long term care emergency preparedness notes pages
TRANSCRIPT
The new rules for Medicare were released in December of 2013 for review. We are nearing the two-year maximum where this rule must be implemented or abandoned. The new rules trouble many, because they are kind of an unfunded mandate that insiststhat LTCs invest time and energy to prepare for disasters. This briefing will discuss these news rules and why they are important to you. We will also provide you with 3 “easy” steps for complying with these new rules.
1
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
2
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
3
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
Here are some interesting facts. The reason that Medicare and Medicaid has updated its rules, is that it found that emergency planning, even in high-occurrence hurricane states such as Louisiana, was lacking. Long Term Care facilities must do a lot of their own heavy lifting. They rely on transportation contracts, food and medicine suppliers and their staff to handle any sort of emergency. When a disaster strikes, their support network can fail leaving them literally stranded to deal with the disaster on their own.
4
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
What’s worse is that researchers found that anything that disturbs residents, makes them move or worry, can lead to increased morbidity and mortality. The elderly are extremely fragile, so every effort must be made to buffer the extreme effects of a disaster. Frail elderly residents can be affected by a disaster for up to 90 days after the event. So moving them is a high-risk prospect. Are you ready?
5
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
I thought this quote was interesting, because it shows the internal dialogue of an administrator who is weighing the costs of staying versus evacuating. There is no question that evacuation is arguably the toughest decision a leader could make in this community.
6
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/som107ap_pp_guidelines_ltcf.pdf
Current regulations already require disaster and emergency preparedness in the form of detailed and written plans. The regulations even ask that LTC’s provide training for new employees and at least some review with existing staff.
7
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/som107ap_pp_guidelines_ltcf.pdf, p665
The physical environment must be robust enough to protect residents including fire suppression and emergency power.
8
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
Reference: Federal Register/Vol. 78, No. 249/ Friday, December 27, 2013/ Proposed Rule. Page 79082
But as a result of the facts we discussed earlier, the proposed rules are a little tougher and require more planning, training and testing. The rule was introduced in December of 2013 and has been under review ever since. However, the rule must be passed or rescinded within two years of issuance. DHHS has been gathering inputs and is scheduled to issue this rule in 2016.
9
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
Reference: Federal Register/Vol. 78, No. 249/ Friday, December 27, 2013/ Proposed Rule. Page 79082, 79109
The rule intends to cross-level the standards and make them consistent with hospital requirements. The rules apply not only to LTC’s, but also to 17 other provider and supplier types who wish to participate in Medicare and Medicaid. There are some variations across these 17 groups depending on existing statutes and to whom the services are provided. Nevertheless, the idea is to standardize the requirements across the entire system.
10
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
Reference: Federal Register/Vol. 78, No. 249/ Friday, December 27, 2013/ Proposed Rule. Page 79085
Sum it up to say that the new rules are based on 4 core elements that Medicare feels are, “Central to an effective and comprehensive framework of emergency preparedness requirements for the various Medicare and Medicaid participating providers and suppliers.” These elements have been tested in other areas of emergency management and have been shown to be effective.
An all-hazards risk assessment is the first step. The risk assessment should be performed first because it informs the entireprocess. We will discuss some ways to conduct a risk assessment and to evaluate your facility later in the seminar.
Policies and procedures are the foundation of your facility’s effort to be prepared. The facility’s policy document describes who is responsible, what is important to focus and reinforces management’s commitment to provide resources and oversight to the program. We will describe what goes into a policy later in the seminar.
Communications Plan is key to ensuring that all stakeholders understand what you intend to do as the result of an incident. Communications must reach your staff, residents, their families and resource providers in the local community such as your localhealthcare coalition.
Lastly, there is training and testing. The new rules spend much more time defining exactly what type of training should be provided, how results of training should be acted on and how often training should be conducted. Training and testing are absolutely vital to maintaining readiness – which is your elusive and difficult-to-maintain capacity to act effectively in a crisis.
11
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
Reference: Federal Register/Vol. 78, No. 249/ Friday, December 27, 2013/ Proposed Rule. Page 79101
Did we mention that the new rules require more training and testing ? Another characteristic of the new rules is they insist that you participate in broader community exercises when presented with the opportunity. This way, you can get a feel for what support you can expect to receive from your local community. I personally wouldn’t wait for a community exercise to come around. Thenext time I did a table top or a drill, I would invite local emergency managers, first responders or members of my healthcarecoalitions. They all have a duty to support your planning efforts.
12
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
Generator failure also comes up in many disaster after action reviews and not just with LTC’s. Organizations invest hundreds-of-thousands of dollars in their power back-up systems, only to have them fail when they need them. Most problems are traced back to poor installation and the lack of a solid testing program.
13
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
So by now, you are probably really concerned. Concerned like, “Where do I start?” “Where am I going to get the money to do thisprogram?” and even worse, “Where am I going to get the time?” No matter how you slice it, an effective emergency management program is a serious investment against future risk.
We have attempted to break this process down into 3 “Easy” steps. By “easy” we meant conceptually easy. There is a lot of work that needs to be done. Most of you likely are not starting from scratch. You will likely have versions of many of these plans that need to be dusted off, updated and practiced.
We recommend that you start with a risk assessment. A risk assessment can be built from a variety of sources. We will go into that a little later.
Once you have a risk assessment, you will need to devise plans that speak directly to these risks. We have some recommendations about what should be in your plan. Remember, when writing plans, the key is not volume. On the contrary, it is about brevity. What is more important than the plan is . . .
Training and rehearsal. Involve as many stakeholders as you can and train regularly. Find ways to do it on the cheap, so that it is done often. We have some suggestion there too.
14
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
An all-hazards risk assessment means all of the possible sources of hazards. The purpose of doing a risk assessment is to understand how these risks will affect your facility in terms of your vulnerability to the consequences (a risk-vulnerability).
A few examples of all-hazards risk include:• Fire• Flood• Earthquake• Crime (such as a high incidence of armed robbery in your community)• Chemical spill (such as if you are near a refinery or train tracks).
You can address risk in two ways. First, you can remove a risk-vulnerability altogether. For example, you may have identified a vulnerability such as a generator fuel line that is prone to break due to an earthquake. If you changed the line out to be moreseismically resistant, then you have removed the risk-vulnerability entirely.
If you can’t remove a risk, because it would be too expensive, then you are going to deal with risk-vulnerability consequences. A majority of vulnerabilities are dealt with this way. When dealing with consequences, you want to reduce the effect of these consequences. So for example, if you identified flooding as a vulnerability you could decide that evacuation to an alternate location is a means of mitigating the effect of the consequences of flooding. Thus, by planning, coordinating and practicing an evacuation prior to the event – you are putting capabilities in place to mitigate your flooding risk-vulnerability.
15
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
So where do you start? Each county and city is mandated to maintain an up-to-date risk assessment. It normally discusses risk in terms of severity and probability of occurrence. When taken together, these two factors indicate what you should focus on first, second and third.
Your location in geographical terms is probably the most important thing to consider. The terrain surrounding your campus is will either help protect your facility or just the opposite, offer little protection from your most common risks. Get outside and walk around your campus. Learn to see the risks in your environment. Below are some easy questions to start with:
Flooding:• Are you near a river, creek or stream?• If so, are you protected by a levy or other civil works project such as a dam?• Are you on a flood plain? (if so, your county likely has flood inundation maps that show the extent of flooding that could occur in
your neighborhood)
Seismic:• Is your building recent construction? • How is your building constructed (stacked masonry, reinforced concrete, stick-built)?• Are you on poorly consolidated soils (such as a flood plain)? Areas that have a high seismicity maintain soil liquefaction maps.
Landslide:• Are you near a slope?• Is the slope landslide prone? Many counties maintain slide maps of areas prone to landslide to keep people from building on
them.
Hazardous Materials Transportation• Are you near any pipelines, such as natural gas or petroleum? Check with your state’s utilities transportation commission.
16
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
• Are you near train tracks?
Crime:• What are the crime statistics in your neighborhood? Most police departments are required to maintain and report
crime statistics to the FBI. Many jurisdictions have maps that show the location and nature reported crimes.• Does your building have access controls and ways to keep someone from breaking in?
Forest Fire:• Are you in a forested area – prone to forest fires?• Those beautiful trees outside your LTC – do they provide a path for fire to reach your facility?
Demystifying the New Medicare Rules 3/29/2016
©Takouba – all rights reserved 16
Reference: Federal Register/Vol. 78, No. 249/ Friday, December 27, 2013/ Proposed Rule. Page 79096
A solid policy is vital for a successful program. A policy documents management’s commitment to making your facility resilient. A good policy document follows these guidelines:
• Identifies who is responsible for coordinating the program• Identifies the mission critical functions of the organization• States management’s commitment to provide necessary resources to maintain the program• Integrates the program into the management review process, so it can be regularly reviewed for progress.
The policy should be supported by procedures that support your risk assessment process should be updated regularly as your facility is changed (such as if it was remodeled), or your local EM changes the risk assessment. The procedures should also support EM and Communications plan development.
Finally, all plans should be reviewed and updated at least annually as a part of management review. Plan reviews normally consist of a Corrective Action Plan (CAP) that documents needed improvements as the result of the last exercise. To be successful, management must hold someone accountable to make the needed changes highlighted in the CAP.
17
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
Reference: Federal Register/Vol. 78, No. 249/ Friday, December 27, 2013/ Proposed Rule. Page 79096-97
The proposed rules outline several subjects that providers and suppliers should outline in their EM plan. In general, these processes must be adequate enough to, “Provide continuing patient care during the emergency.”
18
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
Reference: Federal Register/Vol. 78, No. 249/ Friday, December 27, 2013/ Proposed Rule. Page 79097
The rules also emphasize the need to adequately track patients in manner where the data is, “Available, accurate and shareableamong officials within and across the emergency response system.” There is definitely a cyber-emphasis in the new regulations that should be evaluated, so your facility will have a robust information assurance program. This is a pretty tough issue to resolve, especially in austere disaster environments.
The new rules also propose, “That facilities would have to have policies and procedures in place to address the use of volunteers in an emergency or other emergency staffing strategies, including the process and role for integration of state orfederally designated health care professionals to address surge needs during an emergency.” Many states now have volunteer registration services that manage volunteer credentials. But you plans must go beyond registration and include how you use and integrate volunteers into your care-stream.
19
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
Reference: Federal Register/Vol. 78, No. 249/ Friday, December 27, 2013/ Proposed Rule. Page 79099
While the proposed rule seems focus on a hospital’s communication plan, the rule goes on to state, “We believe this requirement would best be applied only to providers and suppliers who provide continuous care to patients, as well as to those providers and suppliers that have responsibilities and oversight for care of patients who are homebound or receiving services at home.”
It many ways it only makes sense that an LTC have a robust communications plan. This will enable the LTC to integrate with the rest of the healthcare response, keep families informed and to receive support as required.
20
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
Reference: Federal Register/Vol. 78, No. 249/ Friday, December 27, 2013/ Proposed Rule. Page 79100
Training is the toughest part of the readiness – preparedness challenge. The new rule proposes that everyone with a care-stream provide table-tops and mock disaster drills which include an evacuation to at least a same-floor “safe-zone” to, “Ensure the safety of both ambulatory patients and those who are wheelchair users, have mobility impairments or have other special needs.” The rule also encourages providers and suppliers to participate in community or coalition level training.
The rule indicates many publicly available training resources that instruct you how to conduct an Homeland Security Exercise and Evaluation Program compliant exercise. Keep in mind – that training does not necessarily result in improved readiness. The next several slides will explain the concept of readiness, how it is extremely perishable and what factors affect it.
21
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules

The bottom line is that readiness is a team sport. It is both a grassroots and an executive level enterprise. Without buy-in from the “team” your effort is sabotaged from the start. To that end, we propose a committee be established to regularly review training plans, results and corrective actions.
The committee should meet frequently until some level of readiness is established, then every other month. We also encourageyou to meet and engage with your local healthcare coalition – as they have the charter to improve your readiness.
22
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
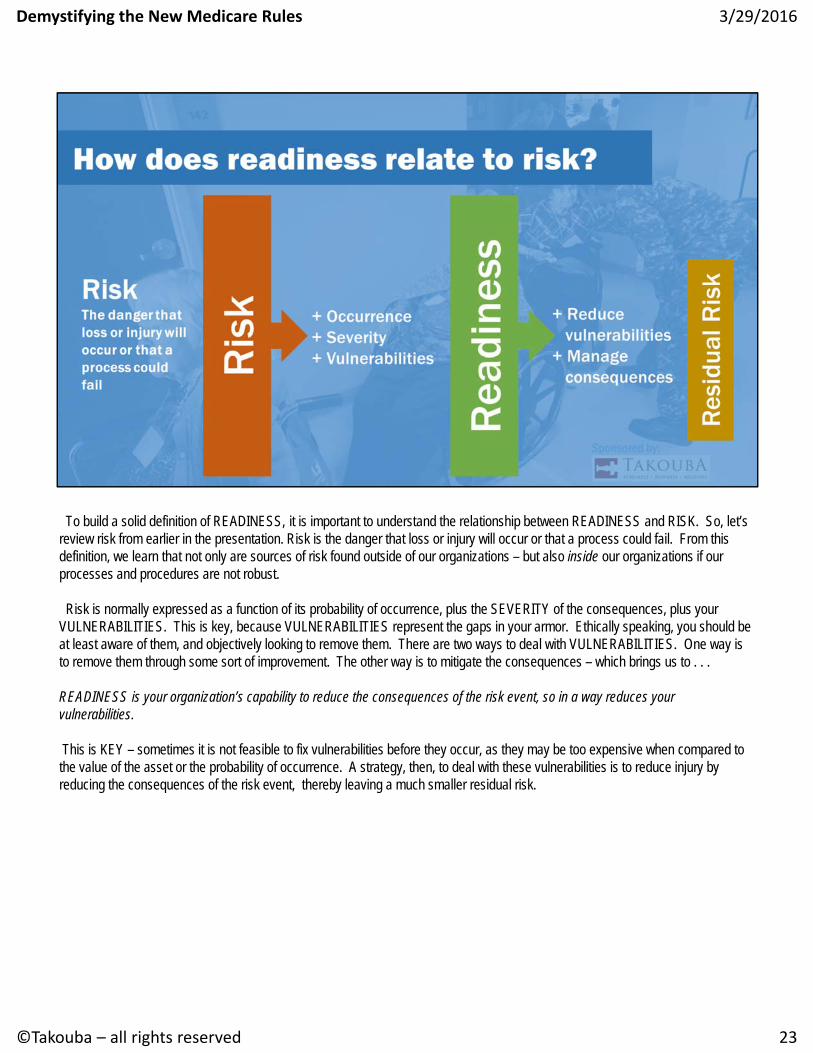
To build a solid definition of READINESS, it is important to understand the relationship between READINESS and RISK. So, let’s review risk from earlier in the presentation. Risk is the danger that loss or injury will occur or that a process could fail. From this definition, we learn that not only are sources of risk found outside of our organizations – but also inside our organizations if our processes and procedures are not robust.
Risk is normally expressed as a function of its probability of occurrence, plus the SEVERITY of the consequences, plus your VULNERABILITIES. This is key, because VULNERABILITIES represent the gaps in your armor. Ethically speaking, you should be at least aware of them, and objectively looking to remove them. There are two ways to deal with VULNERABILITIES. One way isto remove them through some sort of improvement. The other way is to mitigate the consequences – which brings us to . . .
READINESS is your organization’s capability to reduce the consequences of the risk event, so in a way reduces your vulnerabilities.
This is KEY – sometimes it is not feasible to fix vulnerabilities before they occur, as they may be too expensive when compared to the value of the asset or the probability of occurrence. A strategy, then, to deal with these vulnerabilities is to reduce injury by reducing the consequences of the risk event, thereby leaving a much smaller residual risk.
23
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
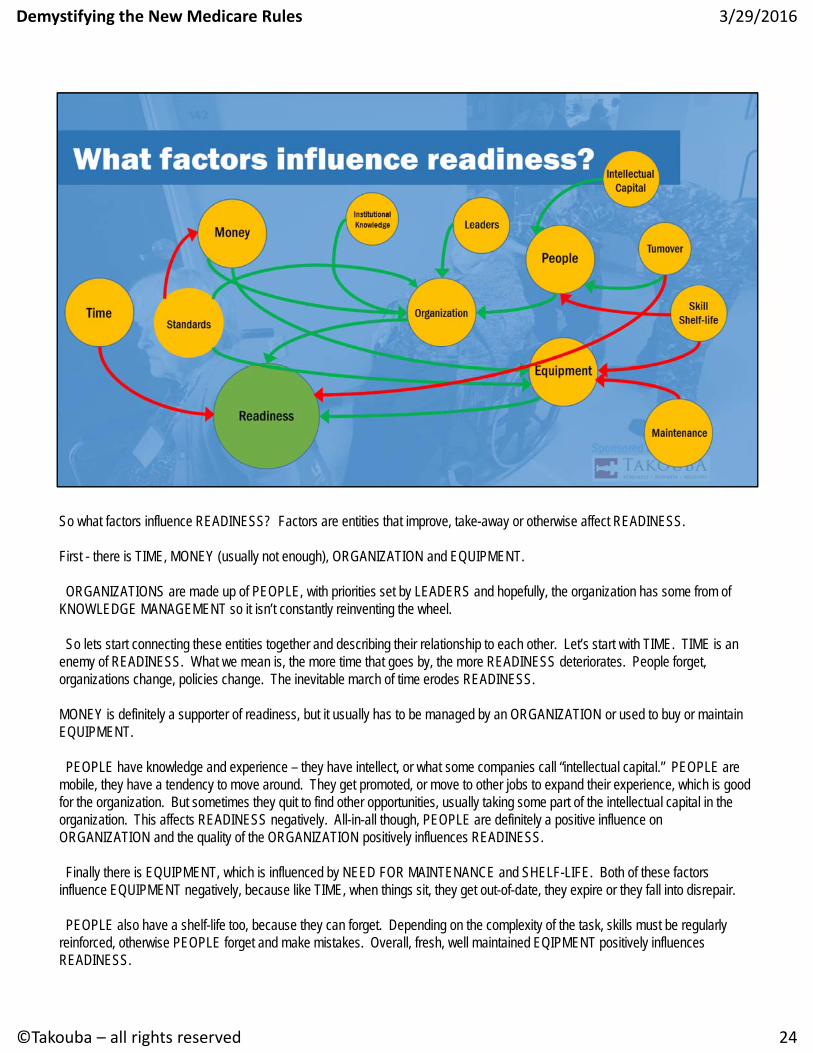
So what factors influence READINESS? Factors are entities that improve, take-away or otherwise affect READINESS.
First - there is TIME, MONEY (usually not enough), ORGANIZATION and EQUIPMENT.
ORGANIZATIONS are made up of PEOPLE, with priorities set by LEADERS and hopefully, the organization has some from of KNOWLEDGE MANAGEMENT so it isn’t constantly reinventing the wheel.
So lets start connecting these entities together and describing their relationship to each other. Let’s start with TIME. TIME is an enemy of READINESS. What we mean is, the more time that goes by, the more READINESS deteriorates. People forget, organizations change, policies change. The inevitable march of time erodes READINESS.
MONEY is definitely a supporter of readiness, but it usually has to be managed by an ORGANIZATION or used to buy or maintain EQUIPMENT.
PEOPLE have knowledge and experience – they have intellect, or what some companies call “intellectual capital.” PEOPLE are mobile, they have a tendency to move around. They get promoted, or move to other jobs to expand their experience, which is goodfor the organization. But sometimes they quit to find other opportunities, usually taking some part of the intellectual capital in the organization. This affects READINESS negatively. All-in-all though, PEOPLE are definitely a positive influence on ORGANIZATION and the quality of the ORGANIZATION positively influences READINESS.
Finally there is EQUIPMENT, which is influenced by NEED FOR MAINTENANCE and SHELF-LIFE. Both of these factors influence EQUIPMENT negatively, because like TIME, when things sit, they get out-of-date, they expire or they fall into disrepair.
PEOPLE also have a shelf-life too, because they can forget. Depending on the complexity of the task, skills must be regularlyreinforced, otherwise PEOPLE forget and make mistakes. Overall, fresh, well maintained EQIPMENT positively influences READINESS.
24
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
That is quite a plate of spaghetti and meatballs! The bottom line, is that assessing READINESS is complicated because it is influenced by so many different factors. The purpose of this brief seminar is to discuss how to structure your approach to assessing READINESS.
Demystifying the New Medicare Rules 3/29/2016
©Takouba – all rights reserved 24
So how do we develop our team?
The first thing to assess is individual competence and provide individual training. Individual training is a foundation, because it ensures that an individual can fulfill their individual duties or tasks in their primary job. Individual training is normally provided on-the-job or through employer provided training.
Note: With respect to disaster training, individual training would focus on what role the person performs during an emergency, which is usually documented on a job action sheet. In this discussion, individual training would focus on the tasks the individual would perform in an emergency situation.
25
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
Next – we train as a team.
This is called collective training, where trainers provide CONTEXT for the learning event. Examples of collective training would include drills, functional and full-scale exercises. Collective training events are meant to evaluate the adequacy of a system, in this case an emergency management system, and to provide context for individuals to interact with each other. Finally, besides learning, collective training events test processes – like planning and reporting.
26
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
And we develop leaders -
The final dimension of team-building is preparing confident leaders. Collective training such as exercises provide leaders (if they participate) with a way to build confidence in their team, to provide a venue to test out processes and procedures and to ultimately validate that the organization is ready. Leadership confidence is indispensable.
27
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
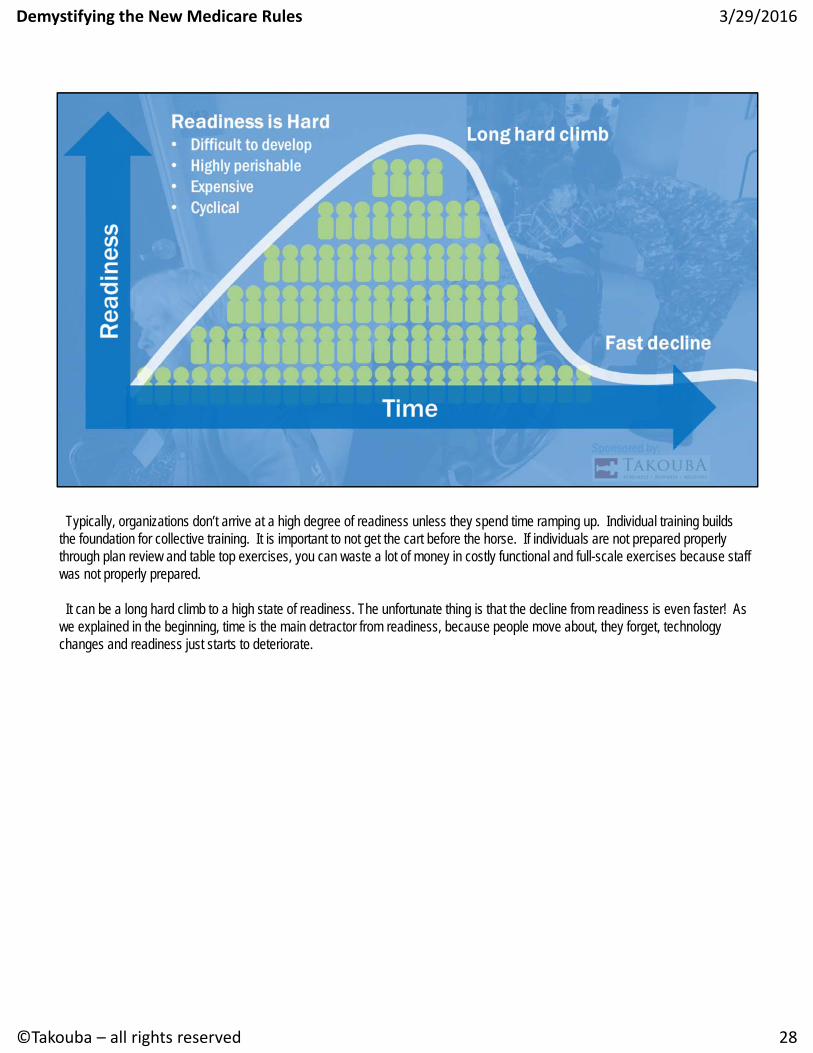
Typically, organizations don’t arrive at a high degree of readiness unless they spend time ramping up. Individual training builds the foundation for collective training. It is important to not get the cart before the horse. If individuals are not prepared properly through plan review and table top exercises, you can waste a lot of money in costly functional and full-scale exercises because staff was not properly prepared.
It can be a long hard climb to a high state of readiness. The unfortunate thing is that the decline from readiness is even faster! As we explained in the beginning, time is the main detractor from readiness, because people move about, they forget, technology changes and readiness just starts to deteriorate.
28
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
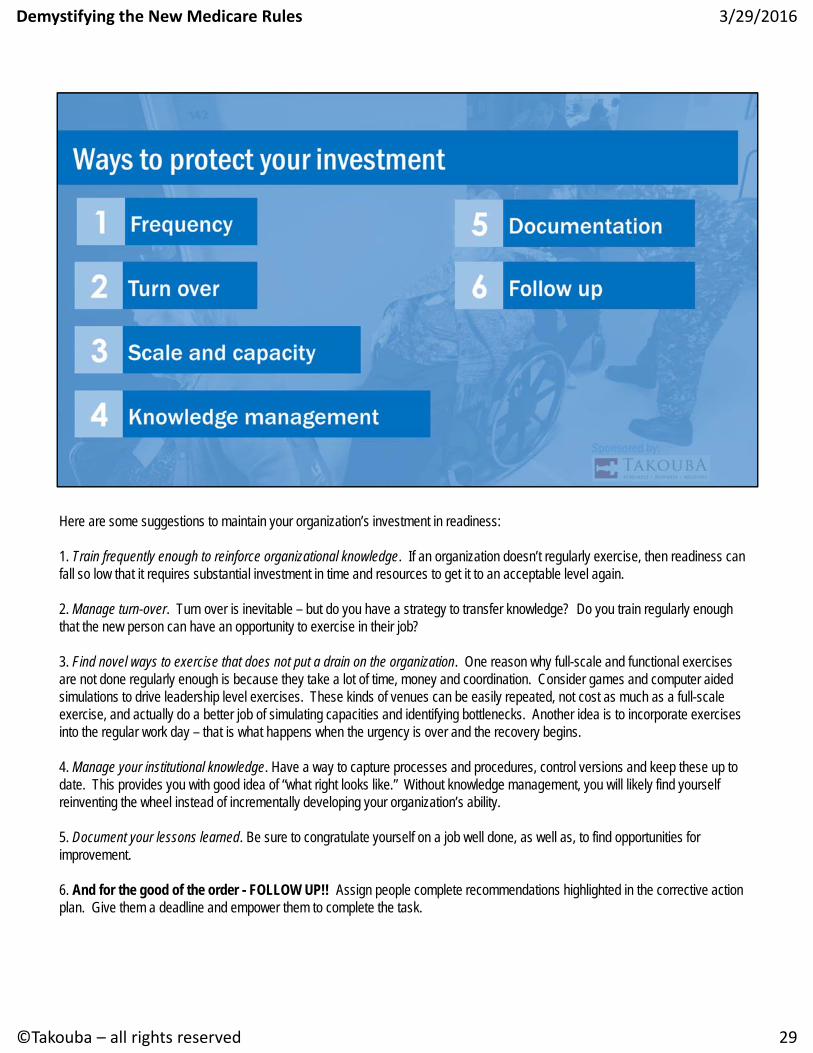
Here are some suggestions to maintain your organization’s investment in readiness:
1. Train frequently enough to reinforce organizational knowledge. If an organization doesn’t regularly exercise, then readiness can fall so low that it requires substantial investment in time and resources to get it to an acceptable level again.
2. Manage turn-over. Turn over is inevitable – but do you have a strategy to transfer knowledge? Do you train regularly enough that the new person can have an opportunity to exercise in their job?
3. Find novel ways to exercise that does not put a drain on the organization. One reason why full-scale and functional exercises are not done regularly enough is because they take a lot of time, money and coordination. Consider games and computer aided simulations to drive leadership level exercises. These kinds of venues can be easily repeated, not cost as much as a full-scaleexercise, and actually do a better job of simulating capacities and identifying bottlenecks. Another idea is to incorporate exercises into the regular work day – that is what happens when the urgency is over and the recovery begins.
4. Manage your institutional knowledge. Have a way to capture processes and procedures, control versions and keep these up to date. This provides you with good idea of “what right looks like.” Without knowledge management, you will likely find yourselfreinventing the wheel instead of incrementally developing your organization’s ability.
5. Document your lessons learned. Be sure to congratulate yourself on a job well done, as well as, to find opportunities for improvement.
6. And for the good of the order - FOLLOW UP!! Assign people complete recommendations highlighted in the corrective action plan. Give them a deadline and empower them to complete the task.
29
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules
https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/SurveyCertEmergPrep/HealthCareProviderGuidance.html
Thank you so much for joining us for this session. We hope that you found it informative. Preparing for a disaster is never easy. But with consistent effort over the long term, you can incrementally prepare your organization to face the worst that life has to offer.
I invite you to download this CMS checklist. In can be found at the web address listed. This CMS website page providesinformation for emergency preparedness and planning.
Thank you!
30
3/29/2016
©Takouba – all rights reserved
Demystifying the New Medicare Rules