lymphoproliferative disorders of the gastrointestinal tract · lymphoproliferative disorders of the...
TRANSCRIPT

Lymphoproliferative Disorders of theGastrointestinal Tract
A Review and Pragmatic Guide to Diagnosis
Jerome S. Burke, MD
N Context.—The gastrointestinal tract is the most commonsite of extranodal lymphomas. Although all histologic catego-ries of malignant lymphoma develop in the gastrointestinaltract, large B-cell lymphomas predominate, followed byextranodal marginal zone lymphomas of mucosa-associatedlymphoid tissue (MALT) type; the latter is especially prevalentin stomach. The acceptance of extranodal marginal zonelymphoma of MALT type as a clinicopathologic entity hasreduced the number of cases that formerly were interpreted asflorid lymphoid hyperplasia (‘‘pseudolymphoma’’). Nonethe-less, the distinction of lymphoid hyperplasia from a lymphomaof MALT type in small biopsy specimens remains problematic.
Objective.—To assess the relevant morphologic, immu-nologic, molecular, and genetic properties of gastrointes-tinal lymphomas and to present a feasible tactic fordiagnosis, expressly for small biopsy specimens.
Data Sources.—Case-derived material and literaturereview using PubMed (National Library of Medicine).
Conclusions.—Most gastrointestinal lymphomas are read-ily amenable to an unqualified diagnosis, primarily thosecases consisting of monomorphic large cells whether of B- orT-cell lineage, including cases associated with enteropathy.Diagnosis for infiltrates dominated by small lymphocytesremains taxing, as the differential diagnosis embraces notonly MALT lymphoma and lymphoid hyperplasia but alsomantle cell lymphoma, follicular lymphoma, and chroniclymphocytic leukemia/small lymphocytic lymphoma. Ad-herence to strict morphologic criteria is the standard fordiagnosis, but these criteria should be augmented byimmunologic studies together with judicious use of molec-ular techniques to determine clonality. In establishing adiagnosis of gastric marginal zone lymphoma of MALT type,determination of t(11;18)(q21;q21) status may be requiredsince this translocation has clinical ramifications.
(Arch Pathol Lab Med. 2011;135:1283–1297; doi: 10.5858/arpa.2011-0145-RA)
The gastrointestinal tract is the most common location ofextranodal lymphomas, with the stomach as the most
frequent site of involvement and with the small intestinesecond in frequency.1 Large intestinal and rectal lympho-mas are far less common but are discovered in patientswith AIDS and sporadically in patients with ulcerativecolitis and Crohn disease.2–4 In a study of 371 patients withprimary gastrointestinal lymphomas registered in a Ger-man multicenter study, stomach accounted for 277 ofcases (74.8%), whereas small intestine and ileocecal regionrepresented 61 cases (16.4%).5 Only 9 cases (2.4%) in thatseries were restricted to the colorectal area, with theremaining cases involving multiple gastrointestinal sites.The incidence of primary gastric lymphomas, specificallyextranodal marginal zone lymphomas of mucosa-associ-ated lymphoid tissue (MALT) type, has vacillated, with
a peak reached in the 1990s subsequent to the in-creasing recognition of MALT lymphoma as a specificdiagnostic entity, followed by a persistent decline in thepast decade; this decline may be related to the improvedclinical management and reduction in Helicobacter pyloriinfection.6
The concept of extranodal marginal zone lymphomaof MALT type has revolutionized the criteria for themorphologic diagnosis of an extranodal lymphoma,specifically those lymphomas dominated by small lym-phocytes. Since the initial descriptions of lymphomas ofMALT in 1983 and 1984, the morphologic criteria haveevolved and expanded to encompass the following: amore precise definition of various cell types in MALTlymphoma, proposals for ‘‘lymphoepithelial lesions’’ and‘‘follicular colonization,’’ the relationship between MALTlymphomas and marginal zone B cells, and a scoringsystem for diagnosis of gastric MALT lymphoma.7–12
Moreover, the morphologic criteria have expanded toembrace immunophenotypic, biologic, molecular genetic,and clinical discoveries.9,13–18 Developments, such as theassociation of gastric MALT lymphoma with H pyloriinfection, the notion of acquired MALT, the biology ofautoantigen activation and continuous somatic mutations,the documentation of genetic aberrations, for example, thediscovery of the t(11;18)(q21;q21) chromosomal transloca-tion in lymphomas of MALT, and the clinical implications
Accepted for publication June 9, 2011.From the Department of Pathology, Alta Bates Summit Medical
Center, Berkeley, California.The author has no relevant financial interest in the products or
companies described in this article.Presented in part at the Tutorial on Pathology of the GI Tract,
Pancreas, and Liver, Westin Diplomat Resort & Spa, Hollywood,Florida, November 15–19, 2010.
Reprints: Jerome S. Burke, MD, Department of Pathology, AltaBates Summit Medical Center, 2450 Ashby Ave, Berkeley, CA 94705(e-mail: [email protected]).
Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke 1283

of specific cytogenetic alterations, have been the subject ofexcellent reviews and will not be recapitulated to anydegree.19–21 The goal of this review is to critique the salientmorphologic, immunologic, molecular, and genetic attri-butes of gastrointestinal lymphomas and to provide astrategy for a solid foundation for diagnosis, especiallywith respect to small gastrointestinal biopsy specimens.
FLORID LYMPHOID HYPERPLASIA(‘‘PSEUDOLYMPHOMA’’) VERSUS
MALIGNANT LYMPHOMA
In establishing a histologic diagnosis of an extranodallymphoma, pathologists are aware that various forms ofreactive lymphoid hyperplasia clinically and pathologi-cally mimic gastrointestinal lymphomas, such as gastriclymphoid hyperplasia and chronic lymphocytic gastritis.To confuse the issue, malignant lymphoma of extranodalmarginal zone (MALT) type may develop in associationwith these reactive lymphoid infiltrates, including those instomach.22
In the 1960s and 1970s, the morphologic criteria todistinguish extranodal lymphoma from extranodal lym-phoid hyperplasia were derived from those used tradi-tionally to distinguish malignant lymphoma from lym-phoid hyperplasia in lymph nodes.23 The major criteriafor this distinction included monomorphic lymphocyticinfiltrates, cellular atypia, germinal centers, and architec-tural disruption.24
Since most gastrointestinal lymphomas are large B-celllymphomas with associated monomorphism, cellular atyp-ia, and architectural destruction (eg, eradication of glands),these conventional criteria generally have proved germane.At the converse end of the continuum, obvious reactivelymphoid conditions similarly do not usually presentdiagnostic difficulties. Lymphocytic infiltrates that displaypolymorphism, that contain a range of mature lymphocytesencompassing plasma cells and immunoblasts, that exhibitwell-defined germinal centers, and that do not raze thearchitectural landmarks of the gastrointestinal site usuallycan be diagnosed assertively as benign and reactive.
The main difficulty in the separation of gastrointestinallymphomas from lymphoid hyperplasia concerns mar-ginal zone lymphomas of MALT type that are dominatedby small lymphocytes and that commonly are associatedwith germinal-center formation.25 For such cases, theconventional histologic criteria are not valid (Figure 1, Aand B). Many histologically ambivalent gastrointestinalsmall lymphocytic proliferations prove to be monoclonaland are probably malignant lymphomas, especially ofMALT type.26 The application of immunologic andmolecular genetic analyses to gastrointestinal sites, espe-cially gastric small lymphocytic proliferations, has servedto vividly alter the traditional histologic criteria and hasexposed innumerable inconsistencies in these criteria.24 Atthe Armed Forces Institute of Pathology, for example, of97 cases reviewed from 1970 to 1985, which formerly werediagnosed as gastric pseudolymphoma, 79% were reclas-sified as malignant lymphoma, and two-thirds of thenewly classified lymphoma cases subsequently weredesignated as lymphomas of MALT type.27 Lymphoidhyperplasia or atypical lymphocytic infiltrates comprisedthe remaining cases. As a result, the term pseudolymphomais currently considered nebulous and obsolescent and isno longer suitable as a diagnostic term.10
The current perception of small gastrointestinal lym-phocytic proliferations that appear mature has changedsignificantly, not only by refinement of the morphologiccriteria, but also by the utilization of immunologictechniques, including immunohistochemistry, in situhybridization, flow cytometry, and gene rearrangementto analyze the clonality of these lesions. For example, inpatients with documented suspicious lymphocytic infil-trates in gastroscopic biopsy specimens, multiple repeatedbiopsy fragments of the lesion submitted fresh for flowcytometry analysis frequently result in the demonstrationof monoclonality and verification of lymphoma.28 Caution,however, is required in the evaluation of immunoglobulinstudies using polymerase chain reaction (PCR) techniquesin fixed, paraffin-embedded tissues; small monoclonalbands may occur in extranodal reactive lymphoidhyperplasia, as for example in chronic active gastritisassociated with H pylori and associated with lymphoidfollicles.29,30 Therefore, if PCR for immunoglobulin generearrangement is to be performed, the test should belimited to those gastric cases with strong morphologicsuspicion for actual lymphoma.21,30
Lymphoid follicles or reactive germinal centers createanother conundrum in diagnosis. Germinal centers are acommonly accepted histologic trait of gastric lymphoidhyperplasia, and isolated follicles are a common finding ingastric biopsy specimens.31 Germinal centers, however,are regular components of many lymphomas of MALT.The critical morphologic characteristic of MALT lympho-mas is their simulation of normal MALT as typified byPeyer patches found in the terminal ileum.9 The neoplasticB lymphocytes of MALT lymphomas are found inmarginal-type zones adjoining reactive follicles and oftendiminished rims of mantle zone lymphocytes. Thegerminal centers frequently are atrophic owing to en-croachment by the encircling small lymphocytes. InMALT lymphomas of stomach, affiliated with pepticulcer, germinal centers occur at the base of the ulcer and inthe adjacent mucosa, where they appear entrapped by themonotonous marginal zone lymphocytes. Frequently, theneoplastic marginal zone lymphocytes invade the ger-minal centers in a process referred to as ‘‘follicularcolonization.’’ 11 When follicles are numerous, follicularcolonization may imitate follicular lymphoma. In somecases, the lymphomatous infiltrate may result in architec-tural destruction with concealment of remaining germinalcenters; however, the presence of cryptic germinal centerscan be accentuated by the immunohistochemical demon-stration of follicular dendritic cells with an antibodyagainst CD21 or CD23.25,32
Despite honing of the criteria to separate gastrointesti-nal lymphoid hyperplasia from lymphoma, gastrointesti-nal lymphoid hyperplasia remains a relatively commonhistologic alteration. Gastrointestinal lymphoid hyperpla-sia involves not only stomach, but may occur anywherein the intestine, as for example the ileum, where Peyerpatches may be particularly pronounced.33 Lymphoidhyperplasia of the gastrointestinal tract may be focal or,rarely, nodular, encompassing long segments of the smalland large intestine, where it needs to be distinguishedfrom mantle cell lymphoma and follicular lymphoma.34
Lymphoid hyperplasia also may affect the rectum and,on occasion, cause a diagnostic challenge. Localizedlymphoid hyperplasia of the rectum recently has beenreferred to as rectal ‘‘tonsil.’’ 35 Patients may present with
1284 Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke

Figure 1. Massive gastric infiltrate (A) from an archival case in a study from the late 1960s, labeled as ‘‘pseudolymphoma.’’ The diagnosis ofpseudolymphoma most likely was based on the fact that the infiltrate is dominated by small, round lymphocytes with scattered germinal centers (B).With current criteria, this case likely would be labeled gastric marginal zone lymphoma of MALT type (hematoxylin-eosin, original magnifications3150 [A] and 3300 [B]).
Figure 2. Florid lymphoid hyperplasia in the rectum. At both lower (A) and higher magnifications (B), tingible body macrophages are apparent andindicate that the follicles are reactive and not lymphoma. In the rectum, florid lymphoid hyperplasia has been referred to as rectal ‘‘tonsil’’ and somecases can be mistaken for lymphoma (hematoxylin-eosin, original magnifications 330 [A] and 3150 [B]).
Figure 3. Large B-cell lymphoma is the most common type of lymphoma in stomach (A). The diagnosis is supported by an immunoperoxidase stainfor CD20 (B) (hematoxylin-eosin, original magnification 3300 [A]; original magnification 3300 [B]).
Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke 1285

either rectal bleeding or abdominal pain and at endoscopyexhibit a raised polypoid lesion or mucosal nodularity andeven a mass. The lymphoid hyperplasia or tonsil involvesthe lamina propria or submucosa (Figure 2, A and B). Inmost examples, the lymphoid follicles are readily recog-nized, but a minority of cases require immunohistochem-istry to verify that the lesions are reactive rather thanlymphoma.35 Chlamydial proctitis may be a cause of somecases of florid lymphoid hyperplasia of the rectum.36
CLASSIFICATION OF GASTROINTESTINAL LYMPHOMAS
No separate classification for gastrointestinal lympho-mas is offered by the World Health Organization (WHO),although extranodal marginal zone lymphoma of MALT(including immunoproliferative small-intestinal disorder)and enteropathy-associated T-cell lymphoma form 2 dis-tinct categories among the mature B-, T- and natural killer(NK)–cell neoplasms.37,38 Isaacson39 previously proposeda classification of primary gastrointestinal non-Hodgkinlymphoma that comprised cases of both low-grade andhigh-grade MALT; however, the current WHO lymphomaclassification no longer uses such terminology, and cases ofhigh-grade MALT have been subsumed into the large B-celllymphoma category (Table 1).37,40
GASTROINTESTINAL B-CELL LYMPHOMAS,PREDOMINATELY NON-MALT
Most primary gastrointestinal lymphomas, both instomach and intestine and irrespective of their associationwith MALT, are large B-cell lymphomas, especially thosecomposed of centroblasts, but may also include casesdominated by immunoblasts and, on occasion, plasma-blasts. The relationship between the more common largeB-cell gastrointestinal lymphomas and the low-gradelymphomas of MALT is unclear. In a recent Germanmulticenter study of 398 cases of gastric lymphoma, 59.5%were large B-cell lymphomas of which 18.1% had asimultaneous small cell component compatible withderivation from MALT.40 This incidence is consonant with2 studies from the 1990s in which 17% to 21% of primarymalignant lymphomas of the stomach showed coexistence
of a low-grade and a high-grade lymphoma;41,42 it wassuggested that increased numbers of histologic sectionsmight demonstrate a still higher percentage of cases with alow-grade component. The terms low-grade MALToma andhigh-grade MALToma formerly were used to describe suchlesions, but, as discussed above, the diagnosis of MALTlymphoma currently is restricted to a lymphoma com-posed principally of small lymphocytes and should not beused to classify large B-cell lymphomas, including thoseassociated with a MALT component or arising in a MALTsite.37
The diagnosis of large B-cell lymphoma usually is nota problem because of the tendency of the lymphoma tobe diffuse, to lack cohesive cell aggregates, and to becomposed of cells that are approximately double the size ofnormal small lymphocytes with open vesicular chromatinand nucleoli, which are either adjacent to the nuclearmembrane or, in the case of immunoblasts, central andfrequently eosinophilic. In small endoscopic biopsy spec-imens, the diagnosis may be more tenuous, but immuno-histochemical verification of the diagnosis is advised and isparticularly valuable in delineating cases of large B-celllymphoma from undifferentiated gastrointestinal carcino-ma. The infiltration by lymphoma around, or into, partiallyintact gastric and intestinal glands, negative mucin andkeratin staining, positive reactivity for B-cell antigens suchas CD20, and the lack of syncytial cell aggregates ormalignant acinar formation aid in the distinction of largeB-cell lymphoma from poorly differentiated or undif-ferentiated carcinoma, even in small biopsy specimens(Figure 3, A and B). Occasionally, gastrointestinal large B-cell lymphoma requires distinction from other large cellmalignant neoplasms that simulate lymphoma, as forexample malignant melanoma and myeloid sarcoma.22
Small gastrointestinal biopsy specimens, however, areprone to sampling errors and artifactual distortion, and itmay be necessary to request a second biopsy in order todeliver a more complete diagnosis.
Mantle cell lymphoma is another type of non-MALTlymphoma found in the gastrointestinal tract that canpresent as a nonspecific lymphocytic infiltrate, but isbest known for presentation as multiple lymphomatouspolyposis.43,44 This is an unusual, but distinct, gastrointes-tinal lymphoma characterized by the polypoid accumula-tion of lymphoma involving long segments of the smalland large intestine.3 Lymphomatous polyposis has areported frequency of 4% to 9% among all gastrointestinalB-cell non-Hodgkin lymphomas.45 Patients generally aremiddle-aged males who present with weight loss, fatigue,diarrhea, abdominal pain, and often iron deficiency.44–46
The lymphoma forms a series of coalescing polypoid nod-ules composed of atypical centrocyte-type cells involvingmucosa and/or submucosa (Figure 4, A). Occasionally,reactive germinal centers are trapped in the nodularlymphomatous infiltrate and this observation aids inmorphologically distinguishing lymphomatous polyposisfrom follicular lymphoma of the gastrointestinal tract(Figure 4, B). The mantle cells in lymphomatous polyposisexhibit a characteristic CD20+, CD5+, CD232 phenotypeand cyclin D1 overexpression, as well as bcl-1 rearrange-ments with t(11;14)(q13;q32).46–48 Cases of intestinal mantlecell lymphoma also frequently contain the a4b7 mucosalhoming receptor.49 However, a subset of lymphomatouspolyposis cases are, in fact, follicular lymphomas andsuch cases appear limited to the small intestine, whereas
Table 1. Classification ofGastrointestinal Lymphomasa
B Cell
Extranodal marginal zone, MALT typeIPSID (heavy chain disease)
Others (lymph node equivalents)Mantle cell (lymphomatous polyposis)FollicularLarge B cell, NOS (,40% extranodal)Burkitt
T Cell
Enteropathy associated (EATL)Classic and type II
Others (non–enteropathy associated)NK/T, nasal typegdALCL
Abbreviations: ALCL, anaplastic large cell lymphoma; EATL, enteropathy-associated T-cell lymphoma; IPSID, immunoproliferative small intestinaldisease; MALT, mucosa-associated lymphoid tissue; NK, natural killer;NOS, not otherwise specified.a Reprinted and modified with permission from Isaacson.39
1286 Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke
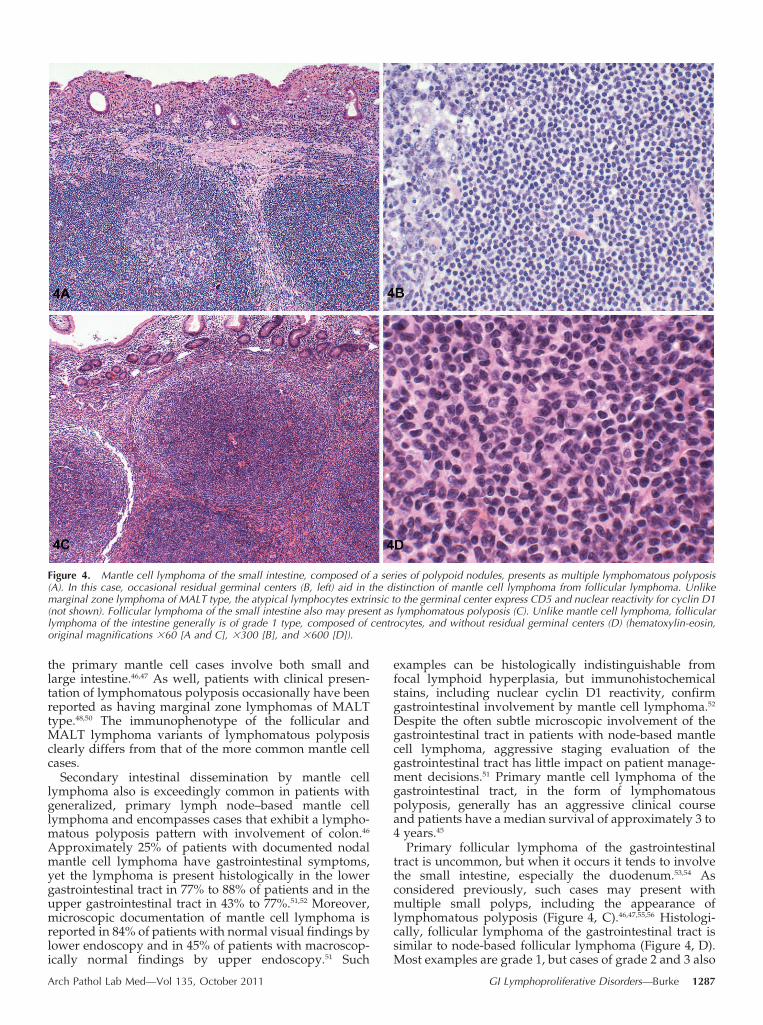
the primary mantle cell cases involve both small andlarge intestine.46,47 As well, patients with clinical presen-tation of lymphomatous polyposis occasionally have beenreported as having marginal zone lymphomas of MALTtype.48,50 The immunophenotype of the follicular andMALT lymphoma variants of lymphomatous polyposisclearly differs from that of the more common mantle cellcases.
Secondary intestinal dissemination by mantle celllymphoma also is exceedingly common in patients withgeneralized, primary lymph node–based mantle celllymphoma and encompasses cases that exhibit a lympho-matous polyposis pattern with involvement of colon.46
Approximately 25% of patients with documented nodalmantle cell lymphoma have gastrointestinal symptoms,yet the lymphoma is present histologically in the lowergastrointestinal tract in 77% to 88% of patients and in theupper gastrointestinal tract in 43% to 77%.51,52 Moreover,microscopic documentation of mantle cell lymphoma isreported in 84% of patients with normal visual findings bylower endoscopy and in 45% of patients with macroscop-ically normal findings by upper endoscopy.51 Such
examples can be histologically indistinguishable fromfocal lymphoid hyperplasia, but immunohistochemicalstains, including nuclear cyclin D1 reactivity, confirmgastrointestinal involvement by mantle cell lymphoma.52
Despite the often subtle microscopic involvement of thegastrointestinal tract in patients with node-based mantlecell lymphoma, aggressive staging evaluation of thegastrointestinal tract has little impact on patient manage-ment decisions.51 Primary mantle cell lymphoma of thegastrointestinal tract, in the form of lymphomatouspolyposis, generally has an aggressive clinical courseand patients have a median survival of approximately 3 to4 years.45
Primary follicular lymphoma of the gastrointestinaltract is uncommon, but when it occurs it tends to involvethe small intestine, especially the duodenum.53,54 Asconsidered previously, such cases may present withmultiple small polyps, including the appearance oflymphomatous polyposis (Figure 4, C).46,47,55,56 Histologi-cally, follicular lymphoma of the gastrointestinal tract issimilar to node-based follicular lymphoma (Figure 4, D).Most examples are grade 1, but cases of grade 2 and 3 also
Figure 4. Mantle cell lymphoma of the small intestine, composed of a series of polypoid nodules, presents as multiple lymphomatous polyposis(A). In this case, occasional residual germinal centers (B, left) aid in the distinction of mantle cell lymphoma from follicular lymphoma. Unlikemarginal zone lymphoma of MALT type, the atypical lymphocytes extrinsic to the germinal center express CD5 and nuclear reactivity for cyclin D1(not shown). Follicular lymphoma of the small intestine also may present as lymphomatous polyposis (C). Unlike mantle cell lymphoma, follicularlymphoma of the intestine generally is of grade 1 type, composed of centrocytes, and without residual germinal centers (D) (hematoxylin-eosin,original magnifications 360 [A and C], 3300 [B], and 3600 [D]).
Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke 1287
occur in the gastrointestinal tract;54,56 however, precisegrading may prove difficult in small biopsy specimens.The immunophenotype is identical to that of nodalfollicular lymphoma (CD20+, CD10+, bcl-6+, bcl-2+) andthe cases also exhibit t(14;18).53–56 In contrast to nodalfollicular lymphoma, the primary gastrointestinal casesfrequently express immunoglobulin A (IgA) as well as thea4b7 mucosal homing receptor, to suggest origin fromlocal antigen-experienced B-cells.57 Unlike nodal follicularlymphoma, duodenal follicular lymphoma also exhibitsVH4 gene deviation and lacks activation-induced cytidinedeaminase expression; moreover, its dendritic cell mesh-works tend to be disrupted.58,59 Follicular lymphoma of theduodenum additionally reveals ongoing hypermutationbut the mechanisms differ from those in nodal cases andare more in parallel with the antigen-dependent origin ofMALT lymphoma.59 Clinically, patients with primaryfollicular lymphomas of the gastrointestinal tract tend tohave low-stage IE and IIE disease. As compared to mantlecell lymphoma, gastrointestinal follicular lymphomaexhibits an indolent clinical course, with patient survivalof 62% or more at 5 years.54,56 Moreover, primary stage IEfollicular lymphoma of the duodenum is exceedinglyindolent and patients who are not treated usually do notdevelop extraintestinal spread, nor does the diseasetransform to large cell lymphoma, leading to the recom-mendation of a ‘‘watch and wait’’ approach.60
Immunoproliferative small intestinal disease (IPSID),formerly known as Mediterranean lymphoma or a heavychain disease, is an uncommon and unusual type ofgastrointestinal lymphoma that is included under theumbrella of MALT lymphoma in the current WHOclassification scheme.37 Immunoproliferative small intes-tinal disease mainly occurs in the Middle East and arisesin association with a morphologically benign-appearinginfiltrate, often characterized by a dense, plasma cellproliferation in the intestinal mucosa.39,61 As opposed tothe Western type of lymphoma commonly encountered inEurope and North America, IPSID tends to manifest asmalabsorption instead of obstruction, presents in theduodenum or proximal jejunum rather than distal ileum,and exhibits villous atrophy as well as plasma cellinfiltration of the adjacent intestine.61–63 Immunoprolifer-ative small intestinal disease is either a lymphoma ofMALT with a lymphoplasmacytic appearance or largecell, frequently immunoblastic plasmacytoid lymphomawith IgA heavy-chain restriction, which is related to aheavy chain disease with lack of the V region and lightchains.63–65 The discovery of benign-appearing follicles,together with lymphomatous cells that conform to thecentrocyte-like cells of MALT, add credence to theclassification of IPSID as a form of extranodal marginalcell lymphoma of MALT type developing in mucosa-associated lymphoid tissue of the small intestine.37,64–66 Theexact antigenic stimulus to form reactive follicles in IPSIDis unknown, but recent molecular and immunohistochem-ical studies demonstrate a proposed association withCampylobacter jejuni, although this relationship remainstenuous.65,67,68 Patients at an early stage of mucosalinvolvement frequently respond to antibiotics, whereaspatients whose disease evolves to large cell lymphoma,specifically the immunoblastic variant, classically have abetter median survival than Western patients with denovo large B-cell lymphoma of the intestine.61,62,65
GASTROINTESTINAL T-CELL LYMPHOMAS,PREDOMINATELY ENTEROPATHY ASSOCIATED
Most malignant lymphomas that complicate the diagno-sis of celiac sprue are not IPSIDs but rather T-celllymphomas. These cases have been designated as ‘‘enter-opathy-associated T-cell lymphoma’’ (EATL) and they arecharacterized by prominent intramucosal lymphomatousspread and villous atrophy of uninvolved mucosa (Figure 5,A).38,69 T-cell lymphomas unassociated with malabsorptionalso develop in the intestine and cases may simulate thehistologic pattern of EATL.69,70 T-cell lymphomas caninvolve any part of the gastrointestinal tract especially inpatients in the Far East, and whereas some cases may beexamples of EATL, the Far East is nonendemic for celiacdisease and most cases in this geographic region areperipheral T-cell lymphomas, not otherwise specified(NOS), NK/T-cell lymphomas of nasal type, and caseslinked with the human T-cell lymphotropic virus type 1.71–76
In the current WHO classification, EATL is divided into2 forms. Patients with the first variant have features ofceliac disease and may present with abdominal pain andeven small intestinal perforation.38 The lymphomatousnature of the intestinal infiltrate usually is obvious, but thecases are cytologically mutable, ranging from casescontaining neoplastic large cells with conspicuous nucle-oli; cases with pleomorphic, multinucleated cells; andcases dominated by small to medium-sized lymphocytes(Figure 5, B).69,70,77 Most examples of this type of EATLexhibit necrosis and infiltration by inflammatory cells,specifically histiocytes and eosinophils, which can obscurethe lymphoma.20 Although occasionally subtle, the intes-tinal mucosa adjacent to the main tumor mass frequentlyexhibits enteropathy with villous atrophy, crypt hyper-plasia, increased inflammatory cells in the lamina propria,as well as intraepithelial lymphocytosis.38,77–79
Unlike the primary form of EATL, the type II varietyexhibits villous atrophy, blunting, and intraepithelial lym-phocytosis that is usually confined to the area of lymphomaand perhaps adjacent mucosa (Figure 5, C), whereas themore distant nonlymphomatous mucosa is effectivelyunremarkable and without villous atrophy.78 Despiteinclusion as a form of EATL, paradoxically, most patientswith type II disease do not have a history of celiac disease.The morphologic features of the lymphoma also differ, asthe lymphomas in the type II cases tend to be more homo-geneous and are composed of small to medium-sizedlymphocytes with slightly irregular nuclei and smallnucleoli surrounded by a rim of pale or clear cytoplasm(Figure 5, D).38,78 The type II form of EATL usuallyexpresses CD8 and CD56 in contrast to expression of CD8in only 20% and CD56 in fewer than 10% of cases of themore classic form of EATL.38 Both forms exhibit commongenetic abnormalities with complex segmental gains of the9q31.3 chromosomal region or with deletions in 16q12.1.80,81
Alternatively, the classic form of EATL associated withceliac disease frequently has chromosomal gains in 1q and5q, whereas the type II variant is often characterized by8q24 (MYC) amplifications.81,82 The HLA haplotypes alsodiffer. Like patients with celiac disease, more than 90% ofpatients with the first type of EATL share the HLA-DQ2/-DQ8 genotype, while the genotype found in type II EATL ismore akin to that of normal white populations.38,82
In Northern Europe, EATL generally is regarded as acomplication of celiac disease, but in some patients no
1288 Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke

Figure 5. Enteropathy-associated T-cell lymphoma (EATL) in a patient with celiac disease results in infiltration of the adjacent small intestinalmucosa with associated villous atrophy (A). The neoplastic T cells in EATL are frequently pleomorphic (B). In type II EATL, the neoplastic T cells alsoinvade the adjacent mucosa, leading to villous blunting (C). The neoplastic T cells in the type II variant tend to be of medium size and are relativelyhomogenous (D). In the latter case, the neoplastic T cells expressed CD8 and CD56 versus the usual lack of reactivity for these antigens in classicEATL (not shown). EATL must be distinguished from NK-cell enteropathy, a newly described entity in which atypical cells infiltrate the laminapropria and encircle residual colonic glands (E). Despite the significant atypia, patients with NK-cell enteropathy experience a benign clinical course(hematoxylin-eosin, original magnifications 360 [A], 3600 [B and D], 3150 [C], and 320/0.75NA [E]). E, Reproduced with permission fromMansoor et al94 and courtesy of Elaine S. Jaffe, MD, Chief, Hematopathology Section, Laboratory of Pathology, Center for Cancer Research, NationalCanter Institute, Bethesda, Maryland.
Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke 1289

history of malabsorption exists and villous atrophy andcrypt hyperplasia are discovered only at the time oflymphoma resection. Isaacson and Du20 and Ashton-Keyand associates83 have demonstrated that EATL may bepreceded by refractory celiac disease frequently associatedwith ulcers and referred to as ‘‘ulcerative jejunitis.’’Polymerase chain reaction and sequence analysis showedthat ulcerative lesions and unremarkable, normal-appear-ing intraepithelial lymphocytes share the identical mono-clonal T-cell receptor rearrangement as the adjacentlymphoma. In refractory celiac disease, the intraepitheliallymphocytes may exhibit a normal CD3+, CD8+ immuno-phenotype, but they often are phenotypically anomalouswith loss of surface CD3, and usually CD8, and alsocytogenetically anomalous with partial trisomy of the 1qregion in parallel to cases of EATL.79,84–86 Moreover, clonalT-cell gene rearrangements have been recorded in patientswith refractory celiac disease who do not present withlymphoma, and in cases in which EATL later develops, theidentical clone can be detected in the lymphoma.79,83,84,85,87
Such cases are regarded as ‘‘cryptic EATL’’ (EATL in situ)and patients with refractory celiac disease require contin-ual monitoring of both intraepithelial lymphocyte immu-nophenotype and clonality because of the significant riskof the disease evolving to EATL.38,83,84,87,88
The differential diagnosis of EATL includes not onlylarge B-cell lymphoma of intestine, but also other forms ofT-cell lymphoma including peripheral T-cell lymphomaNOS, anaplastic large cell lymphoma, and extranodal NK/T-cell lymphoma, nasal type.69,72,74,77 For example, theextranodal NK/T-cell lymphomas of nasal type thatpresent in intestine exhibit the usual broad cytologicspectrum of that form of lymphoma, ranging from smallto intermediate-size to large cells with marked nuclearpleomorphism.74,89–91 The adjacent mucosa does not exhibitvillous atrophy. The lymphoma frequently demonstratesulceration, angiocentricity, and angioinvasion with fibri-noid and coagulative necrosis.74,89–91 Phenotypically, theextranodal NK/T-cell lymphomas of nasal type expresscytoplasmic, but not surface, CD3 and similar to type IIEATL, they show TIA-1 and CD56 positivity.74,89,90 Unlikethe type II form of EATL, the extranodal NK/T-celllymphomas generally are CD82 and also are negative forbF1. Most importantly, the NK/T-cell lymphomas of nasaltype are Epstein-Barr virus positive as opposed toEATL.74,89–91 NK/T-cell lymphomas are clinically aggres-sive and the extranasal cases, encompassing those in thegastrointestinal tract, convey a statistically significant evenworse prognosis.74,92 In general, patients with intestinalT-cell lymphoma fare worse that those with intestinalB-cell lymphoma.72,93
One caveat is that EATL and extranodal NK/T-celllymphoma must be distinguished from 2 similar, if notidentical, newly described entities, ‘‘NK-cell enteropathy’’or ‘‘lymphomatoid gastropathy,’’ especially in smallendoscopic biopsy specimens.94,95 Patients present witheither no or varying gastrointestinal symptoms, but haveno features of celiac or inflammatory bowel disease. Theatypical NK-cell infiltrates involve either single or multiplesites, including stomach, duodenum, small intestine, andcolon.96 At endoscopy, multiple superficial, discrete, flat orhemorrhagic lesions may be observed or small (less than1 cm), patchy, superficial ulcers are discovered.94–96 Biopsyspecimens demonstrate a diffuse, well-circumscribed, mu-cosal infiltrate of atypical intermediate to large lymphoid
cells with clear to eosinophilic cytoplasm and with inva-sion or destruction of mucosal glands (Figure 5, E).94–96
Acute inflammation may accompany the infiltrate. Theatypical lymphocytes express cytoplasmic, but not surface,CD3, as well as CD56 and TIA-1. Similar to true NK-celllymphomas of extranodal nasal type, the T-cell receptor inthe enteropathy cases is germline; but, in contrast to NKnasal-type lymphomas, studies for Epstein-Barr virususing Epstein-Barr virus–encoded RNA yield negativeresults.94–96 Of most significance, and as opposed to bothextranodal NK/T-cell lymphomas and EATL, patientswith NK-cell enteropathy pursue an uneventful clinicalcourse.94,95 The etiology of this syndrome is unknown.
GASTRIC LYMPHOMAS, ESPECIALLY MARGINAL ZONELYMPHOMAS OF MALT TYPE
The morphologic features of extranodal marginal zonelymphoma of MALT type have witnessed gradual changessince the initial descriptions by Isaacson and Wright.7,8
Although originally interpreted to be of follicular center cellorigin, the lymphoma cells of MALT were later designatedas ‘‘centrocyte-like’’ and currently are termed marginal zonecells.7,9,37 Gastric lymphomas of MALT type typically arecharacterized by an expansion of the marginal-like zonessurrounding benign germinal centers (Figure 6, A and B).Marginal zone cells comprise a variety of cell types rangingfrom small to intermediate-sized lymphocytes to large cells.The marginal zone or centrocyte-like cells are small tomedium-sized lymphocytes with variable nuclear mem-brane irregularities, resembling a centrocyte.20 Commonly,the marginal zone cells appear monocytoid with abundantpale-staining cytoplasm and well-delineated borders (Fig-ure 6, C).9 Other forms of gastric MALT resemble smalllymphocytes or are dominated by plasma cells to the extentof simulating a plasmacytoma. Signet ring–type cells alsoare described in gastric MALT lymphomas and appear torepresent a curious type of lymphoepithelial lesion inwhich the foveolar cells, disaggregated by the lymphoma-tous infiltrate, attain a globoid, signet ring–type appear-ance.97 Regardless of cytologic composition, the marginalzone cells of MALT cells share immunophenotypiccharacteristics. Gastric MALT lymphomas are B cellderived with CD20 expression and frequently containnumerous admixed CD3+ reactive T cells. Despite the B-cellphenotype, determination of monoclonality by immuno-peroxidase in fixed, paraffin-embedded tissue usually isnot possible with the exception of cases containing aconspicuous plasma cell component; however, up to 50% ofcases exhibit aberrant coexpression of CD43 that can provehelpful in diagnosis (Figure 6, D).20 Unlike chronic lym-phocytic leukemia/small lymphocytic lymphoma andmantle cell lymphoma, the lymphomas of MALT originusually lack CD5 and are without bcl-1 gene rearrange-ments.10,20 Mucosa-associated lymphoid tissue lymphomasdiffer from follicular lymphomas in that they are CD102
and do not exhibit bcl-2 rearrangements.98 The absence ofCD10 in gastric lymphoma with an apparent folliculararchitecture has been rationalized by the concept of‘‘follicular colonization.’’ 11 As noted earlier, follicularcolonization refers to the replication of follicular lymphomaas a result of invasion by the marginal zone cells of MALTinto preexisting reactive follicles (Figure 6, E and F).
The marginal zone cells of MALT invade not onlyresidual reactive follicles but also epithelium. Epithelialinvasion with frequent destruction by the B cells of MALT
1290 Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke

Figure 6. In classic extranodal marginal zone lymphoma of MALT type, the lymphoid infiltrate in stomach is often massive (A). Residual germinalcenters often are evident that are surrounded and encroached upon by the proliferating neoplastic marginal zone lymphocytes (B). The marginalzone lymphocytes exhibit irregular nuclear contours and frequently have pale-staining cytoplasm to impart a monocytoid appearance (C). Theneoplastic marginal zone B cells may aberrantly coexpress CD43 in contrast to the absence of CD43 expression in a residual germinal center seen atthe upper left (D). Gastric MALT lymphoma also may display a false follicular architecture (E) as the malignant marginal zone cells invade residualgerminal centers referred to as ‘‘follicular colonization’’ (F) (hematoxylin-eosin, original magnifications 360[A and E], 3150 [B], 3600 [C], and3300 [F]; immunoperoxidase, original magnification 3150 [D]).
Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke 1291

has been referred to as a ‘‘lymphoepithelial lesion’’ and isa vital morphologic attribute in the diagnosis of gastricMALT-derived lymphomas.8,9,34 An immunohistochemi-cal stain for cytokeratin usually accentuates these lesions.Lymphoepithelial lesions are most noteworthy as adiagnostic trait in the stomach, but are less germane inother extranodal sites, since they may be observed innonlymphomatous extranodal lymphocytic infiltrates.10,33
In stomach, lymphoepithelial lesions usually are definedas invasion of gastric epithelium by 3 or more lympho-matous B cells.20 A decade following the primary proposalfor a lymphoma of MALT, a histologic scoring system forgastric MALT lymphoma was proposed in which invasionof epithelial structures or lymphoepithelial lesions isconsidered paramount to the diagnosis (Table 2).12
With the scoring system, a definite diagnosis of low-grade B cell lymphoma of MALT is predicated on theexistence of a dense, diffuse infiltrate of centrocyte-likecells/marginal zone cells in the lamina propria withprominent lymphoepithelial lesions. Cases regarded assuspicious lymphocytic infiltrates are those in whichreactive follicles are surrounded by marginal zone cellsthat diffusely infiltrate into the lamina propria and intoepithelium in small groups.12 However, caution is re-quired as dense infiltrates, slight cytologic atypia, and alsolymphoepithelial-like lesions may be found in cases oflymphoid hyperplasia in the stomach. As well, the criteriamay be difficult to apply. In an interobserver study,99 17pathologists, including hematopathologists, gastrointesti-nal pathologists, and general pathologists, reviewed 41hematoxylin-eosin sections of stomach that ranged fromsimple gastritis to lymphoma. Interobserver reproducibil-ity was suboptimal and the degree of disagreement wasdirectly related to the experience of the pathologist inevaluating gastric biopsy specimens for MALT lesions.The study recommended that clinical information, exten-sive sampling, recognition of lymphoepithelial lesions,immunophenotypic information, and cytogenetic resultswould enhance diagnostic accuracy.99 This recommenda-tion was supported by another report100 stating that acombination of the morphologic scoring system and B cellclonality analysis by an advanced PCR method accuratelydiscriminated chronic gastritis from covert gastric mar-ginal zone lymphoma. Polymerase chain reaction wasparticularly valuable in the interpretation of cases thatexhibited an ambiguous score of grade 3 or 4.
Currently, it is well established that most gastricmarginal zone lymphomas of MALT arise in a setting of
‘‘acquired’’ MALT, whereby nonindigenous extranodallymphoid tissue is acquired secondary to H pyloriinfection.20,101,102 Ample epidemiologic, clinical, and histo-logic evidence effectively shows a fixed associationbetween gastric MALT lymphomas and H pylori infec-tion.12,19,20,103–105 For example, in a collaborative study ofmore than 230 000 patients whose serum had been stored,33 cases of gastric lymphoma developed in a median of14 years after serum collection.103 The patients with gastriclymphoma were significantly more likely than matchedcontrols to have evidence of previous H pylori infection. Incontrast, among 31 patients who developed nongastric,non-Hodgkin lymphoma, no association was discoveredbetween this lymphoma and previous H pylori infection.103
In addition, molecular analysis by PCR has documentedthe clonal progression from H pylori–associated chronicgastritis to MALT lymphoma of the stomach, and H pyloriprovides the antigenic stimulus for prolonging theclonal expansion of gastric MALT lymphomas.13,19,106 Ofmost significance, antibiotic treatment with obliteration ofH pylori usually leads to remission of gastric MALTlymphoma.12,18,20,21,107
Clinically, gastric MALT lymphomas arise in adultswith a peak in the seventh decade of life and with a maleto female ratio of approximately 1.5:1.34 Patients common-ly present with nonspecific gastritis and/or a peptic ulcerand at endoscopy, reddened and slightly thickened rugaeare often present with superficial spreading of lesionswithout formation of a tumor mass.18 The gastric lesionscommonly are multifocal and most patients have stage IEdisease.107,108 The link between H pylori and gastric MALTlymphoma led to antibiotic therapy for treatment of low-grade gastric lymphomas of MALT, and this therapyinduces sustained remissions in more than 75% ofpatients.21,107 Consequently, eradication of H pylori is therecommended primary therapy for almost all patientswith MALT lymphoma of stomach irrespective of stage oreven documentation of associated H pylori infection.109,110
With a gastric mapping procedure, an initial follow-upendoscopy is recommended at 3 to 6 months after therapyfor H pylori infection, and additional follow-up evalua-tions should be done at 4- to 6-month intervals for2 years.109,110 For patients monitored for up to 2 yearswhose disease remains refractory to H pylori therapy,other modalities, such as radiotherapy, chemotherapy,or combined treatment are offered; however, no consen-sus exists for the optimal treatment of primary gastriclymphoma unresponsive to H pylori therapy, particularly
Table 2. Gastric Marginal Zone (MALT) Lymphomas: Histologic Scoringa
Grade Description Histologic Features
0 Normal Plasma cells in LPNo lymphoid follicles
1 Chronic active gastritis Lymphocyte clusters in LPNo follicles, LELs
2 Chronic active gastritis with floridlymphoid follicle formation
Prominent follicles with surrounding mantle zone and plasma cellsNo LELs
3 Suspicious lymphoid infiltrate in LP,probably reactive
Follicles surrounded by lymphocytes that infiltrate diffusely in LPand +/2 epithelium
4 Suspicious lymphoid infiltrate in LP,probably lymphoma
Follicles surrounded by CCL cells (MZC) that infiltrate diffusely inLP and epithelium
5 Marginal zone (MALT) lymphoma Dense diffuse infiltrate of CCL cells in LP with prominent LELs
Abbreviations: CCL, centrocyte-like; LELs, lymphoepithelial lesions; LP, lamina propria; MALT, mucosa-associated lymphoid tissue; MZC, marginalzone cells.a Reprinted with permission from Wotherspoon et al.12
1292 Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke

with evidence of progressive lymphoma, although recentanalysis of pooled data proposed that radiotherapy maybe most appropriate in this setting.110–112 Overall, gastricMALT lymphoma is indolent and in one study of thislymphoma treated by various modalities, the 5-yearprojected overall survival was 82%.18
One significant issue for pathologists is the interpreta-tion of stomach biopsy specimens after antibiotic therapyfor gastric MALT lymphoma. Clearly, no diagnosticproblem exists if the biopsy specimen reveals regressionof the lymphoma with loss of lymphocytic aggregatesin the lamina propria (Figure 7, A) or if the specimenexhibits a total absence of histologic regression withpersistence of lymphoma. Parallel to the histologic scoringsystem used for the initial diagnosis of gastric marginalzone lymphoma, a histologic grading system has beenproposed for treated patients which evaluates not onlythe cellular infiltrate and lymphoepithelial lesions but alsostromal changes (Table 3).12,113 The probable minimaldisease category does not signify a requirement for furthertherapy and patients are managed with follow-up asthough they were in remission.21,110 For patients withresponding residual disease (Figure 7, B) or no change, cli-nical management consists of as discussed above, carefulfollow-up and a watch-and-wait approach for up to 2 yearsin the absence of disease progression.110
Of interest, approximately 50% of patients with histo-logically negative gastric biopsy findings after antibiotictherapy exhibit persistent monoclonality by PCR, al-though in some patients the clonality disappears withprolonged follow-up.114–116 For other patients, continuedmonoclonality may result in a delay in realizing remission.However, after antibiotic therapy for gastric MALTlymphoma, the association between ongoing monoclon-ality and risk of relapse is tenuous.117 One bone ofcontention is that serial gastric biopsy specimens fre-quently exhibit an oscillating clonal status, due perhaps tosampling or recurrent H pylori infection.21 Therefore,except for clinical investigations, the determination ofclonality with PCR currently is not considered pragmaticor recommended in the evaluation of posttherapy gastricMALT lymphoma biopsy specimens.21,110
The establishment of extranodal gastric marginal zonelymphoma of MALT type as a recognized clinicopathologicentity has progressed to incorporate molecular genetics andspecific chromosomal translocations. For MALT lymphomasin general, the genetic abnormalities encompass trisomies3, 12, and 18, as well as balanced translocations, specifi-cally t(11;18)(q21;q21), t(14;18)(q32;q21), t(1;14)(p22;q32), andt(3;14)(p14;q32).14–17,19–21,110,118,119 The most common transloca-tion in gastric MALT lymphoma arising in approximately20% to 30% of cases (although at a lower rate in NorthAmerica) is t(11;18)(q21;q21), which fuses the aminoterminal of the API2 gene (that encodes the inhibitor ofapoptosis) at 11q21 to the carboxyl terminal of MALT1 at18q21, leading to a chimeric fusion product.15,17,110 The API2-MALT1 fusion product is detectable by interphase fluores-cence in situ hybridization or reverse transcription-PCR (RT-PCR).21,110 MALT1 is involved in antigen receptor–mediatednuclear factor (NF)–kB activation and MALT lymphomasthat express the translocation exhibit enhanced expression ofNF-kB target genes, whereas MALT lymphomas withoutt(11;18)(q21;q21) support active inflammatory and immuneresponses.120 The t(11;18)(q21;q21) translocation is restrictedto extranodal MALT lymphomas and has not been reported
in other forms of marginal zone lymphoma, such as splenicor nodal, or in chronic gastritis associated with H pylori.121,122
Gastric MALT lymphomas without t(11;18)(q21;q21) oftenexhibit aneuploidy, for example, trisomy 3, 12, or 18.118,119,123
The discovery of t(11;18)(q21;q21) in some patients withgastric MALT lymphoma has led to exciting clinicalprognostic correlations. Specifically, gastric MALT lympho-ma in patients who prove positive for t(11;18)(q21;q21) oftenfails to respond to H pylori therapy, and this translocationfrequently arises in patients who are H pylori nega-tive.21,107,110,116,124–126 With endosonographic staging, sucht(11;18)(q21;q21)-positive patients whose condition doesnot respond to H pylori eradication with antibiotics mayhave lymphoma that has proliferated beyond the gastricsubmucosa into muscularis and/or serosa in contrast topatients with lymphoma limited to the mucosa and sub-mucosa who generally are t(11;18)(q21;q21) negative.16,21,25
Moreover, t(11;18)(q21;q21) is uncommon in extranodaldiffuse large B-cell lymphoma, and for patients harboringthis translocation, the disease rarely metamorphoses todiffuse large B-cell lymphoma.110,118,119 In contrast, patientswith aneuploidy, who are t(11;18)(q21;q21) negative withlymphoma unresponsive to H pylori treatment, are at risk ofhaving the disease evolve to diffuse large B-cell lymphoma.For example, microsatellite screening of gastric MALT andlarge B-cell lymphomas displays allelic imbalances limitedto t(11;18)(q21;q21)-negative patients, which are shared byboth MALT and diffuse large B-cell lymphomas;119 thisobservation advocates that the absence of t(11;18)(q21;q21)is the genesis of most MALT lymphomas that convert toone of large B-cell type.121 One recent report,127 however,deviated from this prevailing view by documentingt(11;18)(q21;q21) in 19% (6 of 31) of cases of gastric largeB-cell lymphoma. Further investigations obviously arerequired, but for patients whose condition does not respondto anti-H pylori therapy, it remains of interest to ascertainwhether or not the gastric marginal zone lymphoma ofMALT type is t(11;18)(q21;q21) positive, since this informa-tion carries prognostic and therapeutic repercussions.21
Nonetheless, routine determination of the t(11;18)(q21;q21)status is controversial since, from a clinical perspective,t(11;18)(q21;q21)-positive patients also are treated initiallyfor H pylori infection, and no definite data exist to indicatethat determining the status of t(11;18)(q21;q21) in the courseof follow-up has a direct bearing on therapeutic decisions.110
By current criteria, marginal zone lymphoma of MALTtype is strictly an indolent or low-grade extranodallymphoma. Despite the considerable recent emphasis onMALT-type lymphomas, in fact almost 60% of gastriclymphomas are diffuse large B-cell lymphomas.40 Asnoted previously, with the exception of small gastroscopicbiopsy specimens, differentiation of large cell lymphomafrom other large cell malignancies usually is not amorphologic issue, but, immunohistochemical verifica-tion is recommended.22 One consequential diagnosticissue is the observation of large cells in a background ofa marginal zone lymphoma of MALT type in a gastricbiopsy specimen. No current consensus prevails as to howmany large cells are required to establish the evolutionfrom MALT lymphoma to one of diffuse large B-cell type.Undoubtedly, the presence of large cells in discretenodular aggregates or sheets is likely an indication oftransformation;20,21,41 however, diagnostic difficulties en-sue for cases in which large cells are numerous anddiffusely admixed with small marginal zone lymphocytes.
Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke 1293

In one study of 106 patients with gastric MALT lympho-mas, the prognostic influence of a large cell componentwas assessed by semiquantitative analysis of clusters anddiffusely intermingled malignant large cells;128 in MALTlymphomas, the observation of a diffuse large cellcomponent in the range of 1% to 10%, with and withoutnonconfluent clusters of large cells, portended a signifi-cantly worse prognosis. Yet, in a report from Italy,129 thepresence of scattered large cells that comprised 5% to 10%of the MALT lymphoma cell population was regardedas prognostically irrelevant, whereas compact clusteredlarge cells that represented more than 10% of the MALTlymphoma proved significant, as they were associatedwith a worse survival. Cases of putative large B-celllymphoma in a background of gastric MALT lymphomatypically express bcl-6, but not CD10 and bcl-2.130
SUMMARY: A PRAGMATIC GUIDE TO DIAGNOSIS
How then does a surgical pathologist arrive at anaccurate diagnosis of suspected gastric marginal zonelymphoma, principally in light of the vagary of thehistologic scoring scheme?12,99 An appropriate integratedalgorithm and diagnostic recommendations have beenproposed, but the all-too-common issue of a gastric biopsyspecimen containing a solitary enlarged lymphocyticnodule composed of small lymphocytes without evidentgerminal centers remains ambiguous and a diagnosticconundrum (Figure 8).21,110 Such biopsy specimens evokea broad differential diagnosis ranging from gastritisto malignant lymphoma, which encompasses not onlyextranodal marginal zone lymphoma of MALT type butalso other lymphomas composed of small lymphocytes,including chronic lymphocytic leukemia/small lympho-cytic lymphoma, mantle cell lymphoma, and evenfollicular lymphoma. In this scenario, the foremost roleof the pathologist is vigilant assessment of the histologicfeatures by the conscious determination of whether anycytologic atypia exists, whether the cells appear monocyt-oid, whether plasma cells are increased, and whetherlymphoepithelial lesions are evident. Although morphol-ogy remains the standard for diagnosis, the morphologiccharacteristics require supplementation by an immuno-peroxidase panel, primarily CD20 and CD3, as well asCD43 and/or CD5, CD21, and possibly cytokeratin and, ifplasma cells are numerous, staining for k and l lightchains.131 Such staining will determine whether anaberrant immunophenotype is present, as for example,a predominance of CD20+ B cells, and whether the Blymphocytes exhibit coexpression with CD43 or CD5,whether the cytokeratin stain highlights lymphoepitheliallesions, whether occult germinal centers exist by positivereactivity for CD21 to imply follicular colonization, andwhether a monoclonal plasma cell population is evidentwith k or l light-chain restriction.11,20,25,32 For example, CD5coexpression should trigger staining for cyclin D1 toexclude mantle cell lymphoma. If the morphologic andimmunophenotypic study results in this setting arestrongly suggestive of, but not absolutely diagnostic of,
Figure 7. Biopsy specimens of gastric MALT lymphoma after therapyfor Helicobacter pylori infection. In one example, no residuallymphoma is present and the lamina propria contains only scatteredinflammatory cells affiliated with mild stromal fibrosis (A). In anothercase, the lymphocytic infiltrate is less than that seen originally, butatypical lymphocytes linger, corresponding to responding residualdisease (rRD) with lymphoepithelial lesions present on the right andbottom (B) (hematoxylin-eosin, original magnifications 3300 [A and B]).
Figure 8. A gastric biopsy specimen contains an enlarged lympho-cytic nodule composed of small lymphocytes without apparentgerminal centers. The differential diagnosis encompasses lymphoidhyperplasia and malignant lymphomas, specifically gastric MALTlymphoma as well as chronic lymphocytic leukemia/small lymphocytic
r
lymphoma, mantle cell lymphoma, and follicular lymphoma. Diagnosisrequires integration of histopathology, immunophenotype analysis, andeven molecular and cytogenetic features (hematoxylin-eosin, originalmagnification 360).
1294 Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke

gastric MALT lymphoma, molecular studies using PCRalso can be requested.12,100,110 In this scenario, interpreta-tion of the histologic, immunophenotypic, and molecularstudies must be placed in context of the clinical milieu,particularly with the awareness that chronic activegastritis may exhibit immunoglobulin gene rearrange-ments without features of clinical malignant lymphoma infollow-up studies.29,30,131 Because of this fact and becauseambiguous cases can be treated and usually respond totherapy for H pylori, some are of the opinion that routinePCR analysis is unnecessary.132 However, our practiceprefers to be as resolute as possible in establishing a diag-nosis; thus, discovery of a positive B-cell gene rearrange-ment by PCR is beneficial in the instance of an equivocallymphocytic infiltrate.100 If the PCR study results provenegative, the possibility of lymphoma in the ambivalentlymphocytic infiltrate persists so that a descriptive diag-nosis is required and, depending on the clinical features,so is a call for repeated biopsy with reservation of freshtissue to determine clonality, whether by flow cytometryor snap freezing, with suitable immunoperoxidase stud-ies. Although flow cytometry may not be a routine pro-cedure for investigating gastric biopsy specimens, it is avaluable technique for rapidly demonstrating clonalityand securing an absolute diagnosis.28 At the time of arepeated biopsy, at least 10 samples are submitted withoutfixative from abnormal-appearing gastric mucosa.110 Afterobtaining and interpreting touch imprints from severalbiopsy fragments, the multiple biopsy specimens aretriaged, with submission of pooled samples to flowcytometry and the remainder for routine microscopy withfixation in B5 and/or formalin. Molecular studies also canbe requested at this stage if the new biopsy findingsremain suspicious and the flow cytometry and/or snapfrozen–tissue studies prove ineffective. Should the newbiopsy specimen be successful in providing a definitivediagnosis of gastric MALT lymphoma, but withoutevidence of H pylori, then detection of t(11;18)(q21;q21)by fluorescence in situ hybridization or reverse transcrip-tion-PCR remains an option and can also aid in diagno-sis.21,110,133 Despite these additional ancillary studies, thediagnosis may still remain unresolved. Since significanttherapeutic consequences exist in rendering a verdict ofextranodal marginal zone lymphoma of MALT type, in asetting of uncertainty, a more fitting, noncommittal diag-nosis might be an ‘‘atypical lymphocytic infiltrate of un-certain malignant potential.’’ 22,134,135 Regardless of theterminology, it remains incontrovertible that the diagnosisof gastric marginal zone MALT lymphoma depends on
adherence to exacting pathologic criteria augmentedby immunophenotypic and judicious molecular and/orcytogenetic studies.
References
1. Graves FD, Linet MS, Travis LB, Devesa SS. Cancer surveillance series: non-Hodgkin’s lymphoma incidence by histologic subtype in the United States from1978 through 1995. J Natl Cancer Inst. 2000;92(15):1240–1251.
2. Knowles DM, Chamulak GA, Subar M, et al. Lymphoid neoplasiaassociated with the acquired immunodeficiency syndrome (AIDS): the NewYork University Medical Center experience with 105 patients (1981–1986). AnnIntern Med. 1988;108(5):744–753.
3. Shepherd, NA, Hall PA, Coates PJ, Levison DA. Primary malignantlymphoma of the colon and rectum: a histopathological and immunohistochem-ical analysis of 45 cases with clinicopathological correlations. Histopathology.1988;12(3):235–252.
4. Askling J, Brandt L, Lapidus A, et al. Risk of haematopoietic cancer inpatients with inflammatory bowel disease. Gut. 2005:54(5):617–622.
5. Koch P, del Valle F, Berdel W, et al. Primary gastrointestinal non-Hodgkin’slymphoma, I: anatomic and histologic distribution, clinical features, and survivaldata of 371 patients registered in the German multicenter study GIT NHL 01/92.J Clin Oncol. 2001;19(18):3861–3873.
6. Luminari S, Cesaretti M, Marcheselli L, et al. Decreasing incidence ofgastric MALT lymphomas in the era of anti-Helicobacter pylori interventions:results from a population-based study on extranodal marginal zone lymphomas.Ann Oncol. 2010;21(4):855–859.
7. Isaacson P, Wright DH. Malignant lymphoma of mucosa-associated lymphoidtissue: a distinctive type of B-cell lymphoma. Cancer. 1983;52(8):1410–1416.
8. Isaacson P, Wright DH. Extranodal malignant lymphoma arising frommucosa-associated lymphoid tissue. Cancer. 1984;53(11):2515–2524.
9. Isaacson PG, Spencer J. Malignant lymphoma of mucosa-associatedlymphoid tissue. Histopathology. 1987;11(5):445–462.
10. Isaacson PG. Lymphomas of mucosa-associated lymphoid tissue (MALT).Histopathology. 1990;16(6):617–619.
11. Isaacson PG, Wotherspoon AC, Pan L. Follicular colonization in B-celllymphoma of mucosa-associated lymphoid tissue. Am J Surg Pathol. 1991;15(9):819–828.
12. Wotherspoon AC, Doglioni C, Diss TC, et al. Regression of primary low-grade B-cell gastric lymphoma of mucosa-associated lymphoid tissue type aftereradication of Helicobacter pylori. Lancet. 1993;342(8871):575–577.
13. Du M, Diss TC, Xu C, Peng H, Isaacson PG, Pan L. Ongoing mutation inMALT lymphoma immunoglobulin gene suggests that antigen stimulation plays arole in the clonal expansion. Leukemia. 1996;10(7):1190–1197.
14. Wotherspoon AC, Finn TM, Isaacson PG. Trisomy 3 in low-grade B-celllymphomas of mucosa-associated lymphoid tissue. Blood. 1995;85(8):2000–2004.
15. Auer IA, Gascoyne RD, Connors JM, et al. t(11;18)(q21;q21) is the mostcommon translocation in MALT lymphomas. Ann Oncol. 1997;8(10):979–985.
16. Liu H, Ye H, Dogan A, et al. t(11;18)(q21;q21) is associated with advancedmucosa-associated lymphoid tissue lymphoma that expresses nuclear BCL10.Blood. 2001;98(4):1182–1187.
17. Remstein ED, Dogan A, Einerson RR, et al. The incidence and anatomicsite specificity of chromosomal translocations in primary extranodal marginalzone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma)in North America. Am J Surg Pathol. 2006;30(12):1546–1553.
18. Zucca E, Bertoni F, Roggero E, Cavalli F. The gastric marginal zone B-celllymphoma of MALT type. Blood. 2000;96(2):410–419.
19. Isaacson PG, Du MQ. MALT lymphoma: from morphology to molecules.Nat Rev Cancer. 2004;4(8):644–653.
20. Isaacson PG, Du MQ. Gastrointestinal lymphoma: where morphologymeets molecular biology. J Pathol. 2005;205(2);255–274.
21. Bacon CM, Du MQ, Dogan A. Mucosa-associated lymphoid tissue (MALT)lymphoma: a practical guide for pathologists. J Clin Pathol. 2007;60(4):361–372.
Table 3. Gastric Marginal Zone (MALT) Lymphoma: Posttherapy Gradinga
Score Lymphoid Infiltrate LELs Stromal Changes
CR Absent or scattered plasma cells and smalllymphoid cells in the LP
2 Normal or empty LP and/or fibrosis
pMRD Aggregates of lymphoid cells or lymphoidnodules in the LP/muscularis mucosa and/or submucosa
2 Empty LP and/or fibrosis
rRD Dense, diffuse, or nodular extending aroundglands in the LP
+/2 Focal empty LP and/or fibrosis
NC Dense, diffuse, or nodular +/2 No changes
Abbreviations: CR, complete histologic remission; LELs, lymphoepithelial lesions; LP, lamina propria; MALT, mucosa-associated lymphoid tissue;NC, no change; pMRD, probable minimal residual disease; rRD, responding residual disease; 2, absent; +/2, present or absent.a Reprinted with permission from Copie-Bergman et al.113
Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke 1295

22. Burke JS. Extranodal hematopoietic/lymphoid disorders: an introduction.Am J Clin Pathol. 1999;111(suppl 1):S40–S45.
23. Saltzstein SL. Extranodal malignant lymphomas and pseudolymphomas.Pathol Annu. 1969;4:159–184.
24. Burke JS. Histologic criteria for distinguishing between benign and malignantextranodal lymphoid infiltrates. Semin Diagn Pathol. 1985;2(3):152–162.
25. Burke JS. Are there site-specific differences among the MALT lympho-mas—morphologic, clinical? Am J Clin Pathol. 1999;111(suppl 1):S133–S143.
26. Kurtin PJ. How do you distinguish benign from malignant extranodal smallB-cell proliferations? Am J Clin Pathol. 1999;111(suppl 1):S119–S126.
27. Abbondanzo SL, Sobin LH. Gastric ‘‘pseudolymphoma’’: a retrospectivemorphologic and immunophenotypic study of 97 cases. Cancer. 1997;79(9):1656–1663.
28. Almasri NM, Zaer FS, Iturraspe JA, Braylan RC. Contribution of flowcytometry to the diagnosis of gastric lymphomas in endoscopic biopsyspecimens. Mod Pathol. 1997;10(7):650–656.
29. Hsi ED, Greenson JK, Singleton TP, Siddiqui J, Schnitzer B, Ross CW.Detection of immunoglobulin heavy chain gene rearrangement by polymerasechain reaction in chronic active gastritis associated with Helicobacter pylori.Hum Pathol. 1996;27(3):290–296.
30. Wundisch T, Neubauer A, Stolte M, Ritter M, Thiede C. B-cellmonoclonality is associated with lymphoid follicles in gastritis. Am J SurgPathol. 2003;27(7):882–887.
31. Carney JA. Gastric mucosal lymphoid follicles: histology, distribution,frequency, and etiologic features. Am J Surg Pathol. 2010;34(7):1019–1024.
32. Isaacson PG. Gastrointestinal lymphomas of T- and B-cell types. ModPathol. 1999;12(2):151–158.
33. Rubin A, Isaacson PG. Florid reactive lymphoid hyperplasia of the terminalileum in adults: a condition bearing a close resemblance to low-grade malignantlymphoma. Histopathology. 1990;17(1):19–26.
34. Isaacson PG, Norton AJ. Extranodal Lymphomas. Edinburgh, Scotland:Churchill Livingstone; 1994.
35. Farris AB, Lauwers GY, Ferry JA, Zukerberg LR. The rectal tonsil: a reactivelymphoid proliferation that may mimic lymphoma. Am J Surg Pathol. 2008;32(7):1075–1079.
36. Cramer SF, Romansky S, Hulbert B, Raugh S, Papp JR, Casiano-Colon AE.The rectal tonsil—a reaction to chlamydial infection [letter]? Am J Surg Pathol.2009;33(3):483–485.
37. Isaacson PG, Chott A, Nakamura S, Muller-Hermelink HK, Harris NL,Swerdlow SH. Extranodal marginal zone lymphoma of mucosa-associatedlymphoid tissue (MALT lymphoma). In: Swedlow SH, Campo E, Harris NL,et al, eds. Haematopoietic and Lymphoid Tissues. Lyon, France: IARC Press;2008:214–217. World Health Organization Classification of Tumours. 4th ed.
38. Isaacson PG, Chott A, Ott G, Stein H. Enteropathy-associated T-celllymphoma. In: Swedlow SH, Campo E, Harris NL, et al, eds. Haematopoietic andLymphoid Tissues. Lyon, France: IARC Press; 2008:289–291. World HealthOrganization Classification of Tumours. 4th ed.
39. Isaacson PG. Gastrointestinal lymphoma. Hum Pathol. 1994;25(10):1020–1029.
40. Koch P, Probst A, Berdel W, et al. Treatment results in localized primarygastric lymphoma: data of patients registered within the German multicenterstudy (GIT NHL 02/96). J Clin Oncol. 2005;23(28):7050–7059.
41. Chan JK, Ng CS, Isaacson PG. Relationship between high-grade lymphomaand low-grade B-cell mucosa-associated lymphoid tissue lymphoma (MALToma)of the stomach. Am J Pathol. 1990;136(5):1153–1164.
42. Cogliatti SB, Schmid U, Schumacher U, et al. Primary B-cell gastriclymphoma: a clinicopathological study of 145 patients. Gastroenterology. 1991;101(5):1159–1170.
43. Isaacson PG, Maclennan KA, Subbuswamy SG. Multiple lymphomatouspolyposis of the gastrointestinal tract. Histopathology. 1994;8(4):641–656.
44. O’Briain DS, Kennedy MJ, Daly PA, et al. Multiple lymphomatouspolyposis of the gastrointestinal tract: a clinicopathologically distinctive form ofnon-Hodgkin’s lymphoma of B-cell centrocytic type. Am J Surg Pathol. 1989;13(8):691–699.
45. Ruskone-Fourmestraux A, Audouin J. Primary gastrointestinal tract mantlecell lymphoma as multiple lymphomatous polyposis. Best Pract Res ClinGastroenterol. 2010;24(1):35–42.
46. Moynihan MJ, Bast MA, Chan WC, et al. Lymphomatous polyposis: aneoplasm of either follicular mantle or germinal center cell origin. Am J SurgPathol. 1996;20(4):442–452.
47. Kumar S, Krenacs L, Otsuki T, et al. bcl-1 rearrangement and cyclin D1protein expression in multiple lymphomatous polyposis. Am J Clin Pathol. 1996;105(6):737–743.
48. Kodama T, Ohshima K, Nomura K, et al. Lymphomatous polyposis of thegastrointestinal tract, including mantle cell lymphoma, follicular lymphoma andmucosa-associated lymphoid tissue lymphoma. Histopathology. 2005;47(5):467–478.
49. Geissmann F, Ruskone-Fourmestraux A, Hermine O, et al. Homingreceptor a4b7 integrin expression predicts digestive tract involvement in mantlecell lymphoma. Am J Pathol. 1998;153(6):1701–1705.
50. Yatabe Y, Nakamura S, Nakamura T, et al. Multiple polypoid lesions ofprimary mucosa-associated lymphoid tissue lymphoma of colon. Histopathology.1998;32(2):116–125.
51. Romaguera JE, Medeiros LJ, Hagemeister FB, et al. Frequency ofgastrointestinal involvement and its clinical significance in mantle celllymphoma. Cancer. 2003;97(3):586–691.
52. Salar A, Juanpere N, Bellosillo B, et al. Gastrointestinal involvement inmantle cell lymphoma: a prospective, clinic, endoscopic, and pathologic study.Am J Surg Pathol. 2006;30(10):1274–1280.
53. Yoshino T, Miyake K, Ichimura K, et al. Increased incidence of follicularlymphoma in the duodenum. Am J Surg Pathol. 2000;24(5):688–693.
54. Shia J, Teruya-Feldstein J, Pan D, et al. Primary follicular lymphoma of thegastrointestinal tract: a clinical and pathologic study of 26 cases. Am J SurgPathol. 2002;26(2):216–224.
55. LeBrun DP, Kamel OW, Cleary ML, Dorfman RF, Warnke RA. Follicularlymphomas of the gastrointestinal tract: pathologic features in 31 cases and bcl-2oncogenic protein expression. Am J Pathol. 1992;140(6):1327–1335.
56. Damaj G, Verkarre V, Delmer A, et al. Primary follicular lymphoma of thegastrointestinal tract: a study of 25 cases and a literature review. Ann Oncol.2003;14(4):623–629.
57. Bende RJ, Smit LA, Bossenbroek JG, et al. Primary follicular lymphoma ofthe small intestine: a4b7 expression and immunoglobulin configuration suggestan origin from local antigen-presenting cells. Am J Pathol. 2003;162(1):105–113.
58. Sato Y, Ichimura K, Tanaka T, et al. Duodenal follicular lymphomas sharecommon characteristics with mucosa-associated lymphoid tissue lymphomas.J Clin Pathol. 2008;61(3):377–381.
59. Takata K, Sato Y, Nakamura N, et al. Duodenal and nodal follicularlymphomas are distinct: the former lacks activation-induced cytidine deaminaseand follicular dendritic cells despite ongoing somatic hypermutations. ModPathol. 2009;22(7):940–949.
60. Schmatz AI, Streubel B, Kretschmer-Chott E, et al. Primary follicularlymphoma of the duodenum is a distinct mucosal/submucosal variant of follicularlymphoma: a retrospective study of 63 cases. J Clin Oncol. 2011;29(11):1445–1451.
61. Galian A, Lecestre MJ, Scotto J, Bognel C, Matuchansky C, Rambaud JC.Pathological study of alpha-chain disease, with special emphasis on evolution.Cancer. 1977;39(5):2081–2101.
62. Lewin KJ, Kahn LB, Novis BH. Primary intestinal lymphoma of ‘‘Western’’and ‘‘Mediterranean’’ type, alpha chain disease and massive plasma cellinfiltration: a comparative study of 37 cases. Cancer. 1976;38(6):2511–2528.
63. Nassar VH, Salem PA, Shahid MJ, et al. ‘‘Mediterranean abdominallymphoma’’ or immunoproliferative small intestinal disease, part II: pathologicalaspects. Cancer. 1978;41(4):1340–1354.
64. Isaacson PG, Dogan A, Price SK, Spencer J. Immunoproliferative small-intestinal disease: an immunohistochemical study. Am J Surg Pathol. 1989;13(12):1023–1033.
65. Al-Saleem T, Al-Mondhiry H. Immunoproliferative small intestinal disease(IPSID): a model for mature B-cell neoplasms. Blood. 2005;105(6):2274–2280.
66. Price SK. Immunoproliferative small intestinal disease: a study of 13 caseswith alpha heavy-chain disease. Histopathology. 1990;17(1):7–17.
67. Lecuit M, Abachin E, Matin A, et al. Immunoproliferative small intestinaldisease associated with Campylobacter jejuni. N Engl J Med. 2004;350(3):239–248.
68. Parsonnet J, Isaacson PG. Bacterial infection and MALT lymphoma. N EnglJ Med. 2004;350(3):213–215.
69. Chott A, Dragosics B, Radaszkiewicz T. Peripheral T-cell lymphomas ofthe intestine. Am J Pathol. 1992;141(6):1361–1371.
70. Domizio P, Owen RA, Shepherd NA, Talbot IC, Norton AJ. Primarylymphoma of the small intestine: a clinicopathological study of 119 cases. Am JSurg Pathol. 1993;17(5):429–442.
71. Tokunaga O, Watanabe T, Shimamoto Y, Tokudome S. Primary T-celllymphoma of the gastrointestinal tract associated with human T-cell lymphotro-pic virus type I: an analysis using in situ hybridization and polymerase chainreaction. Cancer. 1993;71(3):708–716.
72. Kohno S, Ohshima K, Yoneda S, Kodama T, Shirakusa T, Kikuchi M.Clinicopathological analysis of 143 primary malignant lymphomas in the smalland large intestines based on the new WHO classification. Histopathology. 2003;43(2):135–143.
73. Tung CL, Hsieh PP, Chang JH, Chen RS, Chen YJ, Wang JS. Intestinal T-celland natural killer-cell lymphomas in Taiwan with special emphasis on 2 distinctcellular types: natural killer-like cytotoxic T cell and true natural killer cell. HumPathol. 2008;39(7):1018–1025.
74. Chuang SS, Chang ST, Chuang WY, et al. NK-cell lineage predicts poorsurvival in primary intestinal NK-cell and T-cell lymphomas. Am J Surg Pathol.2009;33(8):1230–1240.
75. Ko YH, Karnan S, Kim KM, et al. Enteropathy-associated T-celllymphoma—a clinicopathologic and array comparative genomic hybridizationstudy. Hum Pathol. 2010;41(9):1231–1237.
76. Takeshita M, Nakamura S, Kikuma K, et al. Pathological and immunohis-tological findings and genetic aberrations of intestinal entropathy-associated Tcell lymphoma in Japan. Histopathology. 2011;58(3):395–407.
77. Chott A, Vesely M, Simonitsch I, Mosberger I, Hanak H. Classification ofintestinal T-cell neoplasms and their differential diagnosis. Am J Clin Pathol.1999;111(suppl 1):S68–S74.
78. Chott A, Haedicke W, Mosberger I, et al. Most CD56+ intestinallymphomas are CD8+CD52 T-cell lymphomas of monomorphic small to mediumsize histology. Am J Pathol. 1998;153(5):1483–1490.
79. Bagdi E, Diss TC, Munson P, Isaacson PG. Mucosal intra-epitheliallymphocytes in enteropathy-associated T-cell lymphoma, ulcerative jejunitis, andrefractory celiac disease constitute a neoplastic population. Blood. 1999;94(1):260–264.
1296 Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke

80. Zettl A, Ott G, Makulik A, et al. Chromosomal gains at 9q characterizeenteropathy-type T-cell lymphoma. Am J Pathol. 2002;161(5):1635–1645.
81. Zettl A, deLeeuw R, Haralambieva E, Mueller-Hermelink HK. Enteropathy-type T-cell lymphoma. Am J Clin Pathol. 2007;127(5):701–706.
82. Deleeuw RJ, Zettl A, Klinker E, et al. Whole-genome analysis and HLAgenotyping of enteropathy-type T-cell lymphoma reveals 2 distinct lymphomasubtypes. Gastroenterology. 2007;132(5):1902–1911.
83. Ashton-Key M, Diss TC, Pan L, Du MQ, Isaacson PG. Molecular analysisof T-cell clonality in ulcerative jejunitis and enteropathy-associated T-celllymphoma. Am J Pathol. 1997;151(2):493–498.
84. Cellier C, Delabesse E, Helmer C, et al. Refractory sprue, coeliac disease,and enteropathy-associated T-cell lymphoma. Lancet. 2000;356(9225):203–208.
85. de Mascarel A, Belleannee G, Stanislas S, et al. Mucosal intraepithelial T-lymphocytes in refractory celiac disease: a neoplastic population with a variableCD8 phenotype. Am J Surg Pathol. 2008;32(5):744–751.
86. Verkarre V, Romana SP, Cellier C, et al. Recurrent partial trisomy 1q22-q44 in clonal intraepithelial lymphocytes in refractory celiac sprue. Gastroen-terology. 2003;125(1):40–46.
87. Carbonnel F, Grollet-Bioul L, Brouet JC, et al. Are complicated forms ofceliac disease cryptic T-cell lymphomas? Blood. 1998;92(10):3879–3886.
88. Liu H, Bris R, Lavergne-Slove A, et al. Continual monitoring of intraepitheliallymphocyte immunophenotype and clonality is more important than snapshotanalysis in the surveillance of refractory celiac disease. Gut. 2010; 59(4):452–460.
89. Chan JKC, Sin VC, Wong KF, et al. Nonnasal lymphoma expressing thenatural killer cell marker CD56: a clinicopathologic study of 49 cases of anuncommon aggressive neoplasm. Blood. 1997;89(12):4501–4513.
90. Ng SB, Lai KW, Murugaya S, et al. Nasal-type extranodal natural killer/T-cell lymphomas: a clinicopathologic and genotypic study of 42 cases inSingapore. Mod Pathol. 2004;17(9):1097–1107.
91. Ko YH, Cho EY, Kim Je, et al. NK and NK-like T-cell lymphoma inextranasal sites: a comparative clinicopathological study according to site andEBV status. Histopathology. 2004;44(5):480–489.
92. Au WY, Weisenburger DD, Intragumtornchai T, et al. Clinical differencesbetween nasal and extranasal natural killer/T-cell lymphoma: a study of 136cases from the International Peripheral T-Cell Lymphoma Project. Blood. 2009;113(17):3931–3937.
93. Daum S, Ullrich R, Heise W, et al. Intestinal non-Hodgkin’s lymphoma: amulticenter prospective clinical study from the German Study Group on IntestinalNon-Hodgkin’s Lymphoma. J Clin Oncol. 2003;21(14):2740–2746.
94. Mansoor A, Pittaluga S, Beck PL, Wilson WH, Ferry JA, Jaffe ES. NK-cellenteropathy: a benign NK-cell lymphoproliferative disease mimicking intestinallymphoma—clinicopathological features and follow-up in a unique case series.Blood. 2011;117(5):1447–1452.
95. Takeuchi K, Yokoyama M, Ishizawa S, et al. Lymphomatoid gastropathy: adistinct clinicopathologic entity of self-limited pseudomalignant NK-cell prolif-eration. Blood. 2010;116(25):5631–5637.
96. Vega F, Chang CC, Schwartz MR, et al. Atypical NK-cell proliferation ofthe gastrointestinal tract in a patient with antigliadin antibodies but not celiacdisease. Am J Surg Pathol. 2006;30(4):539–544.
97. Zamboni G, Franzin G, Scarpa A, et al. Carcinoma-like signet-ring cells ingastric mucosa-associated lymphoid tissue (MALT) lymphoma. Am J Surg Pathol.1996;20(5):588–598.
98. Pan L, Diss TC, Cunningham D, Isaacson PG. The bcl-2 gene in primary B celllymphoma of mucosa-associated lymphoid tissue (MALT). Am J Pathol. 1989;135(1):7–11.
99. El-Zimaity HMT, Wotherspoon A, de Jong D. Interobserver variation in thehistopathological assessment of malt/malt lymphoma: towards a consensus.Blood Cells Mol Disease. 2005;34(1):6–16.
100. Hummel M, Oeschger S, Barth TFE, et al. Wotherspoon criteriacombined with B cell clonality analysis by advanced polymerase chain reactiontechnology discriminates covert gastric marginal zone lymphoma from chronicgastritis. Gut. 2006;55(6):782–787.
101. Wotherspoon AC, Ortiz-Hildago C, Falzon MR, Isaacson PG. Helico-bacter pylori-associated gastritis and primary B-cell gastric lymphoma. Lancet.338(8776):1175–1176, 1991.
102. Genta RM, Hamner HW, Graham DY. Gastric lymphoid follicles inHelicobacter pylori infection: frequency, distribution, and response to tripletherapy. Hum Pathol. 1993;24(6):577–583.
103. Parsonnet J, Hansen S, Rodriguez L, et al. Helicobacter pylori infectionand gastric lymphoma. N Engl J Med. 1994;330(18):1267–1271.
104. Nakamura S, Yao T, Aoyagi K, Iida M, Fujishima M, Tsuneyoshi M.Helicobacter pylori and primary gastric lymphoma: a histopathologic andimmunohistochemical analysis of 327 patients. Cancer. 1997;79(1):3–11.
105. Nakamura S, Aoyagi K, Furuse M, et al. B-cell monoclonality precedesthe development of gastric MALT lymphoma in Helicobacter pylori-associatedchronic gastritis. Am J Pathol. 1998;152(5):1271–1279.
106. Zucca E, Bertoni F, Roggero E, et al. Molecular analysis of the progressionfrom Helicobacter pylori-associated chronic gastritis to mucosa-associatedlymphoid-tissue lymphoma of the stomach. N Engl J Med. 1998;338(12):804–810.
107. Zullo A, Hassan C, Christofari F, et al. Effects of Helicobacter pylorieradication on early stage gastric mucosa-associated lymphoid tissue lymphoma.Clin Gastroenterol Hepatol. 2010;8(2):105–110.
108. Wotherspoon AC, Doglioni C, Isaacson PG. Low grade gastric B-celllymphoma of mucosa-associated lymphoid tissue (MALT): a multifocal disease.Histopathology. 1992;20(1):29–34.
109. Zucca E, Dreyling M; ESMO Guidelines Working Group. Gastricmarginal zone lymphoma of MALT type: ESMO clinical practice guidelines fordiagnosis, treatment and follow-up. Ann Oncol. 2010;21(suppl 5):v175–v176.
110. Ruskone-Fourmestraux A, Fischbach W, Aleman BMP, et al. EGILSconsensus report: gastric extranodal marginal zone B-cell lymphoma of MALT.Gut. 2011;60(6):747–758.
111. Ferrucci PF, Zucca E. Primary gastric lymphoma pathogenesis andtreatment: what has changed over the past 10 years? Br J Haematol. 2006;136(4):521–538.
112. Zullo A, Hassan C, Andriani A, et al. Treatment of low-grade gastricMALT-lymphoma unresponsive to Helicobacter pylori therapy: a pooled-dataanalysis. Med Oncol. 2010;27(2):291–295.
113. Copie-Bergman C, Gaulard P, Lavergne-Slove A, et al. Proposal for a newhistological grading system for post-treatment evaluation of gastric MALTlymphoma [letter]. Gut. 2003;52(11):1656.
114. Savio A, Franzin G, Wotherspoon AC, et al. Diagnosis and posttreatmentfollow-up of Helicobacter pylori-positive gastric lymphoma of mucosa-associat-ed lymphoid tissue: histology, polymerase chain reaction, or both? Blood. 1996;87(4):1255–1260.
115. Thiede C, Wundisch T, Alpen B, et al. Long-term persistence ofmonoclonal B cells after cure of Helicobacter pylori infection and completehistologic remission in gastric mucosa-associated lymphoid tissue B-celllymphoma. J Clin Oncol. 2001;19(6):1600–1609.
116. Wundisch T, Thiede C, Morgner A, et al. Long-term follow-up of gastricMALT lymphoma after Helicobacter pylori eradication. J Clin Oncol. 2005;23(31):8018–8024.
117. Bertoni F, Conconi A, Capella C, et al. Molecular follow-up in gastricmucosa-associated lymphoid tissue lymphomas: early analysis of the LY03cooperative trial. Blood. 2002;99(7):2541–2544.
118. Remstein ED, Kurtin PJ, James CD, Wang XY, Meyer RG, Dewald GW.Mucosa-associated lymphoid tissue lymphomas with t(11;18)(q21;q21) andmucosa-associated lymphoid tissue lymphomas with aneuploidy develop alongdifferent pathogenetic pathways. Am J Pathol. 2002;161(1):63–71.
119. Starostik P, Patzner J, Greiner A, et al. Gastric marginal zone B-celllymphomas of MALT type develop along 2 distinct pathogenetic pathways.Blood. 2002;99(1):3–9.
120. Hamoudi RA, Appert A, Ye H, et al. Differential expression of NF-kBtarget genes in MALT lymphoma with and without chromosome translocation:insights into molecular mechanism. Leukemia. 2010;24(8):1487–1497.
121. Rosenwald A, Ott G, Stilgebauer S, et al. Exclusive detection of thet(11;18)(q21;21) in extranodal marginal zone B cell lymphomas (MZBL) of MALTtype in contrast to other MZBL and extranodal large B cell lymphomas. Am JPathol. 1999;155(6):1817–1821.
122. Remstein ED, James CD, Kurtin PJ. Incidence and subtype specificity ofAPI2-MALT1 fusion transcripts in extranodal, nodal, and splenic marginal zonelymphomas. Am J Pathol. 2000;156(4):1183–1188.
123. Rinaldi A, Mian M, Chigrinova E, et al. Genome-wide DNA profiling ofmarginal zone lymphomas identifies subtype-specific lesions with an impact onthe clinical outcome. Blood. 2011;117(5):1595–1604.
124. Liu H, Ruskon-Fourmestraux A, Lavergne-Slove A, et al. Resistance oft(11;18) positive gastric mucosa-associated lymphoid tissue lymphoma toHelicobacter pylori eradication therapy [letter]. Lancet. 2001;357(9249):39–40.
125. Ye H, Liu H, Raderer M, et al. High incidence of t(11;18)(q21;q21) inHelicobacter pylori—negative gastric MALT lymphoma. Blood. 2003;101(7):2547–2550.
126. Yeh KH, Kuo SH, Chen LT, et al. Nuclear expression of BCL10 or nuclearfactor kappa B helps predict Helicobacter pylori-independent status of low-gradegastric mucosa-associated lymphoid tissue lymphoma with and withoutt(11;18)(q21;q21). Blood. 2005;106(3):1037–1041.
127. Toracchio S, Ota H, de Jong D, et al. Translocation t(11;18)(q21;q21) ingastric B-cell lymphomas. Cancer Sci. 2009;100(5):881–887.
128. de Jong D, Boot H, van Heerde P, Hart GAM, Taal BG. Histologicalgrading in gastric lymphoma: pretreatment criteria and clinical relevance.Gastroenterology. 1997;112(5):1466–1474.
129. Ferreri AJM, Freschi M, Dell’Oro S, Viale E, Ponzoni M. Prognosticsignificance of the histopathologic recognition of low- and high-grade componentsin stage I–II B-cell gastric lymphomas. Am J Surg Pathol. 2001;25(1):95–102.
130. Omonishi K, Yoshino T, Sakuma I, Kobayashi K, Moriyama M, Agaki T.bcl-6 protein is identified in high-grade but not low-grade mucosa-associatedlymphoid tissue lymphomas of the stomach. Mod Pathol. 1998;11(2):181–185.
131. O’Sullivan MJ, Ritter JH, Humphrey PA, Wick MR. Lymphoid lesions ofthe gastrointestinal tract: a histologic, immunophenotypic, and genotypicanalysis of 49 cases. Am J Clin Pathol. 1998:110(4);471–477.
132. Owens SR, Smith LB. Molecular aspects of H pylori-related MALTlymphoma. Patholog Res Int. 2011;2011:193149.
133. Wang G, Auerbach A, Wei M, et al. t(11;18)(q21;q21) in extranodalmarginal zone B-cell lymphoma of mucosa-associated lymphoid tissue instomach: a study of 48 cases. Mod Pathol. 2009;22(1):79–86.
134. Burke JS, Sheibani K, Nathwani, BN, Winberg CD, Rappoport H.Monoclonal small (well-differentiated) lymphocytic proliferations of the gastro-intestinal tract resembling lymphoid hyperplasia: a neoplasm of uncertainmalignant potential. Hum Pathol. 1987;18(12):1238–1245.
135. Collins RD. Is clonality equivalent to malignancy: specifically, isimmunoglobulin gene rearrangement diagnostic of malignant lymphoma? HumPathol. 1997;28(7):757–759.
Arch Pathol Lab Med—Vol 135, October 2011 GI Lymphoproliferative Disorders—Burke 1297