low cardiac output syndrome in children
TRANSCRIPT
ARTICLE IN PRESS
Current Anaesthesia & Critical Care (2005) 16, 347–358
0953-7112/$ - sdoi:10.1016/j.c
�Correspondifax: +61 7 3212
E-mail addr
www.elsevier.com/locate/cacc
FOCUS ON: CARDIOVASCULAR
Low cardiac output syndrome in children
Bryn Jones, Mark Hayden�, John F. Fraser, E Janes
Critical Care Research Group and Queensland Paediatric Intensive Care Service,The Prince Charles Hospital, Rode Road, Chermside, Queensland 4032, Australia
KEYWORDSPaediatric;Cardiac surgery;Low cardiac output;Peri-operative com-plications
ee front matter & 2006acc.2006.02.011
ng author. Tel.: +61 7 35575.ess: Mark_Hayden@heal
Summary Clinicians caring for critically ill children will commonly encounter lowcardiac output states, especially after cardiac surgery. Anticipation and preventioncan go some way to reducing morbidity and mortality. This article outlines the causesand assessment of this syndrome. Management strategies are discussed aimed atimproving cardiac output by optimisation of left- and right-ventricle preload andafterload. Pharmacological strategies utilising well-established as well as new agentsare outlined. Non-pharmacological strategies are presented, as well as methods ofreducing the adverse effects of low cardiac output on the child.& 2006 Published by Elsevier Ltd.
Introduction
Low cardiac output syndrome (LCOS) is a clinicalsyndrome seen commonly (25%) after paediatriccardiac surgery, but also occurring secondary toacute myocarditis and septic shock. Regardless ofaetiology, the clinical effects of the resultingshock, namely inadequate organ perfusion, areconstant, and result in organ dysfunction. Wereview current strategies for prevention and treat-ment of LCOS in the paediatric population.
Causes and prevention
Numerous factors lead to myocardial dysfunctionpostoperatively1 (Table 1). Postoperative increases insystemic and pulmonary vascular resistance coincidewith the dysfunction, further reducing cardiac output.
Published by Elsevier Ltd.
350 8111;
th.qld.gov.au (M. Hayden).
This occurs typically 6–18h after cardiopulmonarybypass, which is usually in the middle of the night!
As the pathogenesis is multifactorial, techniquesaimed at reducing the inflammatory effects ofcardiopulmonary bypass are often combined. Pre-operative steroids and intraoperative ultrafiltrationare widely used. Modified ultrafiltration (MUF)reduces total body water, postoperative blood loss,and the duration of mechanical ventilation.2 It mayalso remove inflammatory mediators from thecirculation. Many centres routinely use MUF inneonatal cases. Surgical technique also affects thelikelihood of LCOS with prolonged bypass and cross-clamp times and extensive myomectomies delayingrecovery.3 Advances in surgical techniques, such asthe Sano modification of the Norwood procedure canalso improve postoperative haemodynamic status.4
Assessment
Anticipation is the key to the diagnosis andmanagement of LCOS. While LCOS is fundamentally

ARTICLE IN PRESS
Table 1
Causes of postoperative LCOS
Inflammatory cascade triggered bycardiopulmonary bypass (CPB)—complementactivation, endotoxin release, leukocyteactivation, release of inflammatory mediatorsAortic cross-clamp leading to myocardial ischaemiaHypothermiaReperfusion injuryPericardial tamponade
B. Jones et al.348
a clinical diagnosis there are useful direct andindirect methods of assessment.
Clinical
The classical features of LCOS are tachycardia,oliguria (o0.5ml/kg/h), poor peripheral perfusionand low blood pressure. Peripheral perfusion isassessed using the capillary refill time and core–
peripheral temperature difference. Their value isquestionable in the context of fever and the use ofvasoactive medications, and they have been shownto correlate poorly with measured markers ofpostoperative cardiac output.5 Oliguria may bedue to fluid restriction, renal dysfunction and SIADHso cannot be assumed to reflect LCOS. LCOS can bepresent with a normal or high blood pressure. Sinustachycardia not due to fever, seizures or pain isprobably the most useful clinical sign. The ability ofclinicians to assess cardiac output from clinicalexamination alone is poor.6
Investigation
Metabolic acidosisMetabolic acidosis as assessed by base deficit maybe misleading due to factors such as hyperchlor-aemia from pump priming solutions. True tissueacidosis is better assessed either by the anion gapcorrected for albumin concentration, or the strongion difference.7 While requiring a spreadsheet tocalculate easily, an elevated strong ion differencehas recently been shown to predict poor outcomepostoperatively better than lactate measure-ments.8
LactateBlood lactate levels correlate with the degree ofanaerobic metabolism,9 representing inadequateoxygen delivery or impaired peripheral utilization.Serial measurements in neonates are a more
reliable prognosticator for poor outcome followingcardiac surgery than a single measurement. Thepositive predictive value (PPV) for death or extra-corporeal membrane oxygenation (ECMO) of alactate 46mmol/l was 38% versus a PPV of 100%for a lactate rising at 40.75mmol/l/h.10 Treat-ment algorithms based on serial measurements mayimprove outcome, particularly in high-risk pa-tients.11 Intraoperative factors such as bloodpriming12 and the ability of the patient to clearthe lactate (e.g. hepatic failure), may affectpostoperative levels. High or rising lactates are auseful marker for LCOS.
Mixed venous oxygen saturationA fall in cardiac output or an increase in oxygenconsumption can result in a fall in the mixed venousoxygen saturation.13 This may occur prior to a risein blood lactate levels. The optimal sites of mixedvenous oxygen saturation measurement are in thepulmonary arteries or the right ventricle. Measure-ments taken in the SVC/ IVC or RA may not beaccurate. For the purpose of following trendshowever, these inaccuracies may not be clinicallyrelevant. Continuous measurement of mixed ve-nous saturation, via placement of a co-oximeter inthe SVC following stage 1 Norwood palliation,14 hasbeen used to direct management with the aim ofSvO2450%. In an acyanotic child SvO2470% wouldbe an acceptable goal. Intermittent sampling doesnot require specialist catheters (which are notcurrently available yet although a suitable paedia-tric catheter is under development).
EchocardiographyEchocardiography (echo) is a valuable tool to assessboth structure and function. Systolic and diastolicfunction can be assessed and cardiac outputestimated. Unlike other methods echo can definecontributory causes of LCOS including; pericardialeffusion, residual structural lesions, regional wallmotion abnormalities, atrial and ventricular dilata-tion, valvular stenosis and regurgitation.
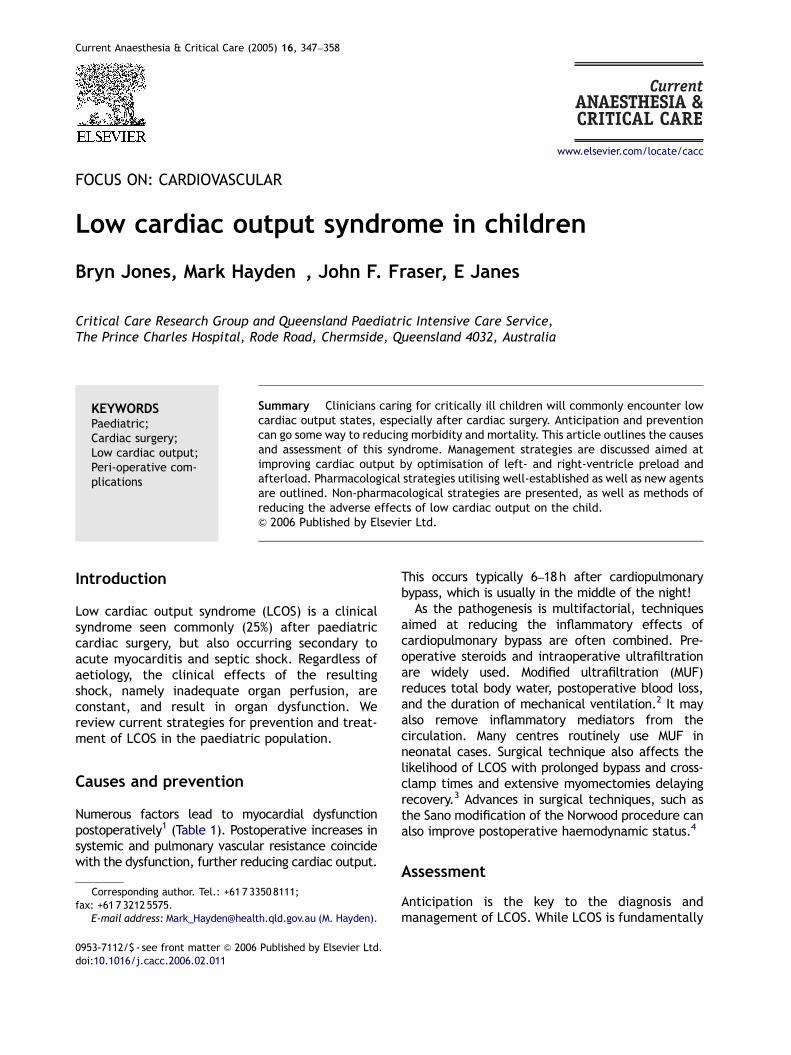
Reduced systolic function in paediatrics is usuallydefined by an left ventricular (LV) shorteningfraction of o30% but can be inaccurate, particu-larly if there are regional wall abnormalities ratherthan global dysfunction. Diastolic dysfunction isharder to quantify on echocardiography. Diastolicdysfunction in either ventricle can be assessed byexamining early (E) and late (A) ventricular fillingpatterns as early filling relates to active relaxation(Fig. 1). Complicating assessment of diastolicdysfunction in children are the maturation changesin the pattern of E and A wave ratios and pulmonaryvein flows with infants having a reversal of the
ARTICLE IN PRESS
Figure 1 Diastolic dysfunction: (A) Normal transmitral flow in a patient in sinus rhythm. (B) Impaired relaxation withnormal filling pressures.70
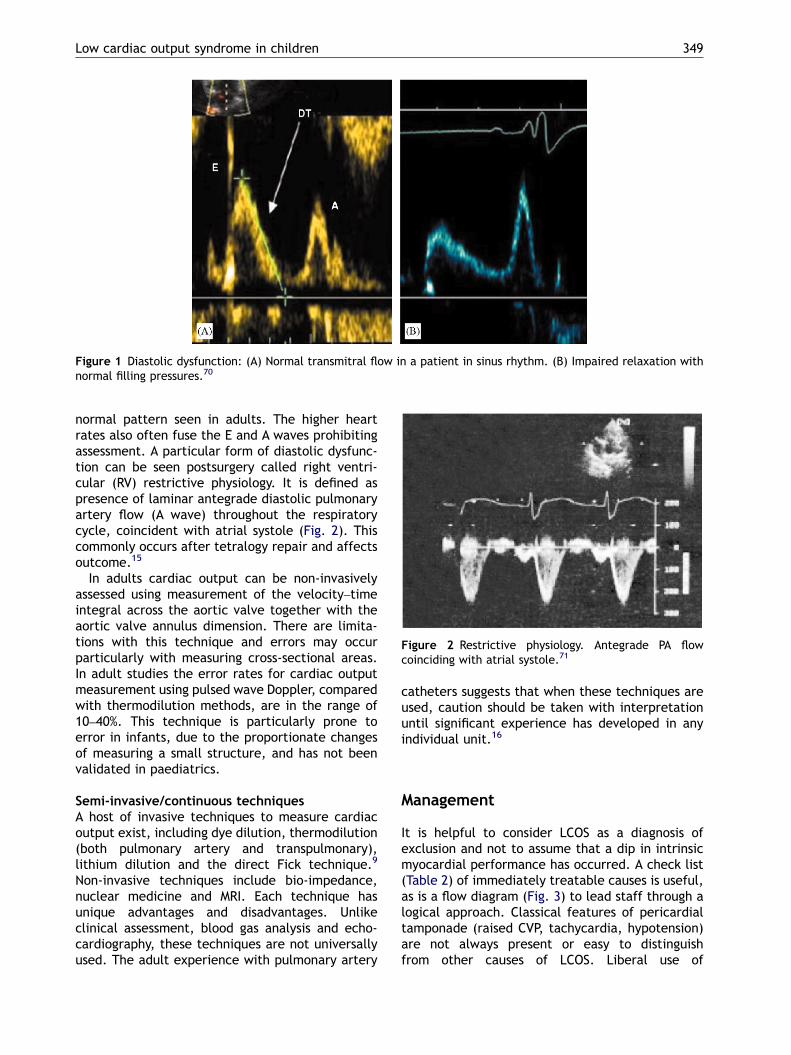
Figure 2 Restrictive physiology. Antegrade PA flowcoinciding with atrial systole.71
Low cardiac output syndrome in children 349
normal pattern seen in adults. The higher heartrates also often fuse the E and A waves prohibitingassessment. A particular form of diastolic dysfunc-tion can be seen postsurgery called right ventri-cular (RV) restrictive physiology. It is defined aspresence of laminar antegrade diastolic pulmonaryartery flow (A wave) throughout the respiratorycycle, coincident with atrial systole (Fig. 2). Thiscommonly occurs after tetralogy repair and affectsoutcome.15
In adults cardiac output can be non-invasivelyassessed using measurement of the velocity–timeintegral across the aortic valve together with theaortic valve annulus dimension. There are limita-tions with this technique and errors may occurparticularly with measuring cross-sectional areas.In adult studies the error rates for cardiac outputmeasurement using pulsed wave Doppler, comparedwith thermodilution methods, are in the range of10–40%. This technique is particularly prone toerror in infants, due to the proportionate changesof measuring a small structure, and has not beenvalidated in paediatrics.
Semi-invasive/continuous techniquesA host of invasive techniques to measure cardiacoutput exist, including dye dilution, thermodilution(both pulmonary artery and transpulmonary),lithium dilution and the direct Fick technique.9
Non-invasive techniques include bio-impedance,nuclear medicine and MRI. Each technique hasunique advantages and disadvantages. Unlikeclinical assessment, blood gas analysis and echo-cardiography, these techniques are not universallyused. The adult experience with pulmonary artery
catheters suggests that when these techniques areused, caution should be taken with interpretationuntil significant experience has developed in anyindividual unit.16
Management
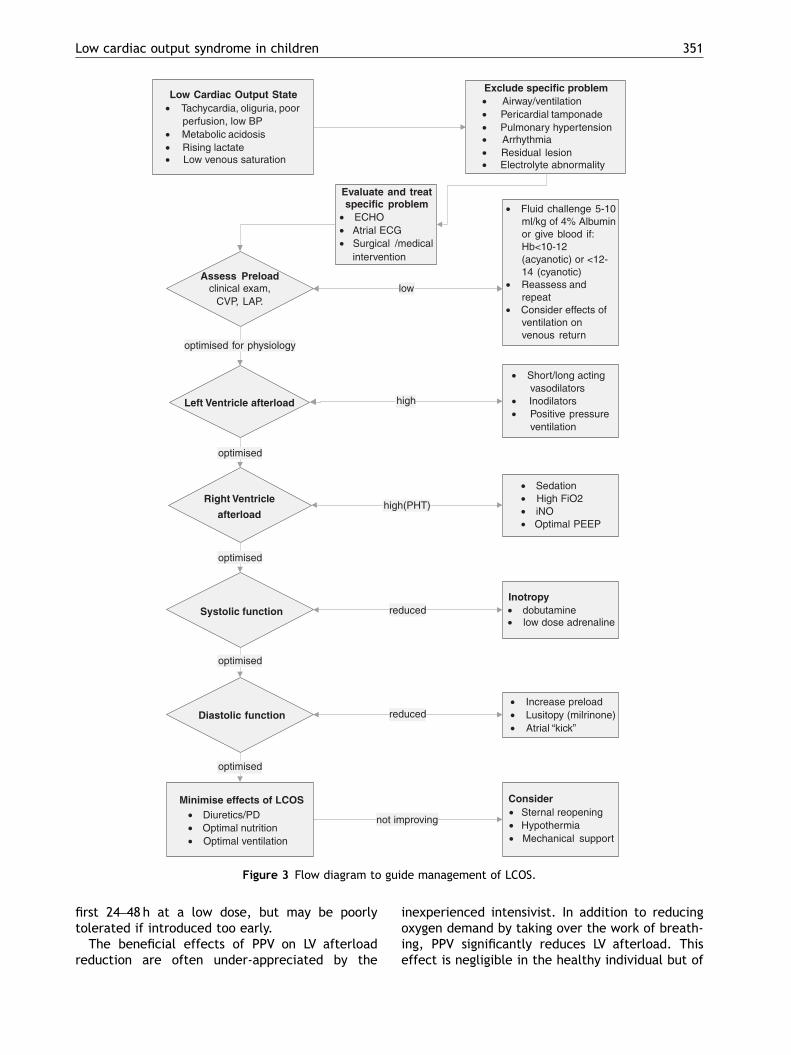
It is helpful to consider LCOS as a diagnosis ofexclusion and not to assume that a dip in intrinsicmyocardial performance has occurred. A check list(Table 2) of immediately treatable causes is useful,as is a flow diagram (Fig. 3) to lead staff through alogical approach. Classical features of pericardialtamponade (raised CVP, tachycardia, hypotension)are not always present or easy to distinguishfrom other causes of LCOS. Liberal use of

ARTICLE IN PRESS
Table 2
Check list of causes of postoperative LCOS to exclude
Adequate airway (tube position, size and patency) and ventilation (atelectasis, pneumothorax)Pericardial tamponadePulmonary hypertensive crisisArrhythmias (loss of AV synchrony, tachycardia or bradycardia)Significant residual lesion (e.g. residual VSD post-Fallot repair, AV regurgitation post-AVSD repair)Electrolyte abnormality (e.g. hypocalcaemia)
B. Jones et al.350
echocardiography allows confident exclusion ofcollections but ‘‘dry tamponade’’ can occur (seesection on Delayed Sternal Closure).
Preload
Preload is traditionally assessed by measuring fillingpressures from right and left atrial lines. Auto-transfusion by hepatic pressure may give usefulinformation as to the likely effects of a volume loadon filling pressures, heart rate and blood pressure.Variations in pulse pressure and systolic pressurewith mechanical ventilation (systolic swing on thearterial line) imply relative hypovolaemia and likelyfluid responsiveness. Absolute values of right andleft atrial pressure need to be assessed in thecontext of the surgical procedure. Following aFallot’s repair a child may well require a high rightatrial filling pressure (12–18mmHg) due to poorventricular compliance or loss of atrial ‘‘kick’’secondary to junctional ectopic tachycardia (JET).Equally, it may be unwise to overfill a postoperativearterial switch procedure patient, as over disten-sion of the heart may distort coronary anatomy. Ingeneral, administering small aliquots (5–10ml/kg)of fluid by hand, while observing the patient andtheir cardiovascular response, is better than pre-scribing infusions over longer periods.
In addition to absolute intravascular volume,venous capacitance also affects venous return.Venodilatation often occurs on rewarming andmay be exacerbated by drugs such as glyceryltrinitrate (GTN).
In the setting of the Fontan repair, systemic (left)ventricular preload may be inadequate due to poorflow in the pulmonary circuit. In these circum-stances a fenestration allowing desaturated bloodto bypass the lungs (right to left shunt) may bebeneficial to systemic ventricular filling,17 albeit atthe expense of the systemic saturation. Similarly,leaving an atrial connection in a Fallot’s repair may
allow the right side of the heart to ‘‘blow off’’ andimprove LV preload.
Finally, positive pressure ventilation (PPV) willtend to reduce RV preload by inhibiting venousreturn. Therefore, early extubation may be bene-ficial for situations where right-sided preload iscrucial such as the Fontan circuit. In situationswhere extubation is not feasible, negative pressureventilation has been used to improve venousreturn.18
Left ventricular afterload
Reduction in LV afterload will improve cardiacoutput, as long as an adequate diastolic pressureis maintained for coronary perfusion. This maybe achieved with long- or short-acting vasodi-lators, inodilators (discussed in inotropy section)or PPV.
Short-acting vasodilators are commonly used asthey may be rapidly adjusted in response tochanges in the clinical condition. GTN has asignificant venodilatory effect and will tend toreduce preload as well as afterload, in the doserange of 1–10mcg/kg/min. Sodium nitroprusside ismore effective at reducing afterload, but has thecomplication of cyanide toxicity when used athigher doses for prolonged periods.
Phenoxybenzamine and captopril are commonlyused longer-acting dilators. Phenoxybenzamine isan irreversible blocker of a1 and a2 adrenoceptors,which results in a reduction of peripheral vascularresistance. It is usually well tolerated especially ifstarted ‘‘on pump’’, and ensures a stable dilatedsystemic circulation, preventing acute fluctuations.In postoperative patients with a univentricularcirculation, phenoxybenzamine helps ‘‘balance’’the circulation and improves systemic oxygendelivery.19 Some centres routinely use phenoxy-benzamine postarterial switch procedure to pre-vent acute rises in afterload. Captopril is anexcellent agent that is often introduced after the
ARTICLE IN PRESS
Low Cardiac Output State• Tachycardia, oliguria, poor
perfusion, low BP• Metabolic acidosis• Rising lactate• Low venous saturation
Assess Preloadclinical exam,
CVP, LAP.
• Fluid challenge 5-10 ml/kg of 4% Albuminor give blood if:Hb<10-12(acyanotic) or <12-14 (cyanotic)
• Reassess andrepeat
• Consider effects of ventilation onvenous return
low
Left Ventricle afterload
• Short/long actingvasodilators
• Inodilators• Positive pressure
ventilation
optimised for physiology
high
Right Ventricle
afterload
optimised
• Sedation• High FiO2• iNO• Optimal PEEP
high(PHT)
optimised
Inotropy• dobutamine• low dose adrenaline
reduced
Consider• Sternal reopening• Hypothermia• Mechanical support
Exclude specific problem• Airway/ventilation• Pericardial tamponade• Pulmonary hypertension• Arrhythmia• Residual lesion• Electrolyte abnormality
Evaluate and treatspecific problem
• ECHO• Atrial ECG• Surgical /medical
intervention
Diastolic function
not improving
Systolic function
optimised
• Increase preload• Lusitopy (milrinone)• Atrial “kick”
reduced
Minimise effects of LCOS• Diuretics/PD• Optimal nutrition• Optimal ventilation
optimised
Figure 3 Flow diagram to guide management of LCOS.
Low cardiac output syndrome in children 351
first 24–48 h at a low dose, but may be poorlytolerated if introduced too early.
The beneficial effects of PPV on LV afterloadreduction are often under-appreciated by the
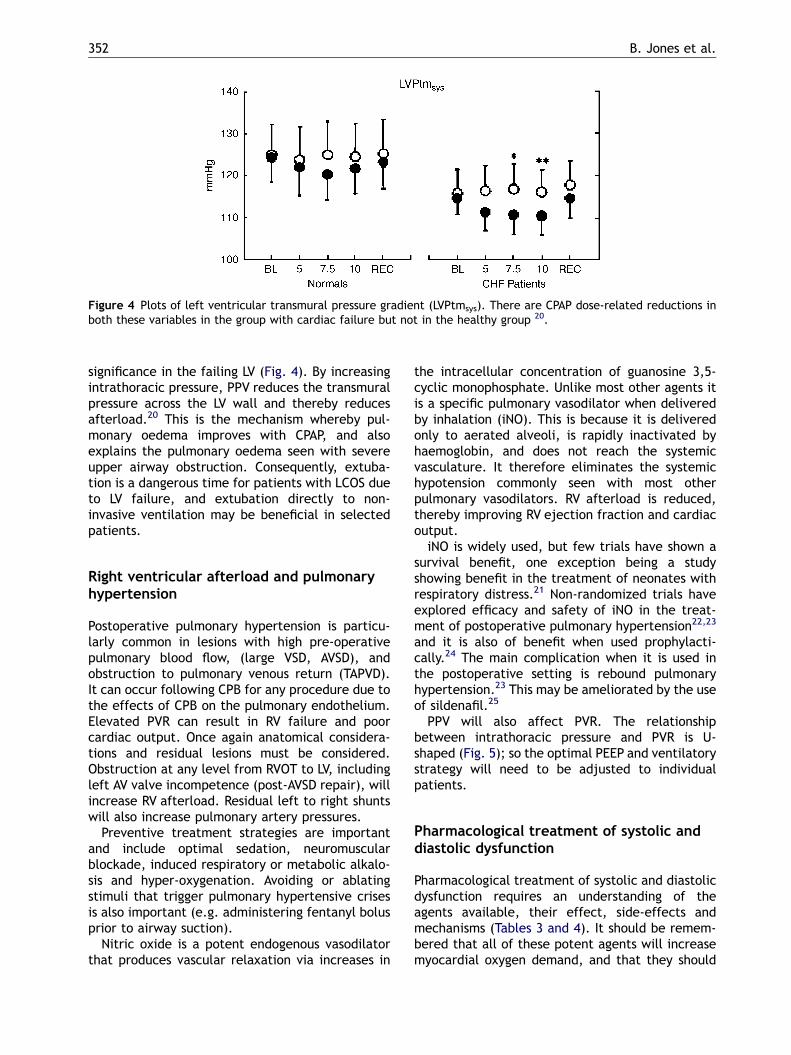
inexperienced intensivist. In addition to reducingoxygen demand by taking over the work of breath-ing, PPV significantly reduces LV afterload. Thiseffect is negligible in the healthy individual but of
ARTICLE IN PRESS
Figure 4 Plots of left ventricular transmural pressure gradient (LVPtmsys). There are CPAP dose-related reductions inboth these variables in the group with cardiac failure but not in the healthy group 20.
B. Jones et al.352
significance in the failing LV (Fig. 4). By increasingintrathoracic pressure, PPV reduces the transmuralpressure across the LV wall and thereby reducesafterload.20 This is the mechanism whereby pul-monary oedema improves with CPAP, and alsoexplains the pulmonary oedema seen with severeupper airway obstruction. Consequently, extuba-tion is a dangerous time for patients with LCOS dueto LV failure, and extubation directly to non-invasive ventilation may be beneficial in selectedpatients.
Right ventricular afterload and pulmonaryhypertension
Postoperative pulmonary hypertension is particu-larly common in lesions with high pre-operativepulmonary blood flow, (large VSD, AVSD), andobstruction to pulmonary venous return (TAPVD).It can occur following CPB for any procedure due tothe effects of CPB on the pulmonary endothelium.Elevated PVR can result in RV failure and poorcardiac output. Once again anatomical considera-tions and residual lesions must be considered.Obstruction at any level from RVOT to LV, includingleft AV valve incompetence (post-AVSD repair), willincrease RV afterload. Residual left to right shuntswill also increase pulmonary artery pressures.
Preventive treatment strategies are importantand include optimal sedation, neuromuscularblockade, induced respiratory or metabolic alkalo-sis and hyper-oxygenation. Avoiding or ablatingstimuli that trigger pulmonary hypertensive crisesis also important (e.g. administering fentanyl bolusprior to airway suction).
Nitric oxide is a potent endogenous vasodilatorthat produces vascular relaxation via increases in
the intracellular concentration of guanosine 3,5-cyclic monophosphate. Unlike most other agents itis a specific pulmonary vasodilator when deliveredby inhalation (iNO). This is because it is deliveredonly to aerated alveoli, is rapidly inactivated byhaemoglobin, and does not reach the systemicvasculature. It therefore eliminates the systemichypotension commonly seen with most otherpulmonary vasodilators. RV afterload is reduced,thereby improving RV ejection fraction and cardiacoutput.
iNO is widely used, but few trials have shown asurvival benefit, one exception being a studyshowing benefit in the treatment of neonates withrespiratory distress.21 Non-randomized trials haveexplored efficacy and safety of iNO in the treat-ment of postoperative pulmonary hypertension22,23
and it is also of benefit when used prophylacti-cally.24 The main complication when it is used inthe postoperative setting is rebound pulmonaryhypertension.23 This may be ameliorated by the useof sildenafil.25
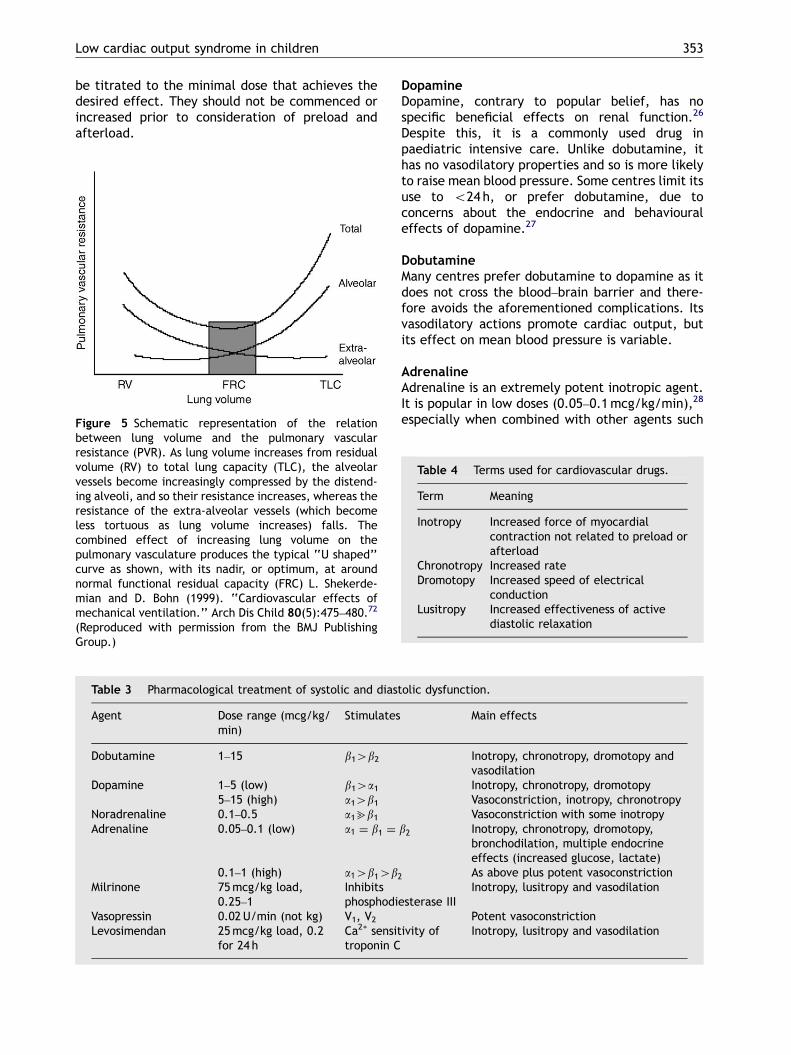
PPV will also affect PVR. The relationshipbetween intrathoracic pressure and PVR is U-shaped (Fig. 5); so the optimal PEEP and ventilatorystrategy will need to be adjusted to individualpatients.
Pharmacological treatment of systolic anddiastolic dysfunction
Pharmacological treatment of systolic and diastolicdysfunction requires an understanding of theagents available, their effect, side-effects andmechanisms (Tables 3 and 4). It should be remem-bered that all of these potent agents will increasemyocardial oxygen demand, and that they should
ARTICLE IN PRESS
Low cardiac output syndrome in children 353
be titrated to the minimal dose that achieves thedesired effect. They should not be commenced orincreased prior to consideration of preload andafterload.
Figure 5 Schematic representation of the relationbetween lung volume and the pulmonary vascularresistance (PVR). As lung volume increases from residualvolume (RV) to total lung capacity (TLC), the alveolarvessels become increasingly compressed by the distend-ing alveoli, and so their resistance increases, whereas theresistance of the extra-alveolar vessels (which becomeless tortuous as lung volume increases) falls. Thecombined effect of increasing lung volume on thepulmonary vasculature produces the typical ‘‘U shaped’’curve as shown, with its nadir, or optimum, at aroundnormal functional residual capacity (FRC) L. Shekerde-mian and D. Bohn (1999). ‘‘Cardiovascular effects ofmechanical ventilation.’’ Arch Dis Child 80(5):475–480.72
(Reproduced with permission from the BMJ PublishingGroup.)
Table 3 Pharmacological treatment of systolic and diast
Agent Dose range (mcg/kg/min)
Stimulates
Dobutamine 1–15 b14b2
Dopamine 1–5 (low) b14a15–15 (high) a14b1
Noradrenaline 0.1–0.5 a1bb1Adrenaline 0.05–0.1 (low) a1 ¼ b1 ¼
0.1–1 (high) a14b14b2Milrinone 75mcg/kg load,
0.25–1Inhibitsphosphodi
Vasopressin 0.02U/min (not kg) V1, V2Levosimendan 25mcg/kg load, 0.2
for 24 hCa2+ sensittroponin C
DopamineDopamine, contrary to popular belief, has nospecific beneficial effects on renal function.26
Despite this, it is a commonly used drug inpaediatric intensive care. Unlike dobutamine, ithas no vasodilatory properties and so is more likelyto raise mean blood pressure. Some centres limit itsuse to o24 h, or prefer dobutamine, due toconcerns about the endocrine and behaviouraleffects of dopamine.27
DobutamineMany centres prefer dobutamine to dopamine as itdoes not cross the blood–brain barrier and there-fore avoids the aforementioned complications. Itsvasodilatory actions promote cardiac output, butits effect on mean blood pressure is variable.
AdrenalineAdrenaline is an extremely potent inotropic agent.It is popular in low doses (0.05–0.1mcg/kg/min),28
especially when combined with other agents such
olic dysfunction.
Main effects
Inotropy, chronotropy, dromotopy andvasodilationInotropy, chronotropy, dromotopyVasoconstriction, inotropy, chronotropyVasoconstriction with some inotropy
b2 Inotropy, chronotropy, dromotopy,bronchodilation, multiple endocrineeffects (increased glucose, lactate)As above plus potent vasoconstriction
esterase IIIInotropy, lusitropy and vasodilation
Potent vasoconstrictionivity of Inotropy, lusitropy and vasodilation
Table 4 Terms used for cardiovascular drugs.
Term Meaning
Inotropy Increased force of myocardialcontraction not related to preload orafterload
Chronotropy Increased rateDromotopy Increased speed of electrical
conductionLusitropy Increased effectiveness of active
diastolic relaxation

ARTICLE IN PRESS
26.7
17.7
9.6
0
5
10
15
20
25
30
placebo (n=75) low dose (n=79) high dose (n=73)
% p
ts
RRR=34%p=.183
RRR=64%p=.007
Figure 6 PRIMACORP study of prophylactic milrinone 33.Primary end-point: development of LCOS/death in thefirst 36 h. RRR ¼ relative risk reduction.
B. Jones et al.354
as milrinone. At higher doses it remains a usefuldrug but adverse effects are frequent, particularlyeffects on hypokalaemia, hyperglycaemia andraised lactate. The resultant lactic acidosis canfurther compromise the failing heart. Indeed it isoften hard to decide if the rising lactate in apatient on a high-dose adrenaline infusion isbecause of, or despite, the adrenaline.
NoradrenalineNoradrenaline should be used with caution in thesetting of LCOS. At doses of 40.1mcg/kg/min itsmain effect is vasoconstriction. While beneficial formean blood pressure, this may be at the expense ofcardiac output. Noradrenaline is useful in the settingof very low diastolic pressures due to excessive long-acting vasodilators or sepsis. Similarly, Vasopressinmay be used in situations of excessive a1 blockade,but should be used with caution.
MilrinoneMilrinone acts by inhibition of phosphodiesterasetype 3, increasing intracellular levels of cyclic AMPand leading to increased intracellular calcium andmyocardial contractility. As it does not rely onadrenergic receptors, it is particularly useful whenthese receptors have become downregulated29
through prolonged catecholamine use, althoughanimal data suggest that milrinone’s efficacy willalso be reduced.30 Peripheral vasodilatation ac-companies increased contractility, hence the terminodilator. Its effects on calcium re-uptake improveventricular relaxation during diastole (lusitropy),thereby reducing diastolic dysfunction. This is ofparticular help in the setting of a postoperativeFallot’s repair where the hypertrophied rightventricle has suffered a significant surgical insultand may be very stiff and non-compliant. The useof milrinone in acute heart failure in adults iscontroversial with many advocating avoidance.31,32
The situation is significantly different in paedia-trics, perhaps due to the absence of ischaemia as amajor pathology, and milrinone is a popular agent.Much of this popularity follows the PRIMACORPstudy33 which randomized 238 infants followingrelatively high risk (biventricular repair) surgery.They used LCOS or death as their primaryend-point, and compared placebo with high-(0.75mcg/kg/min) or low-dose (0.25mcg/kg/min)milrinone. They found a 64% relative risk reduction(95%CI: 21–84%) in LCOS with the high dose, withthe number needed to treat to avoid developingLCOS in one patient being six (95% CI, 3–20)(Fig. 6).Whilst administration of the loading dose withmilrinone can lead to a significant reduction inmean blood pressure, often requiring volume
loading this can be minimized by loading ‘‘onpump’’, or omitting the loading dose but runninga higher infusion rate (1mcg/kg/min) for 24 h.While the PRIMACORP study was imperfect, thereare few other randomized controlled trials ofsimilar weight on the management of LCOS.
LevosimendanLevosimendan is one of a new class of inodilators/calcium sensitizers.34 Levosimendan binds to tro-ponin C with high affinity. It does not increase theCa2+ binding affinity of cardiac troponin C butstabilizes the conformation of Ca2+–troponin Ccomplex.35 In addition, Levosimendan is a selectivephosphodiesterase III inhibitor. Levosimendan mayact preferentially as a Ca2+ sensitizer at lowerconcentrations, whereas at higher concentrations itacts as a phosphodiesterase III inhibitor. Levosi-mendan generates more energy-efficient myocar-dial contractility than achieved via catecholaminestimulation or phosphodiesterase inhibition.35 Le-vosimendan additionally induces vasodilatationthrough activation of ATP-dependant potassiumchannels, reducing afterload and promoting cor-onary artery vasodilatation. The advantages areless risk of intracellular calcium overload that couldpotentially result in arrhythmias and cell death aswell as improving lusitropy. Adult studies havedemonstrated positive haemodynamic effects inpatients with decompensated heart failure. TheLIDO study36 compared Levosimendan with dobuta-mine and placebo in adult patients with severelow-output cardiac failure. In this multicentre,randomized, double-blinded study, the investiga-tors demonstrated a significantly greater haemo-dynamic improvement (430% increase in cardiacoutput, or425% reduction in left atrial pressure) inpatients with a 24 h infusion of Levosimendan thanwith dobutamine. Remarkably although the studywas not designed to detect a mortality effect, only

ARTICLE IN PRESS
Low cardiac output syndrome in children 355
eight (8%) of 103 patients in the Levosimendangroup died within 31 days compared with 17 (17%)of 100 assigned dobutamine (hazard ratio 0.43 [95%CI 0.18–1.00]; P ¼ 0.049). There is evidence thatthe pharmacokinetic profile in children with con-genital heart disease is different from that in adultswith congestive heart failure and the dose shouldbe based on surface area.37 The use of thispromising agent in paediatrics is increasing butremains largely anecdotal.38,39
Thyroid hormoneThyroid hormone has an essential role in cellularmetabolism and in maintaining haemodynamic stabi-lity. It is required for the synthesis of contractileproteins and to maintain normal myocardial contrac-tion. Suppression of thyroid hormone levels has beendemonstrated in children following CPB, maximalbetween 12 and 48h and lasting up to 7 days afterCPB.40,41 Theoretically supplementing with T3 mightimprove cardiac output particularly in LCOS. Thereare possible harmful effects however and T3 supple-mentation may delay return to a euthyroid state ininfants.40 Adult studies have demonstrated dose-dependant increases in cardiac output when given tri-iodothyronine supplementation.42 A small (n ¼ 40)randomized controlled trial in children treated withtriiodothyronine after CPB demonstrated improvedmyocardial function43 but the results are difficult tointerpret. A systematic review of thyroid hormonesupplementation in infants, which excluded theaforementioned trial, concluded that there was lackof evidence to demonstrate benefit.44
NesiritideB-type natriuretic peptide is synthesized andexcreted from the ventricular myocardium inresponse to myocardial stretch. Nesiritide is arecombinant 32-amino acid B-type peptide that isidentical to the endogenous peptide. It results innatriuresis, diuresis and vascular smooth musclerelaxation. Clinically it is said to augment preloadand reduce afterload.45 Benefit has been demon-strated in adults with congestive heart failure.46 Todate only an open-label trial has been reported inchildren47 where niseritide did result in a signifi-cant improvement in fluid balance and urine outputwith an acceptable side-effect profile.
Non-pharmacological treatment of systolicand diastolic dysfunction
Delayed sternal closureDelayed sternal closure is an accepted practice inpaediatric patients with, or expected to have,
significant LCOS. Indications for delayed sternalclosure include post-Stage I Norwood procedure,ECMO, haemodynamic instability and persistentbleeding.48 The aim is to allow the heart to recover,and become less oedematous without the addedproblem of ‘‘dry’’ tamponade. While some unitsembrace delayed closure enthusiastically,48 othersonly use it in selected patients even after theNorwood procedure.4 Delayed closure is associatedwith an increased risk of mediastinitis (particularlywith gram negative organisms) in some units,49 andthyroid suppression from iodine absorption fromiodine-based antiseptics.50 When the sternum isclosed, significant haemodynamic and respiratorychanges51 can occur and should be anticipated.
Induced hypothermiaIntraoperative hypothermia is used routinely incardiac surgery to provide myocardial protection.In the postoperative patient with LCOS there mayalso be some benefit from hypothermia. Reducingthe body temperature results in a reduction inmetabolic rate,52 oxygen demand and heart rate,and may have a direct beneficial effect on cardiacfunction.53 SVR is increased and stroke volume andMAP are maintained. There is some evidence ofbenefit in the treatment of intractable heart failureunresponsive to conventional therapy, with animprovement in cardiac output seen with coolingto 32–33 1C.53,54 While a useful rescue strategy,hypothermia is not without risks, includingsepsis, coagulation disorders and altered pharma-cokinetics. Neuromuscular paralysis is usually re-quired to prevent shivering which, if unopposed,will increase oxygen consumption and lactateproduction.
Mechanical supportIn refractory cases of LCOS, mechanical extracor-poreal life support (ECLS) may be initiated. Themajor benefit of mechanical circulatory support inthe treatment of LCOS is allowing time formyocardial recovery whilst preventing ongoingdamage to other organ systems. Its use impliesthat cardiac dysfunction is potentially reversible.Choice of type of support will vary due toavailability, experience and the patient’s respira-tory status. Veno-arterial (VA) ECMO, and LV and/orRV assist devices are the two commonest methodsof mechanical support. Selection and assessment ofcandidates for ECLS is extremely important. Care-ful evaluation of the surgical repair is paramount,looking particularly for residual defects as they maybe responsible for subsequent haemodynamic com-promise.55 Bleeding is the most common complica-tion, particularly from the wound, but intracranial

ARTICLE IN PRESS
B. Jones et al.356
haemorrhage can occur usually resulting in with-drawal of therapy. Survival to hospital dischargehas remained between 40% and 55% in most seriesand ECLS registry reports.56 ECLS as a bridge totransplant in LCOS secondary to non-surgical insultshas recently been described with promising re-sults.57,58 ECLS is the subject of several excellentreviews.59,60
Pacing and arrhythmia managementArrhythmias that result in loss of AV synchrony, orsignificantly affect heart rate, are common(425%)61 and poorly tolerated in the setting ofLCOS. Tachycardia can allow inadequate time forventricular filling, especially with a poorly compli-ant ventricle; bradycardia is also poorly tolerated,particularly in neonates post-ASO. Bradycardia isusually easy to overcome, often with atrial pacingalone. Non-sinus tachycardia can be more proble-matic and appropriate treatment depends on theexact type. AV synchrony is particularly importantin LCOS as the effects of atrial systole (atrial kick)on ventricular preload can be significant, contri-buting up to 20% of stroke volume. Even if thearrhythmia is at an acceptable rate, efforts toachieve AV synchrony, either by AV sequentialpacing or treating the arrhythmia can be reward-ing. JET62 is the commonest arrhythmia in thissetting, and rate control by temperature reductionor amiodarone followed by AV pacing, is appro-priate management. Resynchronization therapy hasbeen of benefit in the adult population withcongestive cardiac failure and QRS delay, improvingsymptoms, reversing ventricular dilatation andmitral regurgitation, and increasing cardiac out-put.63,64 Following cardiac surgery in children, AVand intraventricular conduction delay is frequentlyseen. Biventricular pacing techniques have beenused in some children following cardiac surgery tooptimize haemodynamics.65
Minimizing the consequences of LCOSClassically, a prolonged period of LCOS can lead to aventilator-dependant, oedematous, malnourishedchild, with significant sedation problems andvascular access difficulties. Much can be done tominimize the effects of LCOS while awaitingintrinsic myocardial recovery.
Renal failure and fluid retention are common dueto poor renal perfusion and low mean bloodpressure. Diuretics are usually necessary after thefirst 24 h. Continuous infusions of frusemide areoften preferable to boluses, with greater fluid lossand less cardiovascular instability.66 Early perito-neal dialysis (PD) started prior to significantoedema formation, can prevent excessive fluid
bolus administration, ionotrope escalation andfrusemide toxicity.67 Many surgeons routinely placedialysis catheters at operation in high-risk cases.68
This significantly lowers the threshold for commen-cing PD. Volumes up to 30ml/kg seem to be welltolerated.68 A recent series found PD was used in20% of CPB cases and that the risk factors forneeding PD were identical to those for developingLCOS.69
Respiratory failure following LCOS is usuallymultifactorial, resulting from fluid overload, mal-nutrition, muscle weakness, critical illness poly-neuropathy, atelectasis, upper airway oedema andintrinsic lung disease, with significant reduction inFRC secondary to sternotomy. Appropriate ventila-tion strategies that optimize PEEP, minimize tidalvolume (6-8ml/kg) and avoid paralysis are optimal.
Optimal nutrition is often difficult due to fluidrestriction and gut failure. Early enteral nutritionand the early use of jejunal feeding strategies areimportant. TPN is sometimes required but canoften be avoided by jejunal feeding. It is oftenworth starting PD to make space for increasedcaloric intake.
Optimal sedation and uncomplicated venousaccess are always strived for but rarely achieved.
Conclusions
LCOS is a common problem in paediatric intensivecare that is often predictable and sometimespreventable. Diagnosis relies on anticipation, clin-ical features and investigation. Management isaimed at achieving the optimal balance betweenoxygen delivery and oxygen consumption. Preloadand afterload should be optimized prior to escala-tion of inotropic support. The effects of PPV andnon-pharmacological strategies should not be un-derestimated.
References
1. Ravishankar C, Tabbutt S, Wernovsky G. Critical care incardiovascular medicine. Curr Opin Pediatr 2003;15(5):443–53.
2. Wan S, LeClerc JL, Vincent JL. Inflammatory response tocardiopulmonary bypass: mechanisms involved and possibletherapeutic strategies. Chest 1997;112(3):676–92.
3. Brown KL, Ridout DA, Goldman AP, Hoskote A, Penny DJ. Riskfactors for long intensive care unit stay after cardiopulmon-ary bypass in children. Crit Care Med 2003;31(1):28–33.
4. Pizarro C, Malec E, Maher KO, Januszewska K, Gidding SS,Murdison KA, et al. Right ventricle to pulmonary arteryconduit improves outcome after stage I Norwood forhypoplastic left heart syndrome. Circulation 2003;108(Suppl. 1):II155–60.

ARTICLE IN PRESS
Low cardiac output syndrome in children 357
5. Tibby SM, Hatherill M, Murdoch IA. Capillary refill andcore–peripheral temperature gap as indicators of haemody-namic status in paediatric intensive care patients. Arch DisChild 1999;80(2):163–6.
6. Tibby SM, Hatherill M, Marsh MJ, Murdoch IA. Clinicians’abilities to estimate cardiac index in ventilated children andinfants. Arch Dis Child 1997;77(6):516–8.
7. Murray DM, Olhsson V, Fraser JI. Defining acidosis inpostoperative cardiac patients using Stewart’s method ofstrong ion difference. Pediatr Crit Care Med 2004;5(3):240–5.
8. Durward A, Tibby SM, Skellett S, Austin C, Anderson D,Murdoch IA. The strong ion gap predicts mortality in childrenfollowing cardiopulmonary bypass surgery. Pediatr Crit CareMed 2005;6(3):281–5.
9. Tibby SM, Murdoch IA. Monitoring cardiac function inintensive care. Arch Dis Child 2003;88(1):46–52.
10. Charpie JR, Dekeon MK, Goldberg CS, Mosca RS, Bove EL,Kulik TJ. Serial blood lactate measurements predict earlyoutcome after neonatal repair or palliation for complexcongenital heart disease. J Thorac Cardiovasc Surg 2000;120(1):73–80.
11. Rossi AF, Khan DM, Hannan R, Bolivar J, Zaidenweber M,Burke R. Goal-directed medical therapy and point-of-caretesting improve outcomes after congenital heart surgery.Intens Care Med 2005;31(1):98–104.
12. Schroeder TH, Hansen M. Effects of fresh versus old storedblood in the priming solution on whole blood lactate levelsduring paediatric cardiac surgery. Perfusion 2005;20(1):17–9.
13. Francis DP, Willson K, Thorne SA, Davies LC, Coats AJ.Oxygenation in patients with a functionally univentricularcirculation and complete mixing of blood: are saturation andflow interchangeable? Circulation 1999;100(21):2198–203.
14. Tweddell JS, Hoffman GM, Fedderly RT, Ghanayem NS,Kampine JM, Berger S, et al. Patients at risk for low systemicoxygen delivery after the Norwood procedure. Ann ThoracSurg 2000;69(6):1893–9.
15. Cullen S, Shore D, Redington A. Characterization of rightventricular diastolic performance after complete repair oftetralogy of Fallot. Restrictive physiology predicts slowpostoperative recovery. Circulation 1995;91(6):1782–9.
16. Gnaegi A, Feihl F, Perret C. Intensive care physicians’insufficient knowledge of right-heart catheterization at thebedside: time to act? Crit Care Med 1997;25(2):213–20.
17. Lemler MS, Scott WA, Leonard SR, Stromberg D, RamaciottiC. Fenestration improves clinical outcome of the Fontanprocedure: a prospective, randomized study. Circulation2002;105(2):207–12.
18. Shekerdemian LS, Bush A, Shore DF, Lincoln C, Redington AN.Cardiopulmonary interactions after Fontan operations:augmentation of cardiac output using negative pressureventilation. Circulation 1997;96(11):3934–42.
19. Tweddell JS, Hoffman GM, Fedderly RT, Berger S, Thomas JrJP, Ghanayem NS, et al. Phenoxybenzamine improvessystemic oxygen delivery after the Norwood procedure.Ann Thorac Surg 1999;67(1):161–7 [discussion 167-8].
20. Naughton MT, Rahman MA, Hara K, Floras JS, Bradley TD.Effect of continuous positive airway pressure on intrathor-acic and left ventricular transmural pressures in patientswith congestive heart failure. Circulation 1995;91(6):1725–31.
21. Schreiber MD, Gin-Mestan K, Marks JD, Huo D, Lee G,Srisuparp P. Inhaled nitric oxide in premature infants withthe respiratory distress syndrome. N Engl J Med 2003;349(22):2099–107.
22. Journois D, Pouard P, Mauriat P, Malhere T, Vouhe P, Safran D.Inhaled nitric oxide as a therapy for pulmonary hypertensionafter operations for congenital heart defects. J ThoracCardiovasc Surg 1994;107(4):1129–35.
23. Atz AM, Adatia I, Wessel DL. Rebound pulmonary hyperten-sion after inhalation of nitric oxide. Ann Thorac Surg1996;62(6):1759–64.
24. Miller OI, Tang SF, Keech A, Pigott NB, Beller E, CelermajerDS. Inhaled nitric oxide and prevention of pulmonaryhypertension after congenital heart surgery: a randomiseddouble-blind study. Lancet 2000;356(9240):1464–9.
25. Atz AM, Wessel DL. Sildenafil ameliorates effects ofinhaled nitric oxide withdrawal. Anesthesiology 1999;91(1):307–10.
26. Bellomo R, Chapman M, Finfer S, Hickling K, Myburgh J. Low-dose dopamine in patients with early renal dysfunction: aplacebo-controlled randomised trial. Australian and NewZealand Intensive Care Society (ANZICS) Clinical TrialsGroup. Lancet 2000;356(9248):2139–43.
27. Van den Berghe G. Endocrine evaluation of patients withcritical illness. Endocrinol Metab Clin North Am 2003;32(2):385–410.
28. Setty SP, et al. Stage one Norwood procedure results: thegreen lane experience. Heart Lung Circ 2001;10(3):136–41.
29. Bristow MR, Ginsburg R, Minobe W, Cubicciotti RS, SagemanWS, Lurie K, et al. Decreased catecholamine sensitivity andbeta-adrenergic-receptor density in failing human hearts. NEngl J Med 1982;307(4):205–11.
30. Sato N, Asai K, Okumura S, Takagi G, Shannon RP, Fujita-Yamaguchi Y, et al. Mechanisms of desensitization to a PDEinhibitor (milrinone) in conscious dogs with heart failure. AmJ Physiol 1999;276(5 Pt 2):H1699–705.
31. Bayram M, De Luca L, Massie MB, Gheorghiade M. Reassess-ment of dobutamine, dopamine, and milrinone in themanagement of acute heart failure syndromes. Am J Cardiol2005;96(6A):47G–58G.
32. Cuffe MS, Califf RM, Adams KF, Bourge RC, Colucci W, MassieB, et al. Rationale and design of the OPTIME CHF trial:outcomes of a prospective trial of intravenous milrinone forexacerbations of chronic heart failure. Am Heart J 2000;139(1 Pt 1):15–22.
33. Hoffman TM, Wernovsky G, Atz AM, Kulik TJ, Nelson DP,Chang AC, et al. Efficacy and safety of milrinone inpreventing low cardiac output syndrome in infants andchildren after corrective surgery for congenital heartdisease. Circulation 2003;107(7):996–1002.
34. Kwak YL. Calcium sensitizers, a new class of inodilators. IntAnesthesiol Clin 2005;43(2):115–33.
35. Endoh M. Mechanisms of action of novel cardiotonic agents.J Cardiovasc Pharmacol 2002;40(3):323–38.
36. Follath F, Cleland JG, Just H, Papp JG, Scholz H,Peuhkurinen K, et al. Efficacy and safety of intravenouslevosimendan compared with dobutamine in severe low-output heart failure (the LIDO study): a randomised double-blind trial. Lancet 2002;360(9328):196–202.
37. Turanlahti M, Boldt T, Palkama T, Antila S, Lehtonen L,Pesonen E. Pharmacokinetics of levosimendan in pediatricpatients evaluated for cardiac surgery. Pediatr Crit CareMed 2004;5(5):457–62.
38. Braun JP, Schneider M, Dohmen P, Dopfmer U. Successfultreatment of dilative cardiomyopathy in a 12-year-old girlusing the calcium sensitizer levosimendan after weaningfrom mechanical biventricular assist support. J CardiothoracVasc Anesth 2004;18(6):772–4.

ARTICLE IN PRESS
B. Jones et al.358
39. Braun JP, Schneider M, Kastrup M, Liu J. Treatment of acuteheart failure in an infant after cardiac surgery usinglevosimendan. Eur J Cardiothorac Surg 2004;26(1):228–30.
40. Murzi B, Iervasi G, Masini S, Moschetti R, Vanini V, ZucchelliG, et al. Thyroid hormones homeostasis in pediatric patientsduring and after cardiopulmonary bypass. Ann Thorac Surg1995;59(2):481–5.
41. Mitchell IM, Pollock JC, Jamieson MP, Donaghey SF, Paton RD,Logan RW. The effects of cardiopulmonary bypass on thyroidfunction in infants weighing less than five kilograms.J Thorac Cardiovasc Surg 1992;103(4):800–5.
42. Klemperer JD, Klein I, Gomez M, Helm RE, Ojamaa K,Thomas SJ, et al. Thyroid hormone treatment aftercoronary-artery bypass surgery. N Engl J Med 1995;333(23):1522–7.
43. Bettendorf M, Schmidt KG, Grulich-Henn J, Ulmer HE,Heinrich UE. Tri-iodothyronine treatment in children aftercardiac surgery: a double-blind, randomised, placebo-con-trolled study. Lancet 2000;356(9229):529–34.
44. Dimmick S, Badawi N, Randell T. Thyroid hormone supple-mentation for the prevention of morbidity and mortality ininfants undergoing cardiac surgery. Cochrane Database SystRev 2004(3):CD004220.
45. Baden HP. Does nesiritide offer something new in themanagement of pediatric heart failure? Pediatr Crit CareMed 2005;6(5):613–4.
46. Colucci WS, Elkayam U, Horton DP, Abraham WT, Bourge RC,Johnson AD, et al. Intravenous nesiritide, a natriureticpeptide, in the treatment of decompensated congestiveheart failure. Nesiritide Study Group. N Engl J Med2000;343(4):246–53 [Erratum in: N Engl J Med 2000;343(20):1504. N Engl J Med 2000;343(12):896].
47. Mahle WT, Cuadrado AR, Kirshbom PM, Kanter KR, Simsic JM.Nesiritide in infants and children with congestive heartfailure. Pediatr Crit Care Med 2005;6(5):543–6.
48. McElhinney DB, Reddy VM, Parry AJ, Johnson L, Fineman JR,Hanley FL. Management and outcomes of delayed sternalclosure after cardiac surgery in neonates and infants. CritCare Med 2000;28(4):1180–4.
49. Long CB, Shah SS, Lautenbach E, Coffin SE, Tabbutt S,Gaynor JW, et al. Postoperative mediastinitis in children:epidemiology, microbiology and risk factors for Gram-negative pathogens. Pediatr Infect Dis J 2005;24(4):315–9.
50. Kovacikova L, Kunovsky P, Lakomy M, Skrak P, Hraska V,Kostalova L, et al. Thyroid function and ioduria in infantsafter cardiac surgery: comparison of patients with primaryand delayed sternal closure. Pediatr Crit Care Med 2005;6(2):154–9.
51. Main E, Elliott MJ, Schindler M, Stocks J. Effect of delayedsternal closure after cardiac surgery on respiratory functionin ventilated infants. Crit Care Med 2001;29(9):1798–802.
52. Li J, Schulze-Neick I, Lincoln C, Shore D, Scallan M, Bush A,et al. Oxygen consumption after cardiopulmonary bypasssurgery in children: determinants and implications. J ThoracCardiovasc Surg 2000;119(3):525–33.
53. Deakin CD, Knight H, Edwards JC, Monro JL, Lamb RK,Keeton B, et al. Induced hypothermia in the postoperativemanagement of refractory cardiac failure following paedia-tric cardiac surgery. Anaesthesia 1998;53(9):848–53.
54. Dalrymple-Hay MJ, Deakin CD, Knight H, Edwards JC, KeetonB, Salmon AP, et al. Induced hypothermia as salvage
treatment for refractory cardiac failure following paediatriccardiac surgery. Eur J Cardiothorac Surg 1999;15(4):515–8.
55. Salzer-Muhar UE, Marx M, Wimmer M. Pediatric cardiacextracorporeal membrane oxygenation in congenital heartdisease: the cardiologist’s view. Artif Organs 1999;23(11):995–1000.
56. Bartlett RH, Roloff DW, Custer JR, Younger JG, Hirschl RB.Extracorporeal life support: the University of Michiganexperience. JAMA 2000;283(7):904–8.
57. Goldman AP, Cassidy J, de Leval M, Haynes S, Brown K,Whitmore P, et al. The waiting game: bridging to paediatricheart transplantation. Lancet 2003;362(9400):1967–70.
58. Boucek M. Paediatric acute heart failure—from deck chairsto lifeboats. Lancet 2003;362(9400):1948–9.
59. Shekerdemian L. Nonpharmacologic treatment of acuteheart failure. Curr Opin Pediatr 2001;13(3):240–6.
60. Wessel DL. Managing low cardiac output syndrome aftercongenital heart surgery. Crit Care Med 2001;29(10, Suppl.):S220–30.
61. Hoffman TM, Wernovsky G, Wieand TS, Cohen MI, JenningsAC, Vetter VL, et al. The incidence of arrhythmias in apediatric cardiac intensive care unit. Pediatr Cardiol 2002;23(6):598–604.
62. Hoffman TM, Bush DM, Wernovsky G, Cohen MI, Wieand TS,Gaynor JW, et al. Postoperative junctional ectopic tachy-cardia in children: incidence, risk factors, and treatment.Ann Thorac Surg 2002;74(5):1607–11.
63. Saxon LA, Ellenbogen KA. Resynchronization therapy for thetreatment of heart failure. Circulation 2003;108(9):1044–8.
64. Young JB, Abraham WT, Smith AL, Leon AR, Lieberman R,Wilkoff B, et al. Combined cardiac resynchronization andimplantable cardioversion defibrillation in advanced chronicheart failure: the MIRACLE ICD trial. JAMA 2003;289(20):2685–94.
65. Blom NA, Bax JJ, Ottenkamp J, Schalij MJ. Transvenousbiventricular pacing in a child after congenital heart surgeryas an alternative therapy for congestive heart failure.J Cardiovasc Electrophysiol 2003;14(10):1110–2.
66. Singh NC, Kissoon N, al Mofada S, Bennett M, Bohn DJ.Comparison of continuous versus intermittent furosemideadministration in postoperative pediatric cardiac patients.Crit Care Med 1992;20(1):17–21.
67. Sorof JM, Stromberg D, Brewer ED, Feltes TF, Fraser Jr CD.Early initiation of peritoneal dialysis after surgical repair ofcongenital heart disease. Pediatr Nephrol 1999;13(8):641–5.
68. Morris KP, Butt WW, Karl TR. Effect of peritoneal dialysis onintra-abdominal pressure and cardio-respiratory function ininfants following cardiac surgery. Cardiol Young 2004;14(3):293–8.
69. Chan KL, Ip P, Chiu CS, Cheung YF. Peritoneal dialysis aftersurgery for congenital heart disease in infants and youngchildren. Ann Thorac Surg 2003;76(5):1443–9.
70. Mottram PM, Marwick TH. Assessment of diastolic function:what the general cardiologist needs to know. Heart2005;91(5):681–95.
71. Rathore KS, Gupta N, Kapoor A, Modi N, Singh PK, Tewari P,et al. Assessment of right ventricular diastolic function: doesit predict post-operative course in tetralogy of Fallot. IndianHeart J 2004;56(3):220–4.
72. Shekerdemian L, Bohn D. Cardiovascular effects of mecha-nical ventilation. Arch Dis Child 1999;80(5):475–80.