ludwig © 2013 heinz ludwig department of medicine i center for oncology, hematology and palliative...
TRANSCRIPT
Ludwig© 2013
Heinz LudwigDepartment of Medicine I
Center for Oncology, Hematology and Palliative CareWilhelminenhospital, Vienna, Austria
What we know about myeloma in elderly patients from trials and observational
studies?

Ludwig© 2013
Rapid symptom control
Optimal quality of life
Few and acceptable side effects
Best possible quality of response
Long PFS
Long OS
Cure ?
Goals of therapy in elderly patients

Ludwig© 2013
1-drug* 2 - drugs 3- drugs 4 - drugs
Dex Bendamustine+P
MPT VMPT
Thal VD VMP
MP* CTD
Thal-Dex VTD
L-ldDex
Most commonly used combinations contain 2-3 drugs
*only exceptional cases
Drug combinations for elderly patients
Possible options

H. Ludwig 2013
Characteristics of the Elderly Patient Chronological age does not necessarily correlate with biological age
The variation in biological fitness in a specific age cohort increases with rising age, but the ‚biology‘ of myeloma cells does not vary with age
All three individuals are 70 years old
Fit Minor morbidity significant morbidity

Ludwig© 2013
Assess fraility
Fit Unfit Frail
Full go
Slow go
Very slow go
2 or 3 drug regimen
reduce dose 2 (3) drug regimen
further dose reduction MP, CTX-P
VD, Ld
Treatment of patients with multiple myeloma not eligible for transplantation

H. Ludwig 2013
Instruments for assessing fraility and allocation to treatment groups
Fit Unfit Frail
Age <80 yr Fit >80 yr Unfit >80 yr
ADL 6
IADL 8
Charlson 0
ADL 5
IADL 6-7
Charlson 1
ADL ≤4
IADL ≤5
Charlson ≥2
Go-go Moderate-go Slow-go
Full-dose
regimens
Dose level 0
Reduced-dose
regimens
Dose level -1
Reduced-dose
Palliative
approach
Dose level -2
Palumbo A et al. IMW 2013
AssessAgeADLIADLCharlson comorbidity score

H. Ludwig 2013
Adaptation of dose according to risk factors
Agent Dose level 0 Dose level-1 Dose level - 2
Dexamethasone 40 mg 20 mg 10 mg
Melphalan0.25 mg/kg or 9
mg/m2
0.18 mg/kg or 7.5 mg/m2
0.13 mg/kg or 5 mg/m2
Thalidomide 100 mg 50 mg 50 mg/qod
Lenalidomide 25 mg 15 mg 10 mg
Bortezomib1.3 mg twice weekly, sc
1.3 mg weekly, sc1.0 mg weekly,
sc
Prednisone 60 mg/m2 30 mg/m2 15 mg/m2
Cyclophosphamide 100 mg 50 mg 50 mg/qod
Palumbo et al.,BLOOD 2011Palumbo et al.,BLOOD 2011

H. Ludwig 2013
Polyneuropathy Avoid bortezomib (or use once weekly sc)
Renal impairment Consider dose adaptations when using lenalidomide
Bone marrow insufficiencyCareful dosing of cytoreductive drugs, consider single agent dexamethasone
Cardiac arrhythmias/
dysfunctionCave: Thalidomide & high dose dexamethasone
Immune system Careful dosing of cytoreductive drugs
Diabetes Cave: high dose dexamethasone
Cognitive function/compliance
Consider iv regimens
Comorbidities relevant for treatment selection in myeloma

H. Ludwig 2013
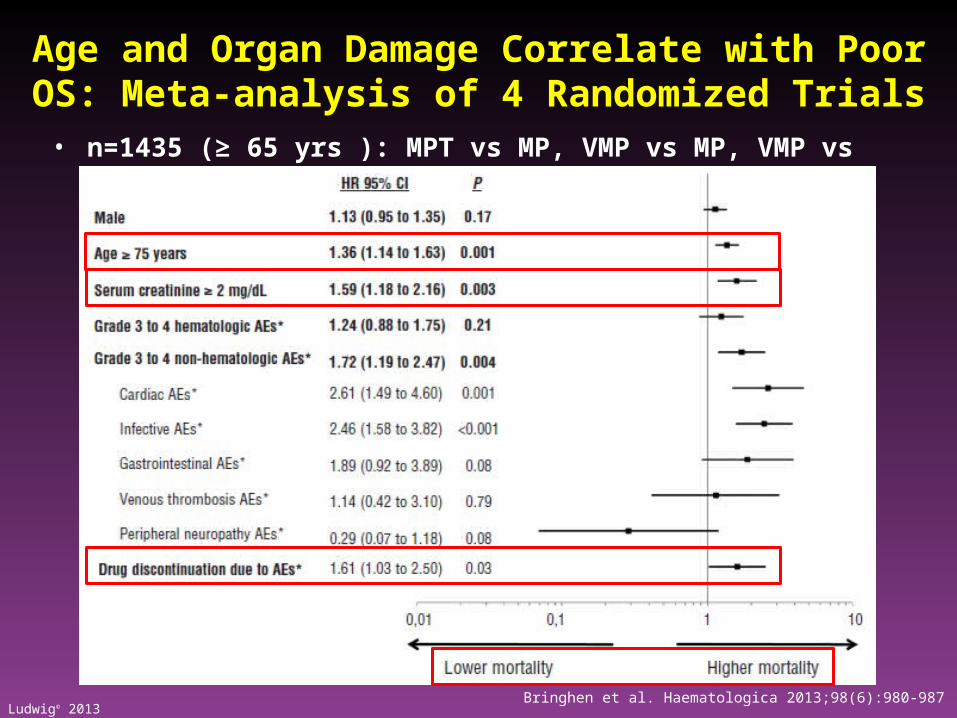
Higher risk of mortality in patients ≥ 75 years of age
• Median follow up 33 months
• Median OS in total population 50 months
• Estimated 3-year OS 68% in patients < 75 years of age vs 57% in patients ≥ 75 years of age (HR 1.44, CI 1.20-1.72, p < 0.001)
Bringhen S, et al. Haematologica. 2013;98:980-7.
Retrospective meta-analysis of 4 EU phase III trials (N = 1,435) with MP, MPT, VMP, and VMPT
HR (95% CI) p value
All 1.44 (1.20–0.72) < 0.001
MP 1.21 (0.90–1.64) 0.21
MPT 1.12 (0.81–1.56) 0.49
VMP 1.62 (1.04–2.52) 0.03
VTP/VMPT 3.02 (1.86–4.90) < 0.001
Higher mortality in patients ≥ 75 years of age
1 100.1
Higher mortality in patients < 75 years of age
Ludwig© 2013
• n=1435 (≥ 65 yrs ): MPT vs MP, VMP vs MP, VMP vs VMPT-VT
Bringhen et al. Haematologica 2013;98(6):980-987
Age and Organ Damage Correlate with Poor OS: Meta-analysis of 4 Randomized Trials

H. Ludwig 2013
New Regimen Comparator Outcome
MPT (6 Trials)* vs. MP MPT PFS 5/6, OS 2/6
CTDa vs. MP CTDa ORR
VMP vs. MP VMP PFS, OS
VMPT VT vs. VMP VMPT VT
PFS. OS
VMP VT or VP VDT VT or VP
ns
MPR R vs. MPR
or MP
MPR R
PFS
LD vs. Ld Ld PFS, OS
LD continous vs. Ld x 18, vs MPT x 12
Ld cont PFS, OS
*Meta-analysis of the 6 trials: PFS () OS
Phase III studies incorporating novel agents in the non-transplant setting

H. Ludwig 2013
MPT vs MP: Meta-analysis of 1685 individual-patient data of 6 randomized trials
Fayers et al. Blood 2011, accepted for publication 30 May 2011
0.0
0.2
0.4
0.6
0.8
1.0
Su
rviv
al p
rop
ort
ion
0 12 24 36 48
months
MPMPT
Median 14.9 mos (14.0-16.6)
Median 20.3 mos (18.8-21.6)
HR=0.67 in favor of MPT, p<0.0001
PFS
0.0
0.2
0.4
0.6
0.8
1.0
0 12 24 36 48months
Median 32.7 mos (30.5-36.6)
Median 39.3 mos(35.6-44.6)
HR=0.83 in favor of MPT, p=0.005*
OS
*Cox model for treatment, with analysis stratified by study using a random effects (frailty) model
MPMPT
H. Ludwig 2013
MPT: Pros and Cons
Pros
Survival benefit
Oral regimen
Not expensive
Cons
Thalidomide toxicity
Suboptimal in cytogenetic high risk
group
Shorter survival after relapse
H. Ludwig 2013
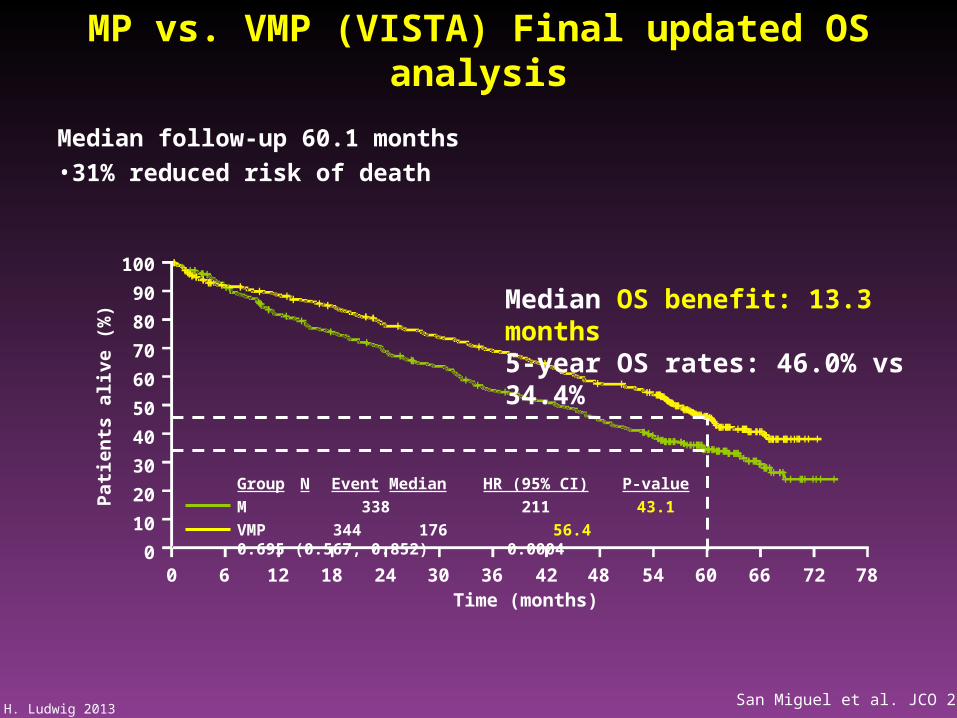
MP vs. VMP (VISTA) Final updated OS analysis
Median follow-up 60.1 months
•31% reduced risk of death
Median OS benefit: 13.3 months5-year OS rates: 46.0% vs 34.4%
100
90
80
70
60
50
40
30
20
10
0
Patie
nts
aliv
e (%
)
0 6 12 18 24 30 36 42 48 54 60 66 72 78Time (months)
Group N Event Median HR (95% CI) P-value
M 338 211 43.1
VMP 344 176 56.4 0.695 (0.567, 0.852) 0.0004
San Miguel et al. JCO 2013

H. Ludwig 2013San Miguel et al., JCO 2013
Overall survival in different subgroups: VMP vs. MP

H. Ludwig 2013
Time to next therapyTime to progression
Treatment-free interval Overall survival
Harousseau JL et al., BLOOD 2010
VMP induced CR is associated with improved outcome

H. Ludwig 2013
VD vs. VTD vs. VMP followed by bortezomib maintenance therapy
Niesvitzky R. et al., BLOO, 116 2010
Para-meter
VD VTD VMP
>VGPR 36% 44% 40%
ORR 68% 78% 71%
PNP G3-4
15% 26% 20%
PFS (mos)
13.8 18.4 17.3

H. Ludwig 2013
Global QoL during VD, VTD and VMP induction therapy
Niesvizky R et al., ASH 2011
VD vs. VTD or VMP: shorter PFS, similar OS, better tolerance
H. Ludwig 2013
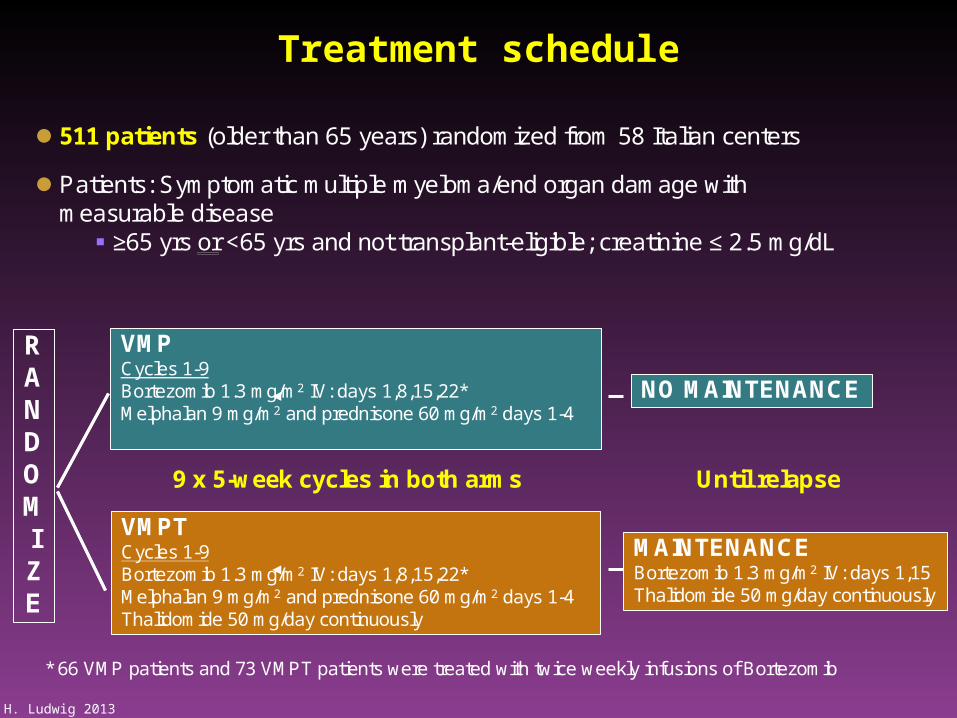
VMPCycles 1-9Bortezomib 1.3 mg/m2 IV: days 1,8,15,22*Melphalan 9 mg/m2 and prednisone 60 mg/m2 days 1-4
VMPTCycles 1-9Bortezomib 1.3 mg/m2 IV: days 1,8,15,22*Melphalan 9 mg/m2 and prednisone 60 mg/m2 days 1-4Thalidomide 50 mg/day continuously
RANDOMIZE
9 x 5-week cycles in both arms
511 patients (older than 65 years) randomized from 58 Italian centers
Patients: Symptomatic multiple myeloma/end organ damage with measurable disease
≥65 yrs or <65 yrs and not transplant-eligible; creatinine ≤ 2.5 mg/dL
Treatment scheduleTreatment schedule
MAINTENANCEBortezomib 1.3 mg/m2 IV: days 1,15Thalidomide 50 mg/day continuously
NO MAINTENANCE
Until relapse
* 66 VMP patients and 73 VMPT patients were treated with twice weekly infusions of Bortezomib
Treatment schedule

H. Ludwig 2013Palumbo A et al. ASH 2012
Progression free survival Overall survivallandmark analysis
PFS and OS: VMP vs VMPT –VT

H. Ludwig 2013
Age < 75 years
HR 0.76, 95% CI, 0.42-1.37, p =.36
Age ≥ 75 years
HR 0.60, 95% CI, 0.41-0.89, p=0.009 0.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70
0.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 700.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70
0.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70
0.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70
0.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70
0.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70
0.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70
0.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70
0.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70
0.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70
0.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60 70
ISS 3 VGPR/PR
ISS 1-2 CR
HR 0.66, 95% CI, 0.43-1.00, p =.05
HR 0.64, 95% CI, 0.31-1.31, p =.22
HR 0.45, 95% CI, 0.24-0.86, p =.01
HR 0.80, 95% CI, 0.54-1.20, p =.28
Off therapyVT maint. VMPT
VMP No maint.Off therapy
VT maint. VMPT
VMP No maint.No maint.Off therapy
VT maint. VMPT
VMP No maint.Off therapy
VT maint. VMPT
VMP No maint.No maint.Off therapy
VT maint. VMPT
VMP No maint.Off therapy
VT maint. VMPT
VMP No maint.No maint.
Overall survival Landmark analysis
Overall survival Landmark analysisOverall survival, Landmark analysis

H. Ludwig 2013
Overall survival from relapseOverall survival from relapse
HR 0.92, 95% CI, 0.66-1.28, p =.630.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60
HR 0.92, 95% CI, 0.66-1.28, p =.630.00
0.25
0.50
0.75
1.00
0 10 20 30 40 50 60
Pat
ien
ts (
%)
Time (months)
3-years OS Median OS
VMP
VMPT-VT
46% 27.3 months
47% 27.8 months
3-years OS Median OS
VMP
VMPT-VT
46% 27.3 months
47% 27.8 months
Palumbo et al. ASH 2012 (Abstract 200)
Overall survival from relapse

H. Ludwig 2013
VMPT-VT versus VMP in newly diagnosed elderly patients
• Significant OS benefit in patients
– < 75 years of age (none in pts > 75 years)
– With stage ISS 1-2 (tendency for OS in stage ISS 3)
– With CR (none in pts with VGPR/PR)
• Benefit in ‚good risk‘ patients with CR only
• Grade 3- 4 adverse events during VT maintenance
– PN 7%
– Hematological toxicity 5%
– Infection 3%
– Discontinuation due to AEs 12%
Palumbo et al. ASH 2012 (Abstract 200), oral presentation

H. Ludwig 2013
How to reduce toxicity of Bortezomib and and maintain efficacy?
Bortezomib once weekly
longer duration of therapy
similar cumulative dose
similar efficacy
less toxicty (G3/4 neurotoxicity)
Bortezomib subcutaneously
10 times lower serum peak concentration
similar area under the curve
less neurotoxicity
similar efficacy

H. Ludwig 2013
-
•Stratified by age (<75 years vs > 75 years) and stage (ISS I/II vs III)
• -ISS, International Staging System; MP, melphalan, prednisone; MPR, melphalan, prednisone, lenalidomide; MPR-R, melphalan, prednisone, lenalidomidewith lenalidomidemaintenance; PBO, placebo.
MP
M: 0.18 mg/kg, days 1-4
P: 2 mg/kg, days 1-4
PBO: days 1-21
MPR
M: 0.18 mg/kg, days 1-4P: 2 mg/kg, days 1-4
R: 10 mg/day po, days 1-21Placebo
Placebo
MPR-R
M: 0.18 mg/kg, days 1-4
P: 2 mg/kg, days 1-4R: 10 mg/day po, days 1-21
RA
ND
OM
IZA
TIO
N
Double-blind Treatment Phase
DiseaseProgression
Maintenance
Lenalidomide
(25 mg/day) +/-
Dexamethasone
Open-Label Extension Phase
Lenalidomide10 mg/daydays 1-21
Cycles (28-day) 1-9 Cycles 10+
N = 459, 82 centers in Europe, Australia, and Israel
MPR-R vs. MPR vs. MP (MM015 trial)

H. Ludwig 2013
0
HR, hazard ratio; MP, melphalan, prednisone; MPR, melphalan, prednisone, lenalidomide ; MPR -R, melphalan, prednisone, lenalidomidewith lenalidomidemaintenance; OS, overall survival; PFS, progression- free survival; TTP, time to progression.
Progression-Free and Overall SurvivalAll Patients
• TTP HR advantages were similar: MPR- R vs MP = 0.337; MPR vs MP = 0.826
Time (Months)
Pat
ien
ts (
%)
HR 0.395 P < .001
HR 0.796P = .135
0 10 20 30 400
25
50
75
100
Median PFS
MPR-R 31 months
MPR 14 months
MP 13 months
Median PFS
MPR-R 31 months
MPR 14 months
MP 13 months
0 20 30 40 50 60
4-year OS
MPR-R 59%
MPR 58%
MP 58%
4-year OS
MPR-R 59%
MPR 58%
MP 58%
Pat
ien
ts (
%)
25
50
75
10
100
HR 0.898 P = .579
HR 1.089P = .648
Time (Months)
Progression-free and overall survival

H. Ludwig 2013
HR, hazard ratio; MP, melphalan, prednisone; MPR, melphalan, prednisone, lenalidomide; MPR-R, melphalan, prednisone, lenalidomide with lenalidomide maintenance; OS, overall survival; PFS, progression-free survival.
PFS and OS With MPRPFS and OS With MPR--R and MPRR and MPRPatients Aged 65Patients Aged 65--75 Years75 Years
Time (Months)
Pa
tien
ts (
%)
0 10 20 30 400
25
50
75
100
Median PFS
MPR-R 31 months
MPR 15 months
MP 12 months
Median PFS
MPR-R 31 months
MPR 15 months
MP 12 months
HR 0.301 P < .001
HR 0.618P = .006
0 10 20 30 40 50 600
25
50
75
100
Time (Months)
Pa
tien
ts (
%)
4-Year OS
MPR-R 69%
MPR 61%
MP 58%
4-Year OS
MPR-R 69%
MPR 61%
MP 58%
HR 0.706 P = .133
HR 0.902P = .639
PFS and OS with MPR-R and MPR patients aged 65-75 years

H. Ludwig 2013
FIRST: Phase 3 trial of Lenalidomide + low-dose Dex vs MPT (IFM 07-01; MM-020)
Inclusion criteriaN = 1,623
•Previously untreated MM
•Age 65 years or not eligible for a transplant
•No neuropathy of grade > 2
Rd (28-day cycle; until disease progression)Lenalidomide 25 mg/day, days 1–21 Dexamethasone* 40 mg/day, days 1, 8, 15, and 22
Rd (28-day cycle; until disease progression)Lenalidomide 25 mg/day, days 1–21 Dexamethasone* 40 mg/day, days 1, 8, 15, and 22
Rd (28-day cycle; up to 18 cycles)Lenalidomide 25 mg/day, days 1–21 Dexamethasone* 40 mg/day, days 1, 8, 15, and 22
Rd (28-day cycle; up to 18 cycles)Lenalidomide 25 mg/day, days 1–21 Dexamethasone* 40 mg/day, days 1, 8, 15, and 22
Centres in EU, Switzerland, APAC, USA, and Canada
*In patients aged > 75 years: Dex 20 mg/day, melphalan 0.20 mg/kg/day, thalidomide 100 mg/day
MPT (6-week cycle; up to 12 cycles )Melphalan* 0.25 mg/kg/day, days 1–4Prednisone 2.0 mg/kg/day, days 1–4Thalidomide* 200 mg/day
MPT (6-week cycle; up to 12 cycles )Melphalan* 0.25 mg/kg/day, days 1–4Prednisone 2.0 mg/kg/day, days 1–4Thalidomide* 200 mg/day
Primary end-point: PFS
NCT00689936. Available from: www.clinicaltrials.gov.
RANDOMIZATION

H. Ludwig 2013
Trials & duration of therapy (months)
VMP (Vista) 12
MPT trials 6-18.5
CTDa 6-9
MPR-R 9, R untill PD
VMPT-VT 12.5, VT maintenance: 2 years
LD (MM20) Continously until PD/intolerance
Duration of therapy: minimally 6, maximally 12 monthsMost experts recommend ≈ 9 months
What is the optimal duration of first line therapy?

H. Ludwig 2013
CR rate (%) Median PFS (months) Median OS (months)
MP1,2 rare 11–20 29 - 43.45 - 49.42
BP2 - 14* 32
MPT3 10 20.3 39
CTDa4 13 13 33
VMP5 30 21.7–27.4 56.4
MPR-R6 10 31 59% (4-yr OS)
VMP-VT/VP7 42 35 58% (5-yr OS)
VMPT-VT8,9 42 35.3 59.3% (5-yr OS)
LD continuous10
≥PR 75% vs. 62%
28% ↓ risk for PD 22% ↓ risk for death
1MTCG. J Clin Oncol 1998;16(12):3832-422Ludwig et al., BLOOD 2009
2Pönisch et al. J Cancer Res Clin Oncol. 2006;132:205-12.3Fayers et al. Blood 2011; 118(5):1239-1247
4Morgan et al. Blood 2011;118:1231-8
5San Miguel et al. JCO 2013; 31(4): 448-4556Palumbo et al. N Engl J Med 2012;366(19):1759-69
7Mateos et al. Blood 2012; 120: 2581-25888Palumbo et al. ASH 2012 (Abstract 200), oral presentation9Palumbo et al. ASH 2011 (Abstract 653), oral presentation
10Facon et al. ASH 2013 (Abstract 2), oral presentation
Outcome with novel combinations

H. Ludwig 2013 Gay et al. Blood 2011; 117(11):3025-31
• Retrospective analysis: 3 randomized European trials of GIMEMA and HOVON groups (N=1175)
• First-line treatment
MP (n=332), MPT (n=332), VMP (n=257), VMPT-VT (n=254)
Significant benefit also seen when analysis is restricted to patients >75 years old
PFS OS
P<0.001 P<0.001
CR
VGPR
PR
CR
VGPR
PR
Pro
bab
ility
Pro
bab
ility
Hematologic CR correlates with long PFS and OS in elderly patients treated with novel agents

H. Ludwig 2013
100
80
60
40
20
PFS
Immunophenotypic CR 90% at 3y
“Stringent CR” 38% at 3y
Conventional CR 57% at 3y
PR (≥70% reduction) 28% at 3y
Paiva et al; J Clin Oncol. 2011;29(12):1627-33.
Immunophenotypc CR correlates with OS GEM2005 >65y

H. Ludwig 2013
Cytogenetic abnormalities are a major prognostic factor in elderly patients with MM: IFM experience
1,890 patients (median age 72, range 66–94), including 1,095 patients with updated data on treatment modalities and survival
1,890 patients (median age 72, range 66–94), including 1,095 patients with updated data on treatment modalities and survival
Whatever the treatment, t(4;14) and del(17p) were associated with shorter PFS and OS; similar results were achieved in the subgroup of 335 patients > 75 years
Whatever the treatment, t(4;14) and del(17p) were associated with shorter PFS and OS; similar results were achieved in the subgroup of 335 patients > 75 years
1. Avet-Loiseau H, et al. J Clin Oncol. 2013 31(22):2806-9. 2. Hulin et al. Blood 2012:[abstract 204].
0.50
1.00
0.75
0.25
0.00
Pro
bab
ilit
y o
f O
S
Time (years)1 2 3 4 50
OS according to t(4:14)
t(4:14) negt(4:14) pos
0.50
1.00
0.75
0.25
0.00
Pro
bab
ilit
y o
f O
S
Time (years)1 2 3 4 50
OS according to del(17p)
del(17p) < 60del(17p) ≥ 60
p < 10.4 p < 10.6

H. Ludwig 2013
The challenge of high-risk CA [t(4;14), del(17p), t(14;16)] in NDMM elderly patients
StudyNo of pts with high-risk CA
Outcome of high-risk CA patients
MPT/MP1 NR NR
CTDa/MP1
(MRC Myeloma IX)NR
CTDa does not overcome the effect of high-risk CA and is not significantly better than MP in high-risk CA
RD/Rd2 (E4A03) 21 2y OS=76% for high-risk CA vs 91%
VMP/MP3 (VISTA) 46Absence of OS benefit, median OS 44.1mo. VMP vs 50.6 mo., MP
VMP/VTP – VT/VP4
(GEM-05)44
Adverse prognosis of both t(4;14) and del (17p) regardless of induction and maintenance. Median OS t(4;14)=29 mo., del(17p) = 27mo.
First generation novel agents only partly overcome the negative prognosis of high-risk CA in newly diagnosed elderly patients with MM
First generation novel agents only partly overcome the negative prognosis of high-risk CA in newly diagnosed elderly patients with MM
1. Bergsagel PL, et al. Blood. 2013;121:884-91. 2. Rajkumar SV, et al. Lancet Oncol. 2010;11:29-37. 3. San Miguel J, et al. J Clin Oncol. 2013;31:448-55. 4. Mateos MV, et al. Blood. 2011;118:4547-53.

H. Ludwig 2013
Thalidomide
PFS
no improvement in OS
Reduced OS after relapse
Negative impact on high risk pts
Clinical practice
recommendations50 mg for ≈ 12 mos may be considered
Lenalidomide PFS-no improvement in OS-increased risk for SPM
Bortezomib-thalidomide Tendency for PFS and OS but not
significant superior over VP
Maintenance studies - summary

H. Ludwig 2013
Summary: Treatment results in elderly patients
MPT, PFS, +/- OS, can be toxic in elderly pts
VMP, PFS OS, may induce severe PNP
Ld, PFS, OS, low dose Dex recommended
Thal-Dex, an option for fit pts
CTDa vs MP, overall response rate, CR, VGPR
Bendamustine-Pred, approved for first line TX
Thalidomide maintenance PFS, but not OS
MPR with Lenalidomide maintenance PFS, but not OS
VT maintenance not significantly better than VP

H. Ludwig 2013
Maintenance
The natural course of multiple myeloma

H. Ludwig 2013
Treatment of relapsed/refractory MMGeneral considerations
Components of initial therapy
– Alkylating-based
– Dexamethasone-based
– IMiD-based
– Bortezomib-based
Efficacy of initial therapy
– Quality of response
– Tolerance of tretament
– Duration of respose
Patient status and type of relapse
– Age, performance status, glucose
metabolism
– Aggressive vs non-aggressive
relapse
– Bone marrow reserve
– Renal function impairment
– Pre-existing peripheral
neuropathy
– Oral vs. iv therapy
IMiD, immunomodulatory derivative; MM, multiple myeloma

H. Ludwig 2013
Frontline Therapy successful?
Yes No
Long duration of response Select other TX (Class switch)
Yes No
Repeat first line TX Select other TX
Bortezomib based frontline TX:
IMiD based frontline TX
IMiD-based TD MPT CTD Rd (MPR)
Bort-based VD VMP VTD
Treatment of Relapsed/Refractory Myeloma
Old TypeMPDCEPM-100 +ASCT Ludwig et al.
The Oncologist 2011
Pomalidomide

H. Ludwig 2013
Retreatment with bortezomib: a meta-analysis including 23 studies
• 23 trials, 1051 patients
• Patients refractory or not refractory to bortezomib
• 11 studies including bortezomib-refractory pts
• 6 studies excluding bortezomib-refractory pts
• 6 studies missing information on bortezomib-refractory pts
• Combinations
• Bortezomib ± Dex: 4 studies
• Bortezomib + combination therapy: 19 studies
Knopf et al. IMW 2013 (Abstract P-228), poster presentation
H. Ludwig 2013
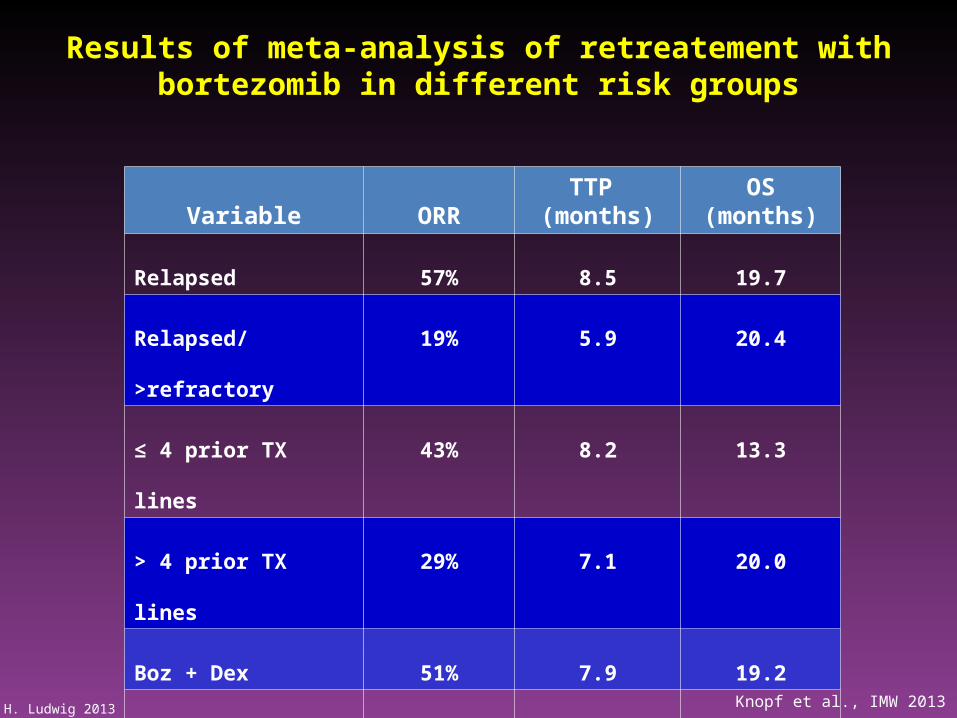
Results of meta-analysis of retreatement with bortezomib in different risk groups
Variable ORRTTP
(months)OS
(months)
Relapsed 57% 8.5 19.7
Relapsed/>refractory 19% 5.9 20.4
≤ 4 prior TX lines 43% 8.2 13.3
> 4 prior TX lines 29% 7.1 20.0
Boz + Dex 51% 7.9 19.2
Combination 36% 7.1 16.2
Pooled analysis 51% 8.4 19.2
Knopf et al., IMW 2013

H. Ludwig 2013
Carfilzomib a second generation proteasome inhibitor

H. Ludwig 2013
Single agent Carfilzomib in relapsed/refractory patients
Response category
All patients(n=267)
High risk cytogenetics(n=71)
CR 0.4% 0
VGPR 5.1% 4.2%
PR 18.3% 25.4%
MR 13.2% 4.2%
ORR 37% 29.5%
PFS(median) 3.7 mos 3.6 mos
DOR (median) 7.8 mos 6.9 mos
Progressive disease at enrollment, Relapsed from 2 prior TX lines, Must include bortezomib
Must include thalidomide or lenalidomide, Refractory to last line
Siegel D et al., BLOOD 2012
H. Ludwig 2013
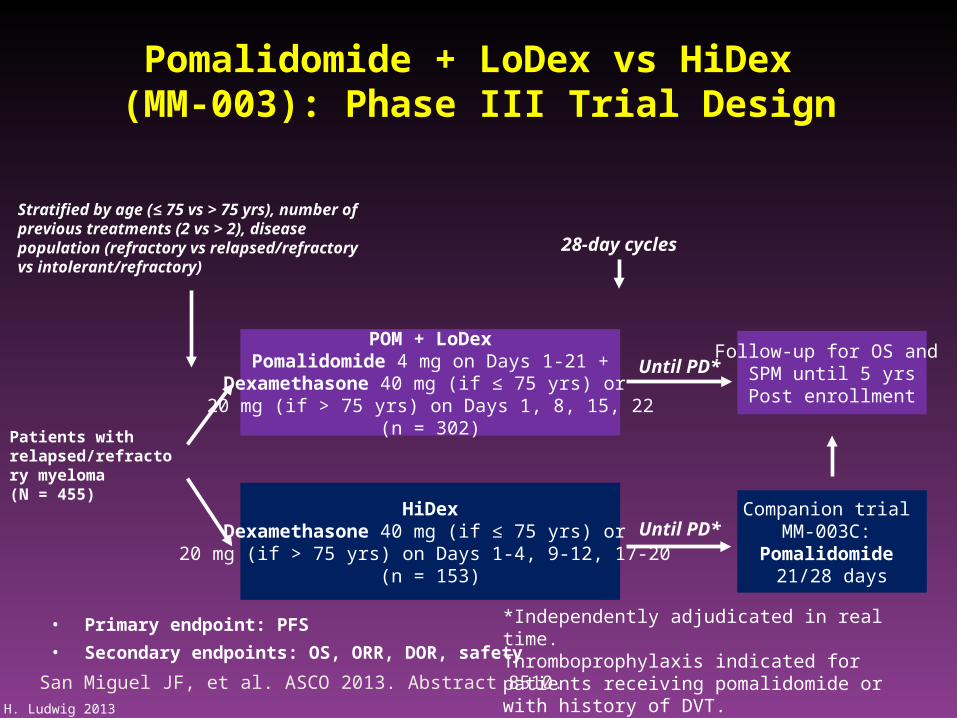
Patients with relapsed/refractory myeloma(N = 455)
POM + LoDexPomalidomide 4 mg on Days 1-21 +
Dexamethasone 40 mg (if ≤ 75 yrs) or 20 mg (if > 75 yrs) on Days 1, 8, 15, 22
(n = 302)
HiDexDexamethasone 40 mg (if ≤ 75 yrs) or
20 mg (if > 75 yrs) on Days 1-4, 9-12, 17-20 (n = 153)
28-day cycles
Stratified by age (≤ 75 vs > 75 yrs), number of previous treatments (2 vs > 2), disease population (refractory vs relapsed/refractory vs intolerant/refractory)
Until PD*Companion trial
MM-003C: Pomalidomide
21/28 days
Follow-up for OS and SPM until 5 yrsPost enrollment
Until PD*
San Miguel JF, et al. ASCO 2013. Abstract 8510.
Pomalidomide + LoDex vs HiDex (MM-003): Phase III Trial Design
• Primary endpoint: PFS
• Secondary endpoints: OS, ORR, DOR, safety *Independently adjudicated in real time.Thromboprophylaxis indicated for patients receiving pomalidomide or with history of DVT.

H. Ludwig 2013
Pomalidomide + LoDex vs HiDex: Key Criteria for Pts With Relapsed/Refractory MM
• All patients
– Refractory to last therapy
– ≥ 2 previous therapies
• ≥ 2 consecutive cycles of lenalidomide and bortezomib (alone or in combination) or
adequate previous alkylator therapy
– Failed bortezomib and lenalidomide
• Progression within 60 days; PR with progression within 6 mos, and/or bortezomib
intolerant after ≥ 2 cycles and achieving ≤ MR
– Refractory or relapsed/refractory
• Primary refractory (never achieved better than PD to any therapy) or relapsed and
refractory (relapsed after having ≥ SD for ≥ 2 cycles of therapy to ≥ 1 previous regimen
and then developed PD ≤ 60 days of completing their last treatment)
San Miguel JF, et al. ASCO 2013. Abstract 8510.

H. Ludwig 2013
Mos
Pomalidomide + LoDex vs HiDex (MM-003)
PFS (ITT Population) OS (ITT Population)
Mos
San Miguel JF, et al. ASCO 2013. Abstract 8510.

H. Ludwig 2013
Pomalidomide + LoDex vs HiDex Adverse Events (MM-003)
AE, % POM + LoDex(n = 300)
HiDex(n = 150)
Grade 3/4 hematologic AEs
Neutropenia 48 16
Anemia 33 37
Thrombocytopenia 22 26
Grade 3/4 nonhematologic AEs
Infections 30 24
– Pneumonia 13 8
Bone pain 7 5
Fatigue 5 6
Asthenia 4 6
Grade 3/4 AEs of interest
DVT/PE 1 0
Peripheral neuropathy* 1 1
Discontinuation due to AEs 9 10
*Includes hyperesthesia, peripheral sensory neuropathy, paraesthesia, hypoesthesia, and polyneuropathy.
San Miguel JF, et al. ASCO 2013. Abstract 8510.
H. Ludwig 2013
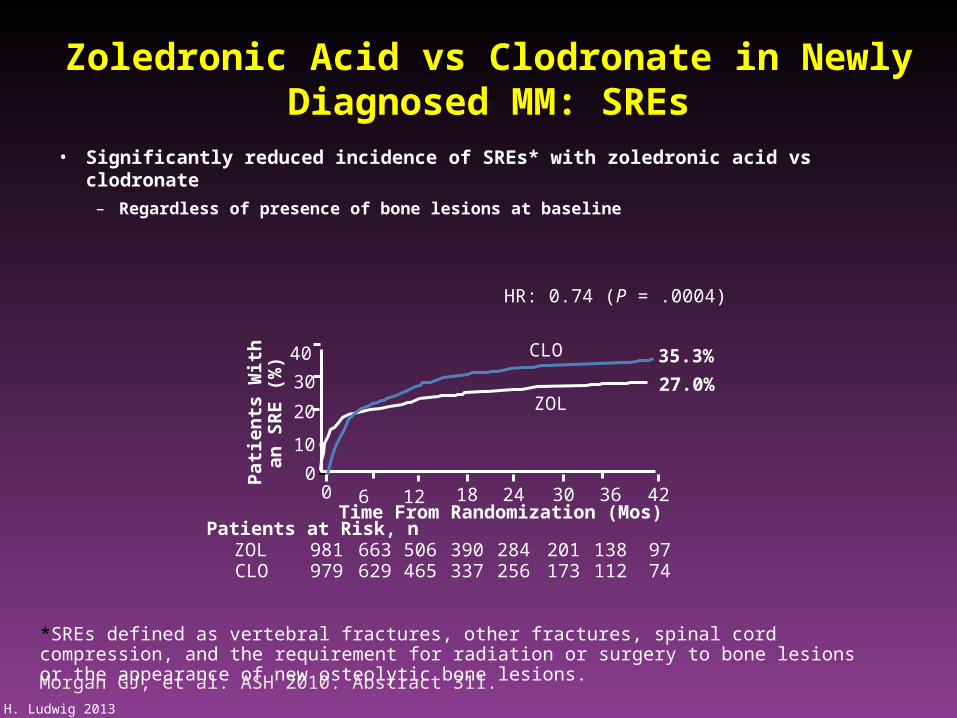
Zoledronic Acid vs Clodronate in Newly Diagnosed MM: SREs
Morgan GJ, et al. ASH 2010. Abstract 311.
• Significantly reduced incidence of SREs* with zoledronic acid vs clodronate
– Regardless of presence of bone lesions at baseline
HR: 0.74 (P = .0004)
*SREs defined as vertebral fractures, other fractures, spinal cord compression, and the requirement for radiation or surgery to bone lesions or the appearance of new osteolytic bone lesions.
Patients at Risk, n
0
10
20
30
ZOL
Pat
ien
ts W
ith
an
S
RE
(%
)
CLO981979
390337
284256
0 18 24
ZOL
Time From Randomization (Mos)
CLO40
138112
36
9774
42
663629
6
201173
30
506465
12
35.3%
27.0%

H. Ludwig 2013
Planned and/or ongoing studies
VD vs VTD vs VMP + V maintenance (UPFRONT study)
VRd vs Rd + Rd maintenance (SWOG S0777)
Rd vs MPT vs Rd + Rd maintenance (MM20/IM(FIRST trial)
Rd vs MPR vs CRP + maintenance R vs RP (EMNTG)
MPT+T vs MPR+R (HOVON 87-NMSG 18, ECOG EA1A06)
CTDa vs RCD +/- R maintenance (MRC Myeloma XI)
VP vs VMP vs VCP + VP maintenance (EMNTG)
Carfilzomib + MP ((CARMYSAP trial): ORR of 92% (40% VGPR). EHA 2012
MLN9708 plus LD and MLN9708 plus MP: EHA 2012
Rd vs MEL140 (DSMM XIII)
Pomalidomide + Dex vs Dexamethasone: MM 005
Alternating treatment with different regimens: VMP and RD (PETHEMA/GEM)
Bortezomib + Bendamustine + Prednisone (PETHEMA/GEM)

H. Ludwig 2013
New drugs in clinical evaluation
Agent Mechanism of action
Panobinostat, Vorinostat, Givinostat, Romidepsin
HDAC inhibitor
Perifosine, GSK2110183 Akt inhibitor
Temsirolismus, Everolismus mTOR inhibitor
Selumetinib MEK/ERK inhibitor
Plitidepsin (aplidin)Jun N-terminal Kinase (JNK) activator, anti-angiogenic activity
Dinaciclib CDK inhibitor
MLN8237 Aurora kinase inhibitor
ARRY-520 Kinesin spindle protein (KSP) inhibitor
Elotuzumab anti-CS1
Daratumumab anti-CD38
BHQ880 anti-DKK1
BT062 anti-CD138
Tabalumab Anti-B cell activiating factor (BAFF)
BI-505 Anti-intercellular adhesion molecule 1 (ICAM-1)

H. Ludwig 2013
Assess
- comorbidities
- degree of functional impairment
Select most appropriate drug regimen
Adapt dose if required
Consider the increased risk of infections within
first weeks/months of therapy
Optimize supportive care
-Antibiotics, antivirals, growth factors, anti-thrombotics
Recommendations for clinical practice

H. Ludwig 2013
Thank you for your attention
The future looks bright for elderly myeloma patients
The future looks bright for elderly myeloma patients

H. Ludwig 2013