"managing difficult issues regarding patient prescription drug abuse: an educational program...
TRANSCRIPT

"Managing Difficult Issues Regarding Patient Prescription Drug Abuse: An Educational Program for Emergency
Physicians"
Maine ACEP Chapter Grant
Project Coordinator Michael Gibbs and Tamas Peredy, MD

Program Description
• Maine ACEP proposes to hold five three-hour educational programs for Maine’s emergency physicians on the issue of patient diversion of drugs for street use over the course of the 18-month grant period in 2009/2010 at various rural locations across the state.
• Objectives– 1. Increase clinician awareness of the issues surrounding opioid
misuse including risk of oligoanalgesia, factors that may identify high risk patients and rights and responsibilities of law enforcement reporting.
– 2. Increase enrollment in the Maine’s Electronic Web-based Prescription Monitoring Program.
– 3. Share evidence-based Pain Management Policies and Protocols.

Conference Speakers
• Maine ACEP– Michael Gibbs, MD, FACEP Tamas Peredy, MD, FACEP
• Maine Medical Association– Gordon Smith, ESQ, Andrew MacLean, ESQ
• Maine OSA/Prescription Monitoring Program– Daniel Eccher, MPH, Stacey Chandler, Anne Rogers, M Ed,
• Maine DEA– Officers Chris Gardner, James Pease, Lowell Woodman,
Kevin Cashman, Gerry Baril
Special Thanks to
• Anna Bragdon– Chapter Executive, MACEP
• Maine Medical Center – Hannaford Center for Safety, Innovation and
Simulation• Marcella Sorg, PhD
– Margaret Chase Smith Policy Center – University of Maine
• Scott Kemmerer, MD– Immediate Past President MACEP

Conference Sites
• Pilot Programs: – Portland 10/16/2008– Bangor 3/12/2009
• Augusta/Waterville 3/31/2011
• Orono 4/12/2011
• Lewiston/Auburn 4/21/2011
• Topsham 4/27/2011
• Biddeford 4/28/2011
Hannaford Center for Safety, Innovation and Simulation
• Department of Medical Education• 4 Case scenarios
– 1) Ankle Fx in chronic pain pt, 2) Forged script with back pain pt, 3) Migraine HA in drug seeker and 4) Dental pain with and without brief assessment
• Appeared in Scenarios– Tamas Peredy, MD Michael Gibbs, MD– Shelly Chipman, Todd Dadaleares and Susie Lane

Challenge
• Increased dispensation of opioids coupled with changing societal attitudes towards prescription opioids has contributed to our current pandemic of non-medical pain reliever misuse.

Response
• To develop a balanced approach to the proper distribution of pain medication to those in need while developing safeguards that reduce the amount of diversion.

General Articles
• McLellan AT, Turner B, Prescription Opioids, Overdose Deaths and Physician Responsibility, JAMA, 300(22): 2672-2673.
• MacCarberg BH, Balancing Patient Needs and Provider Responsibilities in the use of Opioids, P&T Digest, 32-38, 2006.
• Woodcock J, A Difficult Balance – Pain Management, Drug Safety and the FDA, NEJM, 361(22): 2105-2107.

Societies
• American College of Emergency Physicians• American Society of Interventional Pain Physicians• International Association for the Study of Pain• American Pain Society• American Academy of Pain Medicine

Oligoanalgesia in the Emergency Department
Developed by Michael Gibbs, MD
Excerpts from Presentation #1

Human Beings Are Good
A Lot Of Them ComeTo The ED With Pain
It Is Our Job ToAlleviate Pain & Suffering
We Don’t Do A VeryGood Job!

Barriers to Adequate Analgesia
• Lack of Medical Provider Education• Non-existence of Pain Treatment Quality Management
Programs• Lack of ED Pain Treatment Efficacy Studies (including
pediatric, geriatric…)• Clinician’s attitudes about addiction, drug-seeking• Opiophobia – safety concerns relative to other modalities• Unappreciated cultural and gender differences in pain
reporting• Racial and ethnic stereotyping
Rupp T, Inadequate Analgesia in Emergency Medicine, Ann Emerg Med 43(4): 494-503, 2004Millard WB, Grounding Frequent Flyers, Not Abandoning Them: Drug Seekers in the ED, Ann Emerg Med 49(4): 2007.


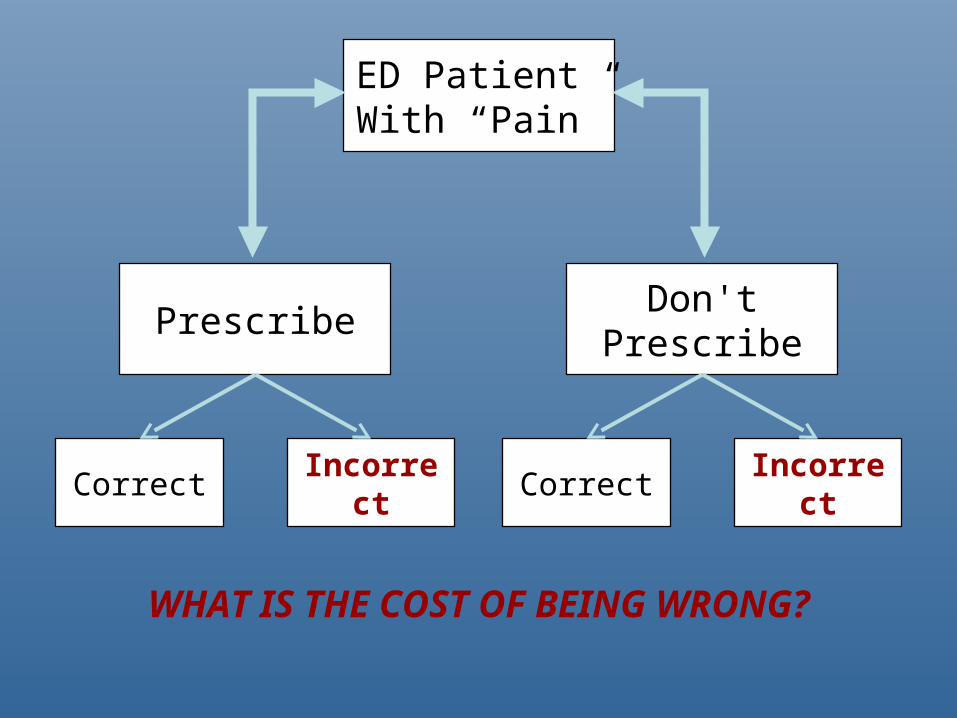
ED Patient With “Pain”
Don'tPrescribe
Prescribe
Correct Incorrect IncorrectCorrect
WHAT IS THE COST OF BEING WRONG?
Oligoanalgesia Articles• Todd KH, Samaroo N, Hoffman JR, Ethnicity as a Risk Factor for Inadequate Emergency
Department, JAMA, 269: 1537-1539, 1993.• Todd KH, Deaton Cm D’Adamo AP et al, Ethnicity and Analgesic Practice, Ann Emerg
Med, 35(1): 11-16, 2000.• Pletcher MJ, Kertesz SG, Kohn MA et al, Trends in opioid prescribing by race/ethnicity for
patients seeking care in US emergency departments. JAMA. 299:70-78, 2009.• Jones JS, Johnson K, McNinch M, Age as a Risk Factor for Inadequate Analgesia in the
Emergency Department, Am J Emerg Med, 14:157-160, 1996.• Brown JC, Klein EJ, Lewis CW, Emergency Department Analgesia for Fracture Pain, Ann
Emerg Med, 42(2): 197-205, 2003.• Rupp T, Delaney KA, Inadequate Analgesia in Emergency Medicine, Ann Emerg Med
43(4): 494-503, 2004.• Alexander J, Manno M, Underuse of Analgesia in Very Young Pediatric Patients with
Isolated Painful Injuries Ann Emerg Med, 41(5):617-622, 2003. • Goldman RD, Crum D, Bromberg R et al, Analgesia Administration for Acute Abdominal
Pain in the Pediatric Emergency Department, Pedi Emerg Care, 22(1):18-21, 2006.• Pines JM, Hollander JE, Emergency Department Crowding is Associated with Poor Care
for Patients with Severe Pain, Ann Emerg Med 51(1): 1-5, 2008. • Decosterd I, Hugli O, Tamches E et al, Oligoanalgesia in the Emergency Department,
Ann Emerg Med, 50(4): 462-471, 2007.• Duignan M, Dunn V, Barriers to Pain Management in Emergency Departments, Emerg
Nurse, 15(9): 30-34, 2008.• Chan L, Winegard B, Attitudes and Behaviors Associated with Opioid Seeking in the
Emergency Department, J Opioid Manage, 3(5): 244-248, 2007.
Pandemic of Prescription Misuse
Excerpts from Presentation #2
Developed by Tamas Peredy
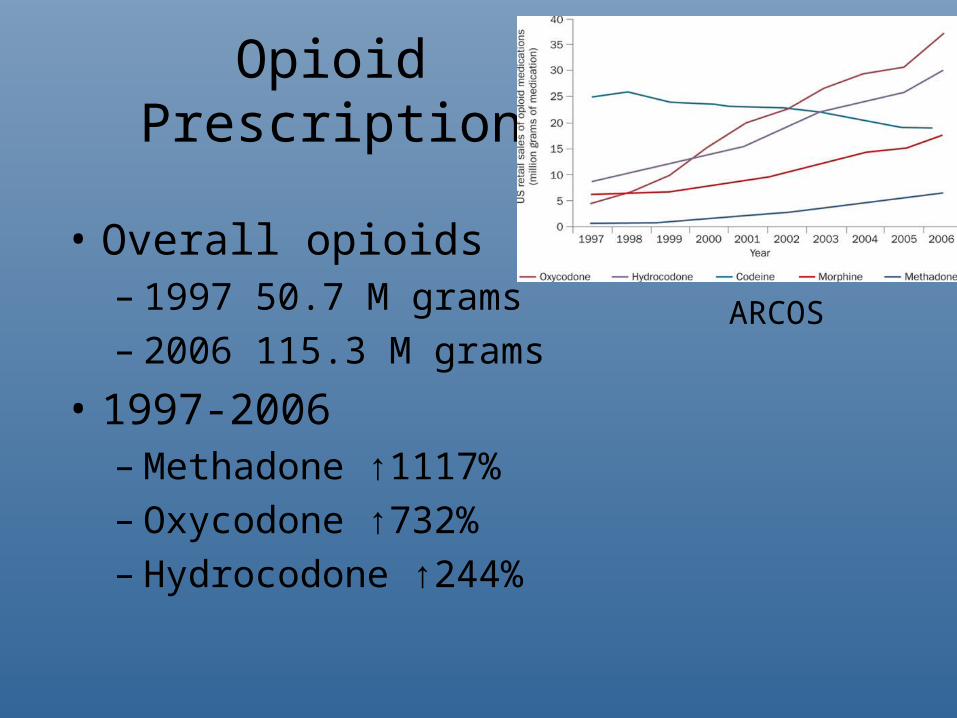
Opioid Prescriptions
• Overall opioids– 1997 50.7 M grams– 2006 115.3 M grams
• 1997-2006– Methadone ↑1117%– Oxycodone ↑732%– Hydrocodone ↑244%
ARCOS
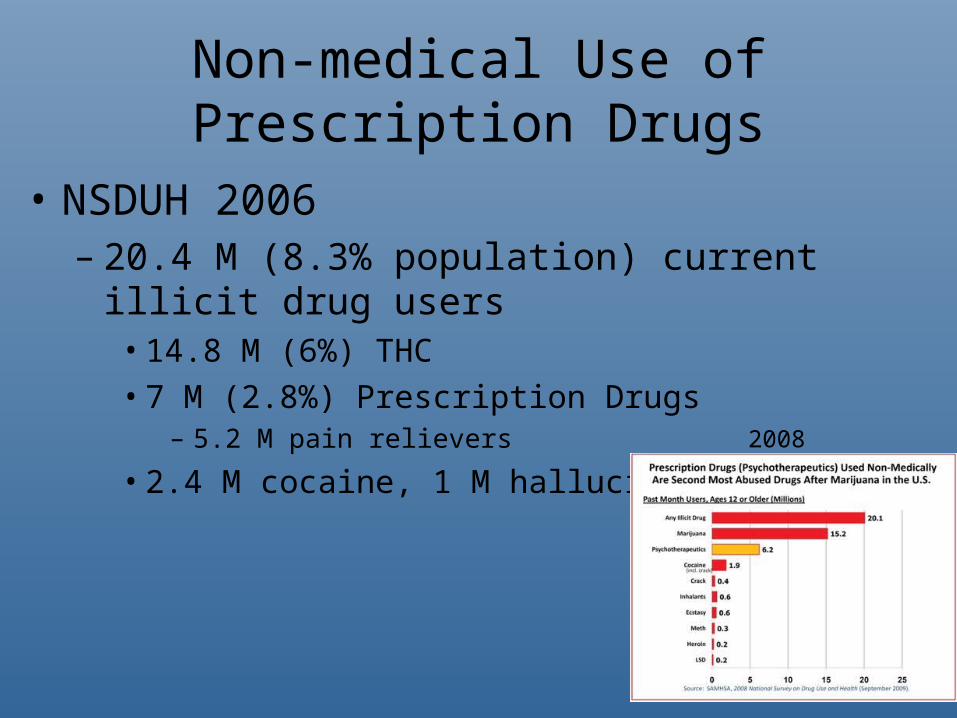
Non-medical Use of Prescription Drugs
• NSDUH 2006– 20.4 M (8.3% population) current illicit drug users
• 14.8 M (6%) THC• 7 M (2.8%) Prescription Drugs
– 5.2 M pain relievers
• 2.4 M cocaine, 1 M hallucinogens 2008

Drug Diversion
• Doctor shopping• Wrote fake prescription• Internet pharmacy $4B• Stolen from doctor’s office/pharmacy• Illicit script from Prescriber
80% from one doctor

1. Reported Methods of Obtaining‘Its nice to share’
all those who met definition of dependent/abuser

Emergency Department Visits
• Drug Abuse Warning Network (DAWN) 2005
• 1.3 M visits drug use/misuse– 196,000 visits opioids (↑24% since 2004)– >2/3rds multiple drugs

Total Drug Deaths
0
50
100
150
200
Total Drug Deaths 34 54 66 60 90 166 153 162 176 167 154
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Suicides are included,and are about 15% ofthese totals.
Maine
Maine Medical Examiner’s Office: 429% increase in drug deaths 1997-2006

Source: NVSS, CDC WONDER, Paulozzi, 2008
0
1
2
3
4
5
6
7
8
'70 '72 '74 '76 '78 '80 '82 '84 '86 '88 '90 '92 '94 '96 '98 '00 '02 '04
Year
Cru
de
rate
per
100
,000
U.S. Crude Death Rate: Unintentional Drug Overdose
63%

Unintentional Poisoning Deaths by Specific Drug Type
US1999-2005
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
'99 '00 '01 '02 '03 '04 '05
Year
Nu
mb
er o
f d
eath
s
prescription opioid
cocaine
heroin
Paulozzi, LJ. Budnitz, DS. Xi, YIncreasing deaths from opioid analgesics in the United StatesPharmacoepidemiol Drug Saf. 2006 Sep;15(9):628-31

Epidemiology Articles
• Paulozzi LJ, Ryan GW, Opioid Analgesics ad Rates of Fatal Drug Poisoning in the US, Am J Prev Med, 31(6): 506-511, 2006.
• Bailey JE, Campagna E, Dart RC et al, The Under recognized Toll of Prescription Opioid Abuse on Young Children, Ann Emerg Med, 2008.
• Hall AJ, Logan JE, Toblin RL et al, Patterns of Abuse Among Unintentional Pharmaceutical Overdose Fatalities, JAMA, 300(22): 2613-2620, 2008.
• McCabe SE, Cranford JA, Boyd CJ et al, Motives, Diversion and Routes of Administration Associated with Non-Medical Use of Prescription Opioids, Addict Behav, 32: 562-575, 2007.

Opioid Addiction TherapyHistory
• Harrison Narcotic Act 1914– Webb vs. United States 1919
• Physicians could not prescribe narcotics for addiction
• Methadone– Treatment for Opioid began 1964 (NYC)– Narcotic Addict Treatment Act 1974
• Federal Regulation SAMHSA CSAT– ~15% addicts in a program, 150,000 participants
• Drug Addiction Treatment Act Oct 2000– Schedule II, III, IV medications for the detoxification or maintenance of
opioid dependency• FDA approval buprenorphine (+/- naloxone) Oct 2002
– Schedule III drug for detoxification or maintenance of opioid dependency– Office-based Opioid Treatment (OBOT)
Fudala PJ et al NEJM 2003

Figure 2 Tolerance versus opioid-induced hyperalgesia
Crofford, L. J. (2010) Adverse effects of chronic opioid therapy for chronic musculoskeletal painNat. Rev. Rheumatol. doi:10.1038/nrrheum.2010.24
•Chronic Pain•Tolerance•Hyperalgesia•Dependency (risk of withdrawal)

Methadone Pharmacology• Mu agonist, NMDA agonist• Usual dosing 60-120 mg/ once per day
– High dose protocols (Strain, Shinderman)• Analgesic action 4-8 hrs• Elimination half-life 8-59 hrs• Major metabolite
– EDDP metabolite• QT prolongation (Black Box Warning) Krantz Ann Inter
Med 2002

Methadone Unintended Deaths
• Nationally (FDA warning 2006)– # scripts ↑700% 1998-2006– Deaths 790 in 1999 → 3849 in 2004 (↑468%)
• 82% unintentional (most polydrug e.g. benzos)
– Increase not related to MMTP
• Locally– Vermont 17→79 2001-2006 Shapiro 2007– Maine 23→67 2001-2006 Sorg 2007
Coben JH Am J Prev Med 2006SAMHSA Substance Abuse Treatment Advisory, Spring 2009Martin TC Curr Drug Safety 2011
*ED visits41,000 in 2005↑659% 1999-2005

Buprenorphine Pharmacology• Partial mu agonist
– May induce withdrawal in dependent patients• High mu affinity
• Elimination half-life 4-5 hours
• Analgesic ceiling ~32 mg/day
• Usual dosing 4-16 mg/day BID
Sporer KA Ann Emerg Med 2004

Acute Pain Management in Chronic Pain Patients
• Re-emphasize non-pharmaceutical and non-opioid treatments
• Do not vary long-acting opioid dosing– methadone or fentanyl patch dose
• Buprenorphine frequency or dose may be increased to q6 or up to 32 mg/day
• Titrate a short-acting opioid• Rapid referral or re-check to reduce quantity
dispensed

Chronic Pain Articles• Savage SS, Kirsch KL, Passik SD, Challenges in Using Opioids to Treat Pain in
Persons with Substance Use Disorders, Addict Sci Clin Pract, 4-25, 2008• Martin TC, Rocque M, Accidental and Non-Accidental Ingestion of Methadone and
Buprenorphine in Childhood, Curr Drug Safe, 6(1): 1-5, 2011.• Toombs JD, Kral LA, Methadone Treatment for Pain States, Am Fam Phys, 71(7):
1353-8, 2005.• Wolff K, Characterization of Methadone Overdose, Therapeu Drug Monitor, 24(4):
457-470, 2002.• Fudala PJ, Bridge TP, Herbert S et al, Office-Based Treatment of Opioid Addiction
with SL Buprenorphine and Naloxone, NEJM, 349(10): 949-958, 2003.• Berg ML, Idrees U, Ding R et al, Evaluation of the Use of Buprenorphine for Opioid
Withdrawal in an Emergency Department, Drug Alco Depend, 2006.• Bell JR, Butler B, Lawrence A et al, Comparing Overdose Mortality Associated with
Methadone and Buprenorphine Treatment, Drug Alco Depend, 104: 73-77, 2009.• Sporer KA, Buprenorphine: A Primer for Emergency Physicians, Ann Emerg Med,
43(5): 580-584, 2004.

Maine Prescription Monitoring Program
Developed by Daniel Eccher, MPH
Excerpts from Presentation #3

Top Five Rx Drugs of Abuse
PMP Data, SFY 2009. According to the Maine Drug Enforcement Agency, these drugs are the top 5 of concern for law enforcement.
Drug Name Tablets Dispensed
Hydrocodone/APAP 26.4 million
Oxycodone HCl 17.3 million
Oxycodone/APAP 10.6 million
Alprazolam 9.2 million
Diazepam 4.0 million

How to register as a Requester
1. Go to: http://www.maine.gov/pmp
2. Click on “RxSentry Data Requester Forms” link.
3. Download appropriate Registration Form.
4. Fill it out, sign it in front of a Notary Public, have them notarize it, and mail it to OSA at the address on the form.
Questions: (207) 287-2595

Sub-account User Registration
• Go to www.maine.gov/pmp.
• Click on “RxSentry Data Requester Forms” link.
• Download “Sub-account User Form.”
• Fill it out; prescriber signs middle; sub-account user-to-be signs in front of a Notary Public; then, send original form to OSA at address on form.
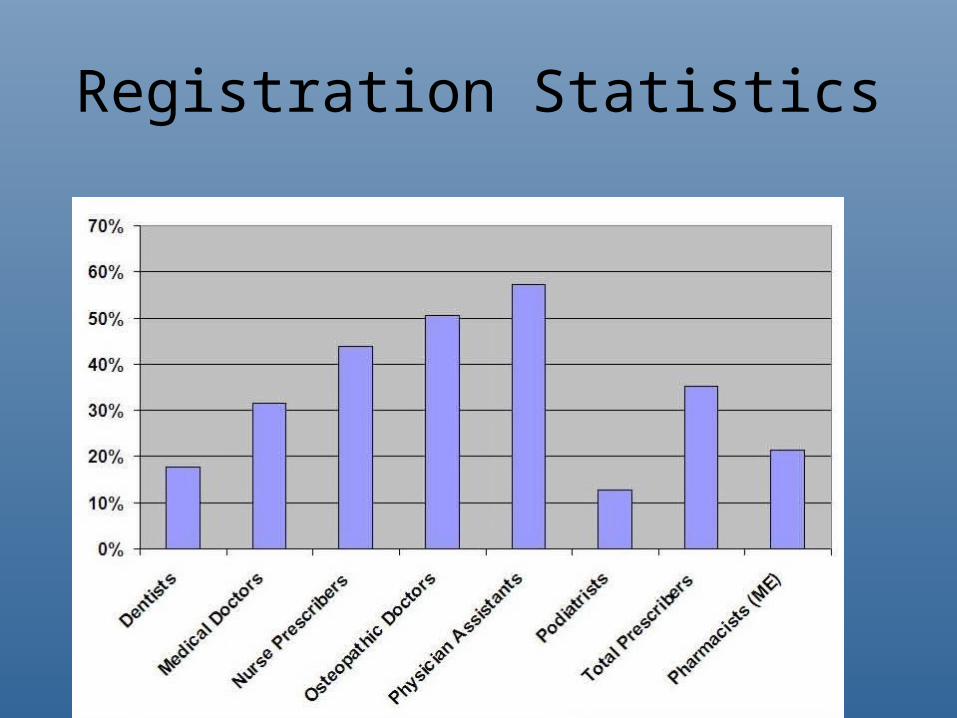
Registration Statistics
PMP Articles
• Fishman SM, Papazian JS, Gonzalez S et al, Regulating Opioid Prescribing Through Prescription Monitoring Programs, Am Acad Pain Med, 5(3): 309-324, 2004.
• Reisman RM, Shenoy PJ, Atherly AJ et al, Prescription Opioid Usage and Abuse Relationships, Subst Abuse Res Treat, 3: 41-51, 2009.
• Baehren DF, Marco CA, Droz DE et al, A Statewide Prescription Monitoring Program Affects Emergency Department Prescribing Behaviors, Ann Emerg Med, 56(1): 19-23, 2010.
• Todd KH, Pain and Prescription Monitoring Program in the Emergency Department, Ann Emerg Med , 56(1): 24-26, 2010.

ED Pain Management Guidelines
Excerpts from Presentation #4
Developed by Tamas Peredy
Chronic Pain Ambulatory Care Guidelines (Universal Precautions)
• Evaluation• Risk Assessment• Controlled Substance Prescribing Contract• Prescription Monitoring Program• Drug Education
– Addiction (4C’s), Dependency, Tolerance
• Adherence monitoring– Pill counts– Urine drug screening

Fundamental Goals
– ‘Fifth vital sign’ (0-10 scale) JCAHO 2001• One-dimensional• Best used to assess therapeutic success
– Identify cause or causes• Objective testing, if needed• Therapy may begin simultaneously
– Treatment• Expedience/Titration• Individual benefit versus risks (balance)• Background: environmental costs
ACEP Board of Directors Statement 2009FSMB Published Statement 2004
Multidisciplinary Treatment Modalities
• Physical– Heat/ice, immobilization, massage, acupuncture
• Psychobehavioral– Relaxation, biofeedback, sleep management,
cognitive restructuring
• Interventional– Blocks, stimulators
• Medications– APAP, NSAIDS, topical therapy, Adjuncts, Opioids

ED Pain Metric
• Inclusion: – Age range: all– Complaint: pain– Acuity: < 1 week
• Exclusion:– Unstable vital signs– Clear indications for emergent transfer to:
• L&D, Cath Lab, Operating Room

ED Flow• Triage Evaluation of Pain (PQRST) and implementation of non-pharmacological
measures within 15 minutes– Positioning, ice, immobilization
• Assess medications, allergies, mental status, respiratory status, circulation and gastrointestinal complaints (nausea, vomiting)
• Pain VAS– 1-3 minor
• Initiate APAP or NSAID– 4-10 major
• Obtain urine specimen• Check PMP• Ask if patient can wait 30 minutes for medications to work?
– Yes, give APAP 1g, NSAID ibuprofen 10 mg/kg plus Oxycodone 0.1 mg/kg» Reassess 30 minutes, notify provider
– No, give fentanyl 1 mg/kg up to 100 mcg IV» Reassess 10 minutes, notify provider
– Provider assessment within 1 hour• Secondary intervention or documentation of exclusion criteria
– Complete pain relief, Disingenuous pain, etc..
• Metric– %secondary assessment within 30-60 min– %achieved pain relief 50% or greater
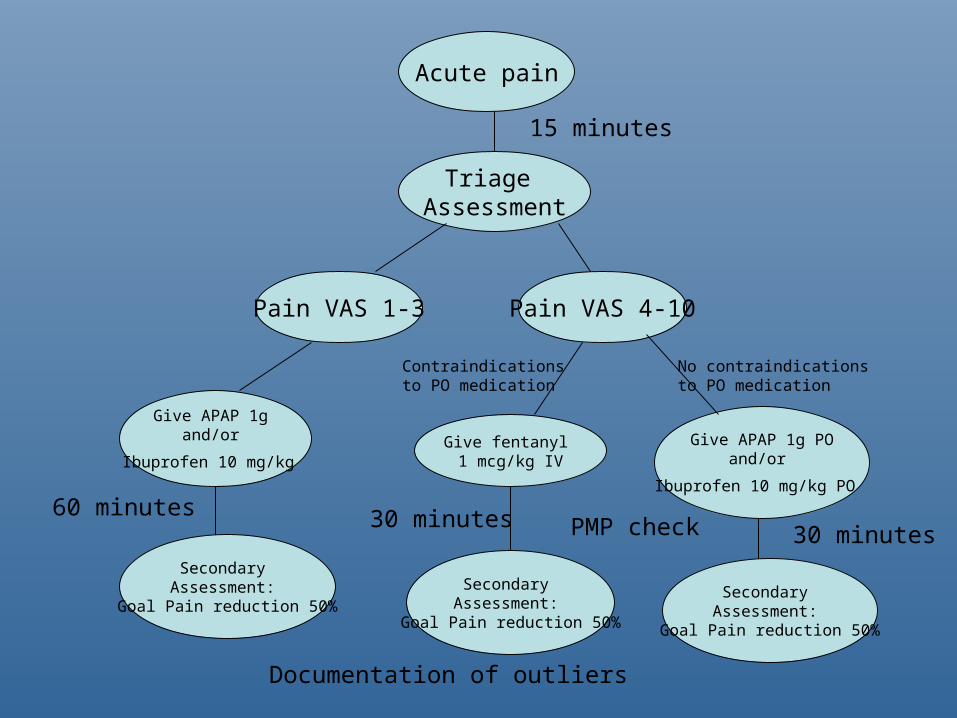
Acute pain
Triage Assessment
Pain VAS 1-3 Pain VAS 4-10
15 minutes
Give APAP 1g and/or
Ibuprofen 10 mg/kg
Secondary Assessment:
Goal Pain reduction 50%
Give fentanyl 1 mcg/kg IV
Give APAP 1g POand/or
Ibuprofen 10 mg/kg PO 60 minutes
No contraindications to PO medication
Contraindications to PO medication
Secondary Assessment:
Goal Pain reduction 50%
Secondary Assessment:
Goal Pain reduction 50%
30 minutes30 minutes PMP check
Documentation of outliers

Risk Assessment Tools (screening tools)
• ABD Addiction Behavior Checklist• CAGE-AID• COMM Current Opioid Misuse Measure• CRAFFT
– Car, relax, alone, forgetfulness, friend tolf you to quit, trouble with law• DIRE
– Diagnosis, intractability, risk, efficacy
• SISAP Screening Instrument for Substance Abuse Potential SOAPP – CAGE plus mood, legal problems, personal, friend and family Hx
substance abuse, psychological problems, treatment and treatment failure
• ORT (opioid risk tool)– Personal and family Hx substance abuse, age, social factors,
psychological diseases
Urine Drug Screen
• Rarely impacts acute medical care
• Opioids (cutoffs, threshold)– Typically detection of codeine, hydrocodone,
hydromorphone, morphine, heroin (diacetyl-morphine)
– Variable cross reactivity with oxycodone
• Special assays required for– Methadone, buprenorphine, oxycodone, fentanyl

Minimum Documentation
• Past visits resulting in opioid scripts (recurrence)• Past failures of non-opioid pain relieving treatments• History of drug use including alcohol and tobacco
– Past treatment for drug problems
• Family situation (including relations with substance abuse)
• Outpatient resources (primary care doctor)
Vukmir RB, Drug Seeking Behavior, Am J Drug Alco Abuse, 30(3): 551-575, 2004.
125th Maine Legislature First Regular Session LD 1501
ED Pain Management Articles
• Wilsey B, Fishman S, Rose JS et al, Pain Management in the ED, Am J Emerg Med, 22(1): 51-57, 2004.
• McIntosh SE, Leffler S, Pain Management After Discharge From the ED, Am J Emerg Med, 22(2): 98-100, 2004.
• Tamches E, Buclin T, Hugli O et al, Acue Pain in Adults Admitted to the Emergency Room: Development and Implementation of Abbreviated Guidelines, Swiss Med Weekly, 137: 223-227, 2007.
• Rasor J, Harris G, Using Opioids for Patients with Moderate to Severe Pain, JAOA, 107(9) S5: ES4-10, 2007.

Legal and Law Enforcement Issues associated with Opioid Dispensing
Developed by Gordon Smith, EVP, MMA207-622-3374, ext. [email protected]
Excerpts from presentation #5

Maine State Law
• §1109. Stealing drugs • 1. A person is guilty of stealing drugs if the person
violates chapter 15, section 353, 355 or 356-A knowing or believing that the subject of the theft is a scheduled drug, and it is in fact a scheduled drug, and the theft is from a person authorized to possess or traffick in that scheduled drug.
• [ 2003, c. 1, §9 (AMD) .] • 2. Stealing drugs is: • A. A Class C crime if the drug is a schedule W, X or Y
drug; or [2001, c. 419, §21 (NEW).]• B. A Class D crime if the drug is a schedule Z drug.
[2001, c. 419, §21 (NEW).]

Searching for Balance
• Practitioners have a legal & ethical duty to effectively diagnose & manage pain
• Practitioners must be aware of federal & state laws governing the prescription of controlled substances for pain management & must keep them in mind when developing treatment plans
• Following medically-based, peer reviewed, & nationally-recognized guidelines, documenting good faith prior exams, & outlining the parameters of treatment plans will put you in the best position to defend enforcement actions
• Following BOLIM Rule Chapter 21 essential
State Law Aimed at Preventing Diversion
• Joint Rule Chapter 21, Use of Controlled Substances for Treatment of Pain
• MDEA Rule Chapter 1, Requirements of Written Prescriptions of Schedule II Drugs (with printer & waiver lists)
• Board of Pharmacy Rule Chapter 19, Receipt and Handling of Prescription Drug Orders
• An Act to Facilitate Communication between Prescribers & Dispensers of Prescription Medication (P.L. 2003, Chapter 483; effective 9/13/03) – Prescription Monitoring Program

Health Information Privacy Laws & Diversion
• 22 M.R.S.A. sec. 1711-C, Confidentiality of health care information (Maine’s privacy statute, effective 2/1/00)
• 45 C.F.R. Parts 160 & 164, Standards for Privacy of Individually Identifiable Health Information (the HIPAA privacy rule, effective 4/14/03)
• FAQ: What disclosure to law enforcement officials is permitted under these privacy laws?– Is there any recognized privacy interest in criminal activity?– Can practitioner disclose facts about patient conduct that
suggest diversion without disclosing PHI?• L.D. 1425, An Act to Facilitate the Reporting of the Crime
of Acquiring Drugs by Deception (P.L. 2007, Chapter 382; effective 9/20/07)

Amendment to Crime of Acquiring Drugs by Deception
• L.D. 1425 amends 17-A M.R.S.A. sec. 1108, Acquiring drugs by deception, as follows:– 6. A prescribing health care provider, or a person acting under
the direction or supervision of a prescribing health care provider, who knows or has reasonable cause to believe that a person is committing or has committed deception may report that fact to a law enforcement officer. A person participating in good faith in reporting under this subsection, or in participating in a related proceeding, is immune from criminal or civil liability for the act of reporting or participating in the proceeding.
Medical Marijuana
• Maine Medical Marijuana Act: passed by referendum in 1999; repealed & replaced by referendum in 2009; amended by legislature in 2010
• Expanded list of “debilitating medical conditions”• Role of physician: may, but is not required to, provide
“written certification” of eligibility• Issues of informed consent
– Uncertain status under federal law: AG Holder statement– Drug regulatory concerns: not FDA-approved; don’t “prescribe” or
“dispense”– Potential exposure to claims of negligence: unregulated drug; may
not know strength or impurities
• Is this at odds with our concern about Maine’s drug problem?
Legal Articles
• Lawrence LL, Legal Issues in Pain Management: Striking a Balance, Emerg Med Clin N Am, 23: 573-584, 2005.
• Goldenbaum DM, Christopher M, Gallagher RM et al, Physicians Charged with Opioid Analgesic-Prescribing Offenses, Pain Med, 9(6): 737-747, 2008
• Fishbain DA, Lewis JE, Gao J et al, Alleged Breaches of “Standards of Medical Care” in a Patient Overdose Death, Am Acad Pain Med, 10(3): 565-572, 2009.
• Model Policy for the Use of Controlled Substances for the Treatment of Pain, Federation of State Medical Boards.