lymphoma dr: gehan mohamed. learning objectives important types of lymphoma clinical presentation...
TRANSCRIPT

Lymphoma
DR: Gehan Mohamed

Learning objectives
• important types of lymphoma
• Clinical presentation
• Diagnosis
• Staging

ALLALL Myeloma Myeloma CLLCLL LymphomasLymphomas
Hematopoieticstem cell
Neutrophils
Eosinophils
Basophils
Monocytes
Platelets
Red cells
Myeloidprogenitor
Myeloproliferative disordersMyeloproliferative disordersAMLAML
Lymphoidprogenitor T-lymphocytes
Plasmacells
B-lymphocytes
nanaïïveve

Normal structure of reactive lymph node

Microscopic picture of reactive lymphoid follicles

lymphoma• Definition : malignant neoplasm of lymphoid
origin, typically causing solid tissue mass usually in form of lymphadenopathy but may be presented as extra nodal mass as in brain or intestine.

Epidemiology of lymphomas
• 5th most frequently diagnosed cancer in both sexes
• males > females

Causes of lymphoma
• Genetic alterations causing mutations in chromosomes.
• Infection specially with viruses as Human T- cell leukemia Lymphoma virus , Epestein Bar virus.
• Immunosuppression

Pathogenesis of lymphoma
• There is monoclonal expansions of lymphocytic cells at certain developmental stages either of the :
(1)immature type which arise from lymphoblast .
(2) the mature type which arise from lymphocyte.
WHO classification of lymphoid neoplasms
•B cell neoplasm.
•T cell neoplasm.
•Hodgkin lymphoma.

B-CELL NEOPLASMS(A)Precursor B cell Iymphoblastic leukemia/ Iymphoma
(B)Peripheral B-Cell Neoplasms•B-cell chronic Iymphocytic leukemia/small Iymphocytic Iymphoma .•lymphoplasmacytic lymphoma•Mantle cell Iymphoma:•Follicular Iymphoma•Marginal Zone B-cell Lymphoma of mucosa-associated Iymphoid tissue (MALT) type•Hairy cell leukemia•Burkitt Iymphoma

T-CELL NEOPLASMS(A)Precursor T cell lymphoblastic leukemia/lymphoma .
(B)Peripheral T-cell and NK-cell neoplasms
•Aggressive NK cell leukemia
•Nasal and nasal-type NK/T cell Iymphoma.
•Mycosis fungoides .
•Angio-immunoblastic T-cell Iymphoma.
•Adult T-cell leukemia/lymphoma (HTLV1+).
•anaplastic large cell Iymphoma (ALCL) .

Lymphoma are classified according to the presence or absence of Reed sternberg
cell (R.S)into:
• (1) Hodgkin lymphoma which have R.S cell.
• (2) Non Hodgkin lymphoma which have no R.S cell.

Reed-Sternberg cell

Risk factors for NHL
• immunosuppression or immunodeficiency
• family history of lymphoma
• infectious agents
• ionizing radiation

Sites for non Hodgkin lymphoma
• A- Nodal lymphoma start in the lymph nodes.
• B-extra nodal lymphoma: - intestine
- Central nervous system
- Skin
- Brain
- testis
- spleen
- ovary

Clinical manifestations• Variable
• severity: range from asymptomatic to extremely ill.
• Systemic manifestations• weight loss, anorexia.
• Local manifestations• lymphadenopathy, splenomegaly most common• any tissue potentially can be infiltrated

Diagnosis of lymphoma
• A- gross examination
• B- microscopic examination: requires an adequate biopsy before treatment is initiated So we do :
- Haematoxylin and eosin stained sections.
- immunohistochemical stained sections using tumor
markers.

Gross picture for intestinal lymphoma

Microscopic picture of Non Hodgkin lymphoma
• Lost normal histologic architecture of the lymph nodes.
• Diffuse infiltration of the lymph node by monoclonal type of malignant lymphocytes.
• Immunohistochemical staining can help in the diagnosis as:
- T cell lymphoma are +ve for CD3.
- B cell Lymphoma are +ve for CD20

Microscopic picture of reactive lymphoid follicles

Non Hodgkin Lymphoma (H&E)
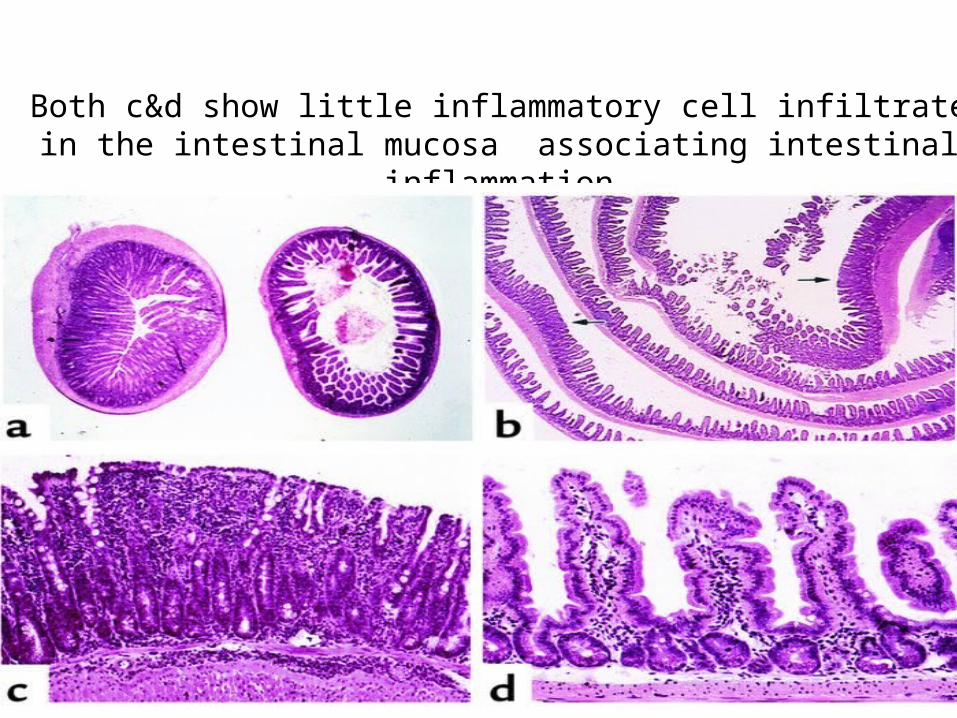
Both c&d show little inflammatory cell infiltrate in the intestinal mucosa associating intestinal inflammation

Intestinal lymphoma

Immuno-histochemical diagnosis for NHL using CD20 for B cell lymphoma

Hodgkin lymphoma
Thomas Hodgkin(1798-1866)

Classical Hodgkin Lymphoma

Epidemiology
• less frequent than non-Hodgkin lymphoma
• overall M>F
• peak incidence in 3rd decade
Associated (etiological?) factors
• Epestein Bar Virus infection.
• May associate Human Immunodeficiency Virus infection.
• possible genetic predisposition.

Hodgkin lymphoma
• cell of origin: B-lymphocyte present in germinal centre can change to Reed-Sternberg cells (or RS variants) which is the malignant cells but the other surrounding white blood cells in the affected lymph node are reactive cells
( polyclonal) not neoplastic cells.

Hodgkin lymphoma

Reed-Sternberg cell

A possible model of pathogenesis
germinalcentreB cell
transformingevent(s)
loss of apoptosis
RS cellinflammatory
response
EBV?
cytokines

Microscopic picture of Hodgkin lymphoma
• Lost normal histologic architecture of the lymph nodes.
• The only malignant cells is the classic Reed sternberg cell or one of its variants.
• But the surrounding cells for the RS cells are reactive and not malignant.
• Immunohistochemical staining can help in the diagnosis as:
- R.S cell is +ve for CD15, CD30.

HODGKIN LYMPHOMA (Hodgkin's Disease) are
further subclassified into :(A)Nodular lymphocyte predominance Hodgkin Iymphoma.
(B) Classical Hodgkin Iymphoma which include:
•Nodular sclerosis .
•Classical Hodgkin lymphoma, lymphocyte-rich.• lymphocyte depleted.
•Mixed cellularity type.

RS cell and variants
popcorn celllacunar cellclassic RS cell(mixed cellularity
Hodgkin lymphoma)(nodular sclerosisHodgkin lymphoma)
(lymphocytePredominanceHodgkin lymphoma)

Clinical manifestations:
• lymphadenopathy
• extranodal sites relatively uncommon except in advanced disease

Stage I Stage II Stage III Stage IV
Staging of lymphoma to identify the degree of spread of Hodgkin
lymphoma
A: absence of B symptomsB: fever, night sweats, weight loss

complications of lymphoma
• bone marrow failure due to infiltration.
• CNS infiltration
• compression of structures (e.g spinal cord, ureters)