manual therapy in athletics joel harman d.c., cert. mdt, cktp manchester family chiropractic
TRANSCRIPT
MANUAL THERAPY IN ATHLETICS
Joel Harman D.C., Cert. MDT, CKTP
Manchester Family Chiropractic
OBJECTIVES• Learn and get a hands-on understanding of joint mechanics in
the shoulder, and thoracic spine.
• Learn basic movement patterns that will help guide treatment.
• Palpate, palpate, palpate.
• Learn mobilisation techniques for the shoulder, and thoracic spine.
• Leave with an integrated approach to handling common and difficult dysfunctions.
GOALS• Learn to palpate the junctional areas of the spine and
shoulder.
• Learn how to functionally assess the musculoskeletal system to locate primary areas of dysfunction.
• Learn to manually treat these findings.
• Learn how to teach the patient how to reinforce your treatment actively.
WE ARE WHAT WE REPEATEDLY DO.
EXCELLENCE, THEN, IS NOT AN ACT, BUT A HABIT.
- ARISTOTLE
10,000 HOURS
The hand is the greatest diagnostic and therapeutic tool that has ever been, or will be, invented.
- Karel Lewit
Orthopedic Testing• Active Compression Test (O’Brien’s)• Apprehension Test• Sulcus Sign• Hawkin’s • Neer’s• Drop Arm• Empty Can• Speed’s • Yergason’s
Functional Testing• Arm Abduction (Janda)
• Push-Up Test (Janda)
• T4 Extension
• Wall Angels
• Internal/External Rotation
Look for Texas-sized deficits!
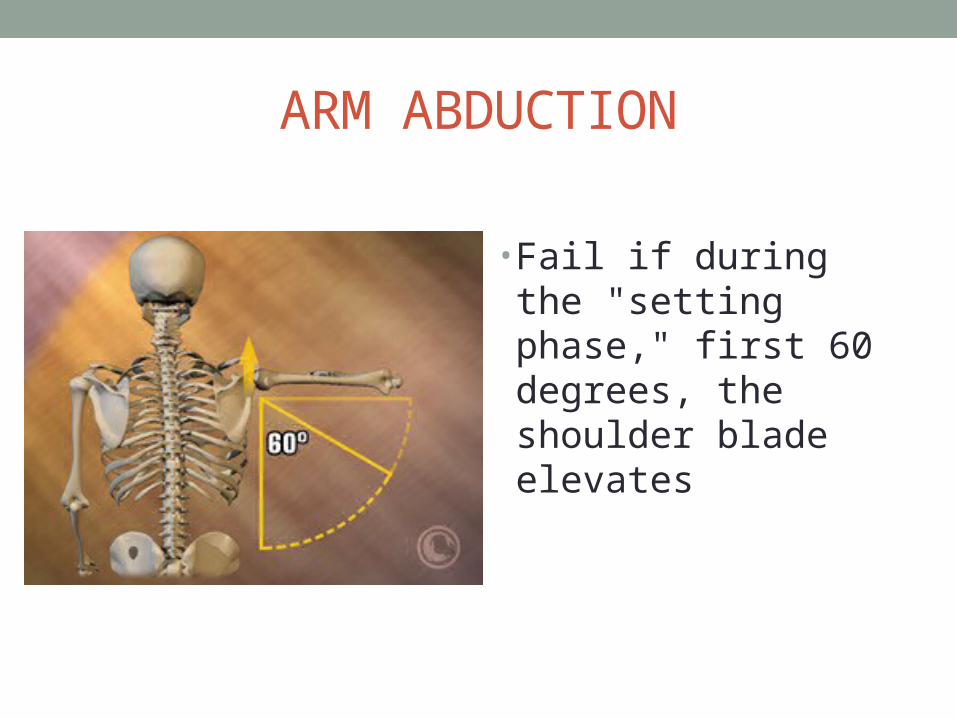
ARM ABDUCTION
• Fail if during the "setting phase," first 60 degrees, the shoulder blade elevates
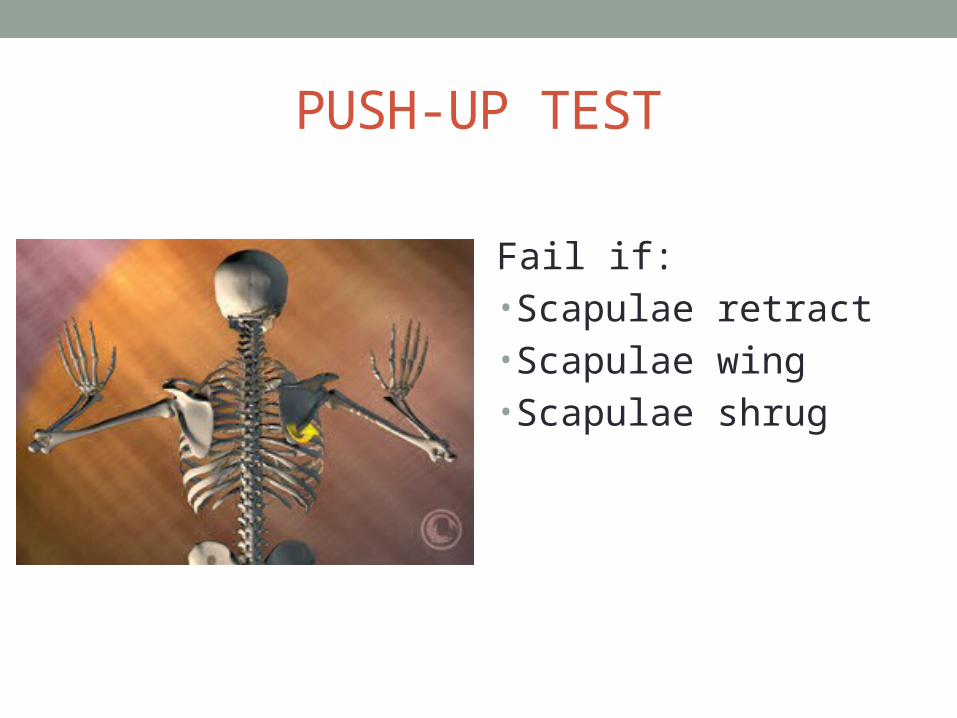
PUSH-UP TEST
Fail if: • Scapulae retract• Scapulae wing• Scapulae shrug
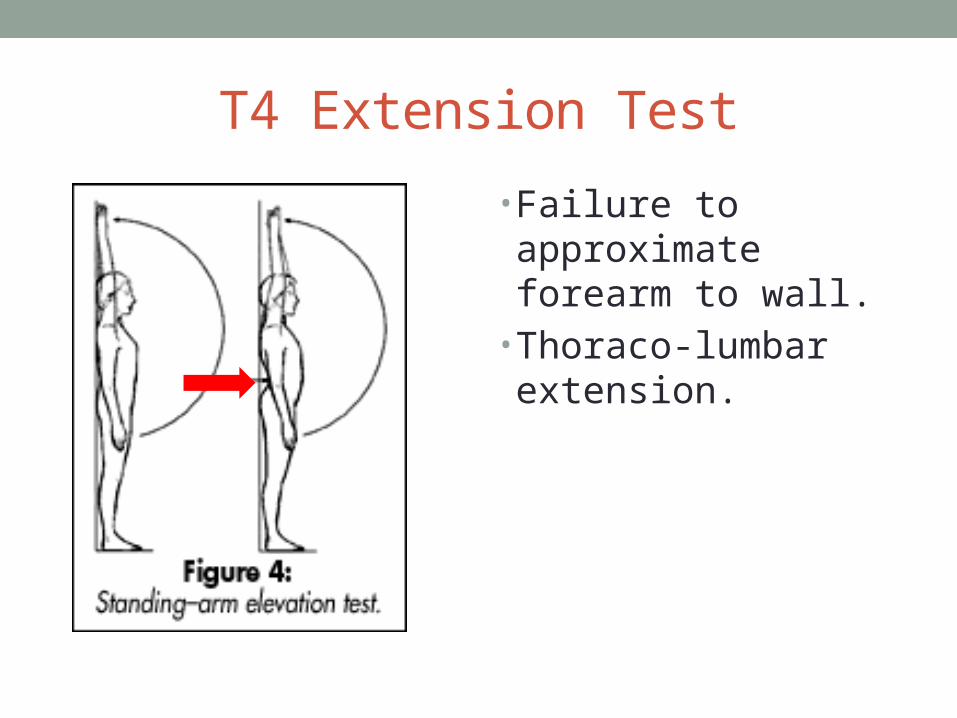
T4 Extension Test
• Failure to approximate forearm to wall.
• Thoraco-lumbar extension.
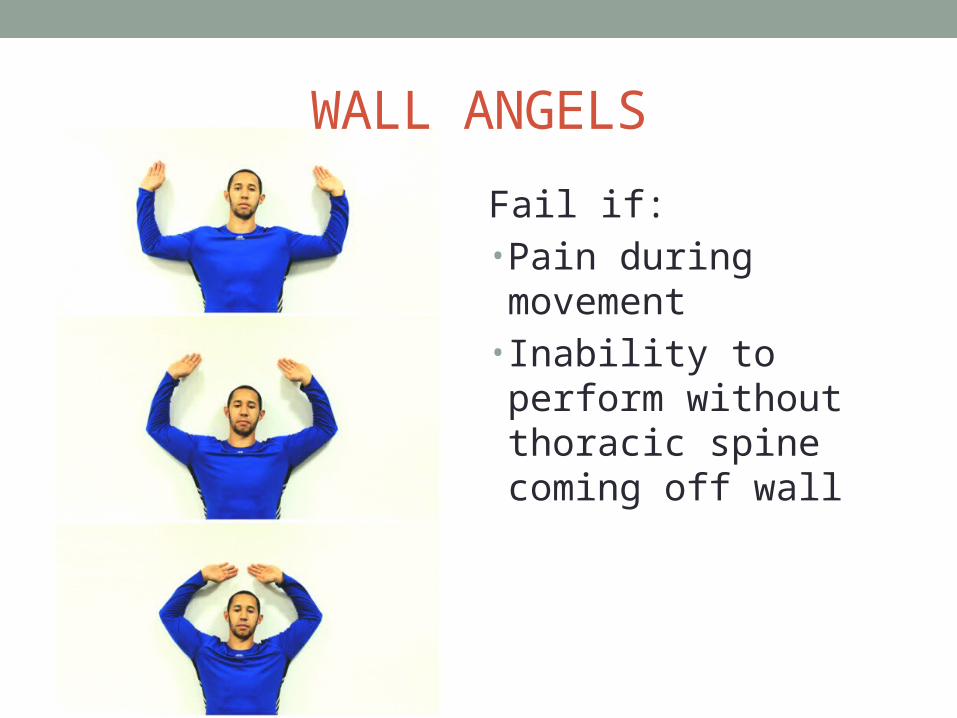
WALL ANGELS
Fail if: • Pain during movement• Inability to perform without thoracic spine coming off wall
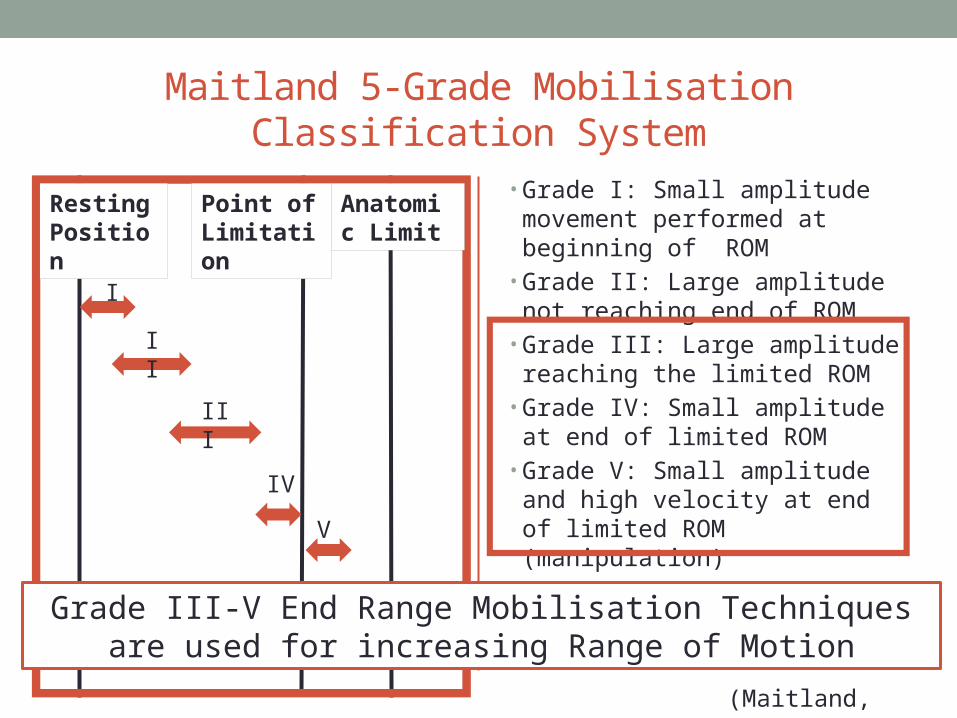
Maitland 5-Grade Mobilisation Classification System
• Grade I: Small amplitude movement performed at beginning of ROM
• Grade II: Large amplitude not reaching end of ROM
• Grade III: Large amplitude reaching the limited ROM
• Grade IV: Small amplitude at end of limited ROM
• Grade V: Small amplitude and high velocity at end of limited ROM (manipulation)
(Maitland, 1977)
Resting Position
Point of Limitation
Anatomic Limit
I
II
III
V
IV
Grade III-V End Range Mobilisation Techniquesare used for increasing Range of Motion
Shoulder Mobilisations
• Glenohumeral Mobs• AP• PA• FLEXION• ABDUCTION (INF GLIDE)
• EXT. ROT• INT. ROT• LONG-AXIS
DISTRACTION
• AC Accessory Mobs
AC Joint Caudal Glide Clavicle Rotation
• Scapular Mobilisations• Elevation/Depression• Protraction/Retraction• External/Internal Rotation
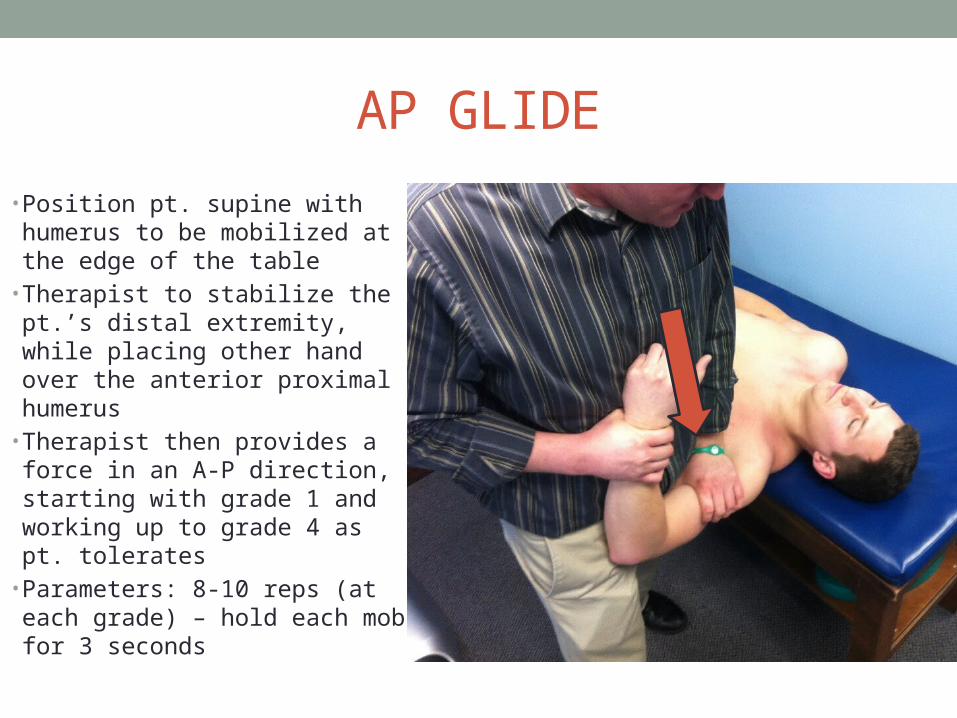
AP GLIDE
• Position pt. supine with humerus to be mobilized at the edge of the table
• Therapist to stabilize the pt.’s distal extremity, while placing other hand over the anterior proximal humerus
• Therapist then provides a force in an A-P direction, starting with grade 1 and working up to grade 4 as pt. tolerates
• Parameters: 8-10 reps (at each grade) – hold each mob for 3 seconds
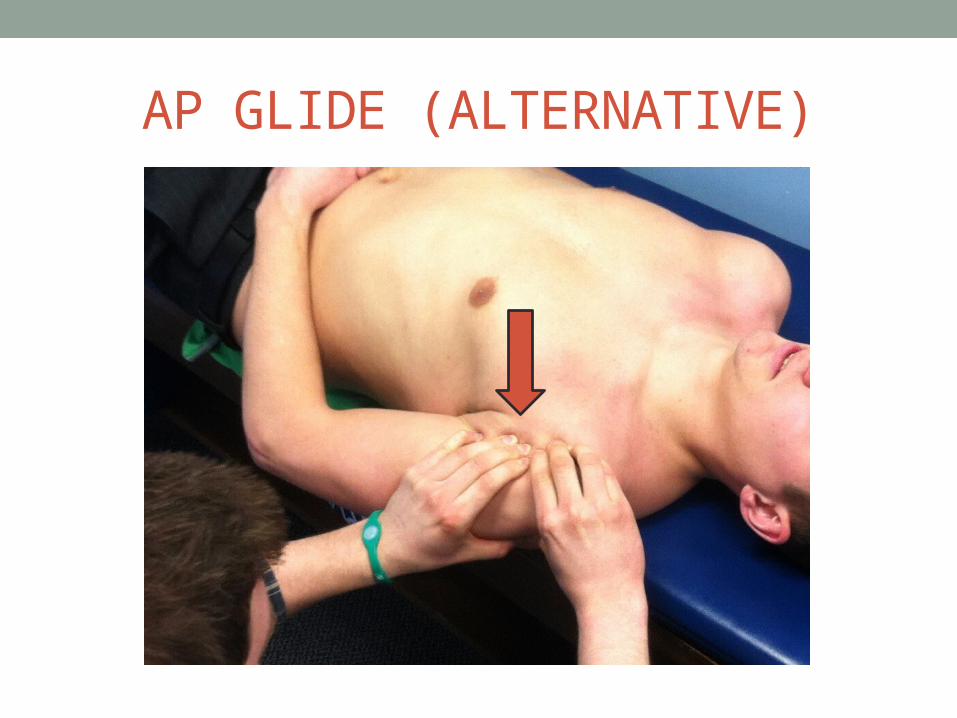
AP GLIDE (ALTERNATIVE)
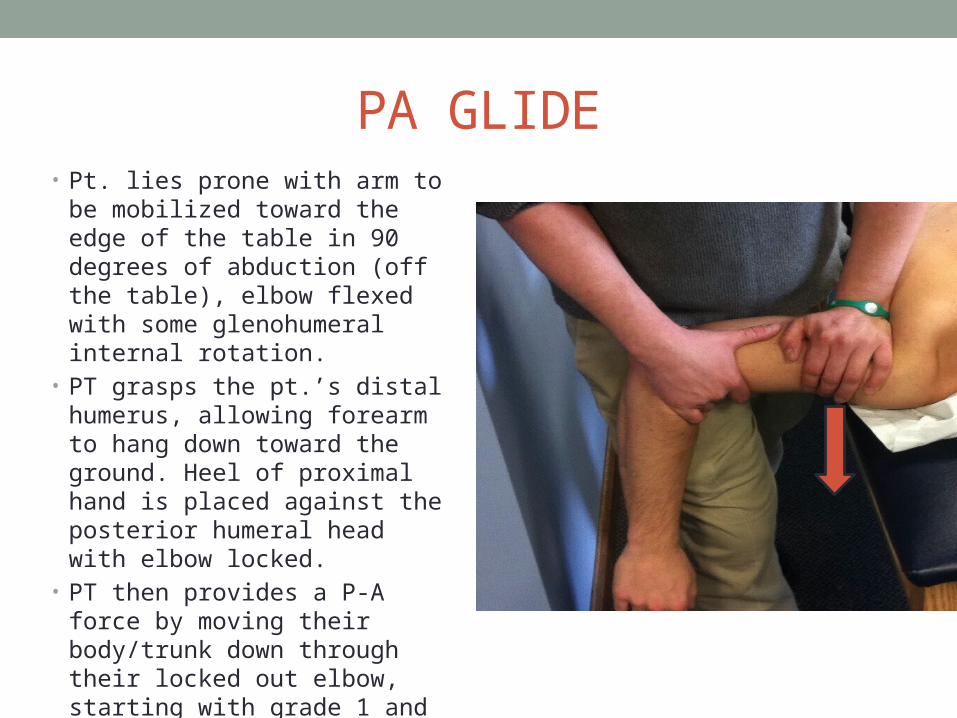
PA GLIDE• Pt. lies prone with arm to be
mobilized toward the edge of the table in 90 degrees of abduction (off the table), elbow flexed with some glenohumeral internal rotation.
• PT grasps the pt.’s distal humerus, allowing forearm to hang down toward the ground. Heel of proximal hand is placed against the posterior humeral head with elbow locked.
• PT then provides a P-A force by moving their body/trunk down through their locked out elbow, starting with grade 1 and working up to grade 4 as pt. tolerates
• Parameters: 8-10 reps (at each grade) – hold each mob for 3 seconds
FLEXION
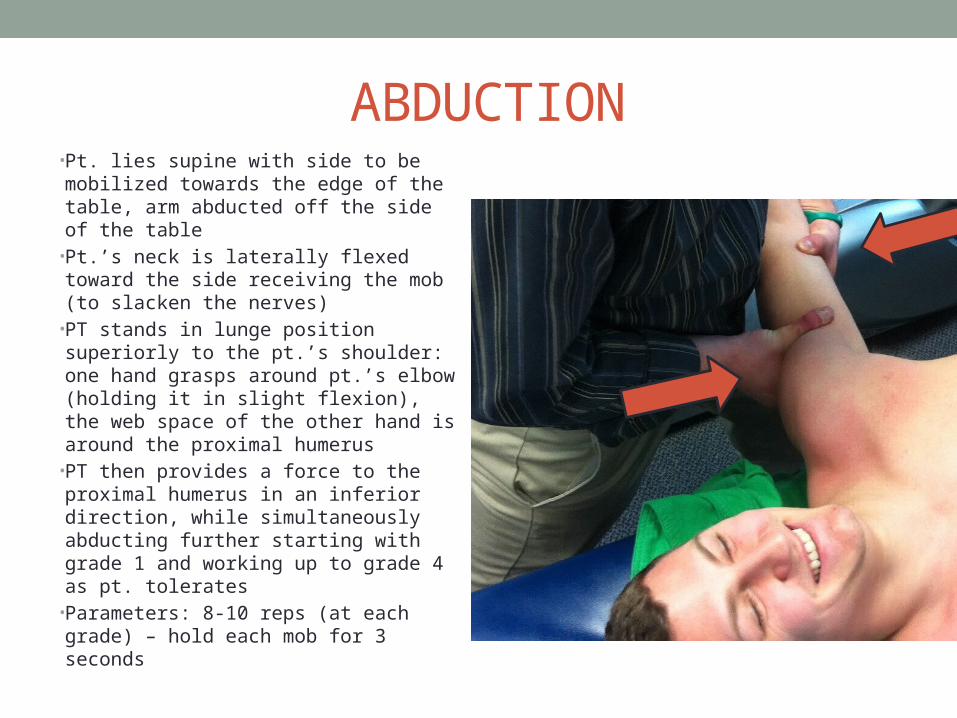
ABDUCTION• Pt. lies supine with side to be
mobilized towards the edge of the table, arm abducted off the side of the table
• Pt.’s neck is laterally flexed toward the side receiving the mob (to slacken the nerves)
• PT stands in lunge position superiorly to the pt.’s shoulder: one hand grasps around pt.’s elbow (holding it in slight flexion), the web space of the other hand is around the proximal humerus
• PT then provides a force to the proximal humerus in an inferior direction, while simultaneously abducting further starting with grade 1 and working up to grade 4 as pt. tolerates
• Parameters: 8-10 reps (at each grade) – hold each mob for 3 seconds
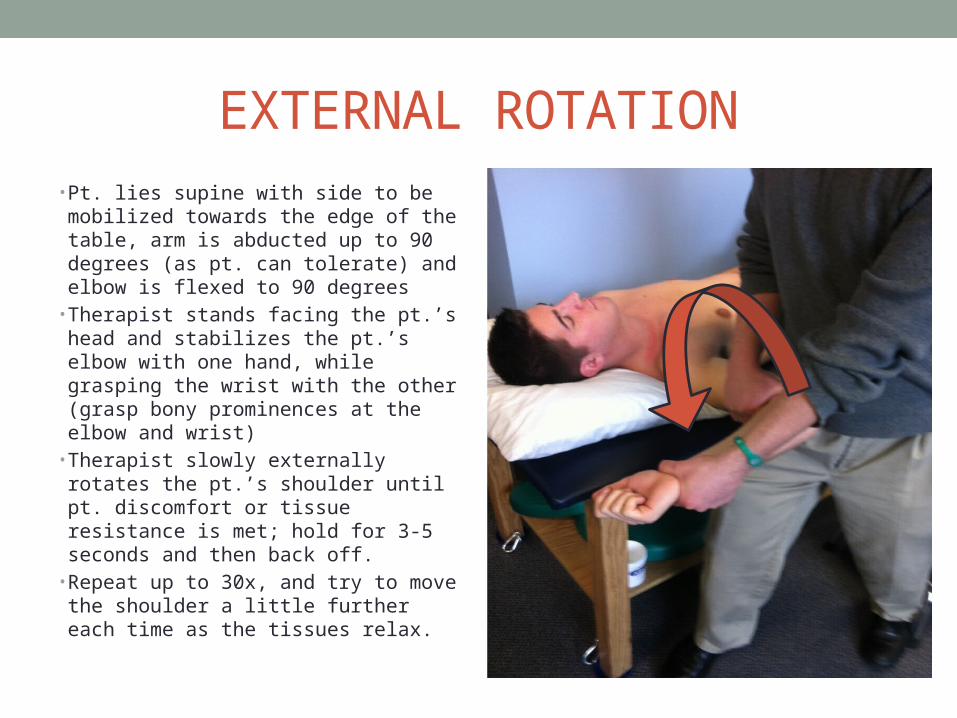
EXTERNAL ROTATION• Pt. lies supine with side to be
mobilized towards the edge of the table, arm is abducted up to 90 degrees (as pt. can tolerate) and elbow is flexed to 90 degrees
• Therapist stands facing the pt.’s head and stabilizes the pt.’s elbow with one hand, while grasping the wrist with the other (grasp bony prominences at the elbow and wrist)
• Therapist slowly externally rotates the pt.’s shoulder until pt. discomfort or tissue resistance is met; hold for 3-5 seconds and then back off.
• Repeat up to 30x, and try to move the shoulder a little further each time as the tissues relax.
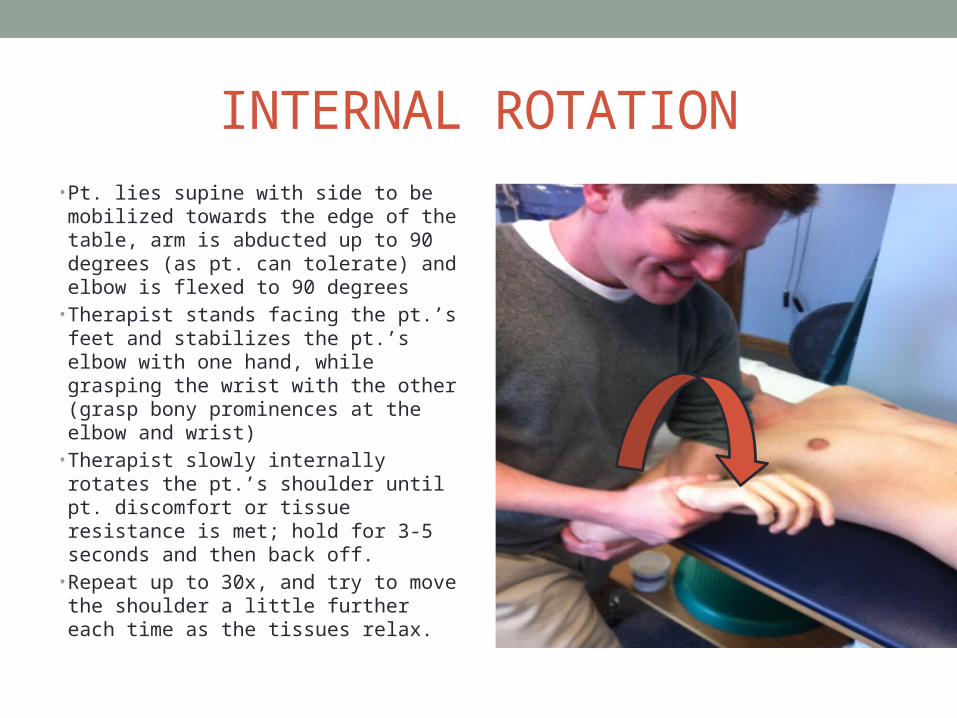
INTERNAL ROTATION• Pt. lies supine with side to be
mobilized towards the edge of the table, arm is abducted up to 90 degrees (as pt. can tolerate) and elbow is flexed to 90 degrees
• Therapist stands facing the pt.’s feet and stabilizes the pt.’s elbow with one hand, while grasping the wrist with the other (grasp bony prominences at the elbow and wrist)
• Therapist slowly internally rotates the pt.’s shoulder until pt. discomfort or tissue resistance is met; hold for 3-5 seconds and then back off.
• Repeat up to 30x, and try to move the shoulder a little further each time as the tissues relax.
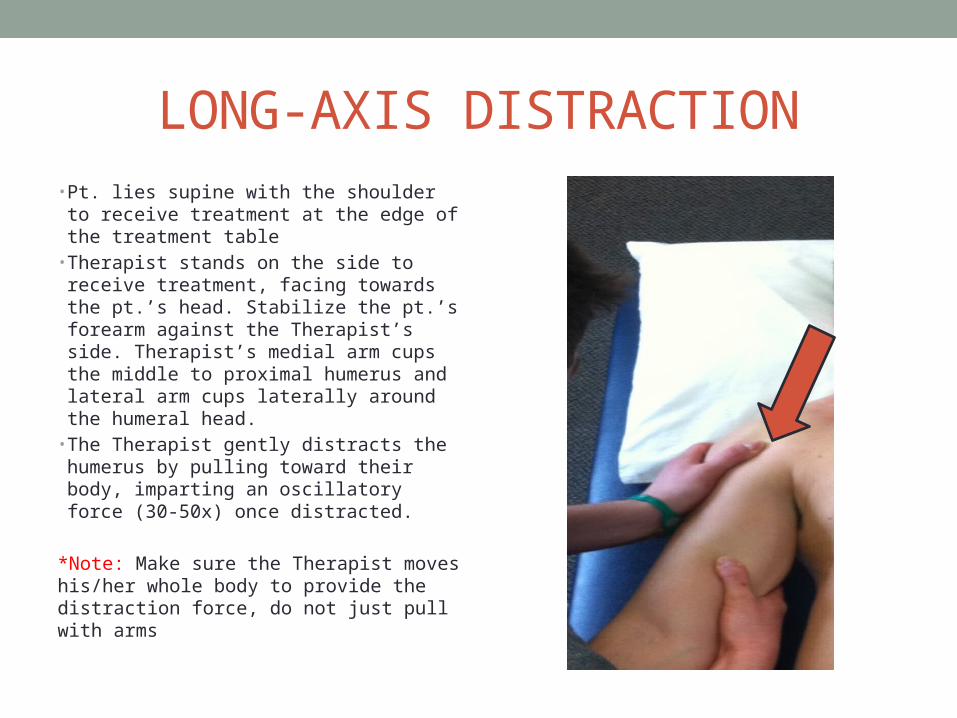
LONG-AXIS DISTRACTION• Pt. lies supine with the shoulder to
receive treatment at the edge of the treatment table
• Therapist stands on the side to receive treatment, facing towards the pt.’s head. Stabilize the pt.’s forearm against the Therapist’s side. Therapist’s medial arm cups the middle to proximal humerus and lateral arm cups laterally around the humeral head.
• The Therapist gently distracts the humerus by pulling toward their body, imparting an oscillatory force (30-50x) once distracted.
*Note: Make sure the Therapist moves his/her whole body to provide the distraction force, do not just pull with arms
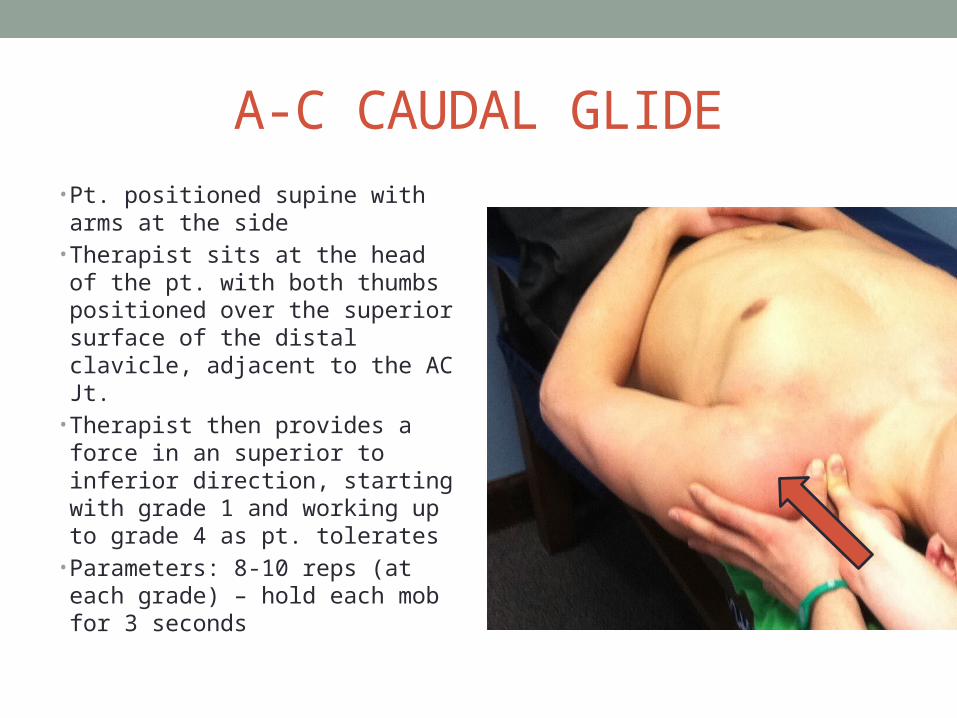
A-C CAUDAL GLIDE
• Pt. positioned supine with arms at the side
• Therapist sits at the head of the pt. with both thumbs positioned over the superior surface of the distal clavicle, adjacent to the AC Jt.
• Therapist then provides a force in an superior to inferior direction, starting with grade 1 and working up to grade 4 as pt. tolerates
• Parameters: 8-10 reps (at each grade) – hold each mob for 3 seconds

CLAVICLE ROTATION• Pt. positioned supine with arms at
the side• Stand near the pt.’s shoulder,
facing towards the clavicle• Gently grip the middle of the
clavicle using your thumbs on the inferior surface and fingertips on the superior surface
• Apply a gentile mobilization force using a rocking or “wiggling” motion through repetitive wrist flexion and extension to impart rotation of the clavicle on its long axis
• Parameters: 8-10 reps each grade (up to grade 3)
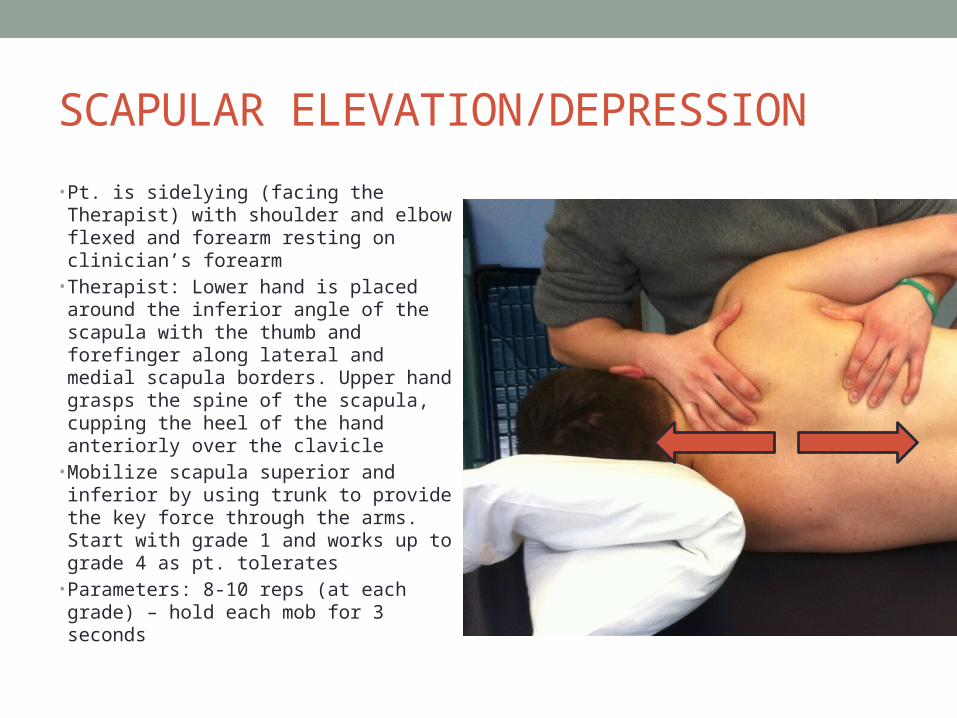
SCAPULAR ELEVATION/DEPRESSION
• Pt. is sidelying (facing the Therapist) with shoulder and elbow flexed and forearm resting on clinician’s forearm
• Therapist: Lower hand is placed around the inferior angle of the scapula with the thumb and forefinger along lateral and medial scapula borders. Upper hand grasps the spine of the scapula, cupping the heel of the hand anteriorly over the clavicle
• Mobilize scapula superior and inferior by using trunk to provide the key force through the arms. Start with grade 1 and works up to grade 4 as pt. tolerates
• Parameters: 8-10 reps (at each grade) – hold each mob for 3 seconds
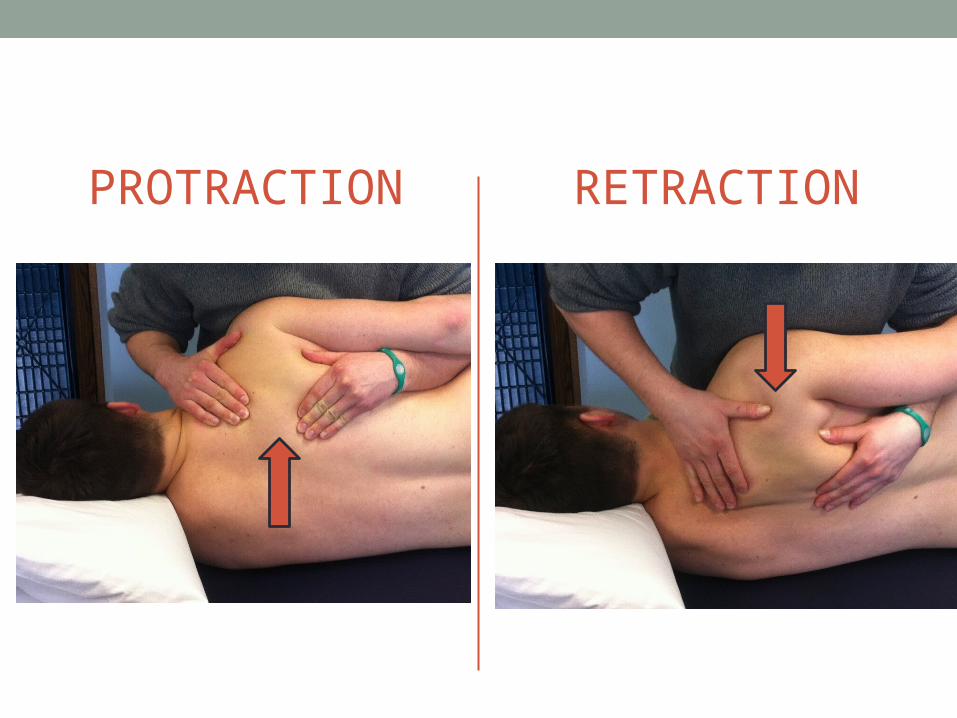
PROTRACTION RETRACTION
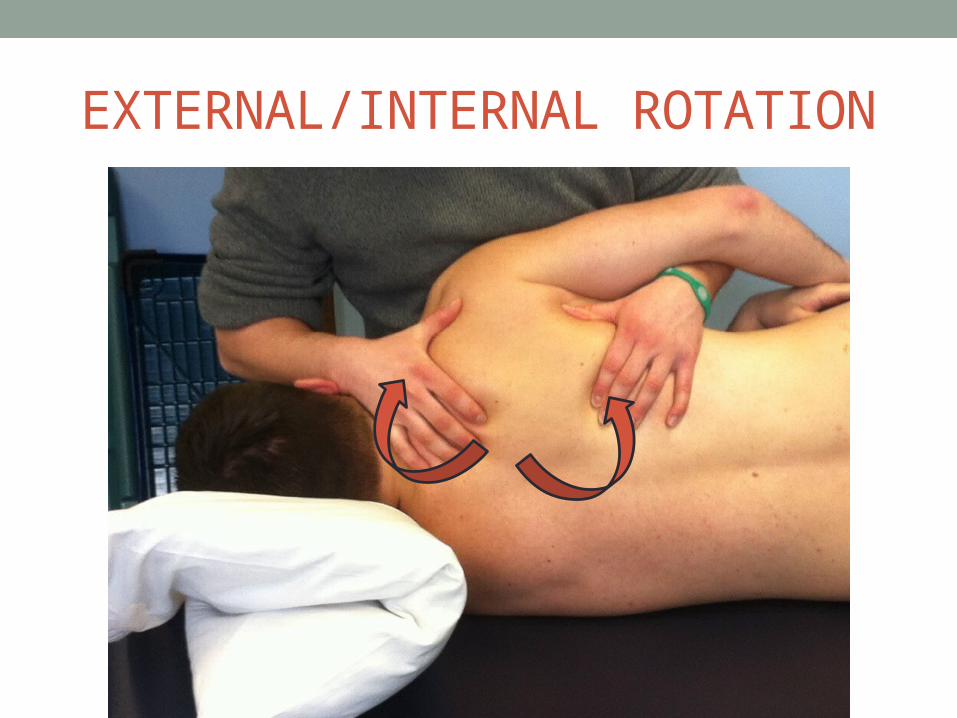
EXTERNAL/INTERNAL ROTATION
OTHER GOOD THERAPIESMcKenzie Diagnosis and Therapy
Kinesio-Tape
PIR/PNF/SNAGS
QUESTIONS?
REFERENCES• References• Faye L Motion Palpation and Chiropractic Technic, 2nd Edition. Huntington Beach: The Motion Palpation Institute,
1990.• Lewit K. Manipulative Therapy in Rehabilitation of the Locomotor System, 3rd Edition. Boston: Butterworth-
Heineman, 1999.• Kolar P. Facilitation of Agonist-Antagonist Co-activation by Reflex Stimulation Methods. In: Liebenson
C. Rehabilitation of the Spine, 2nd Edition. Baltimore: Lippincott/Williams and Wilkins, 2007.• Boyles RE, Ritland BM, Miracle BM, et al. Man Ther, 2009;14:375-380.• Cleland JA, Childs JD, McRae M, Palmer JA, Stowell T. Immediate effects of thoracic manipulation in patients with
neck pain: a randomized clinical trial. Man Ther, 2005;10:127-135.• Cleland JA, Childs JD, Fritz JM, Whitman JM, Eberhart SL. Development of a clinical prediction rule for guiding
treatment of a subgroup of patients with neck pain: use of thoracic spine manipulation, exercise, and patient education. Phys Ther, 2007;87:9-23.
• Norlander S, Nordgren B. Clinical symp- toms related to musculoskeletal neck- shoulder pain and mobility in the cervico- thoracic spine. Scand J Rehabil Med, 1998;30:243-251.
• Bang MD, Deyle GD. Comparison of supervised exercise with and without manual physical therapy for patients with shoulder impingement syndrome. Journal of Orthopaedic and Sports Physical Therapy, 2000;30:126-37.
• Bergman GJ, Winters JC, Groenier KH, Pool JJ, Meyboom-de Jong B, Postema K, et al. Manipulative therapy in addition to usual medical care for patients with shoulder dysfunction and pain: a randomized, controlled trial. Annals of Internal Medicine,2004;141:432-9.
• Liebenson CS. Treatment of mid-thoracic dysfunction: a key link in the body axis. Part 1: overview and assessment. Journal of Bodywork and Movement Therapies, 2001;5(2):90-98.
• Cook G. Movement: Functional Movement Systems. On Target Publications, Santa Cruz, CA: 2010.• Janda V, Frank C, Liebenson C. Evaluation of Muscle Imbalance. In: Liebenson C.Rehabilitation of the Spine, 2nd
Edition. Baltimore: Lippincott/Williams and Wilkins, 2007.