lower extremity workshop gil c. grimes, md february 22 nd 2007
TRANSCRIPT

Lower Extremity Workshop
Gil C. Grimes, MDFebruary 22nd 2007
Objectives
Indications for aspiration and injections
Contraindications to aspiration Contraindications to injection Medications Tests to consider Adverse reactions and complications Techniques
Indications for Arthrocentesis
Crystal-induced arthropathy Hemarthrosis Limiting joint damage from an
infectious process Symptomatic relief of a large
effusion Unexplained joint effusion Unexplained monarthritis

Contraindications for Aspiration Bacteremia Clinician unfamiliar with anatomy of or
approach to the joint Inaccessible joints Joint prosthesis Overlying infection in the soft tissues Severe coagulopathy Severe overlying dermatitis Uncooperative patient
Contraindications for Injections
Adjacent osteomyelitis Bacteremia Hemarthrosis Impending (scheduled within days)
joint replacement surgery Infectious arthritis

Contraindications for Injections
Joint prosthesis Osteochondral fracture Periarticular cellulitis Poorly controlled diabetes mellitus Uncontrolled bleeding disorder or
coagulopathy Failure to improve with prior
injections

Medications Considerations
Duration of effect (related to solubility) Potency of steroid Mineralocorticoid effects
Hydrocortisone acetate (Hydrocortone) Low potency Short 10 to 25 mg for soft tissue and small joints
50 mg for large joints
Medications
Methylprednisolone acetate (Depo-Medrol) or triamcinolone acetonide (Aristocort) Intermediate potency Intermediate duration 2 to 10 mg for soft tissue and small
joints 10 to 80 mg for large joints

Medications
Betamethasone sodium phosphate and acetate (Celestone Soluspan) High potency Long duration 1 to 3 mg for soft tissue and small
joints 2 to 6 mg for large joints

Medications
Dexamethasone sodium phosphate (Decadron) High potency Long duration 0.5 to 3 mg for soft tissue and small
joints 2 to 4 mg for large joints

Steroid AgentsAgent Relative anti-
inflammatory potency
Relative mineralocorticoid potency
Solubility
Hydrocortisone acetate 1 2-3 High
Prednisolone tebutate 4 1 Medium
Methylprednisolone acetate 5 0 Medium
Triamcinolone acetonide Triamcinolone diacetate Triamcinolone hexacetonide
5 0 Medium
Betamethasone sodium phosphate and acetate
20-30 0 Low
Dexamethasone acetate and sodium phosphate
20-30 0 Low

Anesthetic Agents
Use higher concentration smaller volume for small joints
Drug Onset of action Duration of action Maximum volume
Lidocaine HCl
1% 1-2 min ~1 hr 20 mL
2% 1-2 min ~1 hr 10 mL
Bupivacaine HCl
0.25% 30 min 8 hr 60 mL
0.5% 30 min 8 hr 30 mL
Hyaluronic Derivatives Hylan G-F 20 (Synvisc) Systematic review suggests efficacy Cochrane review of 76 trials
40 vs placebo 6 vs NSAIDs 10 vs steroids
Median quality About as good as steroids
Cochrane Library 2006 Issue 2:CD005328
Hyaluronic Costs Euflexxa 20 mg/2 mL $139.20, repeated
weekly for 3 weeks Hyalgan 20 mg/2 mL $138.94, repeated
weekly for 3-5 weeks, also available in 2 mL vials
Orthovisc 30 mg/2 mL $123.90, repeated weekly for 3-4 weeks
Synvisc 16 mg/2 mL $233.08, repeated weekly for 3 weeks
Supartz 25 mg/2.5 mL $120.70, repeated weekly for 3-5 weeks

Steroid Costs Methylprednisolone acetate 20-80 mg
as generic $1.40, Depo-Medrol $1.61 Triamcinolone acetonide (Kenalog)
20-80 mg $1.39 Triamcinolone diacetate (Aristocort
Forte) 20-80 mg $1.44 Triamcinolone hexacetonide
(Aristospan Intra-articular) 20-80 mg $1.26
The Medical Letter 2006 Mar 27;48(1231):25

Tests to Consider If there is warmth, painful effusion,
marked pain with range of motion, exquisite tenderness consider infections Blood work- ESR, glucose, protein Joint Fluid
Cell count and differential Glucose and protein Cultures Gram stain Crystal analysis
Complications
Caused by injection Bleeding (rare) Infection (1 in 10,000) Joint injury (incidence unknown):
Avoid by aspirating slowly and not moving needle side to side in joint
Complications Caused by corticosteroid agent
Acceleration of septic joint Subcutaneous fat atrophy (<1%),
particularly if injection is <5 mm beneath skin surface
Fistulous tract formation Steroid flare with pain 6 to 12 hr after
injection (2% to 5%) Exacerbation of diabetes (rare) Osteoporosis (high doses over long period) Cartilage damage, particularly in weight-
bearing joints
Complications Caused by corticosteroid agents
Tendon rupture (<1%) Facial flushing (<1%) Transient paresis of injected extremity (rare) Asymptomatic pericapsular calcification (43%) Adverse gastrointestinal effects Mood alterations Fluid retention Menstrual irregularities Allergic or hypersensitivity reactions

Techniques Knee
Lateral mid patella approach preferred Most likely to hit
the joint Study of 80
patients injected 3 separate times by same physician
Knee ExtendedJ Bone Joint Surg Am 2002 Sep;84-A(9):1522

Techniques Knee Need the following
Large syringe for aspiration
Second syringe with medications
Up to 10 ml total volume
22 gauge needle 1.5 inches long
Alcohol wipes Betadine wipes Bandage

Techniques Ankle Foot
Techniques Ankle I
Medication total volume should not exceed about 7 ml
Palpate the junction of the fibula and the tibia just superior to the talus
Palpate this soft triangular space Advance needle into space If bone encountered redirect medial
and superiorly
Techniques Ankle II
The space between anterior border of the medial malleolus
The medial border of the tibialis anterior tendon
Palpates this space for the articulation of the talus and tibia.
Direct the needle postero-laterally

Techniques Ankle Foot

Techniques Tarsal Tunnel
Caused by compression of posterior tibial nerve
Tunnel is formed by medial malleolus and fibrous flexor retinaculum
Chief complaint is burning sensation over the medial 1/3 of the foot
Look for Tinel’s sign

Techniques Tarsal Tunnel Medication volume should not
exceed 3 ml Needle is inserted 2 cm proximal
to the identified location Angle is 30 degrees to the foot Tunnel is very superficial Aspirate prior to injection to make
sure not in a vessel

Techniques Tarsal Tunnel
Patient in lateral position with affected foot on bed
Find positive Tinel’s sign Identify the posterior tibial tendon Patient inverts foot against
resistant Nerve lies behind the tendon
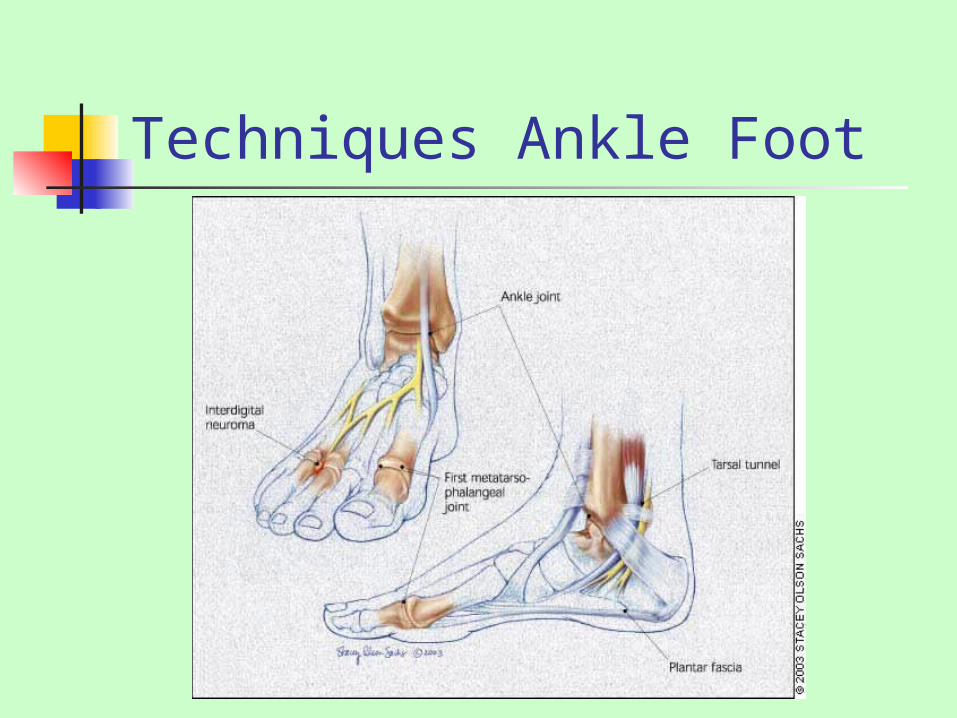
Techniques Ankle Foot

Techniques 1st MTP Joint Total volume should not exceed 2
ml Roughly 1 ml Lidocaine Roughly 0.25-0.5 ml Celestone
May be difficult to palpate this joint Distraction helps open the joint Insert from medial approach Angle 60-70 degrees to conform to
joint angles
General References
Zuber TJ. Knee join aspiration and injection. American Family Physician 2002 Oct 15;66(8):1497-500, 1503-4, 1507
Rifat SF, Moeller JL. Basics of joint injection: general techniques and tips for safe, effective use. Postgraduate Medicine 2001;109(1):157-166
Rifat SF, Moeller JL. Site-specific techniques of joint injection: useful additions to your treatment repertoire. Postgraduate Medicine 2001;109(3):123-36