malabsorption dr. wm simmonds internal medicine (gastroenterology) 15 august 2011
TRANSCRIPT

MALABSORPTION
Dr. WM SimmondsInternal Medicine
(Gastroenterology)
15 August 2011

Aims
Define malabsorption and discuss various causes.
Briefly discuss celiac disease. Discuss chronic pancreatitis.

Malabsorption
A state arising from abnormality in absorption of single or multiple nutrients across the gastrointestinal (GI) tract.
Abnormalities in 3 necessary processes Intraluminal MALDIGESTION
– Bile or pancreatic enzyme deficiency whereby fat and protein malabsorption results.
Mucosal MALABSORPTION– Small bowel resection or small bowel epithelial damage causing a
diminished absorptive surface area and brush border enzyme activity.
Post-mucosal lymphatic system obstruction– Prevents uptake and transport of nutrients
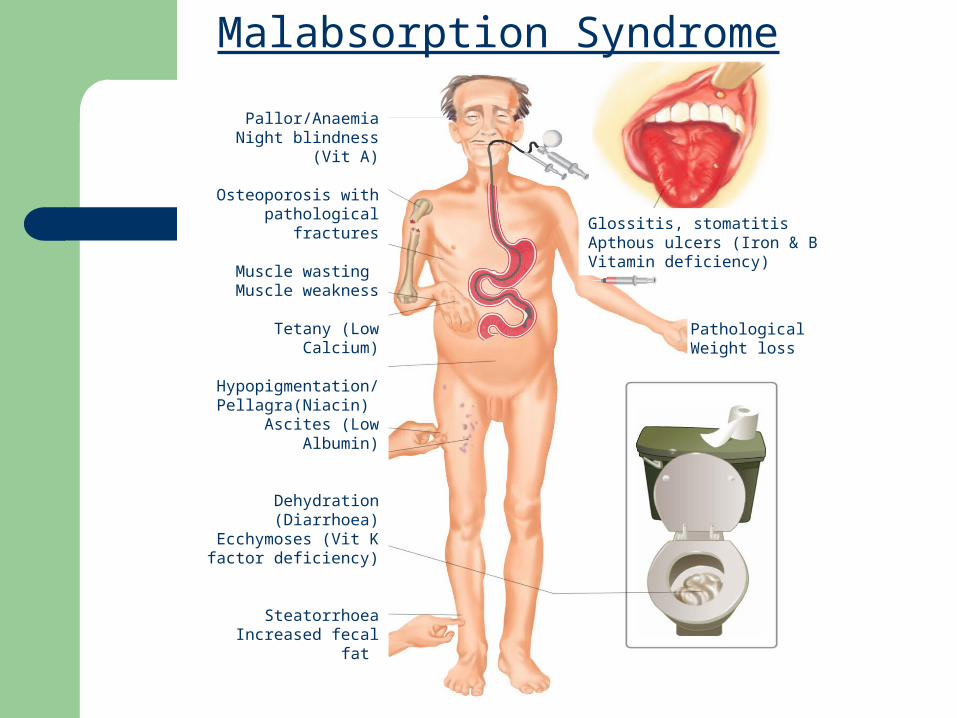
Malabsorption Syndrome
Pallor/AnaemiaNight blindness (Vit A)
Osteoporosis withpathological fractures
Muscle wasting Muscle weakness
Tetany (Low Calcium)
Hypopigmentation/Pellagra(Niacin)
Ascites (Low Albumin)
Dehydration (Diarrhoea)Ecchymoses (Vit K
factor deficiency)
SteatorrhoeaIncreased fecal fat
Oedema (Low Albumin)Peripheral neuropathy
(B12 def)
Glossitis, stomatitisApthous ulcers (Iron & BVitamin deficiency)
Pathological Weight loss
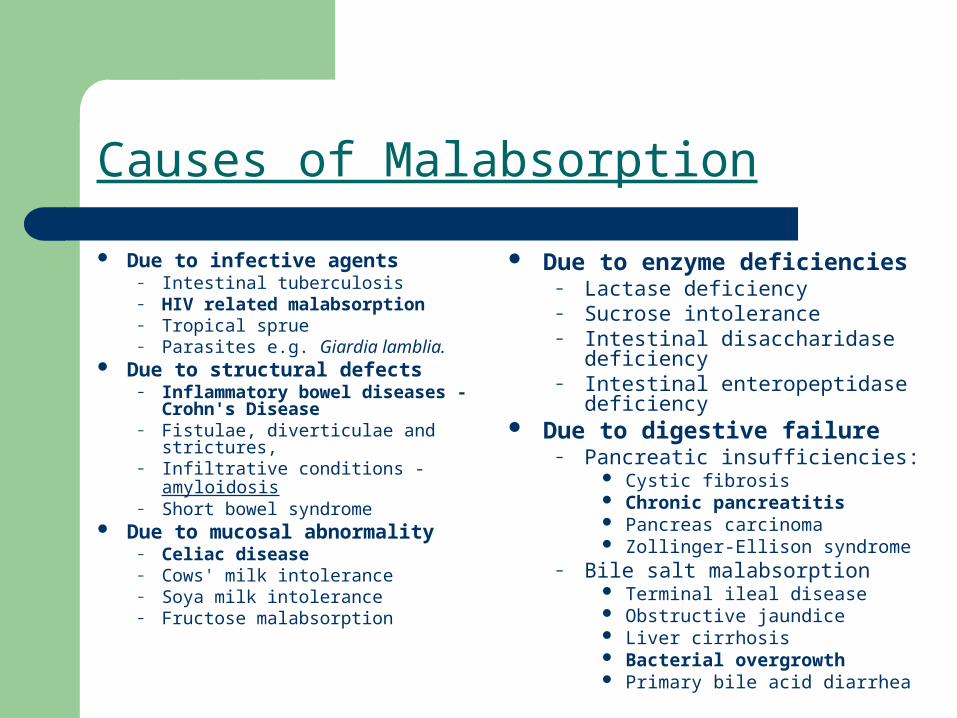
Causes of Malabsorption
Due to infective agents – Intestinal tuberculosis – HIV related malabsorption – Tropical sprue – Parasites e.g. Giardia lamblia.
Due to structural defects– Inflammatory bowel diseases -
Crohn's Disease – Fistulae, diverticulae and
strictures, – Infiltrative conditions - amyloidosis– Short bowel syndrome
Due to mucosal abnormality– Celiac disease – Cows' milk intolerance – Soya milk intolerance – Fructose malabsorption
Due to enzyme deficiencies– Lactase deficiency– Sucrose intolerance – Intestinal disaccharidase deficiency – Intestinal enteropeptidase
deficiency Due to digestive failure
– Pancreatic insufficiencies: Cystic fibrosis Chronic pancreatitis Pancreas carcinoma Zollinger-Ellison syndrome
– Bile salt malabsorption Terminal ileal disease Obstructive jaundice Liver cirrhosis Bacterial overgrowth Primary bile acid diarrhea
Celiac disease
Gluten-sensitive enteropathy More common in caucasian populations
(1:300 in European countries) Rare in black populations HLA DQ2 and DQ8 Can present at any age Classically - fatigue, weight loss and
anaemia in a young to middle aged female.

Celiac disease
Celiac disease
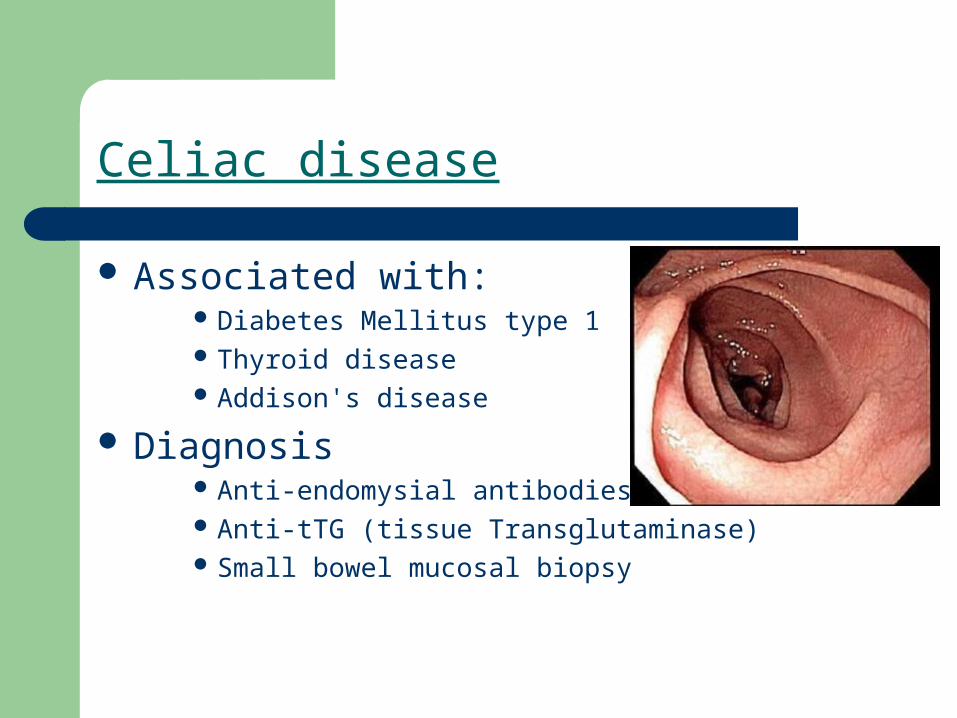
Associated with: Diabetes Mellitus type 1 Thyroid disease Addison's disease
Diagnosis Anti-endomysial antibodies Anti-tTG (tissue Transglutaminase) Small bowel mucosal biopsy
Celiac disease
Treatment– Strict Gluten free diet. Dietary advice.– Supplementation (FeSo4, Vitamins)– Exclude other related autoimmune conditions.– Follow up using clinical parameters as well as
antibodies.

Chronic Pancreatitis

Chronic PancreatitisDefinition
Permanent and irreversible damage to the pancreas
Histological or radiological evidence of chronic inflammation and fibrosis
Destruction of exocrine (acinar cell) and endocrine (islets of Langerhans) pancreatic tissue
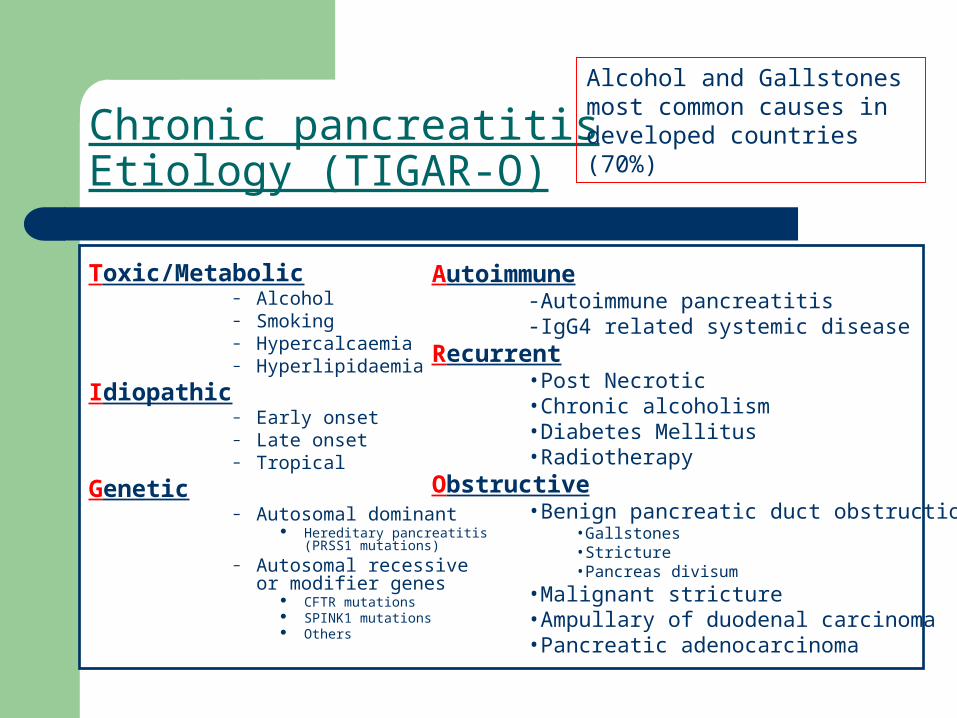
Chronic pancreatitisEtiology (TIGAR-O)
Toxic/Metabolic– Alcohol– Smoking– Hypercalcaemia– Hyperlipidaemia
Idiopathic– Early onset– Late onset– Tropical
Genetic– Autosomal dominant
Hereditary pancreatitis (PRSS1 mutations)
– Autosomal recessive or modifier genes
CFTR mutations SPINK1 mutations Others
Alcohol and Gallstones most common causes in developed countries (70%)
Autoimmune-Autoimmune pancreatitis-IgG4 related systemic disease
Recurrent•Post Necrotic•Chronic alcoholism•Diabetes Mellitus•Radiotherapy
Obstructive•Benign pancreatic duct obstruction
•Gallstones•Stricture•Pancreas divisum
•Malignant stricture•Ampullary of duodenal carcinoma•Pancreatic adenocarcinoma

Gallstones
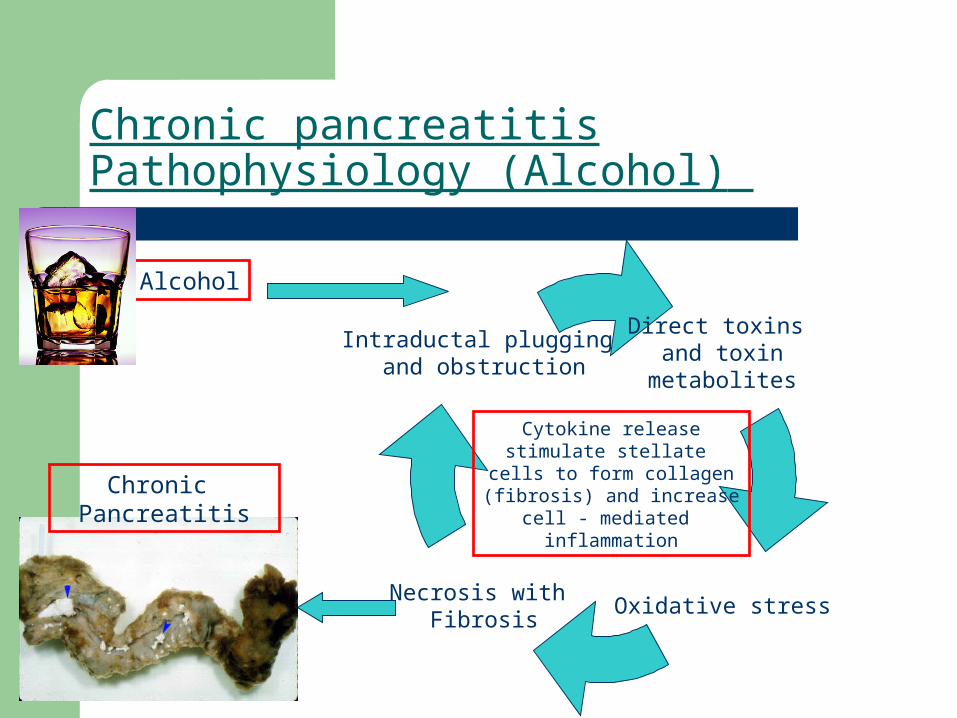
Chronic pancreatitisPathophysiology (Alcohol)
Direct toxins and toxin
metabolites
Necrosis with Fibrosis
Intraductal plugging and obstruction
Oxidative stress
Alcohol
Cytokine releasestimulate stellate
cells to form collagen(fibrosis) and increase
cell - mediated inflammation
Chronic Pancreatitis

Jaster, Molecular Cancer. 2004 3:26 doi:10.1186/1476-4598-3-2

Chronic PancreatitisClinical features
Chronic PancreatitisClinical features
Abdominal pain

Chronic PancreatitisClinical features
Abdominal pain
Diabetes Mellitus

Chronic PancreatitisClinical features
Abdominal pain
SteatorrhoeaDiabetes Mellitus
Chronic PancreatitisClinical features
Abdominal pain
SteatorrhoeaDiabetes Mellitus
Other:- Constitutional symptoms, malaise etc- Weight loss due to malabsorption- Pain associated with meals with high protein and fat content
Chronic PancreatitisAbdominal pain
Most common clinical problem Decreases appetite and limits food
consumption - weight loss and malnutrition Dramatic reduction in quality of life Character:
– Epigastric, often with radiation to the back. – Boring, deep, and penetrating and is often – Associated with nausea and vomiting.– Relieved by sitting forward or leaning forward, the
knee-chest position– Worsens after a meal and often is nocturnal.
Possible causes:– Acute inflammation/noxious stimuli– Increased intra-pancreatic pressure and ischaemia– Neuropathic (Alterations in nociceptive nerves) – Other

Chronic pancreatitisSteatorrhoea
Exocrine insufficiency. Passage of bulky, floating, foul-smelling
stools or may even note the passage of frank oil droplets.
Occurs when pancreatic lipase secretion is reduced to less than 10% of the maximum output.
A feature of far-advanced chronic pancreatitis or complete blockage of the pancreatic duct.

Chronic PancreatitisDiabetes Mellitus
Endocrine insufficiency Half of patients with chronic
pancreatitis who develop diabetes will require insulin.
Insulin-producing beta cells and glucagon-producing alpha cells are injured.
Increased risk of prolonged and severe hypoglycemia with over vigorous insulin treatment due to the lack of a compensatory release of glucagon.

Chronic pancreatitisDiagnosis(1)
Clinical features (Abdominal pain, Steatorrhoea, Diabetes Mellitus)
Test of pancreatic function– Direct Tests
Direct hormonal stimulation tests are believed to be the most sensitive function test for chronic pancreatitis. Bicarbonate estimation after Secretin administration. (ERCP) – invasive, not routinely done.
– Indirect Tests Serum Trypsinogen Pancreatic Enzymes in Stool eg chymotrypsin or elastase Fecal Fat Excretion/Steatocrit

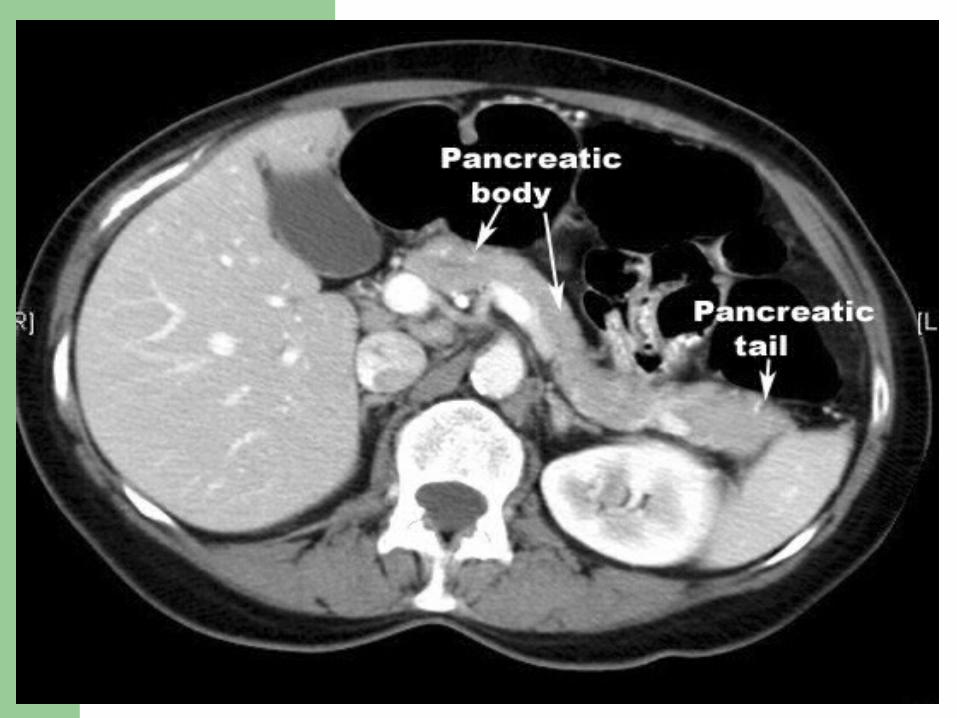
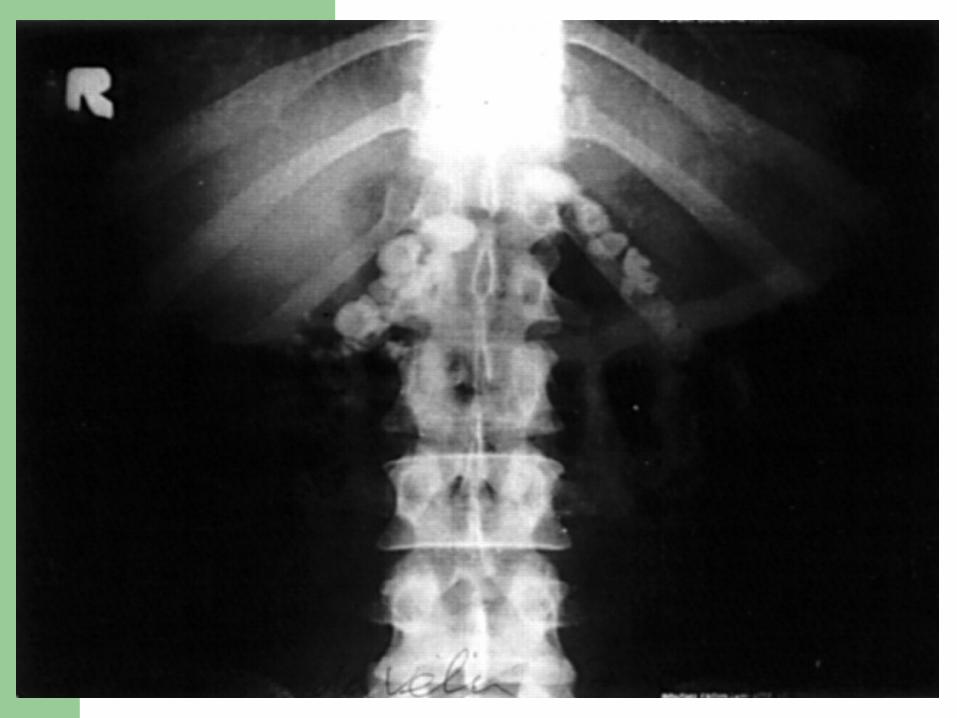
Chronic pancreatitisDiagnosis(2)
Tests of pancreatic structure– Abdominal xray with pancreas calcifications– CT Scan/MRI– Ultrasound (Conventional/EUS)– ERCP/MRCP
Other – IgG4, ESR, RF, Calcium, Triglyceride levels



Chronic pancreatitisTreatment
No curative therapy available Treatment of the cause Stop smoking. Stop alcohol. Abdominal pain
Analgesics (Paracetamol, NSAIDs, Opiates) Decrease intra-pancreatic pressure by oral pancreatic enzyme supplementation (eg. Creon) Surgery (Endoscopic or Open surgery)
Steatorrhoea Dietary fat restriction (<20g/day) Pancreatic enzyme supplementation (eg. Pancrelipase - CreonTM) PPI to increase duodenal pH for optimal pancreatic enzyme activity
Diabetes Mellitus Carbohydrate restriction Insulin therapy (NB. Be wary of risk of hypoglycaemia)
Other Supplemenation of fat soluble vitamins (A, D, E, K)

Chronic pancreatitisComplications
Pseudocysts Bleeding Obstruction Pancreatic Fistulae
– Follows seudocyst– External (surgery)– Internal (Ascites, pleural effusion)
Malignancy– Risk highest with hereditary pancreatitis
and smoking– Pancreatic adenocarcinoma – CA19-9
Dysmotility– Gastroparesis and antroduodenal dysmotility
perigastric inflammation hormonal changes associated with chronic pancreatitis (e.g. CCK) side effect of narcotic analgesics.
Thank you.