“long-term management of - eis.hu.edu.jo · ferris fl iii, wilkinson cp, bird a, et al. clinical...
TRANSCRIPT
“Long-term Management of AMD”
Motasem Al-latayfeh, MDAssistant Prof. Ophthalmology
Hashemite UniversityJordan
DEFINITION1
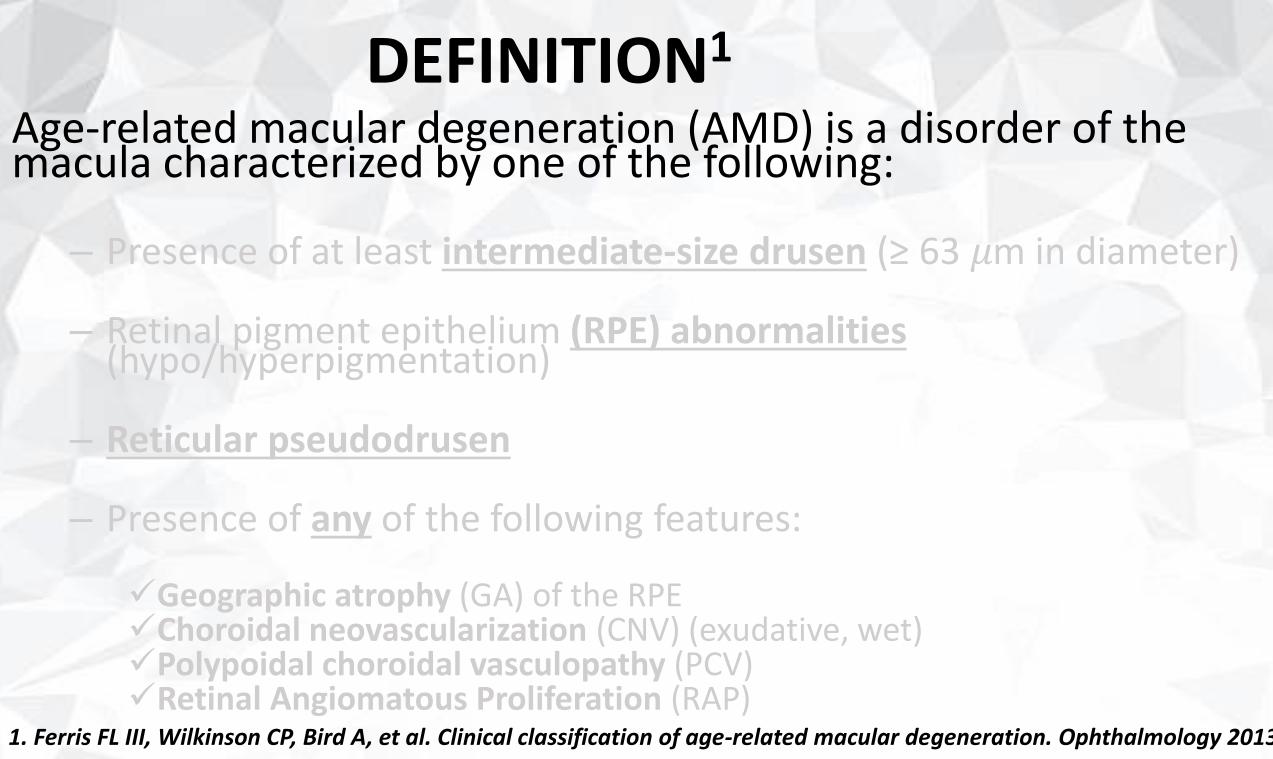
Age-related macular degeneration (AMD) is a disorder of the macula characterized by one of the following:
– Presence of at least intermediate-size drusen (≥ 63 𝜇m in diameter)
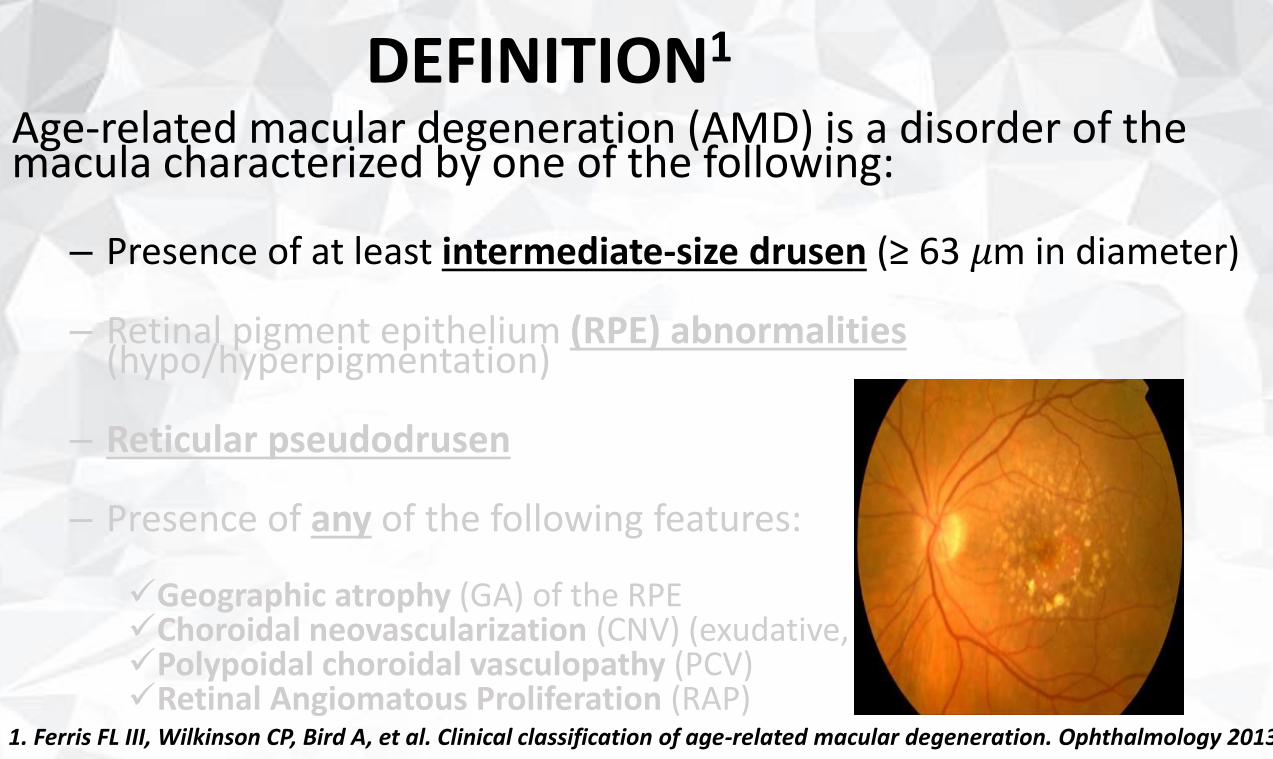
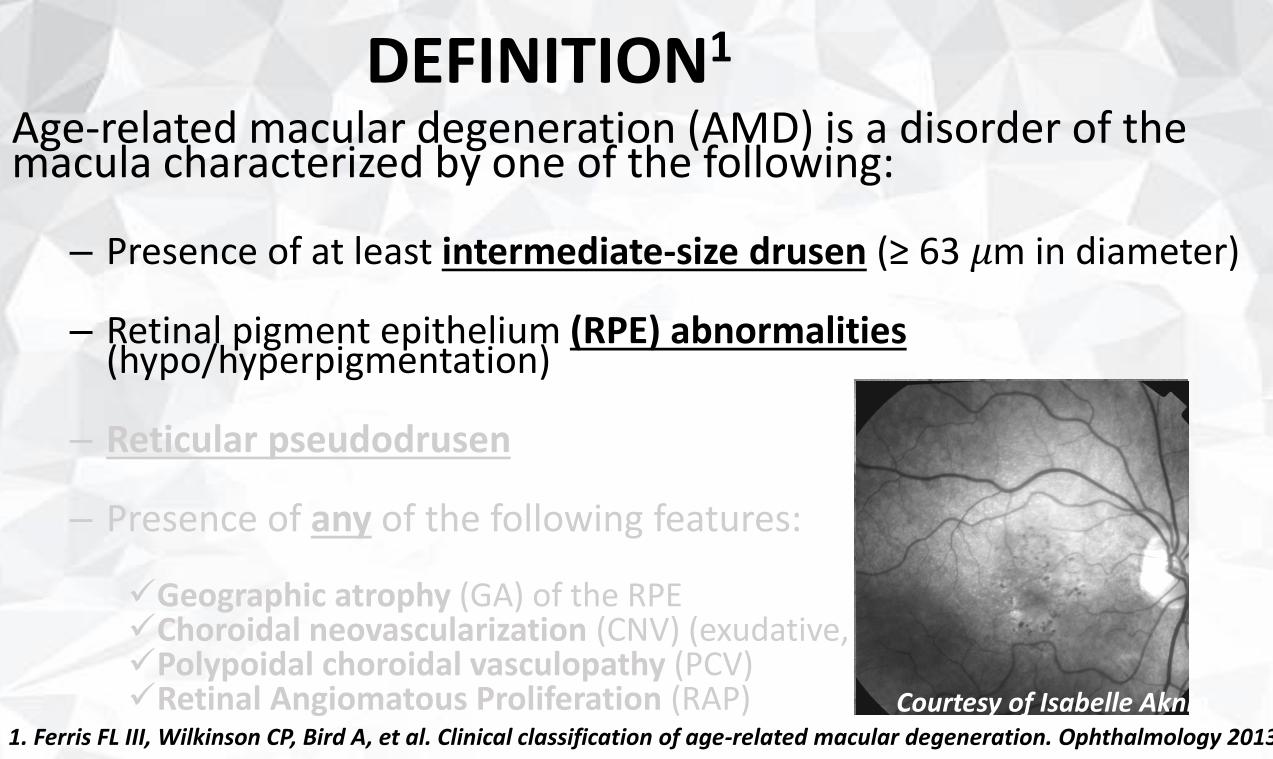
– Retinal pigment epithelium (RPE) abnormalities (hypo/hyperpigmentation)
– Reticular pseudodrusen
– Presence of any of the following features:
✓Geographic atrophy (GA) of the RPE✓Choroidal neovascularization (CNV) (exudative, wet)✓Polypoidal choroidal vasculopathy (PCV)✓Retinal Angiomatous Proliferation (RAP)
1. Ferris FL III, Wilkinson CP, Bird A, et al. Clinical classification of age-related macular degeneration. Ophthalmology 2013;1
DEFINITION1
Age-related macular degeneration (AMD) is a disorder of the macula characterized by one of the following:
– Presence of at least intermediate-size drusen (≥ 63 𝜇m in diameter)
– Retinal pigment epithelium (RPE) abnormalities (hypo/hyperpigmentation)
– Reticular pseudodrusen
– Presence of any of the following features:
✓Geographic atrophy (GA) of the RPE✓Choroidal neovascularization (CNV) (exudative, wet)✓Polypoidal choroidal vasculopathy (PCV)✓Retinal Angiomatous Proliferation (RAP)
1. Ferris FL III, Wilkinson CP, Bird A, et al. Clinical classification of age-related macular degeneration. Ophthalmology 2013;1
DEFINITION1
Age-related macular degeneration (AMD) is a disorder of the macula characterized by one of the following:
– Presence of at least intermediate-size drusen (≥ 63 𝜇m in diameter)
– Retinal pigment epithelium (RPE) abnormalities (hypo/hyperpigmentation)
– Reticular pseudodrusen
– Presence of any of the following features:
✓Geographic atrophy (GA) of the RPE✓Choroidal neovascularization (CNV) (exudative, wet)✓Polypoidal choroidal vasculopathy (PCV)✓Retinal Angiomatous Proliferation (RAP)
1. Ferris FL III, Wilkinson CP, Bird A, et al. Clinical classification of age-related macular degeneration. Ophthalmology 2013;1
Courtesy of Isabelle Aknin
DEFINITION1
Age-related macular degeneration (AMD) is a disorder of the macula characterized by one of the following:
– Presence of at least intermediate-size drusen (≥ 63 𝜇m in diameter)
– Retinal pigment epithelium (RPE) abnormalities (hypo/hyperpigmentation)
– Reticular pseudodrusen
– Presence of any of the following features:
✓Geographic atrophy (GA) of the RPE✓Choroidal neovascularization (CNV) (exudative, wet)✓Polypoidal choroidal vasculopathy (PCV)✓Retinal Angiomatous Proliferation (RAP)
1. Ferris FL III, Wilkinson CP, Bird A, et al. Clinical classification of age-related macular degeneration. Ophthalmology 2013;1
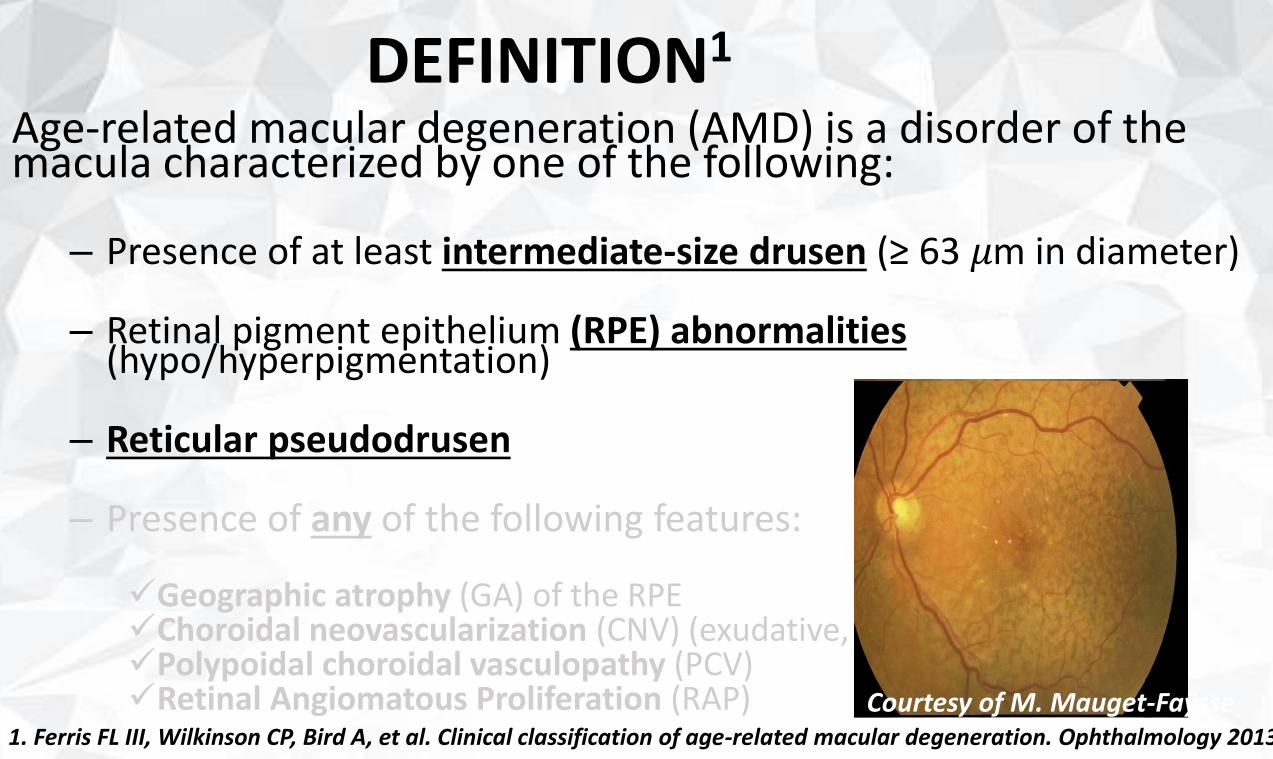
Courtesy of M. Mauget-Faÿsse
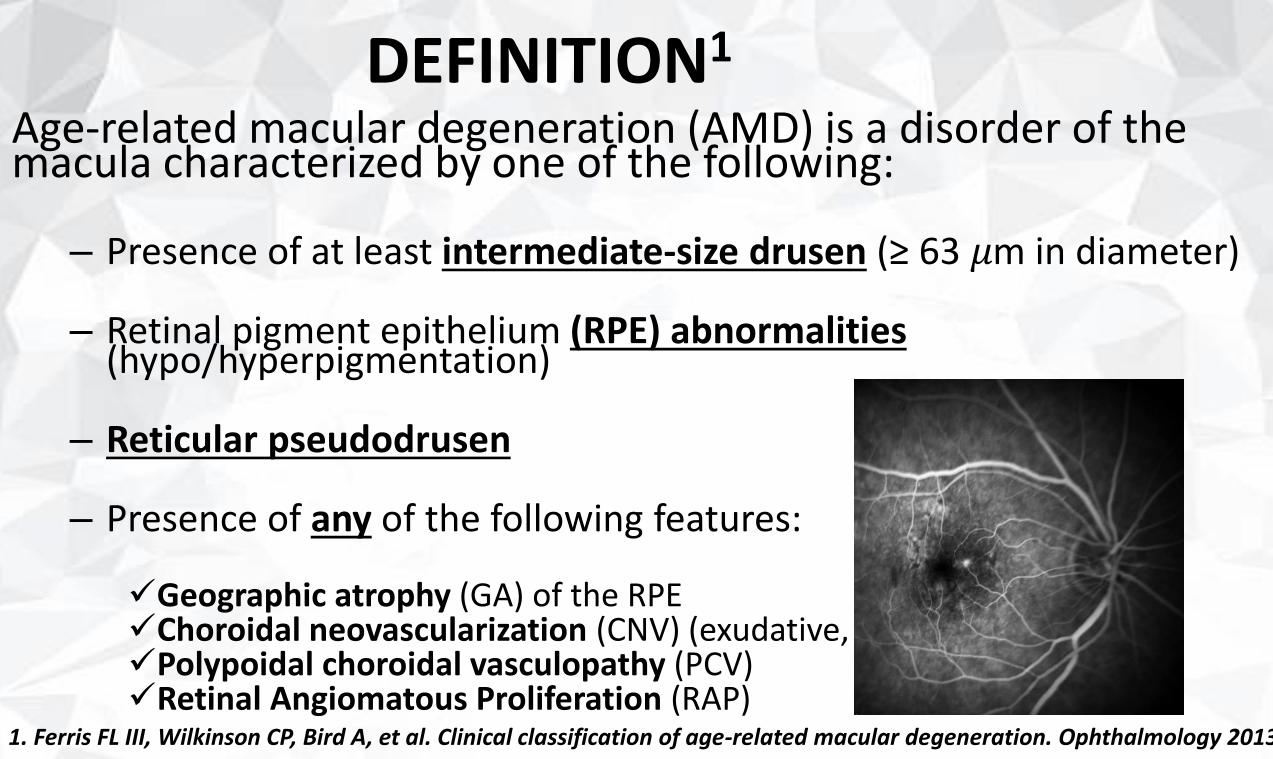
DEFINITION1
Age-related macular degeneration (AMD) is a disorder of the macula characterized by one of the following:
– Presence of at least intermediate-size drusen (≥ 63 𝜇m in diameter)
– Retinal pigment epithelium (RPE) abnormalities (hypo/hyperpigmentation)
– Reticular pseudodrusen
– Presence of any of the following features:
✓Geographic atrophy (GA) of the RPE✓Choroidal neovascularization (CNV) (exudative, wet)✓Polypoidal choroidal vasculopathy (PCV)✓Retinal Angiomatous Proliferation (RAP)
1. Ferris FL III, Wilkinson CP, Bird A, et al. Clinical classification of age-related macular degeneration. Ophthalmology 2013;1
“Guidelines For The Management of AMD”
PREVALENCE
“Guidelines For The Management of AMD”
PREVALENCE
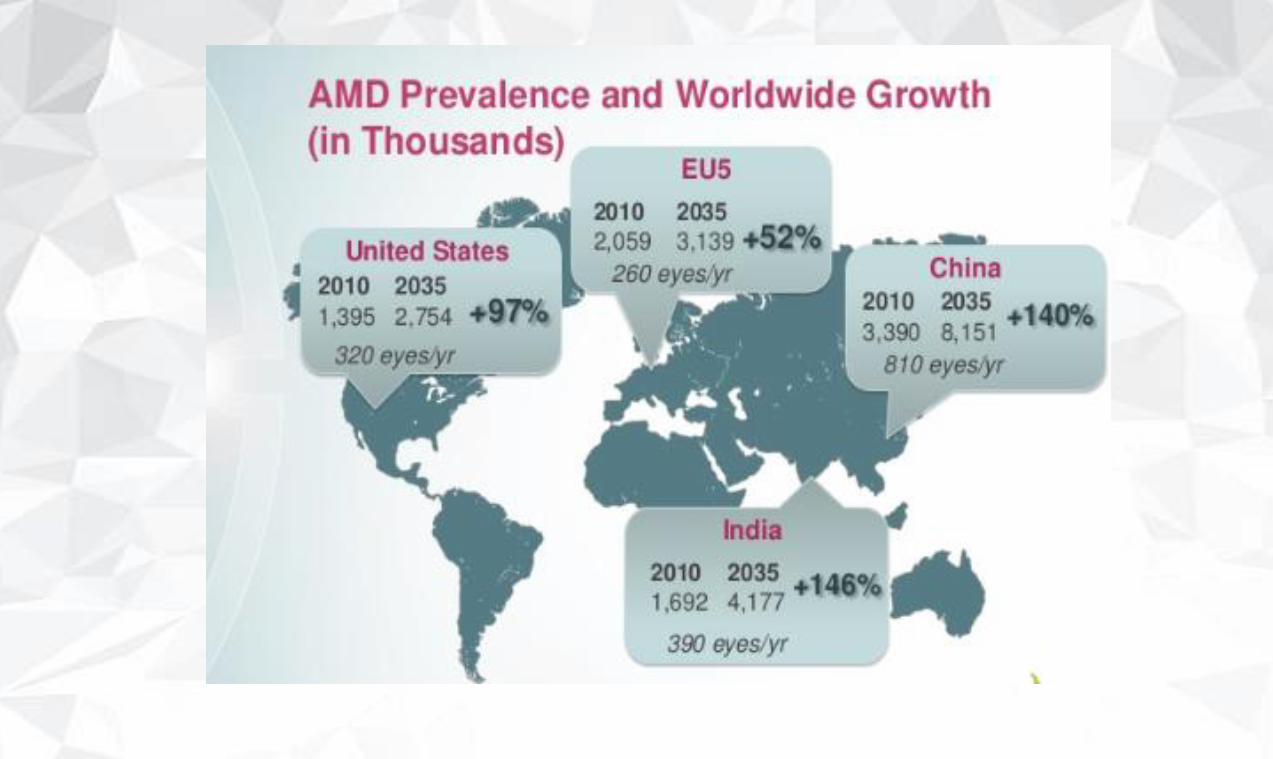
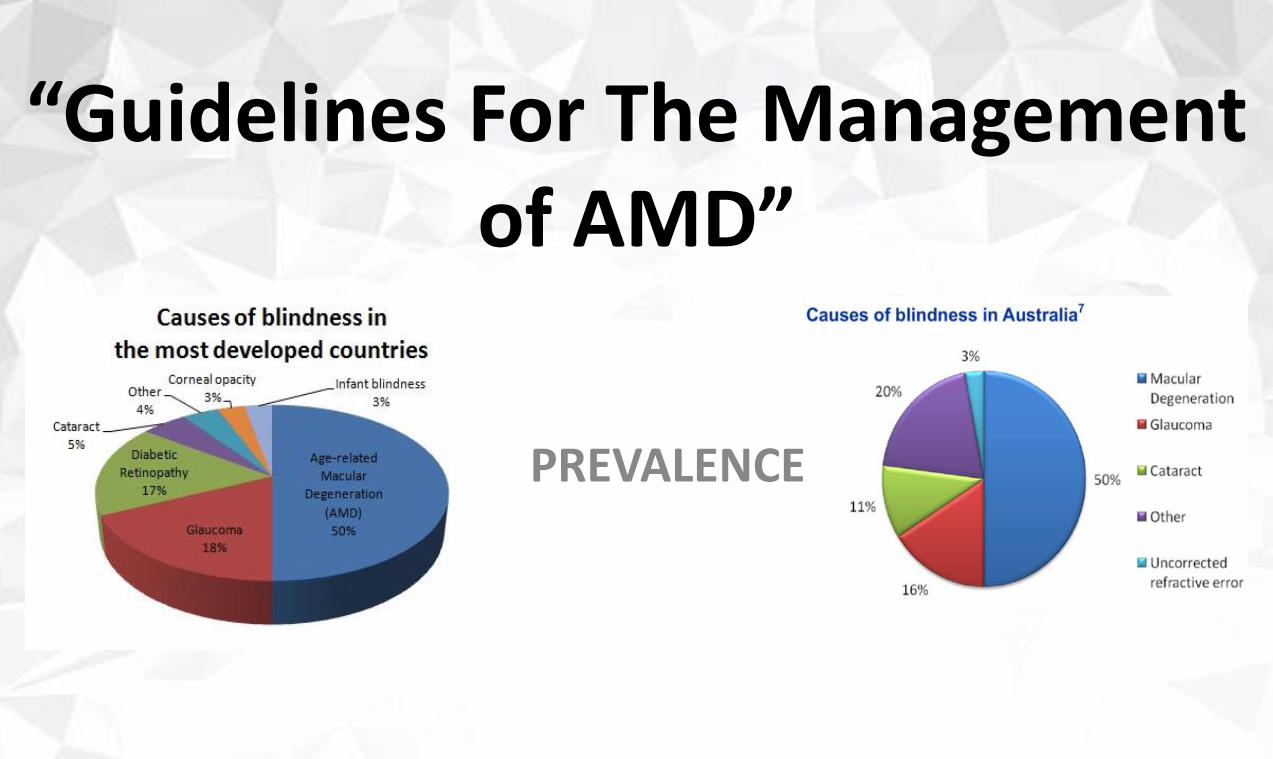
Prevalence2
• Leading cause of severe, irreversible vision impairment in developed countries:o USA in 2004:
✓1.75 M ≥ 40 yo neovascular AMD/geographic atrophy in at least 1 eye
✓7.3 M have high risk features (large drusen ≥ 125 𝜇m)
o USA in 2020:✓3 M ≥ 40 yo neovascular AMD/geographic atrophy in at least 1 eye
• Antioxidants vitamins (e.g. vitamin C, vitamin E), lutein, zeaxanthin, and zinc ↘ progression AMD by approximately 25% at 5 years
2. Congdon N, O’Colmain B, Klaver CC, et al. Causes and prevalence of visual impairment among adults in the united states. Arch Ophthlmol 2004;122:564
3. Klein R, Klein BE, Tomany SC, et al. Ten-year incidence and progression of age-related maculopathy: The Beaver Dam Eye Study. Ophthalmology 2006;109:1767
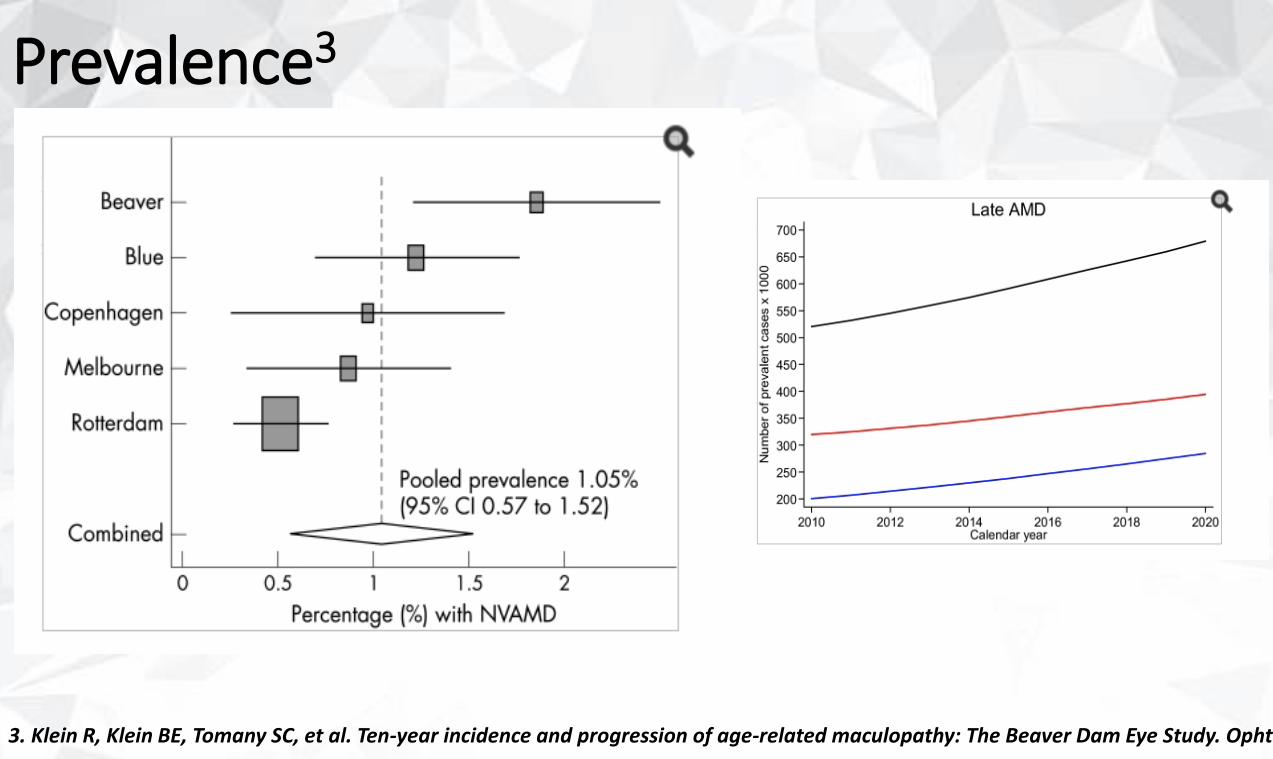
Prevalence3
• AMD is responsible for an estimated 46% of cases of severe visual loss (VA ≤ 20/200)
o Although 80% of AMD patients have the non-neovascular (atrophic) form
o The neovascular form is responsible for 90% of the severe VA loss
“Guidelines For The Management of AMD”
RISK FACTORS
Risk Factors4
• Age (≥ 75 yo)• Race (caucasians)• Smoking
o Dose response relationship o R AMD in subjects who did not smoke ≥ 20y = R AMD in nonsmokerso Smoking cessation is strongly recommendedo Hypertension & other cardiovascular diseases are not risk factors
4. Age-Related Eye Disease Study 2 (AREDS2) Research Group, Chew EY, SanGiovanni JP, Ferris FL, et al. Lutein/Zeaxanthin for the treatment of age-related cataract: AREDS 2 randomized trial report number 4. JAMA Ophthalmol 2013;131:843-50
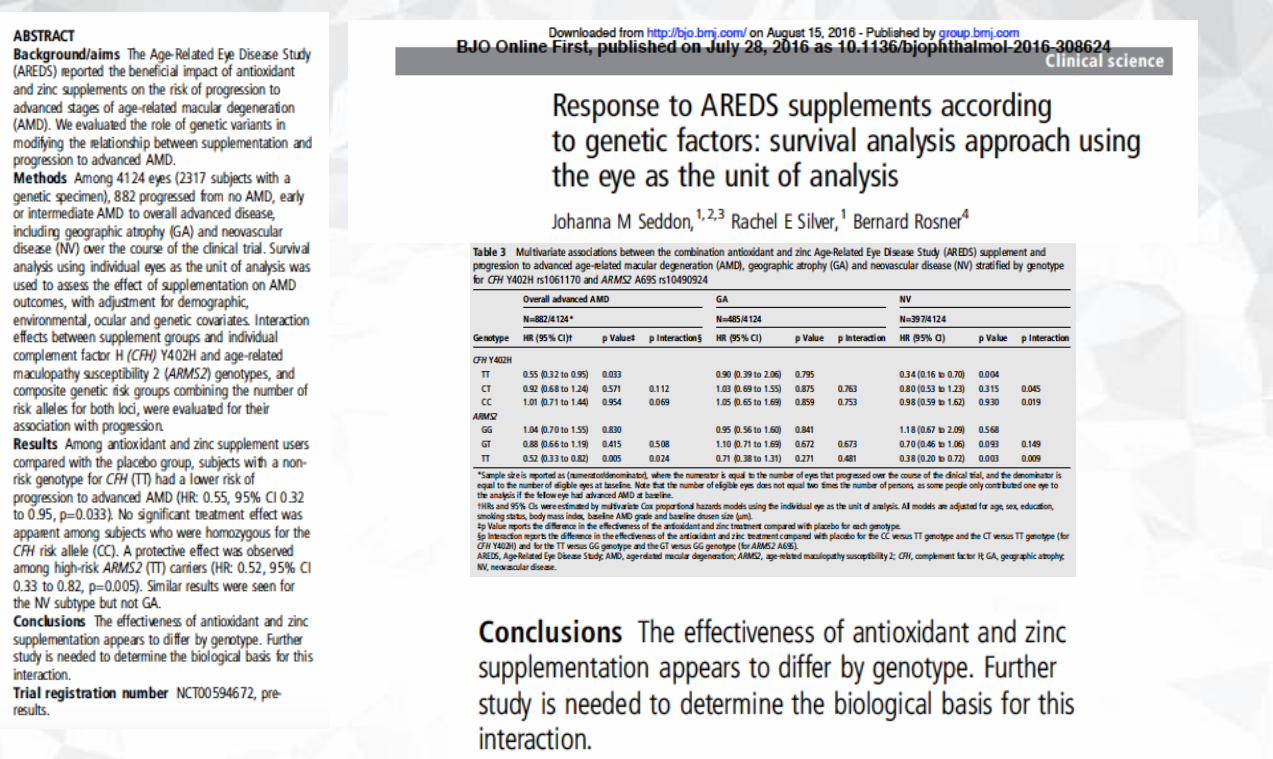
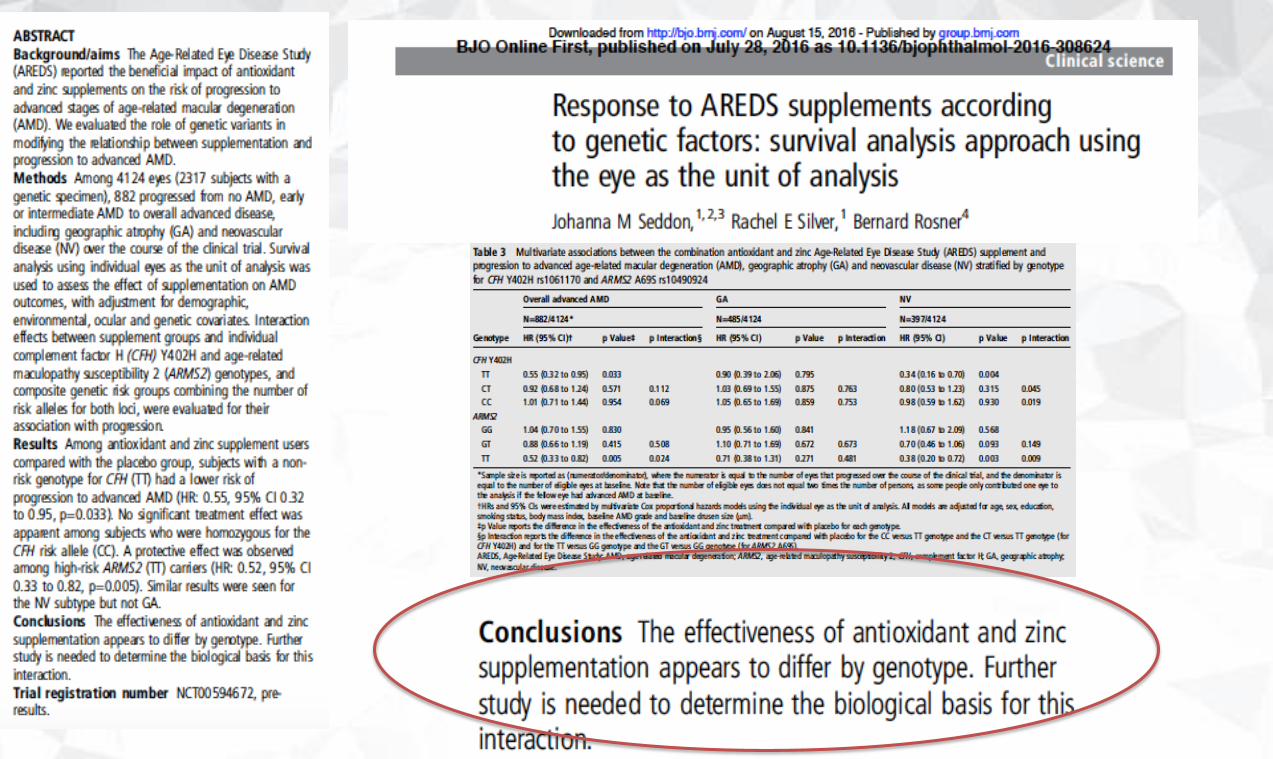
• Levels of antioxidants o Inconsistent data in identifying low levels of plasma levelso Antioxidants vitamins (Vit C, Vit A, beta-carotene) + zinc
↘ progression AMD by 25% at 5 yearso Replacement of beta-carotene with lutein/zeaxanthin in
the new AREDS2 formulationo ↘ competitive absorption of lutein/zeaxanthin o ↘ incidence lung cancer in smokers
• Dieto ↘ incidence dietary intake of foods rich in omega-3 long-
chain polyunsaturated fatty acids (fish) o Not necessarily in the form of supplemento ↗ incidence with higher intake of saturated fat o ↗ incidence BMI
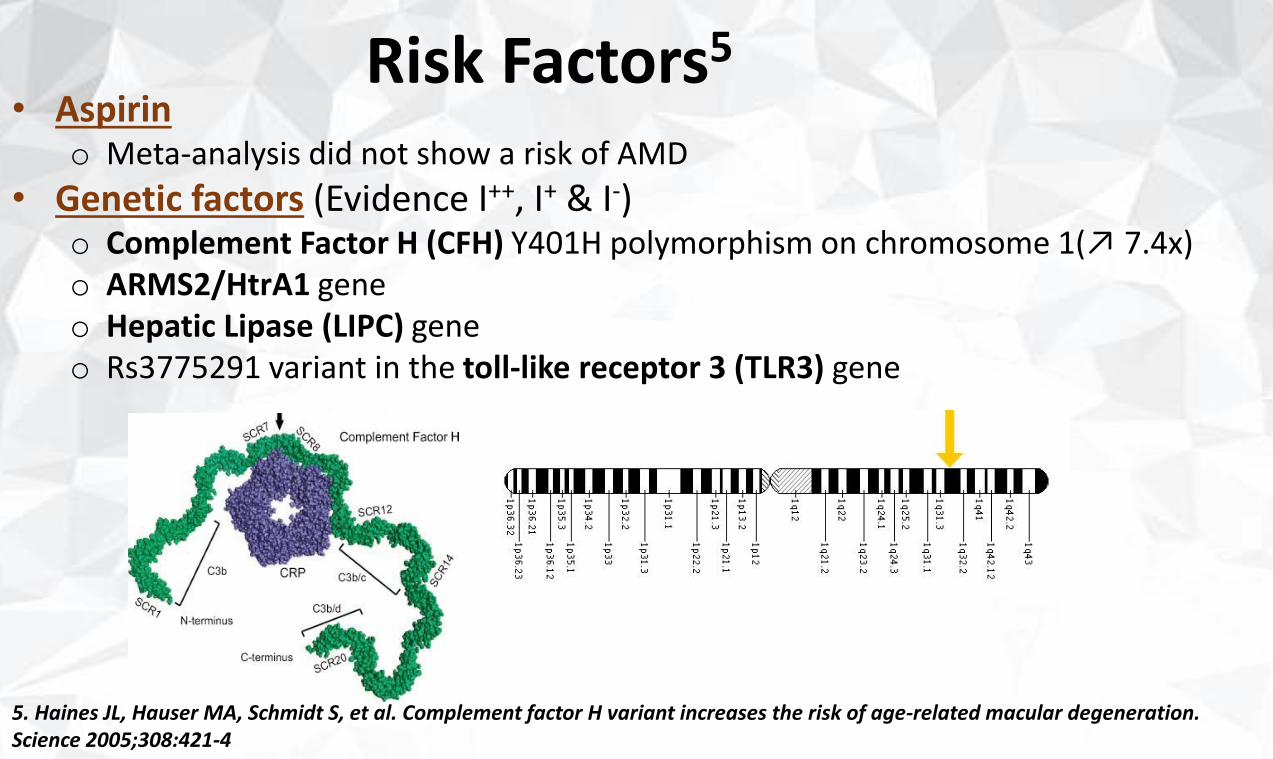
Risk Factors5
• Aspirino Meta-analysis did not show a risk of AMD
• Genetic factors (Evidence I++, I+ & I-)o Complement Factor H (CFH) Y401H polymorphism on chromosome 1(↗ 7.4x)o ARMS2/HtrA1 geneo Hepatic Lipase (LIPC) geneo Rs3775291 variant in the toll-like receptor 3 (TLR3) gene
5. Haines JL, Hauser MA, Schmidt S, et al. Complement factor H variant increases the risk of age-related macular degeneration. Science 2005;308:421-4
Risk Factors5
• Other risk factors
oWaist/hip ratio for men
o Hormonal status
o Sunlight exposure
oMarkers of inflammation: ↗ C-reactive protein, ↗ erythrocytesedimentation rate
o Alcohol use
o Vitamins B & D status, Calcium?
5. Haines JL, Hauser MA, Schmidt S, et al. Complement factor H variant increases the risk of age-related macular degeneration. Science 2005;308:421
“Guidelines For The Management of AMD”
DIAGNOSIS
DIAGNOSIS• History
– Symptomso Metamorphopsiao Decreased vision o Photopsiao Difficulties in dark adaptation
– Medication and nutrition supplement use– Ocular history – Medical history (including hypersensitivity reactions)– Family history (AMD)– Social history (Smoking)
• Physical examination– Comprehensive eye examination– Stereoscopic biomicroscopic examination of the macula
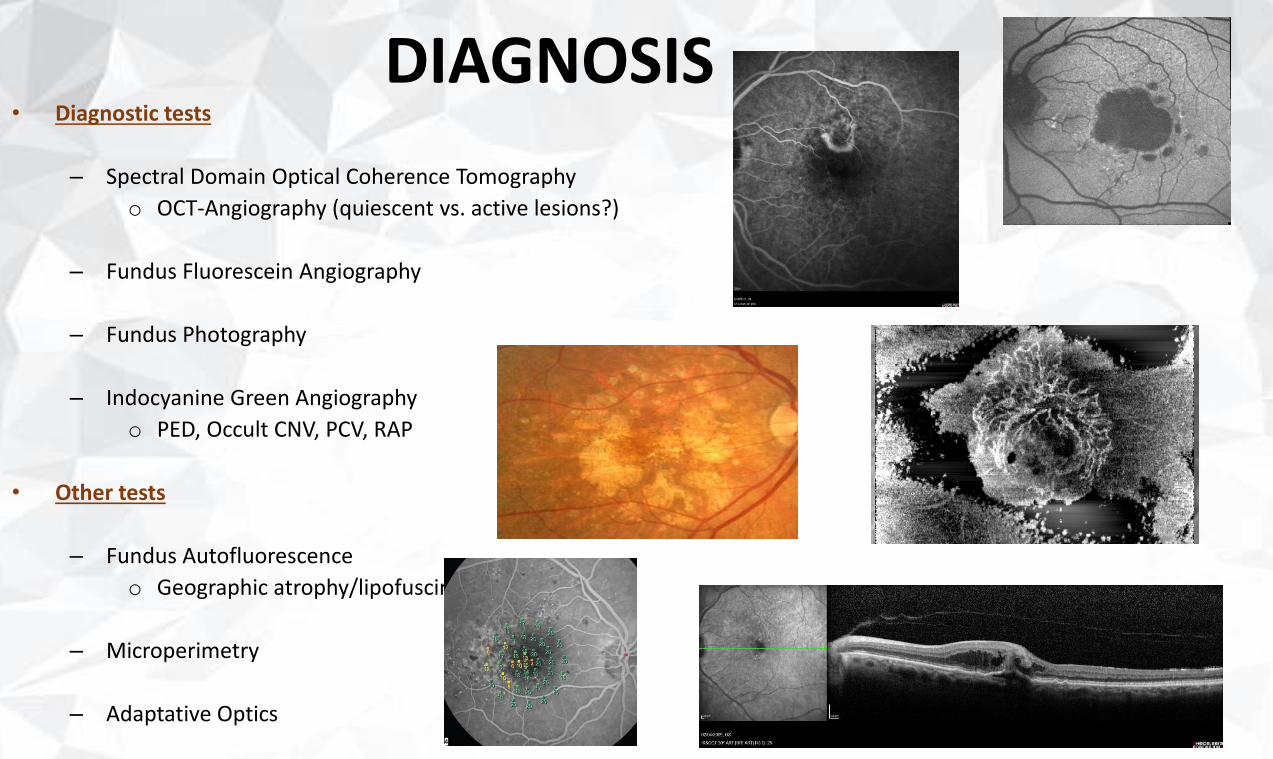
DIAGNOSIS• Diagnostic tests
– Spectral Domain Optical Coherence Tomography
o OCT-Angiography (quiescent vs. active lesions?)
– Fundus Fluorescein Angiography
– Fundus Photography
– Indocyanine Green Angiography
o PED, Occult CNV, PCV, RAP
• Other tests
– Fundus Autofluorescence
o Geographic atrophy/lipofuscin
– Microperimetry
– Adaptative Optics
“Guidelines For The Management of AMD”
CLASSIFICATION
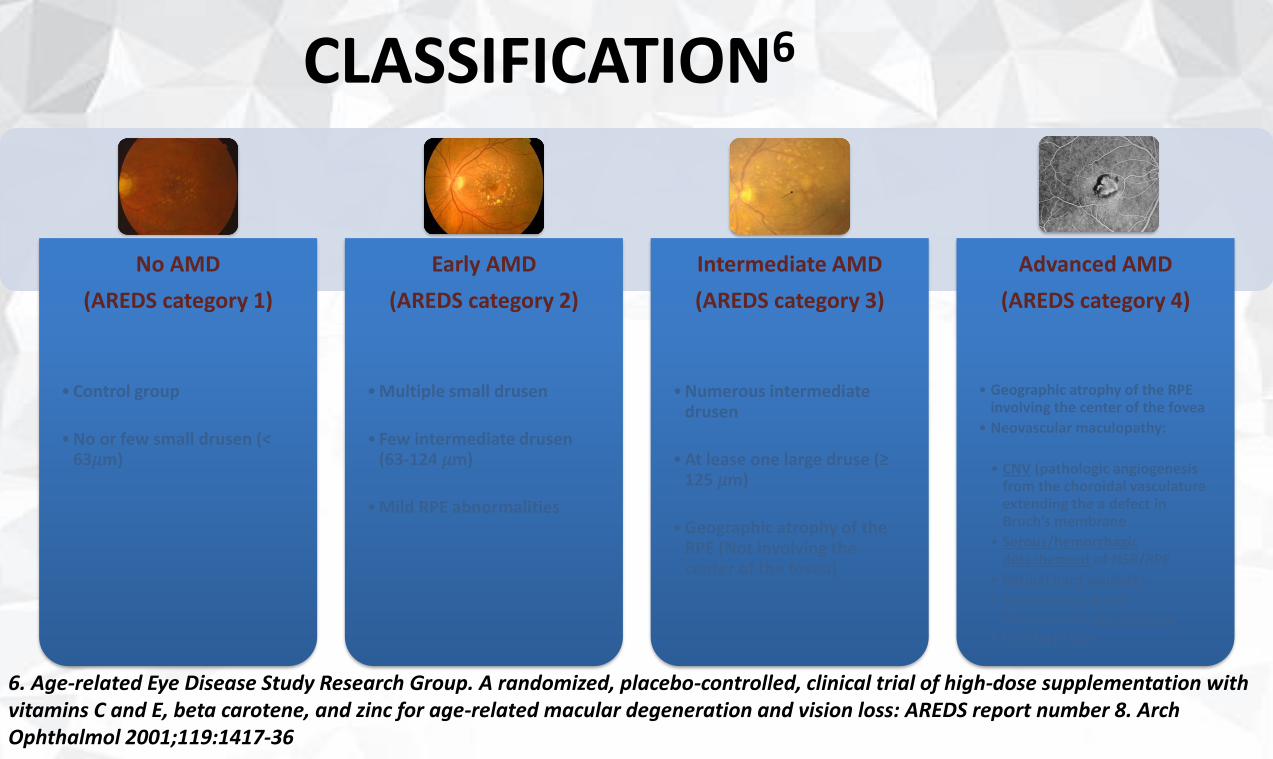
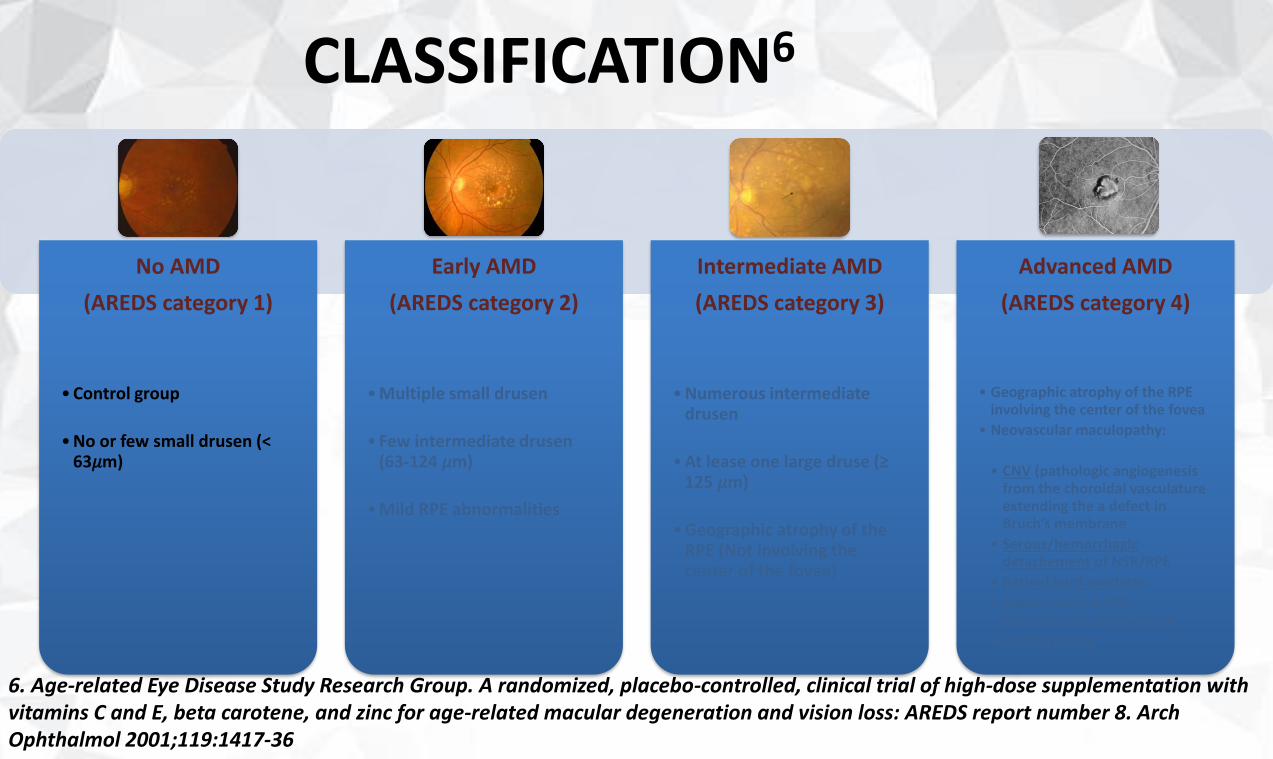
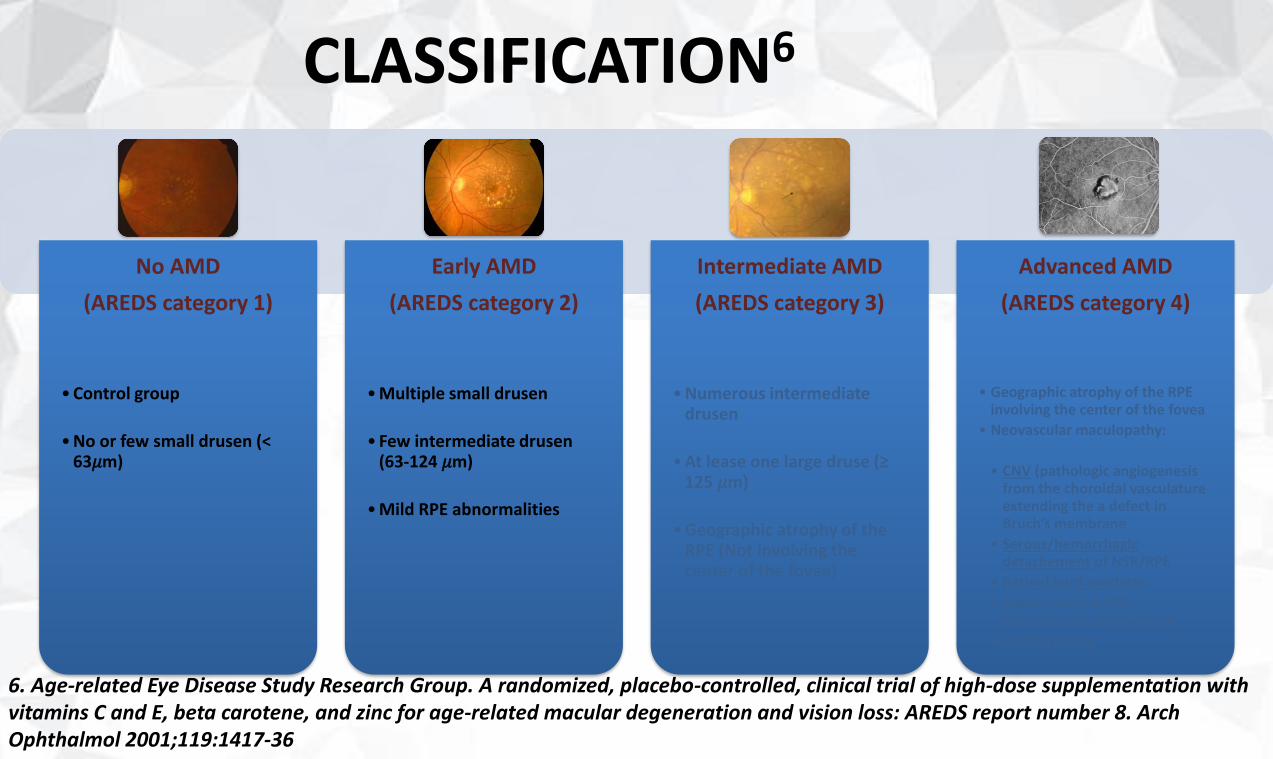
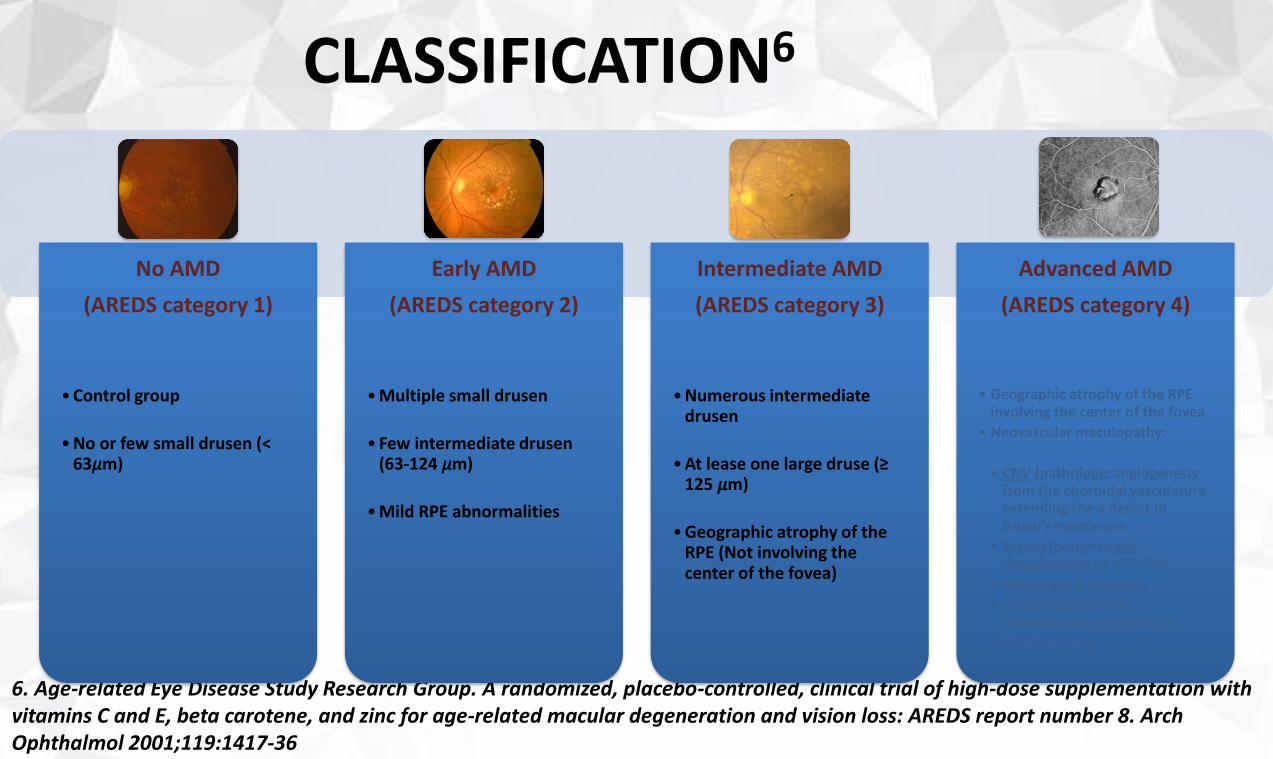
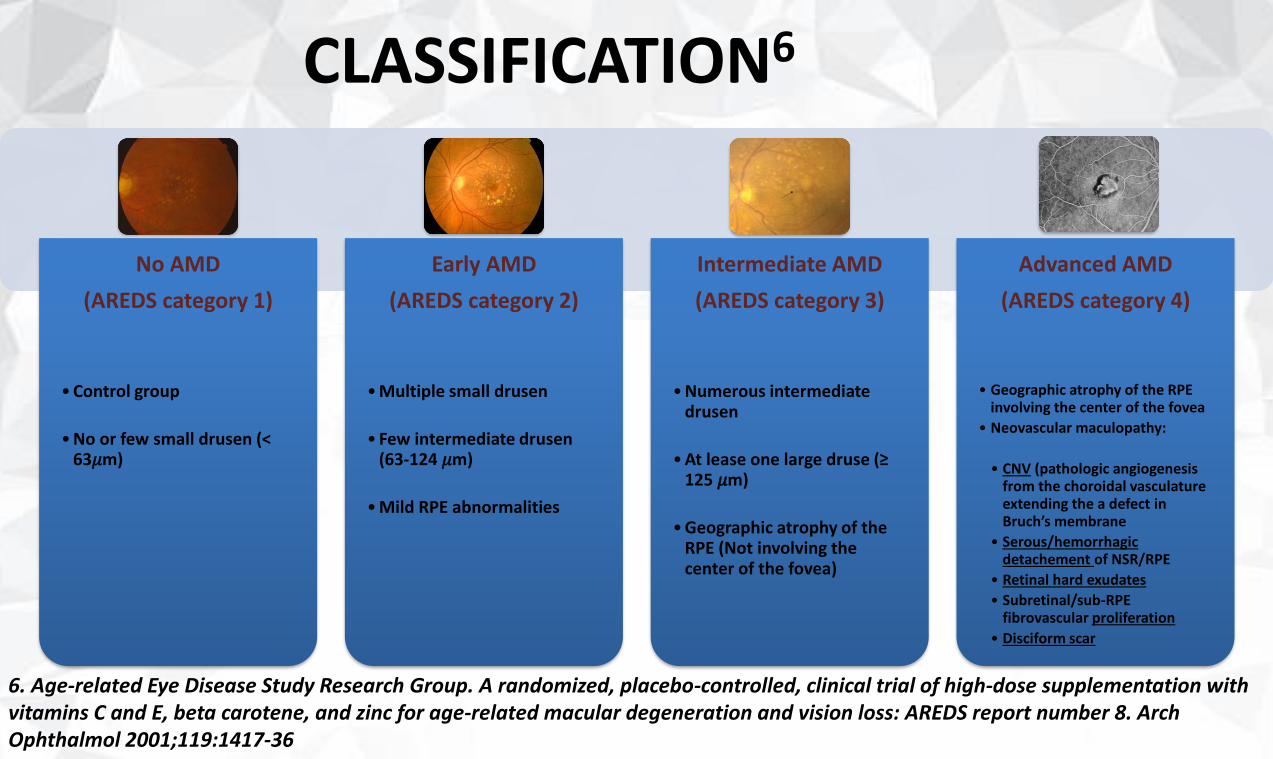
CLASSIFICATION6
6. Age-related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report number 8. Arch Ophthalmol 2001;119:1417-36
No AMD
(AREDS category 1)
• Control group
• No or few small drusen (< 63𝜇m)
Early AMD
(AREDS category 2)
• Multiple small drusen
• Few intermediate drusen(63-124 𝜇m)
• Mild RPE abnormalities
Intermediate AMD
(AREDS category 3)
• Numerous intermediate drusen
• At lease one large druse (≥ 125 𝜇m)
• Geographic atrophy of the RPE (Not involving the center of the fovea)
Advanced AMD
(AREDS category 4)
• Geographic atrophy of the RPEinvolving the center of the fovea
• Neovascular maculopathy:
• CNV (pathologic angiogenesisfrom the choroidal vasculature extending the a defect in Bruch’s membrane
• Serous/hemorrhagic detachement of NSR/RPE
• Retinal hard exudates
• Subretinal/sub-RPEfibrovascular proliferation
• Disciform scar
CLASSIFICATION6
6. Age-related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report number 8. Arch Ophthalmol 2001;119:1417-36
No AMD
(AREDS category 1)
• Control group
• No or few small drusen (< 63𝜇m)
Early AMD
(AREDS category 2)
• Multiple small drusen
• Few intermediate drusen(63-124 𝜇m)
• Mild RPE abnormalities
Intermediate AMD
(AREDS category 3)
• Numerous intermediate drusen
• At lease one large druse (≥ 125 𝜇m)
• Geographic atrophy of the RPE (Not involving the center of the fovea)
Advanced AMD
(AREDS category 4)
• Geographic atrophy of the RPEinvolving the center of the fovea
• Neovascular maculopathy:
• CNV (pathologic angiogenesisfrom the choroidal vasculature extending the a defect in Bruch’s membrane
• Serous/hemorrhagic detachement of NSR/RPE
• Retinal hard exudates
• Subretinal/sub-RPEfibrovascular proliferation
• Disciform scar
CLASSIFICATION6
6. Age-related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report number 8. Arch Ophthalmol 2001;119:1417-36
No AMD
(AREDS category 1)
• Control group
• No or few small drusen (< 63𝜇m)
Early AMD
(AREDS category 2)
• Multiple small drusen
• Few intermediate drusen(63-124 𝜇m)
• Mild RPE abnormalities
Intermediate AMD
(AREDS category 3)
• Numerous intermediate drusen
• At lease one large druse (≥ 125 𝜇m)
• Geographic atrophy of the RPE (Not involving the center of the fovea)
Advanced AMD
(AREDS category 4)
• Geographic atrophy of the RPEinvolving the center of the fovea
• Neovascular maculopathy:
• CNV (pathologic angiogenesisfrom the choroidal vasculature extending the a defect in Bruch’s membrane
• Serous/hemorrhagic detachement of NSR/RPE
• Retinal hard exudates
• Subretinal/sub-RPEfibrovascular proliferation
• Disciform scar
CLASSIFICATION6
6. Age-related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report number 8. Arch Ophthalmol 2001;119:1417-36
No AMD
(AREDS category 1)
• Control group
• No or few small drusen (< 63𝜇m)
Early AMD
(AREDS category 2)
• Multiple small drusen
• Few intermediate drusen(63-124 𝜇m)
• Mild RPE abnormalities
Intermediate AMD
(AREDS category 3)
• Numerous intermediate drusen
• At lease one large druse (≥ 125 𝜇m)
• Geographic atrophy of the RPE (Not involving the center of the fovea)
Advanced AMD
(AREDS category 4)
• Geographic atrophy of the RPEinvolving the center of the fovea
• Neovascular maculopathy:
• CNV (pathologic angiogenesisfrom the choroidal vasculature extending the a defect in Bruch’s membrane
• Serous/hemorrhagic detachement of NSR/RPE
• Retinal hard exudates
• Subretinal/sub-RPEfibrovascular proliferation
• Disciform scar
CLASSIFICATION6
6. Age-related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report number 8. Arch Ophthalmol 2001;119:1417-36
No AMD
(AREDS category 1)
• Control group
• No or few small drusen (< 63𝜇m)
Early AMD
(AREDS category 2)
• Multiple small drusen
• Few intermediate drusen(63-124 𝜇m)
• Mild RPE abnormalities
Intermediate AMD
(AREDS category 3)
• Numerous intermediate drusen
• At lease one large druse (≥ 125 𝜇m)
• Geographic atrophy of the RPE (Not involving the center of the fovea)
Advanced AMD
(AREDS category 4)
• Geographic atrophy of the RPEinvolving the center of the fovea
• Neovascular maculopathy:
• CNV (pathologic angiogenesisfrom the choroidal vasculature extending the a defect in Bruch’s membrane
• Serous/hemorrhagic detachement of NSR/RPE
• Retinal hard exudates
• Subretinal/sub-RPEfibrovascular proliferation
• Disciform scar
“Guidelines For The Management of AMD”
NATURAL HISTORY
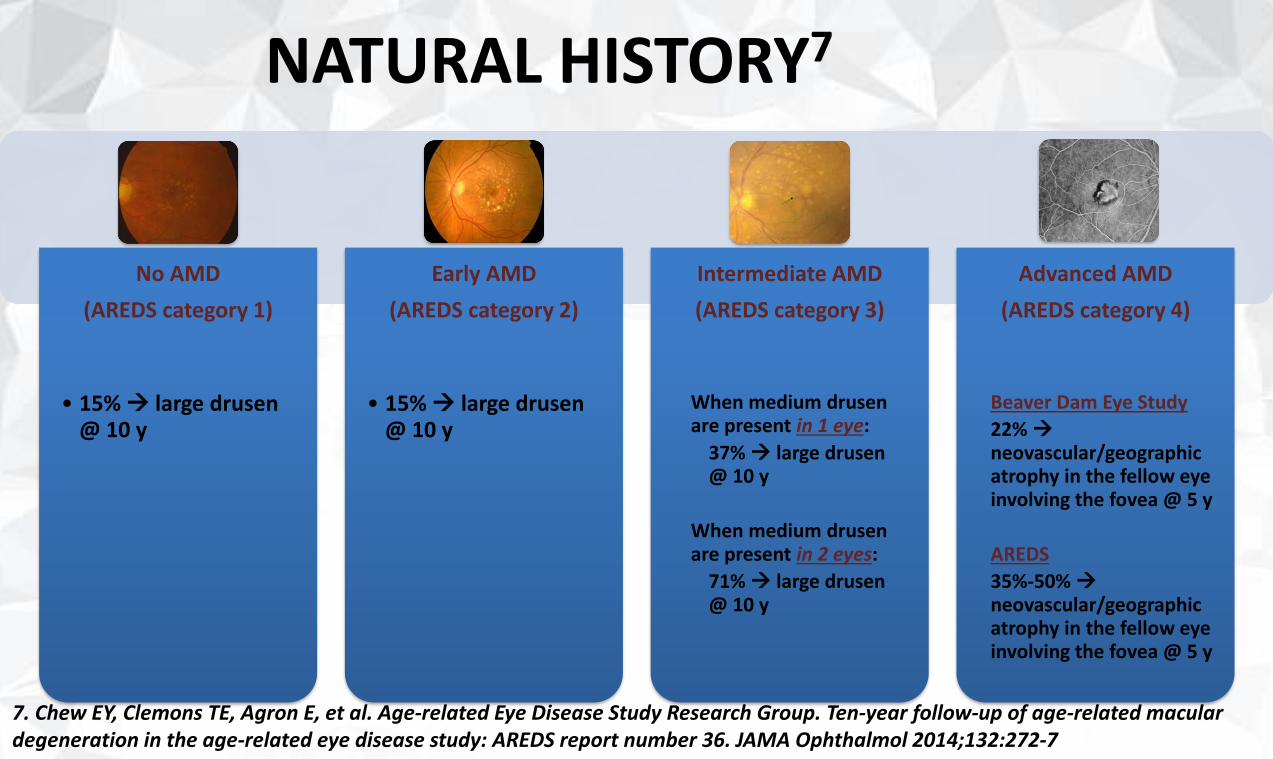
NATURAL HISTORY7
7. Chew EY, Clemons TE, Agron E, et al. Age-related Eye Disease Study Research Group. Ten-year follow-up of age-related macular degeneration in the age-related eye disease study: AREDS report number 36. JAMA Ophthalmol 2014;132:272-7
No AMD
(AREDS category 1)
• 15% large drusen@ 10 y
Early AMD
(AREDS category 2)
• 15% large drusen@ 10 y
Intermediate AMD
(AREDS category 3)
When medium drusenare present in 1 eye:
37% large drusen@ 10 y
When medium drusenare present in 2 eyes:
71% large drusen@ 10 y
Advanced AMD
(AREDS category 4)
Beaver Dam Eye Study
22%
neovascular/geographic atrophy in the fellow eye involving the fovea @ 5 y
AREDS
35%-50% neovascular/geographic atrophy in the fellow eye involving the fovea @ 5 y
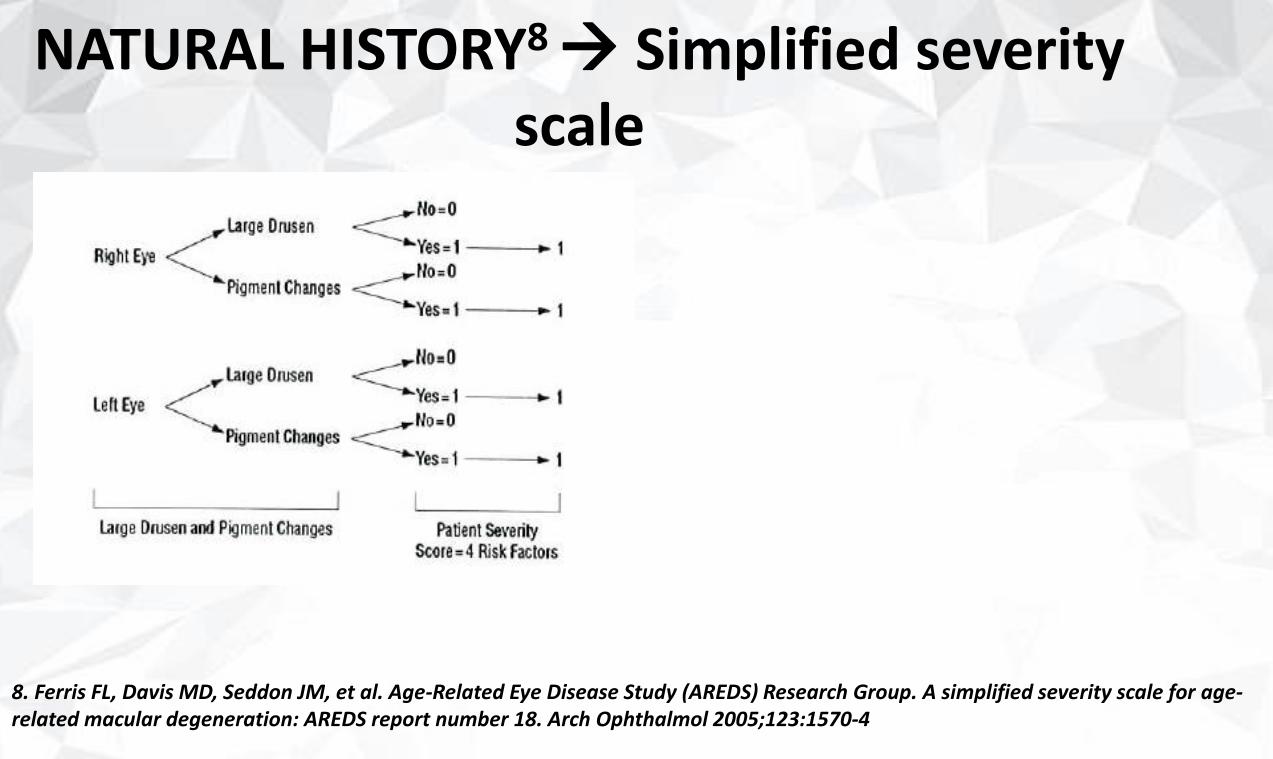
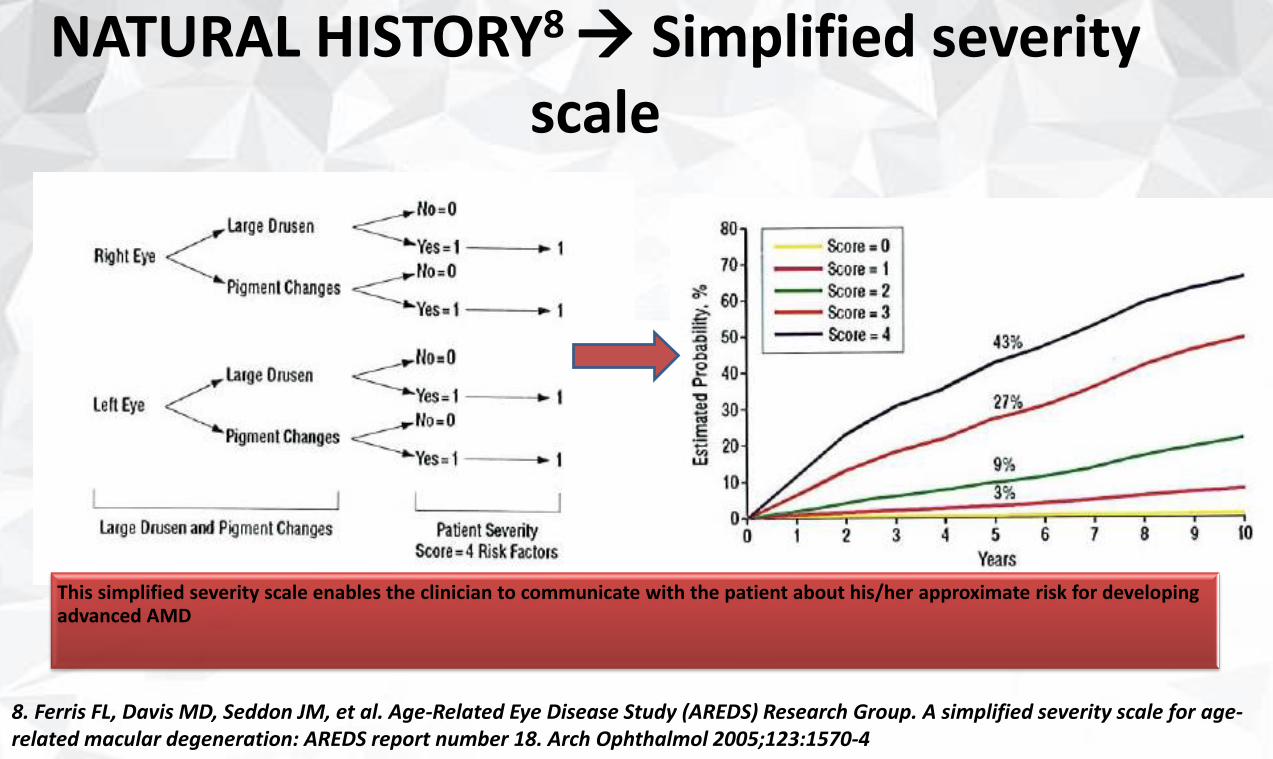
NATURAL HISTORY8 Simplified severity
scale
8. Ferris FL, Davis MD, Seddon JM, et al. Age-Related Eye Disease Study (AREDS) Research Group. A simplified severity scale for age-related macular degeneration: AREDS report number 18. Arch Ophthalmol 2005;123:1570-4
NATURAL HISTORY8 Simplified severity
scale
8. Ferris FL, Davis MD, Seddon JM, et al. Age-Related Eye Disease Study (AREDS) Research Group. A simplified severity scale for age-related macular degeneration: AREDS report number 18. Arch Ophthalmol 2005;123:1570-4
This simplified severity scale enables the clinician to communicate with the patient about his/her approximate risk for developingadvanced AMD
“Guidelines For The Management of AMD”
RATIONALE FOR TREATMENT
“Guidelines For The Management of AMD”
RATIONALE FOR TREATMENT
✓ Prospective randomized controlled clinical trials support the use of antioxidant vitamins and minerals for:• slowing the progression to later stages of AMD• Decreasing the load of other modalities of treatment
✓ In 2017, there is no proven therapy to prevent or treat geographicatrophy
“Guidelines For The Management of AMD”
TREATMENT MODALITIES

Visual Rehabilitation

Life Style Modification
ANTI-OXIDENTS
• Vitamins and Minerals
• Lutein/Zeaxanthin
• Omega -3 Fatty Acids
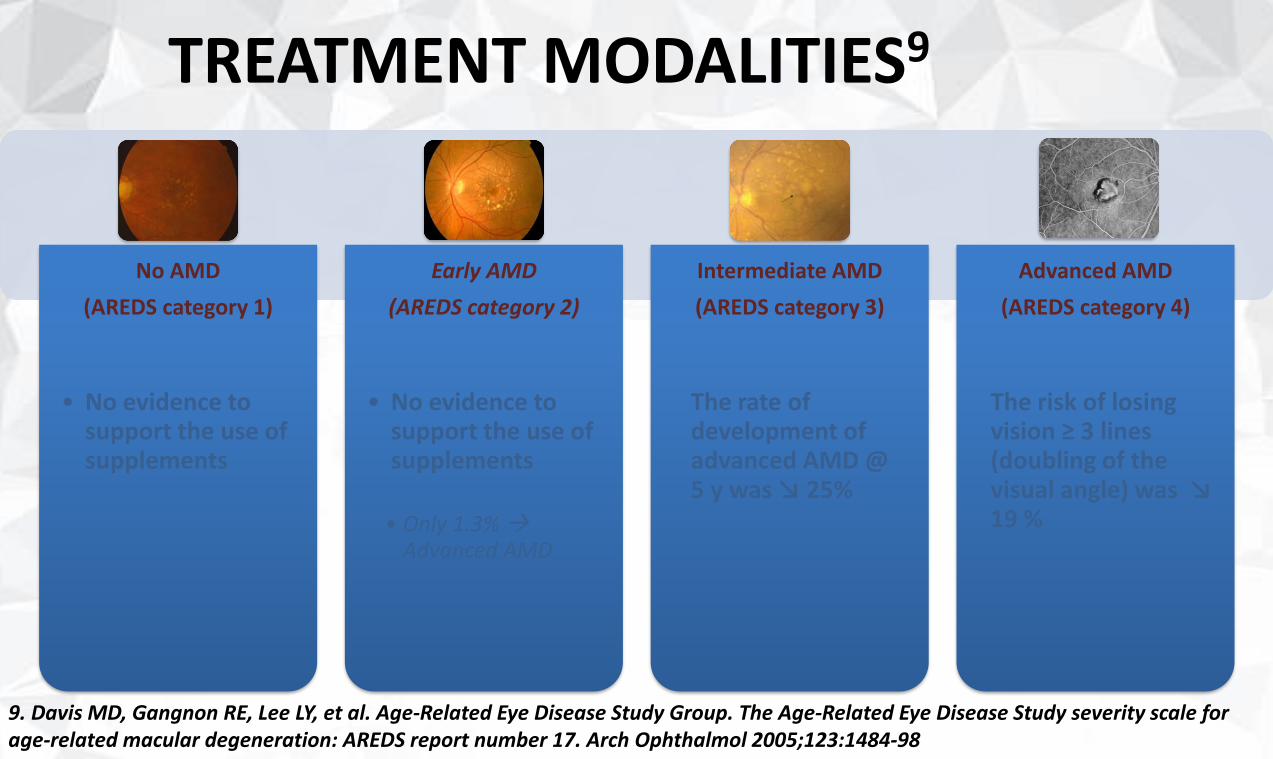
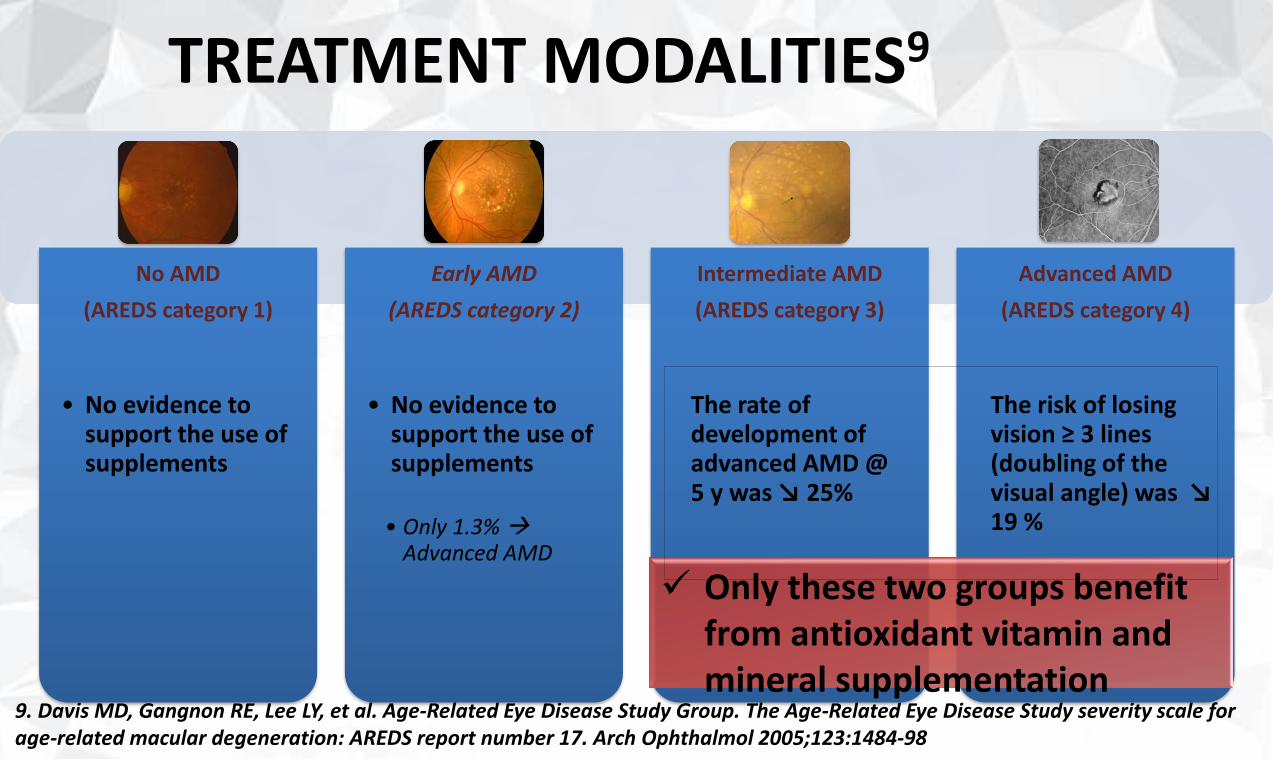
TREATMENT MODALITIES9
9. Davis MD, Gangnon RE, Lee LY, et al. Age-Related Eye Disease Study Group. The Age-Related Eye Disease Study severity scale for age-related macular degeneration: AREDS report number 17. Arch Ophthalmol 2005;123:1484-98
No AMD
(AREDS category 1)
• No evidence to support the use of supplements
Early AMD
(AREDS category 2)
• No evidence to support the use of supplements
• Only 1.3% Advanced AMD
Intermediate AMD
(AREDS category 3)
The rate of development of advanced AMD @ 5 y was ↘ 25%
Advanced AMD
(AREDS category 4)
The risk of losing vision ≥ 3 lines (doubling of the visual angle) was ↘ 19 %
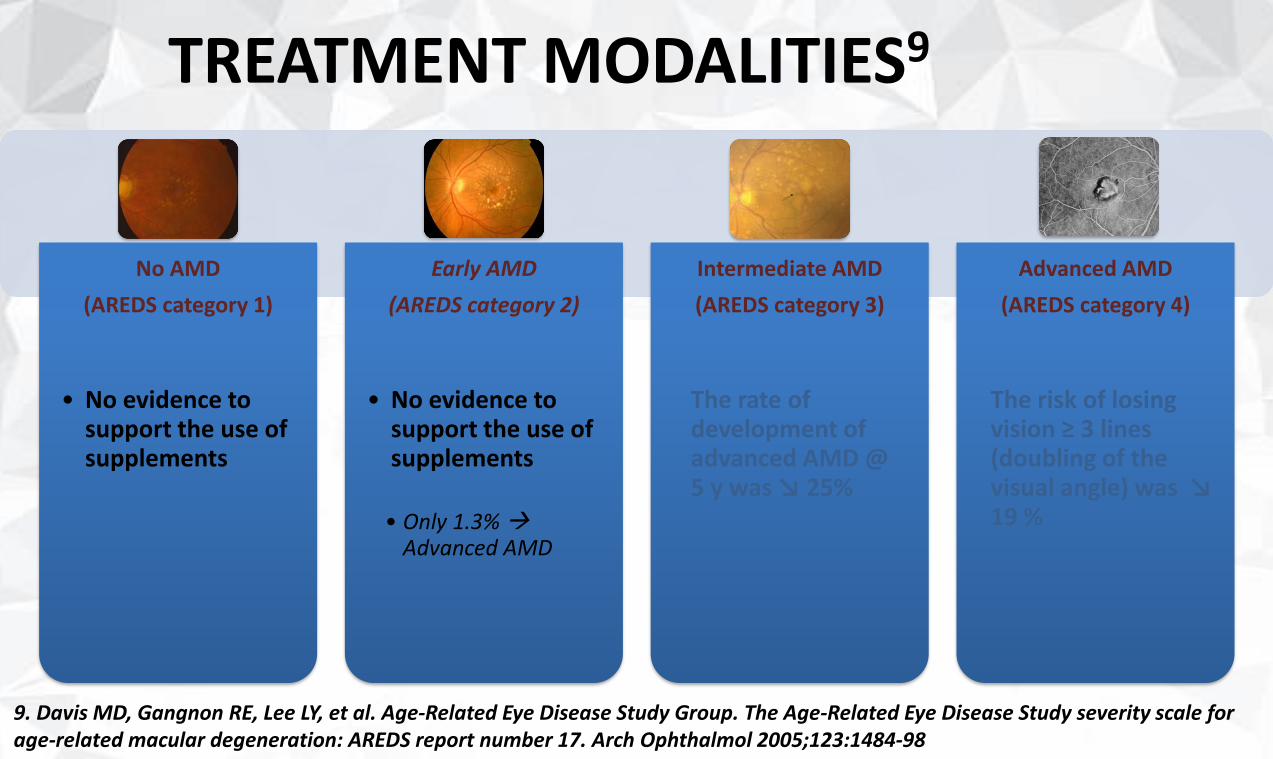
TREATMENT MODALITIES9
9. Davis MD, Gangnon RE, Lee LY, et al. Age-Related Eye Disease Study Group. The Age-Related Eye Disease Study severity scale for age-related macular degeneration: AREDS report number 17. Arch Ophthalmol 2005;123:1484-98
No AMD
(AREDS category 1)
• No evidence to support the use of supplements
Early AMD
(AREDS category 2)
• No evidence to support the use of supplements
• Only 1.3% Advanced AMD
Intermediate AMD
(AREDS category 3)
The rate of development of advanced AMD @ 5 y was ↘ 25%
Advanced AMD
(AREDS category 4)
The risk of losing vision ≥ 3 lines (doubling of the visual angle) was ↘ 19 %
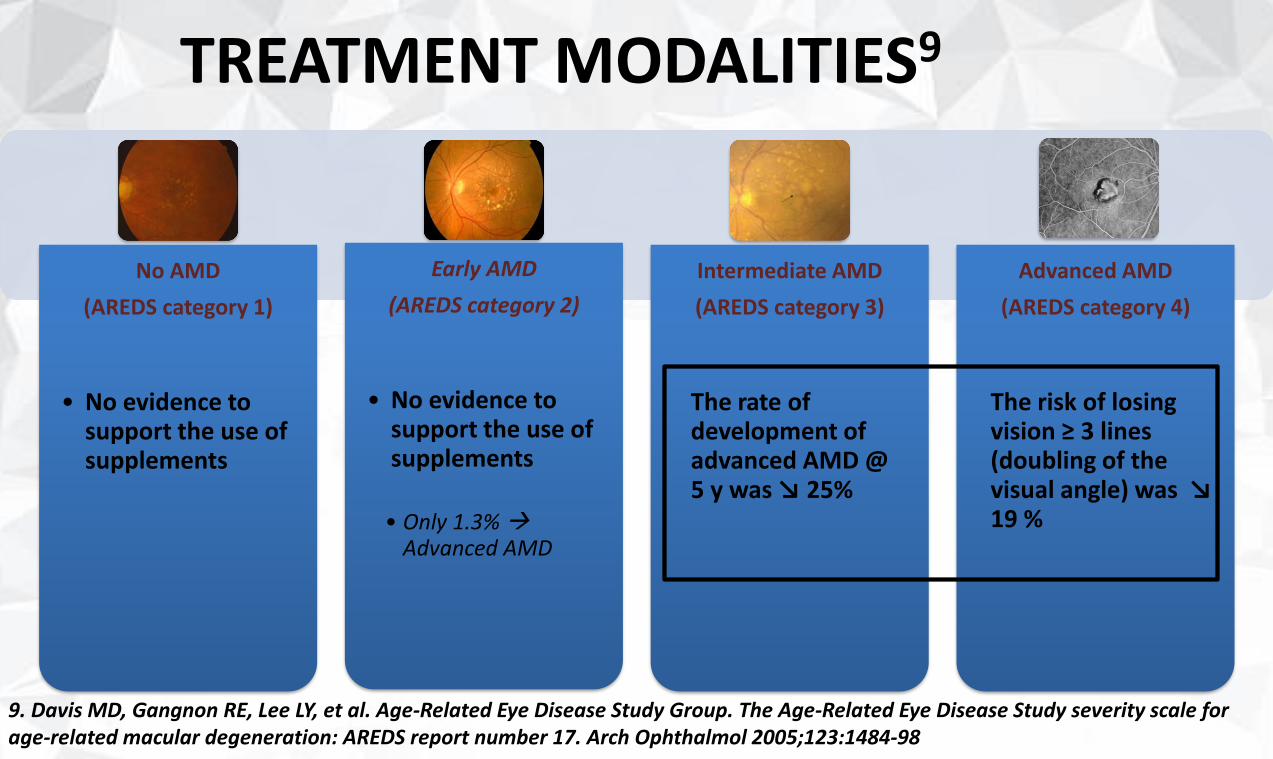
TREATMENT MODALITIES9
9. Davis MD, Gangnon RE, Lee LY, et al. Age-Related Eye Disease Study Group. The Age-Related Eye Disease Study severity scale for age-related macular degeneration: AREDS report number 17. Arch Ophthalmol 2005;123:1484-98
No AMD
(AREDS category 1)
• No evidence to support the use of supplements
Early AMD
(AREDS category 2)
• No evidence to support the use of supplements
• Only 1.3% Advanced AMD
Intermediate AMD
(AREDS category 3)
The rate of development of advanced AMD @ 5 y was ↘ 25%
Advanced AMD
(AREDS category 4)
The risk of losing vision ≥ 3 lines (doubling of the visual angle) was ↘ 19 %
TREATMENT MODALITIES9
9. Davis MD, Gangnon RE, Lee LY, et al. Age-Related Eye Disease Study Group. The Age-Related Eye Disease Study severity scale for age-related macular degeneration: AREDS report number 17. Arch Ophthalmol 2005;123:1484-98
No AMD
(AREDS category 1)
• No evidence to support the use of supplements
Early AMD
(AREDS category 2)
• No evidence to support the use of supplements
• Only 1.3% Advanced AMD
Intermediate AMD
(AREDS category 3)
The rate of development of advanced AMD @ 5 y was ↘ 25%
Advanced AMD
(AREDS category 4)
The risk of losing vision ≥ 3 lines (doubling of the visual angle) was ↘ 19 %
✓ Only these two groups benefitfrom antioxidant vitamin and mineral supplementation
TREATMENT MODALITIES
10. Heier JS et al. VIEW 1 and VIEW 2 Study group. Intravitreal aflibercept in wet age-related macular degeneration. Ophthalmology 2012;119:2537-4811. Schmidt-Erfurth U et al. Perspectives on verteporfin therapy combined with intravitreal corticosteroids. Arch Ophthalmol 2006;124:561-312. Kasier et al. DENALI Study Group. Verteporfin plus ranibizumab for choroidal neovascularization in AMD: 12 months results. Ophthalmology 2012;119:1001-1013. Larsen M et al. MONT BLANC Study Group. Verteporfin plus ranibizumab for choroidal neovascularization in AMD: 12 months results. Ophthalmology 2012;119:992-100014. Koh et al. EVEREST Study: Efficacy and safety of verteporfin PDT in combination with ranibizumab or alone versus ranibizumab monotherapy in patints with symptomatic macular polypoidal choroidal vasculopathy. Retina 2012;32:1453-64
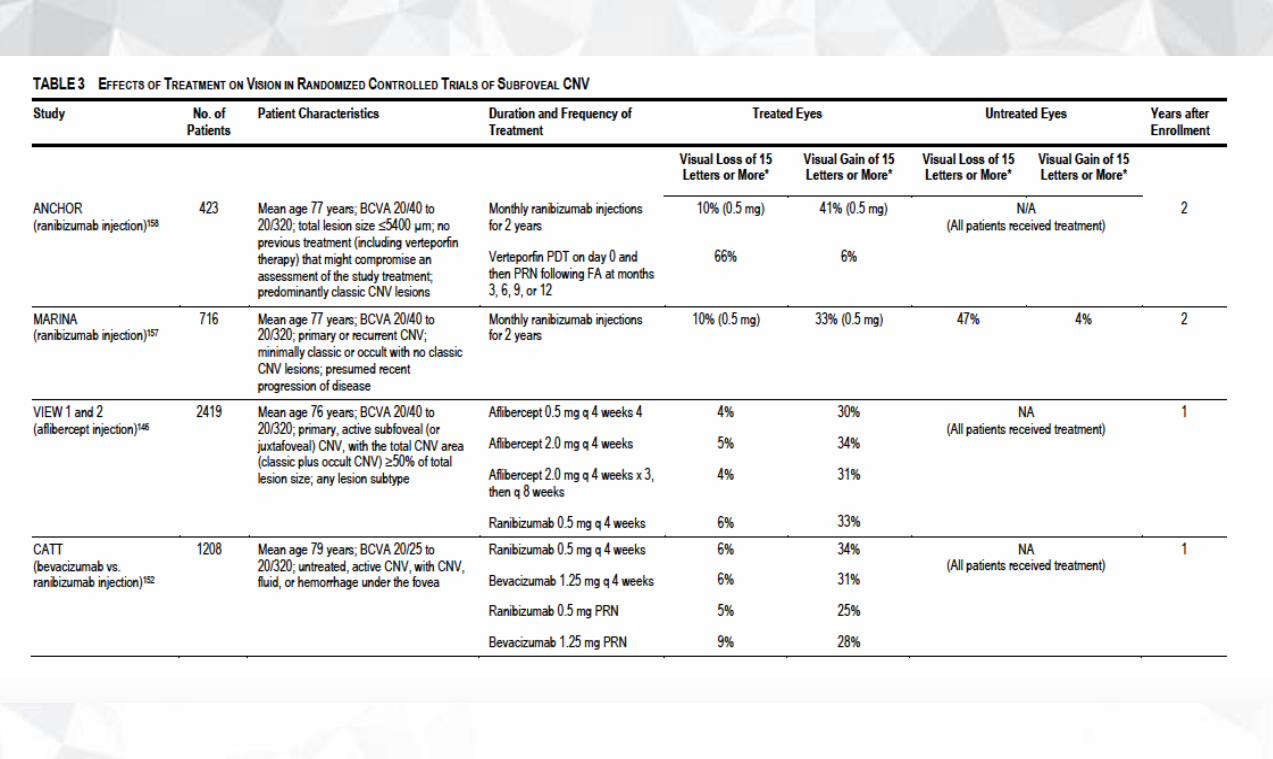
• Anti-VEGF (Aflibercept, Ranibizumab, Bevacizumab) are currently the preferred therapy to treat neovascular AMD over PDT and laser photocoagulation10
• This applies for subfoveal, juxtafoveal and extrafoveal lesions10
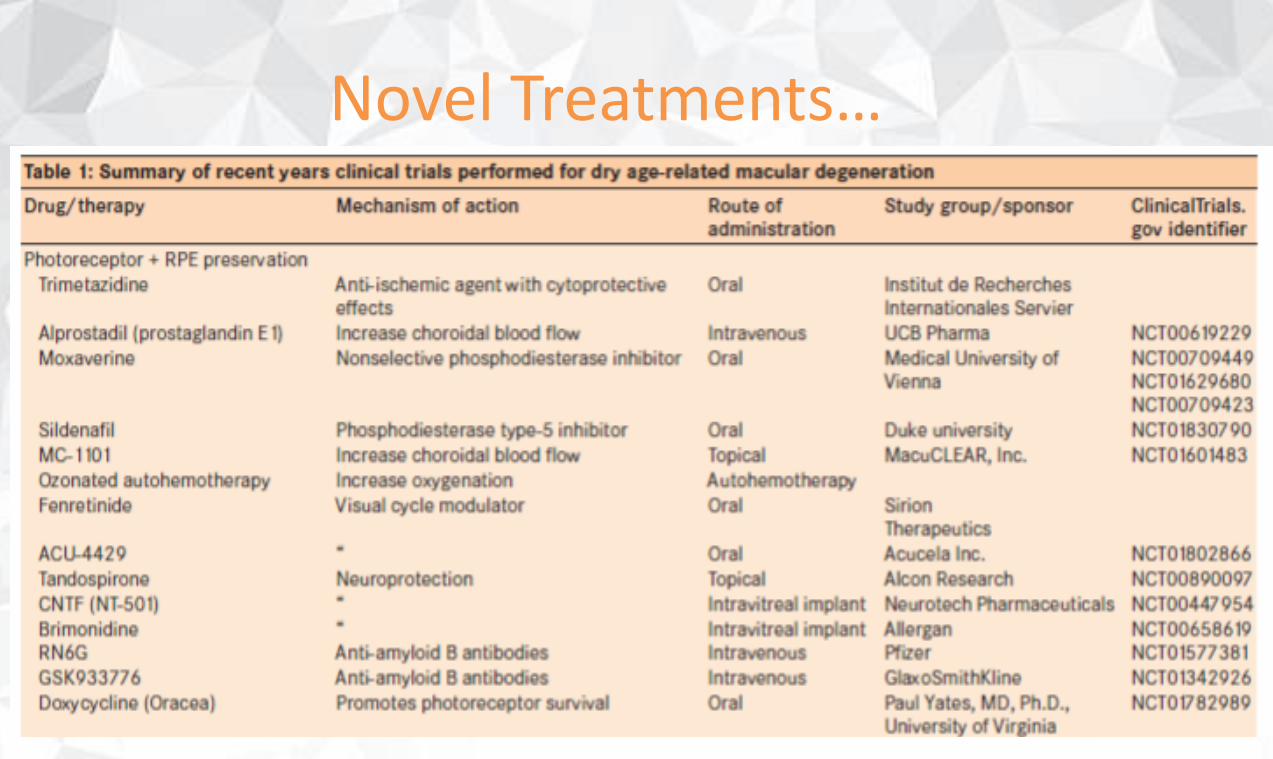
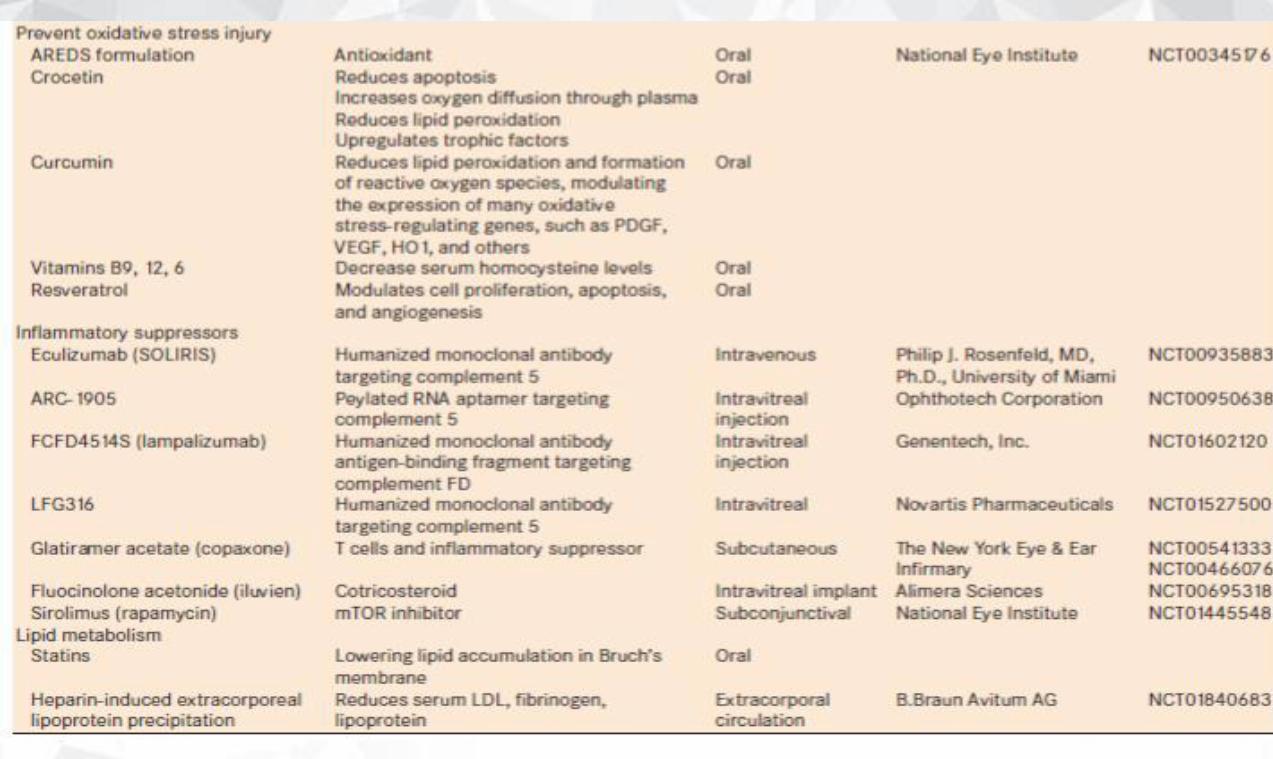
Novel Treatments…
“Guidelines For The Management of AMD”
MANAGEMENT
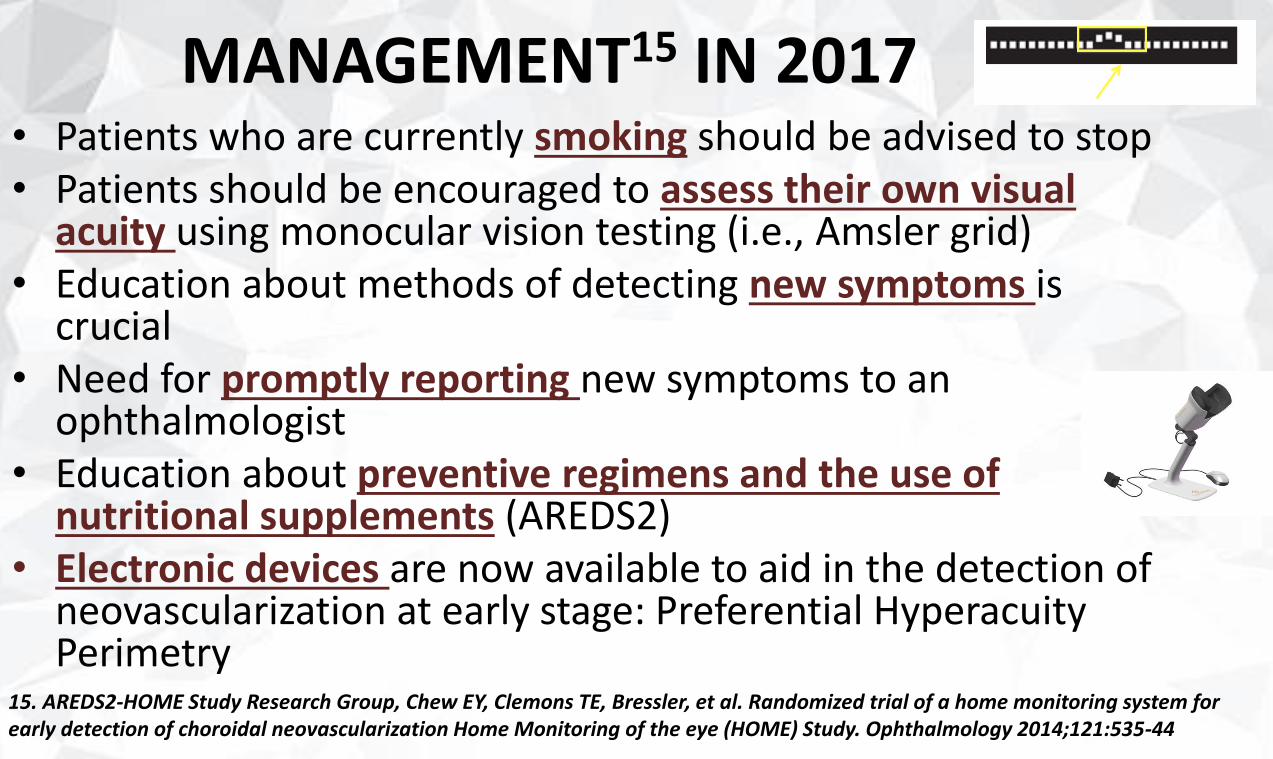
MANAGEMENT15 IN 2017
15. AREDS2-HOME Study Research Group, Chew EY, Clemons TE, Bressler, et al. Randomized trial of a home monitoring system for early detection of choroidal neovascularization Home Monitoring of the eye (HOME) Study. Ophthalmology 2014;121:535-44
• Patients who are currently smoking should be advised to stop• Patients should be encouraged to assess their own visual
acuity using monocular vision testing (i.e., Amsler grid)• Education about methods of detecting new symptoms is
crucial • Need for promptly reporting new symptoms to an
ophthalmologist • Education about preventive regimens and the use of
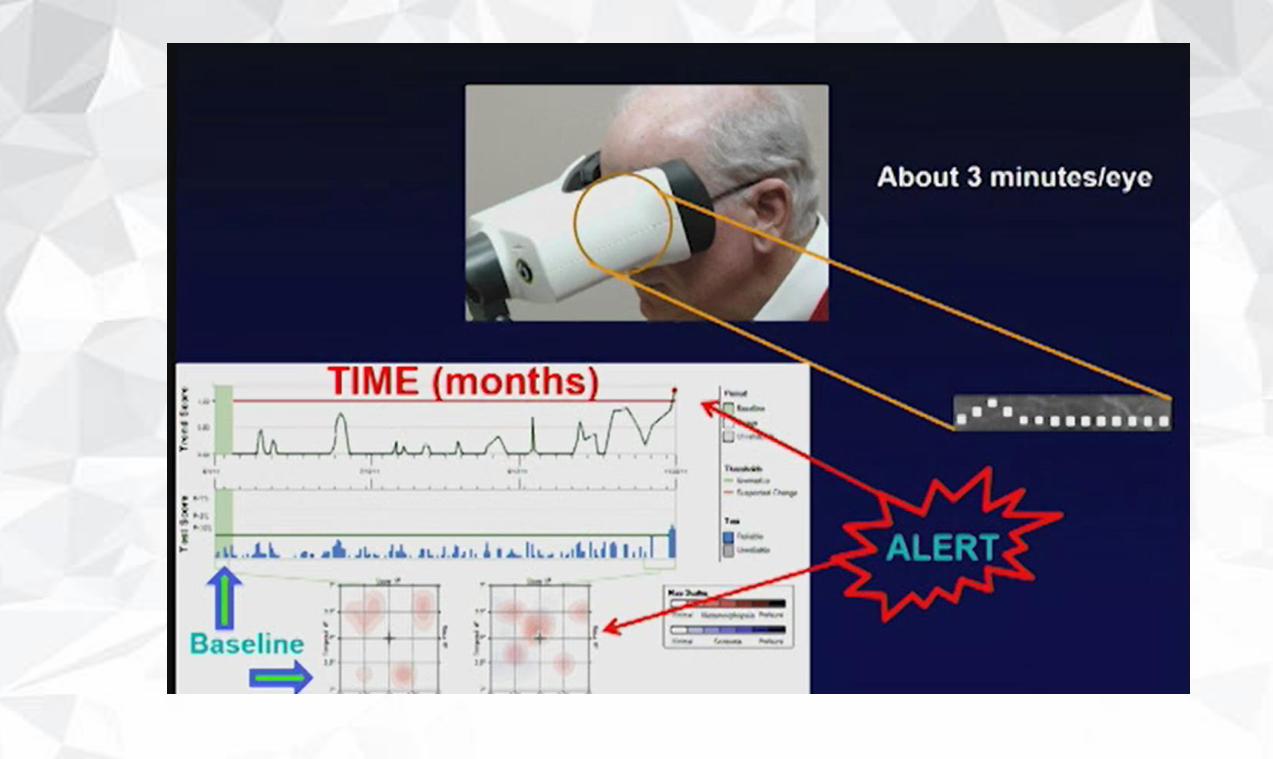
nutritional supplements (AREDS2)• Electronic devices are now available to aid in the detection of
neovascularization at early stage: Preferential HyperacuityPerimetry
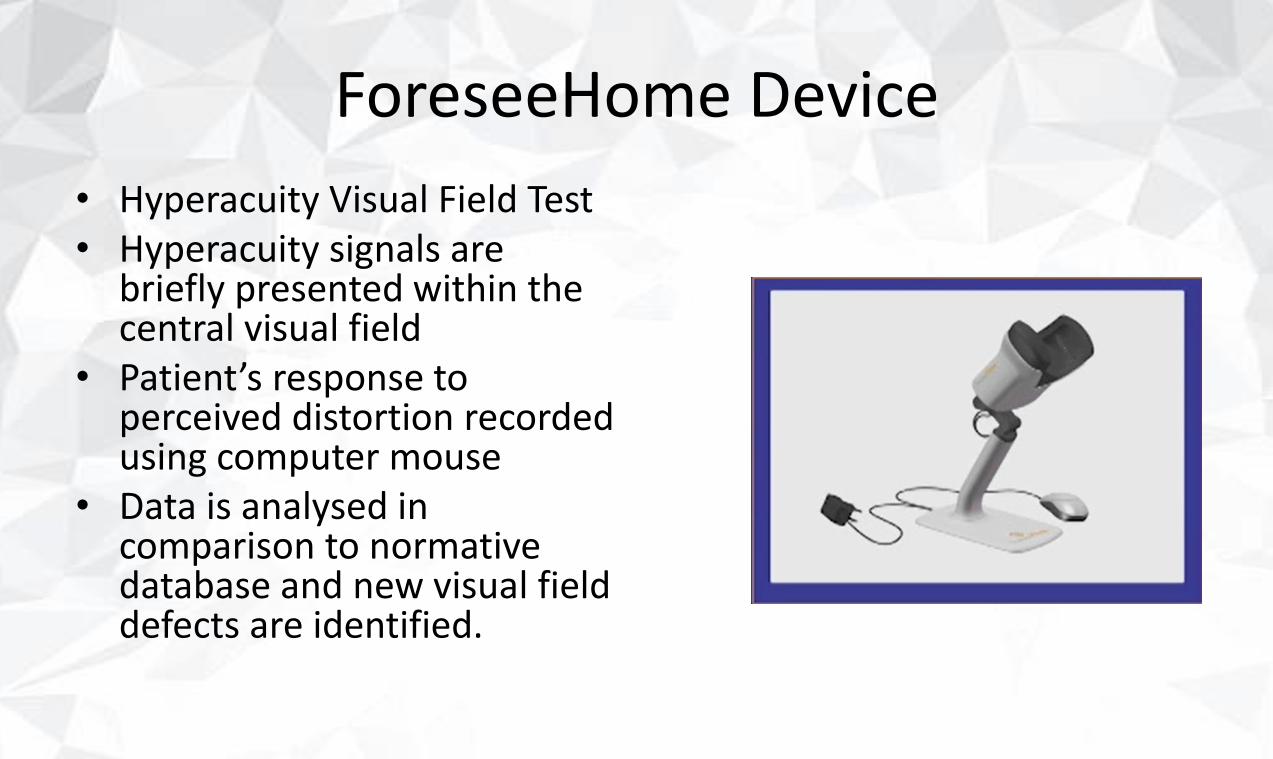
ForeseeHome Device
• Hyperacuity Visual Field Test• Hyperacuity signals are
briefly presented within the central visual field
• Patient’s response to perceived distortion recorded using computer mouse
• Data is analysed in comparison to normative database and new visual field defects are identified.
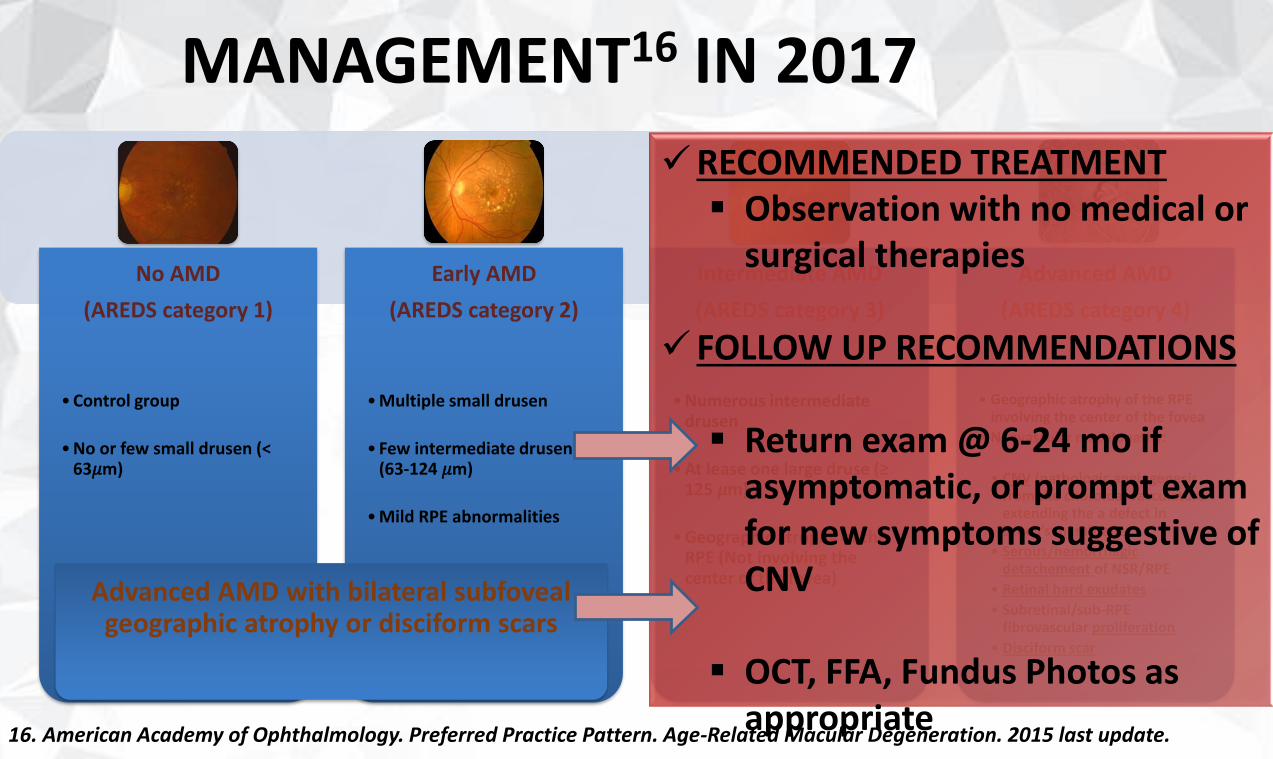
MANAGEMENT16 IN 2017
No AMD
(AREDS category 1)
• Control group
• No or few small drusen (< 63𝜇m)
Early AMD
(AREDS category 2)
• Multiple small drusen
• Few intermediate drusen(63-124 𝜇m)
• Mild RPE abnormalities
Intermediate AMD
(AREDS category 3)
• Numerous intermediate drusen
• At lease one large druse (≥ 125 𝜇m)
• Geographic atrophy of the RPE (Not involving the center of the fovea)
Advanced AMD
(AREDS category 4)
• Geographic atrophy of the RPEinvolving the center of the fovea
• Neovascular maculopathy:
• CNV (pathologic angiogenesisfrom the choroidal vasculature extending the a defect in Bruch’s membrane
• Serous/hemorrhagic detachement of NSR/RPE
• Retinal hard exudates
• Subretinal/sub-RPEfibrovascular proliferation
• Disciform scar
✓RECOMMENDED TREATMENT▪ Observation with no medical or
surgical therapies
✓ FOLLOW UP RECOMMENDATIONS
▪ Return exam @ 6-24 mo if asymptomatic, or prompt exam for new symptoms suggestive of CNV
▪ OCT, FFA, Fundus Photos as appropriate
Advanced AMD with bilateral subfoveal geographic atrophy or disciform scars
16. American Academy of Ophthalmology. Preferred Practice Pattern. Age-Related Macular Degeneration. 2015 last update.
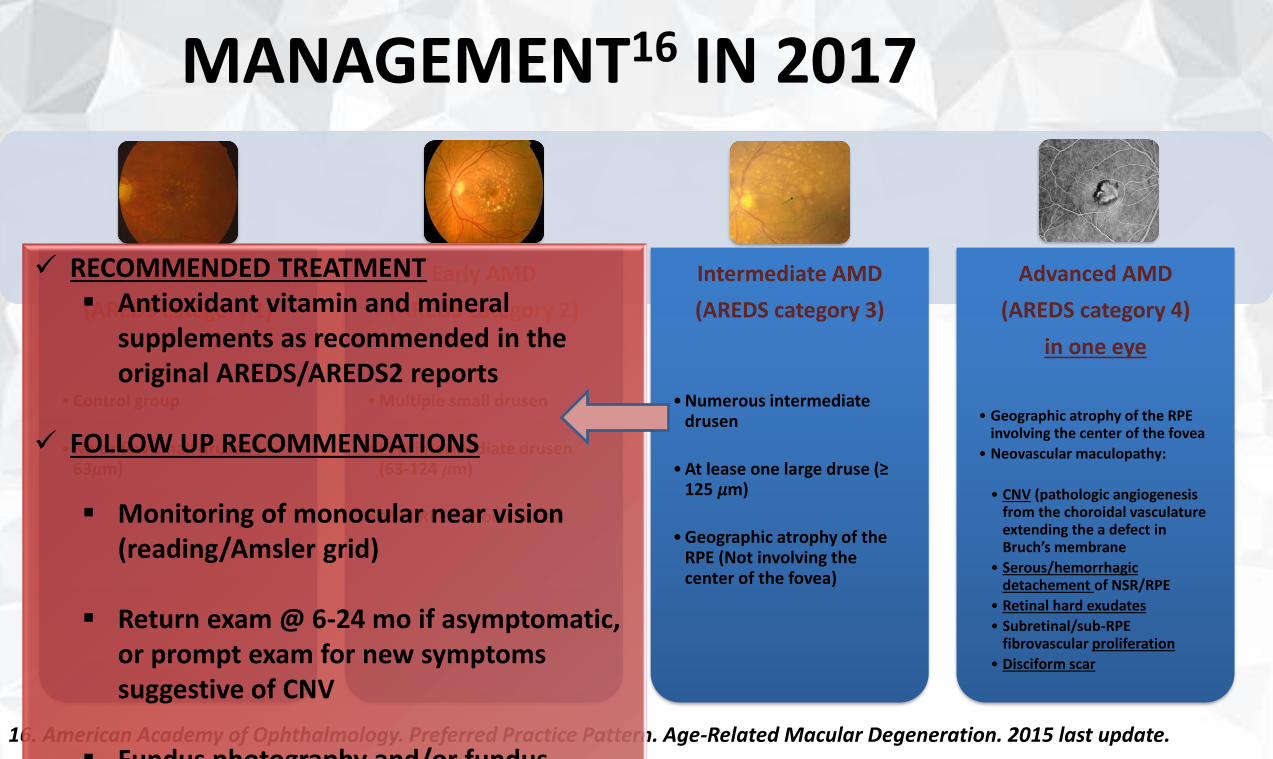
MANAGEMENT16 IN 2017
16. American Academy of Ophthalmology. Preferred Practice Pattern. Age-Related Macular Degeneration. 2015 last update.
No AMD
(AREDS category 1)
• Control group
• No or few small drusen (< 63𝜇m)
Early AMD
(AREDS category 2)
• Multiple small drusen
• Few intermediate drusen(63-124 𝜇m)
• Mild RPE abnormalities
Intermediate AMD
(AREDS category 3)
• Numerous intermediate drusen
• At lease one large druse (≥ 125 𝜇m)
• Geographic atrophy of the RPE (Not involving the center of the fovea)
Advanced AMD
(AREDS category 4)
in one eye
• Geographic atrophy of the RPEinvolving the center of the fovea
• Neovascular maculopathy:
• CNV (pathologic angiogenesisfrom the choroidal vasculature extending the a defect in Bruch’s membrane
• Serous/hemorrhagic detachement of NSR/RPE
• Retinal hard exudates
• Subretinal/sub-RPEfibrovascular proliferation
• Disciform scar
✓ RECOMMENDED TREATMENT▪ Antioxidant vitamin and mineral
supplements as recommended in the original AREDS/AREDS2 reports
✓ FOLLOW UP RECOMMENDATIONS
▪ Monitoring of monocular near vision (reading/Amsler grid)
▪ Return exam @ 6-24 mo if asymptomatic, or prompt exam for new symptomssuggestive of CNV
▪ Fundus photography and/or fundus
“Guidelines For The Management of AMD”
CONCLUSION
Conclusion• AMD is the leading cause of irreversible visual impairment in the developed
countries
• Early detection and treatment are crucial to help preserve patients’ quality of live
• Smoking cessation is strongly recommended
• The use of nutritional supplements (AREDS2), when indicated, ↘ rate of development of advanced AMD by 25% in 5 years
• All patients should be educated about the prognosis of the disease and the potential value of treatment as appropriate for their visual and functional status
• Patients can be educated that while central visual loss is common, total visual loss is extremely rare hence the role of low vision aid
Conclusion• AMD is the leading cause of irreversible visual impairment in the developed
countries
• Early detection and treatment are crucial to help preserve patients’ quality of live
• Smoking cessation is strongly recommended
• The use of nutritional supplements (AREDS2), when indicated, ↘ rate of development of advanced AMD by 25% in 5 years
• All patients should be educated about the prognosis of the disease and the potential value of treatment as appropriate for their visual and functional status
• Patients can be educated that while central visual loss is common, total visual loss is extremely rare hence the role of low vision aid
Conclusion• AMD is the leading cause of irreversible visual impairment in the developed
countries
• Early detection and treatment are crucial to help preserve patients’ quality of live
• Smoking cessation is strongly recommended
• The use of nutritional supplements (AREDS2), when indicated, ↘ rate of development of advanced AMD by 25% in 5 years
• All patients should be educated about the prognosis of the disease and the potential value of treatment as appropriate for their visual and functional status
• Patients can be educated that while central visual loss is common, total visual loss is extremely rare hence the role of low vision aid
Conclusion• AMD is the leading cause of irreversible visual impairment in the developed
countries
• Early detection and treatment are crucial to help preserve patients’ quality of live
• Smoking cessation is strongly recommended
• The use of nutritional supplements (AREDS2), when indicated, ↘ rate of development of advanced AMD by 25% in 5 years
• All patients should be educated about the prognosis of the disease and the potential value of treatment as appropriate for their visual and functional status
• Patients can be educated that while central visual loss is common, total visual loss is extremely rare hence the role of low vision aid
Conclusion• AMD is the leading cause of irreversible visual impairment in the developed
countries
• Early detection and treatment are crucial to help preserve patients’ quality of live
• Smoking cessation is strongly recommended
• The use of nutritional supplements (AREDS2), when indicated, ↘ rate of development of advanced AMD by 25% in 5 years
• All patients should be educated about the prognosis of the disease and the potential value of treatment as appropriate for their visual and functional status
• Patients can be educated that while central visual loss is common, total visual loss is extremely rare hence the role of low vision aid
Conclusion• AMD is the leading cause of irreversible visual impairment in the developed
countries
• Early detection and treatment are crucial to help preserve patients’ quality of live
• Smoking cessation is strongly recommended
• The use of nutritional supplements (AREDS2), when indicated, ↘ rate of development of advanced AMD by 25% in 5 years
• All patients should be educated about the prognosis of the disease and the potential value of treatment as appropriate for their visual and functional status
• Patients can be educated that while central visual loss is common, total visual loss is extremely rare hence the role of low vision aid