magnetic resonance imaging - gastroenterologiaroma.it · mata a, et al. gastrointest endosc 2005;...
TRANSCRIPT

5th SESSION HOW TO INVESTIGATE THE SMALL BOWEL
Chairpeople: S. Cucchiara, F. Maccioni
Emanuele Casciani
[email protected] Responsabile U.O.S. Diagnostica del trauma in Urgenza U.O.C. Radiologia d’Urgenza, Direttore Prof. GF Gualdi
Azienda Policlinico Umberto I, Università “La Sapienza” - Roma
Magnetic Resonance Imaging

• Esophagus, stomach and colon are studied with routine endoscopic methods while evaluating clinical/endoscopic SB is difficult
• Imaging is an important step in the diagnosis and follow-up of SB diseases
• The ideal imaging should be
– Non-invasive
– No X-ray
– Repeatable
– Able to give information about the lumen/mucosa/ intestinal wall and surrounding structures
– Inexpensive

MR enterography
Adequate preparation (distension of SB loops) of children for the MRI examination is vital to achieve good results

How to image a young ill, non-cooperative child in MRI with parents?
Triks and tips for imaging children in MRI

The ‘mock MRI’ procedure involves children undergoing a simulated scan with the assistance of a play therapist prior to the actual diagnostic scan
Triks and tips for imaging children in MRI
• The ‘mock MRI’ • reduced the n° of pts who have required anesthetic
Carter AJ. Pediatric Radiology 2010 • reduced the time required for the diagnostic scan de Amorim e Silva. Australasian Radiology 2006
• The “mock MRI” acts • as a screening tool, • to prepare the children, by familiarizing them with the
environment, sounds, and equipment

Problems and tips for imaging children in MRI
IV cannulation is a major cause of anxiety in young patients presenting for MRI examination
Drink at least 1 liter of saline solution
Enter into a tube
It is helpful to separate the procedures of IV placement and the MR exam by placing the cannula before the MR exam
Improve the taste of drink!
Children typically find it difficult to satisfactorily hold their breath, creating significant challenges in abdominal imaging To teach to maintain apnea before the MR exam
Spaceship !!

Techniques in scanning children
MR enteroclysis under sedation in 1-year old male with CD at colonoscopy
Free breathing MR enterography sequences in 4-year old male with Meckel Diverticulum High Resolution MR enterography – colonography in 16-year old famale with Crohn’s Disease

• Initial investigation should consist of colonoscopy (including terminal ileal intubation) with multiple biopsies, upper GI endoscopy with multiple biopsies, and small bowel imaging.
• The technique used to examine the SB will depend on local expertise; but dynamic contrast-enhanced MRI can reliably show most lesions of Crohn's disease without exposure to ionizing radiation.
The 2° European evidence-based Consensus on the diagnosis and management of Crohn's disease
Van Assche G and European Crohn's and Colitis Organisation Journal of Crohn's and Colitis 2010; 4: 63–101

J Am Coll Radiol. 2011 - ACR Appropriateness Criteria on Crohn's disease
ACR Appropriateness Criteria on Crohn's disease 2011
Child or young adult. Initial presentation. Suspected Crohn disease

Small-Bowel Crohn Disease • Spectrum of findings
– Active inflammation
– Penetrating Disease
– Fibro-stenosing Disease
• Disease Location and extent: jejunum, ileum, colon • Stricture • Extraenteric Assessment
– Fistulas and sinuses, abscess, colonic abnormalities
– Perianal fistulas
• Differential diagnosis
Patients may exhibit characteristics of more than one disease subtype
It is common for a single resected bowel specimen to contain areas of acute and chronic inflammation, and fibrosis
Di Nardo G, Aloi M, Oliva S, Civitelli F, Casciani E, Cucchiara S. Investigation of small bowel in pediatric Crohn's disease. IBD 2012;18:1760-76

• In older children the location of CD is similar to the AP: terminal ileum (50%–70%)
• The significant difference between PP and AP CD can best be demonstrated in patients less than 5 years of age: these patients tend to have significant large bowel involvement (isolated or colon and SB disease together) Kelsen J, Baldassano RN. Inflamm Bowel Dis. 2008
• PP are more likely to have upper gastrointestinal involvement than their adult peers.
Levine A. Dig Dis. 2009
Differences in the location and activity of CD lesions between adult and pediatric patients with MRI
• High activity (score 3): PP 34 % vs AP 9 % • Involvement of terminal ileum was significantly different in the two groups: 100 % of AP vs 58 % of PP. Conversely, the colon was diseased in 84 % of PP vs 64 % of AP (left colonic segments in PP)
Maccioni F, et al. Eur Radiol 2012

Stratified or layered appearance on contrast-enhanced T1-w fat-
suppressed image
CD Nicolò 8 y-old CD Elena 13 y-old
Increased mesenteric vascularity (comb sign) on contrast-enhanced fat-suppressed T1-w fat-suppressed image
Active Inflammation MRI findings

MRI Findings
– Wall thickness (mm)
– RCE (relative contrast enhancement)
– Edema – Ulcers/pseudopolyps
– Enlarged lymph nodes Rimola J, et al. Gut 2011; 58: 1113
Mary J, Modigliani R. Gut 1989; 30: 983
Sensitivity 81% Specificity 89%
According to Severity of Endoscopic Lesions (CDEIS)

• PCDAI and MRE score were found to have a statistically significant positive correlation of 0.37 (P=0.020426)
• Because PCDAI is a validated tool to assess disease severity, this suggests that MRE has a potential role in assessing clinical significant degrees of mucosal inflammation
• What remains to be seen is whether MRE is sensitive enough to adequately predict complete mucosal healing [clinical remission in CD]
MR Enterography vs Pediatric Crohn’s Disease Activity Index (PCDAI)
Silverstein J, et al JPGN 2012

Settembre 2009 Giugno 2010
Wall thickness and pseudopolyps
Submucosal Edema
Comb sign and enlarged lymph-nodes
Stratified appearance
Active inflammation In remission
Crohn’s Disease evolution
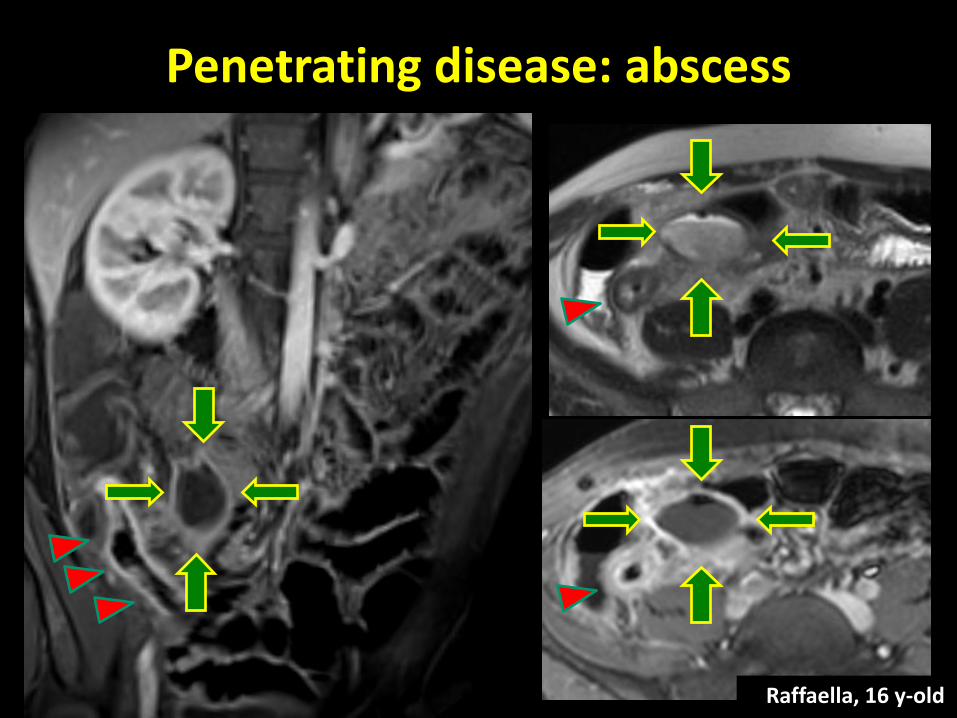
Penetrating disease: abscess
Raffaella, 16 y-old

Terminal ileitis and perianal fistula
Antonio 12 y-old
Pelvic MRI should be the initial procedure because it is accurate and non-invasive, although it is not needed routinely in simple fistulae
Van Assche G and European Crohn's and Colitis Organisation Journal of Crohn's and Colitis 2010; 4: 63–101

SB occlusion Active disease Fibro-stenosing disease

Disease course and efficacy of medical therapy in stricturing paediatric Crohn's disease
A stricturing phenotype is not uncommon at the diagnosis of CD in children (36% had an “early” stenosis, while 64% developed it at the follow-up) Purely inflammatory MR features of stenosis predict a high rate of response to medical therapy. In the absence of these features, early surgery could be considered as an effective approach to PP with stricturing CD
Aloi M, Viola F, D'Arcangelo G, Di Nardo G, Civitelli F, Casciani E, Oliva S, Nuti F, Dilillo A, Cucchiara S. Disease course and efficacy of medical therapy in stricturing
paediatric Crohn's disease. Dig Liver Dis. 2013

Functional MR techniques for Crohn’s Disease
Motility imaging DWI

MR enterography vs US
• Good correlation for individuation and CD locations
• MR < CE for mucosal abnormalities, but MR > CE for transmural/extramural abnormalities
MR enterography vs CE
• Same accuracy for active inflammation in CD
• Sensitivity MR (98%) > US (76%) respect to endoscopy
• Accuracy US (89%) > MR (73%) [no MR enterography]
No studies with “state of the art” methods
Potthast S et Eur Radiol 2002
Pascu M et al Inflamm Bowel Dis 2004
Martinez MJ Abd Im 2009; Pauls S Eur Radiol 2006; Miao YM Clinical Radiol 2002
Casciani E, Di Nardo G, Oliva S, Cucchiara S, Gualdi G. MR enterography versus capsule endoscopy in paediatric patients with suspected Crohn’s disease. Eur Radiol 2011

• Almost 70% of PJS patients undergo a laparotomy before
adulthood and many of them require repeated laparotomies over their lifetimes
• Lifetime incidence of malignancy is 60%, most commonly in the SB • Current guidelines recommend biennial examination of the SB to
detect large polyps • Initial data have shown CE to be a superior technique to barium
studies for detecting polyps, but CE has some limitations, such as:
• Size estimation and anatomic localization of polyps may be inaccurate
• Polyps can be double-counted or missed altogether (retrograde
peristalsis, rapid capsule transit, and limited video frame capture rate)
Peutz-Jeghers Syndrome
Brown G, et al. Endoscopy 2006; Schulmann K, et al. Am J Gastroenterol 2005 Mata A, et al. Gastrointest Endosc 2005; Soares J, et al. Endoscopy 2004

Peutz-Jeghers Syndrome
• MR enterography is a promising alternative to CE for SB surveillance in adults with PJS (19 patients) • CE is more comfortable for the patient • MR may be less prone to miss large polyps and may
be more reliable in their size assessment • MR offers the potential for detecting extraluminal
cancers Gupta A, et al. AJR 2010
Maccioni F, et al. Abdom Imaging 2012
• In 8 PJS patients concordance between MRE and endoscopy was • 72.6% for polyps <15 mm • 93% for polyps >15 mm

2009 2012 2011
Peutz-Jeghers Syndrome
Same patient

...Crohn’s Disease and beyond… Appendicitis
Diana 16 y-old Diarrhea, fever, abdominal pain US: Terminal ileum wall thickening

Raffaella, 17 y-old
...Crohn’s Disease and beyond… Meckel Diverticulum
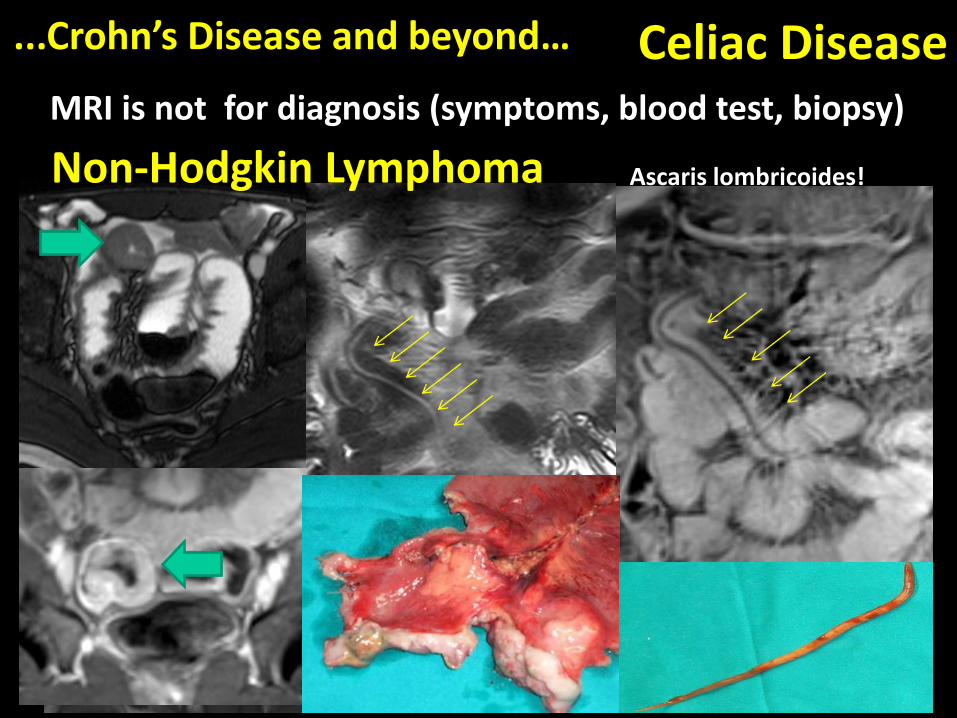
Celiac Disease MRI is not for diagnosis (symptoms, blood test, biopsy)
Reversal of the fold pattern, with more prominent folds in the ileum than in the
jejunum
...Crohn’s Disease and beyond…
Non-Hodgkin Lymphoma Ascaris lombricoides!

...Crohn’s Disease and beyond… SB giant cavernous hemangioma Annalisa, 6 y-old with syncope
Anemia Hb 3.5 mg/dl Negative upper and lower GI endoscopy
T2-w T2-w fat-suppressed contrast-enhanced T1-w fat-suppressed (venous phase)
contrast-enhanced T1-w fat-suppressed (delayed phase)

Alessandra, 9 y-old 3 years vomiting and diarrhea Colonoscopy: only the sigmoid colon was explored
...Crohn’s Disease and beyond… Descending colon volvulus

• Why MR enterography
– Non-invasive, no X-ray, repeatable,
– Better than other methods
– Able to give information on lumen/mucosal/ intestinal wall and surrounding structures
• When MR enterography
– IBD (staging, active inflammation, follow-up, perianal fistula, …)
– Familial polyposis follow-up
– Problem solving
TAKE HOME POINTS

• Where and How MR enterography
– Specialized pediatric hospital with High-field MR scan
– Specialized staff and equipment
– Gastrointestinal subspecialty for radiologists
TAKE HOME POINTS
There is no ‘one size fits all’ approach to imaging children and pediatric MRI requires dedicated specialist knowledge, flexibility, and expert input from the technologist, nurse and doctor!!