major illness and dementia. precipitating factors of...
TRANSCRIPT
Dr Maria Mylona MD, PhDSenior Resident of Internal Medicine
1st Department of Propaedeutic & Internal Medicine, Laiko General Hospital, AthensUniversity Medical School, Athens, Greece
Major illness and dementia.Precipitating factors of delirium in hospitalized
patients.

MAJOR ILLNESS ANDDEMENTIA
PNEUMONIA ARDS SEPSIS ICU COGNITIVE DECLINE
MAJOR ILLNESS ANDDEMENTIA
PNEUMONIA

PNEUMONIA ANDDEMENTIA
Pneumonia is common among patients with advanceddementia, especially toward the end of life.
Whether antimicrobial treatment improves survival orcomfort is not well understood.
The effect of antimicrobial treatment for suspectedpneumonia on survival and comfort in patients withadvanced dementia has been examined.
Survival and Comfort After Treatment of Pneumonia in Advanced Dementia/Arch Intern Med. 2010 Jul 12;170(13): 1102–1107.
Long-term Cognitive Impairment and Functional DisabilityAmong Survivors of Severe Sepsis
Theodore J. Iwashyna, M2010;304(16):D, PhD; E. Wesley Ely, MD, MPH; Dylan M. Smith, PhD; Kenneth M. Langa,MD, PhD /JAMA. 1787-1794. doi:10.1001/jama.2010.1553
From 2003 to 2009, data were prospectively collected from 323nursing home residents with advanced dementia in 22 facilities inthe area of Boston, Massachusetts.
Participants were from the Choices, Attitudes, and Strategies forCare of Advanced Dementia at the End-of-Life (CASCADE) study; aprospective cohort study of NH residents with advanced dementiaand their health care proxies (HCPs).
Each resident was followed up for as long as 18 months or untildeath.
All suspected pneumonia episodes were ascertained, andantimicrobial treatment for each episode was categorized as none,oral only, intramuscular only, or intravenous (or hospitalization.
PNEUMONIA AND DEMENTIA (1)
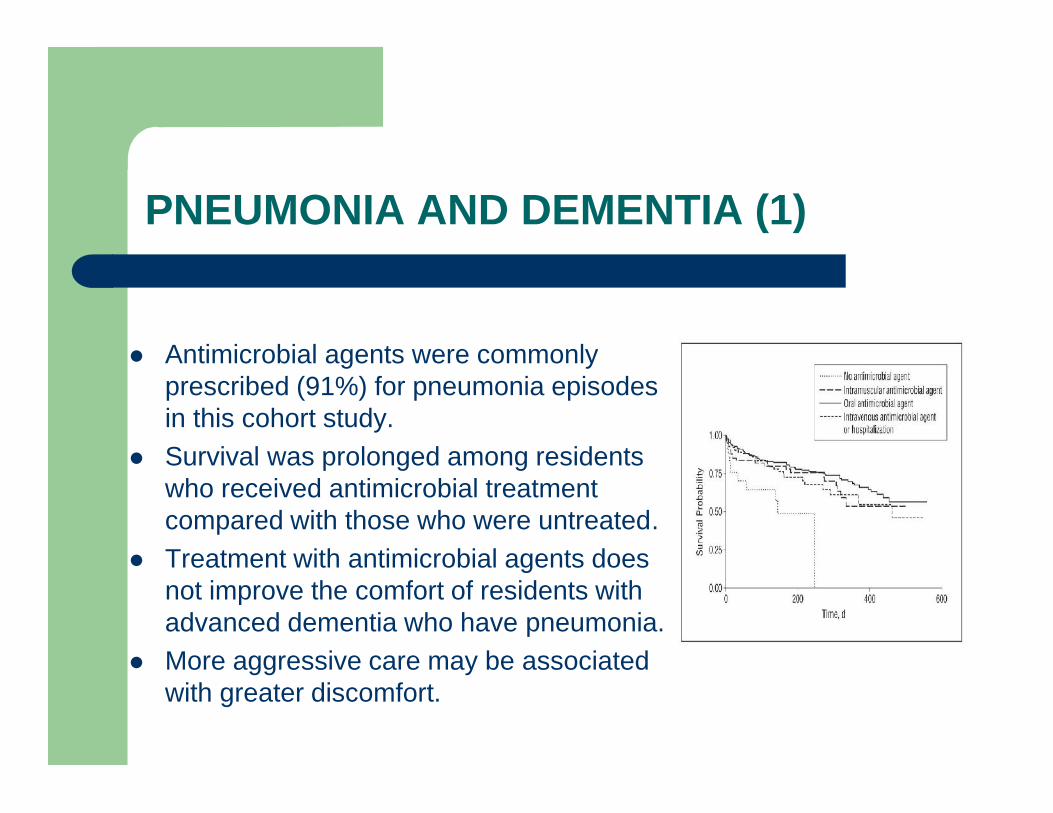
Antimicrobial agents were commonlyprescribed (91%) for pneumonia episodesin this cohort study.
Survival was prolonged among residentswho received antimicrobial treatmentcompared with those who were untreated.
Treatment with antimicrobial agents doesnot improve the comfort of residents withadvanced dementia who have pneumonia.
More aggressive care may be associatedwith greater discomfort.

PNEUMONIA ANDDEMENTIA (2)
A prospective cohort involving 1194 patients with 1520hospitalizations for severe sepsis drawn from the Health andRetirement Study, a nationally representative survey of USresidents (1998-2006).
A total of 9223 respondents had a baseline cognitive andfunctional assessment; 516 survived severe sepsis and 4517survived a nonsepsis hospitalization to at least 1 follow-up surveyand are included in the analysis.
Long-term Cognitive Impairment and Functional Disability Among Survivors of Severe SepsisTheodore J. Iwashyna, MD, PhD; E. Wesley Ely, MD, MPH; Dylan M. Smith, PhD; Kenneth M. Langa, MD, PhD
JAMA. 2010;304(16):1787-1794. doi:10.1001/jama.2010.1553.

PNEUMONIA ANDDEMENTIA (3)
A high rate of new functional limitations was seen followingpneumonia and sepsis.
Pneumonia and sepsis were independently associated withsubstantial and persistent new cognitive impairment and functionaldisability.
Long-term Cognitive Impairment and Functional Disability Among Survivors of Severe SepsisTheodore J. Iwashyna, MD, PhD; E. Wesley Ely, MD, MPH; Dylan M. Smith, PhD; Kenneth M. Langa, MD, PhD
JAMA. 2010;304(16):1787-1794. doi:10.1001/jama.2010.1553.
MAJOR ILLNESS AND DEMENTIA
SEPSIS
SEPSIS AND DEMENTIA
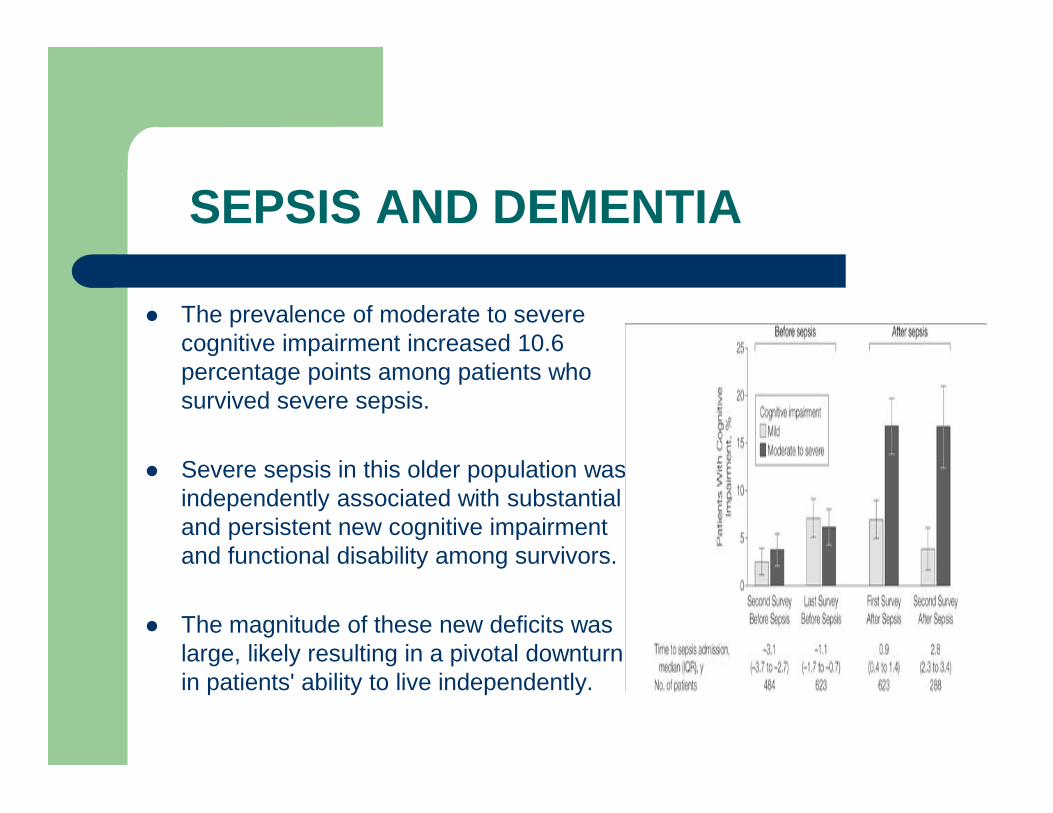
The prevalence of moderate to severecognitive impairment increased 10.6percentage points among patients whosurvived severe sepsis.
Severe sepsis in this older population wasindependently associated with substantialand persistent new cognitive impairmentand functional disability among survivors.
The magnitude of these new deficits waslarge, likely resulting in a pivotal downturnin patients' ability to live independently.
MECHANISMS OF SEPSIS RELATEDDEMENTIA DETERIORATION(1)
Hospitalization-acquired weakness, chronic illness myopathy and polyneuropathy suggests that there is a direct inflammatory
and hypoperfusion-mediated degradation of muscle fibersand neurons, which may be exacerbated by prolongedimmobility and lack of physical therapy.
Similarly, frank hypotension or relative hypoperfusion maydirectly contribute to brain injury and subsequent cognitiveimpairment.
MECHANISMS OF SEPSISRELATED DEMENTIADETERIORATION (2)
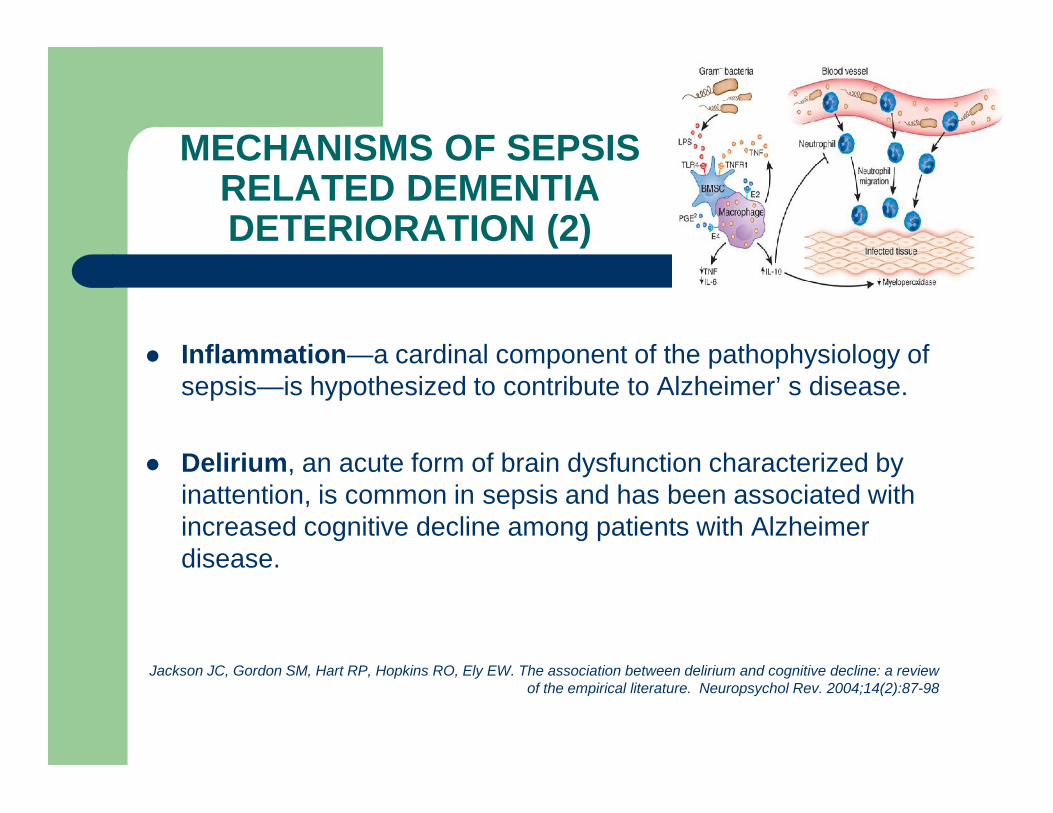
Inflammation—a cardinal component of the pathophysiology ofsepsis—is hypothesized to contribute to Alzheimer’ s disease.
Delirium, an acute form of brain dysfunction characterized byinattention, is common in sepsis and has been associated withincreased cognitive decline among patients with Alzheimerdisease.
Jackson JC, Gordon SM, Hart RP, Hopkins RO, Ely EW. The association between delirium and cognitive decline: a reviewof the empirical literature. Neuropsychol Rev. 2004;14(2):87-98
SEPSIS AND COGNITIVEIMPAIRMENT
3 out of 5 sepsis survivors experienced serious physical and/ormental declines in the years following the event.
Close to 60% of the hospitalizations for severe sepsis wereassociated with worsened mental and physical function, or both,in the years following the event.
Moderate to severe cognitive impairment almost tripled in thesepsis survivors, from 6% before sepsis to almost 17% after.
Among people with no mental or physical limitations beforesepsis, around 40% could not walk without assistance in theyears after.
A core part of sepsis is delirium and delirium is associated withprogression of Alzheimer’s disease and cognitive decline.
MAJOR ILLNESS AND DEMENTIA
ARDS.
ARDS AND DEMENTIA (1)
ARDS patients experience several physical, mental, andpsychological morbidities that significantly impair their health-related quality of life (HRQL).
Persistent for years after hospital discharge, decrements infunctional and neuropsychological outcomes result in lost savings,employment reduction, and a reduction in HRQL among survivorsand their caregivers.
Long-term outcomes in patients surviving acute respiratory distress syndrome/Semin Respir Crit Care Med. 2010Feb;31(1):55-65.

ARDS AND DEMENTIA (2)
Survivors of acute respiratory distress syndrome (ARDS) are atrisk for long-lasting cognitive decline due to:
1. hypoxemia,2. sepsis and/or3. psychological sequelae associated with4. aggressive supportive care in the intensive care unit (ICU).
All ARDS survivors with cognitive deficits were disabled,whereas only 22.9% (n=8) of the cognitively not impairedpatients gave evidence of disability.
ARDS AND DEMENTIA(3)
Patients with cognitive deficits described the lowest HRQOL withmajor limitations in the domains role-physical and socialfunctioning when compared to patients without cognitiveimpairments.
Long-term ARDS survivors exhibit impaired health status and thepresence of cognitive deficits is associated with disability andconsiderable Impairments in HRQOL.
.The relationship between cognitive performance and employment and health status in long-term survivors of the acute
respiratory distress syndrome/ Gen Hosp Psychiatry. 2001 Mar-Apr;23(2):90-6
MAJOR ILLNESS AND DEMENTIA
ICU COGNITIVE DECLINE
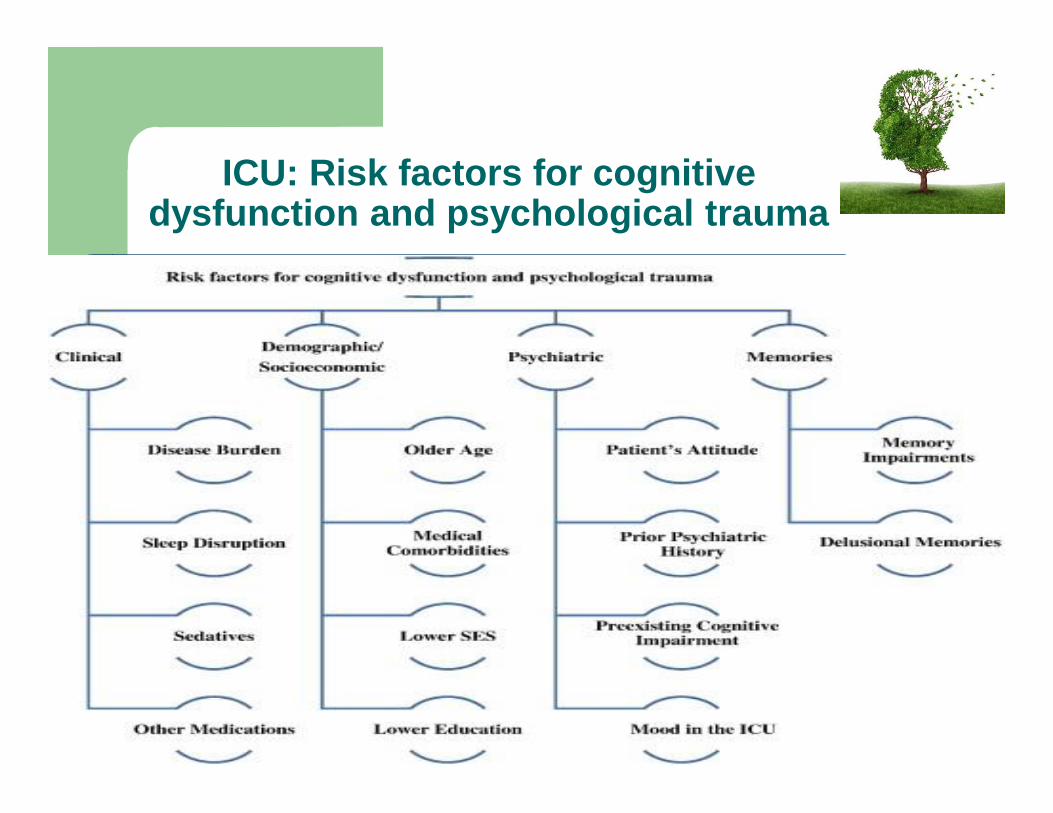
ICU: Risk factors for cognitivedysfunction and psychological trauma
DEMENTIA – ICU(1)
Critically ill patients frequently develop cognitive and psychiatricimpairments during and after the hospital stay manifesting asimpaired memory and executive function, delirium, acute stressresponse, posttraumatic stress disorder (PTSD), anxiety, anddepression.
Both physical and psychiatric sequelae of critical illness maypersist for years after discharge.

DEMENTIA – ICU (2)
Patients often have poor recall of their illness, and periods ofamnesia may be replaced with inaccurate recollections, oftenresulting in delusional and paranoid memories leading to:
1. anxiety,2. depression,3. PTSD,4. hospital phobias and5. panic attacksthat impair recovery and diminish quality of life as well as increasedifficulty of future medical care.
DEMENTIA – ICU(3)
Resultant problems with mental health, cognitive, and physicalimpairments have been termed post intensive care syndrome(PICS), an entity that is disturbingly common and yet still likelyunderrecognized.
Up to 85% to 95% of ICU survivors struggle with persistentweakness.
50% to 70% have difficulties completing activities of daily living 30% to 80% have cognitive impairment and more than 50% manifest various forms of psychiatric morbidity,
which affect not only the patients but their caregivers as well.Together, these impairments lead to an inability to return to theworkforce and increased health care utilization.
Denehy, L. and Elliott, D. Strategies for post ICU rehabilitation. Curr Opin Crit Care. 2012; 18: 503–508

MECHANISMS OF COGNITIVEIMPAIRMENT IN ICU (1)
Pathogenesis of cognitive dysfunction and psychiatric morbidityis incompletely understood.
Multiple risk factors such as:1. Preexisting disease burden (defined as Charlson Comorbidity
Index score >3) was predictive of adverse psychologicaloutcome after critical illness.
2. Neuroimaging and neuropsychological data suggest anassociation of cognitive impairment with a nonspecificacquired brain injury.

MECHANISMS OF COGNITIVEIMPAIRMENT IN ICU (2)
3. Nearly all medical conditions requiring intensive care may havepsychiatric manifestations.
4. Long-term cognitive impairment has been reported inassociation with hypoxia, hypotension, anemia, anddysglycemia commonly seen in the critically ill.
The similarity of cognitive impairment across the populationssuggests that the critical illness itself, regardless of the etiology,may be casually linked with cognitive impairment.
ICU AND SLEEP DISTURBANCES(1)
Sleep disruption and deprivation, due to underlying psychologicalstressors, mechanical ventilation,
noise, light, patient care interactions and medicationsare exceedingly common in the ICU and have been associated withdelirium, cognitive impairment, and worsened psychologicalrecovery from critical illness.
Barr, J., Fraser, G.L., Puntillo, K., Ely, E.W., Gélinas, C., Dasta, J.F. et al. American College of Critical Care Medicine: clinicalpractice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care
Med. 2013; 41: 263–306
ICU AND SLEEPDISTURBANCES (2)
Sleep deprivation may be clinically impossible to distinguish fromdelirium as both can manifest with inattention, variable mentalstatus, and cognitive dysfunction; furthermore, severe sleepdeprivation is similarly characterized by emergence of psychoticbehavior and paranoia that tend to worsen during the night.
Weinhouse, G.L., Schwab, R.J., Watson, P.L., Patil, N., Vaccaro, B., Pandharipande, P. et al. Bench-to-bedside review:delirium in ICU patients—importance of sleep deprivation. Crit Care. 2009; 13: 234
Kamdar, B.B., Needham, D.M., and Collop, N.A. Sleep deprivation in critical illness: its role in physical and psychologicalrecovery. J Intensive Care Med. 2012; 27: 97–111
ICU STRESS/ EMOTIONS
Emotions experienced in the ICU such as agitation and depressionare also important predictors of future psychological problems
Inhospital acute stress symptoms were independently associatedwith increased severity of PTSD and depressive symptoms in theyear after ICU discharge.
Davydow, D.S., Zatzick, D., Hough, C.L., and Katon, W.J. A longitudinal investigation of posttraumatic stress and depressivesymptoms over the course of the year following medical-surgical intensive care unit admission. Gen Hosp Psychiatry. 2013; 35:
226–23
Mood in the ICU (composed of symptoms such as anger,nervousness, low temperament, and confusion) and early intrusivememories of intensive care were the strongest acute psychologicalrisk factors for PTSD and depression.
Wade, D.M., Howell, D.C., Weinman, J.A., Hardy, R.J., Mythen, M.G., Brewin, C.R. et al. Investigating risk factors forpsychological morbidity three months after intensive care: a prospective cohort study. Crit Care. 2012; 16: R192
PREVENTION OFHOSPITALIZATION
Early recognition of precipitating factors leadingto delirium in dementia patients who underwentmajor illness.
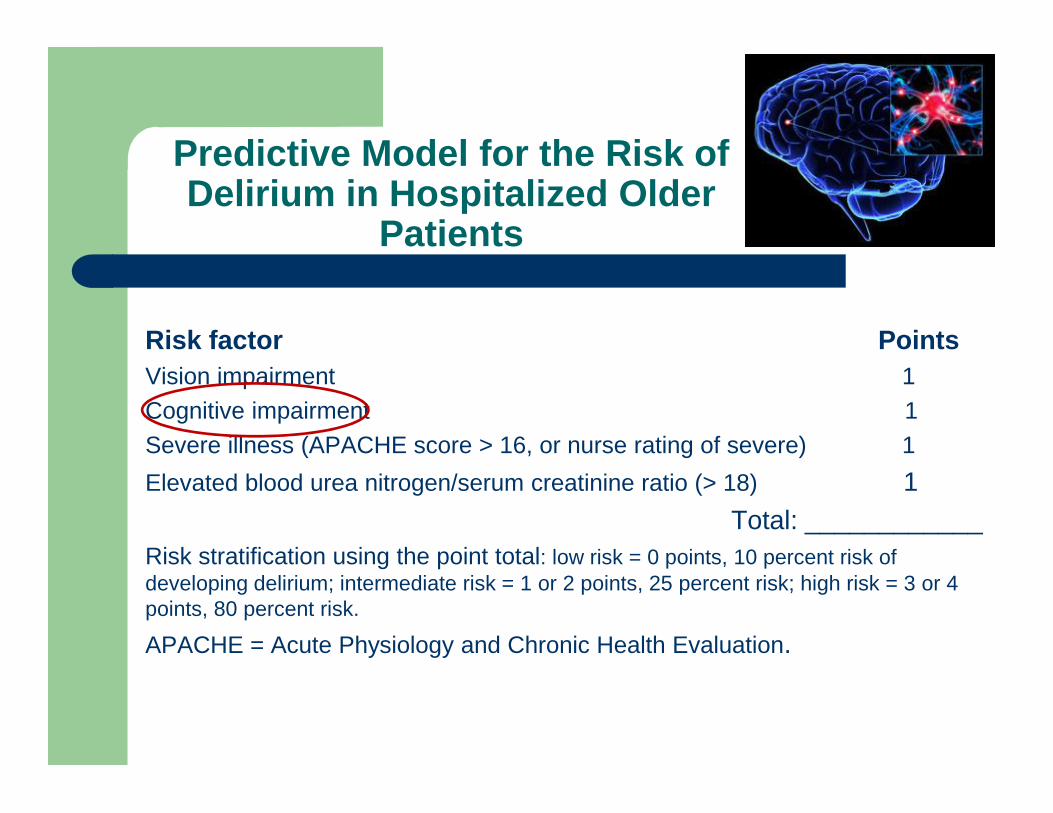
Predictive Model for the Risk ofDelirium in Hospitalized Older
Patients
Risk factor PointsVision impairment 1Cognitive impairment 1Severe illness (APACHE score > 16, or nurse rating of severe) 1Elevated blood urea nitrogen/serum creatinine ratio (> 18) 1
Total: ____________Risk stratification using the point total: low risk = 0 points, 10 percent risk ofdeveloping delirium; intermediate risk = 1 or 2 points, 25 percent risk; high risk = 3 or 4points, 80 percent risk.
APACHE = Acute Physiology and Chronic Health Evaluation.
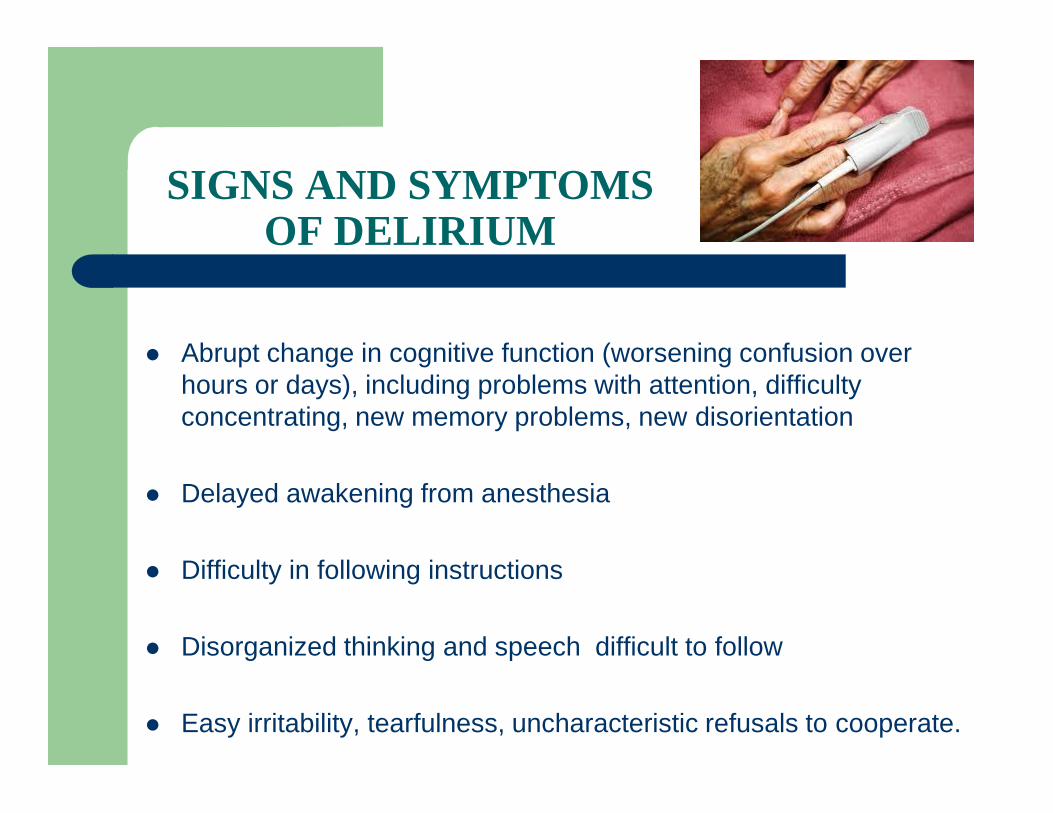
SIGNS AND SYMPTOMSOF DELIRIUM
Abrupt change in cognitive function (worsening confusion overhours or days), including problems with attention, difficultyconcentrating, new memory problems, new disorientation
Delayed awakening from anesthesia
Difficulty in following instructions
Disorganized thinking and speech difficult to follow
Easy irritability, tearfulness, uncharacteristic refusals to cooperate.

SIGNS AND SYMPTOMS OFDELIRIUM
New paranoid thoughts or delusions,illusions,hallucinations Motor changes such as slowed or decreased movements,
purposeless fidgeting or restlessness, new difficulties in maintainingposture such as sitting or standing
Sleep/wake cycle changes such as sleeping during the day and/orawake and active at night
Decreased appetite New incontinence of urine or stool Fluctuating symptoms and/or level of arousal over the course of
minutes to hours
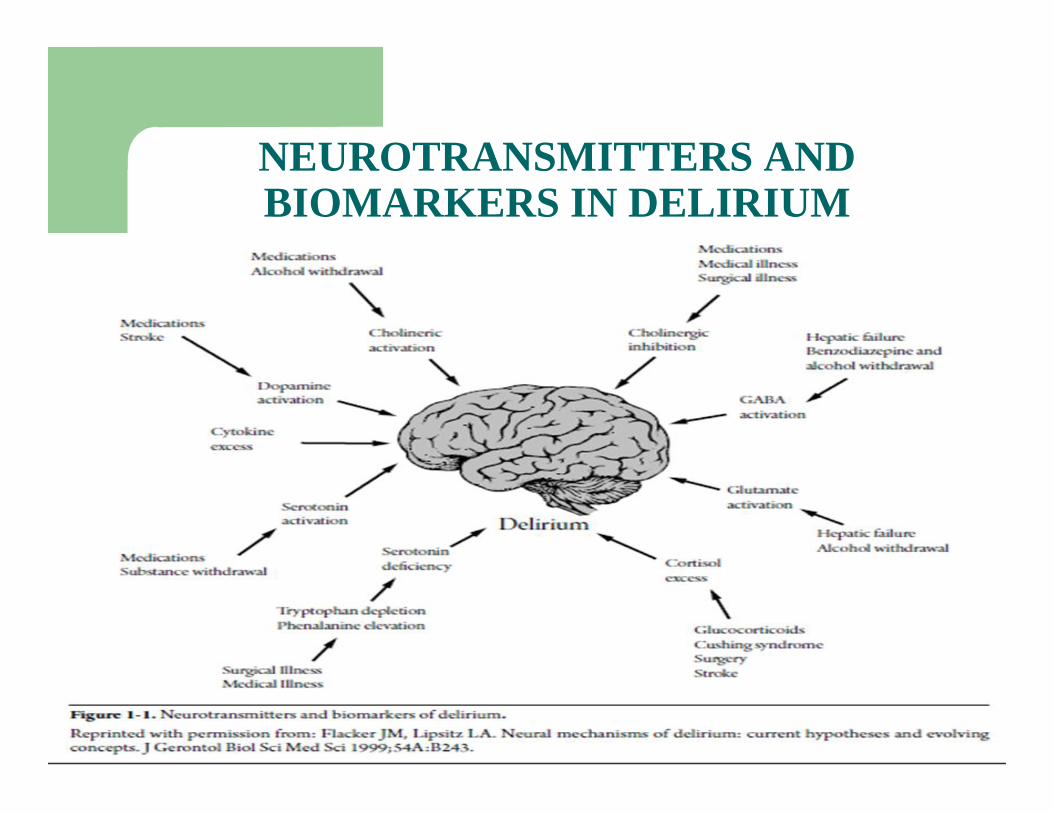
NEUROTRANSMITTERS ANDBIOMARKERS IN DELIRIUM
DELIRIUM
DELIRIUM

FREQUENCY AND CHARACTERISTICS OF IATROGENICHYPOGLYCEMIA REQUIRING MEDICAL ASSISTANCE. A
MULTICENTER STUDY IN TERTIARY HOSPITALS.Mylona M1, S. Kalopita2, L. Lanaras2, A. Papazafiropoulou3, S. Papas3, Aggelis N4, Karamagkiolis S4, Vazintari
V5, Melidonis A5, Ntova V6, Xilomenos A6, Basagiannis Ch1, Voukali M7, Ioannidis I7, Zilos A8, Kaltsas G8,Karametos I9, Kapsalas D9, Liatis S1.
8 hospitals (9 clinics) in 5 citiesparticipated in this 22-month,prospective survey ofdocumented iatrogenichypoglycemia at the emergencydepartments (ED).
295 episodes were recorded in294 patients (compared tomatched controls.)
The majority of patients haveT2D, they are elderlyindividuals suffering fromserious medical conditionsand in their great majority aretreated with insulin or SUs.
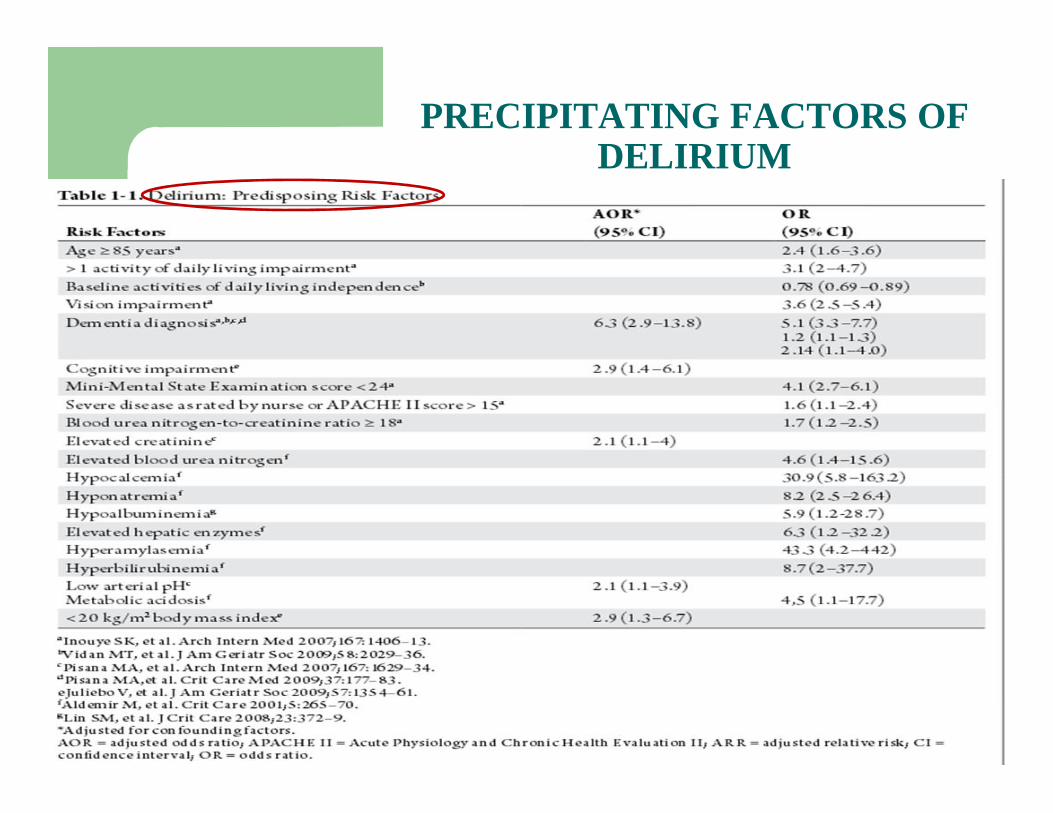
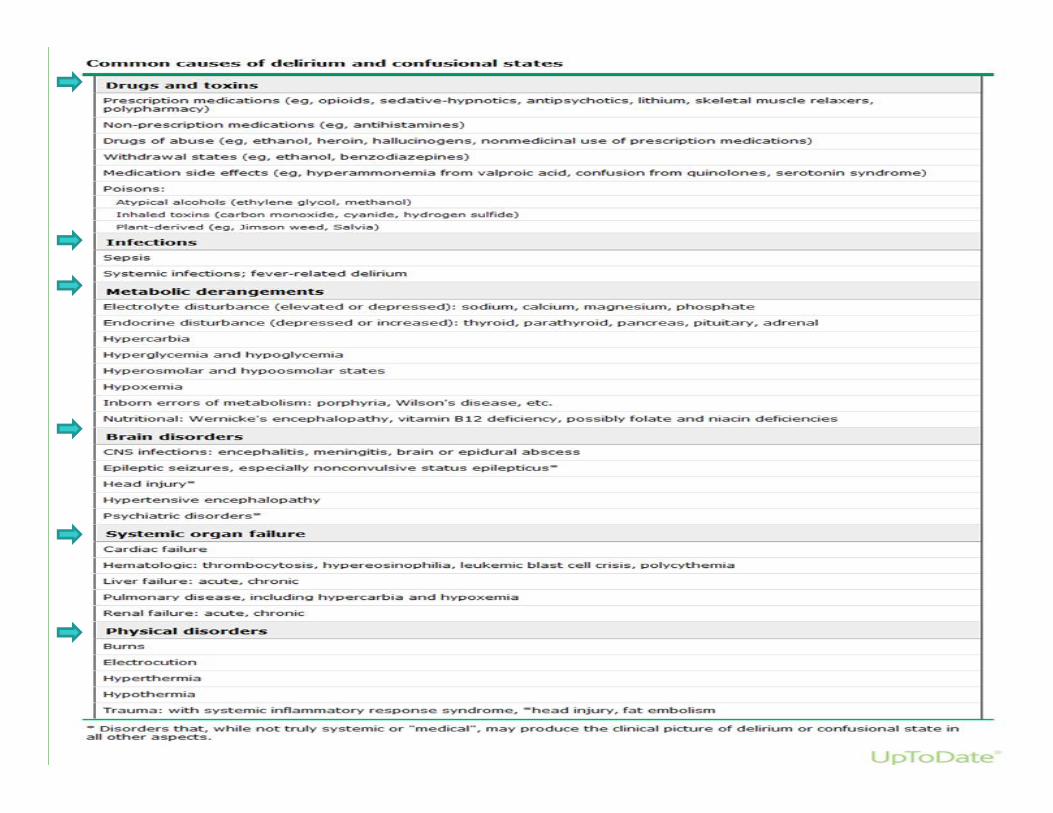
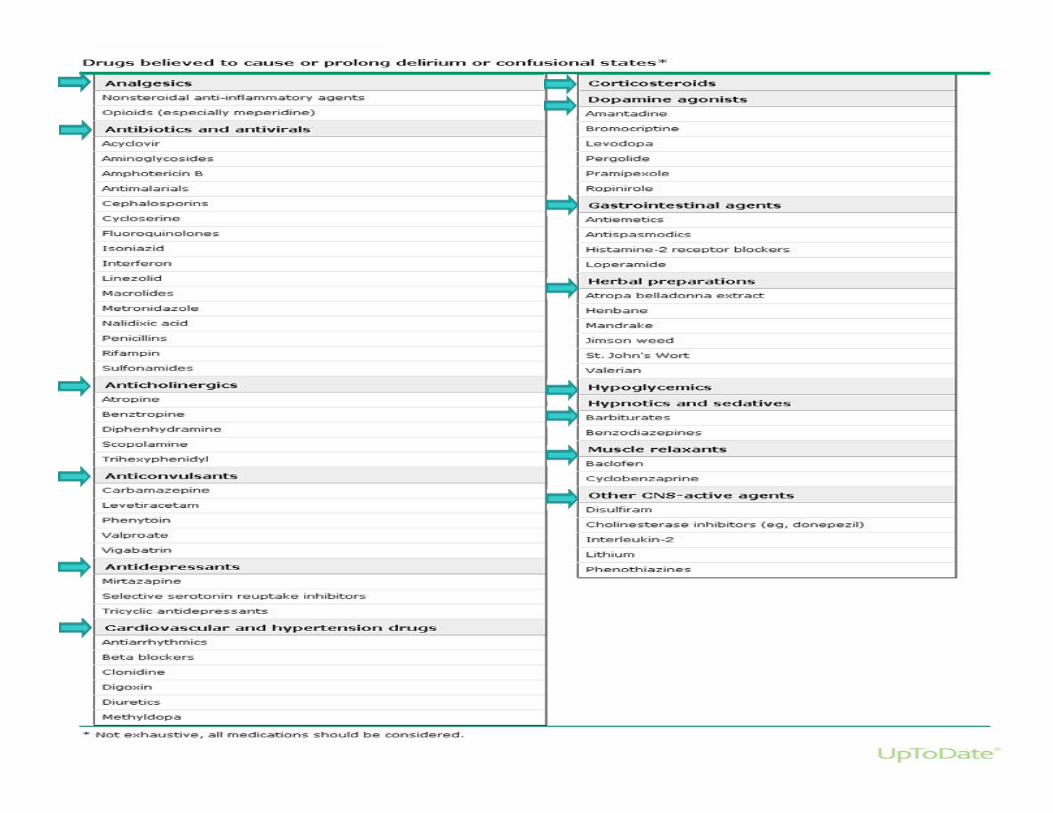
PRECIPITATING FACTORS OFDELIRIUM
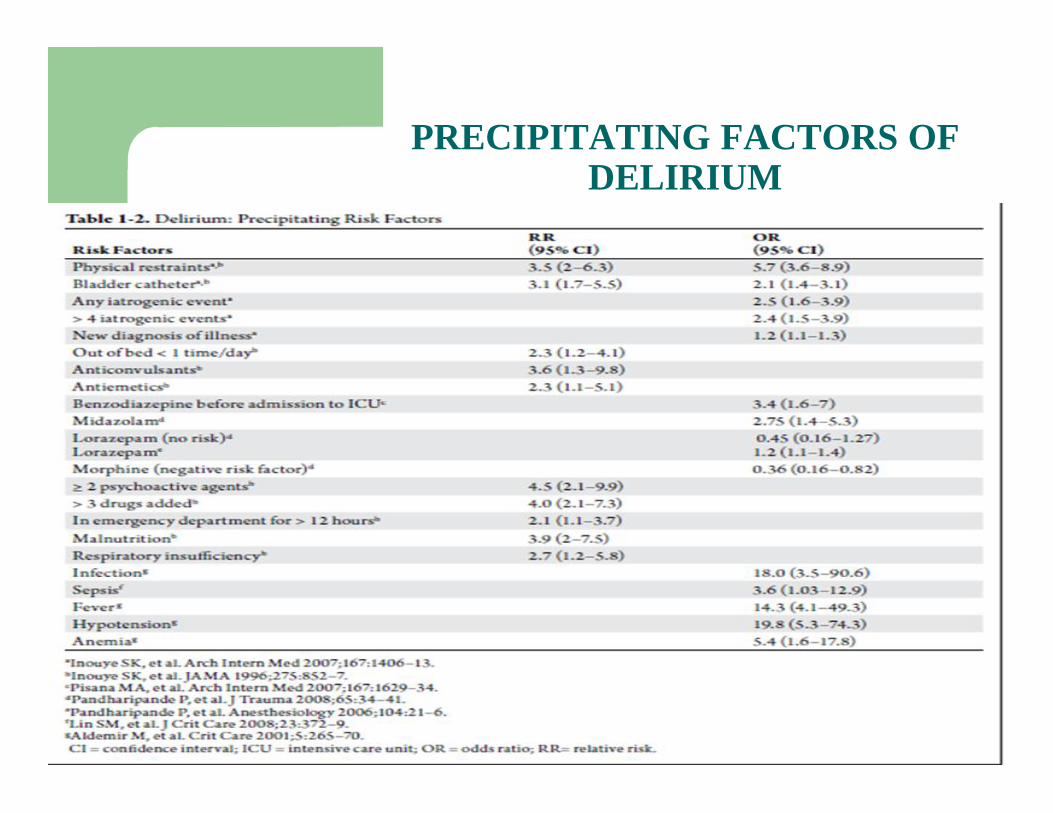
PRECIPITATING FACTORS OFDELIRIUM
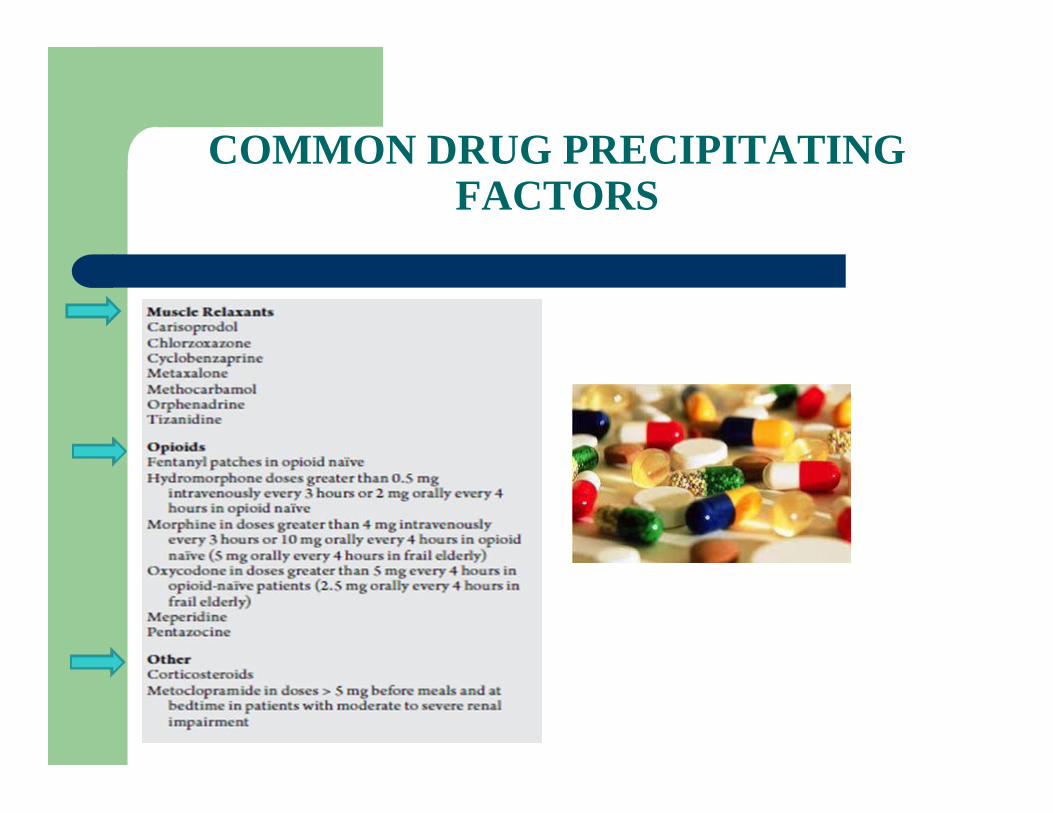
COMMON DRUG PRECIPITATINGFACTORS

COMMON DRUGPRECIPITATING
FACTORS
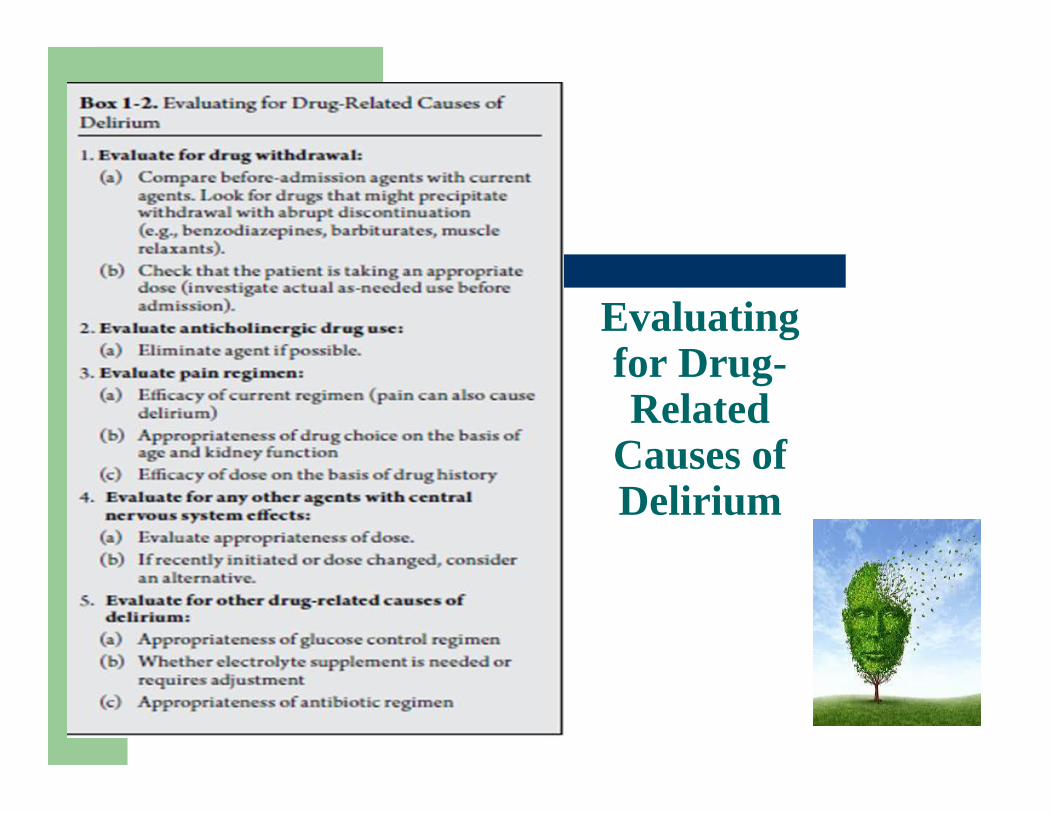
Evaluatingfor Drug-Related
Causes ofDelirium

TREATMENT OPTIONS
• treatment of underlying conditions thatpredispose the individual to delirium
• non-pharmacological interventions
• pharmacological interventions
KEY CONCLUSIONS
Major illness contributes to cognitive impairmentby multiple mechanisms.
Early recognition of delirium in dementedpatients is crucial.
Multiple precipitating factors contribute to itsarousal.
Always respect the dignity and independence ofthe patient to prevent further disability.
Τίμα το γήρας, ου γαρ έρχεται μόνον.Μένανδρος, 4ος αιών π.Χ., Αρχαίος Έλληνας ποιητής
THANK YOU