lumen diameter ofnormal human coronary...
TRANSCRIPT

232
Lumen Diameter of NormalHuman Coronary Arteries
Influence of Age, Sex, Anatomic Variation, and LeftVentricular Hypertrophy or Dilation
J. Theodore Dodge Jr., MD; B. Greg Brown, MD, PhD;Edward L. Bolson, MS; and Harold T. Dodge, MD
Background. Precise knowledge of the expected "normal" lumen diameter at a given coronary anatomiclocation is a first step toward developing a quantitative estimate of coronary disease severity that could bemore useful than the traditional "'percent stenosis."Methods and Resuls. Eighty-three arteriograms were carefuly selected from among 9,160 consecutive
studies for their smooth lumen borders indicating freedom from atherosclerotic disease. Of these, 60 menand 10 women had no abnormalities of cardiac function, seven men had idiopathic dilated cardiomyop-athy, and six men had left ventricular hypertrophy associated with significant aortic stenosis. Lumendiameter was measured at 96 points in 32 defined coronary segments or major branches. Measurementswere scaled to the catheter, corrected for imaging distortion, and had a mean repeat measurement errorof 0.12 mm. When sex, anatomic dominance, and branch length were accounted for, normal lumendiameter at each of the standard anatomic points could usually be specified with a population varianceof ±O.6 mm or less (SD) and coefficient ofvariation of <0.25 (SD/mean). For example, the left main arterymeasured 4.5±0.5 mm, the proximal left anterior descending coronary artery (LAD) 3.7+0.4 mm, and thedistal LAD 1.9+0.4 mm. For the LAD, lumen diameter was not affected by anatomic dominance (rightversus left), but for the right coronary artery, proximal diameter varied between 3.9±0.6 and 2.8±0.5 mm(p<O.Ol) and for the left circumflex, between 3.4±0.5 and 4.2±0.6 mm (p<0.01). Women had smallerepicardial arterial diameter than men (-9%o; p<0.001), even after normalization for body surface area(p<O.Ol). Branch artery caliber was unaffected by the anatomic dominance but increased with branchlength, expressed as a fraction of the origin-to-apex distance (p<0.001). Lumen diameter was not affectedby age or by vessel tortuosity but was significantly increased among men with left ventricular hypertrophy(+17%; p<O.001) or dilated cardiomyopathy (+12%; p<O.OOl).
Conclusions. This is a reference normal data set against which to compare lumen dimensions in variouspathological states. It should be of particular value in the investigation of diffuse atherosclerotic disease.(Circulation 1992;86:232-246)KEY WoRDs * coronary anatomy * vessels, coronary, size * computer graphics * arteriography,
quantitative
In humans, certain pathological and physiologicalprocesses influence coronary artery lumen caliber.Diffuse arteriosclerotic intimal thickening is said
to reduce lumen diameter at pathological examina-tion,1-3 although a compensatory enlargement occurs.4Reduced flow demand contracts vessel size by an endo-thelium-dependent process.5 Aging,6'7 ectasia,8-'0 Ka-wasaki syndrome," increased myocardial flow demands,
From the Cardiovascular Research and Training Center, Car-diology Division, Department of Medicine, University of Wash-ington, Seattle.
Supported in part by US Public Health Service grants HL-13517, HL-19451, HL-18805, and HL-30086, in part by an Estab-lished Investigator Award (B.G.B.) from the American HeartAssociation, and in part by a grant from the John L. Locke Jr.Charitable Trust.Address for correspondence: B. Greg Brown, MD, PhD, Cardi-
ology Division, RG-22, University of Washington School of Med-icine, Seattle, WA 98195.
Received December 4, 1990; revision accepted April 8, 1992.
and high-flow coronary fistulae12 are processes that mayincrease lumen caliber. These processes may occur inthe absence of focal narrowing and/or luminal irregu-larity, so we cannot be certain that normal-appearingarterial segments are truly normal. This presents aproblem for the traditional radiographic estimate ofarterial disease severity, the "percent stenosis," which isbased on the ratio of a focal minimum to a nearby"normal" diameter. Percent stenosis is, experimentally,a uniquely effective correlate of the physiological impactof focal coronary narrowing,13-'6 but unfortunately, tothe extent that we cannot accurately assess normallumen diameter in humans, the clinical utility of thisestimate is diminished.2One solution to this problem is to find methods
whereby we may predict normal lumen diameter at agiven point in the coronary anatomy and to use thisdiameter as a normal reference for the percent stenosis.At present, data on the "true" normal diameter ofhuman coronary arteries are not available in a system-
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

Dodge et al Normal Lumen Diameter 233
atic format. In this report, we extend the early measure-ments of MacAlpin et al'7 to demonstrate that, whenanatomic variations are accounted for, it is usuallypossible to specify normal coronary segment diameterin men and women to within +25% (coefficient ofvariation). We also show that left ventricular (LV)hypertrophy (LVH) and, to a lesser extent, dilatedcardiomyopathy (DCM) result in enlargement of nor-mal vessel caliber.
MethodsPatients
Eighty-three patients were selected for the absence ofarterial disease from among 9,160 consecutive clinicalcatheterization studies. Blood pressure was routinelyobtained during the catheterization admission in allcases, and a fasting lipid profile (total cholesterol [TC],low density lipoprotein [LDL], high density lipoprotein[HDL], and apolipoprotein B [apo B]) was obtained inthe great majority. Patients with anemia or diabetesmellitus, those who had received nitroglycerin in thecatheterization laboratory, and those who had takenlong-acting nitrates on the day of catheterization wereexcluded. Films were very carefully inspected by an
See p 331experienced arteriographer; those with any luminalirregularity even faintly suggestive of an atheroscleroticplaque were excluded, leaving only films with smooth,regular arterial borders. In 70 normal patients (10women), heart size on radiography, global ejectionfraction, and end-diastolic LV chamber volume werewithin normal limits (20.52; 50-120 ml/m2). Five pa-tients had mild mitral insufficiency resulting from pro-lapse without evidence of a dilated ventricle. None ofthese normal patients had structural cardiac abnormal-ities. Indications for catheterization were the evaluationof chest pain in 53 patients, history of ventriculararrhythmia (premature contraction, tachycardia, fibril-lation) in eight, Wolff-Parkinson-White disease in four,abnormal exercise tolerance test in three, and beingpotential participants in a drug trial in two. Six otherpatients had concentric LVH caused by aortic stenosis,with or without aortic insufficiency, with aortic valvearea of <1.2 cm2 and/or aortic valve gradient >60mm Hg, evidence of LVH on ECG, and/or wall thick-ening > 13 mm on echocardiogram. Another sevenpatients had DCM with global ejection fraction <0.25(six patients)- and increased end-diastolic LV chambervolume (six patients; .160 ml/m2).
ArteriographyCoronary arteries were cannulated by the Judkins
technique with catheters of known dimension (5F to8F). Selective coronary injections of Renografin 76 werefilmed in standard projections with a General ElectricFluoricon 300 radiographic system (Milwaukee, Wis.)with a resolution of 2.4 line pairs per millimeter.
Anatomic RepresentationThe anatomic segments shown in Figure 1 were
located in each coronary arteriogram. Although coro-nary anatomy tends to be somewhat more variable thanFigure 1 suggests, it was possible in every case to specify
RCA DOMINANT
A)A;
FIGURE 1. Diagram ofcoronary artery segment and branchnomenclature. Top panel: Right coronary artery (RCA)-dominant distribution; bottom panel: balanced and leftcoronary artery (LCA)-dominant distribution. Not shown isthe "small-RCA" distribution, in which the RCA branchesinto the posterior descending branch (RD) and the inferiorwall branch (RI), and the posterior wall branch (CP) arisesfrom the left circumflex artery. Artery segment abbreviationsare fully detailed in Table 5.
segments that corresponded approximately to thesestandard ones. In most cases, these segments were easyto locate, and in no case was a major branch ignored inthis process. We have described this coronary arterysegment and branch nomenclature18 and have applied itin this report with minor alterations including a "small"right coronary artery (RCA) anatomic distribution andanterior (OA) and posterior (OP) branches of theobtuse marginal (OM) branch. A complete descriptionof coronary artery segment and branch nomenclature isincluded in the "Appendix."
Measurements: Data EntryThe coronary angiographic films were projected with
magnification to 4.4 times life-size. Frames with clearimages were selected. All segments and branches of thecoronary artery tree were identified, and the anatomywas reduced to a set of up to 96 defined subsegments inthe following manner. With the exception of Al, A2,and A3, each segment shown in Figure 1 was trisected,and the midpoint of each third of each segment wasidentified as shown in Figure 2. For each artery, wedigitized the two-point diameter of the catheter into aDigital Equipment Corporation VAX-11/750 (May-nard, Mass.). We then digitized the lumen diameters of
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

234 Circulation Vol 86, No 1 July 1992
Y-AxIS (CEPHALAD)
X-AXIS(LATERAL)
FIGURE 2. Diagram showing example sites selected fordiameter measurement. Each artery segment was trisectedalong its length, and the midpoint of each resulting subseg-ment was found. Along the segments ofthe major arteries, thelumen borders of the proximal midpoints, middle midpoints,and distal midpoints (0) were digitized, whereas in arteriesbranchingfrom the main arteries, the lumen diameters at thepoint oforigin (c), proximal midpoints, and middle midpoints(.) were digitized, as illustrated here for the middle leftanterior descending coronary artery (L2), the first septal (Si),and the second diagonal (D2). r is the radial distancefrom thecoronary ostium to the artery segment. 0 is the azimuth anglebetween the projection of r onto the transverse plane (X-Zplane) and the anterior-posterior (AP) axis. (D is the anglebetween r and the transverse plane (X-Z plane). '8
the midpoint of each subsegment in the left main (LM),left anterior descending (LAD) (L1, L2, L3, IA), leftcircumflex (LCx) (Ci, C2, C3, C4), and right coronaryarteries (RCA) (R1, R2, R3, R4) that was present. Forthe three septal (S1, S2, S3), diagonal (D1, D2, D3),marginal (M1, M2, M3), and inferior wall branches(from RD, RI, RP, CP, CI, CD) and for the medianramus, we digitized the lumen diameter at the branchorigin and the proximal and middle midpoints. For an
OM, the length of artery between its origin and itsbifurcation was divided into three equal parts, and thelumen diameters were measured at the midpoint of eachof these subsegments. Diameters of the two longestbranches continuing beyond the bifurcation, OA andOP, were measured as described above for thebranches.
Terminal branches (diagonal, marginal, septal, etc.)were classified by size into one of five groups: long,medium, short, absent, or unseen. This branch sizerating refers to the vessel's length of distribution, not itswidth per se; where these vessels branched, their longestextension was used. This classification was made by
FIGURE 3. Diagram showing example of vessel length clas-sification. Branches were classified by size into one of fivegroups: short, medium, long, absent, or unseen. The classifi-cation wasperformedfrom views roughlyperpendicular to thelong axis of the heart by comparing the visible length of thevessel with the distance between its origin and the apex of theheart as illustrated here for the first marginal branch (M])arisingfrom the left circumflex artery. Ifthe visiblepath ofthevessel was less than 25% of this distance, then the vessel wasneglected ("absent"). When the visible path of the vessel wasbetween 25% and 50%,o or 50% and 75%, or .75% of thisdistance, then it was classified as short, medium, or long,respectively. Vessels that could not be clearly visualized wereclassified as unseen. This left coronary artery model wasgenerated by an updated computer program for anatomicdisplay.'8
comparing the visible length of the branch to thedistance between its origin and the apex of the heart ina view perpendicular to the long axis of the heart, asillustrated in Figure 3. If the visible length of the branchwas less than 25% of this distance, then it was neglected("absent"). When the visible length of the vessel wasbetween 25% and 50%, or 50% and 75%, or >75% ofthis distance, then it was classified as short, medium, orlong, respectively. Branches that could not be clearlyvisualized were classified as unseen. Occasionally, avessel branched extensively and thus supplied a largermyocardial mass than would otherwise be predicted byits length; it was accordingly given a longer classifica-tion. The three largest septal branches were classified; aseptal was long if it had at least three branches andextended >65% of the distance from its origin to thebase of the septum, medium if it had two branches andextended approximately 50% of this distance, and oth-erwise was short. If a single branch of the LCx wasmuch larger than its neighbors, it was considered to bean OM, although a first marginal (M1) or third marginal(M3) was also permitted if present. OM, OA, and OPlength were classified according to the same referencelength: the OM origin-to-apex distance. The posteriordescending artery, RD, and CD were required to reachthe apex to be long.The L4 segment was categorized to investigate
whether the length of apical LAD wrap-around affectsLAD lumen diameter. L4 was short if the LAD barelypassed the apex, medium if the LAD rounded the apexand made a small ramification on the inferior apicalregion, and long if the L4 provided inferior septalbranches. When the LAD did not reach the cardiacapex, L4 was absent.
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

Dodge et al Normal Lumen Diameter 235
FIGURE 4. Representative photographs of the left anterior descending artery with four different degrees of tortuosity:nontortuous, slightly tortuous, moderately tortuous, and very tortuous (from left to right). This figure was present for referencewhen tortuosity was classified.
The continuous spectrum of LAD tortuosity wasclassified into four groups: nontortuous, slightly tortu-ous, moderately tortuous, and very tortuous. Examplesof each degree of tortuosity for the LAD are displayedin Figure 4. Figure 4 was present for reference whentortuosity was graded.Our primary goal was to provide a reference data set
of normal men with right dominant anatomy; a second-ary goal was to highlight differences between this groupand other groups with normal coronary arteries. Wesought to completely measure 20 normal RCA-domi-nant men and 10 patients from each of the other sixgroups (small-RCA-dominant men, balanced men,LCA-dominant men, RCA-dominant women, men withLVH, and men with DCM) and .5 measurements fromeach branch-length group from among the normal men.Though we drew from a pool of 9,160 patients, it wasdifficult to meet these goals. The occurrence of menwith LVH with RCA-dominant anatomy and normalcoronary arteries was approximately 1 in 1,500. As thestudy progressed, it became clear that the low preva-lence of some rarely occurring branch arteries (e.g., longCI) would result in counts too low for a reliablepopulation average. In 73 patients (50 normal men, 10normal women, six men with LVH, and seven men withDCM), all artery subsegments present were measured.The counts for some branches were then augmented bymaking measurements at selected artery sites in 10additional normal male patients, accounting for some ofthe apparent discrepancies in patient numbers in thetables. For groups in which patients could be foundmore frequently, data were collected only until thetarget sample was obtained.
Measurements: TheoreticalTo reduce an angiographic image to true scale, opti-
cal and uniform x-ray magnifications were compensateddirectly by use of the catheter, which was of knowndiameter, as a scale factor. Out-of-plane magnification
caused by divergence of the x-ray beam was also cor-rected in the scaling process.'8'19 Pincushion distortionis a small source of selective image magnification withour modern equipment and small (5-6-in.) image fieldsand was neglected in this analysis for all arterial sub-segments. However, the diameter of the scaling cathe-ter, usually found in the periphery of the image, wasadjusted for pincushion effects.'9
Validation of Vessel, Dominance, andTortuosity Classification MethodsWe determined the repeatability of our classification
of anatomic dominance, tortuosity, branch artery iden-tity, and length after an interval of more than 3 months.All 73 completely measured arteriograms were ran-domly ordered, and the anatomic dominance of eachwas consecutively reclassified. Tortuosity was consecu-tively reclassified in a random subset of 36 normal malepatients. Each branch artery in 15 consecutive, ran-domly selected patients was reidentified with our no-menclature system (Figure 1 and "Appendix"), and thelength of each was reclassified with the above origin-to-apex system. These reclassifications were then com-pared with the original set.
Validation of Measurement MethodsWe determined the accuracy and variability of this
method by measuring known diameters from films of aroughly heart-sized styrofoam block in multiple viewingangles with the General Electric Fluoricon 300 radio-graphic equipment. This block contained a householdpin, the head representing the location of a coronaryostium, and two brass tubes positioned to represent thecatheter and a subsegment with 3.25-mm lumen diam-eter. The spatial relations between these locations weredetermined.'8 At the selected site, opposite sides of thetube were digitized in a fashion identical to that de-scribed for the arteries. The widths at these locations
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from
236 Circulation Vol 86, No 1 July 1992
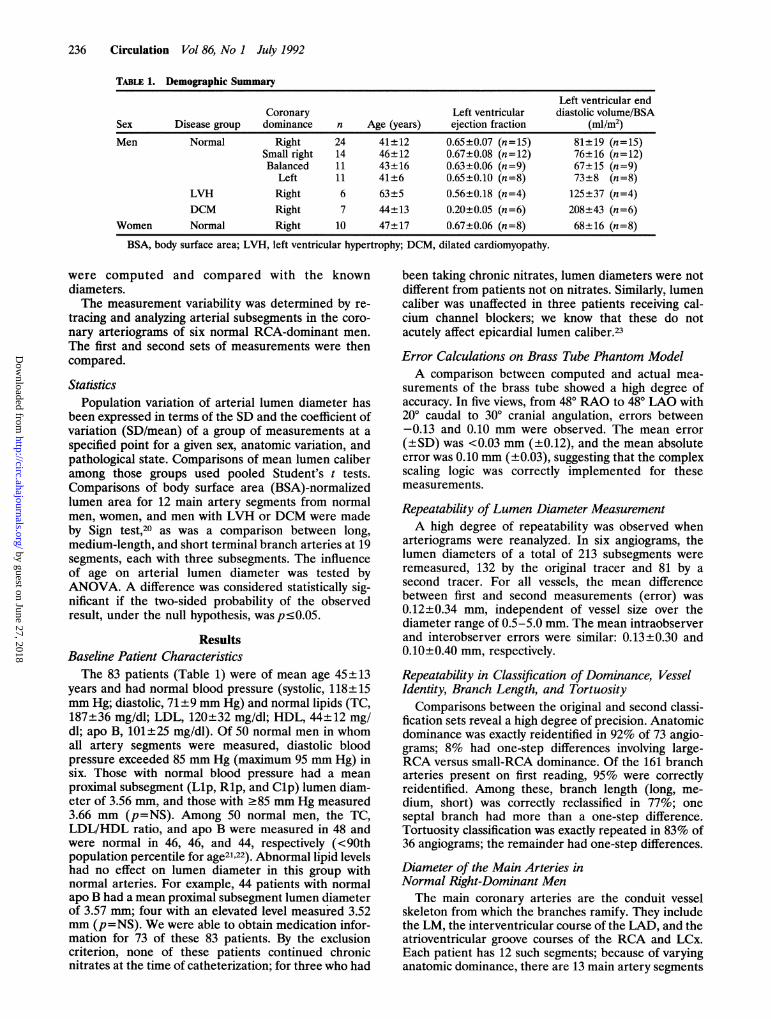
TABLE 1. Demographic SummaryLeft ventricular end
Coronary Left ventricular diastolic volume/BSASex Disease group dominance n Age (years) ejection fraction (mi/m2)Men Normal Right 24 41+12 0.65±0.07 (n= 15) 81+19 (n=15)
Small right 14 46±12 0.67±0.08 (n=12) 76+16 (n=12)Balanced 11 43±16 0.63±0.06 (n=9) 67±15 (n=9)
Left 11 41±6 0.65±0.10 (n=8) 73+8 (n=8)LVH Right 6 63±5 0.56±0.18 (n=4) 125+37 (n=4)DCM Right 7 44±13 0.20±0.05 (n=6) 208+43 (n=6)
Women Normal Right 10 47±17 0.67±0.06 (n=8) 68+16 (n=8)BSA, body surface area; LVH, left ventricular hypertrophy; DCM, dilated cardiomyopathy.
were computed and compared with the knowndiameters.The measurement variability was determined by re-
tracing and analyzing arterial subsegments in the coro-nary arteriograms of six normal RCA-dominant men.The first and second sets of measurements were thencompared.
StatisticsPopulation variation of arterial lumen diameter has
been expressed in terms of the SD and the coefficient ofvariation (SD/mean) of a group of measurements at aspecified point for a given sex, anatomic variation, andpathological state. Comparisons of mean lumen caliberamong those groups used pooled Student's t tests.Comparisons of body surface area (BSA)-normalizedlumen area for 12 main artery segments from normalmen, women, and men with LVH or DCM were madeby Sign test,20 as was a comparison between long,medium-length, and short terminal branch arteries at 19segments, each with three subsegments. The influenceof age on arterial lumen diameter was tested byANOVA. A difference was considered statistically sig-nificant if the two-sided probability of the observedresult, under the null hypothesis, was p<0.05.
ResultsBaseline Patient CharacteristicsThe 83 patients (Table 1) were of mean age 45+± 13
years and had normal blood pressure (systolic, 118+15mm Hg; diastolic, 71+9 mm Hg) and normal lipids (TC,187±36 mg/dl; LDL, 120±32 mg/dl; HDL, 44±12 mg/dl; apo B, 101±25 mg/dl). Of 50 normal men in whomall artery segments were measured, diastolic bloodpressure exceeded 85 mm Hg (maximum 95 mm Hg) insix. Those with normal blood pressure had a meanproximal subsegment (Llp, Rlp, and Clp) lumen diam-eter of 3.56 mm, and those with 285 mm Hg measured3.66 mm (p=NS). Among 50 normal men, the TC,LDL/HDL ratio, and apo B were measured in 48 andwere normal in 46, 46, and 44, respectively (<90thpopulation percentile for age21.22). Abnormal lipid levelshad no effect on lumen diameter in this group withnormal arteries. For example, 44 patients with normalapo B had a mean proximal subsegment lumen diameterof 3.57 mm; four with an elevated level measured 3.52mm (p=NS). We were able to obtain medication infor-mation for 73 of these 83 patients. By the exclusioncriterion, none of these patients continued chronicnitrates at the time of catheterization; for three who had
been taking chronic nitrates, lumen diameters were notdifferent from patients not on nitrates. Similarly, lumencaliber was unaffected in three patients receiving cal-cium channel blockers; we know that these do notacutely affect epicardial lumen caliber.23
Error Calculations on Brass Tube Phantom ModelA comparison between computed and actual mea-
surements of the brass tube showed a high degree ofaccuracy. In five views, from 480 RAO to 480 LAO with200 caudal to 300 cranial angulation, errors between-0.13 and 0.10 mm were observed. The mean error(+SD) was <0.03 mm (±0.12), and the mean absoluteerror was 0.10 mm (+0.03), suggesting that the complexscaling logic was correctly implemented for thesemeasurements.
Repeatability of Lumen Diameter MeasurementA high degree of repeatability was observed when
arteriograms were reanalyzed. In six angiograms, thelumen diameters of a total of 213 subsegments wereremeasured, 132 by the original tracer and 81 by asecond tracer. For all vessels, the mean differencebetween first and second measurements (error) was0.12+0.34 mm, independent of vessel size over thediameter range of 0.5-5.0 mm. The mean intraobserverand interobserver errors were similar: 0.13±0.30 and0.10+0.40 mm, respectively.
Repeatability in Classification of Dominance, VesselIdentity, Branch Length, and Tortuosity
Comparisons between the original and second classi-fication sets reveal a high degree of precision. Anatomicdominance was exactly reidentified in 92% of 73 angio-grams; 8% had one-step differences involving large-RCA versus small-RCA dominance. Of the 161 brancharteries present on first reading, 95% were correctlyreidentified. Among these, branch length (long, me-dium, short) was correctly reclassified in 77%; oneseptal branch had more than a one-step difference.Tortuosity classification was exactly repeated in 83% of36 angiograms; the remainder had one-step differences.
Diameter of the Main Arteries inNormal Right-Dominant MenThe main coronary arteries are the conduit vessel
skeleton from which the branches ramify. They includethe LM, the interventricular course of the LAD, and theatrioventricular groove courses of the RCA and LCx.Each patient has 12 such segments; because of varyinganatomic dominance, there are 13 main artery segments
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

Dodge et al Normal Lumen Diameter
TABLE 2. Diameter Measurements of the Main Coronary Arteries in Normal Men
RCA dominant Small RCA dominant Balanced LCA dominantLocation n Diameter (mm) n Diameter (mm) n Diameter (mm) n Diameter (mm)Ri middle 20 3.9±0.6 9(a) 3.8±0.5 10 3.0±0.5t 10 2.8±0.5tR3 middle 20 3.1±0.5 10 2.6±0.6* 10 2.0±0.6t 10 1.1±0.4tLM middle 18(b) 4.5±0.5 10 4.6±0.7 9(b) 4.4±0.4 10 4.6±0.4Li middle 20 3.6±0.5 10 3.8±0.4 10 3.6±0.4 10 3.7±0.2L3 middle 20 1.7±0.5 10 1.9±0.5 10 1.8±0.4 10 2.0±0.3
Cl middle 20 3.4±0.5 10 3.5±0.8 10 3.4±0.5 10 4.2±0.6tC3 middle 19(c) 1.6±0.6 10 2.2±0.8* 10 2.5±0.5t 10 3.2±0.5tRCA, right coronary artery; LCA, left coronary artery; R, right coronary artery; LM, left main; L, left anterior
descending; C, circumflex (refer to Figure 1 and Table 5). Values are mean±SD.Reported segment numbers vary because of: (a) catheter-induced Rl spasm; (b) absent LM; (c) absent C3.*p<0.05, tp<0.01, small-RCA, balanced, or LCA-dominant groups compared with RCA-dominant group.For a complete tabulation see Table 6.
in this description (a patient may have either R4 or C4).As shown in Table 2 and Figure 5, lumen caliber at themidpoint of each segment varied from 4.5-mm diameterin the LM artery to 1.6 mm in the terminal LCx (C3).The coefficient of variation (SD/mean) of lumen diam-eter at these selected points is <0.25 in 75% of locationsand <0.20 in 58%. (A complete tabulation of the 12main artery segments in RCA-dominant men, each withthree subsegments, is presented in Table 6.)
Differences Among Main Arteries Caused byVariations in Anatomic DistributionAs shown in Table 2, the diameters of the LM artery
and segments of the LAD were unaffected by anatomicdistribution. The LCx, however, was usually significantlylarger when measured in a left-dominant distributionthan in a right. Conversely, the RCA was significantlylarger when measured in a right-dominant than in aleft-dominant or a balanced distribution. The normal
LlmLld12p %%%%%M% ' *
L3m,p13d_L4p'L4m y^XX,,,L4d_
ClmdC2mC2d_
I ** 1 1,
1 2 3 4
Mean Lumen Diameter ± SD (mm)
FIGuRE5. Bargraph showingmean lumendiameters ofmain artery segments in normalright-dominant men. RCA, right coronaryartery; LM, left main artery; LAD, leftanterior descending coronary artery; LCx,left circumflex artery. Artery segment abbre-viations are presented in Table 5.
51
5
RlpRlmRidR2p
RCA
LMpI-Mm_LM
LAD
LCx
C3pC3mC3d
0
aa
11 1
m,m,Zgp~ 0
m25 a
.1
0 A
a02 ^4
a
m71arlwr~l1
--------
p
R3M
=4p a a,R4m 0 9
JLMMLbm 1
1 9 9 a
1 5 a1
237
0
PAd X5XXXt
a! !
9
0a
1
a
EM-Ar-"a
a c
a0
1
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from
238 Circulation Vol 86, No 1 July 1992
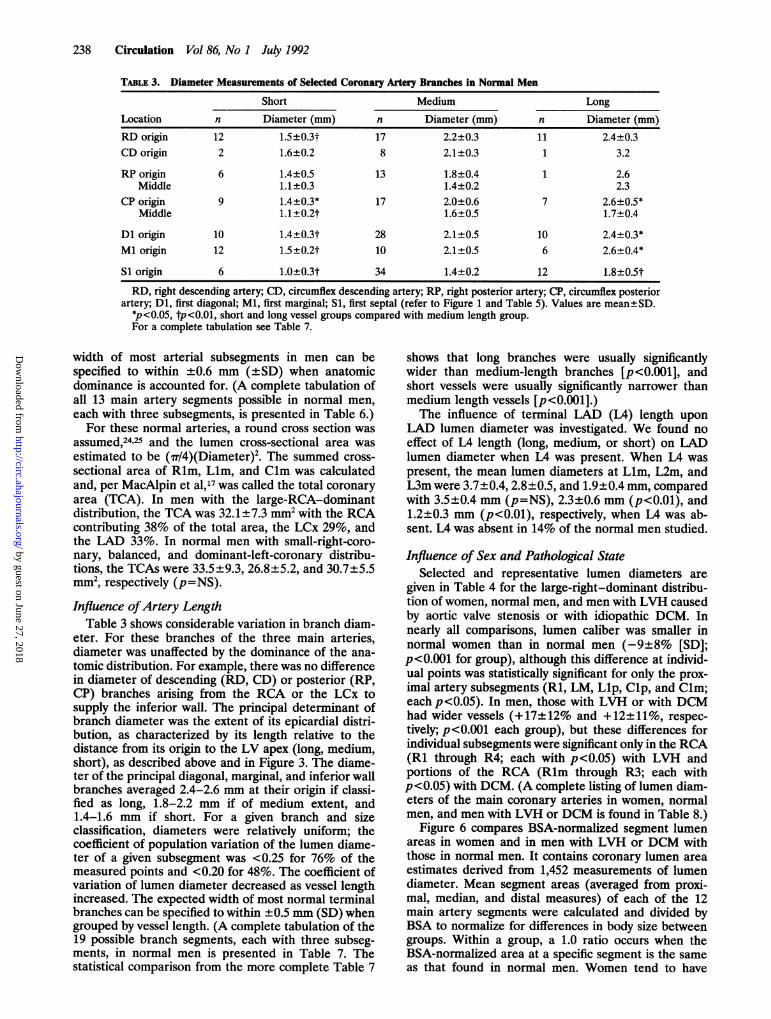
TABLE 3. Diameter Measurements of Selected Coronary Artery Branches in Normal Men
Short Medium LongLocation n Diameter (mm) n Diameter (mm) n Diameter (mm)RD origin 12 1.5±0.3t 17 2.2±0.3 11 2.4±0.3CD origin 2 1.6±0.2 8 2.1±0.3 1 3.2
RP origin 6 1.4±0.5 13 1.8±0.4 1 2.6Middle 1.1±0.3 1.4±0.2 2.3
CPorigin 9 1.4±0.3* 17 2.0±0.6 7 2.6±0.5*Middle 1.1 ±0.2t 1.6±0.5 1.7±0.4
Dl origin 10 1.4±0.3t 28 2.1±0.5 10 2.4±0.3*Ml origin 12 1.5±0.2t 10 2.1±0.5 6 2.6±0.4*
S1 origin 6 1.0±0.3t 34 1.4±0.2 12 1.8±0.5tRD, right descending artery; CD, circumflex descending artery; RP, right posterior artery; CP, circumflex posterior
artery; Dl, first diagonal; Ml, first marginal; S1, first septal (refer to Figure 1 and Table 5). Values are mean±SD.*p<0.05, tp<0.0l, short and long vessel groups compared with medium length group.For a complete tabulation see Table 7.
width of most arterial subsegments in men can bespecified to within ±0.6 mm (±SD) when anatomicdominance is accounted for. (A complete tabulation ofall 13 main artery segments possible in normal men,each with three subsegments, is presented in Table 6.)For these normal arteries, a round cross section was
assumed,24'25 and the lumen cross-sectional area wasestimated to be (i7/4)(Diameter)2. The summed cross-sectional area of Rlm, Llm, and Clm was calculatedand, per MacAlpin et al,17 was called the total coronaryarea (TCA). In men with the large-RCA-dominantdistribution, the TCA was 32.1±7.3 mm2 with the RCAcontributing 38% of the total area, the LCx 29%, andthe LAD 33%. In normal men with small-right-coro-nary, balanced, and dominant-left-coronary distribu-tions, the TCAs were 33.5 ±9.3, 26.8 +5.2, and 30.7+5.5mm2, respectively (p=NS).Influence ofArtery Length
Table 3 shows considerable variation in branch diam-eter. For these branches of the three main arteries,diameter was unaffected by the dominance of the ana-tomic distribution. For example, there was no differencein diameter of descending (RD, CD) or posterior (RP,CP) branches arising from the RCA or the LCx tosupply the inferior wall. The principal determinant ofbranch diameter was the extent of its epicardial distri-bution, as characterized by its length relative to thedistance from its origin to the LV apex (long, medium,short), as described above and in Figure 3. The diame-ter of the principal diagonal, marginal, and inferior wallbranches averaged 2.4-2.6 mm at their origin if classi-fied as long, 1.8-2.2 mm if of medium extent, and1.4-1.6 mm if short. For a given branch and sizeclassification, diameters were relatively uniform; thecoefficient of population variation of the lumen diame-ter of a given subsegment was <0.25 for 76% of themeasured points and <0.20 for 48%. The coefficient ofvariation of lumen diameter decreased as vessel lengthincreased. The expected width of most normal terminalbranches can be specified to within ±0.5 mm (SD) whengrouped by vessel length. (A complete tabulation of the19 possible branch segments, each with three subseg-ments, in normal men is presented in Table 7. Thestatistical comparison from the more complete Table 7
shows that long branches were usually significantlywider than medium-length branches [p<0.001], andshort vessels were usually significantly narrower thanmedium length vessels [p<O.OOi].)The influence of terminal LAD (L4) length upon
LAD lumen diameter was investigated. We found noeffect of L4 length (long, medium, or short) on LADlumen diameter when L4 was present. When L4 waspresent, the mean lumen diameters at Llm, L2m, andL3m were 3.7+0.4, 2.8±0.5, and 1.9±0.4 mm, comparedwith 3.5±0.4 mm (p=NS), 2.3±0.6 mm (p<0.01), and1.2±0.3 mm (p<O.01), respectively, when L4 was ab-sent. LA was absent in 14% of the normal men studied.
Influence of Sex and Pathological StateSelected and representative lumen diameters are
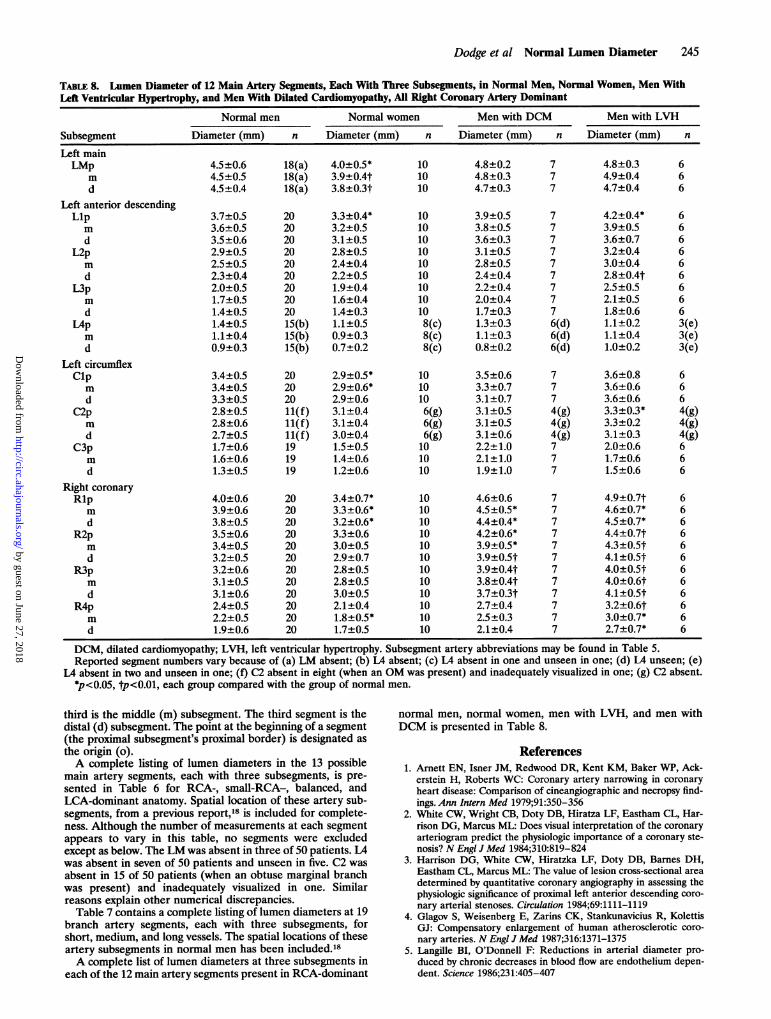
given in Table 4 for the large-right-dominant distribu-tion of women, normal men, and men with LVH causedby aortic valve stenosis or with idiopathic DCM. Innearly all comparisons, lumen caliber was smaller innormal women than in normal men (-9±8% [SD];p<O.OOi for group), although this difference at individ-ual points was statistically significant for only the prox-imal artery subsegments (R1, LM, Llp, Clp, and Clm;each p<0.05). In men, those with LVH or with DCMhad wider vessels (+17±12% and +12±11%, respec-tively; p<0.001 each group), but these differences forindividual subsegments were significant only in the RCA(Ri through R4; each with p<0.05) with LVH andportions of the RCA (Rlm through R3; each withp<0.05) with DCM. (A complete listing of lumen diam-eters of the main coronary arteries in women, normalmen, and men with LVH or DCM is found in Table 8.)
Figure 6 compares BSA-normalized segment lumenareas in women and in men with LVH or DCM withthose in normal men. It contains coronary lumen areaestimates derived from 1,452 measurements of lumendiameter. Mean segment areas (averaged from proxi-mal, median, and distal measures) of each of the 12main artery segments were calculated and divided byBSA to normalize for differences in body size betweengroups. Within a group, a 1.0 ratio occurs when theBSA-normalized area at a specific segment is the sameas that found in normal men. Women tend to have
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

Dodge et al Normal Lumen Diameter 239
TABLE 4. Effect of Sex, Left Ventricular Hypertrophy, and Dilated Cardiomyopathy on Selected Coronary ArteryDiameter Measurements in Right Coronary Artery-Dominant Patients
Normal men Normal women DCM men LVH men
Diameter Diameter Diameter DiameterLocation n (mm) n (mm) n (mm) n (mm)Rl middle 20 3.9±0.6 10 3.3±0.6* 7 4.5±0.5* 6 4.6±0.7*
(1.0±0.2) (0.8±0.2) (1.2±0.1) (1.2±0.2)
LM middle 18* 4.5±0.5 10 3.9±0.4t 7 4.8±0.3 6 4.9±0.4(1.0±0.1) (0.9±0.1) (1.1±0.1) (1.1±0.1)
Li middle 20 3.6±0.5 10 3.2±0.5 7 3.8±0.5 6 3.9±0.5(1.0±0.1) (0.9±0.1) (1.1±0.1) (1.1±0.1)
Cl middle 20 3.4±0.5 10 2.9±0.6* 7 3.3±0.7 6 3.6±0.6(1.0±0.1) (0.9±0.2) (1.0±0.2) (1.1±0.2)
DCM, dilated cardiomyopathy; LVH, left ventricular hypertrophy; R, right coronary artery; LM, left main; L, leftanterior descending artery; C, circumflex artery (refer to Figure 1 and Table 5). For each patient group/artery location,the mean±SD in millimeters is above, and the ratio (mean±SD) in normal men is below in parentheses.tReported segment numbers vary because of absent LM.*p<0.05, tp<0.01.A complete tabulation may be found in Table 8.
15.3% smaller BSA-normalized segment area for mainartery branches (p<O.O1), and men with LVH or withDCM have 36.8% (p<O.O1) or 30.5% (p<0.05) largersegment area, respectively, than normal men.
Influence ofAgeFigure 7 shows that there is no age-related trend in
TCA, as defined above, in normal men when normalizedfor BSA (p=NS). Thus, BSA-normalized TCA is a
constant (15.2±3.6 mm2/m2) for men of all ages. Nor-malized cross-sectional areas of individual main arteriesin all normal men likewise showed no trend with aging.
Influence of TortuosityWe found a positive correlation between age and
LAD tortuosity but none between LAD tortuosity andlumen diameter. The four tortuosity categories werenumbered in increasing order of tortuousness as illus-
Normal Females
3.0 5.0 1.0
Left VentricularHypertrophy
3.0
DilatedCardiomyopathy
5.0 1.0. -3.
3.0
Lumen Diameter in Normal Men (mm)FIGURE 6. Plots showing body surface area (BSA)-normalized lumen area at 12 main artery segment locations in women and
in men with left ventricular hypertrophy and dilated cardiomyopathy as a fraction ofthe area at that same location in normal men.
2.01
MEL O
a o
.0i
Eo4E .5
1.8
1.6
1.4
1.2
1.0
0.8'
0.6
0.4
a
a a
p < 0.01
a
* l
m Ua
p < 0.01
* a
p < 0.050.2'
&.I)
1.8
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
0.0ll
1.0 5.0
_ ~ ~~ ~ ~ ~ ~ ~ ~ --11-, . ...* v n--r-
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

240 Circulation Vol 86, No 1 July 1992
E
Vli.E04U,
0.
20-
10*
0
10 20 30 40 s0 60 70
A~
FIGURE 7. Scatterplot showing body surface area (BSA)-normalized total coronary area (TCA) in normal men versus
age. The best-fit line is y=15. 7-O.lAge. Thus, TCA in menwith apparently normal coronary arteries is virtually constantat 15.2+3.6 mm21m2. *, Large-right dominant (n=20); A,
small-right dominant (n=9); *, balanced (n=10); o, leftdominant (n=10).
trated in Figure 4 (nontortuous, 1; slightly tortuous, 2;moderately tortuous, 3; and severely tortuous, 4). Inpatients younger than 38 years (n=20), those aged38-47 years (n=19), and those older than 47 years(n=21), the average tortuosity (±SD) was 2.3+0.8,3.0+0.8, and 3.2±0.9, respectively (p<0.01 for thecomparison of the younger group with the middle andwith the older group, p=NS for comparison of themiddle and older groups). L3m is in the region of theLAD that would appear most likely to be affected bytortuosity when L4 is present. In such patients, whenthe LAD was nontortuous or slightly tortuous (n=16),moderately tortuous (n= 15), and severely tortuous(n=9), average L3m lumen diameters relative to meansfor the entire group were +4%, -3%, and -2%different, respectively (p=NS).
Computer-Generated Model of Coronary ArteriesThe lumen diameters of normal men were integrated
into a computer program, previously described,'8 togenerate a two-dimensional projection of the coronaryartery tree with expected normal lumen diameters inany of the four anatomic dominances from any desiredviewing angle. This program generated the LCA treeseen in Figure 3.
DiscussionThe lumen diameters at 96 specified points in the
coronary anatomy have been measured in a group of 83patients who have no evidence of atherosclerotic dis-ease. The measurement method used has a mean errorof <0.03 mm for a measurement of 3.25 mm (<4%) inphantom models and a mean error of 0.12 mm inrepeated coronary arteriogram analysis. We found thatthe lumen diameter of most arterial subsegments can bespecified to within ±0.6 mm (SD) when the sex, ana-
tomic variation, branch length, and certain determi-nants of myocardial mass are accounted for. Branchartery caliber is unaffected by dominance of the ana-tomic distribution but is strongly influenced by branchlength. The coefficient of population variation is lessthan 0.25 in 75% of artery subsegments in large-RCA-dominant normal men.
Arteriographic measurements of coronary artery lu-men diameter during life in patients without coronaryartery disease have been reported infrequently.'726-28MacAlpin et al'7 made measurements at 12 locations inthe coronary artery tree using the techniques availablein the early 1970s. Despite method differences, our4,290 measurements of lumen diameters agree in mostcases with those obtained by others arteriographi-cally'7,26 and at postmortem examination.2728 For exam-ple, we report LM at 4.5±0.5 mm versus 4.3+0.6 mm17and 4.0 mm.27 At comparable proximal and middle LADartery subsegments, MacAlpin17 reported 3.5 +0.5 and2.0±0.4 mm versus our finding of 3.6±0.5 mm at themid-Li and 2.3±0.4 mm at the distal L2. A mid-Limeasure of 3.3±0.5 mm has been reported elsewhere.26RD has been reported as 2.11 mm27; pooling vessels ofdifferent lengths, we found 2.0±0.5 mm. Previous re-ports of normal TCA have been 25.7±4.8 mm2 (Refer-ence 17) and 33.3±10.4 mm2 (Reference 28); we reporta range of 26.8±5.2 to 33.5±9.3 mm2 (mean, 31.0+7.2mm2).
It has been suggested that both lumen diameter andvessel length are necessary for a quantitative descrip-tion of the coronary vascular network.29 To categorizelength, we compared the visible length of a branchartery with the distance between its origin and the apexof the heart (Figure 3). With this method, it is possibleto classify branch arteries of different absolute lengthsinto groups that have significantly different lumen di-ameters with reasonably small coefficients of populationvariation. In the LAD, lumen diameter was significantlyaffected by length only when the terminal LAD failed toreach the cardiac apex (approximately 15% ofoccurrences).TCA is known to correlate directly with myocardial
mass in both normal and hypertrophied hearts.28 Lumencross-sectional area in an individual coronary arteryafter maximum dilation is linearly related to the myo-cardial volume perfused in dogs30 and nearly linearlyrelated to the myocardial weight perfused in normalhuman hearts.31 Thus, we chose to compare lumencross-sectional area and not diameter between RCA-dominant normal men, women, and men with LVH orDCM, with normalization using BSA to compensate fordifferences between groups in body size.
In contrast to MacAlpin's'7 statement that differencesin lumen caliber between men and women could beacceptably resolved when TCA was normalized to BSA,we found this not to be the case. In our set of 1,011lumen measurements, women tended to have narrowercoronary arteries than men, a difference that persistedafter adjustment for body size. BSA-normalized coro-nary area in women is approximately 90% that in men,a finding in agreement with the observation that BSA-normalized LV mass in women is approximately 90% ofthat in men.32 The cause of this association with sex isunknown. This difference in vessel size may contributeto the greater operative mortality in women after coro-
Am
CA
U.---O ° -.
* *o A AU
30
. 1 5 9 5 5 1
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

Dodge et al Normal Lumen Diameter 241
nary artery bypass graft surgery33-35; however, ourmeasurements at two of the five most commonly graftedsites (L2 and R3) were not significantly different be-tween men and women. Too few of the remaining threecommon graft sites (M1, Dl, and RD) were measured inwomen to allow comparisons. Other explanations forthis operative mortality difference have been offered.36With 441 lumen measurements in the main arteries of
male patients with LVH or DCM, our results comparefavorably with measurements made by others duringlife7"26 and postmortem.28'37 Resting blood flow per unitmyocardium is normal in patients with severe aorticvalve disease38 and decreased in those with DCM,39whereas myocardial mass is greatly increased inboth.40,4l The total blood flow is thus increased inpatients with aortic stenosis4243 and may be increased inpatients with DCM.39 We found coronary area to besignificantly increased in hypertrophied and dilatedhearts. As total flow equals cross-sectional area multi-plied by velocity, this is probably an adaptive phenom-enon, with coronary size increasing to satisfy myocardialdemand for an augmented blood supply37 while preserv-ing velocity by means of partially characterized autoreg-ulatory pathways.5"12
Arteries are said to dilate with age, as they diffuselynarrow with progressive intimal disease.46,7 Dependingon the predominant effect, either greater or lesserlumen diameter would result. During aging, the histo-logical increase in diameter of the internal elasticaoffsets increased intimal thickness, possibly as an adap-tation to the advance of intimal thickening with agerather than a direct effect of aging on the arterial wall.4We found no evidence that lumen caliber is influencedby age in these adults without angiographically apparentatherosclerosis, a finding in agreement with that ofothers.44The population variation in tortuosity of the coronary
artery tree, increasing with age, has long been noted.45As did others,44 we found a significant positive relationbetween age and tortuosity but no significant relationbetween tortuosity and lumen diameter. Tortuosity maybe a normal aging phenomenon and not secondary to adisease process.The percent diameter stenosis is the most commonly
used arteriographic index of coronary disease severity,but objections have been raised to its use in patientswith atherosclerosis.1-3 Chief among these is that nar-rowed segments are frequently compared with adjacentless narrowed but diffusely diseased segments, and thusthe actual severity of a lesion may be underestimated.As a result, in humans, measures of percent stenosis donot correlate with the physiological significance of cor-onary atherosclerotic lesions ranging from 20% to60%.3The physiological impact of a stenosis is related to the
blood pressure loss (AP) that occurs as blood flowsthrough it. This is reasonably well approximated by thedynamic loss, AP=3.8 (Q/A )2, where Q is blood flow(cm3/sec), A, is minimum lumen cross-sectional area(mm2) in the stenosis, and AP is in millimeters ofmercury.23 Because the arterial flow volume differsgreatly at different points in the coronary anatomy, nosingle value of stenosis area, A,, can be used to estimatea lesion's severity. However, the ratio (normal flow/normal area) (QN/AN) is experimentally a fairly constant
velocity in arteries of various sizes'6 and can be esti-mated at QN/AN= 11.1 cm/sec for a proximal LAD ofarea 10.2 mm2 (3.6 mm diameter; see Table 2) supplyingits basal myocardial needs of 68 ml/min.46 As normaltotal flow is maintained in the face of substantialnarrowing, the physiological impact of the stenosis canbe approximated as AP=0.05 (AN/A,)2 using the twoexpressions above. Thus, hypothetically, a better arte-riographic index of the hemodynamic impact of a ste-notic coronary artery lesion at any site in the coronaryanatomy might result from the above comparison of themeasured minimum area with its expected normal areaat that site. The value of this approach remains to betested. This report represents an important first steptoward investigating this hypothesis by determiningwhether and with what degree of confidence it ispossible to specify the expected lumen caliber of a givennormal coronary artery segment.These normal widths have been included in an edu-
cational Macintosh computer program'8 (see Figure 3)permitting a two-dimensional projection of the three-dimensional normal coronary artery tree from anyuser-specified viewing angle. This may be of benefit tofirst-year cardiology fellows; medicine, surgery, andradiology residents; medical students; and others tryingto develop an appreciation for the normal coronaryanatomy.
Certain limitations of our study may have increasedmeasurement variance. These include infrequent in-stances of retrospectively unavailable information onLV size or wall thickness, concomitant drug use (10 of83 patients), and lack of direct measures of scalingcatheter dimensions, which may introduce 1-2% addi-tional variance.47 Automated quantitative angiographicmeasurements of nonnylon catheters may systematicallyunderestimate true size (by micrometer) by 3.5%47;however, this does not affect dimensional accuracy withthe approach we use.19 Finally, a relatively small num-ber of normal women and men with DCM or LVH werestudied.With this article, an anatomic nomenclature scheme
has now been fully defined. It is concise, easy toremember because of the correspondence of the loca-tion code to the widely accepted coronary arterialnomenclature, and repeatable. We have shown in nor-mal men that the combination of subsegment location,anatomic distribution pattern (RCA dominant, small-RCA dominant, balanced, and LCA dominant), and thebranch artery length categories (long, medium, short,and absent) permits an estimate of normal lumendiameter with a relatively small population variance. Webelieve that this anatomic scheme18 corresponds to theclinically relevant coronary anatomy and should beconsidered for use as a standardized description ofthese vessels in future investigations.
AppendixQuantitative Description of the Human CoronaryAnatomy: Nomenclature and Measurements ofSubsegment Spatial Location andNormal Lumen Diameter
In a coronary arteriogram, the anatomic segments shown inFigure 1 can be located (not all segments are labeled).Although coronary anatomy tends to be somewhat morevariable than Figure 1 suggests, it is usually easy to specify
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

242 Circulation Vol 86, No 1 July 1992
TABLE 5. Abbreviations of Coronary Artery Nomenclature
Abbreviation Name Description
Main arteriesLADLCALCxLMRCA
Main artery segmentsClC2C3C4
LlL2L3L4LMRIR2R3R4
Branch artery segmentsA1-A3
CD
CI
CP
DI-D3
M1-M3
MROAOM
OPRD
RI
RP
S1-S3
Suffixes (subsegments)dm0
p
Left anterior descendingLeft coronary arteryLeft circumflexLeft mainRight coronary artery
LCx first segmentLCx second segmentLCx third segmentLCx fourth segment
LAD first segmentLAD second segmentLAD third segmentLAD fourth segmentLeft mainRCA first segmentRCA second segmentRCA third segmentRCA fourth segment
Acute marginals
Posterior descending
Inferior
Posterior
Diagonals
Marginals
Median ramusAnterior branch OMObtuse marginal
Posterior branch OMPosterior descending
Inferior
Posterior
Septals
DistalMiddleOriginProximal
LCx from its origin at the LM to Mi (or OM, if Ml is absent)LCx from Ml to M2 (or OM) (not present if Ml is absent)LCx from M2 (or OM) to CP (if present, otherwise to end of LCx)LCx from CP along atrioventricular groove to end of LCx (absent in RCAand small-RCA-dominant distributions)
LAD from its origin at the LM to SiLAD from Si to S3LAD from S3 to the cardiac apexLAD from the cardiac apex to its terminal point on the inferior wallLCA from ostium to bifurcation of LCA into LAD and LCxRCA from its origin to AlRCA from Al to A3RCA from A3 to RD (if present, otherwise to end of RCA)RCA from the RD along atrioventricular groove to end of RCA (absent in
balanced and LCA-dominant distributions)
Three largest branches arising from the RCA to supply the rightventricular wall, numbered from most proximal to most distal
Distal most inferior wall branch arises from C4, present only inleft-dominant anatomy
Inferior wall branch arises from C4, present only in balanced andleft-dominant anatomy
Proximal most inferior wall branch arises from junction of C3 and C4,present in small-right, balanced, and left-dominant anatomy
Three largest branches arising from the LAD to supply the left ventricularanterior free wall, numbered from most proximal to most distal
Three largest branches arising from the LCx to supply the left ventricularlateral free wall, numbered from most proximal to most distal
An anatomic variant arising at a trifurcation of the LMAnterior distal branch of OMAnatomic variant present when one branch artery off the LCx is much
larger than its neighbors supplying the left ventricular lateral free wallPosterior distal branch of OMProximal most inferior wall branch arises from junction of R3 and R4,
present in right, small-right, and balanced-dominant anatomyInferior wall branch arises from R4, present only in right and
small-right-dominant anatomyDistal most inferior wall branch arises from R4, present only in
right-dominant anatomyThree largest branches arising from the LAD to supply the interventricular
septal wall, numbered from most proximal to most distal
Midpoint of the distal third of an artery segmentMidpoint of the middle third of an artery segmentOrigin of an artery segment (proximal border)Midpoint of the proximal third of an artery segment
segments that correspond approximately to these standardones as described in Table 5. The LM artery has a singlesegment. The LAD is separated into four segments, as illus-trated in Figure 1, defined by 1) its origin from the LM, 2) thefirst septal perforator (S1), 3) the third septal perforator (S3,not labeled in Figure 1), 4) the cardiac apex, and 5) its terminalpoint on the inferior wall. S3 commonly arises near the bend ofthe LAD in RAO views and often is near the origin of thesecond diagonal. These landmarks may serve as alternativemarkers. If none of these are identified, the L2-L3 transitionis defined as halfway from Si to the cardiac apex. Branchesfrom the main arteries are numbered from proximal (1) todistal (3). The possible branches of the LAD included thethree largest septal branches (S1-S3) and the three largestdiagonal branches (D1-D3). A median ramus branch is an
anatomic variant arising at a trifurcation of the LM and iscalled a branch. Because of the variable nature of the branchesthat originate at or very near the bifurcation of the LM, theangiographer must decide whether a given case is best classi-fied as a first diagonal (D1), first marginal (M1), or if inter-mediate between the two, as a median ramus.The LCx, with a right- and small-right-dominant anatomy,
is divided into three parts (Cl, C2, and C3) by the first andsecond marginal branches (Ml and M2). In this case, theatrioventricular groove continuation of the LCx (C3) is usuallysmall. In the case of small-right-dominant anatomy, theposterior wall branch (CP) originates at the distal end of C3.With a balanced anatomic distribution, the LCx has a fourthsegment (C4) distal to CP and gives rise to an inferior wallbranch (CI). With a left dominant anatomy, the LCx also gives
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

Dodge et al Normal Lumen Diameter 243
TABLE 6. Lumen Diameter and Spatial Location of 13 Main Artery Segments, Each With Three Subsegments, in Normal Men
Lumen diameterRCA dominant Small RCA dominant Balanced dominant LCA dominant Spatial location'8
Subsegment Diameter (mm) n Diameter (mm) n Diameter (mm) n Diameter (mm) n r 6 4' n
18(a) 4.6+0.518(a) 4.6±0.518(a) 4.6+0.5
20202020202020202015(b)15(b)15(b)
20202011(f)11(f)11(f)19(h)19(h)19(h)0
0
0
202020202020202020202020
3.9+0.43.8±0.43.8±0.53.5±0.6t2.9±0.72.5±0.62.1±0.61.9±0.51.7±0.41.3±0.31.1±0.41.0±0.3
3.6±0.73.5±0.83.5±0.83.0±0.83.0±0.82.9±0.82.2±0.8*2.2±0.8*2.1±0.8t
3.9±0.53.8±0.53.7±0.43.3±0.43.2±0.52.8±0.62.6±0.5*2.6±0.6*2.6±0.62.0±0.61.6±0.3t1.5±0.4*
101010
1010101010101010108(c)8(c)8(c)
1010109(g)9(g)9(g)101010000
9(j)9(j)9(j)101010101010101010
4.3±0.44.4±0.44.4±0.3
3.8±0.23.6±0.43.4±0.52.8±0.72.5±0.42.3±0.42.0±0.41.8±0.41.6±0.31.3±0.41.2±0.40.9±0.3
3.6±0.63.4±0.53.5±0.53.1±0.53.2±0.43.1±0.62.6±0.6t2.5±0.5t2.3±0.5t1.7±0.31.5±0.41.5±0.4
3.1±0.4t3.0±0.5t3.0±0.5t2.7±0.4t2.7±0.4t2.5±0.3t2.1±0.5t2.0±0.6t2.0±0.6t
9(a) 4.6+0.49(a) 4.6±0.49(a) 4.5 ±0.4
1010101010101010108(d)8(d)8(d)
1010107(g)7(g)7(g)
1010109 (i)9 (i)9 (i)
1010101010101010100
0
0
3.8+0.33.7+0.23.5±0.33.1±0.42.8+0.42.6±0.4*2.4±0.4*2.0+0.31.9±0.5t1.7±0.41.5±0.2*1.1+0.2
4.3±0.6t4.2+0.6t4.1±0.6t3.4±0.6*3.4+0.6*3.3+0.73.3+0.6t3.2+0.5t2.9+0.5t2.4+0.52.2+0.52.1±0.5
2.8+0.5t2.8+0.St2.7+0.St2.3+0.3t2.2+0.3t1.5+0.4t1.2+0.3t1.1+0.4t0.8+0.3t
RCA, right coronary artery; LCA, left coronary artery; r, radius; 6, azimuth angle between projection of r onto transverse plane andanterior-posterior axis; '1, angle between r and transverse plane. Subsegment artery abbreviations may be found in Table 5. Values aremean±SD.
Reported subsegment numbers vary because of (a) LM absent; (b) L4 absent; (c) L4 absent in one and unseen in one; (d) L4 unseen;(e) L4 absent in one and unseen in two; (f) C2 absent in eight (when an OM was present) and inadequately visualized in one; (g) C2 absent;(h) no atrioventricular groove continuation of LCx after OM; (i) C4 absent because of shared origin of CP and CI; (j) catheter-induced Rlspasm.
*p<0.05, tp<0.01, small-RCA, balanced, or LCA-dominant groups compared with the RCA dominant group.
rise to the posterior descending artery (CD). A large obtusemarginal branch (OM) with anterior (OA) and posterior (OP)branches may substitute for Ml and M2 if a single branch ofthe LCx is much larger than its neighbors, although an Ml or
M3 is permitted if they are also present. With an OM presentand Ml absent, C2 is absent by definition. A third marginal(M3) is usually small and is often absent. The possiblebranches of the LCx include M1-M3, OM, OA, OP, CP, CI,and CD.The RCA, with a right-dominant anatomy, is divided into
four parts between 1) its origin, 2) the first acute marginalbranch (A1), 3) the third acute marginal branch (A3), 4) the
posterior descending branch (RD), and 5) the origin of the
posterior wall branch (RP). An inferior wall branch (RI) isalso specified. With a small-right-dominant anatomy, the RDand RI are present, and the posterior wall vessel arises fromthe LCx. In the case of a balanced anatomy, only the RD arisesfrom the RCA to supply the inferior septum of the LV. Witha left-dominant anatomy, the inferior wall vessels arise fromthe LCx, as described above. The possible terminal branchesof the RCA include the three largest acute marginal branches(A1-A3), which supply the wall of the right ventricle, inaddition to the previously described RD, RI, and RP.Subsegment nomenclature is as follows. All artery segments
can be trisected to create three subsegments. The first segrnentthird is the proximal (p) subsegrnent. The second segment
Left mainLMpmd
Left anteriordescendingLlpmd
L2pmd
L3pmd
L4pmd
Left circumflexClpmd
C2pmd
C3pmd
C4pmd
Right coronaryRlpmd
R2pmd
R3pmd
R4pmd
4.5±0.64.5±0.54.5±0.4
3.7±0.53.6±0.53.5±0.62.9±0.52.5±0.52.3±0.42.0±0.51.7±0.51.4±0.51.4±0.51.1±0.40.9±0.3
3.4±0.53.4±0.53.3±0.52.8±0.52.8±0.62.7±0.51.7±0.61.6±0.61.3±0.5
4.0±0.63.9±0.63.8±0.53.5±0.63.4±0.53.2±0.53.2±0.63.1±0.53.1±0.62.4±0.52.2±0.51.9±0.6
101010
1010101010101010107(e)7(e)7(e)
1010107(g)7(g)7(g)101010101010
101010101010101010000
0.3 8300.7 8001.1 790
1.6 7002.3 6303.0 5904.0 5105.3 44°6.5 3908.0 330
10.1 30011.8 31012.2 32011.8 33011.4 340
1.4 8601.8 9402.2 10202.6 10703.1 11603.6 12004.1 12604.7 13505.4 14105.7 15605.9 16606.2 1180
0.5 -7101.7 -6802.6 -66`3.4 -6904.6 -7205.6 -7706.2 -8406.4 -9106.7 1506.6 14006.2 18106.2 1710
70 1940 1900 19
-30 19-50 19-80 19-90 19
-120 19-170 19-230 19-320 19-400 19-460 16-490 16-520 16
-12° 19-240 19-310 19-330 18-370 18-410 18-450 17-510 17-560 17-67° 6-710 6-730 6
-220 24-24° 24-300 24-390 24-480 24-550 24-620 24-690 24-730 24-710 24-660 24-570 24
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from
244 Circulation Vol 86, No 1 July 1992
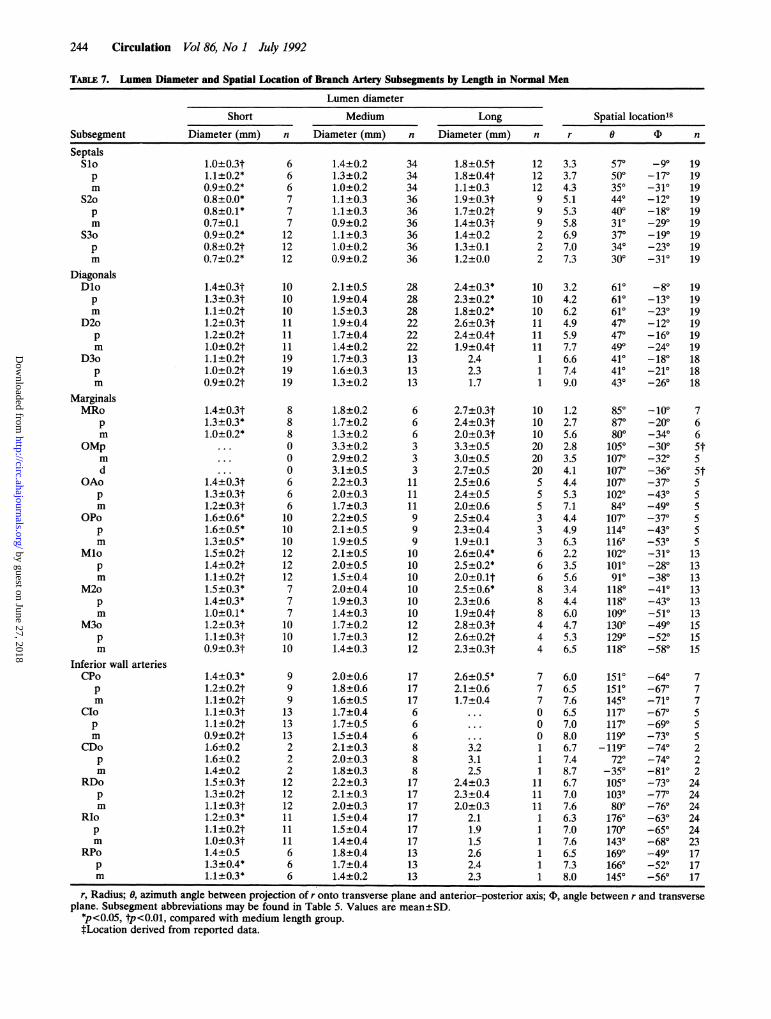
TABLE 7. Lumen Diameter and Spatial Location of Branch Artery Subsegments by Length in Normal Men
Lumen diameter
Short Medium Long Spatial location18Subsegment Diameter (mm) n Diameter (mm) n Diameter (mm) n r 0 ( n
SeptalsSlopm
S2opm
S3opm
DiagonalsDlopm
D2opm
D3opm
MarginalsMRo
pm
OMpm
dOAo
pm
OPopm
Mlopm
M2opm
M3opm
Inferior wall arteriesCPo
pm
CIopm
CDopm
RDopm
RIopm
RPo
pm
1.0L0.3t1.1+0.2*0.9+0.2*0.8±0.0*0.8±0.1*0.7±0.10.9±0.2*0.8±0.2t0.7±0.2*
1.4±0.3t1.3±0.3t1.1±0.2t1.2±0.3t1.2±0.2t1.0±0.2t1.1 ±0.2t1.0±0.2t0.9±0.2t
1.4±0.3t1.3±0.3*1.0±0.2*
. . .
. . .
1.4±0.3t1.3±0.3t1.2±0.3t1.6±0.6*1.6±0.5*1.3±0.5*1.5±0.2t1.4±0.2t1.1±0.2t1.5±0.3*1.4±0.3*1.0±0.1*1.2±0.3t1.1±0.3t0.9±0.3t
1.4+0.3*1.2±0.2t1.1±0.2t1.1±0.3t1.1±0.2t0.9±0.2t1.6±0.21.6±0.21.4±0.21.5±0.3t1.3±0.2t1.1±0.3t1.2±0.3*1.1±0.2t1.0±0.3t1.4+0.51.3±0.4*1.1±0.3*
666777121212
101010111111191919
8880
0
0
666101010121212777
101010
999
131313222121212111111666
1.4±0.21.3±0.21.0±0.21.1±0.31.1±0.30.9±0.21.1±0.31.0+0.20.9±0.2
2.1±0.51.9±0.41.5±0.31.9±0.41.7±0.41.4±0.21.7±0.31.6±0.31.3±0.2
1.8±0.21.7±0.21.3±0.23.3±0.22.9±0.23.1±0.52.2±0.32.0±0.31.7±0.32.2±0.52.1±0.51.9±0.52.1±0.52.0±0.51.5±0.42.0±0.41.9±0.31.4±0.31.7±0.21.7±0.31.4±0.3
2.0±0.61.8±0.61.6±0.51.7±0.41.7±0.51.5±0.42.1±0.32.0±0.31.8±0.32.2±0.32.1±0.32.0±0.31.5±0.41.5±0.41.4±0.41.8±0.41.7±0.41.4±0.2
343434363636363636
282828222222131313
666333
111111999101010101010121212
171717666888171717171717131313
1.8±0.5t1.8±0.4t1.1±0.31.9±0.3t1.7±0.2t1.4±0.3t1.4±0.21.3±0.11.2±0.0
2.4±0.3*2.3±0.2*1.8±0.2*2.6±0.3t2.4±0.4t1.9±0.4t
2.42.31.7
2.7±0.3t2.4±0.3t2.0±0.3t3.3±0.53.0±0.52.7±0.52.5±0.62.4±0.52.0±0.62.5±0.42.3±0.41.9±0.12.6±0.4*2.5±0.2*2.0±0.1t2.5±0.6*2.3+0.61.9±0.4t2.8±0.3t2.6±0.2t2.3±0.3t
2.6±0.5*2.1±0.61.7±0.4
3.23.12.5
2.4±0.32.3±0.42.0±0.3
2.11.91.52.62.42.3
12 3.312 3.712 4.39 5.19 5.39 5.82 6.92 7.02 7.3
10 3.210 4.210 6.211 4.911 5.911 7.71 6.61 7.41 9.0
10 1.210 2.710 5.620 2.820 3.520 4.15 4.45 5.35 7.13 4.43 4.93 6.36 2.26 3.56 5.68 3.48 4.48 6.04 4.74 5.34 6.5
7 6.07 6.57 7.60 6.50 7.00 8.01 6.71 7.41 8.7
11 6.711 7.011 7.61 6.31 7.01 7.61 6.51 7.31 8.0
570500
350440400310370340300
610610610470470490410410430
850870800
10501070107010701020840
10701140116010201010910
11801180109°130012901180
151015101450117011701190
-1190720350
10501030800
176017001430169016601450
_90
-170-31°-12°-18°-290-190-230-310
-80-13°-230-120-160-24`-180-210-260
-100-20`340
-300
-320-360370430490370430530
-31°-280-38°-41`-430-510490
-520-58°
-640-67`-71`-670-690730740
-740-810730770
-760-630-650-680490
-52°-560
1919191919
19191919
191919191919181818
7
66
5t5
5t5S
55
5
13
13
13
13
13
13151515
777S
5
5222
242424242423171717
r, Radius; 0f azimuth angle between projection of r onto transverse plane and anterior-posterior axis; (D, angle between r and transverseplane. Subsegment abbreviations may be found in Table 5. Values are mean±+SD.
*p<0.05, tp<0.01, compared with medium length group.*Location derived from reported data.
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from
Dodge et al Normal Lumen Diameter 245
TABLE 8. Lumen Diameter of 12 Main Artery Segments, Each With Three Subsegments, in Normal Men, Normal Women, Men WithLeft Ventricular Hypertrophy, and Men With Dilated Cardiomyopathy, All light Coronary Artery Dominant
Normal men Normal women Men with DCM Men with LVH
Subsegment Diameter (mm) n Diameter (mm) n Diameter (mm) n Diameter (mm) n
Left mainLMp
md
Left anterior descendingLlpmd
L2pmd
L3pmd
L4pmd
Left circumflexClpmd
C2pmd
C3pmd
Right coronaryRlpmd
R2pmd
R3pmd
R4pmd
4.5±0.64.5±0.54.5+0.4
3.7±0.53.6±0.53.5±0.62.9±0.52.5±0.52.3±0.42.0±0.51.7±0.51.4±0.51.4+0.51.1±0.40.9±0.3
3.4±0.53.4±0.53.3±0.52.8±0.52.8±0.62.7±0.51.7±0.61.6±0.61.3±0.5
4.0±0.63.9±0.63.8±0.53.5±0.63.4±0.53.2±0.53.2±0.63.1±0.53.1±0.62.4±0.52.2±0.51.9±0.6
18(a) 4.0±0.5*18(a) 3.9+0.4t18(a) 3.8±0.3t
20202020202020202015(b)15(b)15(b)
20202011(f)11(f)11(f)191919
202020202020202020202020
3.3±-0.4*
3.2+0.53.1±0.52.8±0.52.4±0.42.2±0.51.9±0.41.6±0.41.4±0.31.1±0.50.9±0.30.7±0.2
2.9±0.5*2.9±0.6*2.9±0.63.1±0.43.1±0.4
3.0±0.41.5±0.51.4±0.61.2±0.6
3.4±0.7*
3.3±0.6*3.2±0.6*3.3±0.63.0±0.52.9±0.72.8±0.52.8±0.53.0±0.52.1±0.41.8±0.5*1.7±0.5
DCM, dilated cardiomyopathy; LVH, left ventricular hypertrophy. Subsegment artery abbreviations may be found in Table 5.Reported segment numbers vary because of (a) LM absent; (b) IA absent; (c) L4 absent in one and unseen in one; (d) L4 unseen; (e)
L4 absent in two and unseen in one; (f) C2 absent in eight (when an OM was present) and inadequately visualized in one; (g) C2 absent.*p<0.05, tp<0.01, each group compared with the group of normal men.
third is the middle (m) subsegment. The third segment is thedistal (d) subsegment. The point at the beginning of a segment(the proximal subsegment's proximal border) is designated asthe origin (o).A complete listing of lumen diameters in the 13 possible
main artery segments, each with three subsegments, is pre-sented in Table 6 for RCA-, small-RCA-, balanced, andLCA-dominant anatomy. Spatial location of these artery sub-segments, from a previous report,"8 is included for complete-ness. Although the number of measurements at each segmentappears to vary in this table, no segments were excludedexcept as below. The LM was absent in three of 50 patients. [Awas absent in seven of 50 patients and unseen in five. C2 was
absent in 15 of 50 patients (when an obtuse marginal branchwas present) and inadequately visualized in one. Similarreasons explain other numerical discrepancies.Table 7 contains a complete listing of lumen diameters at 19
branch artery segments, each with three subsegments, forshort, medium, and long vessels. The spatial locations of theseartery subsegments in normal men has been included.18A complete list of lumen diameters at three subsegments in
each of the 12 main artery segmnents present in RCA-dominant
normal men, normal women, men with LVH, and men withDCM is presented in Table 8.
References1. Arnett EN, Isner JM, Redwood DR, Kent KM, Baker WP, Ack-
erstein H, Roberts WC: Coronary artery narrowing in coronaryheart disease: Comparison of cineangiographic and necropsy find-ings. Ann Intern Med 1979;91:350-356
2. White CW, Wright CB, Doty DB, Hiratza LF, Eastham CL, Har-rison DG, Marcus ML: Does visual interpretation of the coronaryarteriogram predict the physiologic importance of a coronary ste-nosis? N Engl J Med 1984;310:819-824
3. Harrison DG, White CW, Hiratzka LF, Doty DB, Barnes DH,Eastham CL, Marcus ML: The value of lesion cross-sectional area
determined by quantitative coronary angiography in assessing thephysiologic significance of proximal left anterior descending coro-
nary arterial stenoses. Circulation 1984;69:1111-11194. Glagov S, Weisenberg E, Zarins CK, Stankunavicius R, Kolettis
GJ: Compensatory enlargement of human atherosclerotic coro-
nary arteries. N Engl J Med 1987;316:1371-13755. Langille BI, O'Donnell F: Reductions in arterial diameter pro-
duced by chronic decreases in blood flow are endothelium depen-dent. Science 1986;231:405-407
101010
1010101010101010108(c)8(c)8(c)
1010106(g)6(g)6(g)
101010
101010101010101010101010
4.8±0.24.8+0.34.7±0.3
3.9±0.53.8±0.53.6±0.33.1±0.52.8±0.52.4±0.42.2±0.42.0±0.41.7±0.31.3±0.31.1±0.30.8±0.2
3.5±0.63.3±0.73.1±0.73.1±0.53.1±0.53.1±0.62.2±1.02.1±1.01.9±1.0
4.6±0.64.5±0.5*4.4±0.4*4.2±0.6*3.9±0.5*3.9±0.5t3.9±0.4t3.8±0.4t3.7±0.3t2.7±0.42.5±0.32.1±0.4
777
7777777776(d)6(d)6(d)
7774(g)4(g)4(g)777
777777777777
4.8+0.34.90.44.7+0.4
4.2±0.4*3.90.53.6±0.73.2±0.43.0±0.42.8±0.4t2.5±0.52.1±0.51.8±0.61.1±0.21.1±0.41.0±0.2
3.6±0.83.6±0.63.6±0.63.3±0.3*3.3±0.23.1±0.32.0±0.61.7±0.61.5±0.6
4.9±0.7t4.6±0.7*4.5±0.7*4.4±0.7t4.3±0.5t4.1±0.5t4.0-0.5t4.0±0.6t4.1±0.5t3.2±0.6t3.0±0.7*2.7±0.7*
666
6666666663(e)3(e)3(e)
6664(g)4(g)4(g)666
666666666666
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

246 Circulation Vol 86, No 1 July 1992
6. Learoyd BM, Taylor MG: Alterations with age in the viscoelasticproperties of human arterial walls. Circ Res 1966;18:278-292
7. Bader H: Dependence of wall stress in the human thoracic aortaon age and pressure. Circ Res 1967;20:354-361
8. Markis JE, Joffe CD, Cohn PF, Feen DJ, Herman MV, Gorlin R:Clinical significance of coronary artery ectasia.Am J Cardiol 1976;37:217-222
9. Swaye PS, Fisher LD, Litwin P, Vignola PA, Judkins MP, KempHG, Mudd JG, Gosselin AJ: Aneurysmal coronary artery disease.Circulation 1983;67:134-138
10. Hartnell GG, Parnell BM, Pridie RB: Coronary artery ectasia: Itsprevalence and clinical significance in 4,993 patients. Br Heart J1985;54:392-395
11. Takahashi M, Mason W, Lewis AB: Regression of coronary aneu-rysms in patients with Kawasaki syndrome. Circulation 1987;75:387-394
12. Jaffe RB, Glancy DL, Epstein SE, Brown BG, Morrow AG: Cor-onary arterial-right heart fistulae: Long-term observations inseven patients. Circulation 1973;48:133-143
13. Young DF, Cholvin NR, Roth AC: Pressure drop across artificiallyinduced stenoses in the femoral arteries of dogs. Circ Res 1975;36:735-743
14. Gould KL, Lipscomb K: Effects of coronary stenoses on coronaryflow reserve and resistance. Am J Cardiol 1974;34:48-55
15. Gould KL, Lipscomb K, Hamilton GW: Physiologic basis forassessing critical coronary stenosis: Instantaneous flow responseand regional distribution during coronary hyperemia as measuresof coronary flow reserve. Am J Cardiol 1974;33:87-94
16. Gould KL, Kelley KO: Physiological significance of coronary flowvelocity and changing stenosis geometry during coronary vasodi-lation in awake dogs. Circ Res 1982;50:695-704
17. MacAlpin RN, Abbasi AS, Grollman JH, Eber L: Human coronaryartery size during life. Radiology 1973;108:567-576
18. Dodge JT, Brown BG, Bolson EL, Dodge HT: Intrathoracic spatiallocation of specified coronary segments on the normal humanheart. Circulation 1988;78:1167-1180
19. Brown BG, Bolson E, Frimer M, Dodge HT: Quantitative coro-nary arteriography: Estimation of dimensions, hemodynamic resis-tance, and atheroma mass of coronary artery lesions using thearteriogram and digital computation. Circulation 1977;55:329-337
20. Dixon WJ, Massey FJ Jr: Introduction to Statistical Analysis. NewYork, McGraw-Hill Book Co, Inc, 1969, pp 335-340
21. Heiss G, Tamir I, Davis CE, Tyroler HA, Rifkind BM, SchonfeldG, Jacobs D, Frantz ID Jr: Lipoprotein-cholesterol distributions inselected North American populations: The Lipid Research ClinicsProgram prevalence study. Circulation 1980;61:302-315
22. Wahl PW, Warnick GR, Albers JJ, Hoover JJ, Walden CE, Berge-lin RO, Olgilvie JT, Hazzard WR, Knopp RH: Distribution oflipoprotein triglyceride and lipoprotein cholesterol in an adultpopulation by age, sex, and hormone use. Atherosclerosis 1981;39:111-124
23. Brown BG, Bolson EL, Dodge HT: Dynamic mechanisms inhuman coronary stenosis. Circulation 1984;70:917-922
24. Liu LB, Richardson T, Holt JH, Taylor CB: Luminal eccentricityand deformity in atherosclerotic coronary arteries. ParoiArterielle1976;3:167-169
25. Brown BG, Petersen RB: Computer-assisted measurements of cor-onary artery stenosis. (reply) Circulation 1979;60:1196
26. Kimball BP, LiPreti VL, Bui S, Wigle ED: Comparison of proximalleft anterior descending and circumflex coronary artery dimen-sions in aortic valve stenosis and hypertrophic cardiomyopathy.AmJ Cardiol 1990;65:767-771
27. Baroldi G, Scomazzoni G: Coronary Circulation in the Normal andthe Pathologic Heart. Washington, DC, Armed Forces Institutes ofPathology, 1967, pp 5-23
28. Harrison CV, Wood P: Hypertensive and ischemic heart disease: Acomparative clinical and pathological study. Br Heart J 1949;11:205-229
29. Zamir M, Chee H: Segment analysis of human coronary arteries.Blood Vessels 1987;24:76-84
30. Koiwa Y, Bahn RC, Ritman EL: Regional myocardial volumeperfused by the coronary artery branch: Estimation in vivo. Circu-lation 1986;74:157-163
31. Woods JD: Relative ischaemia in the hypertrophied heart. Lancet1961;1:696-698
32. Kennedy JW, Baxley WA, Figley MM, Dodge HT, Blackmon JR:Quantitative angiocardiography: I. The normal left ventricle inman. Circulation 1966;34:272-278
33. Kennedy JW, Kaiser GC, Fisher LD, Fritz JK, Meyers W, MuddJG, Ryan TJ: Clinical and angiographic predictors of operativemortality from the Collaborative Study in Coronary Artery Sur-gery (CASS). Circulation 1981;63:793-802
34. Spray TL, Roberts WC: Status of the grafts and the native coro-nary arteries proximal and distal to coronary anastomotic sites ofaortocoronary bypass grafts. Circulation 1977;55:741-749
35. Fisher LD, Kennedy JW, Davis KB, Maynard C, Fritz JK, KaiserG, Myers WO: Association of sex, physical size, and operativemortality after coronary artery bypass in the Coronary ArterySurgery Study (CASS). J Thorac Cardiovasc Surg 1982;84:334-341
36. Kahn SS, Nessim S, Gray R, Czer LS, Chaux A, Matloff J:Increased mortality of women in coronary artery bypass surgery:Evidence for referral bias. Ann Intern Med 1990;112:561-567
37. Rodriguez FL, Robbins SL: Capacity of human coronary arteries.Circulation 1959;19:570-578
38. Rowe GG, Afonso S, Lugo JE, Castillo CA, Boake WC, CrumptonCW: Coronary blood flow and myocardial oxidative metabolism atrest and during exercise in subjects with severe aortic valve disease.Circulation 1965;32:251-257
39. Henry PD, Eckberg D, Gault JH, Ross J Jr: Depressed inotropicstate and reduced myocardial oxygen consumption in the humanheart. Am J Cardiol 1973;31:300-306
40. Kennedy JW, Twiss RD, Blackmon JR, Dodge HT: Quantitativeangiocardiography: III. Relationships of left ventricular pressure,volume, and mass in aortic valve disease. Circulation 1968;38:838-845
41. Benjamin JI, Schuster EH, Bulkley BH: Cardiac hypertrophy inidiopathic dilated congestive cardiomyopathy: A clinicopathologicstudy. Circulation 1981;64:442-447
42. Fallen EL, Elliott WC, Gorlin R: Mechanisms of angina in aorticstenosis. Circulation 1967;36:480-488
43. Bertrand ME, LaBlanche JM, Tilmant PY, Thieuleux FP, DelforgeMR, Carre AG: Coronary sinus blood flow at rest and duringisometric exercise in patients with aortic valve disease. Am J Car-diol 1981;47:199-205
44. Hutchins GM, BuLldey BH, Miner MM, Boitnott JK: Correlationof age and heart weight with tortuosity and caliber of normalhuman coronary arteries. Am Heart J 1977;94:196-202
45. Gross L: The Blood Supply of the Heart. New York, Hoeber, 1921,p 151
46. Ganz W, Tamura K, Marcus HS, Donoso R, Yoshida S, SwanHJC: Measurement of coronary sinus blood flow by continuousthermodilution in man. Circulation 1971;44:181-195
47. Reiber JHC, Kooijman CJ, den Boer A, Serruys PW: Assessmentof dimensions and image quality of coronary contrast cathetersfrom cineangiograms. Cathet Cardiovasc Diagn 1985;11:521-531
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

J T Dodge, Jr, B G Brown, E L Bolson and H T Dodgevariation, and left ventricular hypertrophy or dilation.
Lumen diameter of normal human coronary arteries. Influence of age, sex, anatomic
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1992 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.86.1.232
1992;86:232-246Circulation.
http://circ.ahajournals.org/content/86/1/232the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from