management of acute anterior shoulder dislocation of acute anterior shoulder dislocation benan...
TRANSCRIPT

Management of acute anterior shoulder dislocationBenan Dala-Ali,1 Marta Penna,1 Jamie McConnell,2 Ivor Vanhegan,1 Carlos Cobiella1
1Department of Trauma andOrthopaedic Surgery, UniversityCollege London Hospital,London, UK2Broomfield Hospital,Chelmsford, Essex, UK
Correspondence toDr Benan Dala-Ali, Departmentof Trauma and OrthopaedicSurgery, University CollegeLondon Hospital, 235 EustonRoad, London NW1 2BU, UK;[email protected]
Received 29 April 2012Accepted 21 June 2012Published Online First21 July 2012
To cite: Dala-Ali B,Penna M, McConnell J,et al. Br J Sports Med2014;48:1209–1215.
ABSTRACTShoulder dislocation is the most common large jointdislocation in the body. Recent advances in radiologicalimaging and shoulder surgery have shown the potentialdangers of traditional reduction techniques such as theKocher’s and the Hippocratic methods, which are stilladvocated by many textbooks. Many non-specialistscontinue to use these techniques, unaware of theirpotential risks. This article reviews the clinical andradiographic presentation of dislocation; some commonreduction techniques; their risks and success rate;analgesia methods to facilitate the reduction; andpostreduction management. Many textbooks advocatemethods that have been superceded by safer alternatives.Trainees should learn better and safer relocationmethods backed up by the current evidence available.
INTRODUCTIONShoulder dislocation is the most common largejoint dislocation in the body, with an incidence of1.7%1 or 8.2–17 per 100 000 per year.2 3
Practitioners should be aware of the potential com-plications and risks of different reduction techni-ques and that they know a safe technique that theyare confident in performing.Recent advances in radiological imaging and
shoulder surgery have shown the potential dangersof traditional reduction techniques such as theKocher’s and the Hippocratic methods, which arestill advocated by many textbooks. Many non-specialists continue to use these techniques,unaware of their potential risks.We review the clinical and radiographic presenta-
tion of dislocation, some common reduction tech-niques, their risks and success rate, analgesiamethods to facilitate the reduction and postreduc-tion management.
PATHOANATOMYThe bony architecture of the glenohumeral jointallows for a large range of movement but conferslittle inherent stability. The shoulder thus relies ona network of critical structures to steady it: bothstatic (such as the glenoid labrum and glenohum-eral ligaments—see table 1) and dynamic (chieflythe rotator cuff muscles). Their compromise canlead to traumatic dislocation and even recurrentinstability.4 5
CLINICAL PRESENTATIONNinety-six percent of all shoulder dislocations areanterior,6 and the patient typically describes a fallonto an outstretched arm. Posterior dislocation canoccur following a fall, electrocution or seizure.The patient will have pain on movement and
have an obvious shoulder deformity.
Clinical examination typically reveals a ‘squared-off ’ deformity. The humeral head may be bothvisible and palpable anteriorly, while the acromionmay be prominent laterally, with a cavity inferiorlywhere the humeral head would normally lie.It is important to check for neurovascular
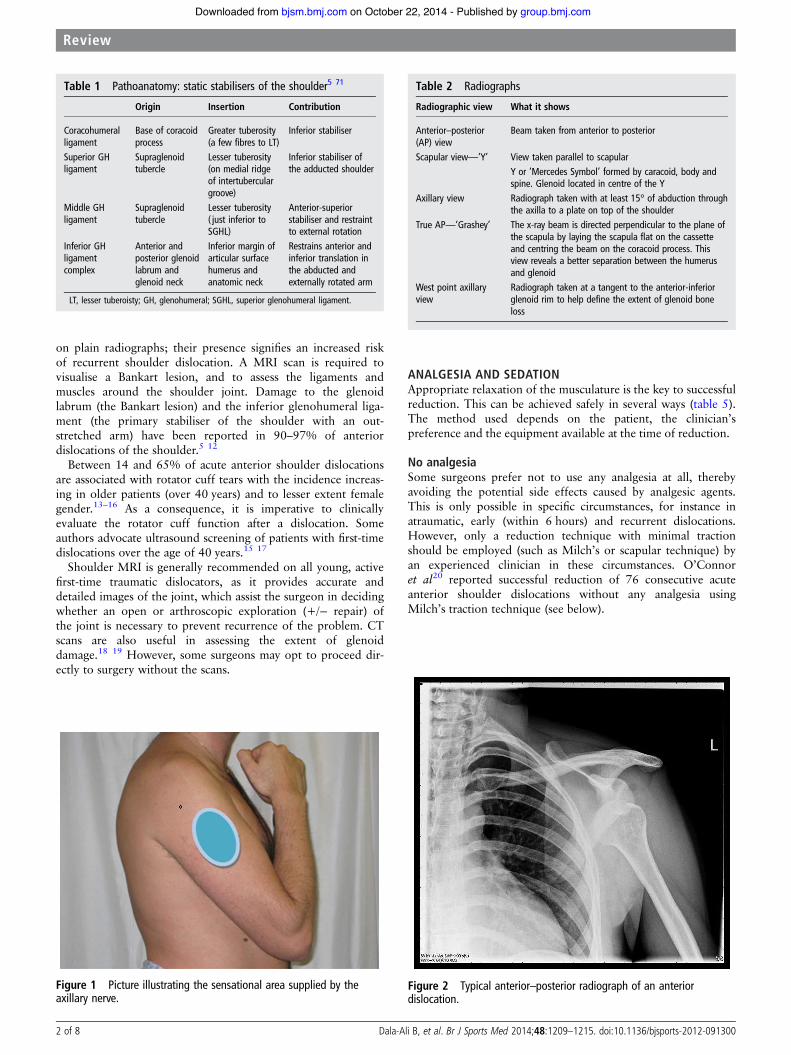
damage, particularly of the axillary nerve, whichprovides sensation to the ‘regimental badge’ regionof skin over the inferior part of deltoid (figure 1).Arterial damage is rare, but has been reported,7
and should be assessed by palpating the radial pulseand assessing capillary refill time (CRT) in thefingers of the injured side. If there is any doubt, anurgent surgical review should be sought. Damageto these structures is more common in elderlypatients, and in those that present with a haema-toma or with an associated fracture.8–10
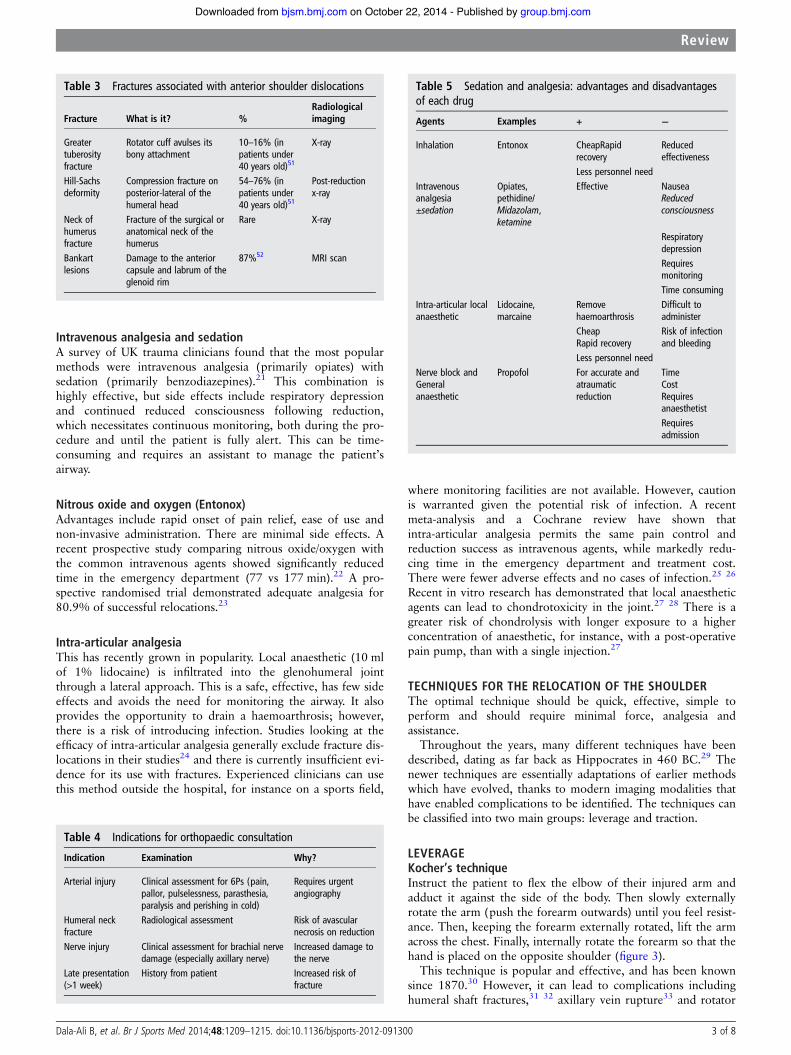
RADIOLOGICAL EVALUATIONAnterior–posterior, scapular (‘Y’) and axillaryradiographs (table 2 and figure 2) should berequested to confirm the diagnosis and reveal anyassociated fractures (table 3). The scapular and axil-lary view will help differentiate an anterior from aposterior dislocation of the humeral head and helpvisualise the position of the humeral head in three-dimensional space in relation to the glenoid fossa.Pre-reduction radiographs are recommended in
all first-time dislocations, patients over 40 years oldand following high-energy trauma. A large retro-spective case–control study over 5 years found thatsignificant fractures occur more commonly in thesegroups and are present in approximately one-quarter of shoulder dislocations overall.11
Post-reduction radiographs are recommended,both to ensure successful reduction and to confirmthat no fracture has been caused by the procedure.An orthopaedic opinion is recommended in the
presence of a fracture dislocation, to ensure thatreduction does not lead to further damage(table 4). For example, attempting to reduce a dis-location with a humeral head fracture could lead topossible avascular necrosis of the humeral head,and increase risk of neurovascular damage. A pro-spective study with extensive electrophysiologicalassessment found that 45% of patients with asso-ciated fractures also sustained nerve damage.9
The most common injuries associated with dis-location are Bankart and Hill-Sachs lesions. Duringan anterior dislocation the humeral head is forcedanteriorly out of the glenoid socket, potentiallycausing damage to the anterior capsule and labrumof the glenoid rim (Bankart lesion). As the final,posterior part of the head is forced out of the joint,it can collide with the anterior aspect of theglenoid rim, leading to a compression fracture ofthe posterior aspect of the humeral head(Hill-Sachs lesion). Hills-Sachs lesions can be seen
Dala-Ali B, et al. Br J Sports Med 2014;48:1209–1215. doi:10.1136/bjsports-2012-091300 1 of 8
Review
group.bmj.com on October 22, 2014 - Published by bjsm.bmj.comDownloaded from
on plain radiographs; their presence signifies an increased riskof recurrent shoulder dislocation. A MRI scan is required tovisualise a Bankart lesion, and to assess the ligaments andmuscles around the shoulder joint. Damage to the glenoidlabrum (the Bankart lesion) and the inferior glenohumeral liga-ment (the primary stabiliser of the shoulder with an out-stretched arm) have been reported in 90–97% of anteriordislocations of the shoulder.5 12
Between 14 and 65% of acute anterior shoulder dislocationsare associated with rotator cuff tears with the incidence increas-ing in older patients (over 40 years) and to lesser extent femalegender.13–16 As a consequence, it is imperative to clinicallyevaluate the rotator cuff function after a dislocation. Someauthors advocate ultrasound screening of patients with first-timedislocations over the age of 40 years.15 17
Shoulder MRI is generally recommended on all young, activefirst-time traumatic dislocators, as it provides accurate anddetailed images of the joint, which assist the surgeon in decidingwhether an open or arthroscopic exploration (+/− repair) ofthe joint is necessary to prevent recurrence of the problem. CTscans are also useful in assessing the extent of glenoiddamage.18 19 However, some surgeons may opt to proceed dir-ectly to surgery without the scans.
ANALGESIA AND SEDATIONAppropriate relaxation of the musculature is the key to successfulreduction. This can be achieved safely in several ways (table 5).The method used depends on the patient, the clinician’spreference and the equipment available at the time of reduction.
No analgesiaSome surgeons prefer not to use any analgesia at all, therebyavoiding the potential side effects caused by analgesic agents.This is only possible in specific circumstances, for instance inatraumatic, early (within 6 hours) and recurrent dislocations.However, only a reduction technique with minimal tractionshould be employed (such as Milch’s or scapular technique) byan experienced clinician in these circumstances. O’Connoret al20 reported successful reduction of 76 consecutive acuteanterior shoulder dislocations without any analgesia usingMilch’s traction technique (see below).
Table 1 Pathoanatomy: static stabilisers of the shoulder5 71
Origin Insertion Contribution
Coracohumeralligament
Base of coracoidprocess
Greater tuberosity(a few fibres to LT)
Inferior stabiliser
Superior GHligament
Supraglenoidtubercle
Lesser tuberosity(on medial ridgeof intertuberculargroove)
Inferior stabiliser ofthe adducted shoulder
Middle GHligament
Supraglenoidtubercle
Lesser tuberosity( just inferior toSGHL)
Anterior-superiorstabiliser and restraintto external rotation
Inferior GHligamentcomplex
Anterior andposterior glenoidlabrum andglenoid neck
Inferior margin ofarticular surfacehumerus andanatomic neck
Restrains anterior andinferior translation inthe abducted andexternally rotated arm
LT, lesser tuberoisty; GH, glenohumeral; SGHL, superior glenohumeral ligament.
Figure 2 Typical anterior–posterior radiograph of an anteriordislocation.
Table 2 Radiographs
Radiographic view What it shows
Anterior–posterior(AP) view
Beam taken from anterior to posterior
Scapular view—‘Y’ View taken parallel to scapularY or ‘Mercedes Symbol’ formed by caracoid, body andspine. Glenoid located in centre of the Y
Axillary view Radiograph taken with at least 15° of abduction throughthe axilla to a plate on top of the shoulder
True AP—‘Grashey’ The x-ray beam is directed perpendicular to the plane ofthe scapula by laying the scapula flat on the cassetteand centring the beam on the coracoid process. Thisview reveals a better separation between the humerusand glenoid
West point axillaryview
Radiograph taken at a tangent to the anterior-inferiorglenoid rim to help define the extent of glenoid boneloss
Figure 1 Picture illustrating the sensational area supplied by theaxillary nerve.
2 of 8 Dala-Ali B, et al. Br J Sports Med 2014;48:1209–1215. doi:10.1136/bjsports-2012-091300
Review
group.bmj.com on October 22, 2014 - Published by bjsm.bmj.comDownloaded from
Intravenous analgesia and sedationA survey of UK trauma clinicians found that the most popularmethods were intravenous analgesia (primarily opiates) withsedation (primarily benzodiazepines).21 This combination ishighly effective, but side effects include respiratory depressionand continued reduced consciousness following reduction,which necessitates continuous monitoring, both during the pro-cedure and until the patient is fully alert. This can be time-consuming and requires an assistant to manage the patient’sairway.
Nitrous oxide and oxygen (Entonox)Advantages include rapid onset of pain relief, ease of use andnon-invasive administration. There are minimal side effects. Arecent prospective study comparing nitrous oxide/oxygen withthe common intravenous agents showed significantly reducedtime in the emergency department (77 vs 177 min).22 A pro-spective randomised trial demonstrated adequate analgesia for80.9% of successful relocations.23
Intra-articular analgesiaThis has recently grown in popularity. Local anaesthetic (10 mlof 1% lidocaine) is infiltrated into the glenohumeral jointthrough a lateral approach. This is a safe, effective, has few sideeffects and avoids the need for monitoring the airway. It alsoprovides the opportunity to drain a haemoarthrosis; however,there is a risk of introducing infection. Studies looking at theefficacy of intra-articular analgesia generally exclude fracture dis-locations in their studies24 and there is currently insufficient evi-dence for its use with fractures. Experienced clinicians can usethis method outside the hospital, for instance on a sports field,
where monitoring facilities are not available. However, cautionis warranted given the potential risk of infection. A recentmeta-analysis and a Cochrane review have shown thatintra-articular analgesia permits the same pain control andreduction success as intravenous agents, while markedly redu-cing time in the emergency department and treatment cost.There were fewer adverse effects and no cases of infection.25 26
Recent in vitro research has demonstrated that local anaestheticagents can lead to chondrotoxicity in the joint.27 28 There is agreater risk of chondrolysis with longer exposure to a higherconcentration of anaesthetic, for instance, with a post-operativepain pump, than with a single injection.27
TECHNIQUES FOR THE RELOCATION OF THE SHOULDERThe optimal technique should be quick, effective, simple toperform and should require minimal force, analgesia andassistance.
Throughout the years, many different techniques have beendescribed, dating as far back as Hippocrates in 460 BC.29 Thenewer techniques are essentially adaptations of earlier methodswhich have evolved, thanks to modern imaging modalities thathave enabled complications to be identified. The techniques canbe classified into two main groups: leverage and traction.
LEVERAGEKocher’s techniqueInstruct the patient to flex the elbow of their injured arm andadduct it against the side of the body. Then slowly externallyrotate the arm (push the forearm outwards) until you feel resist-ance. Then, keeping the forearm externally rotated, lift the armacross the chest. Finally, internally rotate the forearm so that thehand is placed on the opposite shoulder (figure 3).
This technique is popular and effective, and has been knownsince 1870.30 However, it can lead to complications includinghumeral shaft fractures,31 32 axillary vein rupture33 and rotator
Table 5 Sedation and analgesia: advantages and disadvantagesof each drug
Agents Examples + −
Inhalation Entonox CheapRapidrecovery
Reducedeffectiveness
Less personnel needIntravenousanalgesia±sedation
Opiates,pethidine/Midazolam,ketamine
Effective NauseaReducedconsciousness
RespiratorydepressionRequiresmonitoringTime consuming
Intra-articular localanaesthetic
Lidocaine,marcaine
Removehaemoarthrosis
Difficult toadminister
Cheap Risk of infectionand bleedingRapid recovery
Less personnel needNerve block andGeneralanaesthetic
Propofol For accurate andatraumaticreduction
TimeCostRequiresanaesthetistRequiresadmission
Table 4 Indications for orthopaedic consultation
Indication Examination Why?
Arterial injury Clinical assessment for 6Ps (pain,pallor, pulselessness, parasthesia,paralysis and perishing in cold)
Requires urgentangiography
Humeral neckfracture
Radiological assessment Risk of avascularnecrosis on reduction
Nerve injury Clinical assessment for brachial nervedamage (especially axillary nerve)
Increased damage tothe nerve
Late presentation(>1 week)
History from patient Increased risk offracture
Table 3 Fractures associated with anterior shoulder dislocations
Fracture What is it? %Radiologicalimaging
Greatertuberosityfracture
Rotator cuff avulses itsbony attachment
10–16% (inpatients under40 years old)51
X-ray
Hill-Sachsdeformity
Compression fracture onposterior-lateral of thehumeral head
54–76% (inpatients under40 years old)51
Post-reductionx-ray
Neck ofhumerusfracture
Fracture of the surgical oranatomical neck of thehumerus
Rare X-ray
Bankartlesions
Damage to the anteriorcapsule and labrum of theglenoid rim
87%52 MRI scan
Dala-Ali B, et al. Br J Sports Med 2014;48:1209–1215. doi:10.1136/bjsports-2012-091300 3 of 8
Review
group.bmj.com on October 22, 2014 - Published by bjsm.bmj.comDownloaded from
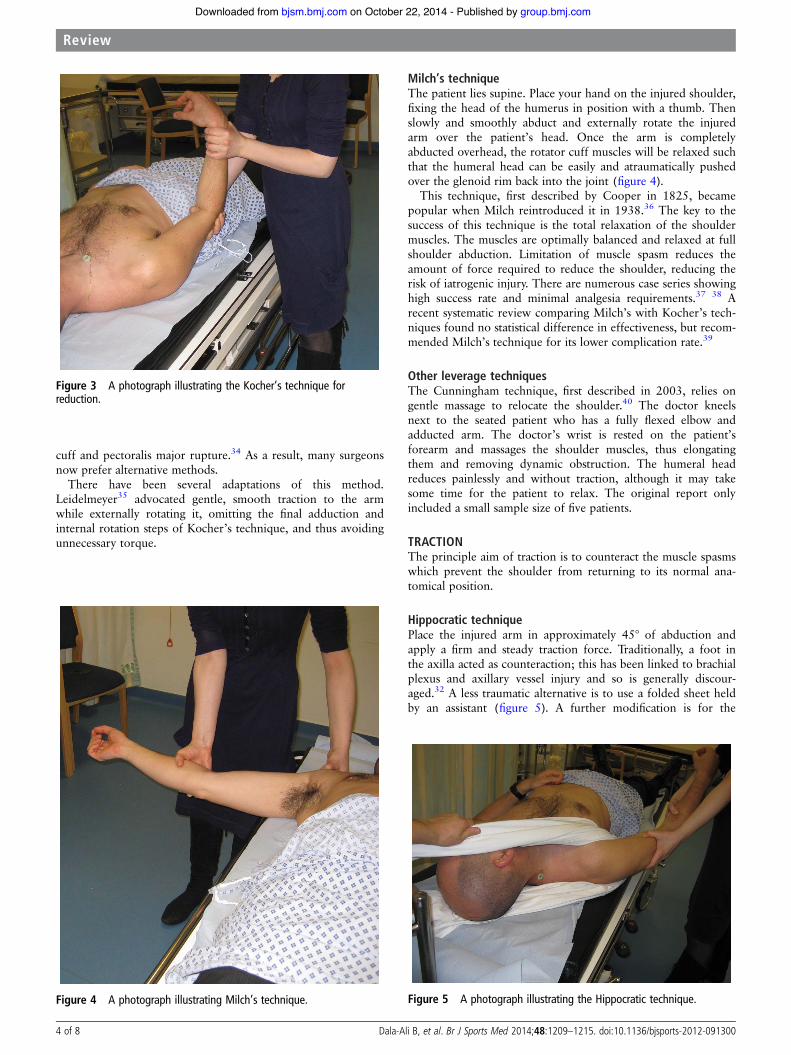
cuff and pectoralis major rupture.34 As a result, many surgeonsnow prefer alternative methods.
There have been several adaptations of this method.Leidelmeyer35 advocated gentle, smooth traction to the armwhile externally rotating it, omitting the final adduction andinternal rotation steps of Kocher’s technique, and thus avoidingunnecessary torque.
Milch’s techniqueThe patient lies supine. Place your hand on the injured shoulder,fixing the head of the humerus in position with a thumb. Thenslowly and smoothly abduct and externally rotate the injuredarm over the patient’s head. Once the arm is completelyabducted overhead, the rotator cuff muscles will be relaxed suchthat the humeral head can be easily and atraumatically pushedover the glenoid rim back into the joint (figure 4).
This technique, first described by Cooper in 1825, becamepopular when Milch reintroduced it in 1938.36 The key to thesuccess of this technique is the total relaxation of the shouldermuscles. The muscles are optimally balanced and relaxed at fullshoulder abduction. Limitation of muscle spasm reduces theamount of force required to reduce the shoulder, reducing therisk of iatrogenic injury. There are numerous case series showinghigh success rate and minimal analgesia requirements.37 38 Arecent systematic review comparing Milch’s with Kocher’s tech-niques found no statistical difference in effectiveness, but recom-mended Milch’s technique for its lower complication rate.39
Other leverage techniquesThe Cunningham technique, first described in 2003, relies ongentle massage to relocate the shoulder.40 The doctor kneelsnext to the seated patient who has a fully flexed elbow andadducted arm. The doctor’s wrist is rested on the patient’sforearm and massages the shoulder muscles, thus elongatingthem and removing dynamic obstruction. The humeral headreduces painlessly and without traction, although it may takesome time for the patient to relax. The original report onlyincluded a small sample size of five patients.
TRACTIONThe principle aim of traction is to counteract the muscle spasmswhich prevent the shoulder from returning to its normal ana-tomical position.
Hippocratic techniquePlace the injured arm in approximately 45° of abduction andapply a firm and steady traction force. Traditionally, a foot inthe axilla acted as counteraction; this has been linked to brachialplexus and axillary vessel injury and so is generally discour-aged.32 A less traumatic alternative is to use a folded sheet heldby an assistant (figure 5). A further modification is for the
Figure 4 A photograph illustrating Milch’s technique. Figure 5 A photograph illustrating the Hippocratic technique.
Figure 3 A photograph illustrating the Kocher’s technique forreduction.
4 of 8 Dala-Ali B, et al. Br J Sports Med 2014;48:1209–1215. doi:10.1136/bjsports-2012-091300
Review
group.bmj.com on October 22, 2014 - Published by bjsm.bmj.comDownloaded from
patient to hang their injured arm over the back of a chair andthen stand while their wrist is held by the doctor.41
Another similar method is the Snowbird technique. Thepatient is again placed on a chair and asked to support hisaffected arm. A Stockinette tubular bandage is placed on thepatient’s wrist, with the elbow held at 90° of flexion. Thepatient is then asked to stand up while the physician’s foot isplaced in the stockinet loop to provide downward traction. Thismethod was successfully employed at the Snowbird EmergencyDepartment in the USA to reduce 97% of 118 anterior disloca-tions with no complications.42
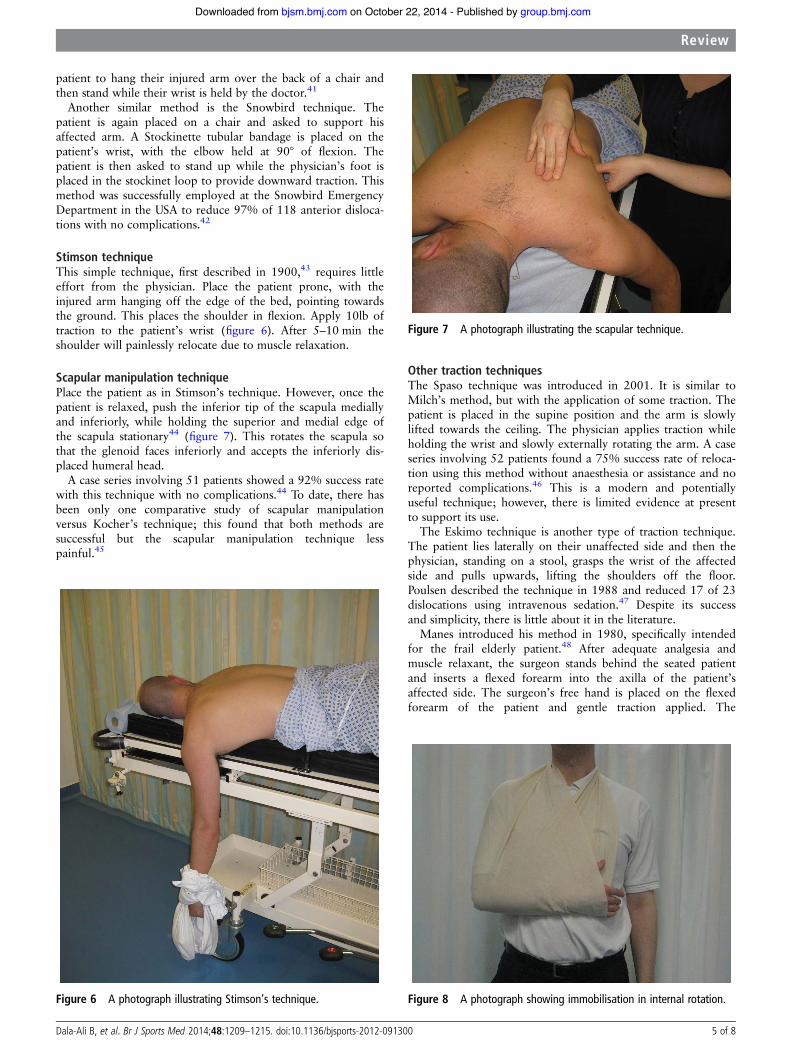
Stimson techniqueThis simple technique, first described in 1900,43 requires littleeffort from the physician. Place the patient prone, with theinjured arm hanging off the edge of the bed, pointing towardsthe ground. This places the shoulder in flexion. Apply 10lb oftraction to the patient’s wrist (figure 6). After 5–10 min theshoulder will painlessly relocate due to muscle relaxation.
Scapular manipulation techniquePlace the patient as in Stimson’s technique. However, once thepatient is relaxed, push the inferior tip of the scapula mediallyand inferiorly, while holding the superior and medial edge ofthe scapula stationary44 (figure 7). This rotates the scapula sothat the glenoid faces inferiorly and accepts the inferiorly dis-placed humeral head.
A case series involving 51 patients showed a 92% success ratewith this technique with no complications.44 To date, there hasbeen only one comparative study of scapular manipulationversus Kocher’s technique; this found that both methods aresuccessful but the scapular manipulation technique lesspainful.45
Other traction techniquesThe Spaso technique was introduced in 2001. It is similar toMilch’s method, but with the application of some traction. Thepatient is placed in the supine position and the arm is slowlylifted towards the ceiling. The physician applies traction whileholding the wrist and slowly externally rotating the arm. A caseseries involving 52 patients found a 75% success rate of reloca-tion using this method without anaesthesia or assistance and noreported complications.46 This is a modern and potentiallyuseful technique; however, there is limited evidence at presentto support its use.
The Eskimo technique is another type of traction technique.The patient lies laterally on their unaffected side and then thephysician, standing on a stool, grasps the wrist of the affectedside and pulls upwards, lifting the shoulders off the floor.Poulsen described the technique in 1988 and reduced 17 of 23dislocations using intravenous sedation.47 Despite its successand simplicity, there is little about it in the literature.
Manes introduced his method in 1980, specifically intendedfor the frail elderly patient.48 After adequate analgesia andmuscle relaxant, the surgeon stands behind the seated patientand inserts a flexed forearm into the axilla of the patient’saffected side. The surgeon’s free hand is placed on the flexedforearm of the patient and gentle traction applied. The
Figure 6 A photograph illustrating Stimson’s technique.
Figure 7 A photograph illustrating the scapular technique.
Figure 8 A photograph showing immobilisation in internal rotation.
Dala-Ali B, et al. Br J Sports Med 2014;48:1209–1215. doi:10.1136/bjsports-2012-091300 5 of 8
Review
group.bmj.com on October 22, 2014 - Published by bjsm.bmj.comDownloaded from
surgeon’s forearm pulls in a proximal and lateral direction andlevers the humeral head into the glenoid socket, after whichtraction is released. Manes states that compared to other techni-ques this method is relatively atraumatic. However, it was onlytested on 35 elderly patients and so larger comparative studiesare needed.
In 2009, orthopaedic surgeons in Greece published a newtechnique called the FARES method, which stands for ‘fast, reli-able and safe’.49 This method involves laying the patient supinewith the affected arm resting by their side with a straight elbowand thumb pointing up. The doctor holds the patient’s handand applies a gentle traction force, pulling the arm down awayfrom the patient’s head. The arm is then slowly abducted whileapplying a vertical oscillating movement, until abduction to 90°is achieved. This is the point at which the doctor externallyrotates the arm and continues with abduction while furtherapplying traction and oscillatory movements. The authors com-pared their FARES method to Kocher’s and Hippocratic techni-ques and showed the FARES method to be significantly moreeffective (success rate 88.7 vs 68% and 72.5%), faster and lesspainful than the two alternatives. However, the study hadlimited numbers, used a potentially biased visual analogue painscore, and did not perform post-reduction imaging to identifyany possible subclinical shoulder injury. Further research isneeded to compare the FARES method to other newertechniques.
POSTREDUCTION MANAGEMENTImmobilisationOnce the shoulder has been relocated, radiographic confirm-ation of the position is advised. A study involving 73 patients
found that 37.5% of fractures could only be seen in the post-reduction radiographs.50
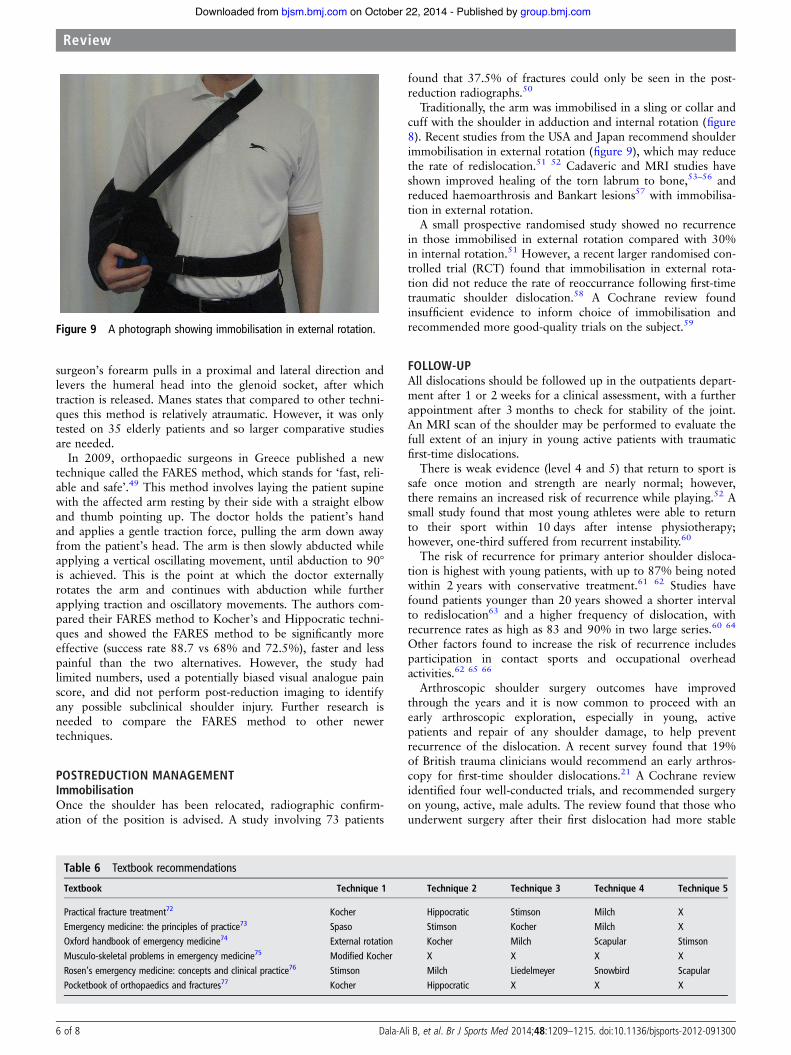
Traditionally, the arm was immobilised in a sling or collar andcuff with the shoulder in adduction and internal rotation (figure8). Recent studies from the USA and Japan recommend shoulderimmobilisation in external rotation (figure 9), which may reducethe rate of redislocation.51 52 Cadaveric and MRI studies haveshown improved healing of the torn labrum to bone,53–56 andreduced haemoarthrosis and Bankart lesions57 with immobilisa-tion in external rotation.
A small prospective randomised study showed no recurrencein those immobilised in external rotation compared with 30%in internal rotation.51 However, a recent larger randomised con-trolled trial (RCT) found that immobilisation in external rota-tion did not reduce the rate of reoccurrance following first-timetraumatic shoulder dislocation.58 A Cochrane review foundinsufficient evidence to inform choice of immobilisation andrecommended more good-quality trials on the subject.59
FOLLOW-UPAll dislocations should be followed up in the outpatients depart-ment after 1 or 2 weeks for a clinical assessment, with a furtherappointment after 3 months to check for stability of the joint.An MRI scan of the shoulder may be performed to evaluate thefull extent of an injury in young active patients with traumaticfirst-time dislocations.
There is weak evidence (level 4 and 5) that return to sport issafe once motion and strength are nearly normal; however,there remains an increased risk of recurrence while playing.52 Asmall study found that most young athletes were able to returnto their sport within 10 days after intense physiotherapy;however, one-third suffered from recurrent instability.60
The risk of recurrence for primary anterior shoulder disloca-tion is highest with young patients, with up to 87% being notedwithin 2 years with conservative treatment.61 62 Studies havefound patients younger than 20 years showed a shorter intervalto redislocation63 and a higher frequency of dislocation, withrecurrence rates as high as 83 and 90% in two large series.60 64
Other factors found to increase the risk of recurrence includesparticipation in contact sports and occupational overheadactivities.62 65 66
Arthroscopic shoulder surgery outcomes have improvedthrough the years and it is now common to proceed with anearly arthroscopic exploration, especially in young, activepatients and repair of any shoulder damage, to help preventrecurrence of the dislocation. A recent survey found that 19%of British trauma clinicians would recommend an early arthros-copy for first-time shoulder dislocations.21 A Cochrane reviewidentified four well-conducted trials, and recommended surgeryon young, active, male adults. The review found that those whounderwent surgery after their first dislocation had more stable
Figure 9 A photograph showing immobilisation in external rotation.
Table 6 Textbook recommendations
Textbook Technique 1 Technique 2 Technique 3 Technique 4 Technique 5
Practical fracture treatment72 Kocher Hippocratic Stimson Milch XEmergency medicine: the principles of practice73 Spaso Stimson Kocher Milch XOxford handbook of emergency medicine74 External rotation Kocher Milch Scapular StimsonMusculo-skeletal problems in emergency medicine75 Modified Kocher X X X XRosen’s emergency medicine: concepts and clinical practice76 Stimson Milch Liedelmeyer Snowbird ScapularPocketbook of orthopaedics and fractures77 Kocher Hippocratic X X X
6 of 8 Dala-Ali B, et al. Br J Sports Med 2014;48:1209–1215. doi:10.1136/bjsports-2012-091300
Review
group.bmj.com on October 22, 2014 - Published by bjsm.bmj.comDownloaded from

and functionally better joints compared to those who weretreated conservatively.67
There is strong evidence in favour of arthroscopic evaluationand primary surgical repair following such injuries.68–70 A level1 RCT demonstrated recurrent dislocation in 3% at 2 years inthose treated surgically versus 54% in those treated conserva-tively. At 10 years’ follow-up, subjective function was good orexcellent in 70% of surgically treated cases versus 75% unsatis-factory outcome in conservatively managed cases.70
CONCLUSIONThe key to successful reduction is relaxation of the patient.Experienced clinicians may attempt reduction initially withoutany analgesia or sedation. If unsuccessful, one could thenproceed to intra-articular analgesia, as it has proven to be safeand effective. Alternatively, sedation with or without analgesiacould be utilised.
It is important to be aware of the potential complications andrisks of different reduction techniques. Traditional techniquessuch as Kocher’s are effective but with potential complicationsand therefore should not be encouraged. Newer methods aresafer and just as effective.
Many textbooks advocate methods that have been supercededby safer alternatives (table 6). Trainees should learn better andsafer relocation methods backed by the current evidenceavailable.
Correction notice An uncorrected version of this paper was mistakenly uploadedto Online First. Our apologies to the author for this oversight.
Contributors BDA is the lead author. MP, JM and IV assisted with the literaturereview and manuscript preparation. MP also prepared the photos for the figures. CCis the senior author and ensured all the information was up-to-date. All authorshave read and approved the final manuscript.
Funding None.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1 Hovelius L. Incidence of shoulder dislocation in Sweden. Clin Orthop Relat Res
1982;166:127–31.2 Krøner K, Lind T, Jensen J. The epidemiology of shoulder dislocations. Arch Orthop
Trauma Surg 1989;108:288–90.3 Simonet WT, Melton LJ III, Cofield RH, et al. Incidence of anterior shoulder
dislocation in Olmsted County, Minnesota. Clin Orthop Relat Res1984;186:186–91.
4 Dumont GD, Russell RD, Robertson WJ. Anterior shoulder instability: a review ofpathoanatomy, diagnosis and treatment. Curr Rev Musculoskelet Med 2011;4:200–7. doi: .
5 Burkart AC, Debski RE. Anatomy and function of the glenohumeral ligaments inanterior shoulder instability. Clin Orthop Relat Res 2002;400:32–9.
6 Goss TP. Anterior glenohumeral instability. Orthopedics 1988;11:87–95.7 Gates JD, Knox JB. Axillary artery injuries secondary to anterior dislocation of the
shoulder. J Trauma 1995;39:581–3.8 Visser CP, Coene LN, Brand R, et al. The incidence of nerve injury in anterior
dislocation of the shoulder and its influence on functional recovery. A prospectiveclinical and EMG study. J Bone Joint Surg Br 1999;81:679–85.
9 de Laat EA, Visser CP, Coene LN, et al. Nerve lesions in primary shoulderdislocations and humeral neck fractures. A prospective clinical and EMG study. JBone Joint Surg Br 1994;76:381–3.
10 Blom S, Dahlbäck LO. Nerve injuries in dislocations of the shoulder joint andfractures of the neck of the humerus. A clinical and electromyographical study. ActaChir Scand 1970;136:461–6.
11 Emond M, Le Sage N, Lavoie A, et al. Clinical factors predicting fractures associatedwith an anterior shoulder dislocation. Acad Emerg Med 2004;11:853–8.
12 Owens BD, Nelson BJ, Duffey ML, et al. Pathoanatomy of first-time, traumatic,anterior glenohumeral subluxation events. J Bone Joint Surg Am 2010;92:1605–11.
13 Robinson CM, Shur N, Sharpe T, et al. Injuries associated with traumatic anteriorglenohumeral dislocations. J Bone Joint Surg Am 2012;94:18–26.
14 Cutts S, Prempeh M, Dre S. Anterior shoulder dislocation. Ann R Coll Surg Engl2009;91:2–7.
15 Mancini GB, Malaspina C, Scalercio AM, et al. Anterior shoulder dislocation andinjuries of the rotator cuff in patients aged over 40 years. Clinical and sonographicstudy. Chir Organi Mov 2001;86:37–44.
16 Simank HG, Dauer G, Schneider S, et al. Incidence of rotator cuff tears in shoulderdislocations and results of therapy in older patients. Arch Orthop Trauma Surg2006;126:235–40.
17 Berbig R, Weishaupt D, Prim J, et al. Primary anterior shoulder dislocation androtator cuff tears. J Shoulder Elbow Surg 1999;8:220–5.
18 d’Elia G, Di Giacomo A, D’Alessandro P, et al. Traumatic anterior glenohumeralinstability: quantification of glenoid bone loss by spiral CT. Radiol Med2008;113:496–503.
19 Chuang TY, Adams CR, Burkhart SS. Use of preoperative three-dimensionalcomputed tomography to quantify glenoid bone loss in shoulder instability.Arthroscopy 2008;24:376–82.
20 O’Connor DR, Schwarze D, Fragomen AT, et al. Painless reduction of acute anteriorshoulder dislocations without anesthesia. Orthopedics 2006;29:528–32.
21 Chong M, Karataglis D, Learmonth D. Survey of the management of acute traumaticfirst-time anterior shoulder dislocation among trauma clinicians in the UK. Ann RColl Surg Engl 2006;88:454–8.
Summary points
▸ The shoulder is the most common large joint dislocation,which dislocates in an anterior direction in 96% of cases.
▸ It is important to assess the neurovascular status of the arm.The axillary nerve is the most common injury; this can betested by assessing sensation in the ‘regimenatry badge’area located around the lateral upper arm.
▸ Experienced clinicians may attempt reduction without anyanalgesia or sedation. If unsuccessful, one could thenproceed to intra-articular analgesia, Entonox or sedation.
▸ Studies have shown both Kocher’s and Hippocratictechniques are associated with complications and should beavoided despite being advocated by most textbooks.Stimson, Milch’s and scapular are newer techniques thathave proven to be easy, safe and effective in reducing theshoulder.
▸ Orthopaedic follow-up should be arranged for one ortwo weeks after the injury.
▸ Young athletes should undergo an arthroscopic exploration.
Additional educational resources
For doctors:▸ Shoulderdoc.co.uk—A website designed to provide
information for patients and medical professionals on allshoulder injuries. Information is available on moderntreatments, rehabilitation and expected surgical outcomes ofshoulder dislocation. No registration needed for access tothe site
▸ Review article—Cunningham N. Techniques for reduction ofanteroinferior shoulder dislocation. Emerg Med Australas2005;17:463–71For patients:
▸ Patient UK Information: www.patient.co.uk/doctor/Shoulder-Dislocation.htm Brief summary for patients’interested in the epidemiology, investigations, complicationand management of the condition
Dala-Ali B, et al. Br J Sports Med 2014;48:1209–1215. doi:10.1136/bjsports-2012-091300 7 of 8
Review
group.bmj.com on October 22, 2014 - Published by bjsm.bmj.comDownloaded from
22 Descamps MJL, Gwilym S, Weldon D, et al. Prospective audit of emergencydepartment transit times associated with entonox analgesia for reduction of theacute, traumatic dislocated shoulder. Accid Emerg Nurs 2007;15:223–7.
23 Uglow MG. Kocher’s painless reduction of anterior dislocation of the shoulder: aprospective randomised trial. Injury 1998;29:135–7.
24 Kahn JH, Mehta SD. The role of post-reduction radiographs after shoulderdislocation. J Emerg Med 2007;33:169–73.
25 Ng VK, Hames H, Millard WM. Use of intra-articular lidocaine as analgesia inanterior shoulder dislocation: a review and meta-analysis of the literature. Can JRural Med 2009;14:145–9.
26 Wakai A, O’Sullivan R, McCabe A. Intra-articular lignocaine versus intravenousanalgesia with or without sedation for manual reduction of acute anterior shoulderdislocation in adults. Cochrane Database Syst Rev 2011;4:CD004919.
27 Piper SL, Kramer JD, Kim HT, et al. Effects of local anesthetics on articular cartilage.Am J Sports Med 2011;39:2245–53.
28 Dragoo JL, Braun HJ, Kim HJ, et al. The in vitro chondrotoxicity of single-dose localanesthetics. Am J Sports Med 2012;40:794–9.
29 Hussein MK. Kocher’s method is 3000 years old. J Bone Joint Surg Br1968;50:669–71.
30 Kocher T. Eine neue reductionsmethode fur schultetrverrenkung. Berliner KlinWehnschr 1870;7:101–5.
31 Beattie TF, Steedman DJ, McGowan A, et al. A comparison of the Milch and Kochertechniques for acute anterior dislocation of the shoulder. Injury 1986;17:349–52.
32 Riebel GD, McCabe JB. Anterior shoulder dislocation: a review of reductiontechniques. Am J Emerg Med 1991;9:180–8.
33 Kirker Jr. Dislocation of the shoulder complicated by rupture of the axillary vessels.J Bone Joint Surg Br 1952;34-B:72–3.
34 Pimpalnerkar A, Datta A, Longhino D, et al. An unusual complication of Kocher’smanoeuvre. BMJ 2004;329:1472–3.
35 Liedelmeyer R. Letter to the editor: external rotation method of shoulder dislocationreduction. Ann Emerg Med 1981;10:228.
36 Milch H. Treatment of dislocation of the shoulder. Surg. 1938;3:732–40.37 Russell JA, Holmes EM III, Keller DJ, et al. Reduction of acute anterior shoulder
dislocations using the Milch technique: a study of ski injuries. J Trauma 1981;21:802–4.38 Janecki CJ, Shahcheragh GH. The forward elevation maneuver for reduction of
anterior dislocations of the shoulder. Clin Orthop Relat Res 1982;164:177–80.39 Ashton HR, Hassan Z. Best evidence topic report. Kocher’s or Milch’s technique for
reduction of anterior shoulder dislocations. Emerg Med J 2006;23:570–1.40 Cunningham NJ. A new drug free technique for reducing anterior shoulder
dislocations. Emerg Med 2003;15:521–4.41 Noordeen MH, Bacarese-Hamilton IH, Belham GJ, et al. Anterior dislocation of the
shoulder: a simple method of reduction. Injury 1992;23:479–80.42 Westin CD, Gill EA, Noyes ME, et al. Anterior shoulder dislocation. A simple and
rapid method for reduction. Am J Sports Med 1995;23:369–71.43 Mattick A, Wyatt JP. From Hippocrates to the Eskimo—a history of techniques used
to reduce anterior dislocation of the shoulder. J R Coll Surg Edinb2000;45:312–16.
44 Bosley R, Miles J. Scapular manipulation for reduction of anterior inferiordislocations. A new procedure. Presented at the American Association ofOrthopedics Surgeons. June 1979.
45 Sahin N, Ozturk A, Ozkan Y, et al. A comparison of the scapular manipulation andKocher’s technique for acute anterior dislocation of the shoulder. Eklem HastalikCerrahisi 2011;22:28–32.
46 Ugras AA, Mahirogullari M, Kural C, et al. Reduction of anterior shoulderdislocations by Spaso technique: clinical results. J Emerg Med 2008;34:383–7.
47 Poulsen SR. Reduction of acute shoulder dislocations using the Eskimo technique: astudy of 23 consecutive cases. J Trauma 1988;28:1382–3.
48 Manes HR. A new method of shoulder reduction in the elderly. Clin Orthop1980;147:200–2.
49 Sayegh FE, Kenanidis EI, Papavasiliou KA, et al. Reduction of acute anteriordislocations: a prospective randomized study comparing a new technique with theHippocratic and Kocher methods. J Bone Joint Surg Am 2009;91:2775–82.
50 Miller SL, Cleeman E, Auerbach J, et al. Comparison of intra-articular lidocaine andintravenous sedation for reduction of shoulder dislocations: a randomized,prospective study. J Bone Joint Surg Am 2002;84-A:2135–9.
51 Itoi E, Hatakeyama Y, Kido T, et al. A new method of immobilization after traumaticanterior dislocation of the shoulder: a preliminary study. J Shoulder Elbow Surg2003;12:413–15.
52 Kuhn JE. Treating the initial anterior shoulder dislocation—an evidence-basedmedicine approach. Sports Med Arthrosc 2006;14:192–8.
53 Siegler J, Proust J, Marcheix PS, et al. Is external rotation the correct immobilisationfor acute shoulder dislocation? An MRI study. Orthop Traumatol Surg Res2010;96:329–33.
54 Itoi E, Sashi R, Minagawa H, et al. Position of immobilization after dislocation ofthe glenohumeral joint. A study with use of magnetic resonance imaging. J BoneJoint Surg Am 2001;83-A:661–7.
55 Hart WJ, Kelly CP. Arthroscopic observation of capsulolabral reduction after shoulderdislocation. J Shoulder Elbow Surg 2005;14:134–7.
56 Miller BS, Sonnabend DH, Hatrick C, et al. Should acute anterior dislocations of theshoulder be immobilized in external rotation? A cadaveric study. J Shoulder ElbowSurg 2004;13:589–92.
57 Liavaag S, Stiris MG, Lindland ES, et al. Do Bankart lesions heal better in shouldersimmobilized in external rotation? Acta Orthop 2009;80:579–84.
58 Liavaag S, Brox JI, Pripp AH, et al. Immobilization in external rotation after primaryshoulder dislocation did not reduce the risk of recurrence: a randomized controlledtrial. J Bone Joint Surg Am 2011;93:897–904.
59 Handoll HH, Hanchard NC, Goodchild L, et al. Conservative management followingclosed reduction of traumatic anterior dislocation of the shoulder. CochraneDatabase Syst Rev 2006;1:CD004962.
60 Buss DD, Lynch GP, Meyer CP, et al. Nonoperative management forin-season athletes with anterior shoulder instability. Am J Sports Med 2004;32:1430–3.
61 Rowe CR. Prognosis in dislocations of the shoulder. J Bone Joint Surg Am1956;38-A:957–77.
62 Robinson CM, Howes J, Murdoch H, et al. Functional outcome and risk of recurrentinstability after primary traumatic anterior shoulder dislocation in young patients.J Bone Joint Surg Am 2006;88:2326–36.
63 Rhee YG, Cho NS, Cho SH. Traumatic anterior dislocation of the shoulder: factorsaffecting the progress of the traumatic anterior dislocation. Clin Orthop Surg.2009;1:188–93.
64 Mclaughlin HL, Cavallaro WU. Primary anterior dislocation of the shoulder. Am JSurg 1950;80:615–21.
65 te Slaa RL, Brand R, Marti RK. A prospective arthroscopic study of acute first-timeanterior shoulder dislocation in the young: a five-year follow-up study. J ShoulderElbow Surg 2003;12:529–34.
66 Sachs RA, Lin D, Stone ML, et al. Can the need for future surgery for acutetraumatic anterior shoulder dislocation be predicted? J Bone Joint Surg Am2007;89:1665–74.
67 Handoll HH, Almaiyah MA, Rangan A. Surgical versus non-surgical treatment foracute anterior shoulder dislocation. Cochrane Database Syst Rev 2004;1:CD004325.
68 Bottoni CR, Wilckens JH, DeBerardino TM, et al. A prospective, randomizedevaluation of arthroscopic stabilization versus nonoperative treatment in patientswith acute, traumatic, first-time shoulder dislocations. Am J Sports Med2002;30:576–80.
69 Kirkley A, Werstine R, Ratjek A, et al. Prospective randomized clinical trialcomparing the effectiveness of immediate arthroscopic stabilization versusimmobilization and rehabilitation in first traumatic anterior dislocations of theshoulder: long-term evaluation. Arthroscopy 2005;21:55–63.
70 Jakobsen BW, Johannsen HV, Suder P, et al. Primary repair versus conservativetreatment of first-time traumatic anterior dislocation of the shoulder: a randomizedstudy with 10-year follow-up. Arthroscopy 2007;23:118–23.
71 Turkel SJ, Panio MW, Marshall JL, et al. Stabilizing mechanisms preventinganterior dislocation of the glenohumeral joint. J Bone Joint Surg Am 1981;63:1208–17.
72 McRae R. Practical fracture treatment. 5th edn. London: Churchill Livingstone,2008:128–9.
73 Fulde GWO. Emergency medicine: the principles of practice. 5th ed. ChurchillLivingstone: Elsevier, 2009:257–8.
74 Wyatt JP, Illingworth RN, Graham CA, et al. Oxford handbook of emergencymedicine. 3rd edn. Oxford: Oxford University Press, 2006:452–3.
75 Wardrope J, English B. Musculo-skeletal problems in emergency medicine. Oxford:Oxford University Press, 1998:102–4.
76 Marx J, Hockberger R, Walls R. Rosen’s emergency medicine: concepts and clinicalpractice. US: Mosby, 2009:579–82.
77 McRae R. Pocketbook of orthopaedic and fractures. 2nd edn. London: ChurchillLivingstone, 2006.
8 of 8 Dala-Ali B, et al. Br J Sports Med 2014;48:1209–1215. doi:10.1136/bjsports-2012-091300
Review
group.bmj.com on October 22, 2014 - Published by bjsm.bmj.comDownloaded from
doi: 10.1136/bjsports-2012-0913002012
2014 48: 1209-1215 originally published online July 21,Br J Sports Med Benan Dala-Ali, Marta Penna, Jamie McConnell, et al. dislocationManagement of acute anterior shoulder
http://bjsm.bmj.com/content/48/16/1209.full.htmlUpdated information and services can be found at:
These include:
References http://bjsm.bmj.com/content/48/16/1209.full.html#ref-list-1
This article cites 70 articles, 17 of which can be accessed free at:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
CollectionsTopic
(749 articles)Trauma (831 articles)Injury
Articles on similar topics can be found in the following collections
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on October 22, 2014 - Published by bjsm.bmj.comDownloaded from