management of septic shock in childrenrfppl.co.in/subscription/upload_pdf/art 3_2ab.pdf ·...
TRANSCRIPT
189
Volume 2 Number 4 Oct - Dec 2010
INTRODUCTION
Sepsis can occur as a result of localizedinfection or generalized infection. It can becaused by bacteria, virus, fungus andparasites. Children are more prone to thedevelopment of sepsis especially
* Infants* Children with serious injuries* On chronic antibacterial therapy* Malnourished children* With chronic medical problems* Immuno suppressed children* 3 months – 3 yr of age with occult
bacteremia
Organism varies with age of patient andimmune status.
Neonates— E.coli, GBS, Listeria, Herpesvirus
Older children—Strep pneumoniae,Neisseria meningitidis, Staph aureus,Toxicshock syndrome.
Immunocompromised Children—Nosocomial, Gram –ve, fungi, polymicrobial.
PATHOGENESIS
Shock is a state of circulatory disturbancewhich can affect multiple organ systems in thebody. Septic shock in children is a prototypecombination of hypovolemia, cardiogenic anddistributive shock. The two forms of septicshock are Warm shock characterised byincreased cardiac out put and decreasedsystemic vascular resistance and Cold shockcharacterised by decreased cardiac output andincreased systemic vascular resistance.
Management of septic shock in children
ABSTRACT
Septic shock is one of the common pediatric emergencies often encountered. Despite theadvances in the preventive and therapeutic medicines, septic shock continues to be a majorlife threatening problem. This review article tries to highlight some of the managementissues for the septic shock in children.
Key words: Sepsis, septic shock, diagnostic criteria, management
Rojo Joy*Abby Rojo**
© Red Flower Publication Pvt. Ltd.
Author’s affiliation: *Senior Resident,Dept. of Pediatrcs,JIPMER. Dr. Abby Rojo, KGHS, Kerala.
Reprint’s request: Dr. Rojo Joy, Rojo Villa”, SubstationRoad, Chevayur P.O. Calicut-17.
Email [email protected].
(Received on 17.10.2010, accepted on 24.12.2010)
Indian Journal of Emergency PediatricsVolume 2 Number 4, Oct - Dec 2010
190
Indian Journal of Emergency Pediatrics
Following the release of endotoxins andsuperantigens, inflammatory cascade getsactivated. This leads to the release ofarachidonic acid mediators, cytokines,interleukins, complement system, myocardialdepressant factors which lead to the cascadeof events that causes endothelial damage andmicrocirculatory dysfunction .Tumor necrosisfactor causes increased vascular permeability,decreased vascular tone, fever. Arachidonicacid metabolites cause fever, ventilationperfusion disturbances, lactic acidosis.Myocardial depression is caused by TNF,increased beta endorphins, production ofmyocardial nitric oxide (1,2,3).
The predominant cause of mortality in adultseptic shock is vasomotor paralysis. But inchildren low cardiac output and not lowsystemic vascular resistance, is associated withmortality. Also contrary to adults, oxygendelivery, not oxygen extraction, is the majordeterminant of oxygen consumption inchildren. Neonatal septic shock can becomplicated by the physiologic transition fromfetal to neonatal circulation. Acidosis and
hypoxia associated with the sepsis can increasethe pulmonary pressure resulting in persistentpulmonary hypertension (PPHN) and canlead to right heart failure (4,7).
CLINICAL FEATURES Child presents initially with
tachypnea, tachycardia, alteration oftemperature. In the initial hyperdynamicphase, one can note the warm peripheries,bounding pulses. As the condition progressesmyocardial failure and vascular leaks sets in,and can develop cool extremities, decreasedurine output, altered mentation, delayedcapillary filling time, low pulse volume. Dueto anaerobic metabolism in tissue lacticacidosis sets in and can have acidotic breathingand myocardial failure. Skin may showfeatures of erythema, jaundice, echymoses,petechiae . In advanced conditions it canprogress to disseminated intravascularcoagulation and multiorgan dysfunctionsyndrome. Hypotension is a late feature andtherefore not useful to detect early shock (4-9).
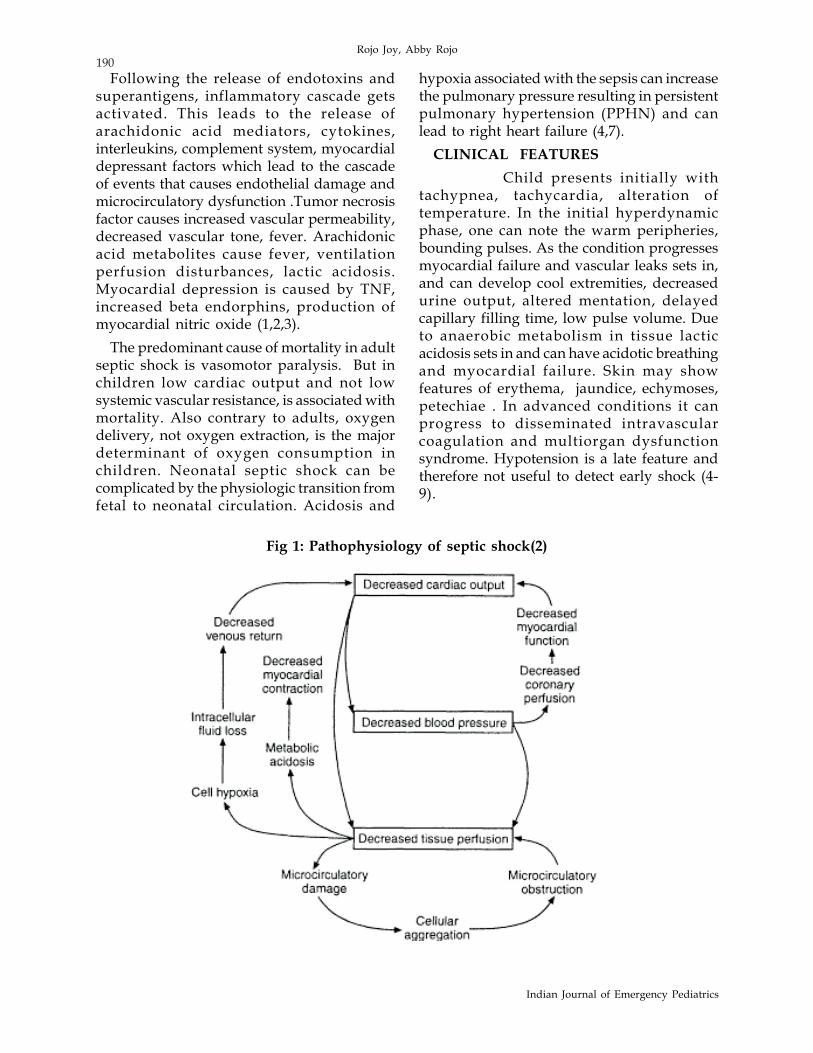
Fig 1: Pathophysiology of septic shock(2)
Rojo Joy, Abby Rojo
191
Volume 2 Number 4 Oct - Dec 2010
DIAGNOSIS
Based on the INTERNATIONALCONSENSUS DEFINITION FORPEDIATRIC SEPSIS(8,10).
InfectionSuspected or proven infection or a clinical
syndrome associated with high probability ofinfection.
Systemic Inflammatory Responsesyndrome(SIRS)
Two out of four criteria out of which 1 mustbe abnormal temperature or abnormalleucocyte count
* Core temperature >38.5o C or <36o C* Tachycardia heart rate > 2 S.D above
mean in the absence of external stimuli,chronic drugs or painful stimuli or
Unexplained persistent elevation over (0.5-4 hr) or
In children <1 yr bradycardia (heart rate <10th percentile) over 0.5 hr in absence of drugs, vagal stimuli
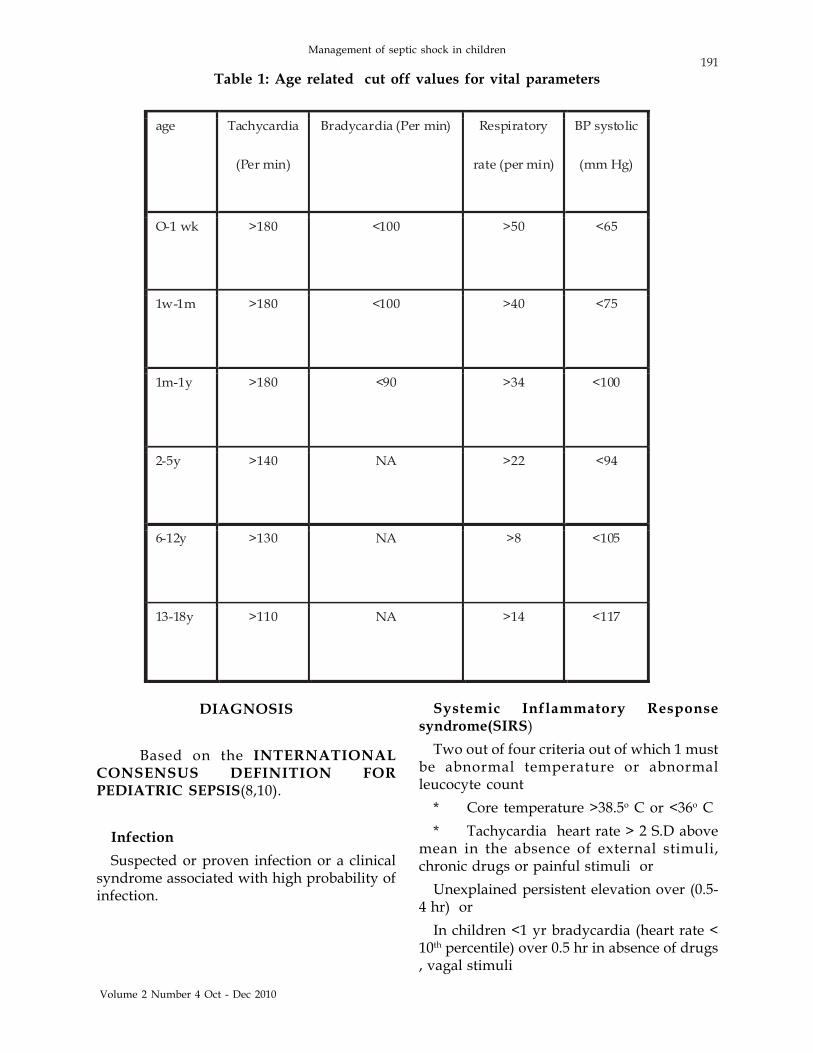
Table 1: Age related cut off values for vital parameters
Management of septic shock in children
192
Indian Journal of Emergency Pediatrics
* Mean respiratory rate > 2 S.D abovemean for age or
Acute need for mechanical ventilation notrelated to neuromuscular disease or generalanesthesia.
* Leukocyte count elevated/depressedfor age/>10% immature neutrophils
SEPSISSIRS plus a suspected or proven infection
SEVERE SEPSISSEPSIS with one of the followingA…Cardiovascular dysfunction, defined asDespite administration of > 40ml/kg/
isotonic iv bolus in 1 hour,Hypotension < 5th centile for age /systolic
BP<2 S.D below normalfor age
ORNeed for inotropes to maintain BP ORAny 2 0f the followingØ Unexplained metabolic acidosis (Base
deficit >5mEq)Ø 2. Lactate in arterial blood>2 times
upper limit of normalØ 3. Urine output<0.5ml/kg/hrØ 4. Capillary filling time of >5 secØ 5. Core to peripheral temp difference
>3oCB… Acute respiratory distress syndrome is
defined by the presence of PaO2/FiO2 < 200mm Hg, bilateral infiltrates in chest radiographand no evidence of left heart failure.
ORSepsis plus 2 or more organ dysfuction
SEPTIC SHOCKSepsis with cardiovascular organ
dysfunction as described above
LABORATORY DIAGNOSISHematology—thrombocytopenia, abnormal
leucocyte counts,prolonged prothrombintime,prolonged activated partialthromboplastin time ,decreasedfibrinogen,elevated fibrin split products .Peripheral smear can show elevated immatureforms of neutrophils, toxic granules, Dohlebodies. Neutropenia is an ominous sign ofsepsis (4,6,8,10).
Biochemically—Hyperglycemia (due tostress response) or Hypoglycemia (storeexhaustion), Hypocalcemia ,acidosis,hypoalbuminemia.
In case of MODS—chest X-Ray featuressuggestive of ARDS ,abnormal renal function,liver function can be seen.
In refractory cases we need to check serumcortisol levels to detect adrenal insufficiency
Culture of blood, urine to isolate theorganism before starting antibiotics.
Imaging to detect the focus of infection(4,6,7,8,10).
MANAGEMENT
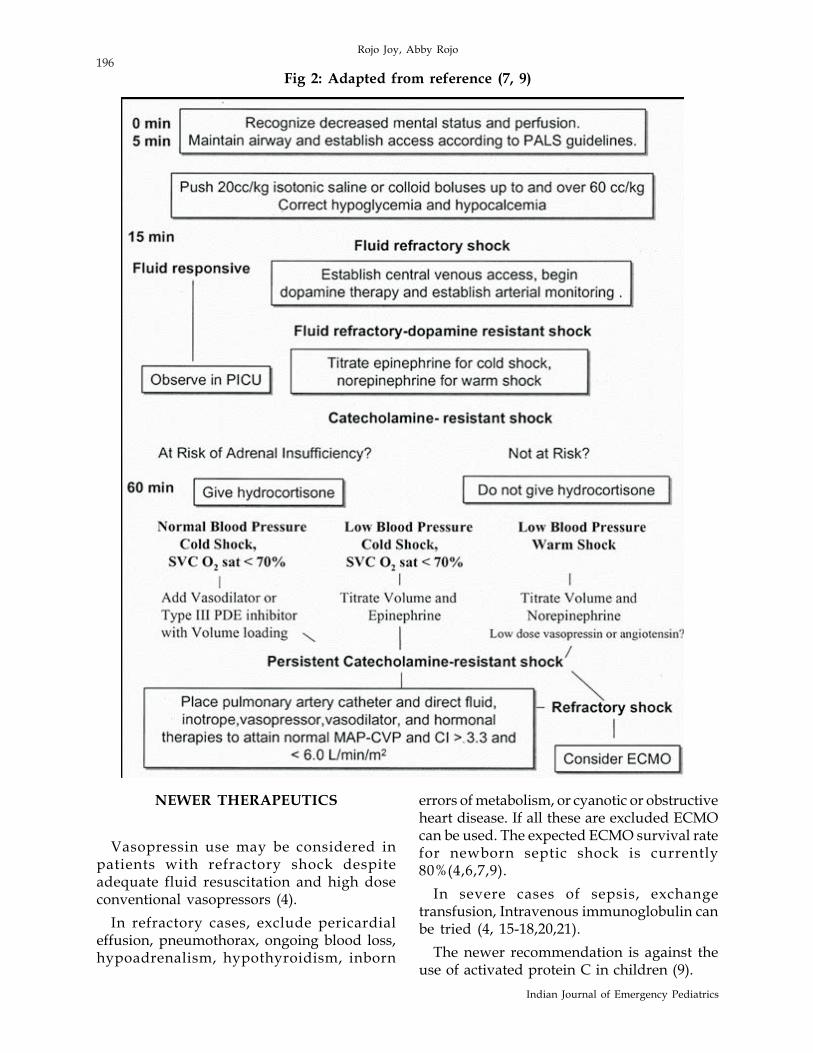
Management guidelines are published byAmerican college of Critical Care medicine /Society for critical care medicine task forcecommittee members and Surviving SepsisCampaign (4-9).
Septic shock can be recognized beforehypotension occurs, by a clinical triad thatincludes hypothermia or hyperthermia, alteredmental status, and peripheral vasodilatation(warm shock) or cool extremities (cold shock).The purpose of treatment of shock is tomaintain perfusion pressure above the criticalpoint below which blood flow cannot beeffectively maintained in individual organs.Because the kidney receives the second highestblood flow to any organ in the body,measurement of urine output and creatinineclearance can be used as an indicator ofadequate perfusion pressure (4,7).
Rapid aggressive resuscitation with fluidsand catecholamines reduces mortality. Early
Rojo Joy, Abby Rojo

193
Volume 2 Number 4 Oct - Dec 2010
goal directed resuscitation in early 6 hours ofrecognition of septic shock is needed for goodoutcome (4-9).
First 0 – 5 minABC OF RESUSCITATIONRecognise decreased mental status &
perfusion. Establish & maintain airway andcirculation according to PediatricADVANCED LIFE SUPPORT guidelines. IV/intra osseous access for maintainingcirculation.
5 min – 15 minThe fluid resuscitation with crystalloids and
colloids is of fundamental importance tosurvival of septic shock. Fluid boluses of 20ml/kg can be rapidly pushed in and some severecases may require boluses of 60ml/kg or evenupto 200ml/kg in first hour .Monitor forfeatures of fluid overload in the form of basalrales (pulmonary edema), hepatomegaly (4-9).
Fluid choices include crystalloids (normalsaline) and colloids (dextran, gelatin, or 5%albumin) based on task force recommendation.Meta-analysis of clinical studies comparingcrystalloid and colloid resuscitation indicateno clinical outcome difference betweencolloids and crystalloids. As the volume ofdistribution is much larger for crystalloidsthan for colloids, resuscitation withcrystalloids requires more fluid to achieve thesame end points and results in more edema.This fluid challenge can replace theintravascular fluid deficit. Most patients willneed aggressive fluid therapy till capillaryleaks settles. Along with correction of fluiddeficit, we need to give the normalmaintenance fluid (4,6,7,12-15).
Fresh-frozen plasma may be infused tocorrect abnormal prothrombin time andpartial thromboplastin time but should not bepushed because it has hypotensive effects likelycaused by vasoactive kinins (7). It is reasonableto maintain hemoglobin concentration withinthe normal range for age.
Correct hypocalcemia, hypoglycemia,acidosis(4-9). (Bicarbonate therapy is notrecommended for pH>7.15 for the purpose ofcorrecting hypotension)(4).
* Start early antibiotic based on the agegroup and general condition(4-11).
NeonateCefotaxime and aminoglycoside; add
Vancomycin in nosocomial Infection (10).
ChildCefotaxime,or Ceftriaxone ; add
vancomycin for meningitis ,areas ofpneumococcal resistance to cephalosporins(10).
Immunocompromised patient :Vancomycinand antipseudomonas agent (10).
Toxic shock: Penicillin and clindamycin(10).
Blood cultures has to be taken beforeantibiotic therapy ,administer broad-spectrumantibiotic therapy within 1 hr of diagnosis ofseptic shock and severe sepsis without septicshock ,reassessment of antibiotic therapy withmicrobiology and clinical data to narrowcoverage when appropriate and a usual 7-10 days of antibiotic therapy guided by clinicalresponse (4,6,7,8,9,10,11).
15 min – 60 minWhen an appropriate fluid challenge fails
to restore adequate blood pressure and organperfusion and resuscitation goals are not met,therapy with vasopressor agents should bestarted. Vasopressor therapy may also beneeded in case of life-threatening hypotension,even when a fluid challenge is in progress andhypovolemia has not yet been corrected (4).
Intensive care admission with central veinaccess and arterial pressure monitoring shouldbe considered and used in children with fluid-refractory shock (4-9).
Monitor* Pulse oximeter
Management of septic shock in children

194
Indian Journal of Emergency Pediatrics
* Continuous electrocardiography* Blood pressure-invasive ideally* Temperature* Urine output* Glucose and ionized calciumDopamine and Norepinephrine are the first
line inotropic agent in the management ofseptic shock. Compared to epinephrine thesedrugs cause less tachycardia and less effecton splanchnic circulation. As Norepinephrineincreases mean arterial pressure with leasteffect on heart rate, it is found to be morepotent than Dopamine in the septic shock inwarm shock. Low-dose dopamine should notbe used for renal protection as part of thetreatment of severe sepsis (4).
In case of dopamine resistant shock we canuse norepinephrine and epinephrine.Epinephrine can be used as a first-line choicefor cold hypodynamic shock in children (7).
Dobutamine inotropic therapy is used onlywhen cardiac output remains low despitefluid resuscitation and combined inotropic/vasopressor therapy (4,7,9).
Cold shock- dopamine resistant or as firstline, use epinephrine—titrate from 0.1-1microgram/kg/min (7,9).
Warm shock- dopamine resistant titratenorepinephrine from 0.1-2 microgram/kg/min (7,9).
60 MinsIf shock doesnot improve, recognise
catecholamine resistant shock. The committeechose the most conservative diagnosticapproach and defines adrenal insufficiency asa total cortisol level between 0 and 18 mg/dL.Based on the newer recommendation, steroidhas to be used only after the demonstration ofadrenal insufficiency. Begin hydrocortisone 50mg/kg for shock, followed by the same doseas a 24-hr infusion (4,7,9 ).
Based on the recommendations if T4 or T3level is low and sick euthyroid syndrome hasbeen excluded, oral Levothyroxine or, ifnecessary, intravenous T3 preparation canbe used to restore normal values for age (7,9).
Titrate the inotropes based on the bloodpressure and systemic vascular resistance.
1. Shock with Low Cardiac index, NormalBlood Pressure, and High Systemic VascularResistance.
Vasodilators like Nitroprusside orNitroglycerin are first line in patients withepinephrine-resistant shock. In patients whoare resistant to such therapy or those whodevelop nitrovasodilator toxicity in the formof cyanide toxicity, methemoglobulinemia, onecan use type III phosphodiesterase inhibitorssuch as Amrinone and Milrinone. Long halflife of these drugs can cause reversible toxicities(hypotension,arrhythmias) ,which can bereversed by noreinephrine infusions (4-9).Other vasodilators used and reported inneonatal and pediatric septic shock includeprostacyclin, phentolamine, pentoxifylline,and dopexamine (7).
2. Shock with High CI and Low SystemicVascular Resistance .
Norepinephrine is the drug of choice forage-dependent dopamine resistance andtitrate voume (7,9).
3. Shock with low CI and High SystemicVascular Resistance Titrate volume andepinephrine (7,9).
Persistent catecholamine shock Place pulmonary artery catheterDirect therapy-fluid, vasopressor,
vasodilator, inotropic support to maintainMean Arterial pressure(MAP) ,Central venouspressure (CVP), Cardiac Index(CI) >3.3 and<6 l/min/m2.
Consider Extra corporeal membraneoxygenation (ECMO) (4-9).
RESUSCITATION GOALS* Capillary filling time of 2 secs* Normal pulses with no differential
between peripheral and central pulses* Warm extremities* Urine output 1 mL/kg/hr,* Normal mental status,
Rojo Joy, Abby Rojo

195
Volume 2 Number 4 Oct - Dec 2010
* Normal blood pressure for age* Superior venacaval oxygen saturation
>70% after 6 hours or resuscitation isconsidered as a good outcome (4-9).
If the patient develops multiorgandysfunction ,targeted organ support strategiesare needed . In case of acute lung injury (ALI)/acute respiratory distress syndrome (ARDS)low tidal volume and limitation of inspiratoryplateau pressure strategy has to be used.Application of at least a minimal amount ofpositive end-expiratory pressure in acute lunginjury has been recommended. Head of bedelevation in mechanically ventilated patientsunless contraindicated and avoiding routineuse of pulmonary artery catheters in ALI/ARDS has been newly recommended(6,9).
In cases of bleeding manifestation due toDIC ,we need to replace coagulation factors,vitamin K and packed cells to maintaintargeted hemoglobin.
Blood sugar has to be controlled andhypoglycemia has to be avoided by givingglucose at 4-6mg/kg/min (4,6,9).
Renal support has to be given in case ofrenal shut down. Based on newerrecommendations , equivalence of continuousveno-venous hemofiltration and intermittenthemodialysis has been noted (6,9).
To prevent gastric stress ulcer, proton pumpinhibitors or H2 blockers can be used especiallyin mechanically ventilated children (4,6,9).
MANAGEMENT CONSIDERATIONSIN NEWBORN
Septic shock should be suspected in anynewborn with respiratory distress andreduced perfusion, particularly in the presenceof a maternal history of chorioamnionitis orprolonged rupture of membranes. Septic shockhas to be differentiated from shock due tocongenital heart disease, which will requireprostaglandin infusions for survival. Newbornseptic shock is typically accompanied byincreased pulmonary artery pressures whichcan cause right ventricle failure (7).
General management principles are same asthe older children with some slight differences.
In newborns, rapid fluid boluses of 10 mL/kg should be administered according to thecommittee recommendations . Up to 60ml/kg may be needed in first hour(7,9). Packedred blood cell transfusion are given to maintainhemoglobin >12 g/dL. Crystalloids are thefluid recommended for use in newborns withhemoglobin >12 g/dl in shock (4,7,9).
In newborn the effect of dopamine onpulmonary vascular resistance should be takeninto account. Usually, a combination ofdopamine at low dosage 8-12microgram /kg/min) and dobutamine (up to 30microgram/kg/min) is used; if the patient isnot responding to the therapy, thenepinephrine should be infused to restorenormal blood pressure and perfusion (7,9).
In newborn, measures to treat PPHN areimportant (7).
* Correct hypoxia* Correct acidosis with sodium
bicarbonate –alkalinisation upto pH of 7.5may be needed
* Maintain good systemic pressure toreduce the shunt
* Proper sedation to reduce thecatecholamine release which can raise thepulmonary artery pressure
* Inhaled Nitric oxide to decrease thepulmonary pressure (7).
* Pulmonary vasodilators such as NOdonors (Sildenafil) and Magnesium sulfate areunder trial
Steroid has to be used only after thedemonstration of adrenal insufficiency. Lowdose Hydrocortisone has been used (3 mg/kg/day) for 3-5 days. But the role of high dosesteroids is controversial due to the long termeffects in the brain development especially invery low birth weight infants (9).
Amrinone, Milrinone –can be used in thecases of cases with shock with increasedperipheral vascular resistance (9,15-18).
Management of septic shock in children
196
Indian Journal of Emergency Pediatrics
NEWER THERAPEUTICS
Vasopressin use may be considered inpatients with refractory shock despiteadequate fluid resuscitation and high doseconventional vasopressors (4).
In refractory cases, exclude pericardialeffusion, pneumothorax, ongoing blood loss,hypoadrenalism, hypothyroidism, inborn
Fig 2: Adapted from reference (7, 9)
errors of metabolism, or cyanotic or obstructiveheart disease. If all these are excluded ECMOcan be used. The expected ECMO survival ratefor newborn septic shock is currently80%(4,6,7,9).
In severe cases of sepsis, exchangetransfusion, Intravenous immunoglobulin canbe tried (4, 15-18,20,21).
The newer recommendation is against theuse of activated protein C in children (9).
Rojo Joy, Abby Rojo
197
Volume 2 Number 4 Oct - Dec 2010
There are trials reporting the efficacyregarding the use of methylene blue for thetreatment of sepsis (22).
In case of severe sepsis with neutropenia(Absolute Neutrophil count <1500),granulocyte monocyte colony stimulatingfactors has shown to improve outcome inneonates.(15-18).
REFERENCES
1. Kotsovolis G, Kallaras K. The role of endotheliumand endogenous vasoactive substances insepsis. Hippokratia, 2010; 14(2): 88-93.
2. Edul VK, Ferrara G, Dubin A. MicrocirculatoryDysfunction in Sepsis. Endocr Metab ImmuneDisord Drug Targets, 2010.
3. Wynn JL, Wong HR. Pathophysiology andtreatment of septic shock in neonates.ClinPerinatol, 2010; 37(2): 439-79.
4. Dellinger RP, Carlet JM, Masur H, GerlachH,Calandra T, Cohen J etal. Surviving sepsiscampaign guidelines for management of severesepsis and septic shock. Crit Care Med, 2004; 32:859-873.
5. Marshall JC, Dellinger RP, Levy M.The SurvivingSepsis Campaign: a history and a perspective. .Surg Infect (Larchmt), 2010; 11(3): 275-81.
6. Dellinger RP .Surviving sepsis campaign:international guidelines for management ofsevere sepsis and septic shock. Crit Care Med,2008; 36(1): 296-327.
7. Carcillo JA, Fields AI. Clinical practiceparameters for hemodynamic support ofpediatric and neonatal patients in septic shock.Crit Care Med, 2002; 30(6): 1365-1377.
8. Khilnani P.Cinical management guide lines ofpediatric septic shock.Indian J Crit Care Med,2005; 9: 164-172.
9. Brierley J, Carcillo JA, Choong K, Cornell T,Decaen A, Deymann A et al. Clinical practiceparameters for hemodynamic support ofpediatric and neonatal septic shock: 2007update from the American College of Critical CareMedicine. Crit Care Med, 2009; 37(2): 666-88.
10. Kleigman RM,Behrman RE,Jenson HB,StantonBF.Nelson text book of pediatrics.18th.South asiaedition. Elsevier, 2007; 8.
11. De Waele JJ. Early source control in sepsis.Langenbecks Arch Surg, 2010; 395(5): 489-94.
12. Fuhong S, Zhen W, Ying C, PeterR, Jean-LouisV. Fluid resuscitation in severe sepsis and septicShock: Albumin, Hydroxyethyl Starch, gelatinor Ringer’s Lactate-does it really make adifference? Shock, 2007; 27: 520-526.
13. Rivers EP, Jaehne AK, Eichhorn-Wharry L, BrownS, Amponsah D. Fluid therapy in septic shock.Curr Opin Crit Care, 2010; 16(4): 297-308.
14. Kohn Loncarica G. Early hemodynamic supportin septic shock.Arch Argent Pediatr, 2010; 108(3):249-54.
15. Perner A, Carlsen S, Marcussen K, Wesche N,Steensen M, Hidestål J et al. Septic shock inintensive care.Ugeskr Laeger, 2010; 172(16):1206-10.
16. Onyejiaka NA, Ali NB, Fogarasi SR. A neonatein septic shock. Clin Pediatr (Phila), 2010; 49(3):297-9.
17. Jones JG, Smith SL. Shock in the critically illneonate. J Perinat Neonatal Nurs, 2009; 23(4):346-54.
18. Lauterbach R, Pawlik D, Tomaszczyk B, CholewaB. Pentoxifylline treatment of sepsis of prematureinfants: preliminary clinical observations.Eur JPediatr, 1994; 153(9): 672-4.
Management of septic shock in children