management of newly diagnosed child with type 1 diabetes
TRANSCRIPT
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 1 of 16
Management of Newly
Diagnosed Child with
Type 1 Diabetes
Reference: 947
Written by: Astha Soni
Peer reviewer: Carrie Mackenzie
Approved: November 2018
Review Due: July 2021
Purpose
The purpose of this guideline is to advise the acute medical team on how to initiate
management on a newly diagnosed diabetic who is well, not acidotic, not significantly
dehydrated and able to tolerate oral rehydration
Intended Audience
This guideline applies to all health care professionals working within Sheffield Children's Hospital involved in day to day care of children and young people with diabetes.

CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 2 of 16
Table of Contents
1. Introduction
2. Intended Audience
3. Guideline Content
a. Insulin
b. Blood Testing
c. Diet
d. General
4. References
1. Introduction
WHO Diagnostic criteria for diabetes based on blood glucose measurements and the presence or absence of symptoms as detailed below.
1. Symptoms of diabetes plus casual plasma glucose concentration≥11.1mmol/l (Casual is defined as any time of the day without regard to time since last meal)
2. Fasting plasma glucose ≥7mmol/l ( fasting is defined as no caloric intake for 8 hours) 3. 2 hour post load glucose≥11.1 mmol/l during an OGTT. ( The test should be performed
as described by WHO, using a glucose load containing 75g anhydrous glucose dissolved in
water or 1.75g/kg of body weight to a maximum of 75 g) This guideline does not cover the management of children presenting in moderate or severe diabetic ketoacidosis (DKA). For children presenting in DKA, please refer to Management of DKA guideline (1108). In the newly presenting well child with diabetes, we aim to keep the patient in hospital until families are reasonably confident in carbohydrate counting, able to administer subcutaneous insulin and test blood sugars. “Newly diagnosed patient starter packs” are kept in the seminar room on Ward 3. They
contain pens, needles, glucose meter, Carbs and Cals book and enough supplies for 24
hours. Please take the full pack from Ward 3 if you are going to start insulin on a newly
diagnosed child. Do NOT break into the packs to get glucose meters or insulin pens for
other inpatients if needed. There are spare pens/meters in the resource room.
2. Intended Audience
This guideline applies to all registered nursing staff and clinicians working within Sheffield Children's Hospital involved in day to day care of children and young people with diabetes.
CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 3 of 16
3. Guideline Content
Investigations to perform at diagnosis.
Send bloods for investigations as listed below before commencing insulin.
Investigations at diagnosis:
Glucose, U&E, HCO3. (Orange tube Lithium heparin)
HbA1C. (EDTA tube, pink)
Anti thyroid antibodies. (Green gel tube) and TSH (orange tube)
Tissue transglutaminase antibodies. (Green gel tube)
Islet cell antibodies and GAD antibodies (green gel tube)
C-peptide (lithium heparin).
Blood gas and blood ketones
Patient EDUCATION is an important part of diabetes management. Majority of it is
delivered by one of the specialist diabetes educators, nurses (Ext. 17320 OR mobile via
switchboard) and diabetes dietitians (Ext 17212 or mobile via switchboard). If the patient is
admitted Mon-Fri (9-5), please let the team know by ringing ext 17320 or bleeping
endocrine registrar on bleep 170. Out of hours, on-call diabetes consultant should be
informed via switch board.
A. INSULIN
A new patient will need approximately 0.5 unit/kg/day if <25 kgs and 0.7 unit/kg/day if >
25 kgs. Please make sure weight on admission is used when prescribing insulin.
We now start all children on multiple daily injection (MDI) regimens. In essence this
entails a long acting background insulin that lasts for approximately 24 hours and given
before bedtime or in the morning for younger patients (Levemir®) with rapid acting
insulin boluses for breakfast, lunch and tea (Novorapid®). For most children, this will
therefore require at least 4 injections daily. We give 40% of the total daily requirement
as background insulin.
If <25 kgs, work out the total daily insulin requirement (approximately 0.5 unit/kg/day).
Give 40% of this amount as Levemir in the morning.
Example:
Child age 6 years – weight 20kg
Insulin requirement 0.5 unit/kg/day i.e. 20kg x 0.5 = 10 units a day
Give 40% as Levemir in the morning. 10 units a day x 40% = 4 units.
If > 25 kgs, work out the total daily insulin requirement (approximately 0.7 unit/kg/day).
Give 40% of this amount as long acting Levemir at bedtime.
Example:
Child age 14 years – weight 50kg

CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 4 of 16
Insulin requirement 0.7 unit/kg/day i.e. 50kg x 0.7 = 35 units a day
Give 40% as longer acting Levemir at bedtime. So 35 units a day x 40% = 14 units at
bedtime. This is prescribed on Insulin prescribing chart. Appendix 2(see Example below)
They will need rapid acting insulin- Novorapid® before meals. This is given 15mins
before they eat. Insulin doses will be calculated based on their insulin to carbohydrate
ratios (ICR) which are based on their weight on admission. Please see appendix1
(Document 1-5) for individual ratios based on weights and see example below.
Insulin MUST be prescribed on Insulin prescription charts which are available on Ward
3. An example prescription chart with worked example can be found at the end of this
document (Appendix2).
Nursing staff/Support workers on Ward 3 have been trained to count carbohydrate
content in food. They should be able to advise on carbohydrate in a child’s meal.
Copies of Carbs and Cals (book with pictures of typical meals and sizes to aid
carbohydrate counting) are available on Ward 3 and will be given to patients on
admission. Insulin will then be administered based on the ICR.
Insulin must be given 15 minutes before child starts eating. The Diabetes team will
educate the family about Carbohydrate Counting from the next working day. Total
amount of insulin given before meal will be dependent on the blood glucose and
amount of carbohydrate in the meal.
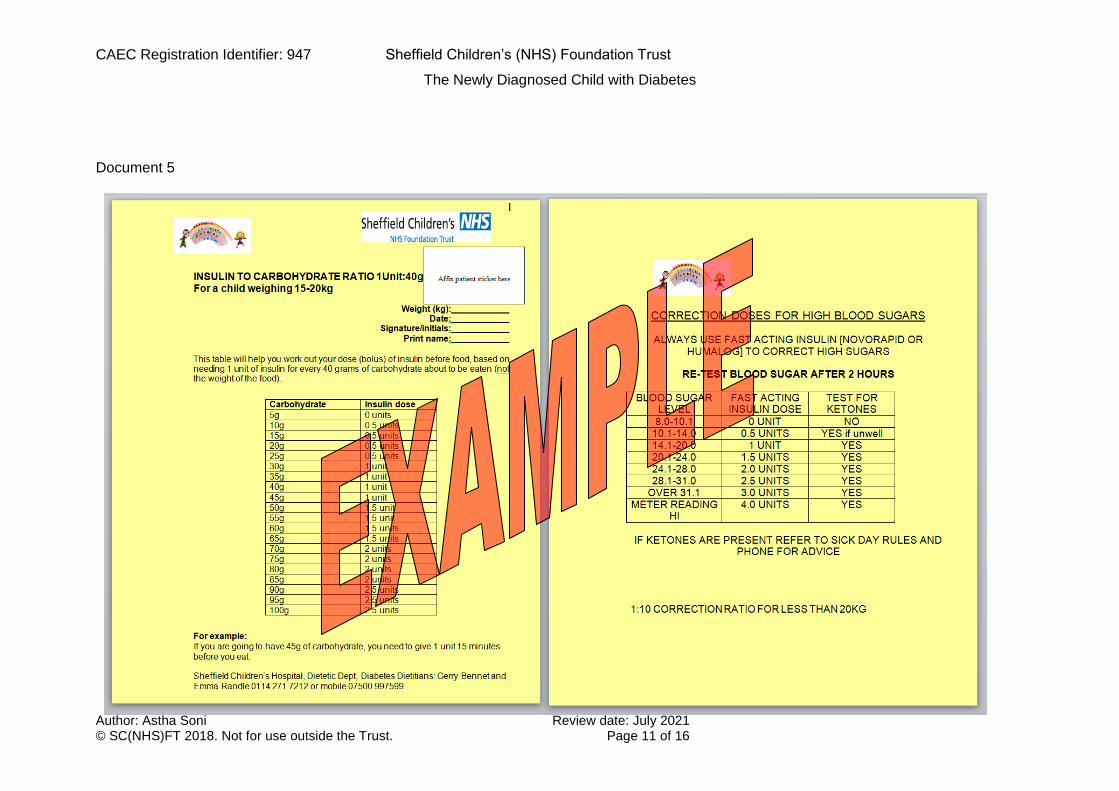
If blood glucose before meal is > 8 mmol/l, the patient will need correction dose of
insulin in addition to the amount calculated for food. These correction doses are
calculated according to patient’s weight following the guide on the back of ICR charts.
These charts are colour coded based on weight and laminated copies are available on
Ward 3.
B. BLOOD TESTING
All parents and patients should be able to test the blood sugar. The parent (and
child if appropriate) should be taught how to use a fastclix (or similar device) to draw blood
from the side (not the pulp) of the finger. To use a meter to measure blood glucose. All
newly diagnosed patients are provided with Accu-check Aviva Expert meters. They are set
up with individual patient ratios/corrections by the diabetes educators. Self-monitoring of
blood glucose (SMBG) is essential to aid adjustment of insulin dosages. Advise the family
to test blood glucose a minimum of 5 times a day (including before breakfast, lunch,
supper and bed time)
All parents/children with diabetes need to be taught how to test for blood ketones as
part of sick day rule advice and be provided with an appropriate ketone meter and
testing strips .This only needs to be routinely used if the blood sugar is persistently
>14mmol and at times of inter-current illness.
Target blood glucose levels:
o between 4 - 7mmol/L before meals,
o between 5-9 mmol/L post prandial (2 hours after meal)

CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 5 of 16
o 4-7 mmol/L at waking
Blood glucose level of <4 mmol/l is defined as hypoglycaemia (‘hypo’) in a child
with diabetes. The symptoms of hypoglycaemia should be explained. (We no longer
demonstrate a controlled hypo just prior to discharge). It is important that all primary
carers e.g. parents understand the possible signs of hypo and understand what
must be done to treat a ‘hypo’
Both parents should know how to use Dextrogel and Glucagon (in an emergency).
A 1mg "Glucagon" pack should be given to each family prior to discharge and the
parents should be shown how to prepare and give the pre-packed injection.
C. DIET
In order for a family to be safe for discharge, the emphasis is on healthy eating and
commencing carbohydrate counting. They will be advised about the relationship between
insulin action and carbohydrate, meal pattern and choosing suitable drinks/snacks.
Carbohydrate counting will commence from new diagnosis of Type 1 Diabetes and
the specialist diabetes educators will see the child and parents/carer on the ward.
They will carry out dietetic assessment and begin education with the child, and
family/carer.
Education is planned around the child’s age and stage and will support the family
with meal planning, choosing suitable drinks and timing of meals in the context of
each child’s individual circumstances.
Teaching of carbohydrate counting will be supported practically by the diabetes
team. Diabetes educators/ nursing/ward staff regarding meals chosen from the
kitchen. They will be helped to weigh the foods, quantify the carbohydrate and to
adjust the insulin dose appropriately. Food tables and Carbs and Cals book are
available to help with this as well as other resources in the ward resource folder.
Insulin will be adjusted according to the food to be eaten and their age/weight as per
guidance with correction doses as per guideline.
All blood glucose levels, food eaten and insulin given will be recorded on the
relevant drug charts to assess management and inform changes.
The dietetic recommendations target age appropriate healthy eating principles,
optimum glycaemic control, and appropriate growth. Any concerns regarding eating
behaviour would be taken into account and addressed with advice from our
psychology team member as needed.
The ward staff, and Diabetes team will assess confidence for discharge once the
child/family demonstrate competence with basic carbohydrate counting for meals
and insulin adjustment. Barriers to learning or concerns regarding patient safety for
home will be assessed and a plan put in place tailored to the patients/family needs
to support them on discharge.

CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 6 of 16
D. GENERAL
Diabetes education will be continued as an out-patient with the family attending 3 (or
more) further sessions to complete their learning and support their progress with
Carbohydrate Counting. The continuing education will include checking food diary, sick
day rules, management of activity and sport and general appropriate healthy eating for
age.
Education is continued as indicated by management at clinic with one to one sessions
arranged as needed
The family must understand that they should contact the duty doctor at the Children's
Trust at any time of day or night if they are worried about their child's immediate health
or can be seen in the next outpatient clinic for less urgent problems.
Out of hours, senior diabetes advice is available through the hospital switchboard if
necessary. Ensure the parents and child know how to contact the Paediatric Nurses for
Diabetes on extension 17320 or through switchboard, who will deal with most day-to-
day problems and visit at home regularly after discharge.
Give the parents and child a folder containing relevant booklets on diabetes.
Equipment checklist at discharge (should be prescribed on Medway TTO): You will need to
prescribe extra test strips, finger pricker lancets, Dextrogel, glucagons and the patient’s
insulins. There is a photo list on the ward of exactly what needs to be prescribed.
• Novorapid 3ml penfill cartridges x (1 box of 5 cartridges)
• Levemir 3 ml penfill x (1 box of 5 cartridges)
o Freestyle Optium OR Accu-check Aviva (please check the meter in new patient
pack) Test strips: ( 2 x boxes of 50 strips)
• BD viva 4 mm pen needles x (1 box of 90 needles)
• Accu-check fastclix lancets x 1 box
• Dextrose 40% oral gel 25 g x 3 tubes
• Glucagon injection 1 mg vial x 1
• 1 L sharps bin x 1
Diabetes team/educators will arrange appropriate follow up on discharge
4. References
1. [NICE (2015) Diabetes (type 1 and type 2) in children and young people. NICE guideline NG18 www.nice.org.uk/guidance/ng18
2. Care of the well child, newly diagnosed with Type 1 Diabetes Mellitus, ACDC guideline working group

CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 7 of 16
Appendix1
Note: These are example charts only. Please DO NOT PRINT.
Copies are available on Ward 3 and in Registrar’s office
Document 1

CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 8 of 16
Document 2

CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 9 of 16
Document 3

CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 10 of 16
Document 4
CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 11 of 16
Document 5
CAEC Registration Identifier Sheffield Children’s (NHS) Foundation Trust
CHO counting
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 12 of 16
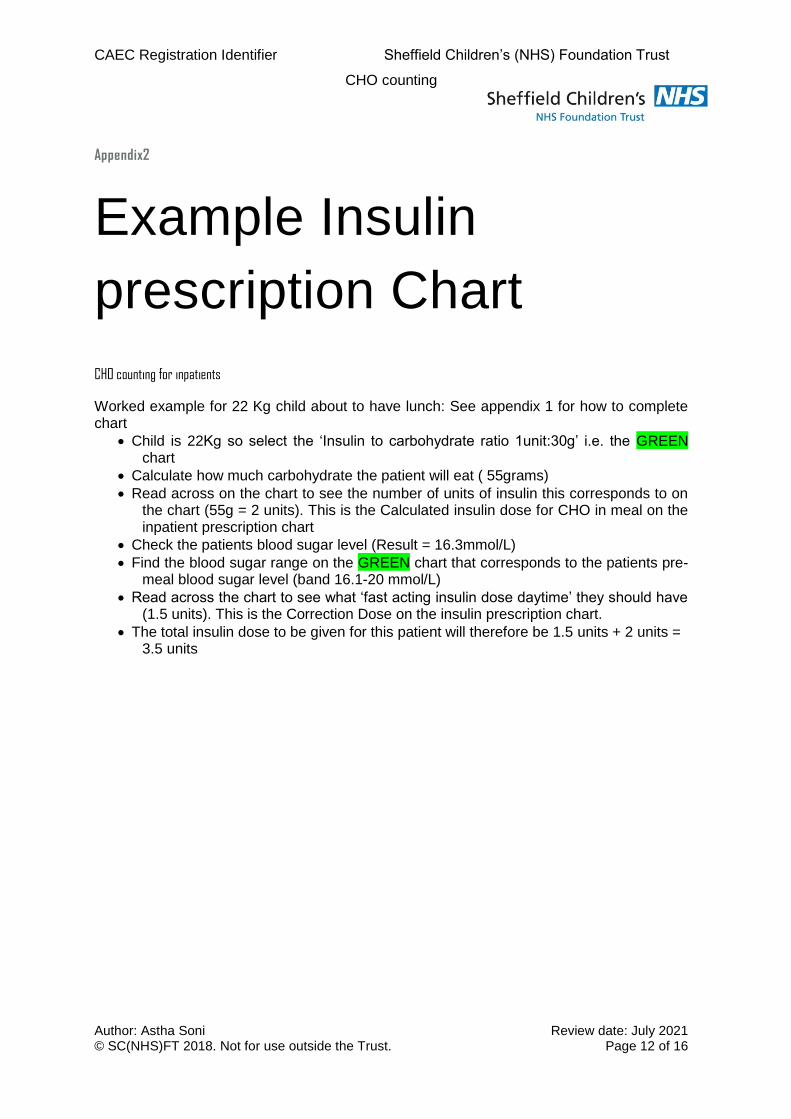
Appendix2
Example Insulin
prescription Chart
CHO counting for inpatients
Worked example for 22 Kg child about to have lunch: See appendix 1 for how to complete chart
Child is 22Kg so select the ‘Insulin to carbohydrate ratio 1unit:30g’ i.e. the GREEN chart
Calculate how much carbohydrate the patient will eat ( 55grams)
Read across on the chart to see the number of units of insulin this corresponds to on the chart (55g = 2 units). This is the Calculated insulin dose for CHO in meal on the inpatient prescription chart
Check the patients blood sugar level (Result = 16.3mmol/L)
Find the blood sugar range on the GREEN chart that corresponds to the patients pre-meal blood sugar level (band 16.1-20 mmol/L)
Read across the chart to see what ‘fast acting insulin dose daytime’ they should have (1.5 units). This is the Correction Dose on the insulin prescription chart.
The total insulin dose to be given for this patient will therefore be 1.5 units + 2 units = 3.5 units

CAEC Registration Identifier Sheffield Children’s (NHS) Foundation Trust
CHO counting
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 13 of 16

CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 14 of 16

CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 15 of 16

CAEC Registration Identifier: 947 Sheffield Children’s (NHS) Foundation Trust
The Newly Diagnosed Child with Diabetes
Author: Astha Soni Review date: July 2021 © SC(NHS)FT 2018. Not for use outside the Trust. Page 16 of 16