ,considerthird‐linedrugsinconsultation with Imipenem Clarithromycin
High‐doseINHconsultationwithanMDR‐TBexpert
4 A iti FDA l4. Awaiting FDA approval
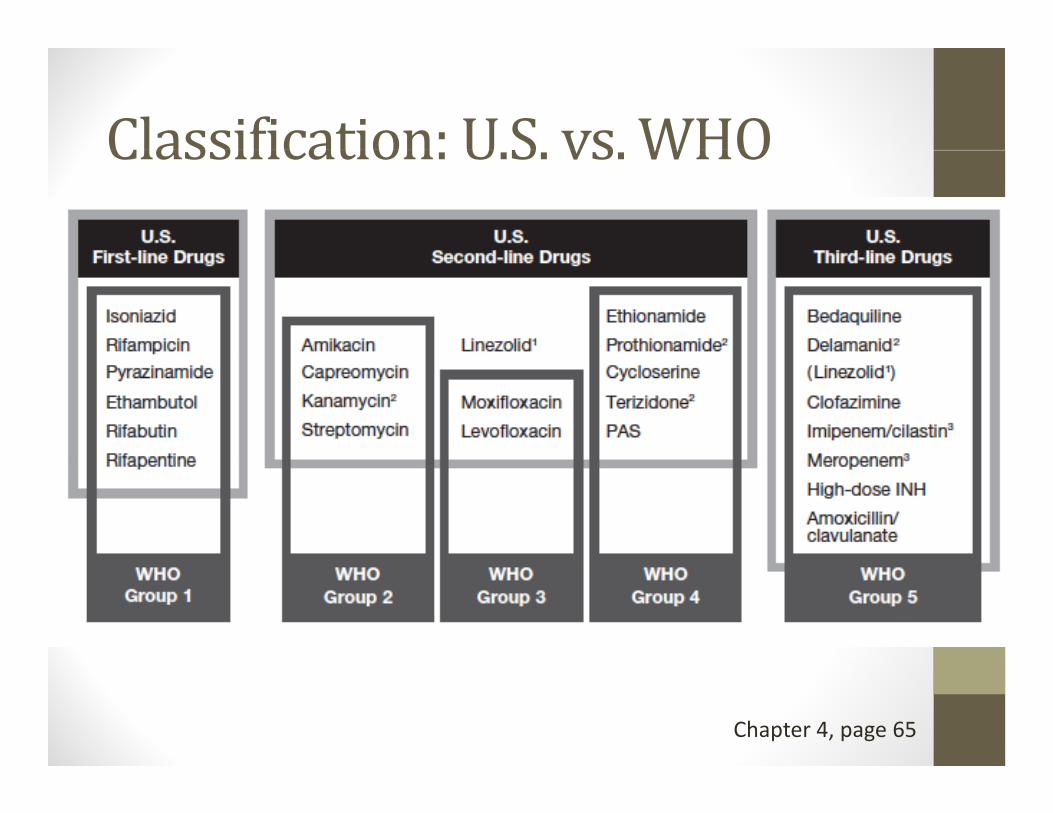
Classification: US vs WHOClassification:U.S.vs.WHO
Chapter 4, page 65

Otherid ticonsiderations
whenchoosingdrugsBeyond susceptibilityBeyond susceptibility results, consider:• Cross‐resistance (table page 76)
• Avoid drugs used previously
• Side effect profile
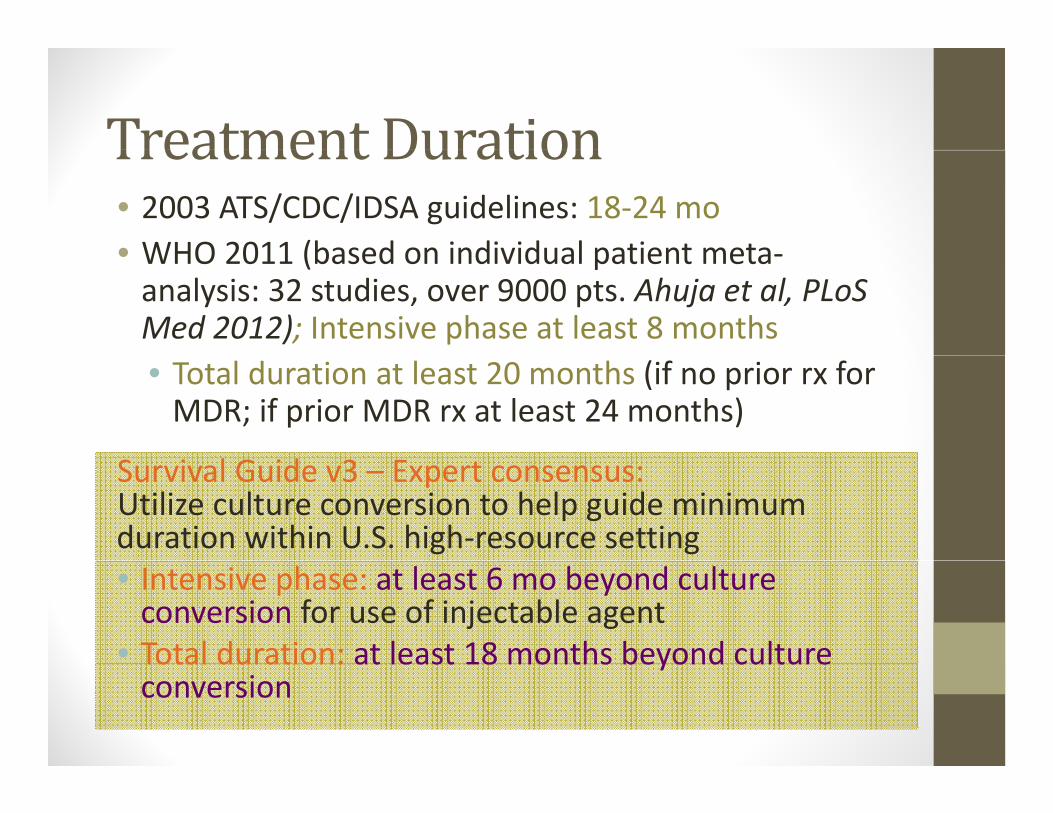
Treatment DurationTreatmentDuration• 2003 ATS/CDC/IDSA guidelines: 18‐24 mo • WHO 2011 (based on individual patient meta• WHO 2011 (based on individual patient meta‐analysis: 32 studies, over 9000 pts. Ahuja et al, PLoSMed 2012); Intensive phase at least 8 months• Total duration at least 20 months (if no prior rx for MDR; if prior MDR rx at least 24 months)
Survival Guide v3 – Expert consensus: Utilize culture conversion to help guide minimum duration within U.S. high‐resource setting• Intensive phase: at least 6 mo beyond culture conversion for use of injectable agent
• Total duration: at least 18 months beyond cultureTotal duration: at least 18 months beyond culture conversion

Treatmentiregimens
• Suggestions based ggon pattern of drug resistanceP XDR d XDR• Pre‐XDR and XDR recommend longer duration (at least (24 mo. post culture conversion)
Chapter 4, page 80

Goodresourcetoknow:U i th M di ti F t Sh tUsingtheMedicationFactSheets
• Drug class/trade name• Activity against TB• Activity against TB• Cross‐resistance• Dose (adult, peds, renal)• Route of administration• Preparation/storage• PharmacokineticsPharmacokinetics• Oral absorbtion/metabolism• CSF penetrationS i l i t• Special circumstances
• Adverse reactions/contraindications• Monitoring• Costs/patient education

“New”Medication Fact SheetsNew MedicationFactSheets
B d ili• Bedaquiline• Delaminid• Meropenam• Rifapentine• Clarithromycin
• New drugs in the pipeline

Monitoring and casemanagementMonitoringandcasemanagement
• Isolation issue – can he go home?• Planning for outpatient injections/infusionsPlanning for outpatient injections/infusions• Patient education and concerns (cost, anxiety)• Monitoring for toxicities
Question:Whentodischargefromhospital?• Pt is still smear positive• On expanded MDR regimenOn expanded MDR regimen• Lives at home with wife and 2 adult daughters (all IGRA negative)( g )
• Pt very concerned about high deductible and big hospital bill

• **A patient may be considered for placement in a lower risk setting without meeting these criteria if no previously unexposed persons will be present (see section: Home isolation)
• Chapter 8, page 230

Home IsolationHomeIsolation
M ti t ith d i t t TB d tMany patients with drug‐resistant TB do not require hospitalization and may be on home isolation at the start of treatment Someisolation at the start of treatment. Some patients may be hospitalized to initiate treatment and become ready for discharge prior to becoming non‐infectious.

Providing the Injectable AgentProvidingtheInjectableAgent
Chapter 8, page 215
PatientEducation:CommunicatingEffectively
Recognize and address the patient’s fears and concerns. Patients are less likely toconcerns. Patients are less likely to comprehend treatment information if they are fearful or preoccupied with worries about their jobs or family members.

Monitoring for ToxicitiesMonitoringforToxicities
Chapter 8, page 235

Comorbidities: DR‐TB and diabetesComorbidities:DR TBanddiabetes
• Slower response to treatment• Potential lower drug levels• Increased risk of acquired drug resistance• Poorer outcomes in treatment MDR‐TB
RecommendationsfortreatingTB i h f DMTBinthepresenceofDM• Follow renal functiono o e a u c o
• Decrease frequency of injectable if impaired• Treat GI symptoms aggressivelyy p gg y• Manage neuropathy
• Change meds if possible• Add tricyclics or gabapentine
• Consider TDM
• If initially INH‐resistant, don’t use intermittent treatment and strongly consider RIF & EMB levels

Drug levelmonitoringDruglevelmonitoring• When to order:
• Injectable (especially impaired renal function or age 60+)Injectable (especially impaired renal function or age 60 )• Cycloserine to establish safe and effective dose for patient• MalabsorptionL k f t d li i l• Lack of expected clinical response
• Few effective drugs in regimen to optimize• Drug‐drug interactions, e.g. rifamycins and HIV antiretrovirals• Renal impairment e.g., EMB
• Where to send:• National Jewish or University of FloridaNational Jewish or University of Florida• Amikacin often done locally
• How/when to collect:• See pages 57 and 58

Next set of DST resultsNextsetofDSTresults• CDC MDDR results:CDC MDDR results:
• Confirmed PSQ results• No pncAmutation• No pncAmutation• embBmutations identified (silent and neutral mutation – so not associated with resistance)mutation so not associated with resistance)
Get these results soon after start – any changes?

Chapter 3, pages 46‐47
Update: firstmonth of rxUpdate:firstmonthofrx
• Frequent nursing calls…..

DR‐TB Contacts Rx optionsDR TBContactsRxoptions
• Duration 6‐12 monthsd b fl l l• Two‐drug combo or fluoroquinolone alone
• Avoid PZA (risk vs. benefit)• Observation/clinical monitoring optionObservation/clinical monitoring option
Update (5weeks into rx):Update(5weeksintorx):
• Phenotypic DST: sensitive to INH, EMB, PZA (confirms RIF mono‐resistant)

Regimen options formono/poly‐DRRegimenoptionsformono/poly DR
• Case: RIF mono‐resistantCase: RIF mono resistant• INH, EMB, PZA, Levo
• (Treatment Chap table 1, pg 70)

Update (5weeks into rx):Update(5weeksintorx):
• Phenotypic DST: sensitive to INH, EMB, PZA (confirms RIF mono‐resistant)
• Last update on management….Last update on management….• Rx for contacts?• Patient education?

MoreMDR resource tips:MoreMDRresourcetips:• Pediatric DR‐TBPediatric DR TB
• New chapter in Survival Guide
• Sentinal Project• International/WHO –International/WHO Companion Handbook
• New US and WHO DR‐TB guidelines underway!

The endTheend.
Here to help :)• California DPH MDR‐TB Service1‐510‐620‐3054
• Warmline (Western region)Warmline (Western region)Curry International Tuberculosis Center1‐877‐390‐NOTB or 1‐877‐390‐6682
tb t f dwww.currytbcenter.ucsf.edu