manual of -...
TRANSCRIPT



Manual of Minor Oral Surgery
for the General Dentist

Manual of Minor Oral Surgery
for the General Dentist
Edited by
Karl R. Koerner

Karl R. Koerner, BS, DDS, MS, is an editor of andcontributor to Manual of Oral Surgery for GeneralDentists (Blackwell Publishing) and has co-authoredColor Atlas of Minor Oral Surgery, 2nd ed. (Mosby)and Clinical Procedures for Third Molar Surgery, 2nded. (PennWell). He also is editor of and contributorto a Dental Clinics of North America (Saunders) vol-ume on basic oral surgery. Dr. Koerner has producedvideo programs and contributed articles to publica-tions such as General Dentistry, Dentistry Today,Dental Economics, and the Journal of Public HealthDentistry.
Dr. Koerner is a past president of the Utah DentalAssociation and a former delegate to the ADA House.He has served as Utah Academy of General Dentistry(AGD) president, is a Fellow in the AGD, and hasmembership in the International College of Dentists.He is licensed in Utah to administer IV sedation andlicensed to practice dentistry in Utah, Idaho, andCalifornia. His practice is now limited to oral surgery.
Dr. Koerner has been teaching clinical courses on oralsurgery to other dentists in the United States andabroad since 1981. In 2002, he joined ClinicalResearch Associates (CRA) in Provo, Utah, as anevaluator and clinician and began teaching their“Update” courses throughout the country and abroad.Since 2002, he has co-presented more than 90 coursesfor CRA and serves on their advisory board.
© 2006 by Blackwell Munksgaard,published by Blackwell Publishing, a BlackwellPublishing Company
Blackwell Publishing Professional2121 State Avenue, Ames, Iowa 50014-8300, USATel: +1 515 292 0140
Editorial Offices:9600 Garsington Road, Oxford OX4 2DQTel: 01865 776868
Blackwell Publishing Asia Pty Ltd, 550 Swanston Street, Carlton South, Victoria 3053, Australia Tel: +61 (0)3 9347 0300
Blackwell Wissenschafts Verlag, Kurfürstendamm 57,10707 Berlin, GermanyTel: +49 (0)30 32 79 060
Europe and AsiaAll rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or trans-mitted, in any form or by any means, electronic,mechanical, photocopying, recording or otherwise,except as permitted by the UK Copyright, Designsand Patents Act 1988, without the prior permissionof the publisher.
The right of the Author to be identified as the Authorof this Work has been asserted in accordance with theCopyright, Designs and Patents Act 1988.
North AmericaAuthorization to photocopy items for internal orpersonal use, or the internal or personal use of specificclients, is granted by Blackwell Publishing, providedthat the base fee of $.10 per copy is paid directly tothe Copyright Clearance Center, 222 RosewoodDrive, Danvers, MA 01923. For those organizationsthat have been granted a photocopy license by CCC,a separate system of payments has been arranged. The fee code for users of the Transactional ReportingService is ISBN-13: 978-0-8138-0559-7; ISBN-10:0-8138-0559-7/2006 $.10.
Library of Congress Cataloging-in-Publication Data
Manual of minor oral surgery for the general dentist /edited by Karl R. Koerner.
p. ; cm.Includes bibliographical references and index.ISBN-13: 978-0-8138-0559-7 (alk. paper)ISBN-10: 0-8138-0559-7 (alk. paper)1. Dentistry, Operative. 2. Mouth—Surgery.
3. Dentistry. [DNLM: 1. Oral Surgical Procedures.2. Surgical Procedures, Minor. WU 600 M2942006] I. Koerner, Karl R.
RK501.M34 2006617.6�05—dc22
2005028549
For further information on Blackwell Publishing, visit our Dentistry Subject Site:www.dentistry.blackwellmunksgaard.com
The last digit is the print number: 9 8 7 6 5 4 3 2 1
ContentsContributors viiPreface ix
Chapter 1 Patient Evaluation and Medical History 3Dr. R. Thane Hales
Chapter 2 Surgical Extractions 19Dr. Hussam S. Batal and Dr. Gregg Jacob
Chapter 3 Surgical Management of Impacted Third Molar Teeth 49Dr. Pushkar Mehra and Dr. Shant Baran
Chapter 4 Pre-Prosthetic Oral Surgery 81Dr. Ruben Figueroa and Dr. Abhishek Mogre
Chapter 5 Conservative Surgical Crown Lengthening 99Dr. George M. Bailey
Chapter 6 Endodontic Periradicular Microsurgery 137Dr. Louay Abrass
Chapter 7 The Evaluation and Treatment of Oral Lesions 201Dr. Joseph D. Christensen and Dr. Karl R. Koerner
Chapter 8 Anxiolysis for Oral Surgery and Other Dental Procedures 221Dr. Fred Quarnstrom
Chapter 9 Infections and Antibiotic Administration 255Dr. R. Thane Hales
Chapter 10 Management of Perioperative Bleeding 277Dr. Karl R. Koerner, and Dr. William L. McBee
Chapter 11 Third World Volunteer Dentistry 295Dr. Richard C. Smith
Index 319
v

Number in brackets following each name is thechapter number.
Louay M. Abrass, DMD [6]Assistant Clinical Professor, Department of
Endodontics, Boston University Schoolof Dental Medicine
Adjunct Assistant Professor, Department ofEndodontics, University of PennsylvaniaSchool of Dental Medicine
Private Practice Limited to Endodontics inBoston and Wellesley, Massachusetts
George M. Bailey, DDS, MS [5]Associate Professor, University of Utah
Medical School and Creighton School ofDentistry
President and Lecturer CPSeminarsPrivate Practice Periodontics
Shant Baran, DMD [3]Resident, Department of Oral and
Maxillofacial Surgery, Boston UniversitySchool of Dental Medicine and BostonMedical Center, Boston, Massachusetts
Hussam S. Batal, DMD [2]Assistant Professor, Department of Oral
and Maxillofacial Surgery, BostonUniversity, Boston, Massachusetts
Joseph D. Christensen, DMD [7]Private General Practice, Salt Lake City,
Utah
Ruben Figueroa, DMD, MS [4]Oral and Maxillofacial SurgeonAssistant Professor, Director Predoctoral
Oral and Maxillofacial Surgery, DirectorOral Surgery Clinic, Boston University,Henry Goldman School of DentalMedicine, Boston, Massachusetts
R. Thane Hales, DMD [1, 9]Founder and Director of the Wasatch
Surgical Institute International Lecturer and Clinician, Private
Practice, Ogden, Utah
Gregg A. Jacob, DMD [2]Private Practice, Summit Oral and
Maxillofacial Surgery, P.A., Summit, New Jersey
Karl R. Koerner, DDS, MS [Editor, 7, 10]International Lecturer and ClinicianPrivate General Practice Limited to Oral
Surgery, Salt Lake City, UtahFormerly Consultant and Instructor for
Clinical Research Associates, Provo, Utah
William L. McBee, DDS [10]Private Practice Limited to Oral and
Maxillofacial Surgery, Provo, Utah
vii
Contributors

viii C O N T R I B U T O R S
Pushkar Mehra, BDS, DMD [3]Director, Department of Dentistry and Oral
and Maxillofacial Surgery, BostonMedical Center
Director, Department of Oral andMaxillofacial Surgery, Boston UniversityMedical Center
Assistant Professor, Department of Oral andMaxillofacial Surgery, Boston UniversitySchool of Dental Medicine, Boston,Massachusetts
Abhishek Mogre BDS [4]Current Advanced Standing DMD StudentVice President Predoctoral Association of
Oral and Maxillofacial Surgery, BostonUniversity, Henry Goldman School ofDental Medicine, Boston, Massachusetts
Dr. Fred Quarnstrom, DDS [8]Clinical Faculty of Dentistry, University of
British ColumbiaAffiliate Assistant Professor, University of
Washington School of DentistryDental Anesthesiologist also in General
Dental Practice, Seattle, Washington
Richard C. Smith, DDS [11]Chairman of Ayuda IncorporatedPrivate General Practice (Retired), Westlake
Village, California

This handbook is a guide for the generaldentist who enjoys doing oral surgery. Abroad range of knowledge and expertise inthis area is found among dentists. Somehave had extensive experience and trainingthrough general practice residencies, mili-tary or other postgraduate programs, or amentoring experience with a more experi-enced dentist; others have had only minimalinstruction and training in dental school.
Dental school oral surgery training varieswidely based on individual school require-ments for graduation. In addition, someschools offer elective or extramural experi-ences, others do not. Even in the samedental school class, a few students mighthave the opportunity to perform extensiveexodontia, but others will remove only afew teeth before moving on to private prac-tice. This handbook is meant to diminishthe discrepancy between experienced andinexperienced generalists and provide aninformation base for the interested clinician.This book presents a review of proceduresand principles in each of several clinicalsurgical areas; this review will enable adentist to perform according to establishedstandards of care.
It is assumed that the reader possessesfundamental knowledge and skills in oralanatomy, patient/operator positioning forsurgery, the care of soft and hard tissue dur-ing surgery, and basic patient managementtechniques. Therefore, the authors haveskipped to the crux of each procedure,addressing such things as case selection,step-by-step operative procedures, and the
prevention and/or management of compli-cations. This handbook will help dentistsperform procedures more quickly, smoothly,easily, and safely—thereby greatly minimiz-ing doctor frustration and patient dis-satisfaction.
The procedures covered in this book arealso done by oral and maxillofacial surgeonsand/or periodontists and endodontists.There are times that the patient would bebetter served by being referred to the spe-cialist, such as when the patient is extremelyapprehensive, medically compromised, anolder patient with dense bone, or has othermitigating circumstances. This book willhelp readers more clearly understand thescope of each procedure and more accuratelydefine their capabilities and comfort zones.
Procedures described are mainly dento-alveolar in nature, such as “surgical” extrac-tions, the removal of impacted wisdomteeth (mainly in younger patients), pre-prosthetic surgery, apicoectomy and retrofilcases, surgical crown lengthening, andbiopsy. Supportive topics include patientevaluation and case selection and the man-agement of problems such as bleeding andinfection. One chapter involves logisticalconsiderations and the use of basic surgicalprinciples for those volunteering services ina third-world setting.
This book is a ready reference for thesurgery-minded general practioner. Withinthese pages, the authors share many pearlsgleaned from years of experience and train-ing to increase the readers’ confidence andcompetence.
ix
Preface


Manual of Minor Oral Surgery
for the General Dentist


Chapter 1
Patient Evaluation and Medical HistoryDr. R. Thane Hales
3
IntroductionThe purpose of this book is to provide thegeneral dentist with specific informationabout oral surgery procedures that are per-formed daily in general dentists’ offices.Some advanced information is also given toprovide the more experienced general dentistthe opportunity to further his or her skillsand knowledge.
The ability of a general dentist to performthese procedures is based on a number offactors. Some dentists have a great interest insurgery, while others have very little interest.Some dentists have had a general practiceresidency or other postgraduate training orexperience; others may not have had the op-portunity. Some are in areas that have littleor no support from a specialist, which makessome surgery mandatory in their practices.Currently, it is accepted that regardless ofwho performs dental procedures, be they ageneralist or a specialist, the standards of careare the same. If a general dentist wants to in-clude the removal of third molars in his orher practice, he or she will usually need moretraining than that provided in dental school.
Just having the desire to do this procedurewill not, in and of itself, qualify a person.The best thing a general dentist can do is tofirst obtain additional training. Surgical ex-pertise is improved by taking postgraduatecourses. The clinician then learns to diagnosethe less complicated procedures and doesthem with supervision until they are per-formed well. State laws do not discriminatebetween a general dentist and a specialist. Alicense gives the same perogative to a gener-alist that an oral surgeon has to extract teeth.Therefore, the generalist has a greater re-sponsibility to acquire training and knowl-edge if he or she expects to do more complexprocedures. This responsibility includes notonly receiving instruction in step-by-stepsurgical techniques, but also the medicalmanagement of such patients and any com-plications that might arise.
Surgical skill is only part of the equation.The judgment of the practitioner in makingappropriate decisions regarding the patient’stotal condition is vital when doing surgicalprocedures. Anxiety management should beaddressed before the surgical procedure is

started. Will sedation be needed to accom-plish the treatment? Some patients requiresedation in order to make them feel com-fortable about the surgery. The dentist whodoesn’t fully understand the many facets oftreating an extremely anxious and medicallycompromised patient should find an appro-priate network of specialists in medicineand/or dentistry and then use a multidisci-plinary team approach.
Dentists must never forget the human el-ements of kindness, compassion, and caring.The patient wants to be treated just like anyperson would want to be treated. Dentistsneed to have enough insight into the pa-tients’ fears and concerns to be able to calmand reassure them that they can handle anyand all contingencies with competence. Alittle compassion and empathy go a long wayin today’s “rushed” society.
Humanism and compassion are the twomost important factors by which a patientjudges a dentist’s skill. Especially in the mindof the patient, the technical aspect of surgeryis secondary to the surgeon’s ability to man-age pain and anxiety. It is a given that a sur-geon has the ability to handle tissues withgreat skill, care, and judgment; the properhandling of and respect for tissues will en-able them to heal more quickly and withoutas many complications.
Medical HistoryThe most important information that a cli-nician can acquire is the medical history of apatient. If any problem is expressed in thehistory, a skilled clinician should be able todecide whether the patient is capable of un-dergoing the procedure. The dentist shouldbe fully able to predict how medical prob-lems might interfere with the patient’s abilityto heal and whether they might react to theanesthetic, antibiotics, or other medications.
The doctor needs to have a detailed ques-tionnaire that covers all major medical prob-lems that could exist in a patient and a space
on the form for any other condition notmentioned. The questionnaire must makesure that the doctor is advised of any com-plications a patient may have had in thepast. The doctor then must be able to fullyevaluate the patient’s situation relative to theprocedure.
In the process of getting medical informa-tion or even biographical data, the doctorshould observe the patient for any illogicalstatements or inconsistent responses thatmight need further evaluation. A bright,well-trained assistant is priceless in a privatepractice—especially during the filling out ofpatient forms and in helping to acquire ac-curate medical information. He/she shouldbring to the attention of the doctor anyproblem on the form that might influencethe procedure. The assistant must also high-light medical problems and mark the outsideof the chart with a coded warning that thepatient is at medical risk.
All medical questionnaires should includea history and description of the patient’schief complaint. Patients should fill out theform in their own words and give as muchinformation as they can about their prob-lems. The clarity of this information, accom-panied by careful and skillful questioning bythe doctor, can help him or her form a rea-sonable diagnosis. If the patient is unable tocompetently give this information, then allaspects of the information should be suspect.A diagnosis can be moved to the next steponly if there is a complete and reliable reviewof the patient’s status. The form should in-clude a statement of confidentiality reassur-ing patients that records will be protected.The only people having access to the recordswill be the doctors in the practice or thepatient’s physician (with permission of thepatient). A signature line is also required toverify that the patient has understood thequestions and that they have been answeredsatisfactorily.
Specifically, the medical history formshould include medical problems patients
4 C H A P T E R 1

might have that would compromise theirsafety (unless proper steps are taken by thedentist). The cardiovascular system is a mainconsideration. Any history of angina, my-ocardial infarction, murmurs, or rheumaticfever should be taken seriously, and appro-priate steps should be taken to protect thepatient. Other illnesses like hepatitis, asthma,diabetes, kidney disease, sexually transmitteddisease, seizures, artificial joints, heart valves,and specific allergies should be noted.Allergies that should be addressed are mainlythose to medications and other items used ina dental office, such as latex. The use of anyanticoagulants (which now include some ofthe common herbal compounds), corticos-teroids, hypertension medication, and othermedications should be thoroughly reviewed.1
Female patients, even young unmarried fe-males, should be asked whether there is anypossibility that they are pregnant. The med-ical history should be updated annually. Agood hygienist or assistant should interviewthe patient to find out whether there hasbeen any change since the patient’s last visit.The hygienist should then record thechanges on the chart and bring them to theattention of the doctor.
After the medical history form is filledout, the doctor sits with the patient and re-views the form in detail. It is crucial that thepatient understands everything they are talk-ing about. This is a good time to evaluate thepatient’s ability to respond and comprehendhis or her condition. Any signs of nervous orpsychological behavior should be noted. Theinterview should help determine whether thepatient is responsible enough for the physi-cian to trust the information the patient hasgiven on the medical form. If there is anydoubt, a responsible family member shouldbe consulted, and when necessary, a call tothe patient’s physician should be made.
Form 1.1 shows a typical medical historyform. Each provider must take responsibilityfor the content of his or her own forms.2
Another important legal paper that has
proven worthwhile is the consent to proceedform (Form 1.2). It gives added protectionto the office staff.2
HIPPAThe dentist is, of course, subject to HIPPA(Health Insurance Portability and Account-ability Act of 1996) regulations. HIPAArequires that all health plans, including theEmployee Retirement Income Security Act(ERISA), health care clearinghouses, and anydentist who transmits health information inan electronic transaction, use a standard for-mat. Those plans and providers that choosenot to use the electronic standards can use aclearinghouse to comply with the require-ment. Providers’ paper transactions are notsubject to this requirement. The security reg-ulations, which the Department of Healthand Human Services released under HIPPA,were conceived to protect electronic patienthealth information. Protected patient healthinformation is anything that ties a patient’sidentity to that person’s health, health care,or payment for health care, such as X-rays,charts, or invoices. Transactions includeclaims and remittances, eligibility inquiriesand response, and claim status and response.Self-training kits can be purchased from theAmerican Dental Association. Electronicprocessing has become the standard and, inmany ways, makes the provider’s life mucheasier.3
Physical ExaminationThe clinician or a well-trained hygienist orassistant should begin the exam with themeasurement of vital signs. This both servesas a screening device for unsuspectedmedical problems and gives a good baselinefor future evaluations. The technique ofmeasuring blood pressure and pulse rate isshown in Figure 1.1.
Despite elevated blood pressure beingcommon, the devices to examine this critical
PAT I E N T E V A L U AT I O N A N D M E D I C A L H I S T O R Y 5

6
Medical HistoryPatient’s Name _________________________________________________ Date of Birth________________________
Physician’s Name _______________________________________________ Phone number ______________________
Please answer the following questions as completely as possible1. Do you consider yourself to be in good health? YES NO2. Are you now or have you been under a physician’s care within the past year? YES NO
If yes, specify the condition being treated: ___________________________________________________________3. Do you take any medication, including birth control pills? YES NO
Please specify name and purpose of medication: __________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
4. Do you have or have you ever had any heart or blood problems? YES NO5. Have you ever been told that you have a heart murmur? YES NO6. Do you require antibiotic medication before treatment for a heart condition? YES NO7. Do you now have or have you ever had high blood pressure? YES NO8. Have you ever been diagnosed as being HIV positive or having AIDS? YES NO9. Have you ever had hepatitis or liver disease? YES NO
10. Have you ever had rheumatic fever, ___ asthma, ___ blood disorder, ____diabetes ___; rhermatism ____; arthritis ____; tuberculosis ___; venereal disease ___; heart attack ___; kidney disease ___; immune system disorder ___; any other diseases ___If so, specify: ________________________________________________________________________________
11. Do you bleed easily? YES NO12. Have you ever had any severe or unusual reaction to, or are you allergic to, any drugs, including the following:
Penicillin____ Ibuprofen_____Aspirin_____ Codeine_____Acetaminophen____ Barbiturates_____
Are you taking any of the following medications?Antibiotics _____ Digitalis or heart medication_____Anticoagulants (Blood thinners)______ Nitroglycerin_____Aspirin _____ Antihistamine_____Tranquilizers ______ Oral contraceptives_____Insulin_____
13. Do you faint easily? YES NO14. Have you ever had a reaction to dental treatment or local anesthetic? YES NO15. Are you allergic to any local anesthetic? YES NO16. Do you have any other allergies? YES NO
If yes, please describe: _____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
17. Have you ever had a nervous breakdown or undergone psychiatric treatment? YES NO18. Have you ever had an addiction problem with alcohol or drugs? YES NO19. Women: Are you or could you be pregnant YES NO
Are you breast feeding now? YES NO20. Are you in pain now? YES NO21. When did you last see a dentist?__________________________________________________________________22. Who was your last dentist? ______________________________________________________________________23. Are your teeth affecting your general health? YES NO24. Do you have or have you had bleeding or sensitive gums? YES NO25. Have you ever taken Fen Phen or similar appetite-suppressant drugs? YES NO26. Do you smoke? If yes, how many cigarettes a day YES NO27. Do you drink alcohol? If yes, how often YES NO
I hereby certify that the answers to the forgoing questions are accurate to the best of my ability. Since a change in my medicalcondition or in medications I take can affect dental treatment, I understand the importance of and agree to take the responsibil-ity for notifying the dentist of any changes at any subsequent appointment.
Signature ________________________________________________________________ Date __________________(Patient, legal guardian, or authorized agent of patient)
Form 1–1

7
Consent to Proceed
I herby authorize Dr._______________ and/or such associates or assistants as s/he may
designate to perform those procedures as may be deemed necessary or advisable to maintain
my dental health or the dental health of any minor or other individual for which I have
responsibility, including arrangement and/or administration of any sedative (including nitrous
oxide), analgesic, therapeutic, and/or other pharmaceutical agent(s) including those related to
restorative, palliative, therapeutic, or surgical treatments.
I understand that the administration of local anesthetics may cause an untoward reaction or
side effects, which may include, but are not limited to, bruising; hematoma; cardiac stimulation;
muscle soreness; and temporary or, rarely, permanent numbness. I understand that occasionally
needles break and may require surgical retrieval.
I understand that as part of dental treatment, including preventive procedures such as
cleanings and basic dentistry including fillings of all types, teeth may remain sensitive or even
possibly quite painful both during and after completion of treatment. After lengthy appointments,
jaw muscles may also be sore and tender. Gums and surrounding tissues may also be sensitive
or painful during and/or after treatment. Although rare, it is also possible for the tongue, cheek,
or other oral tissues of the mouth to be inadvertently abraded or lacerated during routine dental
procedures. In some cases sutures or additional treatment may be required.
I understand that as part of dental treatment, items including, but not limited to, crowns,
small dental instruments, drill components, etc. may be aspirated (inhaled into the respiratory
system) or swallowed. This unusual situation may require a series of x-rays to be taken by a
physician or hospital and may, in rare cases, require a bronchoscope or other procedures to
ensure safe removal.
I do voluntarily assume any and all possible risks, including the risk of substantial and
serious harm, if any, that may be associated with general preventive and operative treatment
procedures in hopes of obtaining the potential desired results, which may or may not be
achieved, for my benefit or the benefit of my minor child or ward. I acknowledge that the nature
and purpose of the forgoing procedures have been explained to me if necessary and that I have
been given the opportunity to ask questions.
Patient Name______________________________________________________________
Signature________________________________________________________________________(Patient, legal guardian, or authorized agent of patient)
Witness__________________________________________________________________
Form 1–2

vital sign are frequently not accurate. Thedentist must routinely calibrate blood pres-sure equipment against a standard mercuryinstrument and update the training of staffmembers periodically to ensure accuracy.Even when automated devices are used,those responsible for recording blood pres-sure must be properly trained, to reducehuman error.
Of the millions of people who have hy-pertension, a large percentage are unaware.The dental team can be instrumental in dis-covering this significant and life-threateninghealth problem. Current studies note thatnearly one-third of the U.S. population hashypertension—defined as a systolic bloodpressure higher than 139 mm Hg or a dias-tolic blood pressure higher than 89 mm Hg.Another one-quarter of the U.S. populationhas prehypertension—defined by a systolicblood pressure between 120 and 139 mmHg and a diastolic blood pressure between80 and 89 mm Hg.4 (Note: Recent publichealth trends are in the direction of advocat-ing even more conservative values than thosementioned here and in Table 1.1.)
Normal to various high values are illus-trated in Table 1.1.
Systolic and diastolic blood pressures, asopposed to pulse pressure, remain the best
means to classify hypertension. The risk ofstroke begins to increase steadily as bloodpressure rises from 115/75 mm Hg to highervalues.
About 15 to 20 percent of patients withstage I hypertension have elevated bloodpressure only in the office setting of a healthcare provider. This type of transient hyper-tension is more common in older men andwomen, and antihypertensive treatment inthese patients may reduce office bloodpressure but not affect ambulatory bloodpressure.
When the blood pressure reading is mildto moderately high, the patient should bereferred to their primary care physician forhypertensive therapy. The patient should bemonitored on each subsequent visit beforetreatment. If needed, the operator can useanxiety control protocol (see Table 1.2 laterin this chapter).
When severe hypertension exists, defertreatment and refer the patient to a primarycare or emergency room physician. Thesepatients can be walking potential strokevictims.
A pulse rate should be taken andrecorded. The most common method is touse the tips of the middle and index fingersof the right hand to palpate the radial arteryat the patient’s wrist. See Figure 1.1.
The heart rate is determined by countingthe number of pulses for 30 seconds and
8 C H A P T E R 1
Figure 1-1. Blood pressure and pulse. Mercurysphygmomanometers are still considered a goldstandard for blood pressure, but most offices nowuse digital equipment.
Table 1-1. Blood pressure classification
Systolic BP Diastolic BP Classification
<120 <80 Normal
120–139 80–89 Prehypertension
140–159 90–99 Stage 1 mild
hypertension
>160 >100 Stage 2 moderate
hypertension
>200 >110 Stage 3 severe
hypertension
BP = blood pressure.
then multiplying that number by two. Thisyields the number of beats per minute. Ifthere is a weakened pulse or irregularrhythm, elective treatment should not beperformed unless the operator has receivedclearance by the patient’s physician.
HEAD AND NECK EXAMINATION
The physical evaluation of a dental patientwill focus on the oral cavity and surroundinghead and neck region, but the clinicianshould also carefully visually evaluate the restof the patient for abnormalities.
The physical evaluation is usually accom-plished in four primary ways: inspection, pal-pation, percussion, and auscultation (listen-ing with a stethoscope to the sounds made bythe heart, lungs, and blood). The dentistshould also examine skin texture and look for possible skin lesions on the head, neck,and any other exposed parts of the body.Submandibular lymph nodes and those onthe neck should be palpated. Include exami-nation of the hair, facial symmetry, eye move-ments and conjunctiva color, and facialmasses. Inspect the oral cavity thoroughly, in-cluding the oropharynx, tongue, floor of themouth, and oral mucosa for any abnormal-looking tissue or indurated areas.
SUSPICIOUS LESIONS
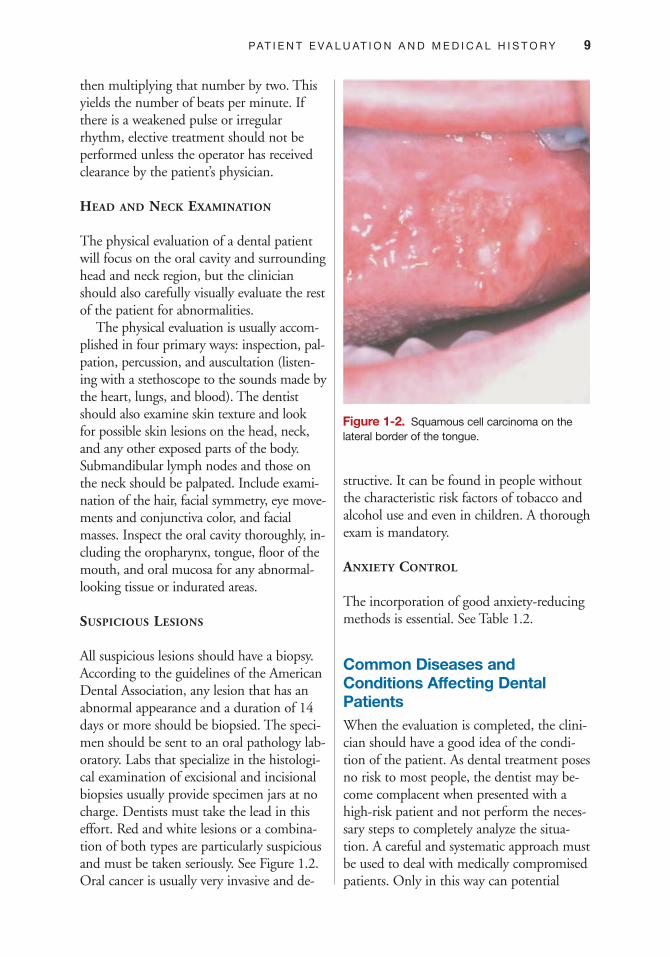
All suspicious lesions should have a biopsy.According to the guidelines of the AmericanDental Association, any lesion that has anabnormal appearance and a duration of 14days or more should be biopsied. The speci-men should be sent to an oral pathology lab-oratory. Labs that specialize in the histologi-cal examination of excisional and incisionalbiopsies usually provide specimen jars at nocharge. Dentists must take the lead in thiseffort. Red and white lesions or a combina-tion of both types are particularly suspiciousand must be taken seriously. See Figure 1.2.Oral cancer is usually very invasive and de-
structive. It can be found in people withoutthe characteristic risk factors of tobacco andalcohol use and even in children. A thoroughexam is mandatory.
ANXIETY CONTROL
The incorporation of good anxiety-reducingmethods is essential. See Table 1.2.
Common Diseases andConditions Affecting DentalPatientsWhen the evaluation is completed, the clini-cian should have a good idea of the condi-tion of the patient. As dental treatment posesno risk to most people, the dentist may be-come complacent when presented with ahigh-risk patient and not perform the neces-sary steps to completely analyze the situa-tion. A careful and systematic approach mustbe used to deal with medically compromisedpatients. Only in this way can potential
PAT I E N T E V A L U AT I O N A N D M E D I C A L H I S T O R Y 9
Figure 1-2. Squamous cell carcinoma on thelateral border of the tongue.

complications be managed or avoided.Following are a few of the most commondiseases and conditions that a clinician willencounter.
CARDIOVASCULAR DISEASE
The progressive narrowing of the arteries tothe heart leads to a difference in myocardialoxygen demand and supply. This demand
can be further increased by exertion, diges-tion, or anxiety during surgical procedures.When the muscle of the heart becomes is-chemic, it can produce pressure in the chestwith pain radiating to the arms, neck, or jaw.Other symptoms include sweating and aslowed heart rate. This condition is calledangina pectoris. Angina is usually reversibleif the proper medications and oxygen are ad-ministered quickly. Oxygen, nitroglycerin,and aspirin should be available in the office.
If, during the examination, the dentistdetermines that the patient has experiencedobstruction of the arterial blood flow to theheart, certain precautions must be taken.The practitioner’s responsibility to the pa-tient is to have necessary medications onhand and initiate preventive measures evenbefore treatment is begun. This will reducethe chance that a surgical procedure will pre-cipitate an anginal episode. If the patient iseasily prone to this condition, supplementaloxygen is recommended. Oral sedation ornitrous oxide can be helpful to relax thesepatients. If anginal pain is a problem duringa dental appointment, the operator shouldactivate the Emergency Medical System (call911). The patient’s physician should be con-sulted prior to subsequent appointments.
Giving a local anesthetic with epinephrineto a patient with a history of cardiac prob-lems has always been controversial, but gen-erally, the benefits outweigh the risks.Endogenous adrenalin surges in response topain stimulation can be equal to or moredangerous than the small amount of vaso-constrictor. It is recommended, however,that with these patients, the dose not exceed4 ml of local anesthetic and an epinephrineconcentration of 1:100,000, for a total adultdose of .04 mg per 30-minute period.1
Monitoring of the vital signs should bedone at regular intervals during surgery.Verbal contact should be ongoing andunforced. Always have a fresh bottle ofnitroglycerin and a good supply of oxygenavailable.
10 C H A P T E R 1
Table 1-2. Antianxiety protocol
01. Administration of a hypnotic agent to promote
sleep the night before the appointment for sur-
gery. (Ambien 10 mg)
02. Administer sedative agent for anxiety control 2
hours before surgery.
03. Make a morning appointment with little or no
waiting.
04. Give frequent verbal reassurances with other
distracting conversations not related to the
surgery.
05. Warn the patient before doing anything that is
uncomfortable.
06. Keep surgical instruments and needles out of
sight.
07. Administer nitrous oxide oxygen.
08. Administer local anesthetics carefully and use
those of sufficient duration and intensity.
09. Use epinephrine 1:100,000, but no more than
4 ml, for a total adult dose of 0.04 mg in any
30-minute period.
10. Administer intravenous sedation if available,
with sufficient monitoring incorporated by
licensed personnel.
11. After surgery give verbal and written instructions
on postoperative care.
12. Write prescriptions for effective analgesics.
13. Give reassurance and get information about
whom to call if problems arise.
14. Call the patient at home that evening to see
how they are doing and whether there are any
questions or problems.

Many scenarios should alert the dentistthat the patient is having more than angina.The following symptoms could indicate aheart attack or myocardial infarction (MI).Among them are the following:
1. The chest pain does not go away.2. The chest pain goes away but comes
back.3. The chest pain worsens.5
If these symptoms persist, the dentistmust get the patient to an emergency roomor call the Emergency Medical System (911).
MYOCARDIAL INFARCTION (MI)
Care must be taken with patients who have ahistory of MI. The blockage of a coronaryartery must be recognized and treated imme-diately. The infarcted area dies, becomesnonfunctional, and eventually necrotic. Themyocardium around the infarction is slightlydamaged but usually heals. It may form anidus that can precipitate abnormalrhythms.
The management of a patient with a his-tory of MI is as follows (as recommended bythe American Heart Association):
1. Consult the patient’s physician.2. Defer all elective procedures for at least
six months after an infarction. After clear-ance from the patient’s physician, imple-ment the antianxiety protocol. Givesupplemental oxygen during each dentalappointment.
3. Have nitroglycerin available. If oral sur-gery is needed, consider referring the pa-tient to an oral and maxillofacial surgeon.6
HEART BYPASS GRAFTS
Bypass graft patients should also be sched-uled for dental treatment no sooner than sixmonths after surgery. This is the routine un-less there have been complications during
healing—then it could be longer. Alwayskeep the anxious patient as relaxed as possi-ble. Carefully monitor the vital signsthroughout treatment. A pulse oximeter is agreat instrument to have attached to anypatient with a history of heart disease. If theoffice is equipped with a heart monitoringdevice (or EKG), it should be used to detectany arrhythmias.
CONGESTIVE HEART FAILURE
This disease of the heart occurs when themyocardium is unable to act as an efficientpump. The heart cannot deliver the outputnecessary to maintain the circulatory system,and the blood begins to pool and back up.The major effect is seen in the pulmonarysystem, the hepatic system, and the mesen-teric vascular beds.
The symptoms of congestive heart failureare orthopnea, ankle swelling, and dyspnea.Orthopnea is a shortness of breath when thepatient is lying down. The patient feels somecomfort in sleeping with the upper body ele-vated to enhance breathing. These patientsare usually on a variety of medications to re-duce fluids. Diuretics and digitoxin are ad-ministered to increase cardiac output. Thepatient may also be taking beta blockers orcalcium channel antagonists to control thework load of the heart.
Patients who are generally well controlledwith their medication can undergo routinedental surgery or other treatments. The den-tist should initiate anxiety control and givesupplemental oxygen during surgery.
Any clinician who serves the medicallycompromised heart patient must be wellqualified to handle emergencies. If not, he orshe should refer the patient to a specialist.
LIVER DYSFUNCTION
The patient who suffers from hepatic dam-age, usually from some infectious disease oralcohol abuse, will need to be given special
PAT I E N T E V A L U AT I O N A N D M E D I C A L H I S T O R Y 11

consideration. This would include a reduc-tion in dose or total avoidance of drugs thatare metabolized in the liver. This requires theprescribing dentist to be cognizant of themetabolic processes of the drug he or sheprescribes. The patient may be prone tobleeding because of the fact that many coag-ulation factors produced in the liver arediminished. A partial prothrombin time(PTT) or a prothrombin time (PT) is usefulin evaluation, especially in the severely liver-damaged patient. Many patients with liverdisease are infectious but can be managedwith routine universal precautions.
DIABETES
Diabetes is classified into insulin-dependentand non-insulin-dependant patients. Insulin-dependent diabetics usually have a history ofdiabetes from childhood or early adulthood.The underproduction of insulin is the majorproblem.
Elevated serum glucose short-term is not dangerous to the diabetic, but hypo-glycemia from not eating after an insulinload can cause disorientation and possiblediabetic or insulin shock. This state must betreated with a glucose load in order to stabi-lize the patient. A drink of orange juicewhen the patient is conscious is effective.Emergency kits should provide a safe modeof delivery for the needed glucose. To man-age an insulin-dependent diabetic, do the following:
01. Make certain the diabetes is well con-trolled. Consult the patient’s physicianbefore treatment is initiated.
02. Place the patient on an anxiety reduc-tion protocol if necessary but do not usedeep sedation.
03. Do not schedule long procedures andmake short morning appointments.
04. Ask the patient before proceeding whathe or she has eaten and whether he orshe has balanced it with insulin.
05. Monitor the patient’s vital signs con-tinuously.
06. Have the patient eat a normal breakfastwith the normal insulin dose.
07. Make sure that the patient is advised toadjust the insulin dose to the caloric in-take after the surgery. Difficulty in eat-ing may cause some alteration in bal-ance. Consult the patient’s physician ifnecessary.
08. Watch for signs of hypoglycemia.09. Keep in touch with the patient on the
development of infection. Do what isnecessary to prevent infection. If any isnoticed, treat it aggressively.
10. Have a source of glucose available in theoffice (orange juice, glucose package,etc.).1
In a non-insulin-dependant diabetic, alldental procedures can be performed withoutspecial precautions—unless the diabetes be-comes uncontrolled.7 Table 1.3 shows thesymptoms of hypoglycemia.
BLEEDING
Bleeding disorders are discussed in Chapter 10.
EPILEPSY
The most common type of seizure an epilep-tic patient will have is a grand mal episode.These episodes occur when an area of thebrain is depolarizing (firing) spontaneously.Ask the patient the following questionsbefore treatment:
• What type of seizures do you have?• What is the medication you are taking?• What is the aura you experience before the
seizure?
The drugs that are taken by an epilepticare CNS depressants. The most common areDilantin, Phenobarbital, Tegretol, andDepakote.
12 C H A P T E R 1

During the medical history find out thefrequency, severity, and duration of theepisodes from the patient and family mem-bers.7 Usually, the seizures last one to threeminutes. If one lasts five minutes or more, itcan be life-threatening. After an epilepticepisode of one or two minutes, the patientwill be extremely tired and usually disori-ented. The only thing you can do during theconvulsions is protect the patient from in-jury. No attempt is to be made to move thepatient to the floor. Insert any mouth propsbefore the procedure (tied with floss). Donot try to insert a mouth prop during anepisode, as you may damage the teeth orgingiva. These patients should be scheduledfor treatment within a reasonable time afterthe seizure-control medicine is taken.Consult with a family member and releasethem to a responsible adult.
PREGNANCY
The concern for the pregnant female is notonly her welfare but the care of the fetus.Potential genetic damage from drugs and ra-diation are serious concerns. It is always bestto defer surgery for the pregnant patientuntil after delivery.
The patient who requires surgery and/ormedication during pregnancy is at best in ahigh-risk situation and should be treated assuch. Drugs are rated by the FDA as to theirpossible effect on the fetus. These classifica-tions are A, B, C, D, and X. A classificationdrugs are the safest. D and X are the leastsafe. The most likely to have a teratogeniceffect are the D and X drugs, but doses of
C and even B drugs should be used with ex-treme caution.(8, 9)
Drugs considered the safest are acetamin-ophen, penicillin, codeine, erythromycin,and cephalosporin. Aspirin and ibuprofenare contraindicated because of the possibilityof postpartum bleeding and prolonging ofthe pregnancy.7
Avoid keeping the near-term patient in asupine position, as that position can com-press the vena cava and limit blood flow. Donot treat any pregnant patients in their firstor last trimester unless absolutely necessary.Even then, it is prudent to consult the pa-tient’s physician.
BREAST-FEEDING
Obviously, the doctor must not prescribemedications that are known to enter breastmilk and potentially affect infants. Only afew drugs commonly used in dentistry couldharm an infant. Some of these include hy-drocortisones, tetracyclines, metronidazole,and aminoglycosides.
Acceptable drugs delivered during breast-feeding can be administered according to theage and size of the baby. The older the child,the less chance of a problem with the drug.The duration of the medication is also a fac-tor. Any drug given long-term must beavoided unless prescribed by the mother’sphysician. Any drug that is commonly ad-ministered to an infant should be fine to ad-minister to a breast-feeding mother, but theduration should be shortened.8 See Table 1.4 for a list of drugs that can be used spar-ingly and of those that would harm a breast-fed infant.
Basic Life SupportIt is essential that all office personnel attenda training program in basic life support. Abrief review of the technique is appropriatehere.
The acronym for treating emergencies is
PAT I E N T E V A L U AT I O N A N D M E D I C A L H I S T O R Y 13
Table 1-3. Signs of diabetic hypoglycemia
Frequent urination Pale
Excessive thirst Sweating
Extreme hunger Increased fatigue
Unusual weight loss Disoriented
Irritability Blurry vision

PABC and D. This acronym is used in allemergencies—not just heart attacks.
P PositionA AirwayB BreathingC CirculationD Definitive treatment
A brief description of each letter is asfollows.
P, POSITIONING THE PATIENT
Positioning the patient is the first step. Theright position is the one that is most com-fortable for the patient, if conscious. For car-diac arrest, the patient needs to be flat on hisor her back. If asthmatic, patients probablywill want to sit up, which helps their abilityto breathe. If a patient is conscious, he or shecan tell you what position feels the best. Ifthe patient is unconscious, place the patienthorizontally with the feet slightly elevated.The most common reason the patient losesconsciousness is low blood pressure. Withthe feet elevated slightly, the patient can re-ceive a larger flow of blood to the head and,thus, stimulate the brain. The patient canstill breathe in the horizontal or supine posi-tion, but the head must be on the sameplane as the heart, not lower.
A, AIRWAY
The second letter in the acronym is for air-way. Airway management is critical in an un-conscious patient. The head is tilted back,and the chin is lifted. One hand is placed onthe forehead, with two fingers of the otherhand on the mandible to rotate the headback. The tongue is attached to themandible so that when you pull themandible forward, the tongue also movesforward. This opens the airway so the pa-tient can breathe, or so you can breathe forthe patient. Make sure that no obstructionsare in the mouth or throat.
B, BREATHING
The person attending must place his or herear one inch away from the patient’s nose.Watch the chest and see whether it is mov-ing. The chest may move, indicating that thepatient is trying to breathe, but it does notmean the patient is breathing. The patientmight have an obstruction. It is crucial thatyou feel air coming through the mouth ornose. In a cardiac arrest, the patient must besupine but not have the heart higher thanthe head. The legs can be elevated slightly toincrease the blood flow to the brain, but ifthe heart is higher than the head, breathingbecomes more difficult.
If the patient is not breathing, it is calledapnea. The rescuer must provide supple-mental breathing to the victim to oxygenatethe blood.
C, CIRCULATION
Maintain the head tilt and check for thecarotid pulse. Knowing how to check thecarotid pulse is critical. Studies have shownthat the carotid pulse is missed 40 percent ofthe time by medical personnel and para-medics. To locate the carotid artery, maintainhead tilt and place the fingers on the Adam’sapple or thyroid cartilage. The fingers are
14 C H A P T E R 1
Table 1-4. Breast-feeding mothers and drugs
Drugs that can be Drugs that are potentially used sparingly harmful to the infant
Acetaminophen Ampicillin
Antihistamines Aspirin
Codiene Atropine
Erythromycin Barbiturates
Flouride Chloral hydrate
Lidocaine Diazepam
Meperidine Metronidazol
Oxacillin Penicillin
Clindamycin Tetracyclines

then, with moderate pressure, slid down theneck toward the rescuer, into a groove on theside of the neck formed by the sternocleido-mastoid muscle. The carotid artery is locatedin that groove. See Figure 1.3. The pulseshould be checked for 10 seconds. If a pulseis not felt, start compressions immediately.You are now circulating oxygenated blood tothe victim’s brain. With the 2005 AmericanHeart Association changes, a lay rescuer doesnot assess signs of circulation before begin-ning chest compressions.
D, DEFINITIVE TREATMENT
The final part of the equation is the diagno-sis of the problem. If the doctor can diag-nose the problem, then, if trained to do so,he or she can give the patient the appropri-ate medication. However, remember thatdrugs do not save the patient; proper lifesupport does. If the dentist is not trained inAdvanced Cardiac Life Support (ACLS),then it is best to continue with basic life sup-port until help arrives.
Clinical signs are what the doctor can see,and symptoms are what the patient tells you.Signs and symptoms of concern are as follows:
1. Altered consciousness2. Respiratory depression
3. Allergic reaction4. Chest pain(1, 10)
BASIC LIFE SUPPORT, CPR
The following is a step-by-step outline ofcardiopulmonary resuscitation. This list isfor review but is not intended to replace for-mal training.
Cardiopulmonary Resuscitation (CPR)1. Call 911
Check the victim for unresponsiveness. Ifthere is no response, call 911 and returnto the victim. Ask for assistance. In mostlocations, the emergency dispatcher canassist you with CPR instructions. If youare not alone, have someone else call andyou begin CPR.
2. BreatheClear the mouth of any foreign objects.Tilt the head back, lift the chin up, andlisten for breathing. Put your ear one inchfrom the victim’s nose and mouth. If thepatient is not breathing normally, pinchhis or her nose, cover the mouth withyours, and blow until you see the chestrise. Give two breaths. All breaths shouldbe given over 1 second with sufficient vol-ume to achieve visible chest rise.
PAT I E N T E V A L U AT I O N A N D M E D I C A L H I S T O R Y 15
Figure 1-3. Carotid pulse. The carotid pulse ismissed 40 percent of the time.
Figure 1-4. Listen for breathing.

3. Chest CompressionsIf the victim is unconscious and unre-sponsive, begin chest compressions. Pushdown on the chest 1 1/2 to 2 inches, 30times right between the nipples. On asmall child or infant, compress the chest 1 to 1.5 inches. Compress the chest at therate of 100/minute. The rescuer shouldthen breathe twice for every 30 compres-sions.
Continue administering CPR until helparrives. Paramedics will continue life supportand transport to a medical center or emer-gency room.
CHOKING
When a patient has a foreign body lodgedin the throat, it is important to act immedi-ately. Most of the time the dentist is able toquickly remove the object before it gets toofar into the trachea to see. If patients strug-gle, they will usually grab the throat. This isthe universal sign for choking. The followingsteps are to be followed for adults as well aschildren.
First Aid for a Choking Conscious Adultand for Children (1–8 years old)
Determine whether the person can speak orcough. If not, proceed to the next step.Perform an abdominal thrust (Heimlich ma-neuver) repeatedly until the foreign body isexpelled. See Figures 1.7 and 1.8. A chestthrust may be used for markedly obese per-sons or those in the late stages of pregnancy.If the adult or child becomes unresponsive,perform CPR; if you see an object in thethroat or mouth, remove it.
16 C H A P T E R 1
Figure 1-5. Breathe two breaths for two sec-onds each.
Figure 1-6. Chest compressions.
Figure 1-7. Heimlich maneuver. Repeat abdomi-nal thrusts.
Emergency KitSeveral emergency kits on the market con-tain the basic drugs and apparatus to help incertain emergencies.
Epinephrine is the only drug that is ofimmediate help with anaphylaxis but it mustbe given within the first few minutes ofsymptoms. This is the only drug you shouldhave in a preloaded syringe. See Figure 1.9.
PAT I E N T E V A L U AT I O N A N D M E D I C A L H I S T O R Y 17
Figure 1-8. Floor position for abdominal thrusts.
Figure 1-9. Epinephrine syringe. This is the only drug that should be preloaded in an emer-gency kit.
Figure 1-10. Emer-gency kit.

Epinephrine can be administered into thethigh muscle right through the clothing ifnecessary. Each minute that passes withoutepinephrine when a patient is experiencinganaphylactic shock considerably lessens thechances of recovery. You can give 1 cc of1:1000 epinephrine up to three times inintervals of five minutes. Also administeroxygen. Do not leave the patient until helparrives.
A good emergency kit should include thefollowing:
01. Ammonia inhalants02. Tourniquet03. CPR pocket mask04. Epinephrine in a preloaded syringe
(1:1000)05. Diphenhydramine06. Albuterol inhaler07. Syringes08. Nitrolingual spray or nitroglycerin
tablets09. Aspirin10. Glucose11. CPR pocket mask
ConclusionMany medical problems can and do occurwith dental treatment. Prevention is the keyto successful and uneventful procedures. Wemust know our patients and be clearly awareof their health status. Each patient who hashealth concerns in their medical history
must be evaluated thoroughly. If the clini-cian is not aware of the effect surgery orroutine dental treatments will have on thepatient, then a consultation with thepatient’s physician is mandatory. We must be prepared for possible medical problemsand have a good understanding of basic lifesupport measures.
Bibliography01. L. Peterson, E. Ellis, J. Hupp, M. Tucker.
Contemporary Oral and Maxillofacial Surgery, 4thedition. St. Louis: Mosby, 2003.
02. Adapted from Professional Insurance Exchangestandard consent to proceed form, March, 2005.
03. American Dental Association Health InsurancePortability and Accountability Act, HIPPA, re-quirements at ADA.org.
04. L. Barclay, C. Vega. The American HeartAssociation Updates Recommendations for BloodPressure Measurements. Medscape Medical News,www.medscape.com, Dec., 2004.
05. S.F. Malamed. Emergency Medicine. MillenniumProductions DVD, 2003.
06. Basic Life Support for Healthcare Providers,American Heart Association, 1997.
07. J. Little, D. Falave, C. Miller, N. Rhodus. DentalManagement of the Medically Compromised Patient,6th edition. St Louis: Mosby, 2002.
08. T.W. Hale, Medications and Mother’s Milk: AManual of Lactational Pharmacology, 11th ed.Pharmasoft Publishing L.P., Amarillo, TX, 2004.
09. Pregnancy categories for prescription drugs, FDADrug Bull. 1982.
10. S. F. Malamed. Medical Emergencies in the DentalOffice, 5th edition. St. Louis: Mosby, 1999.
18 C H A P T E R 1