make it your business: comprehensive tobacco control · in primary care arrange clinic clinic...
TRANSCRIPT

Make it Your Business: Comprehensive Tobacco Control
Charles J. Bentz, MD, FACPMedical Director: Tobacco Cessation and Prevention
Providence Health & Services: Oregon

Providence Health & Services
$ 465,736Charity care and community benefits (in thousands)
188St. Thomas Child & Family Centers (number licensed to serve)
549Providence High School (students)
780University of Great Falls (students)
233,392Health Plan members
369,210Housing and assisted living days
4,748,523Acute outpatient visits
1,293,846Primary care visits
988,009Home health visits / hospice days
626,626Long term care patient days
247,832Acute admissions
46,040Number of employees
27Number of facilities (acute care)

Making It Your Business
• Why business should address tobacco• What works in treating tobacco dependence• Define comprehensive tobacco control• Examples of systems that address tobacco• Implications for business


Costs of Smoking
• Business Costs: – Greater absenteeism– Time spent on smoking rituals– Higher health care costs– Higher life insurance premiums– Higher risk of occupational injury– Higher disability costs– More disciplinary actions
Direct vs. Indirect Costs• Direct Cost: $1600 each year per smoker
– 50% increase in utilization of health services– 19% of health care expenses for employees’ children is
related to second-hand smoke– Double rate of on-the-job accidents
• Indirect Cost: $1700 each year per smoker– Absent an average of 6.5 days more per year – 8% of time in smoking-related activities
• Total Cost: $3300 each year per smoker
Source: Centers for Disease Control and Prevention, Atlanta

Quitting saves lives…•Study of 34,439 male British doctors•Smokers died 10 years younger•Cessation improved life expectancy
Doll R. et al. Mortality in relation to smoking: 50 years‘ observations on male British doctors BMJ, doi:10.1136/bmj.38142.554479.AE (June 2004)
2606509401030
Years gainedAge quit

High Benefit in High Risk
• Randomized clinical trail of intensive cessation• CCU patients Creighton University
– Improved quit rates – Fewer hospitalizations (NNT of 6) – Lower mortality (NNT of 11)
• Several aspects deserve comment– Systematic identification of smokers– Intensive outpatient counseling– Low barrier to medication (free)– Multiple opportunities for re-treatment
Mohiuddin SM, et al. Chest 2007;131:446-452

Adding Mortality-Related Lost Productivity to the Estimate Raises the Total Cost to
$5,606 per smoker per year
$341
$1,882$1,623
$1,760
Smoking Breaks Mortality-Related Lost ProductivityExcess Medical Expenditures Missed Work Days Due to Sickness
Sources: Mercer Human Resource Consulting / Smoking Cessation Leadership Center
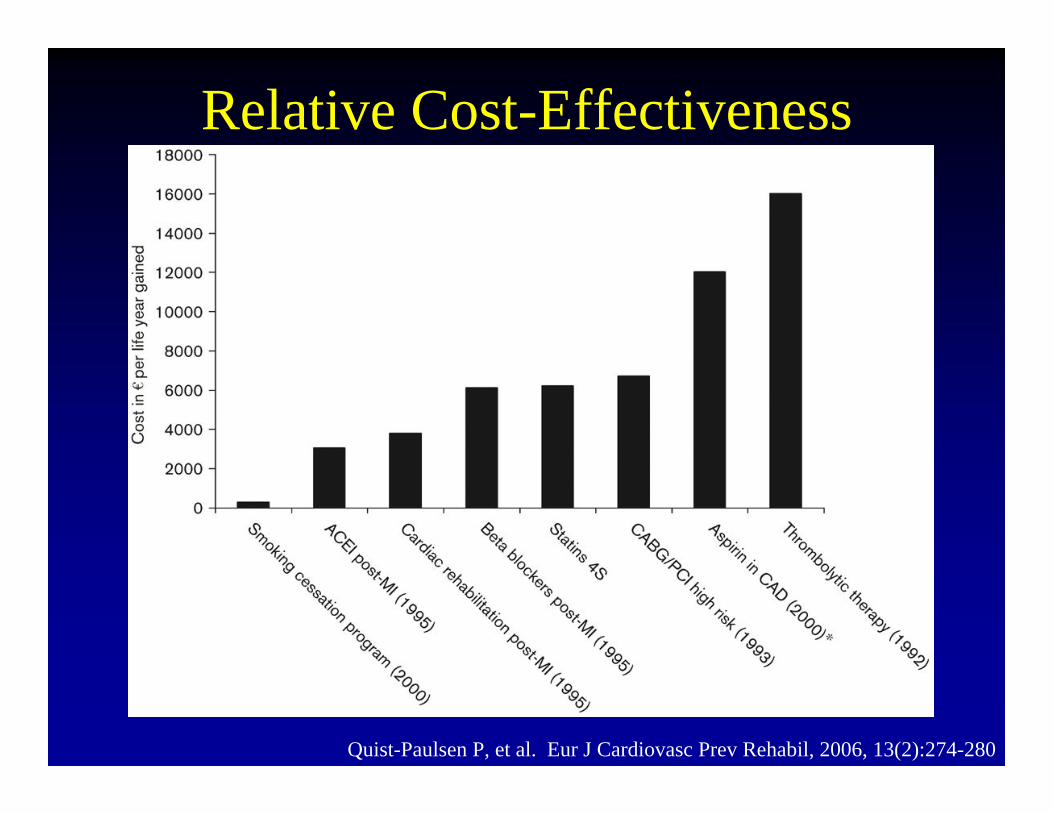
Relative Cost-Effectiveness
Quist-Paulsen P, et al. Eur J Cardiovasc Prev Rehabil, 2006, 13(2):274-280

Cost of workplace tobacco dependence
$ 1,000,000
$ 2,000,000
$ 3,000,000
$ 4,000,000
$ 5,000,000
$ 6,000,000
$ 7,000,000
1,000 2,000 3,000 4,000 5,000 6,000
Blue collar (3
6%)
White collar (15%)Mixed workforce (26%)
Source: Mercer Human Resources Consulting, New York, NY
Number of employees
Return on Investment: ROI• COST:
– comprehensive tobacco benefit: – $1.20 to $4.80 per employee
• Direct ROI:– Three years: Break-even– Five years: Positive cost benefit – Exceptions: (Pregnancy and High Risk employees)
• Indirect ROI:– Demonstrate commitment to employee health– Improve employee healthy lifestyle choices– Provide tools to support consumerism strategy
Sources: Mercer (NY) / Smoking Cessation Leadership Center (UCSF)Center for Disease Control and Prevention (Atlanta)

It is Very Hard to Quit
Actor Bill Talman of TV's Perry Mason, died of lung cancer at the age of 53, shortly after this anti-smoking advertisement in 1968.
His widow, Peggy Talman died from lung cancer at the age of 73 in 2002 in a Providence Hospital, after years of continued smoking.

Neurobiology of Nicotine Addiction
• Nicotine binds to receptors in the brain
• This cause release of a neurotransmitter: dopamine
• Reward: “Pleasure Center”• Long term exposure creates
more receptors• Withdrawal of nicotine
causes symptoms which can last for several weeks.
Coe JW et al. SRNT. 2005. Prague, Czech RepublicPicciotto MR et al. Nicotine Tob Res. 1999; Suppl 2:S121-125.
Paifai:Drugs in Human Behavior, 2nd ed. Landry, Sci Am, 1997:42-45
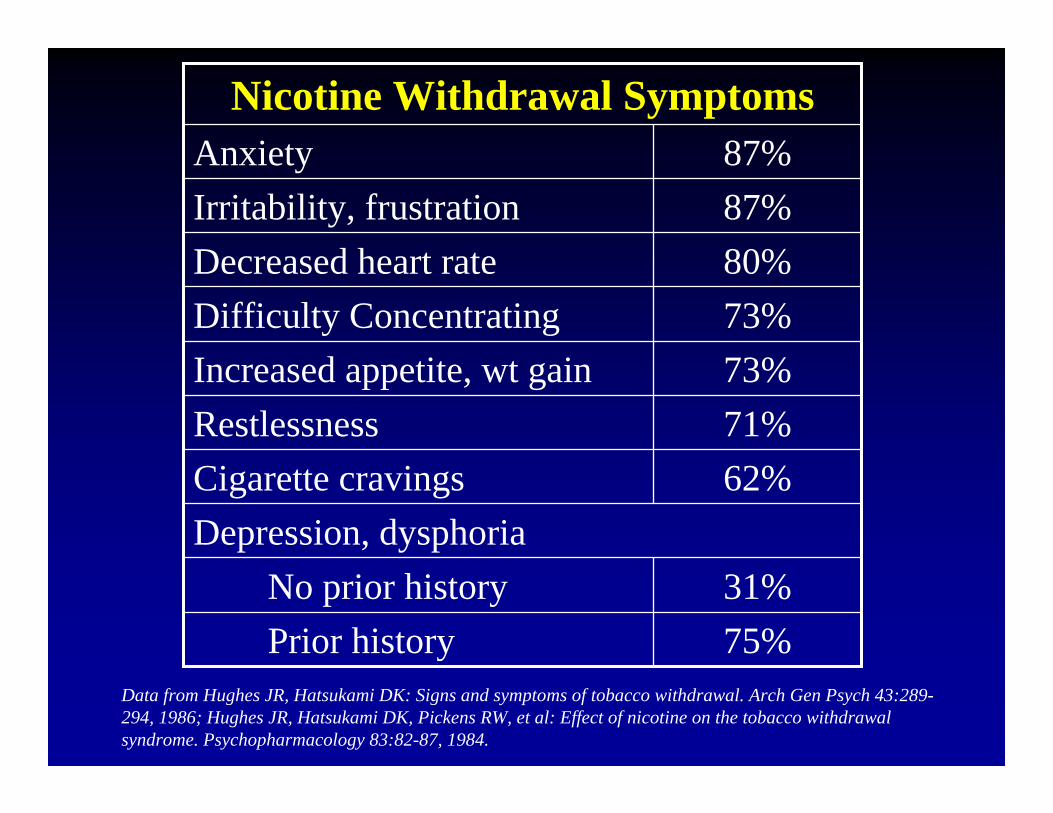
Nicotine Withdrawal Symptoms
75%Prior history31%No prior history
Depression, dysphoria62%Cigarette cravings71%Restlessness73%Increased appetite, wt gain73%Difficulty Concentrating80%Decreased heart rate87%Irritability, frustration87%Anxiety
Data from Hughes JR, Hatsukami DK: Signs and symptoms of tobacco withdrawal. Arch Gen Psych 43:289-294, 1986; Hughes JR, Hatsukami DK, Pickens RW, et al: Effect of nicotine on the tobacco withdrawal syndrome. Psychopharmacology 83:82-87, 1984.
Medications Can Help….• First Line Medications:
– Nicotine Replacement Therapy (5 forms)– Bupropion SR (anti-depressant)– Varenicline (Chantix™) (new: affects nicotine receptor)
• Second Line Medications:– Nortriptyline (anti-depressant)– Clonidine (anti-hypertensive)
• Near Future:– Rimonabant (cannabinoid receptor)– Vaccine (antibody to nicotine)

BUT THEY DON’T WORK ALONE
• Medications can double the quit rates• Work best when used in the setting of a
behavioral modification program• Most smokers have to unlearn smoking• It takes practice to become a non-smoker• Social support really works

Medication with and without counseling
Behavioral Therapy StatusMedication Status
5%
10%
MinimalTherapy*
15%10%No Medication
30%20%Medication
Intense Therapy*
Brief Therapy*
Hughes JR. CA Cancer J Clin. 2000;50:143-151Fiore MC et al. U.S. DHHS, U.S. Public Health Service, 2000Hornbrook MC, et al. ATMC 2000
*Data from NRT and bupropion trials

Medication vs. Behavior
* Behavioral change for triggers, stressors, coping mechanisms, habit patterns, etc…

What is Success?• Spontaneous Quit Rates 2-3% quit @ 1 year • Office-based (dose-response)
– Minimal Counseling: 4%– Brief Counseling: 5%– Counseling: 8-10%
• Interactive internet 5-10%• Interactive telephone 10-25%• Group classes 15-25%• Classes with medication 25-35%• Inpatient residential 45-50%
Public Health Service Guideline 2000, Hughes et al, CA cancer journal clinic, 2000 50:143, Providence Tobacco Cessation & Prevention Program, Mayo Clinic Residential Cessation Program

How do we do a better job….
…treating tobacco use and dependence?

It takes a clearly identified goal…“At every point where patients
come into contact with our health system, tobacco use will be assessed and addressed.”
Providence Tobacco Task Force, 1994
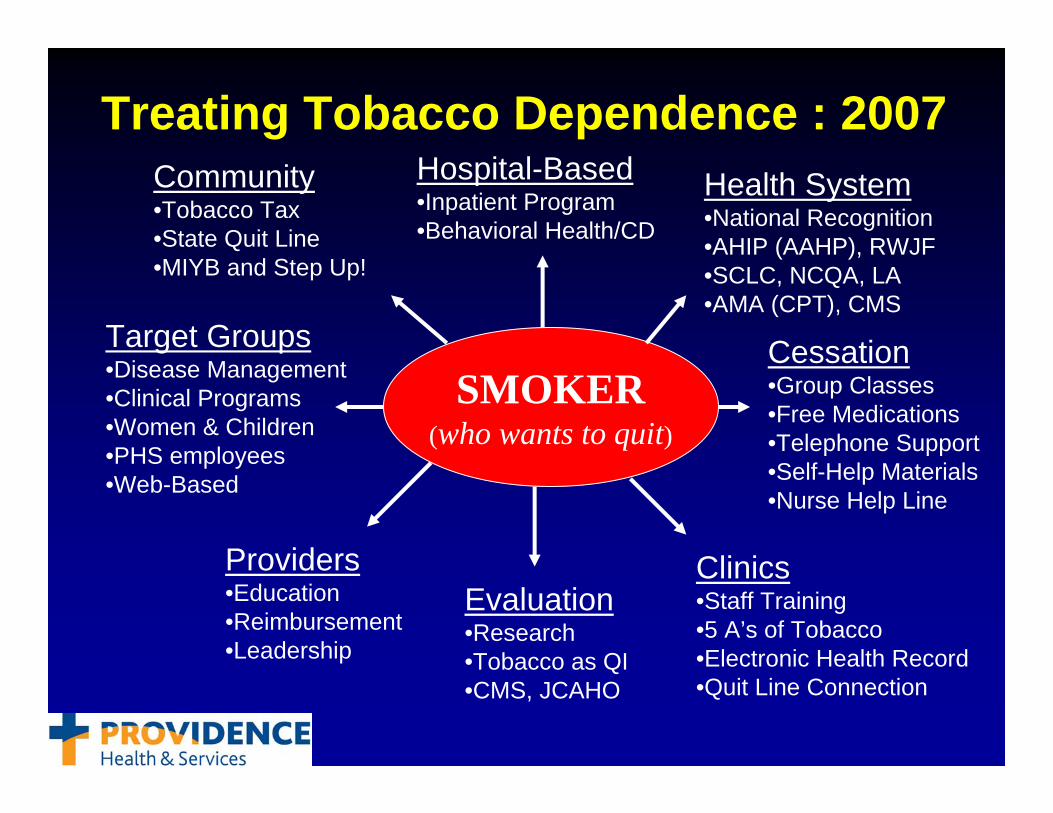
Treating Tobacco Dependence : 2007
Providers•Education•Reimbursement •Leadership
Cessation•Group Classes•Free Medications•Telephone Support•Self-Help Materials•Nurse Help Line
Clinics•Staff Training•5 A’s of Tobacco •Electronic Health Record•Quit Line Connection
Health System•National Recognition•AHIP (AAHP), RWJF•SCLC, NCQA, LA•AMA (CPT), CMS
Target Groups•Disease Management•Clinical Programs•Women & Children•PHS employees•Web-Based
Community•Tobacco Tax•State Quit Line•MIYB and Step Up!
Hospital-Based•Inpatient Program•Behavioral Health/CD
Evaluation•Research•Tobacco as QI•CMS, JCAHO
SMOKER(who wants to quit)
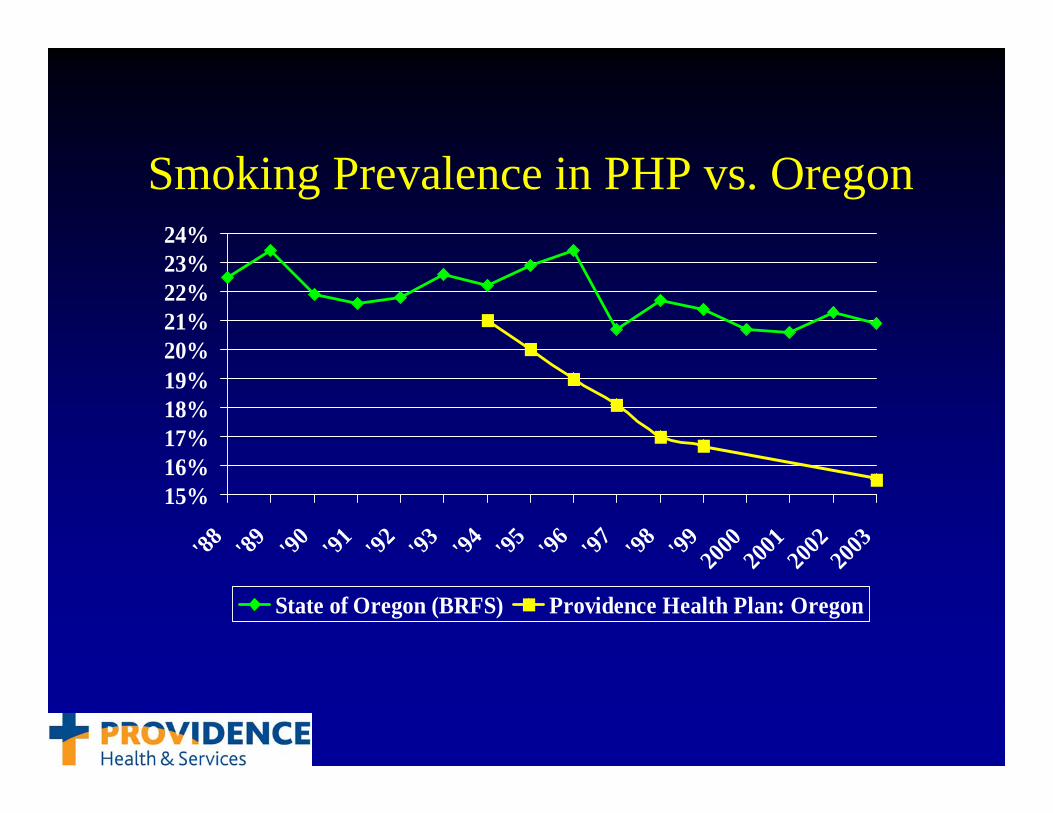
Smoking Prevalence in PHP vs. Oregon
15%16%17%18%19%20%21%22%23%24%
'88 '89 '90 '91 '92 '93 '94 '95 '96 '97 '98 '99 2000
2001
2002
2003
State of Oregon (BRFS) Providence Health Plan: Oregon
“The program at Providence is the platinum standard for
tobacco cessation in health systems”
Steve Schroeder MDChair and CEO of Robert Wood Johnson Foundation (90-02)
Distinguished Professor of Health and Health Care Division of General Internal Medicine, UCSF
Director: Smoking Cessation Leadership CenterSeptember 24, 2004

Resource: Tobacco Quit Lines• Talk to an intake person (informational)• Most have referral to trained counselors
– Develop a customized quit plan– Information about medications – Information / referral to cessation services– A tailored “Quit Kit” is mailed– Proactive Calls to the smoker (one to five)
• 14.8% one-year quit rates (Tobacco Control 2003;12:45-51)

ASKASKADVISEADVISE
Two Options for Two Options for Connection with Connection with
QuitlineQuitline
Diagram of “Quit Line Connection”in Primary Care
ARRANGEARRANGE
ClinicClinic
ClinicClinic
Patient completes Form. Form faxed to Quit Line. Quit Line contacts patient.
After initial smoking cessationintervention, QuitLine staff refer patients to appropriate resources
and return fax form to clinic
PatientPatient
Oregon Quit LineOregon Quit Line
Brochure givenPatient contacts quitline
at their convenience.
PatientPatient
Tobacco Use Documented in
Chart Advice to quit and Stage of readiness to quit Documented in ChartProvider refers to Quit Line
ASSESSASSESS
ASSISTASSIST
Free & ClearFree & Clearoror
Local ProgramsLocal Programs
ProgramProgram
Bentz CJ, et al. American Journal of Preventive Medicine,2006. 30(1): 31-37.

Resource: Pharmacist-Assisted Cessation Classes
• Counselor lead, 11-sessions over 8-weeks• Patients can self-refer• Medications at no out-of-pocket expense• Pharmacist leads first class, remains available
– Pharmacist dispenses medication– Only 2 week supply at a time– Nicotine Replacement, Bupropion, or
Varenicline• Single $15 copay for everything• Onsite at each hospital• Worksite classes offered• 33-35% 1-year quit rates• “How to” Syllabus available fall 2007

Resource: Hospitals
• STEP UP! a collaborative effort to promote– Cessation benefits for all hospital employees– Intensive intervention for all patients – Pharmacist-assisted cessation classes – Hospital tobacco-free campus policies– Hospital efforts to “step up” and lead local
businesses to curb tobacco use
Oregon Tobacco Prevention & Education Program, Oregon Association of Hospitals & Health Systems, Acumentra Health, Oregon Nurses Association, Make It Your Business, Smoking Cessation Leadership Center, many hospitals, health systems, and professional associations in Oregon
Definition: Comprehensive Tobacco Control
• All patients have tobacco use status documented • All tobacco users receive brief provider advice to quit• All smokers have access to intensive counseling and medication • All smokers have coverage for tobacco cessation services• All smokers are aware of their tobacco cessation benefit• Health System cessation intervention is a quality measure• Health System Quality Assurance sets goals, monitors
interventions, and provides feedback to frontline staff• Health System policies, training, and financial incentives support
the delivery of quality cessation efforts

• Evaluate and utilize resources– Programs available from your medical or dental carriers– Investigate Quit Line Connection (1-800-QUIT NOW)– Review the ‘Make It Your Business’ Employer’s Toolkit
• Cover effective tobacco cessation– Cover a range of options (medication & counseling)– Waive fees, co-pays, and other barriers– Opportunity for re-treatment (no benefit limits)– Offer to employee spouses and dependents
How do we get there from here?
• Tobacco-Free Worksite Policy• Understand legal implications
– Local smoke-free ordinances– No legal ground for the claim that smoking is “a right”– Secondhand smoke is classified a group-A carcinogen– HIPAA non-discrimination rules apply to smoking– Any cash incentive reward is taxable to employee– Understand premium differentials (DOL website)
How do we get there from here?

• Communicate (Promote it!)– Clearly state benefits that are offered– Use consistent messaging – Use multiple modes:
• Face-to-face during organizational meetings (if possible)• Memos mailed to employee’s home written by CEO• E-mails at work, inserts in pay envelopes• Posters and flyers advertising the program• HR/manager education and training• Inserts in open-enrollment communications
How do we get there from here?

• Incentives?– Average life insurance premium differential $10 - $30 /month– Up to $500/year in benefit credits for people who meet goals– Discounted life insurance premiums for nonsmokers– Nonsmokers receive a $100 credit toward insurance premiums– $50 for pledging to avoid tobacco, misuse alcohol, or drugs– People who quit smoking get $600 in cash over 18 months– Health System Incentives
How do we get there from here?

Conclusions:
• There is return on investment (ROI)• Most employees do not have access or
coverage for effective tobacco cessation• Employers need to cover cessation• Employers need to promote cessation• Collaborate with Health Systems• Make It Your Business to have a
Tobacco-free Workplace

Employer Resources
Dr. Steven Schroeder: [email protected]
http://smokingcessationleadership.ucsf.edu
Dawn Robbins: [email protected]://www.makeityourbusiness.net
http://www.businesscaseroi.org
Charles J. Bentz MD, FACP [email protected] Tobacco in Healthcare Systems, Connecting to state-level Quit Lines, Pharmacist-assisted cessation classes
http://1800quitnow.cancer.gov