long-term care reform in slovenia: financing perspective - eva zver, slovenia
TRANSCRIPT

LONG-TERM CARE REFORM IN SLOVENIA – FINANCING PERSPECTIVE
E VA Z V E R , I N S T I T U T E O F M A C R O E C O N O M I C A N A LY S I S A N D
D E V E L O P M E N T D AV O R DOMINKUŠ , M I N I S T R Y O F L A B O U R , FA M I LY, S O C I A L A F FA I R S
A N D E Q UA L O P P O R T U N I T I E S
O E C D , 4 T H M E E T I N G O F T H E J O I N T N E T W O R K O N F I S C A L S U S T A I N A B I L I T Y O F H E A L T H S Y S T E M S
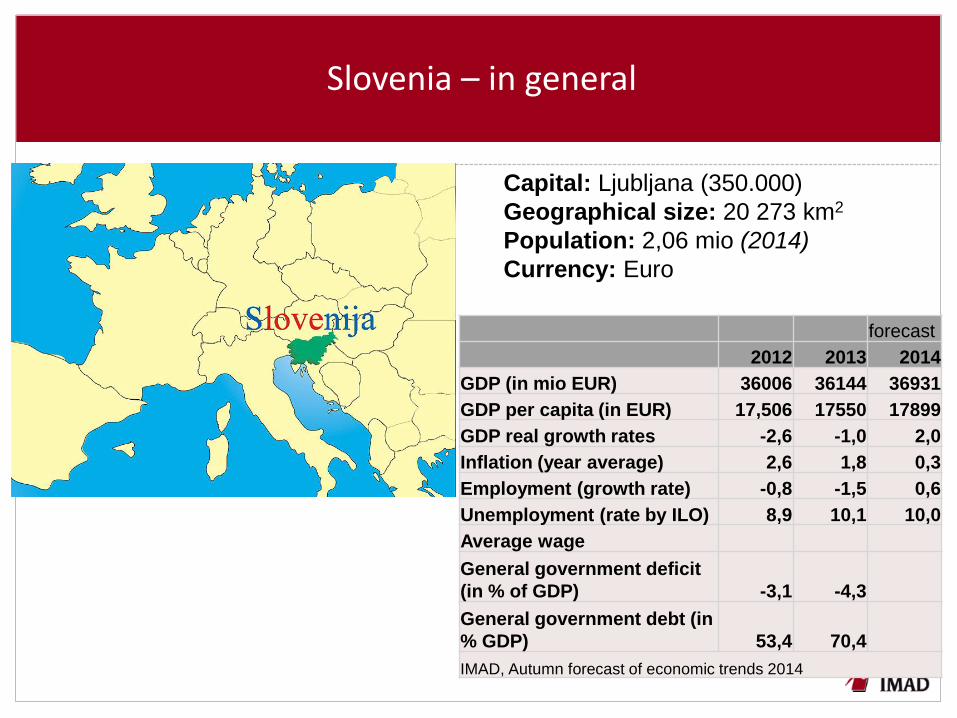
Slovenia – in general
Capital: Ljubljana (350.000)
Geographical size: 20 273 km2
Population: 2,06 mio (2014)
Currency: Euro
forecast
2012 2013 2014
GDP (in mio EUR) 36006 36144 36931
GDP per capita (in EUR) 17,506 17550 17899
GDP real growth rates -2,6 -1,0 2,0
Inflation (year average) 2,6 1,8 0,3
Employment (growth rate) -0,8 -1,5 0,6
Unemployment (rate by ILO) 8,9 10,1 10,0
Average wage
General government deficit
(in % of GDP) -3,1 -4,3
General government debt (in
% GDP) 53,4 70,4
IMAD, Autumn forecast of economic trends 2014
Overview of presentation
1. LTC reform in Slovenia – reasons behind the need for a reform
2. Current state of health and LTC financing
3. Information on the envisaged LTC reform
4. Information on the proposed changes of HC and LTC financing
The focus of presentation is on two questions:
- Why do we have to link LTC and health care funding reform?
- What could be a solution to the problem of additional public (tax)
resources needed to finance LTC in Slovenia?
LTC reform – reasons behind the need for a reform
• Demographic reasons
• Fiscal sustainability reasons
• Social reasons (poverty and social exclusion among the elderly)
• Health reasons (Healthy life years are low; impact on savings in
health expenditure)
• Reasons deriving from the existing system, its imbalances and
fragmentation
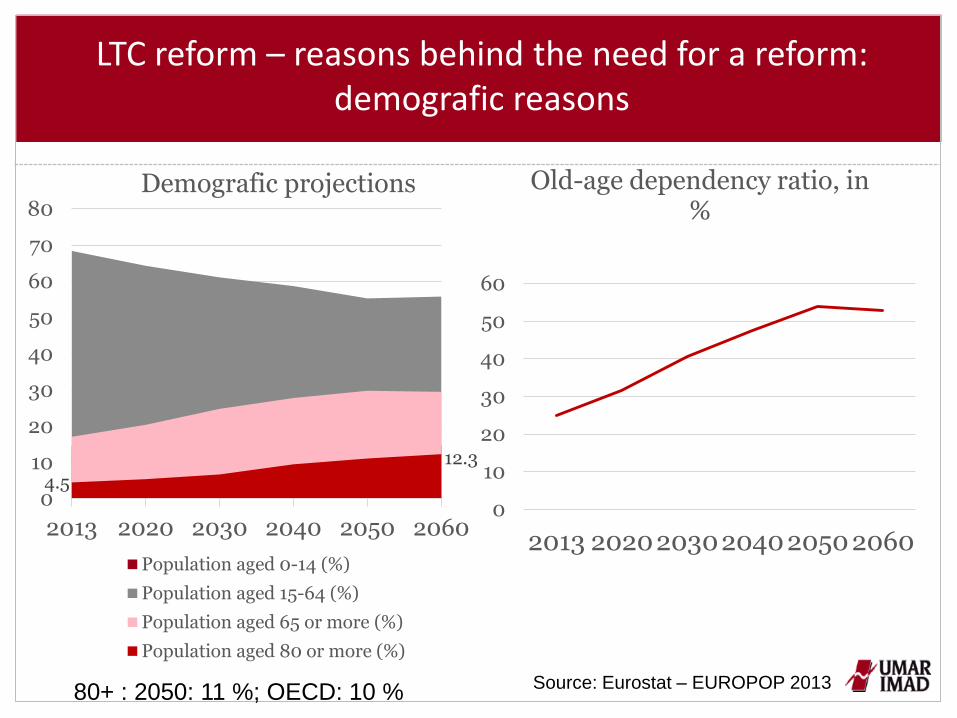
LTC reform – reasons behind the need for a reform: demografic reasons
Source: Eurostat – EUROPOP 2013
0
10
20
30
40
50
60
2013 2020203020402050 2060
Old-age dependency ratio, in %
4.5
12.3
0
10
20
30
40
50
60
70
80
2013 2020 2030 2040 2050 2060
Demografic projections
Population aged 0-14 (%)
Population aged 15-64 (%)
Population aged 65 or more (%)
Population aged 80 or more (%)
80+ : 2050: 11 %; OECD: 10 %
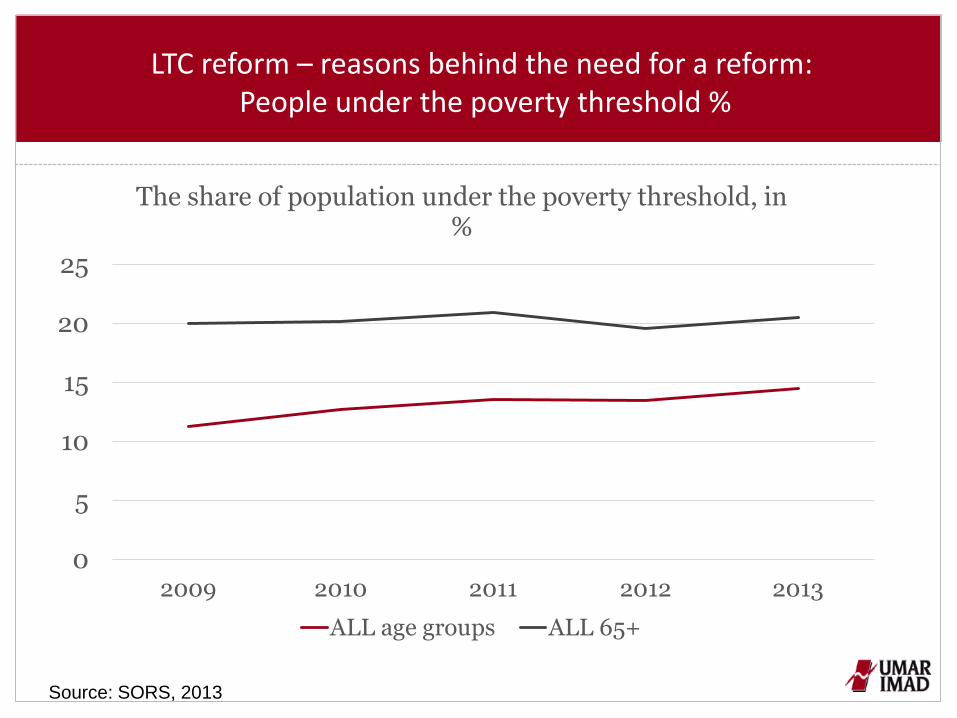
LTC reform – reasons behind the need for a reform: People under the poverty threshold %
Source: SORS, 2013
0
5
10
15
20
25
2009 2010 2011 2012 2013
The share of population under the poverty threshold, in %
ALL age groups ALL 65+
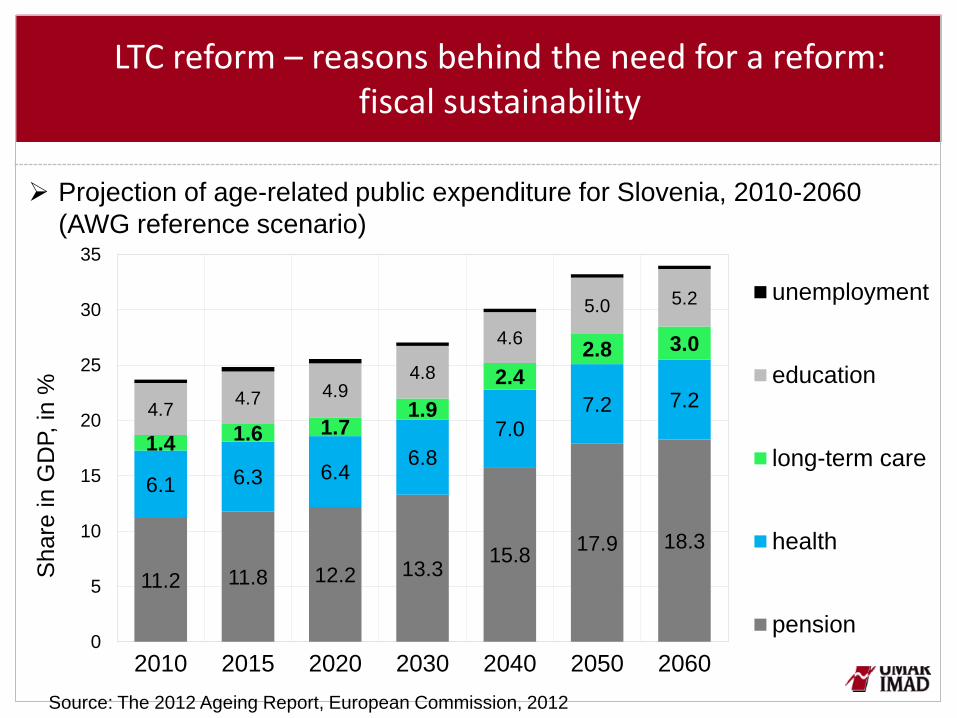
LTC reform – reasons behind the need for a reform: fiscal sustainability
Projection of age-related public expenditure for Slovenia, 2010-2060
(AWG reference scenario)
11.2 11.8 12.2 13.3 15.8
17.9 18.3
6.1 6.3 6.4 6.8
7.0 7.2 7.2
1.4 1.6 1.7
1.9
2.4
2.8 3.0
4.7 4.7 4.9
4.8
4.6
5.0 5.2
0
5
10
15
20
25
30
35
2010 2015 2020 2030 2040 2050 2060
Share
in G
DP, in
%
unemployment
education
long-term care
health
pension
Source: The 2012 Ageing Report, European Commission, 2012

LTC reform – reasons behind the need for a reform: health
50.052.054.056.058.060.062.064.066.068.070.072.074.076.078.080.082.084.086.088.090.0
50
52
54
56
58
60
62
64
66
68
70
72
74
Slo
va
k R
ep
.
Slo
ve
nia
Esto
nia
Fin
lan
d
La
tvia
Ge
rma
ny
Ro
ma
nia
Lith
ua
nia
Po
rtu
ga
l
Hu
ng
ary
De
nm
ark
Po
land
Ne
the
rla
nd
s
Au
str
ia
Ita
ly
EU
-28
Czech
Re
p.
Cro
atia
Fra
nce
Cypru
s
Bu
lgaria
Un
ite
d…
Gre
ece
Be
lgiu
m
Spain
Lu
xe
mb
ou
rg
Ire
lan
d
Sw
itze
rla
nd
Ice
lan
d
Sw
ed
en
No
rwa
y
Ma
lta
Share
, in
%
num
be
r of years
HLY - women HLY - men Ratio HLY/Life expectancy
Source: Eurostat Database; calculations by IMAD
Healthy life years at birth and ratio of HLY to life expectancy
C U R R E N T LY N O U N I F O R M S Y S T E M O F LT C :
• LT C b e n e f i t s i n k i n d a n d c a s h - b e n e f i t s a r e p r o v i d e d a n d
f i n a n c e d w i t h i n :
- health care system,
- social and parental protection systems,
- pension and disability system
• B e n e f i t s i n k i n d :
• Institutional care is prevailing
• Lack of community based services
• Underdeveloped home based services and integrated health/social care
• B e n e f i t s i n c a s h :
- not related to comparable needs
- different levels of benefits related to specific legislation
- not means tested
N o u n i f i e d e n t r y p o i n t a n d n o u n i f i e d n e e d s a s s e s s m e n t
LTC reform – reasons behind the need for a reform: Imbalances and fragmentation of current LTC provision
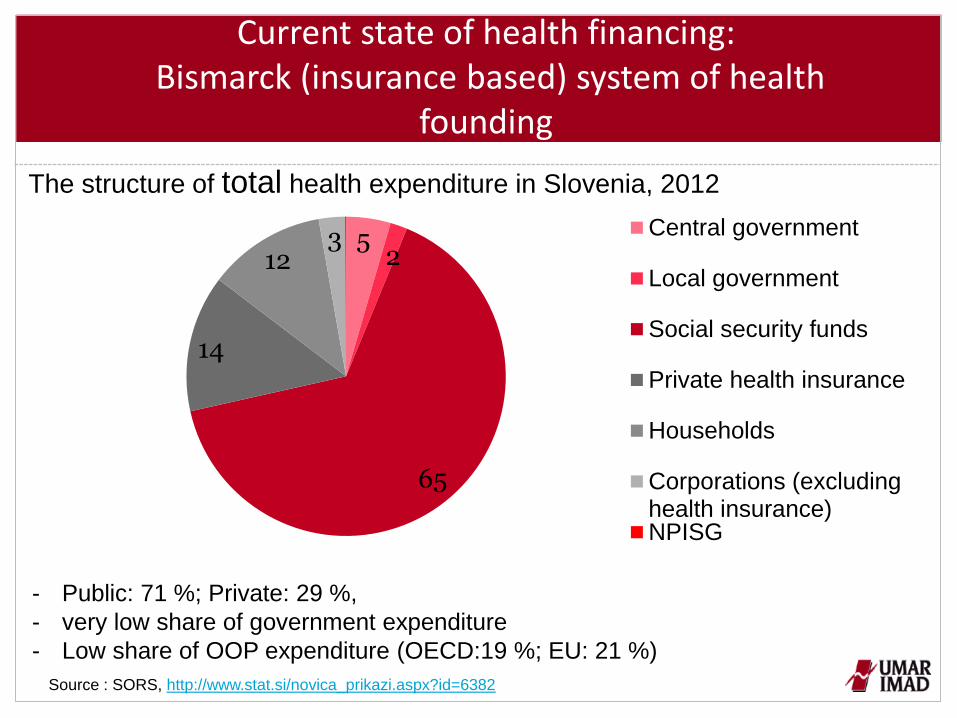
Current state of health financing: Bismarck (insurance based) system of health
founding
The structure of total health expenditure in Slovenia, 2012
Source : SORS, http://www.stat.si/novica_prikazi.aspx?id=6382
5 2
65
14
12 3 Central government
Local government
Social security funds
Private health insurance
Households
Corporations (excludinghealth insurance)NPISG
- Public: 71 %; Private: 29 %,
- very low share of government expenditure
- Low share of OOP expenditure (OECD:19 %; EU: 21 %)
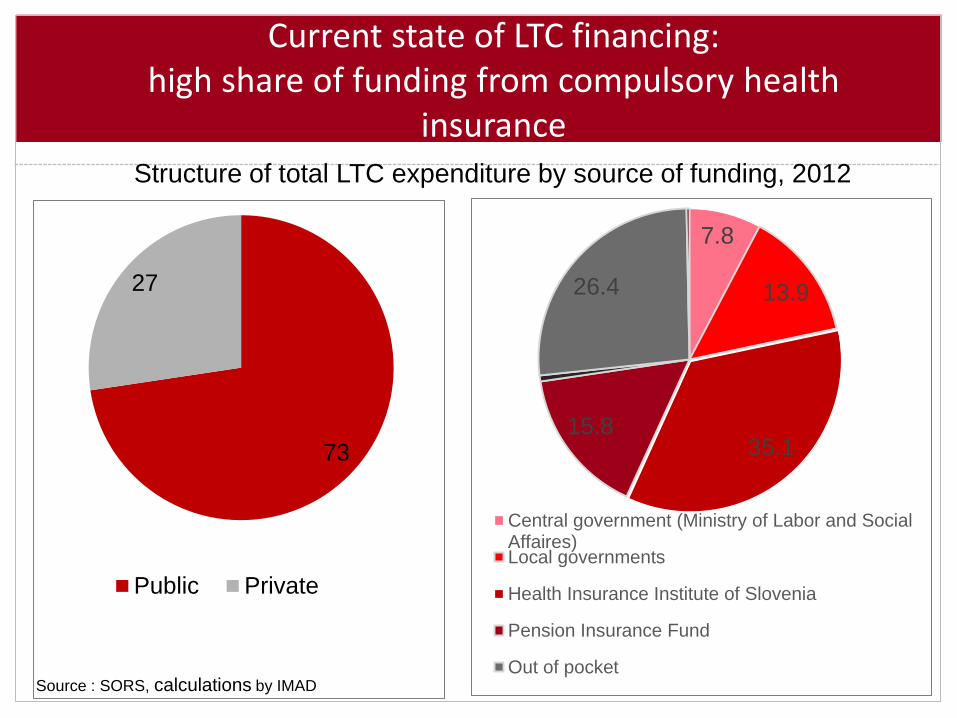
7.8
13.9
35.1 15.8
26.4
Central government (Ministry of Labor and SocialAffaires)Local governments
Health Insurance Institute of Slovenia
Pension Insurance Fund
Out of pocket
Current state of LTC financing: high share of funding from compulsory health
insurance
73
27
Public Private
Structure of total LTC expenditure by source of funding, 2012
Source : SORS, calculations by IMAD
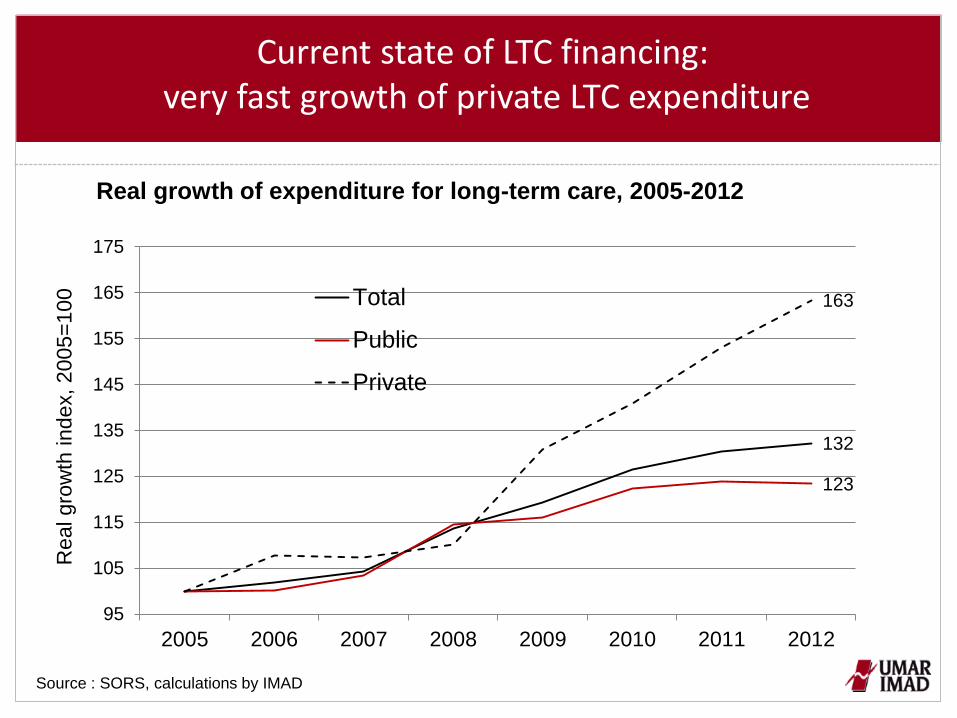
Current state of LTC financing: very fast growth of private LTC expenditure
132
123
163
95
105
115
125
135
145
155
165
175
2005 2006 2007 2008 2009 2010 2011 2012
Real gro
wth
index, 2005=
100
Total
Public
Private
Real growth of expenditure for long-term care, 2005-2012
Source : SORS, calculations by IMAD
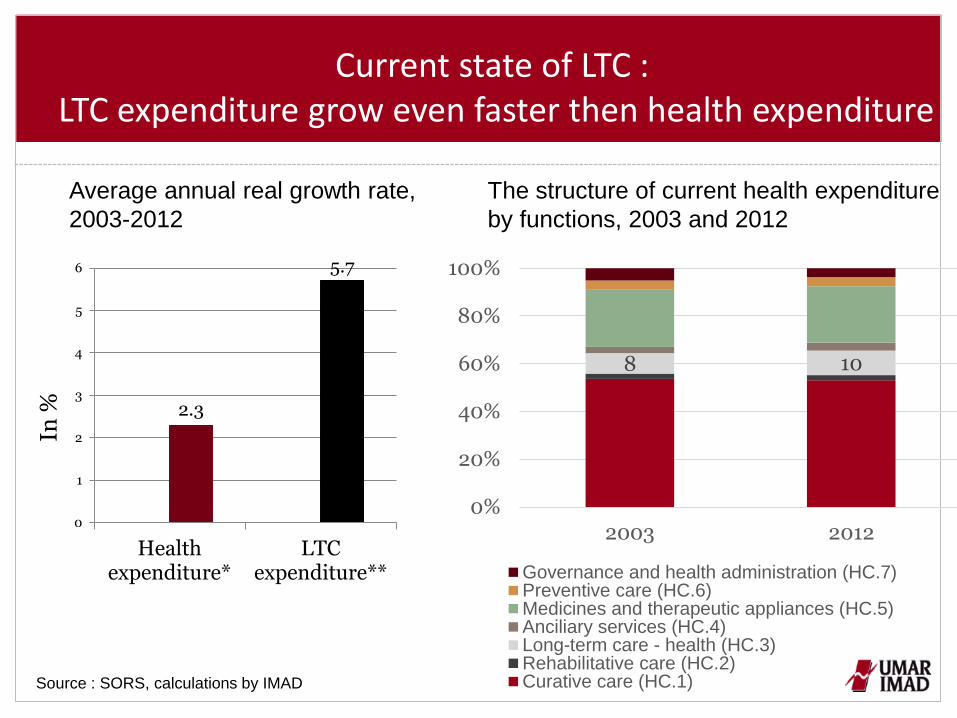
The structure of current health expenditure
by functions, 2003 and 2012
8 10
0%
20%
40%
60%
80%
100%
2003 2012
Governance and health administration (HC.7)Preventive care (HC.6)Medicines and therapeutic appliances (HC.5)Anciliary services (HC.4)Long-term care - health (HC.3)Rehabilitative care (HC.2)Curative care (HC.1)
2.3
5.7
0
1
2
3
4
5
6
Healthexpenditure*
LTCexpenditure**
In %
Average annual real growth rate,
2003-2012
Current state of LTC : LTC expenditure grow even faster then health expenditure
Source : SORS, calculations by IMAD
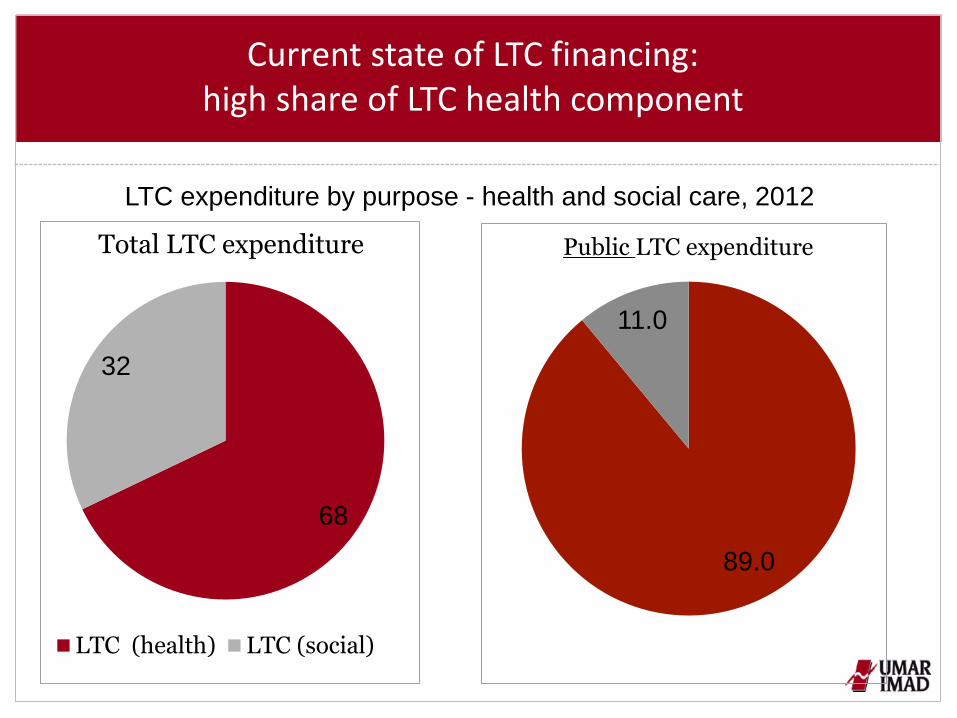
Current state of LTC financing: high share of LTC health component
68
32
LTC (health) LTC (social)
Total LTC expenditure
89.0
11.0
Public LTC expenditure
LTC expenditure by purpose - health and social care, 2012
Current situation – conclution
Key challenges for LTC reform in Slovenia:
- Demographic aging is faster than the average of EU and OECD
countries
- Fiscal sustainability problem is serious
- High share of disabled/dependent – low indicator of Healthy Life Years
- High growth of private LTC expenditure
- Underdeveloped home care and integrated care
- Underdeveloped ICT, preventive and rehabilitative services (important
to lower the costs of health LTC services)
Information on the envisaged LTC reform
Preparation of the LTC reform started 10 years ago!
Since than several drafts of legislative act were prepared
Since 2013 recommendations from EC and OECD
In 2014: developed official statistics on LTC with detailed information
on LTC expenditure and recipients
Since 2014 better collaboration of the Ministry of Health with the
Ministry of Labor, Familiy, Social Affaires and Equal Opportunities
Information on the envisaged LTC reform: planned future financing of LTC services and rights
The starting point of reform: a need for LTC as a (new) social risk
Ensuring a sustainable financing system that needs to be adaptable
and predictable in times
To keep three pilars of funding:
A compulsory public LTC insurance, based on the merged parts of
the existing health and disability/pension insurance currently
intended for LTC
Tax based financing (including the introduction of new special public
source (tax/levy) for LTC provision)
Out of pocket co-payments (and optional voluntary private
insurance)
Major issue still remains…
Where to find additional public resources to finance LTC under new
legislation ! (approx. 0,2 % of GDP)
- After the long period of crisis Slovenia is still facing a problem of
fiscal consolidation! It is not possible to get additional resources for
LTC reform from central or local budgets.
- Contribution rates to social security funds are already very high
- Dedicated tax/levy – the idea comes from the envisaged
health financing reform (proposed in the coalition agreement
of current government)
Information on the envisaged LTC reform

Source: SORS, Health expenditure and financing ( http://www.stat.si/novica_prikazi.aspx?id=6382)
5 2
65
14
12 3
Centralgovernment
Localgovernment
Socialsecurityfunds
Private healthinsurance
Households(OOP)
Other private(corporationsandnonprofit)
5 2
65
14
12 3
Centralgovernment
Localgovernment
Socialsecurityfunds
New publicsource(dedicatedtax?)
Households(OOP)
A replacement of complementary private health insurance with
new public source of funding (dedicated tax/levy ?)
- Very high user-charges even for some health-critical
services
- Currently it is urgent to buy private health insurance
because the risk for not having it is too high (95 % of
population with compulsory health insurance also have
private complementary health insurance)
- High operating administration costs of private health
insurance companies
- Flat rate premiums – no income solidarity
Key reasons for the proposed abolishment of the current
system of complementary private health insurance:
- It has to replace total amount of resources which are
currently collected by complementary private health
insurance premiums
- It should not burden the labour costs (the proposal is to set
up a tax on net personal income?)
- it should not burden only active population - has to be
obligatory also for pensioners (Important for sustainability
in a long-term)
- Income solidarity
Key features that are important for new public source of
health funding:
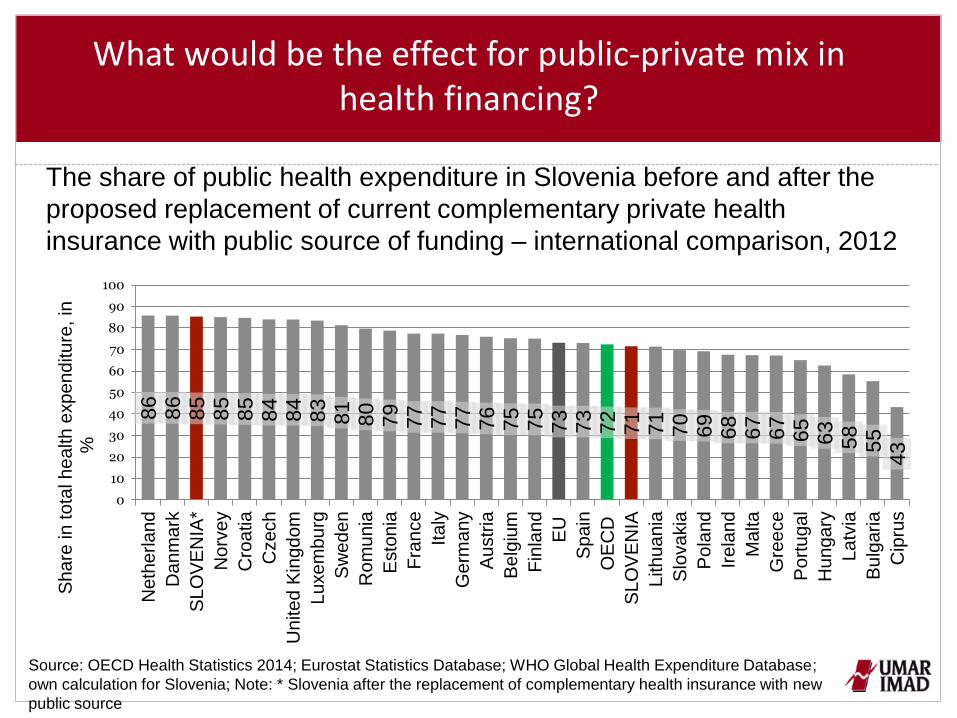
What would be the effect for public-private mix in health financing?
The share of public health expenditure in Slovenia before and after the
proposed replacement of current complementary private health
insurance with public source of funding – international comparison, 2012
Source: OECD Health Statistics 2014; Eurostat Statistics Database; WHO Global Health Expenditure Database;
own calculation for Slovenia; Note: * Slovenia after the replacement of complementary health insurance with new
public source
86
8
6
85
8
5
85
8
4
84
8
3
81
8
0
79
7
7
77
77
7
6
75
7
5
73
7
3
72
7
1
71
7
0
69
6
8
67
67
65
6
3
58
5
5
43
0
10
20
30
40
50
60
70
80
90
100
Ne
the
rla
nd
Da
nm
ark
SL
OV
EN
IA*
No
rve
y
Cro
atia
Czech
Un
ite
d K
ing
do
m
Lu
xe
mb
urg
Sw
ed
en
Ro
mu
nia
Esto
nia
Fra
nce
Ita
ly
Ge
rma
ny
Au
str
ia
Be
lgiu
m
Fin
lan
d
EU
Spain
OE
CD
SL
OV
EN
IA
Lith
ua
nia
Slo
va
kia
Po
land
Ire
lan
d
Ma
lta
Gre
ece
Po
rtu
ga
l
Hu
ng
ary
La
tvia
Bu
lgaria
Cip
rus
Share
in
to
tal h
ea
lth
exp
en
ditu
re, in
%
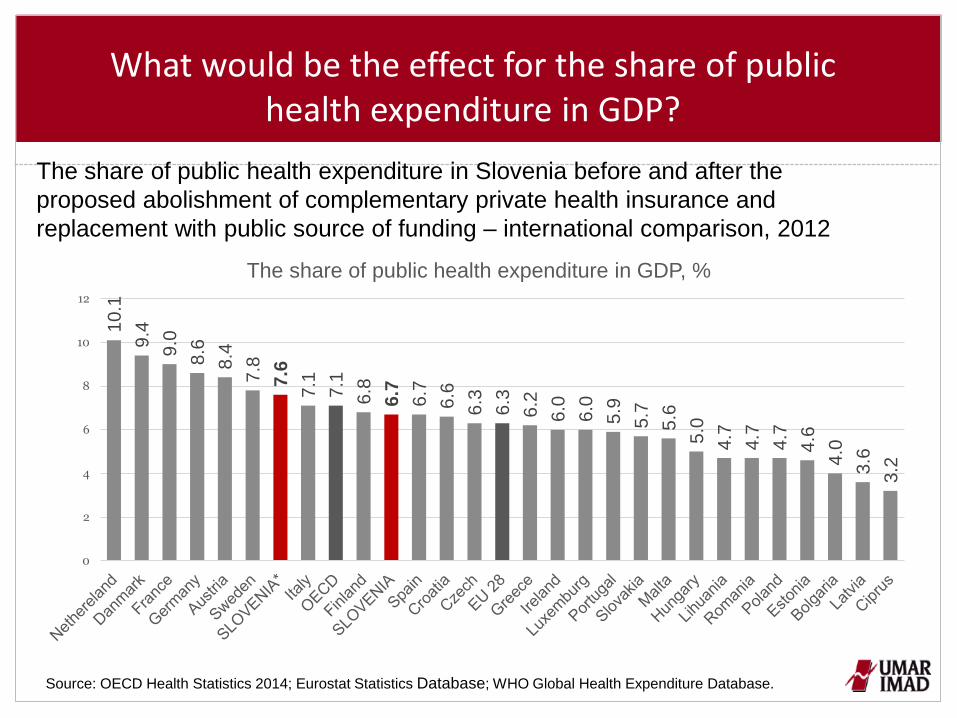
The share of public health expenditure in Slovenia before and after the
proposed abolishment of complementary private health insurance and
replacement with public source of funding – international comparison, 2012
Source: OECD Health Statistics 2014; Eurostat Statistics Database; WHO Global Health Expenditure Database.
What would be the effect for the share of public health expenditure in GDP?
10
.1
9.4
9.0
8.6
8.4
7.8
7.6
7.1
7.1
6.8
6.7
6.7
6.6
6.3
6.3
6.2
6.0
6.0
5.9
5.7
5.6
5.0
4.7
4.7
4.7
4.6
4.0
3.6
3.2
0
2
4
6
8
10
12
The share of public health expenditure in GDP, %
In the case of a replacement of current system of complementary health insurance
with a new public source of funding there would be some room to increase private
funding (at least for 0,2-0,5 % of GDP)
Possible options are:
To set up new (reasonable) user-charges
To set up co-payments (at least small co-payments on medicines and technical
appliances and for the first visit at the doctor)
Changing the scope of rights stemming from compulsory health insurance
Other options: (to set up the system of franchises)
Important:
- Taking into account the criteria of accessibility, efficiency and cost effectiveness
- Protection of certain groups of population
- Introducing the method of health technology assessment (HTA) to prevent
investments in inefficient procedures/treatments
There would be some room to increase private health expenditure…
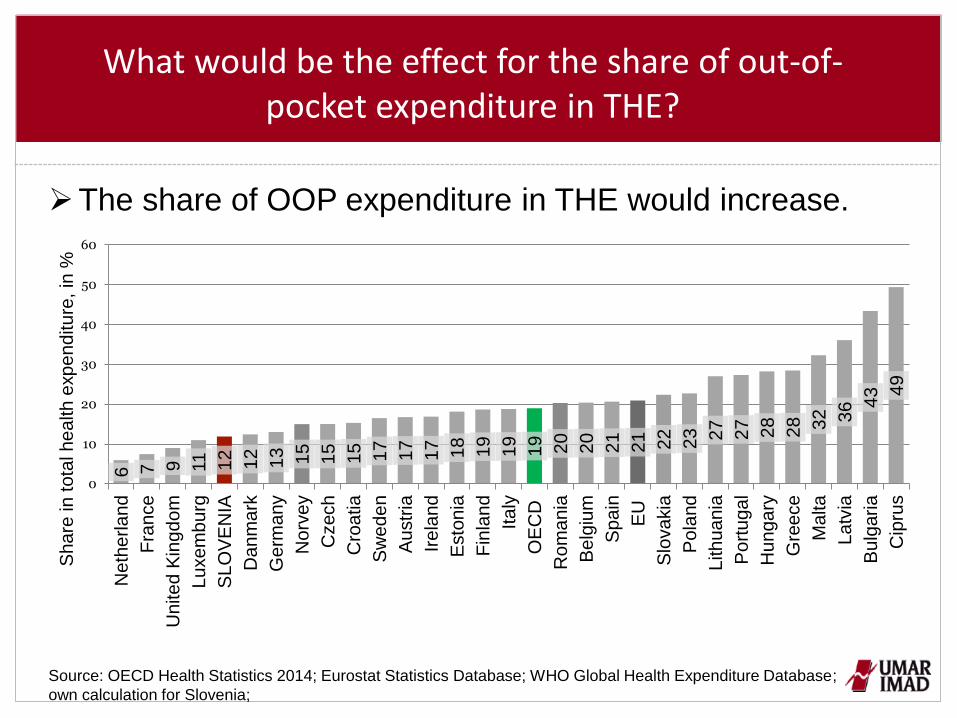
What would be the effect for the share of out-of-pocket expenditure in THE?
The share of OOP expenditure in THE would increase.
Source: OECD Health Statistics 2014; Eurostat Statistics Database; WHO Global Health Expenditure Database;
own calculation for Slovenia;
6 7 9
11
12
12
13
15
15
15
17
17
17
18
19
19
19
20
20
21
21
22
23
27
27
28
28
32
36 43
49
0
10
20
30
40
50
60
Ne
the
rla
nd
Fra
nce
Un
ite
d K
ing
do
m
Lu
xe
mb
urg
SL
OV
EN
IA
Da
nm
ark
Ge
rma
ny
No
rve
y
Czech
Cro
atia
Sw
ed
en
Au
str
ia
Ire
lan
d
Esto
nia
Fin
lan
d
Italy
OE
CD
Ro
ma
nia
Be
lgiu
m
Spain
EU
Slo
va
kia
Po
land
Lith
ua
nia
Po
rtu
ga
l
Hu
ng
ary
Gre
ece
Ma
lta
La
tvia
Bu
lgaria
Cip
rus
Sh
are
in
to
tal h
ea
lth
exp
en
ditu
re,
in %
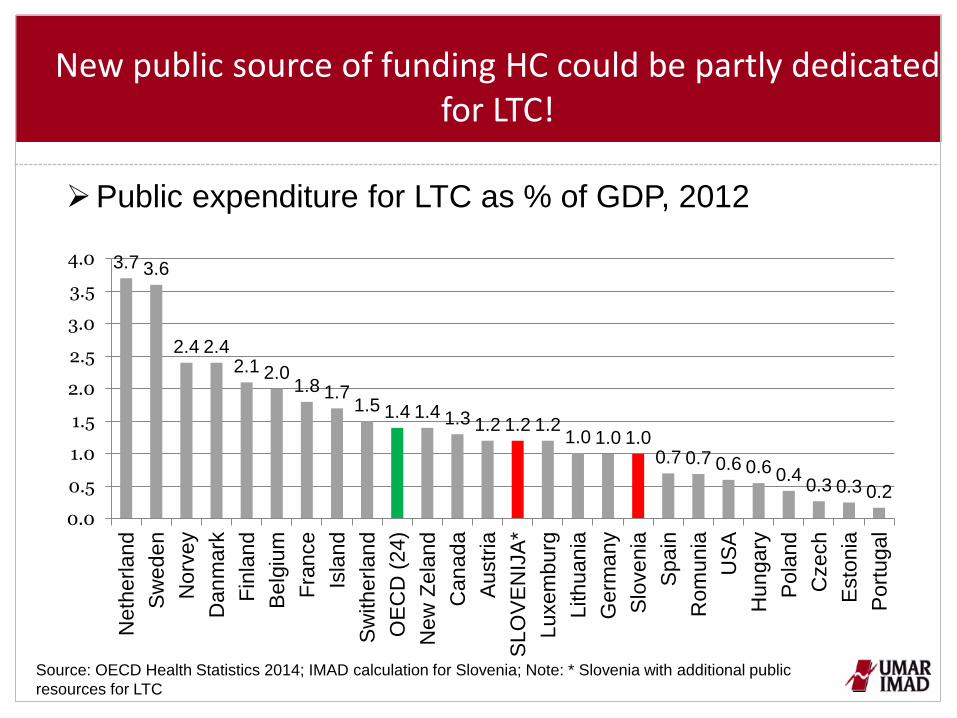
New public source of funding HC could be partly dedicated
for LTC!
Public expenditure for LTC as % of GDP, 2012
3.7 3.6
2.4 2.4 2.1 2.0
1.8 1.7 1.5 1.4 1.4 1.3 1.2 1.2 1.2
1.0 1.0 1.0 0.7 0.7 0.6 0.6 0.4
0.3 0.3 0.2
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
Neth
erland
Sw
ed
en
Norv
ey
Dan
mark
Fin
land
Belg
ium
Fra
nce
Isla
nd
Sw
itherlan
d
OE
CD
(24)
New
Zela
nd
Ca
nad
a
Austr
ia
SLO
VE
NIJ
A*
Luxem
bu
rg
Lithuan
ia
Germ
any
Slo
ve
nia
Spain
Rom
unia
US
A
Hun
gary
Pola
nd
Czech
Esto
nia
Port
ugal
Source: OECD Health Statistics 2014; IMAD calculation for Slovenia; Note: * Slovenia with additional public
resources for LTC
Conclutions
High share of LTC health component in total LTC expenditure
Reform of LTC financing has to be linked to health financing reform (important
is flexibility to move funding between health and LTC system)
Ensuring a sustainable financing system that needs to be adaptable and
predictable in times
In the case of a replacement of complementary private health insurance with
new public source of funding it would be necessary to create new user-
charges and/or copayments for certain services and drugs
New public tax/levy could be partly dedicated to an increase in aggregate
expenditure on health and partly to finance long-term care – to reasses
boundaries between public and private funding at the same time for HC and
LTC
Thank you!
More information on LTC reform in Slovenia could be find on the link:
http://ec.europa.eu/social/main.jsp?catId=1024&langId=en&newsId=2097&
furtherNews=yes