managing monitor alarms: lessons learned - cloud...
TRANSCRIPT
MANAGING MONITOR ALARMS: LESSONS LEARNED
MARIA CVACH, RN, MSN, CCRNASSISTANT DIRECTOR OF NURSING , CLINICAL STANDARDS
THE JOHNS HOPKINS HOSPITAL
October 5th , 2011
Maria Cvach, RN, MSN, CCRN Assistant Director of Nursing, Clinical StandardsThe Johns Hopkins Hospital
Monitor Alarm Task Force Standardizing practices throughout JHH Cardiac and Physiological Monitor Policy
Physician‐Led Alarm Management Committee Revise defaults to actionable levels, house‐wide Develop criteria for placement on and discontinuation of
physiologic monitors
New Clinical Building‐related Pilots for Alarm Management Contracted with ECRI for NCB Alarm Management
ALARM MANAGEMENT INITIATIVES
April 27,
2011
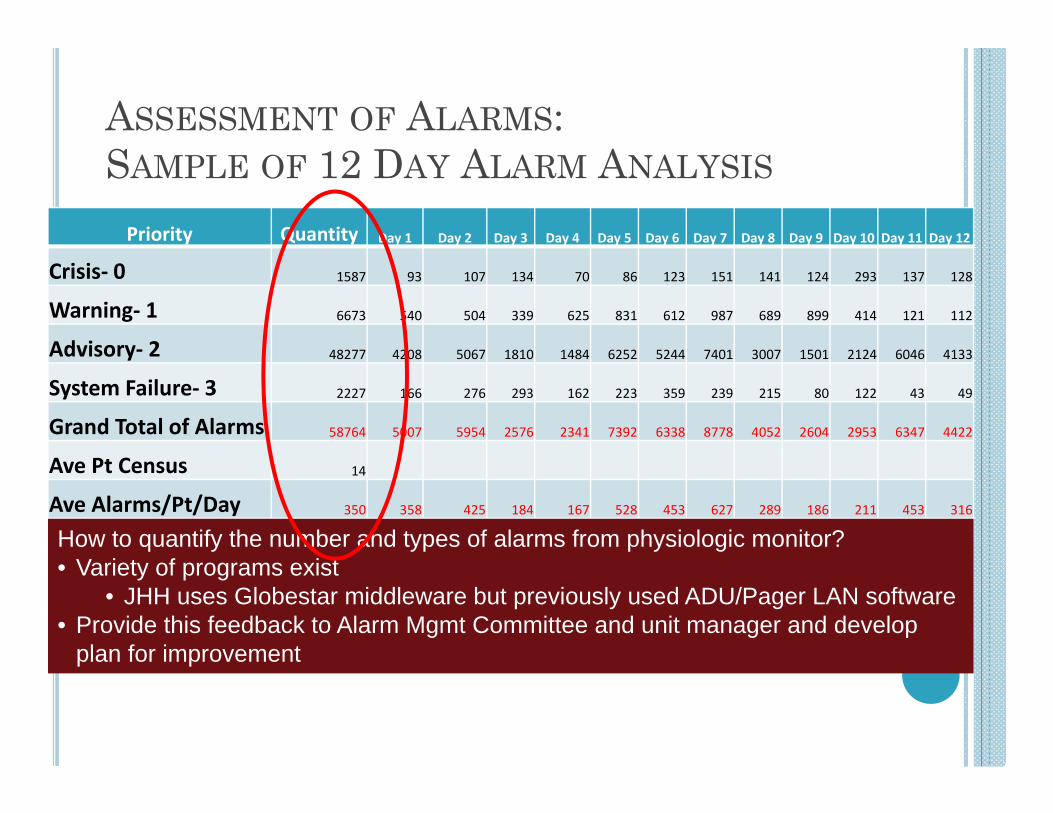
ASSESSMENT OF ALARMS: SAMPLE OF 12 DAY ALARM ANALYSIS
Priority Quantity Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7 Day 8 Day 9 Day 10 Day 11 Day 12
Crisis‐ 0 1587 93 107 134 70 86 123 151 141 124 293 137 128
Warning‐ 1 6673 540 504 339 625 831 612 987 689 899 414 121 112
Advisory‐ 2 48277 4208 5067 1810 1484 6252 5244 7401 3007 1501 2124 6046 4133
System Failure‐ 3 2227 166 276 293 162 223 359 239 215 80 122 43 49
Grand Total of Alarms 58764 5007 5954 2576 2341 7392 6338 8778 4052 2604 2953 6347 4422
Ave Pt Census 14
Ave Alarms/Pt/Day 350 358 425 184 167 528 453 627 289 186 211 453 316
How to quantify the number and types of alarms from physiologic monitor?• Variety of programs exist
• JHH uses Globestar middleware but previously used ADU/Pager LAN software• Provide this feedback to Alarm Mgmt Committee and unit manager and develop
plan for improvement
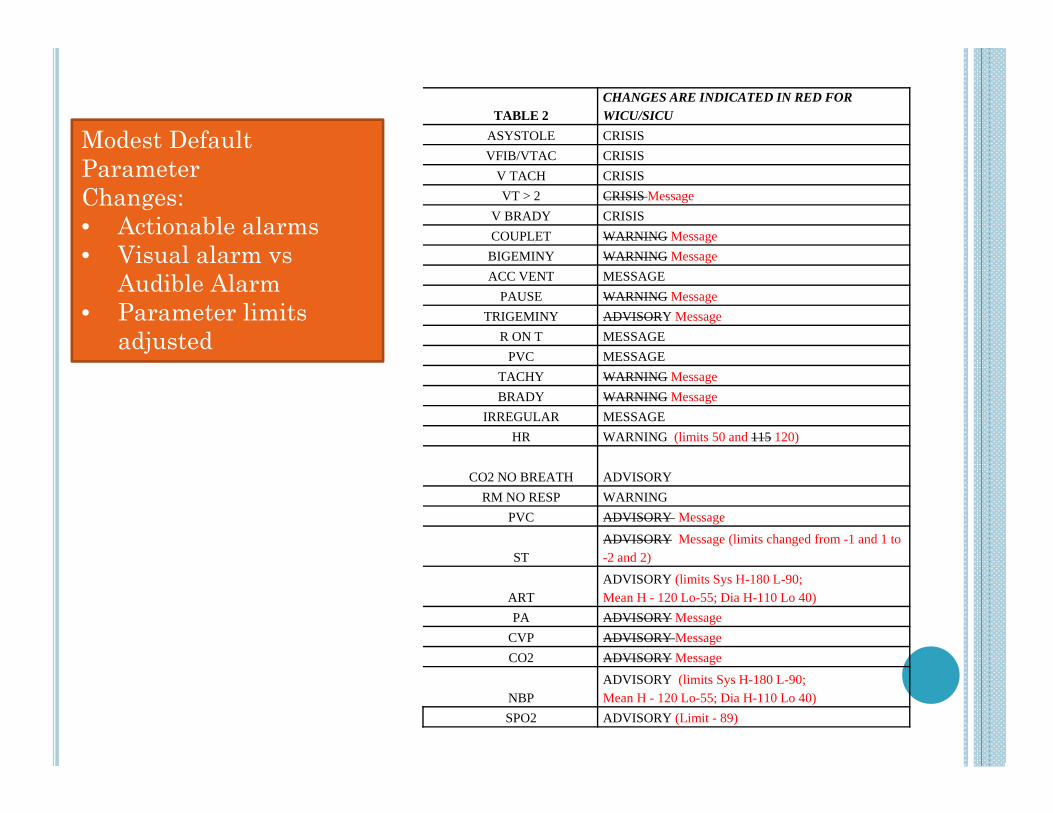
TABLE 2CHANGES ARE INDICATED IN RED FOR WICU/SICU
ASYSTOLE CRISISVFIB/VTAC CRISIS
V TACH CRISISVT > 2 CRISIS Message
V BRADY CRISIS COUPLET WARNING Message
BIGEMINY WARNING MessageACC VENT MESSAGE
PAUSE WARNING MessageTRIGEMINY ADVISORY Message
R ON T MESSAGEPVC MESSAGE
TACHY WARNING MessageBRADY WARNING Message
IRREGULAR MESSAGEHR WARNING (limits 50 and 115 120)
CO2 NO BREATH ADVISORYRM NO RESP WARNING
PVC ADVISORY Message
STADVISORY Message (limits changed from -1 and 1 to -2 and 2)
ARTADVISORY (limits Sys H-180 L-90; Mean H - 120 Lo-55; Dia H-110 Lo 40)
PA ADVISORY MessageCVP ADVISORY MessageCO2 ADVISORY Message
NBPADVISORY (limits Sys H-180 L-90; Mean H - 120 Lo-55; Dia H-110 Lo 40)
SPO2 ADVISORY (Limit - 89)
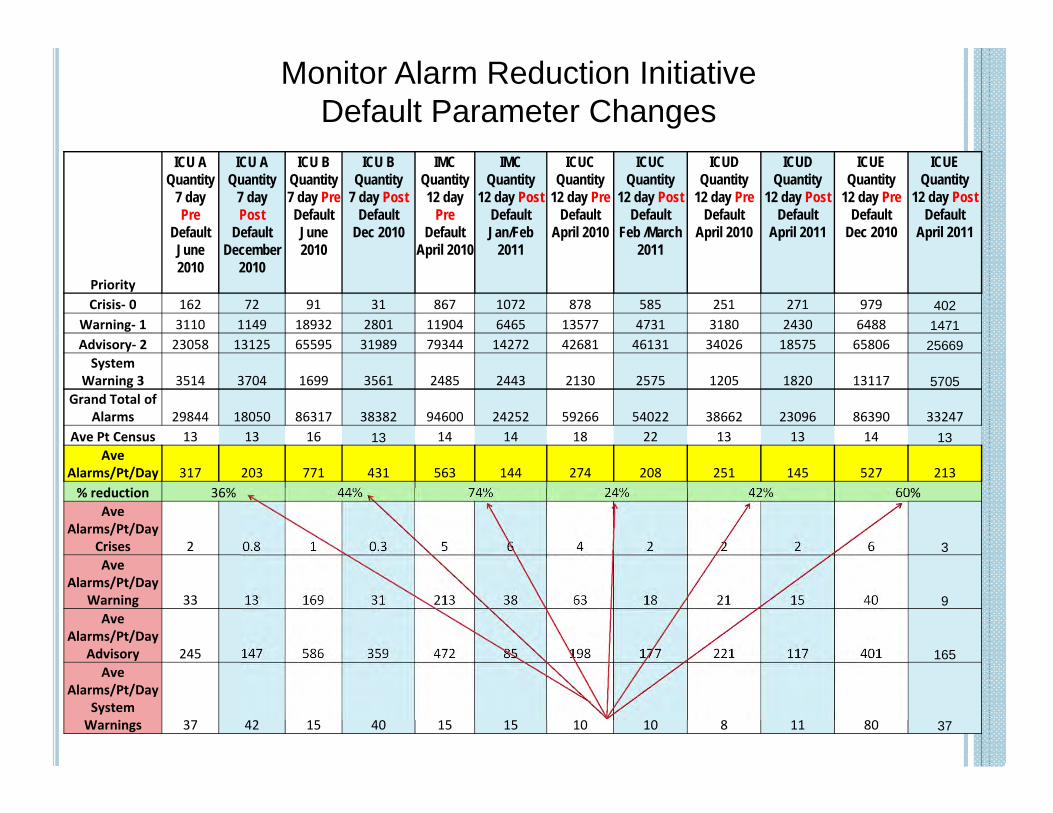
Modest Default Parameter Changes:• Actionable alarms• Visual alarm vs
Audible Alarm• Parameter limits
adjusted
Priority
ICU AQuantity
7 day Pre
DefaultJune 2010
ICU A Quantity
7 dayPost
DefaultDecember
2010
ICU BQuantity7 day PreDefaultJune 2010
ICU BQuantity
7 day PostDefault
Dec 2010
IMCQuantity12 day
PreDefault
April 2010
IMCQuantity
12 day PostDefaultJan/Feb
2011
ICUC Quantity
12 day PreDefault
April 2010
ICUCQuantity
12 day PostDefault
Feb /March 2011
ICUDQuantity
12 day PreDefault
April 2010
ICUDQuantity
12 day PostDefault
April 2011
ICUEQuantity
12 day PreDefault
Dec 2010
ICUEQuantity
12 day PostDefault
April 2011
Crisis‐ 0 162 72 91 31 867 1072 878 585 251 271 979 402Warning‐ 1 3110 1149 18932 2801 11904 6465 13577 4731 3180 2430 6488 1471Advisory‐ 2 23058 13125 65595 31989 79344 14272 42681 46131 34026 18575 65806 25669System
Warning 3 3514 3704 1699 3561 2485 2443 2130 2575 1205 1820 13117 5705Grand Total of
Alarms 29844 18050 86317 38382 94600 24252 59266 54022 38662 23096 86390 33247Ave Pt Census 13 13 16 13 14 14 18 22 13 13 14 13
Ave Alarms/Pt/Day 317 203 771 431 563 144 274 208 251 145 527 213% reduction 36% 44% 74% 24% 42% 60%
Ave Alarms/Pt/Day
Crises 2 0.8 1 0.3 5 6 4 2 2 2 6 3Ave
Alarms/Pt/Day Warning 33 13 169 31 213 38 63 18 21 15 40 9Ave
Alarms/Pt/Day Advisory 245 147 586 359 472 85 198 177 221 117 401 165
Ave Alarms/Pt/Day
System Warnings 37 42 15 40 15 15 10 10 8 11 80 37
Monitor Alarm Reduction Initiative Default Parameter Changes
SYSTEM WARNING-3
ICUA PRE
ICUA POST
ICUBPRE
ICUBPOST
IMCAPRE
IMCA POST
ICUC PRE
ICUCPOST
ICUDPRE
ICUDPOST
ICUEPRE
ICUEPOST
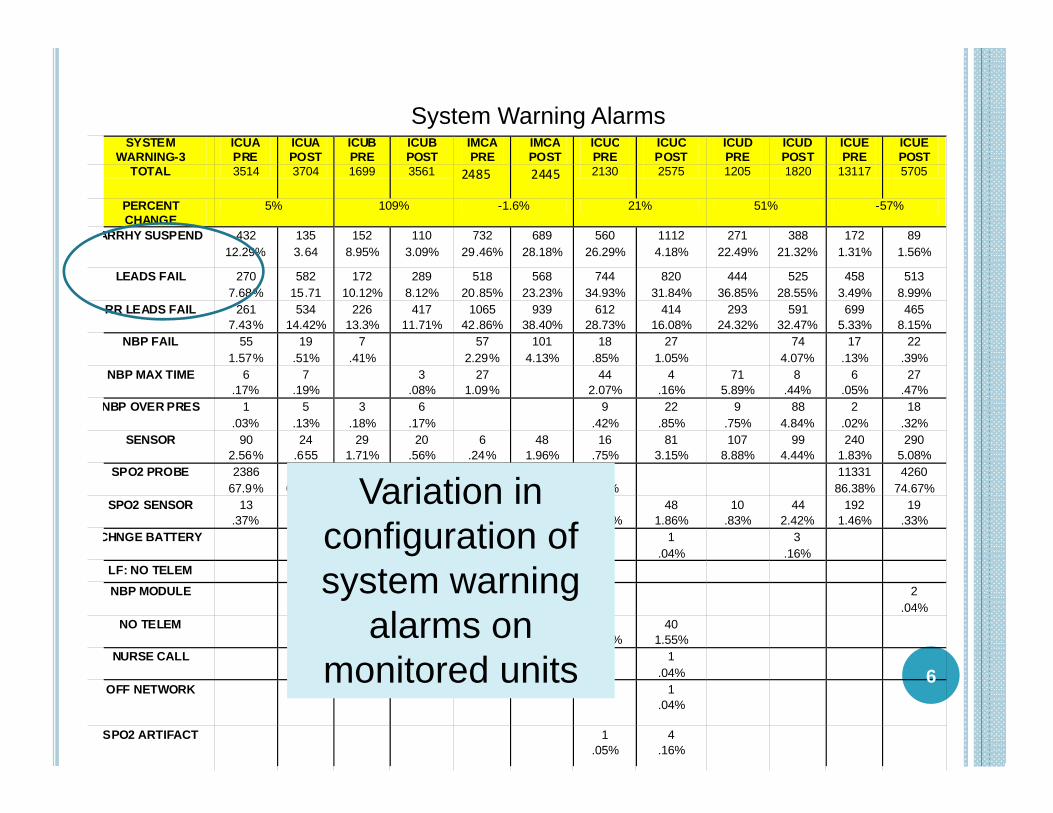
TOTAL 3514 3704 1699 3561 2485 2445 2130 2575 1205 1820 13117 5705
PERCENT CHANGE
5% 109% -1.6% 21% 51% -57%
ARRHY SUSPEND 432 12.29%
135 3.64
152 8.95%
110 3.09%
732 29.46%
689 28.18%
560 26.29%
1112 4.18%
271 22.49%
388 21.32%
172 1.31%
89 1.56%
LEADS FAIL 270 7.68%
582 15.71
172 10.12%
289 8.12%
518 20.85%
568 23.23%
744 34.93%
820 31.84%
444 36.85%
525 28.55%
458 3.49%
513 8.99%
RR LEADS FAIL 261 7.43%
534 14.42%
226 13.3%
417 11.71%
1065 42.86%
939 38.40%
612 28.73%
414 16.08%
293 24.32%
591 32.47%
699 5.33%
465 8.15%
NBP FAIL 55 1.57%
19 .51%
7 .41%
57 2.29%
101 4.13%
18 .85%
27 1.05%
74 4.07%
17 .13%
22 .39%
NBP MAX TIME 6 .17%
7 .19%
3 .08%
27 1.09%
44 2.07%
4 .16%
71 5.89%
8 .44%
6 .05%
27 .47%
NBP OVER PRES 1 .03%
5 .13%
3 .18%
6 .17%
9 .42%
22 .85%
9 .75%
88 4.84%
2 .02%
18 .32%
SENSOR 90 2.56%
24 .655
29 1.71%
20 .56%
6 .24%
48 1.96%
16 .75%
81 3.15%
107 8.88%
99 4.44%
240 1.83%
290 5.08%
SPO2 PROBE 2386 67.9%
2392 64.58%
1109 65.27%
2668 74.92%
1 .05%
11331 86.38%
4260 74.67%
SPO2 SENSOR 13 .37%
6 .16%
1 .06%
16 .45%
17 .68%
26 1.06%
45 2.11%
48 1.86%
10 .83%
44 2.42%
192 1.46%
19 .33%
CHNGE BATTERY 1 .04%
3 .16%
LF: NO TELEM
NBP MODULE 2 .04%
NO TELEM 63 2.58%
80 3.76%
40 1.55%
NURSE CALL 1 .04%
OFF NETWORK 1 .04%
SPO2 ARTIFACT 1 .05%
4 .16%
6
System Warning Alarms
Variation in configuration of system warning
alarms on monitored units
7
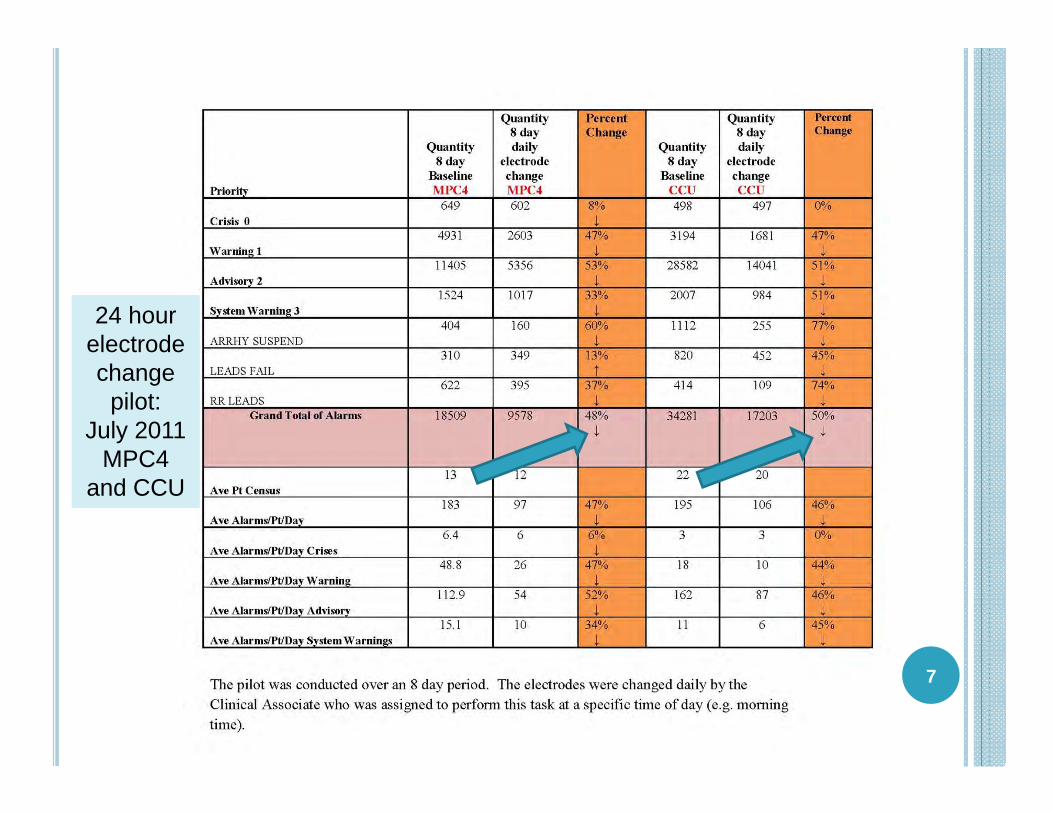
24 hour electrode change
pilot:July 2011
MPC4 and CCU
ALARM NOTIFICATION
HOW DO YOU GET TRUE ANDRELIABLE ALARM INFORMATION
TO THE CARE GIVER?
Weekly Alarm Management Committee8
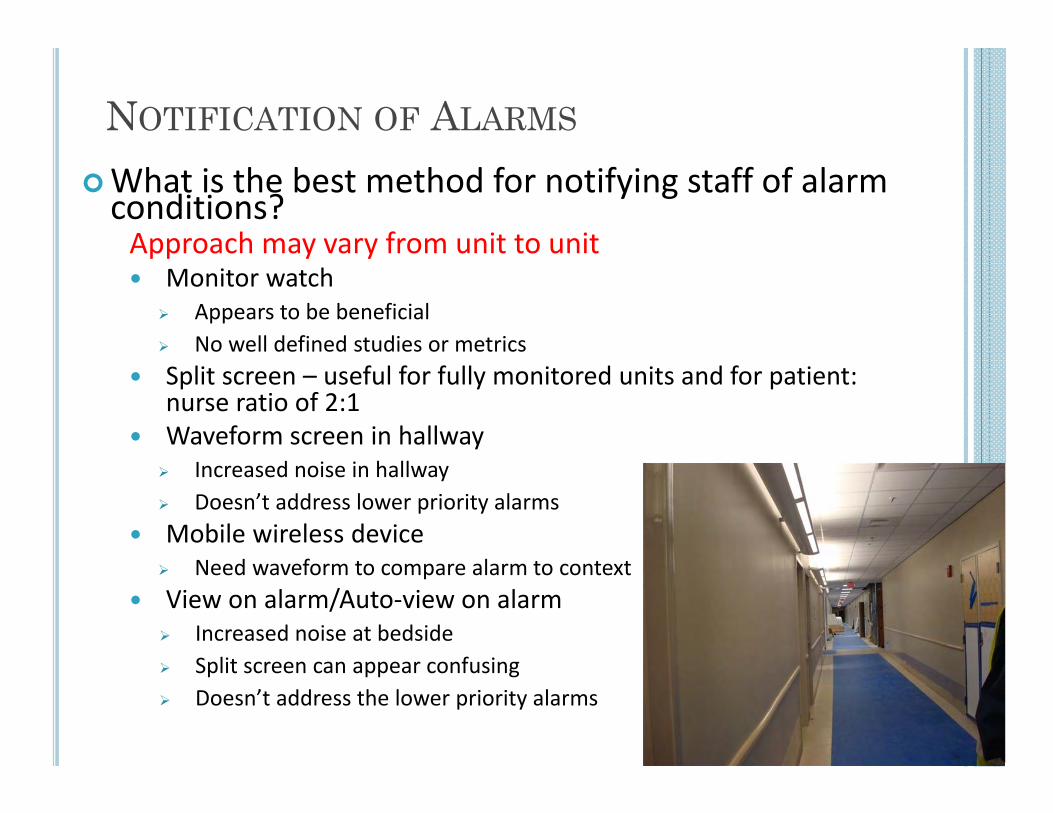
NOTIFICATION OF ALARMS
What is the best method for notifying staff of alarm conditions?Approach may vary from unit to unit Monitor watch
Appears to be beneficial No well defined studies or metrics
Split screen – useful for fully monitored units and for patient: nurse ratio of 2:1
Waveform screen in hallway Increased noise in hallway Doesn’t address lower priority alarms
Mobile wireless device Need waveform to compare alarm to context
View on alarm/Auto‐view on alarm Increased noise at bedside Split screen can appear confusing Doesn’t address the lower priority alarms
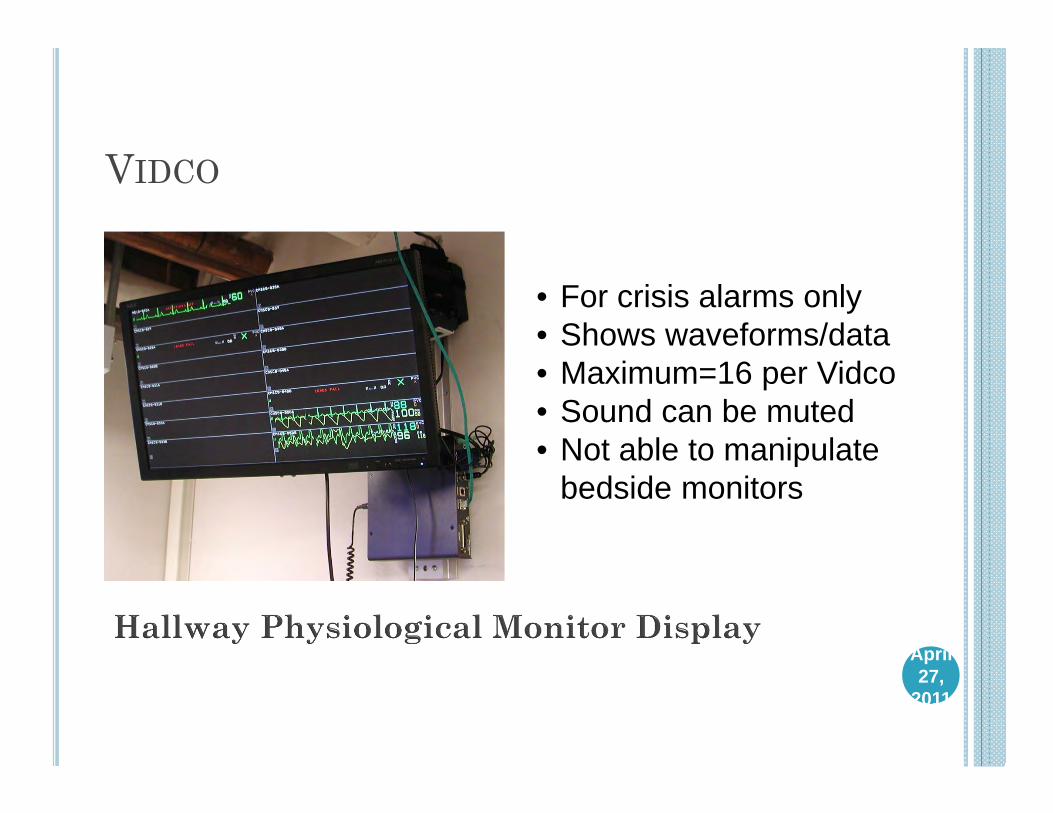
VIDCO
• For crisis alarms only • Shows waveforms/data• Maximum=16 per Vidco• Sound can be muted• Not able to manipulate
bedside monitors
April 27,
2011
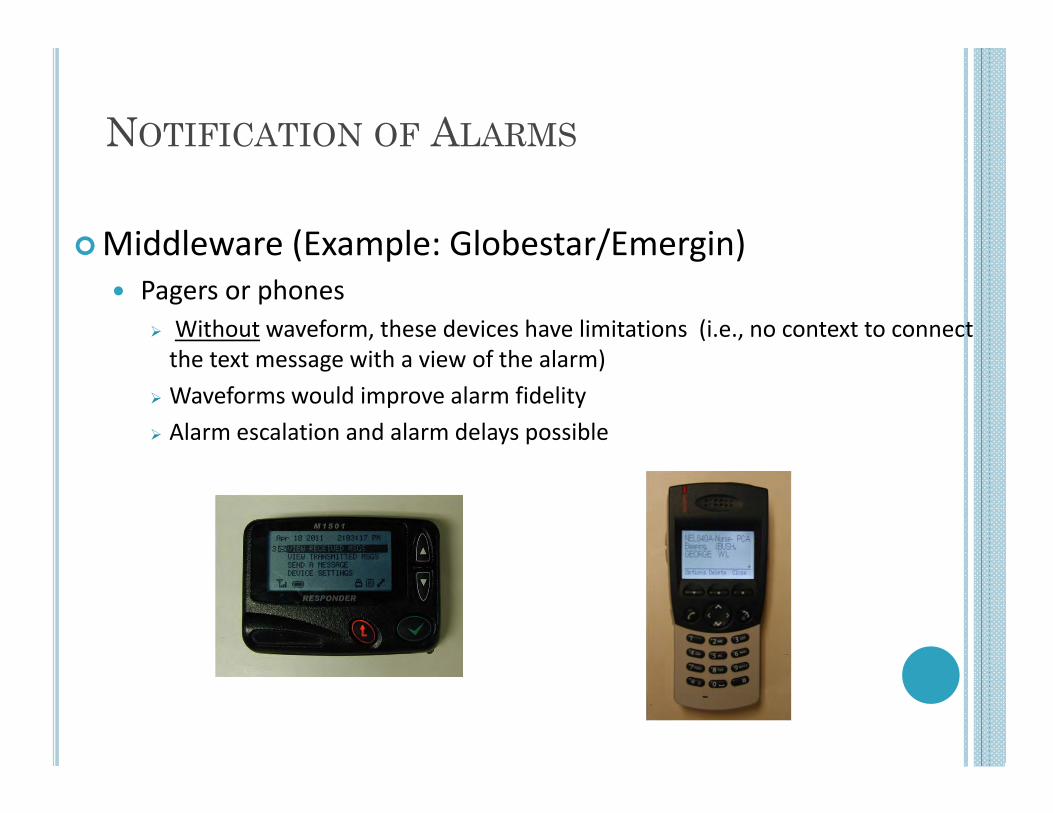
NOTIFICATION OF ALARMS
Middleware (Example: Globestar/Emergin) Pagers or phones
Without waveform, these devices have limitations (i.e., no context to connect the text message with a view of the alarm)
Waveforms would improve alarm fidelity Alarm escalation and alarm delays possible
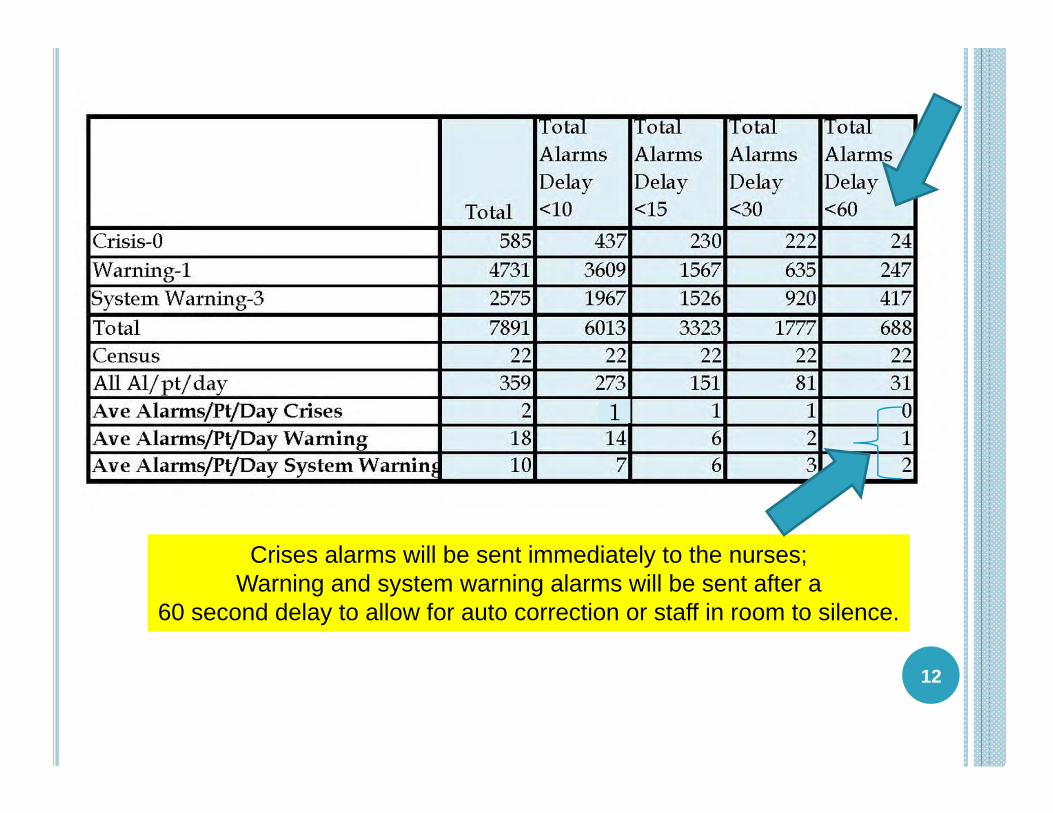
12
Crises alarms will be sent immediately to the nurses;Warning and system warning alarms will be sent after a
60 second delay to allow for auto correction or staff in room to silence.
1
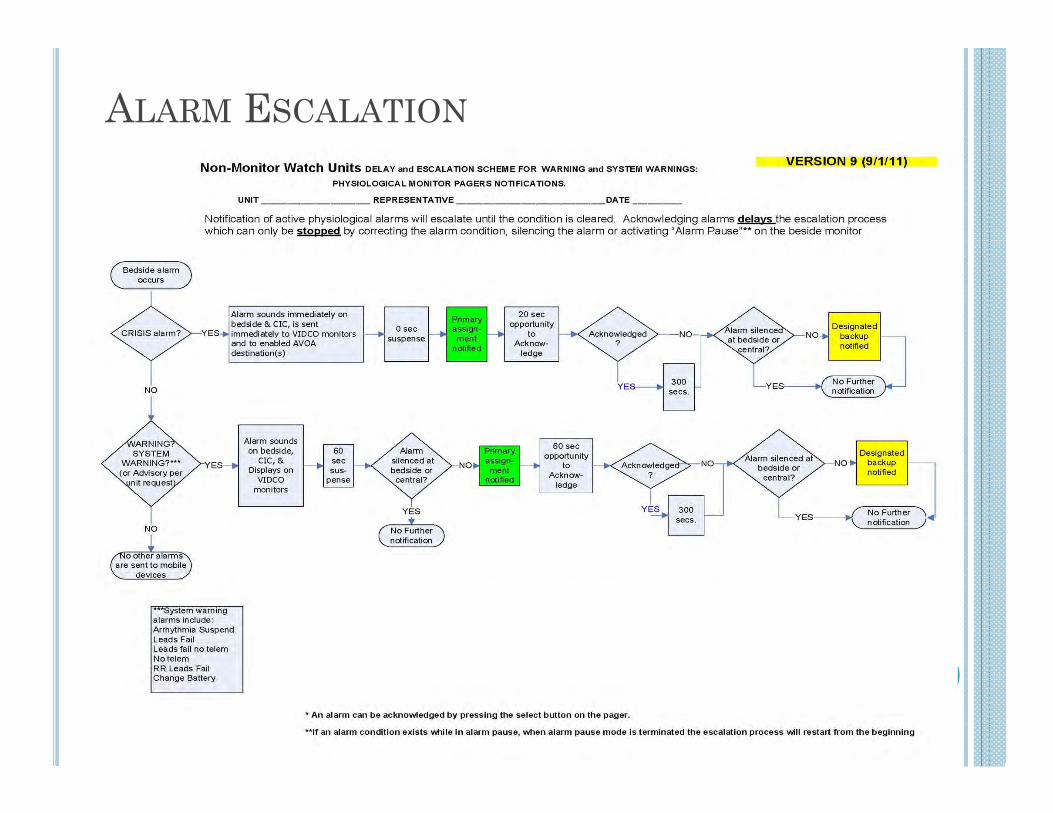
ALARM ESCALATION
SUMMARY
Means to control alarm numbers: Analyze each units monitor
alarms to determine baseline
Set monitor defaults to actionable levels
Individualize alarms based on patient’s baseline
Consider instituting delays to allow for auto correction
Change electrodes daily Foster culture of alarm
safety
Means to assure notification: Monitor watch
Hallway waveform displays Continuous split screen VOA/AVOA Wireless notification
devices Single portal for assignments Institute escalation to other staff
Zoning for large units
14
Redundancy is importantUnits need multiple ways to assure
alarm audibility
Need: Waveform sent to notification device with alarm text message
Multi‐parameter alarm algorithms to reduce frequent false positive alarms
Alarm logic algorithm that increases the urgency of the alarm based on the number of times the alarm has occurred
Ability to access message alarms in patient alarm history Timely physiologic monitor upgrades to match technology improvements in free standing devices
Better understanding of all the default settings and the impact of each 15
Perspective of Bedside User: What is still needed for better alarm management?