management of rheumatoid arthritis raad makadsi. nice guidelines on the management of rheumatoid...
TRANSCRIPT
Management of Rheumatoid Arthritis
Raad Makadsi

NICE guidelines on the management of Rheumatoid Arthritis Feb 2009
• Key priorities for implementation
• Referral for specialist treatment
Investigations
• Rheumatoid factor • Anti-cyclic citrullinated peptide (CCP) antibodies
if: they are negative for rheumatoid factor, and • X-ray the hands and feet
• Once the diagnosis is made
• there is a need to inform decision-making about starting combination therapy
Communication and education • Explain the risks and benefits of Treatment
• Offer verbal and written information
• Education
• Offer the opportunity to take part in
existing educational activities, including self-management programmes

The multidisciplinary team
• Specialist nurse - who is responsible for coordinating the care
• Physiotherapy• Occupational therapy• Psychological interventions (for example,
relaxation, stress management and cognitive coping skills])
• Podiatrist (Functional insoles and therapeutic footwear)
DMARDs
• Offer a combination of DMARDs
• Ideally within 3 months
• Corticosteroids oral, intramuscular or intra-articular
DMARDs
• When sustained and satisfactory levels of disease control have been achieved, cautiously try to reduce drug doses
• If combination DMARD therapy is not appropriate, start DMARD mono-therapy
• Patients in whom disease-modifying or biological drug doses are being decreased or stopped, arrangements should be in place for prompt review

Glucocorticoids
• Short-term - recent-onset or established disease to rapidly decrease inflammation
• Long - term - In established RA continue glucocorticoids when:
- the long-term complications of glucocorticoid therapy have been fully discussed
- all other treatment options (including biological drugs) have been offered
Biological drugs
• Offer anti-TNF if patient failed two DMARDs including Methotrexate
• Do not offer the combination of tumour necrosis factor-α (TNF-α) inhibitor therapy and anakinra for RA
Symptom control
• Paracetamol, codeine or compound analgesics)
• Oral NSAIDs/COX-2 inhibitors should be used at the lowest effective dose for the shortest possible period of time
• If RA patient needs to take low-dose aspirin consider other analgesics before substituting or adding an NSAID or COX-2 inhibitor (with a PPI)

Monitoring rheumatoid arthritis
• Measure CRP and DAS28 regularly
• In early active RA, measure CRP and DAS28 monthly until treatment has controlled the disease to a level previously agreed with the person with RA
Monitoring rheumatoid arthritis
• In satisfactorily controlled established RA Offer patients review appointments at a frequency and location suitable to their needs
• Make sure they:
- have access to additional visits for disease flares
- know when and how to get rapid access to specialist care
- Have an on going drug monitoring
RA annual review• Assess disease activity and damage
• Functional ability (HAQ)
• Comorbidities, such as hypertension, IHD, osteoporosis and depression
• Look for complications, such as vasculitis and cervical spine, lung or eyes involvement
RA annual review
• Organise appropriate cross referral within the multidisciplinary team
• Need for referral for surgery
• The effect the disease is having on a person's life
Vit D role
• Calcium homeostasis
• Bone metabolism
• Regulates many other cellular functions including immunmodulations
SOURCES
• Sunlight and ultraviolet light - photoisomerize provitamin D to vitamin D3 (cholecalciferol) in the skin
• Diet fortified milk, fatty fish, cod-liver oil, and, to a lesser extent, eggs
ABSORPTION AND METABOLISM
• Dietary vitamin D micelles, -absorbed by enterocytes, -packaged into chylomicrons.
• Chylomicrons - liver - Vit D hydroxylation to form 25-hydroxyvitamin D (25OHD)
• Kidney- hydroxylation to 1,25-dihydroxyvitamin D (1,25OHD)
• 1,25OHD active form of vitamin D
ABSORPTION AND METABOLISM
• More than 25 metabolites identified, each with different biologic activities
• The synthesis of vitamin D is closely coupled to calcium homeostasis, and is modulated by parathyroid hormone, serum calcium, and phosphorus levels

DEFICIENCY AND RESISTANCE
caused by one of four mechanisms :• Inadequate dietary vitamin D, fat malabsorptive
disorders, and/or lack of photoisomerization• Impaired hydroxylation by the liver to produce
25-hydroxyvitamin D• Impaired hydroxylation by the kidneys to
produce 1,25-dihydroxyvitamin D• End organ insensitivity to vitamin D metabolites
(hereditary vitamin D resistant rickets)
• In early stage Vitamin D deficiency, hypophosphatemia is more marked than hypocalcemia
• Persistent deficiency, hypocalcemia occurs and causes secondary hyperparathyroidism,
• This leads to phosphaturia, demineralization of bones• More prolonged, lead to osteomalacia in adults and
rickets in children.• Glucocorticoids inhibit intestinal vitamin D-dependent
calcium absorption and therefore can cause osteomalacia
• Vitamin D stores decline with age, especially in the winter
• Vit D and calcium supplementation can reduce the risk of falls and fractures in the elderly
• The Recommended Dietary Allowance for vitamin D is 600 International Units for adults Age 70 years and for children 1 to 18 years of age
• For adults 71 years and older, 800 units (20 micrograms) daily is recommended
• Excessive doses of vit D in adults can result in intoxication
• Symptoms of acute intoxication are due to hypercalcemia and include confusion, polyuria, polydipsia, anorexia, vomiting, and muscle weakness
• Long-term intoxication can cause bone demineralization and pain. In children, the hypercalcemia can cause brain injury

CLINICAL MANIFESTATIONS
• Osteomalacia may be asymptomatic and present radiologically as osteopenia.
• Diffuse bone pain• polyarthralgias, • muscle weakness, and difficulty walking -
Waddling gate• Fracture• Muscle spasms, cramps
Investigations
• Alkaline phosphatase elevated• Serum calcium and phosphorus reduced• 25-hydroxyvitamin D (calcidiol) <15 ng/mL • PTH elevated

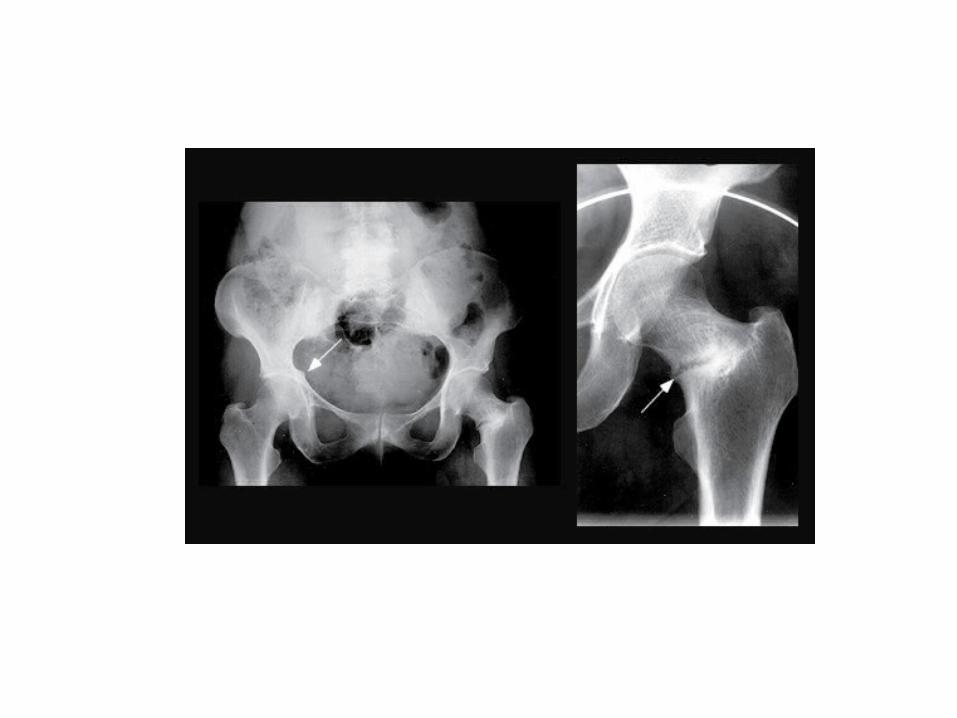
Radiographic findings
• Changes in vertebral bodies — • softening leads to a concavity of the vertebral
bodies called codfish vertebrae. The vertebral disks appear large and biconvex.
• There may be spinal compression fractures, but these are more common in osteoporosis.
• Looser zones — Looser pseudofractures, • Stress fractures
• Vitamin D3 (cholecalciferol) is available in 400, 800, 1000, 2000, 5000, 10,000, and 50,000 unit capsules
IM injection can be extremely painful• Vitamin D2 (ergocalciferol) is available for oral
use in 400 and 50,000 unit capsules A previously available IM preparation is now difficult to obtain