mandated benefits for a new provider class: licsw's
TRANSCRIPT

Clinical Social Work Journal Vol. 13, No. 4, Winter 1985
MANDATED BENEFITS FOR A NEW P R O V I D E R CLASS: LICSW's
Wil l i am Da ley S t ephen P. McLane
ABSTRACT: The purpose of this study is to assess the initial impact of Li- censed Independent Clinical Social Workers (LICSW's) as a new reimbursable provider class in an insured population with mandated nervous and mental bene- fits. History of nervous and mental therapy, previous provider type, age, and sex are examined. Data were obtained from Blue Shield of Massachusetts' nervous and mental claim information from 1979 through 1982 for all patients who saw a social worker during the year of LICSW certification. Results show (1) a large ma- jority of the 1982 social worker patients had no billable psychiatric experience for the three years prior to 1982; (2) the longer a patient is in treatment, the less likely is a provider type switch; and (3) psychologists' patients are more likely to switch to a social worker than psychiatrists' patients. A concern remains for this insurer over the increase in the total number of psychiatric services concomitant with a new provider class introduction.
I N T R O D U C T I O N
Effor ts to include the services of social worke r s unde r th i rd p a r t y re- i m b u r s e m e n t h a v e h a d cons iderable success on both s t a te and na t ion l levels. However , t he re cont inues to be a pauc i ty of r e l e v a n t da t a in the a r ea s of u t i l iza t ion , cost and demograph ics . Consequent ly , i t is difficult to assess the effect of th is p rov ide r group on t r ends in the de l ivery of m e n t a l h e a l t h fee-for-service care.
The P re s iden t ' s Commiss ion on M e n t a l H e a l t h (1978) s tates:
We must improve mental health activity reporting and expand the mental health database in order to evaluate effective mixes of service, resources and need. Such findings should include total cost, unit cost, and length of t reatment by diagnosis and patient characteristics.
Wi th in th i s r epo r t special cons idera t ion was g iven to compar i sons of ser- vices by va r ious m e n t a l h e a l t h p rov iders (e.g., psych ia t r i s t , psychologis t , and cl inical social workers) .
367 �9 1985 Human Sciences Press

368
CLINICAL SOCIAL WORK JOURNAL
In light of tha t message, this report will be the first of several de- signed to investigate the impact of a new provider class on mental health utilization. Based on the experience of Blue Cross and Blue Shield of Massachusetts, Inc., research was targeted towards the following objectives:
�9 Assess utilization of Licensed Independent Clinical Social Workers. �9 Examine the impact of Licensed Independent Clinical Social Work-
ers on other providers of mental health services. To what extent does a shift in provider type occur?
�9 Differentiate utilization of mental health services by selected socio- demographic characteristics.
Massachusetts has a Mental and Nervous Mandate requiring all heal th insurers to provide a minimum level of coverage for diagnoses as- sociated with mental and nervous conditions and alcoholism. This benefit package was included in every Blue Cross and Blue Shield of Massachu- setts contract writ ten or renewed effective January 1, 1976. This policy for mental and nervous conditions include inpatient coverage in a li- censed general hospital equivalent to any other illness, 60 days per calen- dar year in a psychiatric hospital, and up to $500 in outpatient coverage over a 12-month period. For the first time, reimbursement was required for services rendered by a licensed psychologist.
In 1977, the Commonwealth of Massachusetts enacted the social work licensing law (G.L.C. 112, Section 130-137) which specifically au- thorizes the Licensed Independent Clinical Social Worker (LICSW):
To render professional services for any fee, monetary or otherwise, to individuals, families, or groups of individuals, which services involve the application of social work theory and methods in the treatment of mental and emotional disorders through the use of psychotherapy of a nonmedical nature by an individual who is not providing such ser- vices under the employ of a recognized educational institution, or an institution, facility, or agency which is licensed to operate under the laws of the Commonwealth.
On December 24 1981, a vendorship bill was signed becoming Chap- ter 737 of the laws of the Commonwealth requiring insurance coverage for mental heal th services rendered by a Licensed Independent Clinical Social Worker. Under this regulation LICSWs have been granted inde- pendent vendorship status requiring neither physician referral or supervision.
The provision of insurance coverage for psychiatric disorders contin- ues to be a controversial issue, within which parity between health and mental heal th benefits packages is a major concern.

369
WILLIAM DALEY AND STEPHEN P. MCLANE
Those favoring the addition of new providers and/or the expansion of coverage cite several studies which indicate that the inclusion of mental heal th services within an insurance package will not lead to excessive use, and that utilization eventually levels off at a reasonable percentage of total benefits (Reed, 1975; Sharfstein, 1978; Hustead, & Sharfstein, 1978; Liptzin, Regier, Goldberg, 1980).
Other proponents have speculated that greater availability of mental heal th professionals would not only improve consumer access to qualified care, but also increase consumer choice if not direct competition among the recognized professions. In fact, this was the major thrust of the LICSW vendorship proponents in their legislative efforts.
A review of l i terature on the reluctance of third-party payers to in- clude or expand benefits for mental and nervous disorders reveals the following:
1. If studies concerning the prevalence of mental illness are correct, no prepayment mechanism could cope at a premium level the public would pay (Avnet, 1969).
2. Demand elasticities make psychiatric care hard to insure than other types of medical care; i.e., the demand for mental health care is sen- sitive to the elimination of copayments and deductibles (Maguire, 1981). Therefore, overutilization may become a seriuos problem.
3. "Moral hazard" can disrupt the foundation upon which insurance principles are founded. Once a service is covered, a policyholder may self-select a course of t reatment he would not otherwise have chosen if payment for that service were to be made out-of-pocket (Sharfstein, & Taube, 1982; Shavell, 1979; Pauly, 1968).
4. Adverse selection could pose too much of a financial risk for insurers to handle. High utilizers may accumulate disproportionately in a more comprehensive plan or between plans offering similar cover- age but differing in deductibles and copayments (Maguire, 1981; Sharfstein & Taube, 1982).
5. Increases in both coverage and number of providers could lead to ex- orbitant overutilization of services and again subsequent elasticity of demand (Patterson, 1978).
Other areas of concern expressed by insurance carriers include:
Since many psychiatrists ' assistants, counselors, therapists, and li- censed social workers have equivalent educational background and years of patient work, the licensing of independent clinical social workers would establish a precedent, paving the way for numerous providers to utilize legislative mandates to become independent practitioners.

370
CLINICAL SOCIAL WORK JOURNAL
�9 Licensed independent clinical social workers are not allowed to pre- scribe medication, administer or interpret psychological testing, or to authorize a patient 's commitment to a mental hospital. Thus the licensed independent clinical social worker's t rea tment options are limited in comparison to the psychiatrist or psychologist.
Leading to the development of this study was the experience tha t Blue Shield of Massachusetts has in providing mental and nervous cover- age under a mandatory benefit package. Given the limitations of insur- ance data, it is difficult to address such topics as efficacy, appropriateness or medical necessity. However, observations from this experience include:
1. Prior to the implementation of the mandate (1976), mental and ner- vous services had accounted for less than two percent of all units of service. Claim payments for ambulatory mental heal th services amounted to approximately $2 million. By 1980, 10.2 percent of all units of service and 12.1 percent of claim payments were due to mental and nervous services. Currently, these benefits have reached 12 percent of units of service and over 14 percent of all claim payments. A review of payment experience reveals that most of the increase was in outpatient claims which rose from an average of less than $200,000 per quarter to more than $10,000,000 over these years.
2. The 50-minute psychotherapy session ranks first on the list of the "most costly" procedures and nearly twice as much money was paid for this type of claim as for the next procedure; i.e., materni ty care.
3. Transient situation disturbances, anomalously and perennially, ranked among the highest of disorder categories for all provider types. Previous industrywide studies have:
a. Payout stabilized at 7.5 percent for a period of five years (Reed, 1975).
b. Survey of major insurers stated: five percent of the total number of claims are for mental heal th (GLS Associates, 1979).
This experience provides fertile ground for study into how utilization of mental heal th services can be affected by third-party reimbursement.
METHODOLOGY
The source of data utilized in this study is Blue Shield of Massachusetts nerv- ous and mental claim information from 1979 to 1982 for all patients who saw a so-

371
WILLIAM DALEY AND STEPHEN P. MCLANE
cial worker during the index year of LICSW certification; i.e., 1982. Annualiza- tion ratios are based on quarterly totals of the number of social workers certified for reimbursement and the number and size of groups eligible for social worker coverage by enrollment date.
Maximum likelihood estimators (MLE) are calculated to provide tests of sig- nificance for given tables (Bishop, Fienberg, & Holland, 1975).
RESULTS
The data show tha t 3,092 individuals saw a social worker during the year 1982. Of those, 2,200 (71%) saw social workers as their exclusive mental and nervous therapist; the remainder (29%) saw a social worker in consultation with a psychiatrist or psychologist. Among those who saw only a social worker, there were 1,771 (81%) individuals who had no bill- able psychiatric experience in the three years prior to 1982. That group was seen by 568 (36%) of the total 1,590 social workers eligible for Blue Shield reimbursement.
If social worker patients by the actual number of social workers eligi- ble for reimbursement per quarter during this initial year of their certifi- cation were annualized (Table I), the increase in number of patients see- ing only social workers in 1982 with no previous psychiatric care (ceteris paribus) would be 2,922. Coverage for social worker therapy was included at each group's anniversary date. Estimates for one year utilization are at tained by considering the number and size of groups by enrollment date. The number of new social worker patients expected per year equals 6,516 (a full year of LICSW eligibility and all accounts effective for the same time).
TABLE 1
NUMBER OF LICSWs REGISTERED BY CALENDAR QUARTER
1st QUARTER: 0 2nd QUARTER: 915 3rd QUARTER: 424 4th QUARTER: 251
TOTAL: 1,590
Two hundred nineteen (219) patients who switched exclusively to so- cial workers as their mental and nervous providers in 1982 had continu- ous psychiatric care prior to 1982 for at least one year. Forty-four (20.09%) individuals switched to a social worker after three years of con- tinuous care, 61 (27.85%) switched after two years of care, and 114
372
CLINICAL SOCIAL WORK JOURNAL
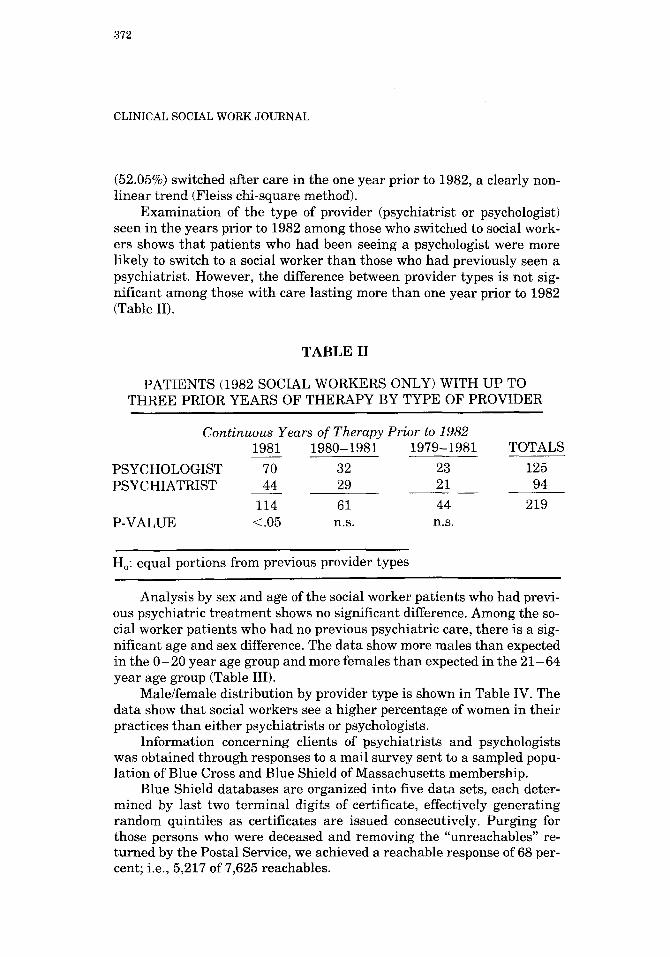
(52.05%) switched after care in the one year prior to 1982, a clearly non- l inear t rend (Fleiss chi-square method).
Examinat ion of the type of provider (psychiatrist or psychologist) seen in the years prior to 1982 among those who switched to social work- ers shows tha t patients who had been seeing a psychologist were more likely to switch to a social worker than those who had previously seen a psychiatrist. However, the difference between provider types is not sig- nificant among those with care lasting more than one year prior to 1982 (Table II).
TABLE II
PATIENTS (1982 SOCIAL WORKERS ONLY) WITH UP TO THREE PRIOR YEARS OF THERAPY BY TYPE OF PROVIDER
PSYCHOLOGIST PSYCHIATRIST
P-VALUE
Continuous Years of Therapy Prior to 1982 1981 1980-1981 1979-1981 TOTALS
70 32 23 125 44 29 21 94
114 61 44 219 .05 n.s. n.s.
Ho: equal portions from previous provider types
Analysis by sex and age of the social worker patients who had previ- ous psychiatric t rea tment shows no significant difference. Among the so- cial worker patients who had no previous psychiatric care, there is a sig- nificant age and sex difference. The data show more males than expected in the 0 -20 year age group and more females than expected in the 21-64 year age group (Table III).
Male/female distribution by provider type is shown in Table IV. The data show tha t social workers see a higher percentage of women in their practices than either psychiatrists or psychologists.
Information concerning clients of psychiatrists and psychologists was obtained through responses to a mail survey sent to a sampled popu- lation of Blue Cross and Blue Shield of Massachusetts membership.
Blue Shield databases are organized into five data sets, each deter- mined by last two terminal digits of certificate, effectively generating random quintiles as certificates are issued consecutively. Purging for those persons who were deceased and removing the "unreachables" re- turned by the Postal Service, we achieved a reachable response of 68 per- cent; i.e., 5,217 of 7,625 reachables.

373
WILLIAM DALEY AND STEPHEN P. MCLANE
TABLE III
FREQUENCY OF PATIENTS (SOCIAL WORKER ONLY--1982) BY AGE, SEX, AND PREVIOUS CARE CATEGORY
Previous Care
YES NO
Age M A L E F E M A L E T O T A L MALE F E M A L E T O T A L 0-20 13 18 31 133 166 299 21-64 55 132 187 427 1,041 1,468
68 150 218 560 1,207 1,767
Age by Sex: p <.01 Previous Care by Age: n.s. Sex by Previous Care n.s. Age by Sex by Previous Care: n.s.
TABLE IV
MALE/FEMALE DISTRIBUTION BY PROVIDER TYPE
SEX PSYCHIATRIST PSYCHOLOGIST SOCIAL WORKER
MALE 44% 43% 32% FEMALE 56% 57% 68%
Sex by Provider Type: p <.01
Methods due to Dillman (1978), were employed, with a total of three mailings.
Nonrespondents were examined for age, sex, and family size and found to be statistically similar with the respondent population (Yates, 1960; Moser, 1959) giving reasonable confidence the response group is quite similar to the total universe. Systematic sampling was used after a random number and skip interval were obtained. This rendered four groups of respondents:
1. Medical claims only. 2. Nervous and mental claims only. 3. Medical and nervous and mental claims only. 4. No claims.

374
CLINICAL SOCIAL WORK JOURNAL
For purposes of Table V only groups two and three were examined and the response rate was not statistically different (Sokal, 1969). Furthermore, respondents and nonrespondents were very similar by age, etc.
1.
2. 3. 4. 5. 6. 7. 8. 9.
10.
TABLE Va
PSYCHIATRISTS RANK ORDER NERVOUS/MENTAL DIAGNOSES 1982
3105 3173 3100 3109 3082 3172 3171 3093
Depressive Neurosis Adjustment Reaction Adult Life Anxiety Neurosis Neuroses (Other and Unspecified) Manic Depressive (Depressed Type) Adjustment Reaction Adolescence Transient Situational Disturbance Psychotic Depression Reaction
3089 Manic Depressive Unspecified Y908 NEC
UNITS OF
SERVICE
137,873 58,692 58,337 19,902 15,541 13,710
8,908 7,011 6,839 4,986
1. 3105 2. 3173 3. 3100 4. 3172 5. 3109 6. 3092 7. 3171 8. 3082 9. 3004
10. 3009
TABLE Vb
LICSWs RANK ORDER NERVOUS/MENTAL DIAGNOSES 1982
Depressive Neurosis Adjustment Reaction Adult Life Anxiety Neurosis Adjustment Reaction Adolescence Neuroses (Other and Unspecified) Other Paranoid States Transient Situational Disturbance Manic Depressive (Depressed Type) Post-Partum Depression Unspecified Physical Condition
UNITS OF
SERVICE
4,836 4,754 3,838 1,160
783 781 566 496 496 308

375
WILLIAM DALEY AND STEPHEN P. MCLANE
TABLE Vc
PSYCHOLOGISTS RANK ORDER NERVOUS/MENTAL DIAGNOSES 1982
UNITS OF
SERVICE
1. 3173 Adjustment Reaction Adult Life 126,289 2. 3105 Depressive Neurosis 81,528 3. 3100 Anxiety Neurosis 57,794 4. 3172 Adjustment Reaction Adolescence 27,577 5. 3171 Transient Situational Disturbance 23,035 6. 3118 Passive-Aggressive Personality 7,066 7. 3109 Neuroses (Other and Unspecified) 6,267 8. 3119 Other and Unspecified Personality Disorder 3,981 9. 3104 Obsessive-Compulsive Neurosis 3,750
10. 3082 Manic Depressive (Depresse(~ Type) 3,446
DISCUSSION
These data show that a large number of patients entered therapy (de- fined as new to Blue Shield of Massachusetts recording) in 1982 with so- cial workers. Three possibilities exist:
1. Patients previously saw LICSWs previous to 1982 and paid out-of- pocket and didn't enter Blue Shield of Massachusetts databases.
2. LICSWs are an attractive alternative to psychiatrists when the ses- sions become reimbursable.
3. The addition of any new provider class will reinforce the insurance maxim tha t "care chases dollars," meaning LICSWs are actively casefinding patients or that any new supply will automatically gen- erate new demand.
With only an initial year of data, we are hesitant to advocate which of the above is the genuine dynamic occuring at Blue Shield of Massachusetts.
However, LICSWs who are predominately females, did see propor- t ionately larger numbers of female patients than did the other two disci- plines, especially in the adult, not child or adolescent group.
An enormous amount of work was expended in purging and puri- fying Blue Shield of Massachusetts files to produce this report. While it is introductory in nature, the topic of benefit influence on utilization pat- terns is very important, especially mandated benefits. Clearly, previous care is a parameter worthy of more study for both its presence and dura-

376
CLINICAL SOCIAL WORK JOURNAL
tion. Fidelity to provider, i.e., continuous therapy with one type of pro- vider, is also addressed in this analysis. It is shown that the longer a per- son is in treatment, the less likely he is to change provider type. The highest percentage of individuals switched to a social worker after ther- apy for only one previous year. The lowest percentage of individuals switched to a social worker after three years of prior care. Therapist- patient bonds which are sustained over longer time periods are less likely to be broken. Type of provider seen also has an effect on the tendency to switch to a social worker. Psychologists' patients are more likely to switch to a social worker than psychiatrists' patients. Blue Shield of Mas- sachusetts plans to either survey the LICSW groups in an inquiry of who did pay out of pocket before or examine our 1983 data quite soon or do both.
The results are both interesting and factual and we invite the reader- ship to draw their own conclusions.
REFERENCES
Avnet, H. (1969). Psychiatric insurance . . , ten years later. American Journal of Psychiatry, 126, 113-120.
Bishop, Y.M.M., Fienberg, S.E., & Holland, S.E. (1975). Discrete multivariate analysis. Cambridge: M.I.T. Press.
Dillman, D. (1978). Mail and Telephone Survey The Total Design Method. New York: Wiley & Sons.
G.L.S. Associates (1979). Analysis of State Programs Which Mandate Mental Health Bene- fits Under Private Health Insurance. N.I.M.H. # 278-780040 (M.H.).
Hustead, E., & Sharfstein, S. (1978). Utilization and cost of mental illness coverage in the federal employees health benefits program. American Journal of Psychiatry, 135, 315-319.
Liptzin, B., Regier, D., & Goldberg, I. (1980). Utilization of health and mental health ser- vices in a large insured population. American Journal of Psychiatry, 137, 553-558.
Maguire, T. (1981). Financing psychotherapy cost effects and public policy. Cambridge: Bal- linger Publishing Company.
Moser, C. (1959). Survey methods in social investigation. Melbourne: Heinemann Ltd. Pattersn, D.Y. (1978). Unlimited mental health coverage? No!! Psychiatric News, 3. Pauly, M. (1968). Economics of moral hazard: Comment. American Economic Review, 58,
531-536. President's Commission on Mental Health (1978). Cost/Financing, 2, 528-529. Sharfstein, S. (1978). Third party payers: To pay or not to pay. American Journal of Psychia-
try, 135, 1185-1188. Sharfstein, S., & Taube, C. (1982). Reductions in insurance for mental disorders: Adverse
selection, moral hazard and consumer demand. American Journal of Psychiatry, 139, 1425 - 1430.
Shavell, S. (1979). On moral hazard and insurance. Quarterly Journal of Economics, 94, 541-562.
Sokal, R., & Rohlf, F. (1969). Biometry. San Francisco: W.H. Freeman. Reed, L.S. (1975). Coverage and Utilization of Care for Mental Conditions under Health
Insurance-Various Studies 1973-74. Washington, D.C.: American Psychiatric Association.
Yates, F. 91960). Sampling methods for census and surveys. New York: Griffin.
1000 Summer Street Boston, MA 02110