lutonix av ide clinical trial - lincapac2019.cncptdlx.com · licht, jonah providence interventional...
TRANSCRIPT

Latest Lutonix AV Clinical Results
Lutonix AV IDE Clinical Trial
Skyi PangVascular Surgeon
Hong Kong

Disclosure
Speaker name:
Skyi Yin Chun Pang
I have the following potential conflicts of interest to report:
Consulting
Employment in industry
Stockholder of a healthcare company
Owner of a healthcare company
Other(s)
I do not have any potential conflict of interest

Objective
Lutonix AV IDE Clinical Results
• Study design & published 6-month data
• Sub-group analysis
• 2-year outcome
• Safety and mortality data
• Current investigations
• Practical applications in 2019

Trial DesignLutonix AV IDE Clinical Trial
ObjectiveTo assess the safety and effectiveness of the LUTONIX® 035 AV Drug Coated Balloon PTA Catheter in the treatment of dysfunctional AV fistulae
Number of Patients/Sites
285 randomized subjects at 23 clinical sites
Primary Effectiveness Endpoint
Target Lesion Primary Patency (TLPP) - 6 months
Primary Safety EndpointFreedom from any serious adverse event(s) involving the AV access circuit through 30 days
Follow Up 1, 3, 6, 9, 12, 18, 24 month visits
StatusFirst Subject: June 2015Enrollment Completion: March 2016
✓ Prospective✓ Multi-Center✓ Randomized (1:1)
✓ Core Lab Adjudicated✓ Clinical Events Committee (CEC)✓ Data & Safety Monitoring Board (DSMB)

Lutonix AV IDE Clinical TrialClinical Trial Sites
Investigator Site Name State Investigator Site Name State
Balamuthusamy,
SaravananTarrant Vascular Clinic TX Nadolski, Greg Hospital of the University of PA PA
Waheed, Umar Southwest Vascular Ctr AZ Atray, Naveen Capital Nephrology Medical CA
Lipkowitz, GeorgeRenal &Transplant Assoc of
NEMA Bratton, Charles Medical University of SC SC
Saad, Theodore Nephrology Associates DE Pflederer, Timothy Renal Care Associates, S.C. IL
Hoggard, Jeffrey Capital Nephrology Assoc. NC Kamel, AhmedUniversity of Alabama at
Birmingham (UAB)AL
Peeler, David University Vascular Access TN Schultz, Scott Minnesota Vascular Surgery Ctr MN
Neyra, RoxanaArizona Kidney Disease and
Hypertension CenterAZ Wilkins, Luke University of Virginia VA
Lawless, Mike Life Access Center OK Irani, Zubin Massachusetts General Hospital MA
Licht, Jonah Providence Interventional RI Tasse, Jordan Rush University IL
Makris, Angelo Chicago Access Care IL Davanzo, William Phoebe Putney Memorial Hospital GA
Molnar, RobertSan Antonio Kidney
DiseaseCtrTX Resnick, Scott Northwestern IL
Kramer, Ari Michigan Vascular Access MI Ross, John Access Connections SC
Chan, Micah Spartanburg Regional Hpt SC

Lutonix AV IDE Clinical TrialDevice Description
• 2 µg/mm2 paclitaxel + polysorbate and sorbitol excipients
• 4-12 mm diameters, 40-100 mm lengths
• .035” guidewire compatible, nylon, semi-compliant balloon
• Over the wire, co-axial shaft
• Nominal 6atm, RBP up to 12atm
Study Device: LUTONIX® 035 DCB
Photo courtesy of BD

Primary Endpoint – 6 Month ResultsLutonix AV IDE Clinical Trial
Trerotola et al, Clin JASN 13:1215-1224, 2018
Sachdeva B, Abreo K, Clin JASN 13:1140-1141, 2018
“The preliminary findings of this study are encouraging and hopefully, will be borne out over the 12 and 24 months of observation. It is our hope that DCB angioplasty will delay recurrent stenosis in AVFs and thereby, decrease morbidity and cost for patients on hemodialysis.”
Re-interventions
LTX DCB(n=141)
StandardPTA
(n=144)
P DCB vs. Control
Number of interventions,
180 days44 64 0.034 31.3% Fewer
Number of interventions,
210 days58 85 0.012 32.8% Fewer

Lutonix AV IDE Clinical TrialSubgroup Analyses
• Antiplatelet agents
• Fistula age
• Diabetes
• Previous intervention
• Fistula location
• Target lesion location

Lutonix AV IDE Clinical TrialAntiplatelet: Aspirin or Clopidogrel
Post-Index Procedure6 Mo. TLPP Diff. P-val
Antiplatelet? LTX Control (95% CI)n/s
Yes-6 months
47/67 (70.1%) 36/63 (57.1%)13.0%
(-3.4%, 29.4%)
No 42/59 (71.2%) 52/77 (67.5%)3.7%
(-11.9%, 19.2%)
Yes-12 months
23/61 (37.7%) 15/62 (24.2%)13.5%
(-2.7%, 29.7%)
No 23/53 (43.4%) 30/70 (42.9%)0.5%
(-17.1%, 18.2%)
Yes-24 months
13/64 (20.3%) 12/64 (18.8%)1.6%
(-12.2%, 15.3%)
No 9/42 (21.4%) 13/61 (21.3%)0.1%
(-16.0%, 16.2%)
• “Antiplatelet treatment protects fistula from thrombosis or loss of patency…..” • Palmer et al, Antiplatelet therapy to prevent hemodialysis vascular access failure: Systematic review and meta-
analysis. Am J Kidney Dis 2013; 61(1):112-122
• “... the use of antiplatelet agents prevented the loss of VA patency in a dose–response manner”• Hsu et al. Antiplatelet agents maintain arteriovenous fistula and graft function in patients receiving
hemodialysis: A nationwide case-control study. PLoS one 2018; 13

Lutonix AV Clinical TrialAge of Fistula
6 Mo. TLPP Diff. 12 Mo. TLPP Diff. 24 Mo. TLPP Diff.P-val
Age of Fistula
LTX Control (95% CI) LTX Control (95% CI) LTX Control (95% CI) n/s
<= 6 Months 2/3 (66.7%)
3/4 (75.0%)
-8.3% (-76.5%, 59.8%)
1/3 (33.3%)
3/4 (75.0%)
-41.7% (-100.0%, 26.5%)
0/2 (0%)
2/3 (66.7%)
66.7% (13.3%, 100.0%)
6-12 Months 10/14 (71.4%)
14/26 (53.8%)
17.6%(-12.9%, 48.0%)
8/12 (66.7%)
7/24 (29.2%)
37.5% (5.2%, 69.8%)
4/11 (36.4%)
5/24 (20.8%)
15.5%(-17.2%, 48.3%)
> 12 Months 77/109 (70.6%)
71/110 (64.5%)
6.1%(-6.3%, 18.5%)
37/99 (37.4%)
35/104 (33.7%)
3.7% (-9.4%, 16.9%)
18/93 (19.4%)
18/98 (18.4%)
1.0%(-10.1%, 12.1%)
• “…the newer the AVF is at angioplasty, the shorter the post-intervention primary patency duration. Angioplasty in AVFs less than 6 months of age….significantly increased the risk of postinterventionprimary patency loss.” • Neuen et al, Factors associated with patency following angioplasty of hemodialysis fistulae JVIR
2014;25:1419-1426
• “…the older the AVF, the smaller the probability of recurrence”• Heye et al, Factors influencing technical success and outcome of percutaneous balloon angioplasty in de novo
native hemodialysis arteriovenous fistulas Eur J Rad 2012;81;2298-2303

Lutonix AV IDE Clinical TrialDiabetes
6 Mo. TLPP Diff. 12 Mo. TLPP Diff. 24 Mo. TLPP Diff.P-val
LTX Control (95% CI) LTX Control (95% CI) LTX Control (95% CI) n/s
Yes49/73
(67.1%)
57/91 (62.6%)
4.5% (10.2%,19.1%)
26/67 (38.8%)
30/88 (34.1%)
4.7%
(-10.6%, 20.0%)
14/63 (22.2%)
15/82 (18.3%)
3.9%
(-9.3%, 17.2%)
No40/53
(75.5%)
31/49 (63.3%)
12.2%
(-5.6%, 30.0%)
20/47 (42.6%)
15/44 (34.1%)
8.5%
(-11.4%, 28.4%)
8/43 (18.6%)
10/43 (23.3%)
-4.7%
(-21.8%, 12.5%)
• “The presence of diabetes mellitus predicted restenosis of AV fistulas after PTA…”– Wu et. al, Baseline plasma glycemic profiles but not inflammatory biomarkers predict symptomatic
restenosis after angioplasty of arteriovenous fistulas in patients with hemodialysis, Atherosclerosis 2010;209:598-600
• “Patients with diabetes mellitus have higher risk for early dysfunction”– Heye et al, Factors influencing technical success and outcome of percutaneous balloon angioplasty in
de novo native hemodialysis arteriovenous fistulas European Journal of Radiology 2012;81:2298-2303
• “Early dysfunction was positively correlated with diabetes”– Atkas et al, Percutaneous transluminal balloon angioplasty in stenosis of native hemodialysis
arteriovenous fistulas: technical success and analysis of factors affecting post procedural fistula patency Diagn Interv Radiol 2015;21:160-166
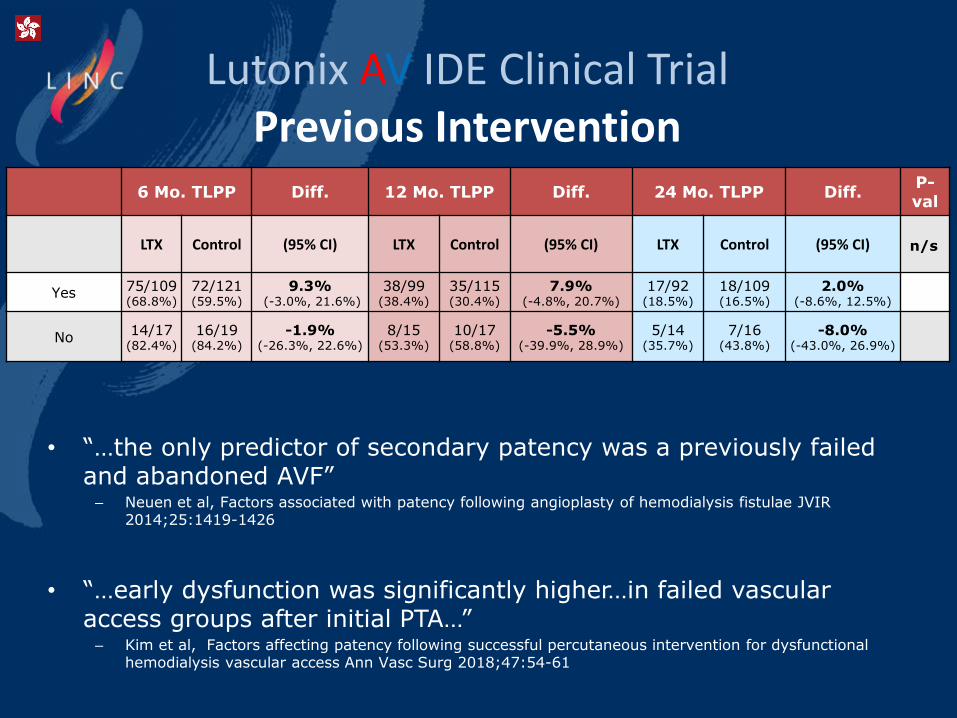
Lutonix AV IDE Clinical TrialPrevious Intervention
6 Mo. TLPP Diff. 12 Mo. TLPP Diff. 24 Mo. TLPP Diff.P-val
LTX Control (95% CI) LTX Control (95% CI) LTX Control (95% CI) n/s
Yes 75/109 (68.8%)
72/121 (59.5%)
9.3%(-3.0%, 21.6%)
38/99 (38.4%)
35/115 (30.4%)
7.9% (-4.8%, 20.7%)
17/92 (18.5%)
18/109 (16.5%)
2.0%(-8.6%, 12.5%)
No14/17
(82.4%)
16/19 (84.2%)
-1.9% (-26.3%, 22.6%)
8/15 (53.3%)
10/17 (58.8%)
-5.5% (-39.9%, 28.9%)
5/14 (35.7%)
7/16 (43.8%)
-8.0% (-43.0%, 26.9%)
• “…the only predictor of secondary patency was a previously failed and abandoned AVF”– Neuen et al, Factors associated with patency following angioplasty of hemodialysis fistulae JVIR
2014;25:1419-1426
• “…early dysfunction was significantly higher…in failed vascular access groups after initial PTA…” – Kim et al, Factors affecting patency following successful percutaneous intervention for dysfunctional
hemodialysis vascular access Ann Vasc Surg 2018;47:54-61

Lutonix AV IDE Clinical TrialPrevious Intervention by Time
6 Mo. TLPP Diff. 12 Mo. TLPP Diff. 24 Mo. TLPP Diff.P-val
PreviousIntervention
LTX Control (95% CI) LTX Control (95% CI) LTX Control (95% CI) n/s
> 90 days59/82
(72.0%)
65/101 (64.4%)
7.60% (-5.9%, 21.1%)
29/73 (39.7%)
33/96 (34.4%)
5.4%(-9.4%, 20.1%)
13/67 (19.4%)
17/90 (18.9%)
0.5%(-11.9%, 13.0%)
< = 90 days 16/27 (59.3%)
7/20 (35.0%)
24.30% (-3.7%, 52.2%)
9/26 (34.6%)
2/19 (10.5%)
24.1% (1.2%, 47.0%)
4/25
(16.0%)
1/19
(5.3%)
10.7%(-6.8%, 28.3%)
No previous intervention
14/17 (82.4%)
16/19 (84.2%)
-1.90% (-26.3%, 22.6%)
8/15 (53.3%)
10/17 (58.8%)
-5.5%(-39.9%, 28.9%)
5/14
(35.7%)
7/16
(43.8%)
-8.0%(-43.0%, 26.9%)
• “…early occurrence was associated with a lower secondary patency rate”– Atkas et al, Percutaneous transluminal balloon angioplasty in stenosis of native hemodialysis
arteriovenous fistulas: technical success and analysis of factors affecting post procedural fistula patency Diagn Interv Radiol 2015; 21:160-166
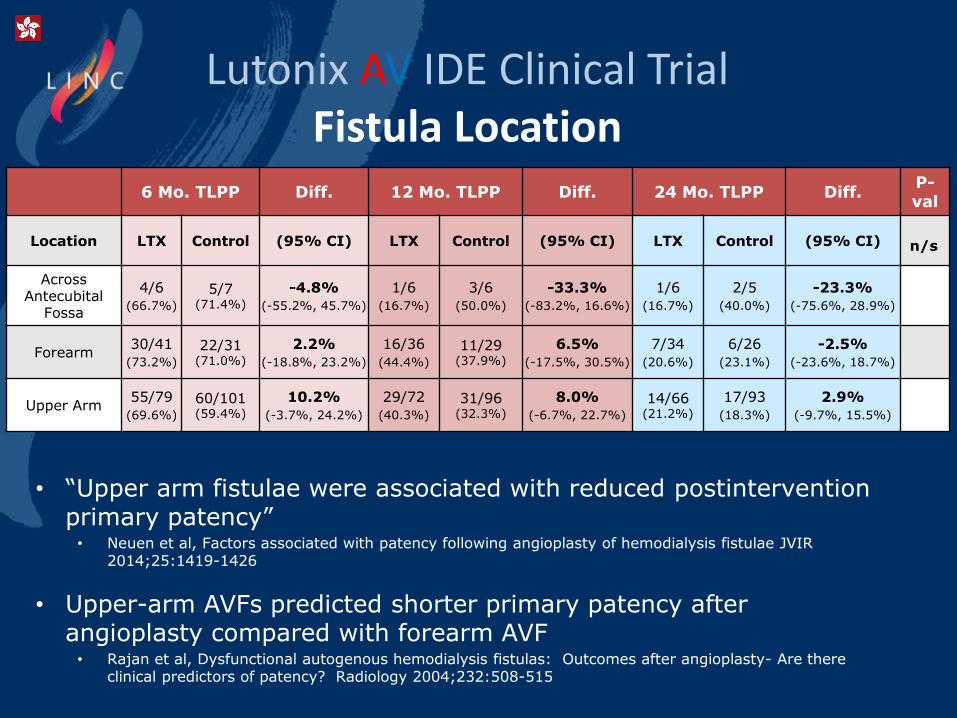
Lutonix AV IDE Clinical TrialFistula Location
6 Mo. TLPP Diff. 12 Mo. TLPP Diff. 24 Mo. TLPP Diff.P-val
Location LTX Control (95% CI) LTX Control (95% CI) LTX Control (95% CI) n/s
AcrossAntecubital
Fossa
4/6
(66.7%)
5/7 (71.4%)
-4.8%
(-55.2%, 45.7%)
1/6
(16.7%)
3/6
(50.0%)
-33.3%
(-83.2%, 16.6%)
1/6
(16.7%)
2/5
(40.0%)
-23.3%
(-75.6%, 28.9%)
Forearm30/41
(73.2%)
22/31 (71.0%)
2.2%
(-18.8%, 23.2%)
16/36
(44.4%)
11/29 (37.9%)
6.5%
(-17.5%, 30.5%)
7/34
(20.6%)
6/26
(23.1%)
-2.5%
(-23.6%, 18.7%)
Upper Arm55/79
(69.6%)
60/101 (59.4%)
10.2%
(-3.7%, 24.2%)
29/72
(40.3%)
31/96 (32.3%)
8.0%
(-6.7%, 22.7%)
14/66 (21.2%)
17/93
(18.3%)
2.9%
(-9.7%, 15.5%)
• “Upper arm fistulae were associated with reduced postinterventionprimary patency”• Neuen et al, Factors associated with patency following angioplasty of hemodialysis fistulae JVIR
2014;25:1419-1426
• Upper-arm AVFs predicted shorter primary patency after angioplasty compared with forearm AVF• Rajan et al, Dysfunctional autogenous hemodialysis fistulas: Outcomes after angioplasty- Are there
clinical predictors of patency? Radiology 2004;232:508-515
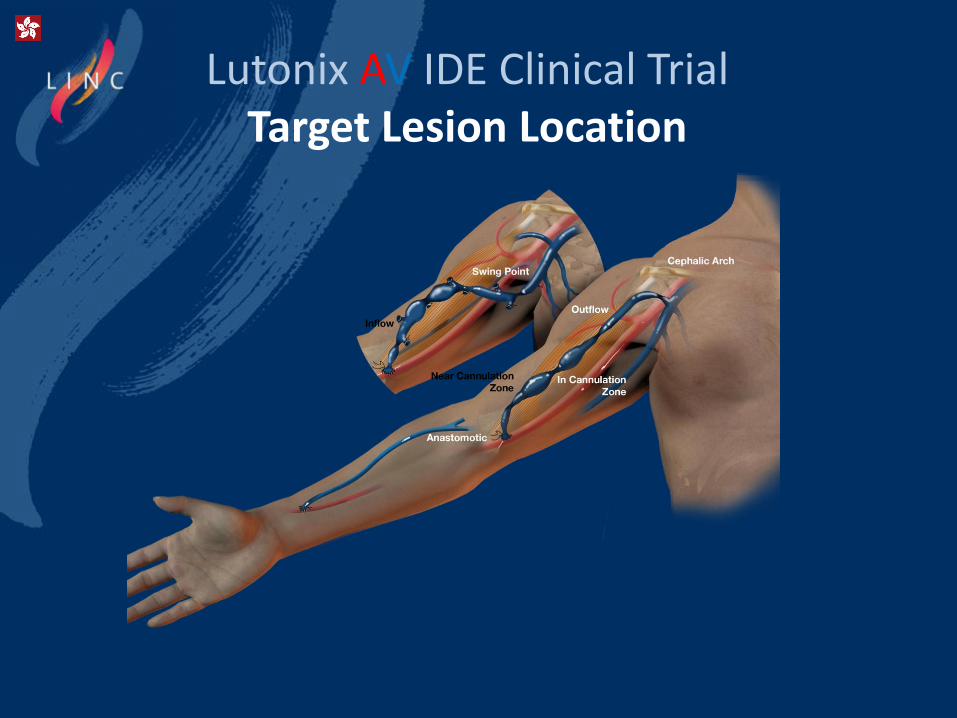
Lutonix AV IDE Clinical TrialTarget Lesion Location

Lutonix AV IDE Clinical TrialTarget Lesion Location
6 Mo. TLPP Diff. 12 Mo. TLPP Diff. 24 Mo. TLPP Diff.P-val
Target Lesion
LocationLTX Control (95% CI) LTX Control (95% CI) LTX Control (95% CI) n/s
Anastomotic13/17
(76.5%)
8/14 (57.1%)
19.3%
(-13.5%, 52.2%)
7/16
(43.8%)
3/13
(23.1%)
20.7%
(-12.7%, 54.1%)
3/16
(18.8%)
1/13
(7.7%)
11.1%
(-12.9%, 35.0%)
Cephalic arch13/25
(52.0%)
14/31 (45.2%)
6.8%
(-19.4%, 33.1%)
5/23
(21.7%)
9/31
(29.0%)
-7.3%
(-30.5%, 15.9%)
1/22
(4.5%)
1/29
(3.4%)
1.1%
(-9.9%, 12.0%)
In cannulation
zone8/11
(72.7%)
11/16 (68.8%)
4.0%
(-30.8%, 38.7%)
6/10
(60.0%)
7/15
(46.7%)
13.3%
(-26.2%, 52.8%)
3/9
(33.3%)
5/14
(35.7%)
-2.4%
(-42.1%, 37.3%)
Inflow13/17
(76.5%)
22/28 (78.6%)
-2.1%
(-27.4%, 23.1%)
9/16
(56.3%)
11/25 (44.0%)
12.3%
(-18.9%, 43.4%)
5/14
(35.7%)
8/23
(34.8%)
0.9%
(-30.8%, 32.7%)
Near cannulation
zone
8/11 (72.7%)
7/8 (87.5%)
-14.8%
(-49.7%, 20.1%)
3/9
(33.3%)
3/5
(60.0%)
-26.7%
(-79.5%, 26.2%)
1/8
(12.5%)
1/4
(25.0%)
-12.5%
(-60.7%, 35.7%)
Outflow25/31
(80.6%)
20/34 (58.8%)
21.8%
(0.2%, 43.4%)
11/28
(39.3%)
9/34
(26.5%)
12.8%
(-10.6%, 36.2%)
7/26
(26.9%)
6/33
(18.2%)
8.7%
(-12.8%, 30.3%)
Swing point9/14
(64.3%)
6/9 (66.7%)
-2.4%
(-42.1%, 37.3%)
5/12
(41.7%)
3/9
(33.3%)
8.3%
(-33.2%, 49.9%)
2/11
(18.2%)
3/9
(33.3%)
-15.2%
(-53.5%, 23.2%)
• Cannulation zone…..more than intimal hyperplasia?• Roy-Chaudhury et al, Hemodialysis vascular access dysfunction: A cellular and molecular viewpoint JASN
2006;17(4):1112-1127
• “Swing-segment lesions predispose to early fistula failure”• Badero et al, Frequency of swing-segment stenosis in referred dialysis patients with angiographically
documented lesions Am J Kidney Dis 2008;51(1):93-98
• Cephalic arch lesions more difficult to treat• Rajan et al, Prevalence and Treatment of Cephalic Arch Stenosis in Dysfunctional Autogenous
Hemodialysis Fistulas JVIR 2003;14:567-573

Lutonix AV IDE Clinical Trial24 Month Data
Lutonix AV IDE Clinical Trial
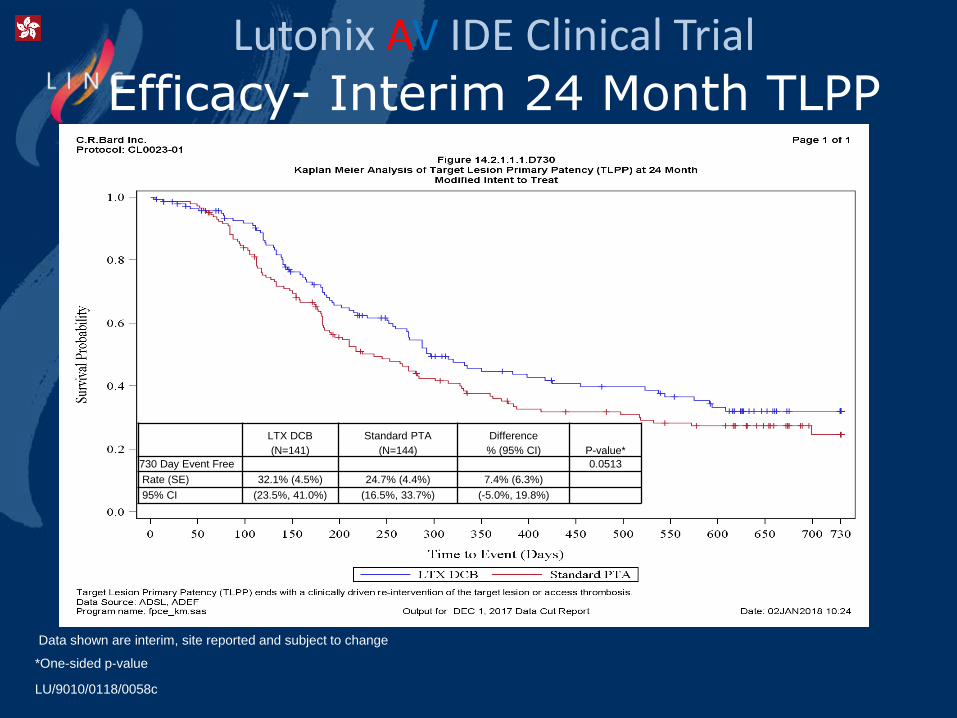
Efficacy- Interim 24 Month TLPP
*One-sided p-value
LTX DCB
(N=141)
Standard PTA
(N=144)
Difference
% (95% CI) P-value*
730 Day Event Free 0.0513
Rate (SE) 32.1% (4.5%) 24.7% (4.4%) 7.4% (6.3%)
95% CI (23.5%, 41.0%) (16.5%, 33.7%) (-5.0%, 19.8%)
Data shown are interim, site reported and subject to change
LU/9010/0118/0058c
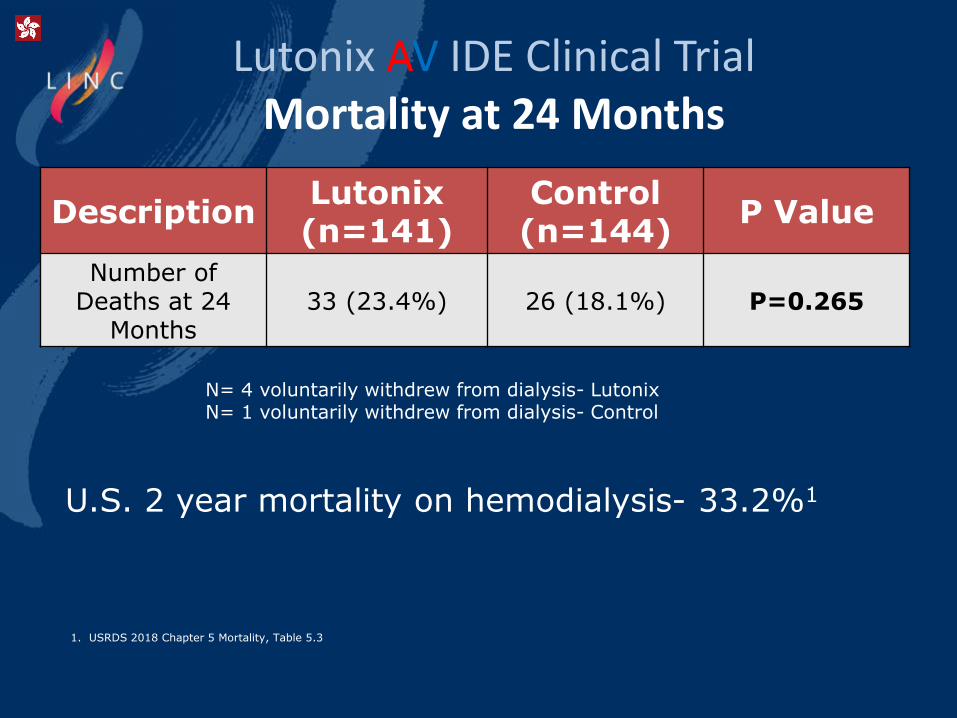
Lutonix AV IDE Clinical TrialMortality at 24 Months
DescriptionLutonix (n=141)
Control (n=144)
P Value
Number of Deaths at 24
Months33 (23.4%) 26 (18.1%) P=0.265
N= 4 voluntarily withdrew from dialysis- LutonixN= 1 voluntarily withdrew from dialysis- Control
U.S. 2 year mortality on hemodialysis- 33.2%1
1. USRDS 2018 Chapter 5 Mortality, Table 5.3

Lutonix AV Clinical TrialLutonix AV Clinical Program
TitleNumber of Subjects
Lutonix AV Clinical Trial - Complete N=285
Lutonix AV Real World Global Registry - Enrolled N=324
Lutonix AV Post Approval Study – Enrolling N=213
Total N=822

Lutonix AV Global Registry6 Month Data

Lutonix AV Global Registry
73.5% TLPP at 6 Months
6 Month TLPP ResultsLutonix AV IDE Clinical Trial
71.4% TLPP at 6 Months
Real World treated lesions; Central vein, ISR, AVG/AVF, Cephalic Arch, Restenotic, etc.
TLPP ends with a clinically driven re-intervention of the target lesion or access thrombosis. Kaplan Meier modified intent to treat.
Mature, dysfunctional fistulae. Central vein and ISR excluded. Restenotic and previous thrombosis included.
Lutonix AV IDE Clinical TrialSummary
DCB effect was not statistically different between subgroups
•DCB appears to work equivalently across access history/lesion location
Mortality rate was comparable to control arm
•None of the deaths were related to the test device or the procedure
Additional analyses to follow
•> 800 subjects part of a Lutonix AV protocol

Thank You

Latest Lutonix AV Clinical Results
Lutonix AV IDE Clinical Trial
Skyi PangVascular Surgeon
Hong Kong