long handout - university of colorado denver
TRANSCRIPT
2
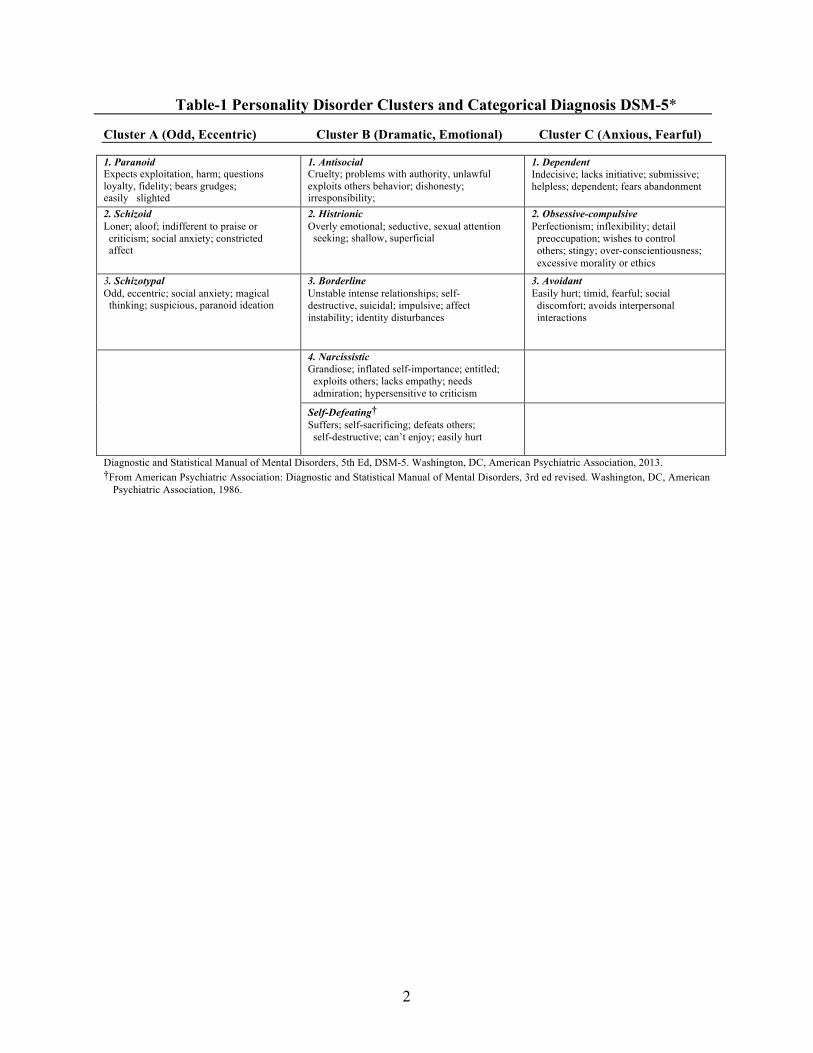
Table-1 Personality Disorder Clusters and Categorical Diagnosis DSM-5*
Cluster A (Odd, Eccentric) Cluster B (Dramatic, Emotional) Cluster C (Anxious, Fearful)
1. Paranoid Expects exploitation, harm; questions loyalty, fidelity; bears grudges; easily slighted
1. Antisocial Cruelty; problems with authority, unlawful exploits others behavior; dishonesty; irresponsibility;
1. Dependent Indecisive; lacks initiative; submissive; helpless; dependent; fears abandonment
2. Schizoid Loner; aloof; indifferent to praise or criticism; social anxiety; constricted affect
2. Histrionic Overly emotional; seductive, sexual attention seeking; shallow, superficial
2. Obsessive-compulsive Perfectionism; inflexibility; detail preoccupation; wishes to control others; stingy; over-conscientiousness; excessive morality or ethics
3. Schizotypal Odd, eccentric; social anxiety; magical thinking; suspicious, paranoid ideation
3. Borderline Unstable intense relationships; self-destructive, suicidal; impulsive; affect instability; identity disturbances
3. Avoidant Easily hurt; timid, fearful; social discomfort; avoids interpersonal interactions
4. Narcissistic Grandiose; inflated self-importance; entitled; exploits others; lacks empathy; needs admiration; hypersensitive to criticism
Self-Defeating† Suffers; self-sacrificing; defeats others; self-destructive; can’t enjoy; easily hurt
Diagnostic and Statistical Manual of Mental Disorders, 5th Ed, DSM-5. Washington, DC, American Psychiatric Association, 2013. †From American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 3rd ed revised. Washington, DC, American
Psychiatric Association, 1986.
3
Movie Analysis
Schema Describe Film Observations Diagnosis
Physician Reaction
Patient Fears & Core
Beliefs
Patient Health
Behaviors
Review on your own See below
Adherence
Review on your own See below
Medical Utilization
Review on your own See below
Coping Styles
Review on your own See below
Defenses
Interventions
4
Movie Analysis Schema Describe Film Observations Diagnosis
Physician Reaction
Patient Fears & Core
Beliefs
Patient Health
Behaviors
Review on your own See below
Adherence
Review on your own See below
Medical Utilization
Review on your own See below
Coping Styles
Review on your own See below
Defenses
Interventions
5
PERSONALITY DISORDERS-DSM-5 [KEY POINTS 1]
• An enduring pattern of inner experience and behavior that deviates markedly from the expectations of the individual’s culture.
• Problems are in at least two of these areas: cognition, affectivity, interpersonal functioning, and impulse control.
• An enduring pattern is inflexible and pervasive across a broad range of persona and social situations.
• The enduring pattern leads to clinically significant distress or impairment in social, occupational or other areas of functioning
• A the pattern is stable and of long duration and onset can be traced back to adolescence or and is diagnosed in adulthood.
• To diagnose begin with dimensional measures: Cluster A-odd eccentric, Cluster B- dramatic emotional Cluster C-avoidant fearful. ( Table-1)
• Use the categorical classification systems to identify the specific personality disorder • A particular patient may have traits from different clusters and may meet criteria for more
than one personality disorder.
SCHEMA FOR MANAGING PATIENTS SUFFERING WITH A PERSONALITY DISORDER [KEY POINTS 2] To create therapeutic relationships with personality disordered patients who might otherwise be experienced as difficult, and to offer a management strategy, the following five-step process is useful for family physicians: • The clinician must first understand patients’ core beliefs, irrational thoughts, and fears; • Identify the patient’s defense mechanisms and coping style, and use confrontation,
clarification, and interpretation to modify these. • Recognize recurrent patient behaviors and how these will likely affect patient adherence
and use of medical services. • Learn to use the physician’s own reactions to the patient to help identify the diagnosis
and management strategy. • Recognize that specific interventions are helpful for different types of patients. (Table 3)
PATIENT CORE BELIEFS, IRRATIONAL THOUGHTS, AND FEARS [KEY POINTS 3]
• Patients have identifiable core beliefs or worldviews, and fears. • These interact and can feed off each other in difficult patients. • Stress activates these core beliefs and precipitates intense and dysfunctional emotions,
fears, thoughts, physical symptoms or maladaptive behaviors which are characteristic for each specific personality disorder ( Table-2)
• Adherence to medical recommendations and use of medical services are somewhat predicable based on the particular personality disorders.
6
DEFENSES AND COPING STYLES [KEY POINTS 4]
• Defense mechanisms are automatic internal psychological processes that protect the patient from anxiety and stresSOR:s and help with adaptation to the environment.
• Patients with specific personality diagnoses use a known range of particular defense mechanisms (see Table 2).
• Patient with unexplained somatic symptoms tend to use denial, externalization, and somatization, converting psycho-social distress and problematic interpersonal relationships, into unexplained physical complaints
• Coping styles are typical behavioral ways of dealing with the external world • Patients with specific personality diagnoses tend to use a known range of coping style
(see Table-2). • Patient with severe unexplained somatic symptoms tend to use high /low anxious coping
styles or manipulative coping styles (See Table -3) PATIENT BEHAVIORS, ADHERENCE, AND USE OF MEDICAL SERVICES [KEY POINTS 5]
• Cluster A personality disorders (paranoid, schizoid, and schizotypal) tend not to adhere to medical recommendations and underuse medical services.
• Cluster B patients (antisocial, histrionic, borderline, narcissistic, and self-defeating) tend to have variable adherence to medical recommendations and may misuse, overuse, or underuse medical care.
• Cluster C patients (dependent, obsessive-compulsive, avoidant) tend to adhere to medical recommendations because of fear of the consequences of non-adherence.
PHYSICIAN REACTIONS TO PATIENTS WITH A PERSONALITY DISORDER [KEY POINTS 6]
• Physician reactions are useful in recognizing, diagnosing, and managing difficult patients • Reactions stirred by the patient are referred to as patient-generated counter-transferences. • Physician reactions are often similar or shared in common by all physicians seeing the
patient, with some elements peculiar to each individual physician. • Difficult patients often generate intense physician feelings. • There may be fantasies or thoughts about the patient that are uncharacteristic for the
physician. • The physician may engage in atypical behaviors that would normally not be typical for him
or her (see Table xx-2).
GENERAL MANAGEMENT PRINCIPLES FOR PATIENTS WITH A PERSONALITY DISORDER [KEY TREATMENT BOX 1] • Attend to the doctor-patient relationship • Focus the interview on manageable goals within the time frame available
7
• Use psychotherapeutic techniques of confrontation, clarification and interpretation when interviewing the patient ( SOR: A)
• Attend to the patient’s emotional needs. SOR: B • Modify the patient’s surroundings.SOR: C • Improve the patient’s capacity to test reality. SOR: B • Empathize with the patient’s worldview. SOR: B • Accept the patient’s limitations and strengths. SOR: C • Manage unreasonable patient expectations and set limits. SOR: C • Question illogical feelings, thoughts, and behaviors. SOR: C • Discuss defenses and coping style and interpret them. Table xx-3. SOR: C • Prescribe medications as needed. SOR:B • Use specific interventions for each kind of difficult patient as detailed in Table xx-3.(SOR:
B) USING MEDICATIONS FOR PATIENT’S WITH PERSONALITY DISORDER; FOCUS ON KEY SYMPTOMS [KEY TREATMENT BOX 2]
• Medications can target anger/impulsive aggression, suicidal ideation, psychotic symptoms, mood instability, interpersonal problems, anxiety and depression (see Table -4).( SOR:; A)
• Doses for symptoms prescribing are the same as doses used for major psychiatric conditions. ( SOR:: B)
• Anger/impulsive aggression, psychotic symptoms, and anxiety in Borderline Personality Disorder can be treated with aripiprazole and olanzapine. (SOR:: A)
• Anger/impulsive aggression, disturbed interpersonal relationships, and anxiety of BPD can be treated with the mood stabilizer topirimate. (SOR: A Evidence)
• Treatment of suicidal behaviors is best targeted with flupentixol or fluphenazine decanoate, paroxetine, or olanzapine. (SOR: B B Evidence)
• Irritability, anger, and mood symptoms in patients with personality disorders are not generally responsive to Selective Serotonin Reuptake Inhibitors (SSRI’s) as previously reported (SOR: A
• Psychotic symptoms can be treated with low doses of typical or atypical antipsychotic medications. (SOR: B Grade B Evidence)
8
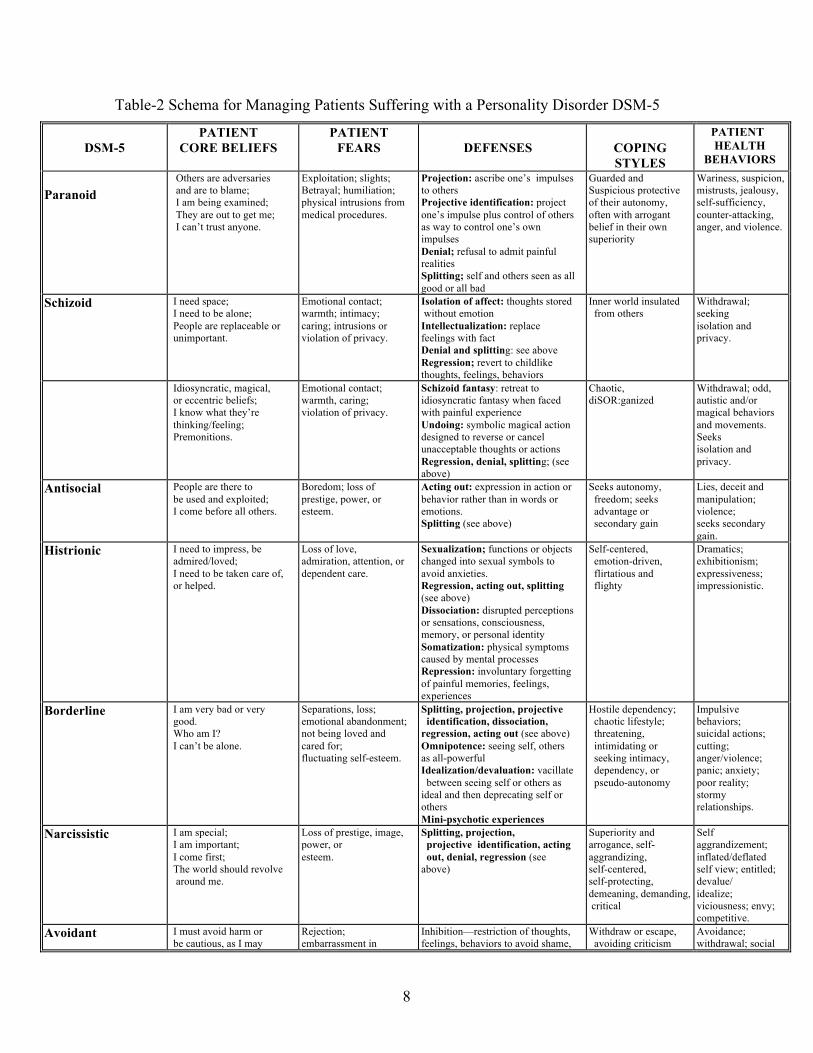
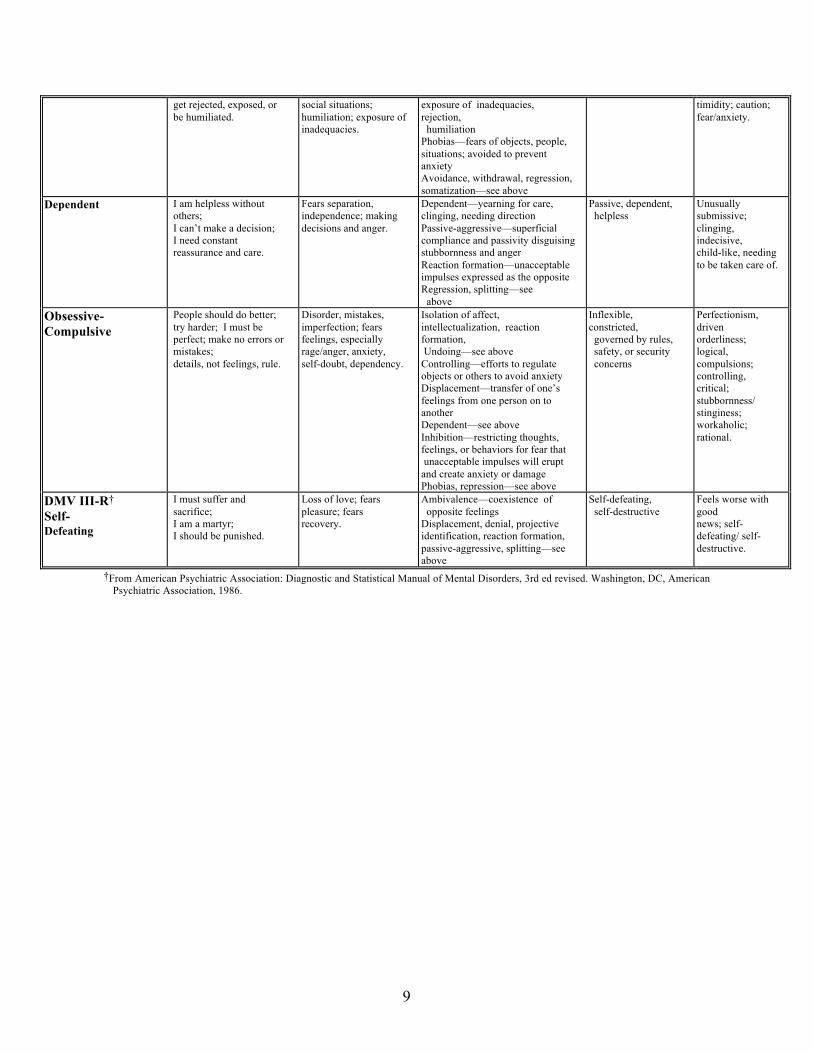
Table-2 Schema for Managing Patients Suffering with a Personality Disorder DSM-5
DSM-5
PATIENT CORE BELIEFS
PATIENT FEARS
DEFENSES
COPING STYLES
PATIENT HEALTH
BEHAVIORS Paranoid
Others are adversaries and are to blame; I am being examined; They are out to get me; I can’t trust anyone.
Exploitation; slights; Betrayal; humiliation; physical intrusions from medical procedures. .
Projection: ascribe one’s impulses to others Projective identification: project one’s impulse plus control of others as way to control one’s own impulses Denial; refusal to admit painful realities Splitting; self and others seen as all good or all bad
Guarded and Suspicious protective of their autonomy, often with arrogant belief in their own superiority
Wariness, suspicion, mistrusts, jealousy, self-sufficiency, counter-attacking, anger, and violence.
Schizoid I need space; I need to be alone; People are replaceable or unimportant.
Emotional contact; warmth; intimacy; caring; intrusions or violation of privacy.
Isolation of affect: thoughts stored without emotion Intellectualization: replace feelings with fact Denial and splitting: see above Regression; revert to childlike thoughts, feelings, behaviors
Inner world insulated from others
Withdrawal; seeking isolation and privacy.
Idiosyncratic, magical, or eccentric beliefs; I know what they’re thinking/feeling; Premonitions.
Emotional contact; warmth, caring; violation of privacy.
Schizoid fantasy: retreat to idiosyncratic fantasy when faced with painful experience Undoing: symbolic magical action designed to reverse or cancel unacceptable thoughts or actions Regression, denial, splitting; (see above)
Chaotic, diSOR:ganized
Withdrawal; odd, autistic and/or magical behaviors and movements. Seeks isolation and privacy.
Antisocial People are there to be used and exploited; I come before all others.
Boredom; loss of prestige, power, or esteem.
Acting out: expression in action or behavior rather than in words or emotions. Splitting (see above)
Seeks autonomy, freedom; seeks advantage or secondary gain
Lies, deceit and manipulation; violence; seeks secondary gain.
Histrionic I need to impress, be admired/loved; I need to be taken care of, or helped.
Loss of love, admiration, attention, or dependent care.
Sexualization; functions or objects changed into sexual symbols to avoid anxieties. Regression, acting out, splitting (see above) Dissociation: disrupted perceptions or sensations, consciousness, memory, or personal identity Somatization: physical symptoms caused by mental processes Repression: involuntary forgetting of painful memories, feelings, experiences
Self-centered, emotion-driven, flirtatious and flighty
Dramatics; exhibitionism; expressiveness; impressionistic.
Borderline I am very bad or very good. Who am I? I can’t be alone.
Separations, loss; emotional abandonment; not being loved and cared for; fluctuating self-esteem.
Splitting, projection, projective identification, dissociation, regression, acting out (see above) Omnipotence: seeing self, others as all-powerful Idealization/devaluation: vacillate between seeing self or others as ideal and then deprecating self or others Mini-psychotic experiences
Hostile dependency; chaotic lifestyle; threatening, intimidating or seeking intimacy, dependency, or pseudo-autonomy
Impulsive behaviors; suicidal actions; cutting; anger/violence; panic; anxiety; poor reality; stormy relationships.
Narcissistic I am special; I am important; I come first; The world should revolve around me.
Loss of prestige, image, power, or esteem.
Splitting, projection, projective identification, acting out, denial, regression (see above)
Superiority and arrogance, self-aggrandizing, self-centered, self-protecting, demeaning, demanding, critical
Self aggrandizement; inflated/deflated self view; entitled; devalue/ idealize; viciousness; envy; competitive.
Avoidant Belief: I I must avoid harm or be cautious, as I may
Rejection; embarrassment in
Inhibition—restriction of thoughts, feelings, behaviors to avoid shame,
Withdraw or escape, avoiding criticism
Avoidance; withdrawal; social
9
get rejected, exposed, or be humiliated.
social situations; humiliation; exposure of inadequacies.
exposure of inadequacies, rejection, humiliation Phobias—fears of objects, people, situations; avoided to prevent anxiety Avoidance, withdrawal, regression, somatization—see above
timidity; caution; fear/anxiety.
Dependent I am helpless without others; I can’t make a decision; I need constant reassurance and care.
Fears separation, independence; making decisions and anger.
Dependent—yearning for care, clinging, needing direction Passive-aggressive—superficial compliance and passivity disguising stubbornness and anger Reaction formation—unacceptable impulses expressed as the opposite Regression, splitting—see above
Passive, dependent, helpless
Unusually submissive; clinging, indecisive, child-like, needing to be taken care of.
Obsessive- Compulsive
People should do better; try harder; I must be perfect; make no errors or mistakes; details, not feelings, rule.
Disorder, mistakes, imperfection; fears feelings, especially rage/anger, anxiety, self-doubt, dependency.
Isolation of affect, intellectualization, reaction formation, Undoing—see above Controlling—efforts to regulate objects or others to avoid anxiety Displacement—transfer of one’s feelings from one person on to another Dependent—see above Inhibition—restricting thoughts, feelings, or behaviors for fear that unacceptable impulses will erupt and create anxiety or damage Phobias, repression—see above
Inflexible, constricted, governed by rules, safety, or security concerns
Perfectionism, driven orderliness; logical, compulsions; controlling, critical; stubbornness/ stinginess; workaholic; rational.
DMV III-R† Self- Defeating
I must suffer and sacrifice; I am a martyr; I should be punished.
Loss of love; fears pleasure; fears recovery.
Ambivalence—coexistence of opposite feelings Displacement, denial, projective identification, reaction formation, passive-aggressive, splitting—see above
Self-defeating, self-destructive
Feels worse with good news; self-defeating/ self-destructive.
†From American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 3rd ed revised. Washington, DC, American Psychiatric Association, 1986.
10
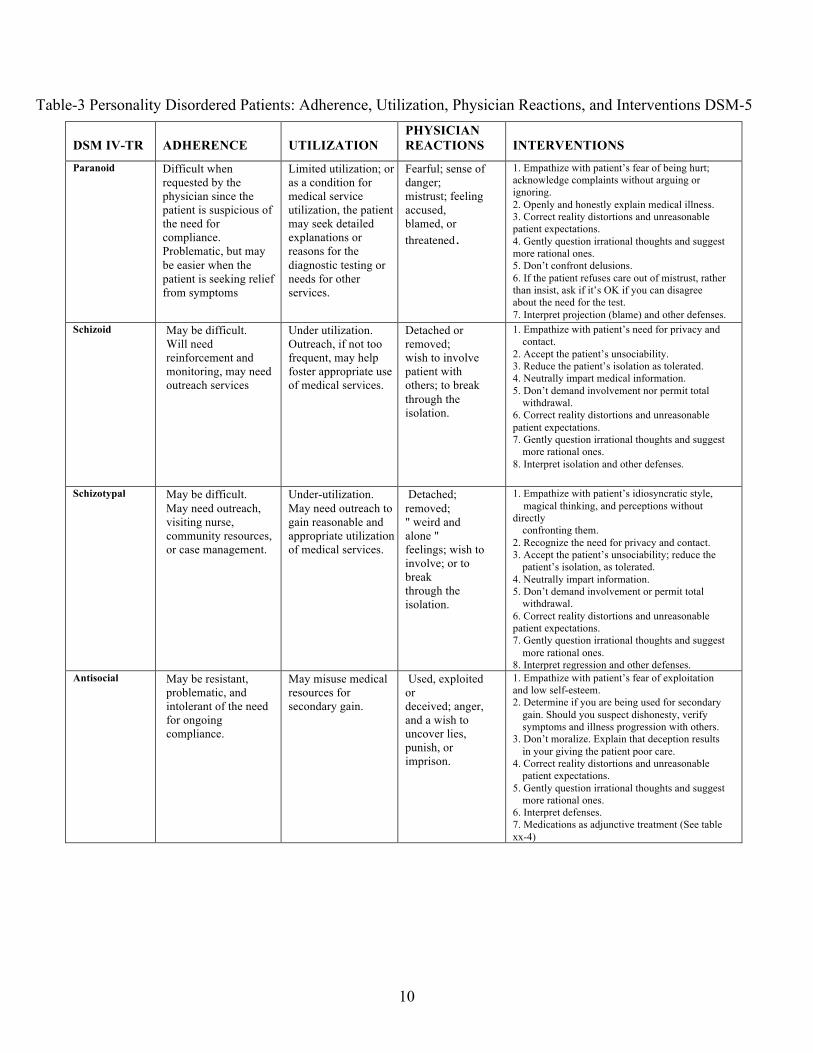
Table-3 Personality Disordered Patients: Adherence, Utilization, Physician Reactions, and Interventions DSM-5 DSM IV-TR
ADHERENCE
UTILIZATION
PHYSICIAN REACTIONS
INTERVENTIONS
Paranoid Difficult when requested by the physician since the patient is suspicious of the need for compliance. Problematic, but may be easier when the patient is seeking relief from symptoms
Limited utilization; or as a condition for medical service utilization, the patient may seek detailed explanations or reasons for the diagnostic testing or needs for other services.
Fearful; sense of danger; mistrust; feeling accused, blamed, or threatened.
1. Empathize with patient’s fear of being hurt; acknowledge complaints without arguing or ignoring. 2. Openly and honestly explain medical illness. 3. Correct reality distortions and unreasonable patient expectations. 4. Gently question irrational thoughts and suggest more rational ones. 5. Don’t confront delusions. 6. If the patient refuses care out of mistrust, rather than insist, ask if it’s OK if you can disagree about the need for the test. 7. Interpret projection (blame) and other defenses.
Schizoid May be difficult. Will need reinforcement and monitoring, may need outreach services
Under utilization. Outreach, if not too frequent, may help foster appropriate use of medical services.
Detached or removed; wish to involve patient with others; to break through the isolation.
1. Empathize with patient’s need for privacy and contact. 2. Accept the patient’s unsociability. 3. Reduce the patient’s isolation as tolerated. 4. Neutrally impart medical information. 5. Don’t demand involvement nor permit total withdrawal. 6. Correct reality distortions and unreasonable patient expectations. 7. Gently question irrational thoughts and suggest more rational ones. 8. Interpret isolation and other defenses.
Schizotypal May be difficult. May need outreach, visiting nurse, community resources, or case management.
Under-utilization. May need outreach to gain reasonable and appropriate utilization of medical services.
Detached; removed; " weird and alone " feelings; wish to involve; or to break through the isolation.
1. Empathize with patient’s idiosyncratic style, magical thinking, and perceptions without directly confronting them. 2. Recognize the need for privacy and contact. 3. Accept the patient’s unsociability; reduce the patient’s isolation, as tolerated. 4. Neutrally impart information. 5. Don’t demand involvement or permit total withdrawal. 6. Correct reality distortions and unreasonable patient expectations. 7. Gently question irrational thoughts and suggest more rational ones. 8. Interpret regression and other defenses.
Antisocial May be resistant, problematic, and intolerant of the need for ongoing compliance.
May misuse medical resources for secondary gain.
Used, exploited or deceived; anger, and a wish to uncover lies, punish, or imprison.
1. Empathize with patient’s fear of exploitation and low self-esteem. 2. Determine if you are being used for secondary gain. Should you suspect dishonesty, verify symptoms and illness progression with others. 3. Don’t moralize. Explain that deception results in your giving the patient poor care. 4. Correct reality distortions and unreasonable patient expectations. 5. Gently question irrational thoughts and suggest more rational ones. 6. Interpret defenses. 7. Medications as adjunctive treatment (See table xx-4)
11
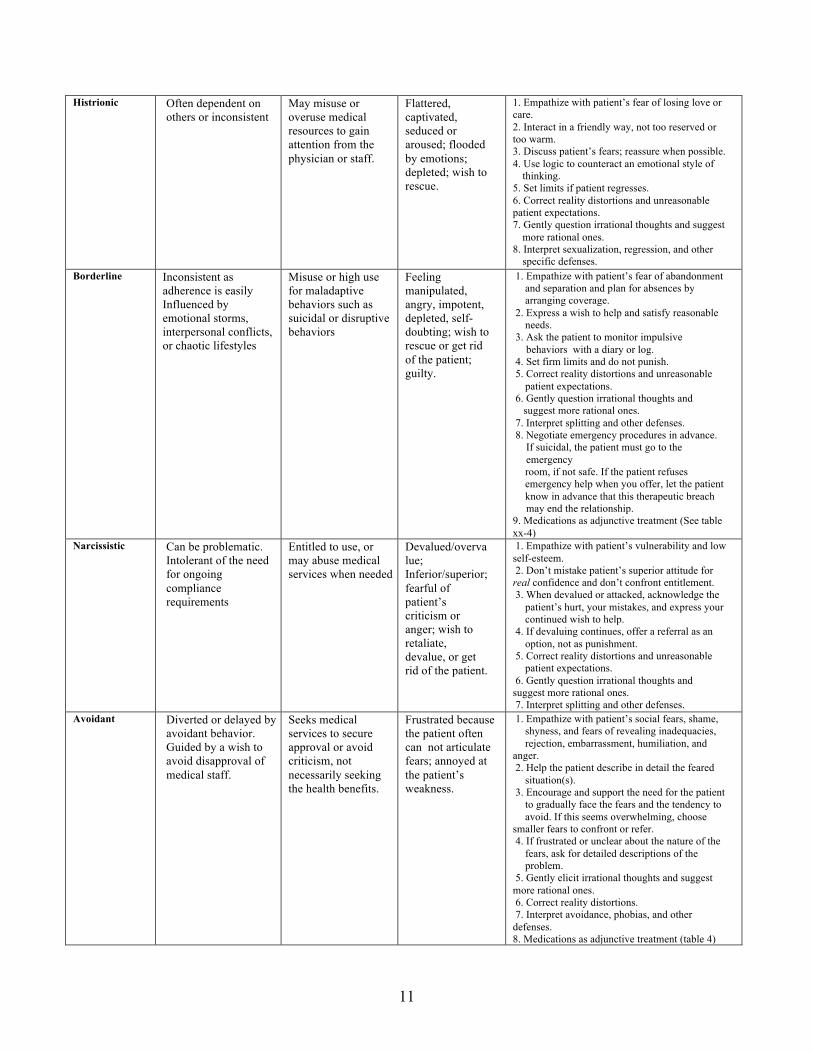
Histrionic Often dependent on others or inconsistent
May misuse or overuse medical resources to gain attention from the physician or staff.
Flattered, captivated, seduced or aroused; flooded by emotions; depleted; wish to rescue.
1. Empathize with patient’s fear of losing love or care. 2. Interact in a friendly way, not too reserved or too warm. 3. Discuss patient’s fears; reassure when possible. 4. Use logic to counteract an emotional style of thinking. 5. Set limits if patient regresses. 6. Correct reality distortions and unreasonable patient expectations. 7. Gently question irrational thoughts and suggest more rational ones. 8. Interpret sexualization, regression, and other specific defenses.
Borderline Inconsistent as adherence is easily Influenced by emotional storms, interpersonal conflicts, or chaotic lifestyles
Misuse or high use for maladaptive behaviors such as suicidal or disruptive behaviors
Feeling manipulated, angry, impotent, depleted, self-doubting; wish to rescue or get rid of the patient; guilty.
1. Empathize with patient’s fear of abandonment and separation and plan for absences by arranging coverage. 2. Express a wish to help and satisfy reasonable needs. 3. Ask the patient to monitor impulsive behaviors with a diary or log. 4. Set firm limits and do not punish. 5. Correct reality distortions and unreasonable patient expectations. 6. Gently question irrational thoughts and suggest more rational ones. 7. Interpret splitting and other defenses. 8. Negotiate emergency procedures in advance. If suicidal, the patient must go to the emergency room, if not safe. If the patient refuses emergency help when you offer, let the patient know in advance that this therapeutic breach may end the relationship. 9. Medications as adjunctive treatment (See table xx-4)
Narcissistic Can be problematic. Intolerant of the need for ongoing compliance requirements
Entitled to use, or may abuse medical services when needed
Devalued/overvalue; Inferior/superior; fearful of patient’s criticism or anger; wish to retaliate, devalue, or get rid of the patient.
1. Empathize with patient’s vulnerability and low self-esteem. 2. Don’t mistake patient’s superior attitude for real confidence and don’t confront entitlement. 3. When devalued or attacked, acknowledge the patient’s hurt, your mistakes, and express your continued wish to help. 4. If devaluing continues, offer a referral as an option, not as punishment. 5. Correct reality distortions and unreasonable patient expectations. 6. Gently question irrational thoughts and suggest more rational ones. 7. Interpret splitting and other defenses.
Avoidant Diverted or delayed by avoidant behavior. Guided by a wish to avoid disapproval of medical staff.
Seeks medical services to secure approval or avoid criticism, not necessarily seeking the health benefits.
Frustrated because the patient often can not articulate fears; annoyed at the patient’s weakness.
1. Empathize with patient’s social fears, shame, shyness, and fears of revealing inadequacies, rejection, embarrassment, humiliation, and anger. 2. Help the patient describe in detail the feared situation(s). 3. Encourage and support the need for the patient to gradually face the fears and the tendency to avoid. If this seems overwhelming, choose smaller fears to confront or refer. 4. If frustrated or unclear about the nature of the fears, ask for detailed descriptions of the problem. 5. Gently elicit irrational thoughts and suggest more rational ones. 6. Correct reality distortions. 7. Interpret avoidance, phobias, and other defenses. 8. Medications as adjunctive treatment (table 4)

12
Dependent Dependent on others for medical supervision and easily overwhelmed by the demands of self monitoring compliance.
Under use when left to themselves, but may overuse service when physician or medical staff becomes the source of needed gratification.
Depleted; annoyed at the patient’s dependence; may deny the patient’s reasonable needs.
1. Empathize with the patient’s need for care. 2. Frustrate total dependence. 3. Be careful to avoid telling the patient what to do. 4. Encourage independent thinking and action. 5. Realize that what the patient says that he or she wants (caretaking) is not necessarily what he or she needs. 6. Ask the patient what it is about independence that is so frightening. 7. Don’t abandon or threaten termination, because some very dependent patients need regular physician contact for life. 8. Correct reality distortions and unreasonable patient expectations. 9. Gently elicit irrational thoughts and suggest more rational ones. 10. Interpret regression and other specific defenses. 11. Medications as adjunctive treatment (See table xx-4)
Obsessive- compulsive
Rigid and inflexibly follows the rules; disrupted or anxious if unexpected changes are required.
Conflicted about utilization. Fears of uncertainty may drive increased use, while fears of loss of control may decrease use.
In a battle of control with negative reactions to patient stinginess, need for order, and stubbornness; distanced from feelings; bored with details.
1. Empathize with patient’s logical, detailed, unemotional style of thinking. 2. If obsessive thoughts are interfering with medical care, ask about the patient’s feelings. 3. Don’t struggle with the patient over control or critical judgments. 4. Avoid abandoning the patient. 5. Correct reality distortions and unreasonable patient expectations. 6. Gently elicit irrational thoughts and suggest more rational ones. 7. Interpret specific defenses.
Self- defeating†
Dependent on other, may be help seeking then help rejecting.
Under use of medical services because they don’t deserve them or they won’t help, or excessive use when they are treated badly.
Wish to rescue; sadistic fantasies that the patient will suffer/ die; defeated; self- blame; self-doubt, or hopelessness and helplessness.
1. Empathize with patient’s suffering. Acknowledge and appreciate the difficulty of the illness and treatment. 2. Emphasize that recovery may be a slow steady process. 3. The need for recovery can be presented as necessary to benefit others. 4. Inquire about obviously self-destructive or self- defeating behaviors. 5. Don’t abandon. 6. Correct reality distortions and unreasonable patient expectations. 7. Gently elicit irrational thoughts and suggest more rational ones. 8. Interpret specific defenses.
†From American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 3rd ed revised. Washington, DC, American Psychiatric Association, 1986.

13
Table-4 Pharmacotherapy for Symptomatic Treatment of Personality Traits and Disorders*
Anger Impulsive Aggression
Suicidal Ideation
Psychotic Symptoms
Mood Instability Interpersonal problems
Anxiety
Depression
Borderline Personality Disorder-Grade B Level of Evidence Haloperidol Aripiprazole Olanzapine Lamotrogine Topiramate
Flupentixol deconoate Olanzapine Fluphenazine decanoate Paroxetine
Aripiprazole Olanzapine
Aripiprazole Olanzapine Divalproex Sodium Topirimate
Aripiprazole Olanzapine Topirimate
Aripiprazole Divalproex Sodium Amitriptyline
Antisocial Personality Disorder- Grade C Level of Evidence Lithium Pheytoin Citalopram Sertraline
Schizotypal Personality Disorder-Grade B Level of Evidence Olanzapine
Resperidone
Avoidant Personality Disorder/Dependent Traits Grade C Level of Evidence Brofaromine
Citalopram Sertratine
*Doses of these medication are in the standard range that are used for the major psychiatric Illnesses 1) Triebwasser J, Siever LJ. Pharmacotherapy
of personality disorders. Journal of Mental Health, February 2007; 16(1): 5 – 50 2) Lieb K, Völlm B, Rücker G, Timmer A, Stoffers JM Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. BJP 2010, 196:4-12.

14
References
1. Abbass AA. Somatization: diagnosing it sooner through emotion-focused interviewing. J Fam Pract. 2005;54:231-243.
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. text revision (DSM-IV-TR). Washington, DC: APA; 2000.
3. American Psychiatric Association. Practice guideline for the treatment of patients with borderline personality disorder. Am J Psychiatry. 2001;158(suppl 10):1-52.
4. Banks MH, Beresford SA, Morrell DC, et al. Factors influencing demand for primary medical care in women aged 20-44 years: a preliminary report. Int J Epidemiology. 1975;4:189-195.
5. Beck AT, Freeman A, eds. Cognitive Therapy of Personality Disorders. New York: Guilford Press; 1990.
6. Bornstein RF, Gold SH. Comorbidity of personality disorder and somatization disorder: a meta-analytic review. J Psychopathol Behav Assess. 2008;30:154-161.
7. Cherkin DC, Eisenberg D, Sherman KJ, et al. Randomized trial comparing traditional Chinese medical acupuncture, therapeutic massage, and self-care education for chronic low back pain. Arch Intern Med. 2001;161:1081-1088.
8. Davanloo H. The technique of unlocking the unconscious in patients suffering from functional disorders. Part I. Restructuring the ego’s defenses. Unlocking the Unconscious. Chichester, England: Wiley & Sons; 1990:283-306.
9. Davanloo H. Intensive short-term dynamic psychotherapy: spectrum of psychoneurotic disorders. Intensive Short-Tern Dynamic Psychotherapy. Chichester, England: Wiley & Sons; 2001.
10. Dickinson WP, Dickinson LM, deGruy FV, et al. A randomized clinical trial of a care recommendation letter intervention for somatization in primary care. Ann Fam Med. 2003;1:228-235.
11. Feinstein RE, Rabinowitz PM, Carey L. A model for office-based cardiovascular risk reduction and behavioral change. In: Feinstein RE, Brewer AA, eds. Primary Care Psychiatry and Behavioral Medicine: Brief Office Treatment and Management Pathways. New York: Springer; 1999:330-359.
12. Grant BF, Stinson FS, Dawson DA. Co-occurrence of 12-month alcohol and drug use disorders and personality disorders in the United States: results from the National Epidemiologic Survey on Alcohol-Related Conditions. Arch Gen Psychiatry. 2004;61:361-368.
13. Greenberger D, Padesky CA. Mind over Mood: a Cognitive Therapy Treatment Manual for Clients. New York: Guilford Press; 1995.
14. Gross R, Olfson M, Gameroff M, et al. Borderline personality disorders in primary care. Arch Intern Med. 2002;162:53-60.
15
15. Groves JE. Taking care of the hateful patient. N Engl Med J. 1978;298:883-887. 16. Hahn SR. Caring for patients experienced as difficult. In: deGruy FV, Dickinson WP,
Staton EW, eds. Twenty Common Problems in Behavioral Health. New York: McGraw-Hill; 2002.
17. Hahn SR, Thompson KS, Wills TA, et al. The difficult doctor-patient relationship: somatization, personality, and psychopathology. J Clin Epidemiol. 1994;47:647-657.
18. Hahn SR, Kroenke K, Spitzer R, et al. The difficult patient in primary care: prevalence, psychopathology, and impairment. J Gen Intern Med. 1996;11:1-8.
19. Kashner TM, Rost K, Cohen B, et al. Enhancing the health of somatization disorder patients: effectiveness of short-term group therapy. Psychosomatics. 1995;36:462-470.
20. Kernberg O. Borderline Conditions and Pathological Narcissism. New York: Jason Aronson; 1975.
21. Kernberg O. Severe Personality Disorders: Psychotherapeutic Strategies. New Haven, Conn: Yale University Press; 1984.
22. Kernberg O. Aggression in Personality Disorders and Perversions. New Haven, Conn: Yale University Press; 1992.
23. Kroenke K. Unexplained physical symptoms and somatoform disorders. In: deGruy FV, Dickinson WP, Staton EW, eds. Twenty Common Problems in Behavioral Health. New York: McGraw-Hill; 2002:341-365.
24. Kroenke K. Efficacy of treatment for somatoform disorders: a review of randomized controlled trials. Psychsom Med. 2007;69:881-888.
25. Kroenke K, Jackson JL. Outcome in general medical patients presenting with common symptoms: a prospective study with a 2-week and a 3-month follow up. Fam Pract. 1998;15:398-403.
26. Kroenke K, Arrington ME, Mangelsdorff AD. The prevalence of symptoms in medical outpatients and the adequacy of therapy. Arch Intern Med. 1990;150:1685-1690.
27. Kroenke K, Spitzer RL, Williams JBW. The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom Med. 2002;64:258-266.
28. Kroenke K, Spitzer RL, Williams JBL, et al. Physical symptoms in primary care: predictors of psychiatric disorders and functional impairment. Arch Fam Med. 1994;3:774-779.
29. Lidbeck J. Group therapy for somatization disorders in general practice: effectiveness of a short cognitive-behavioral treatment model. Acta Psych Scand. 1997;96:14-24.
30. Markovitz PJ. Recent trends in the pharmacotherapy of personality disorder. J Personal DiSOR:d. 2004;18:90-101.
31. McGuire BE, Shore A. Simulated pain on the symptom checklist-90 revised. J Clin Psychol. 2001;57:1589-1596.
32. Moran P, Jenkins R, Tylee A, et al. The prevalence of personality disorder among primary care attenders. Acta Psychiatr Scand. 2000;102:52-57.

16
33. Muller T, Mannel M, Murck H, Rahlfs VW. Treatment of somatoform disorders with St. John’s wort: a randomized double-blind placebo-controlled trial. Psychosom Med. 2004;66:538-547.
34. National Institute for Mental Health in England. Personality disorder: no longer a diagnosis of exclusion. Policy implementation guidance for the development of services for people with personality disorder. 2003:1-54.
35. Nose M, Cipriana A, Biancosino B, et al. Efficacy of pharmacotherapy against core traits of borderline personality disorder: meta-analysis of randomized controlled trials. Int Clin Psychopharmacol. 2006;21:345-353.
36. Oldham JM, Skodol AE, Bender DS, eds. Essentials of Personality Disorders. Washington, DC: American Psychiatric Press; 2009.
37. O’Malley PG, Jackson JL, Santoro J, et al. Antidepressant therapy for unexplained symptoms and symptom syndromes. J Fam Pract. 1999;48:980-994.
38. Owens MK, Ehrenreich D. Literature review of nonpharmacologic methods for the treatment of chronic pain. Holistic Nurs Pract. 1991;6:24-31.
39. Sansone RA, Wiedman MW, Sansone LA. Adult somatic preoccupation and its relationship to childhood trauma. Violence Victims. 2001;16:39-47.
40. Simon GE, Guerje O. Stability of somatization disorder and somatization symptoms among primary care patients. Arch Gen Psychiatry. 1999;56:90-95.
41. Skodol AE, Bender DS, Oldham JM. Future directions. In: Oldham JM, Skodal AE, Bender DS, eds. Essentials of Personality Disorders. Washington, DC: American Psychiatric Press; 2009:381-392.
42. Smith GR, Miller LM, Monson RA. Consultation-liaison intervention in somatization disorder. Hosp Comm Psychiatry. 1986;37:1207-1210.
43. Smith GR, Rost K, Kashner TM. A trial of the effect of a standardized psychiatric consultation on health outcomes and costs in somatizing patients. Arch Gen Psychiatry. 1995;52:238-243.
44. Soeteman DI, Hakkaart-van Roijen L, et al. The economic burden of personality disorders in mental health care. J Clin Psychiatry. 2008;69:259-265.
45. Soloff PH. Psychopharmacology of borderline personality disorder. Psychiatry Clin North Am. 2000;23:169-192.
46. Soloff H. Somatic treatment. In: Oldham JM, Skodol AE, Bender DS, eds. Essentials of Personality Disorders. Washington DC: American Psychiatric Press; 2009:267-288.
47. Spitzer RL, Williams JBW, Kroenke K, et al. Utility of a new procedure for diagnosing mental disorders in primary care: the PRIME-MD 1000 study. JAMA. 1994;272:1749-1756.
48. Strous RD, Ulman AM, Kotler M. The hateful patient revisited: relevance for 21st century medicine. Eur J Intern Med. 2006;17:387-393.

17
49. Volz HP, Murck H, Kasper S, Moller HJ. St John’s wort extract (LI 160) in somatoform disorders: results of a placebo-controlled trial. Psychopharmacology. 2002;164:294-300.
50. Ypriitham R. Psychopharmacology of borderline personality disorder. Curr Sci. 2004;6:225-231.
Web Resources www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001935 National Center for Biotechnology Information Reviews of the major personality disorders and treatments www.nmha.org/go/information/get-info/personality-disorders Mental Health America Consumer information about personality disorders www.nice.org.uk/search/guidancesearchresults.jsp?keywords=Personailty+Disorders&newSearc
h=true&searchType=Guidance National Institute for Health and Clinical Excellence (NICE) Practice guidelines for personality disorders www.guideline.gov/search/search.aspx?term=personality+disorders National Guideline Clearinghouse Practice guidelines for borderline and antisocial personality disorders www.nlm.nih.gov National Institute of Mental Health on Somatization and Personality Disorders www.psych.org American Psychiatric Association Information on somatic and personality disorders
[Tables/boxes]