liver development
TRANSCRIPT

Hepatogenesis Liver
In childBy
Prabht kumar keshav
3rd year5th group
Development of the liver
The liver bud or hepatic diverticulum is formed from an outgrowth of the endodermal epithelial lining of the foregut
The epithelial liver cords and primordia of the biliary system which develop from the hepatic diverticulum grow into the mesenchymal septum transversum
Between the layers of the ventral mesentery derived from the septum transversum these primordial cells differentiate into the parenchyma of the liver and the lining of the ducts of the biliary system
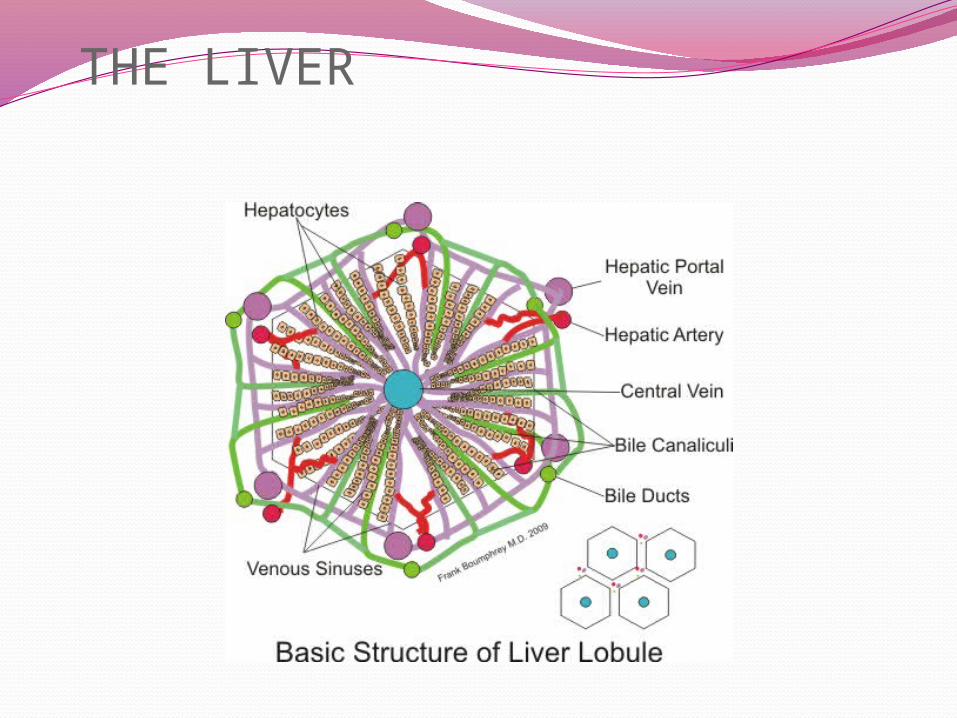
THE LIVER
Early liver morphogenesis1048667Liver is derived from endoderm1048667It forms from a diverticulum (bud) whichbranches out from the primitive gut1048667The pancreas develops dorsally while the liverbud develops ventrally1048667The liver metabolises nutrients absorbed from thegut Therefore first organ to receive intake1048667It removes toxic compounds which are absorbedby modifying them so they are soluble
The gallbladder bile ducts and liver begin to develop during the 4th week of embryogenesis as a ventral bud from the most caudal aspect of the foregut (the future duodenum) This bud is called the hepatic diverticulum and it grows between the
layers of the ventral mesentery (Fig 1) The hepatic diverticulum has two distinct components pars hepatica and pars cystica (1) The pars hepatica the most cranial component gives rise to the liver common hepatic duct and intrahepatic bile ducts The pars cystica the most caudal component gives rise to the cystic diverticulum The cystic diverticulum is the anlage of the gallbladder and the cystic duct The original hepatic diverticulum elongates to form the common bile duct These structures begin
as solid cords but by the 8th week of gestation a lumen has been established throughout the biliary tract
Liver development
Gross Anatomy The liver is divided) into
four lobes the right (the largest lobe) left quadrate and caudate lobes
Supplied with blood via the protal vein and hepatic artery
Blood carried away by the hepatic vein
It is connected to the diaphragm and abdomainal walls by five ligaments
Gall Bladder Muscular bag for the
storage concentration acidification and delivery of bile to small intestine
The liver is the only human organ that has the remarkable property of self-regeneration If a part of the liver is removed the remaining parts can grow back to its original size and shape
Fetal blood supplyIn the growing fetus a major source of
blood to the liver is the umbilical vein which supplies nutrients to the growing fetus The umbilical vein enters the abdomen at the umbilicus and passes upward along the free margin of the falciform ligament of the liver to the inferior surface of the liver There it joins with the left branch of the portal vein The ductus venosus carries blood from the left portal vein to the left hepatic vein and then to the inferior vena cava allowing placental blood to bypass the liver
Fetal blood supplyIn the fetus the liver develops throughout
normal gestation and does not perform the normal filtration of the infant liver The liver does not perform digestive processes because the fetus does not consume meals directly but receives nourishment from the mother via the placenta The fetal liver releases some blood stem cells that migrate to the fetal thymus so initially the lymphocytes called T-cells are created from fetal liver stem cells Once the fetus is delivered the formation of blood stem cells in infants shifts to the red bone marrow
The liver and biliarysystem develop from the hepatic diverticulum
bullThe distal end of the hepatic divertivculum proliferates rapidly in the septum transversum to form the hepatocytes and intra-hepatic biliary system bullThe proximal part in the ventral mesogastrium does not proliferate rapidly becomes relatively narrow and forms the extrahepatic biliary system A secondary outgrowth from it forms the gall bladder and cystic duct during the 4thweek (day 24)bullThe vitelline and umbilical veins disrupted by growth of hepatic cells in the septum transversum form the liver sinusoids bullThe septum transversum mesoderm surrounding the hepatic cords forms the Kuppfer cells and haemopoietic cells
Developemental stagesAfter birth the umbilical vein and ductus
venosus are completely obliterated in two to five days the former becomes the ligamentum teres and the latter becomes the ligamentum venosum In the disease state of cirrhosis and portal hypertension the umbilical vein can open up again
During childhood-At birth the liver comprises roughly 4 of body weight and is at average 120g Over the course of development it will increase to 14ndash16 kg but will only take up 25ndash35 of body weight
Cardiac mesoderm is necessaryfor liver formation1048667In mid 1960rsquos Le Douarin developed amodel using cultured fragments of tissuefrom chick embryos1048667 Piece of primitive gut (endoderm) cannotdevelop into liver by itself1048667 Requires interaction with cardiac mesoderm toproduce glycogen storing hepatocytes1048667 A physical barrier between the two
The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

Development of the liver
The liver bud or hepatic diverticulum is formed from an outgrowth of the endodermal epithelial lining of the foregut
The epithelial liver cords and primordia of the biliary system which develop from the hepatic diverticulum grow into the mesenchymal septum transversum
Between the layers of the ventral mesentery derived from the septum transversum these primordial cells differentiate into the parenchyma of the liver and the lining of the ducts of the biliary system
THE LIVER
Early liver morphogenesis1048667Liver is derived from endoderm1048667It forms from a diverticulum (bud) whichbranches out from the primitive gut1048667The pancreas develops dorsally while the liverbud develops ventrally1048667The liver metabolises nutrients absorbed from thegut Therefore first organ to receive intake1048667It removes toxic compounds which are absorbedby modifying them so they are soluble
The gallbladder bile ducts and liver begin to develop during the 4th week of embryogenesis as a ventral bud from the most caudal aspect of the foregut (the future duodenum) This bud is called the hepatic diverticulum and it grows between the
layers of the ventral mesentery (Fig 1) The hepatic diverticulum has two distinct components pars hepatica and pars cystica (1) The pars hepatica the most cranial component gives rise to the liver common hepatic duct and intrahepatic bile ducts The pars cystica the most caudal component gives rise to the cystic diverticulum The cystic diverticulum is the anlage of the gallbladder and the cystic duct The original hepatic diverticulum elongates to form the common bile duct These structures begin
as solid cords but by the 8th week of gestation a lumen has been established throughout the biliary tract
Liver development
Gross Anatomy The liver is divided) into
four lobes the right (the largest lobe) left quadrate and caudate lobes
Supplied with blood via the protal vein and hepatic artery
Blood carried away by the hepatic vein
It is connected to the diaphragm and abdomainal walls by five ligaments
Gall Bladder Muscular bag for the
storage concentration acidification and delivery of bile to small intestine
The liver is the only human organ that has the remarkable property of self-regeneration If a part of the liver is removed the remaining parts can grow back to its original size and shape
Fetal blood supplyIn the growing fetus a major source of
blood to the liver is the umbilical vein which supplies nutrients to the growing fetus The umbilical vein enters the abdomen at the umbilicus and passes upward along the free margin of the falciform ligament of the liver to the inferior surface of the liver There it joins with the left branch of the portal vein The ductus venosus carries blood from the left portal vein to the left hepatic vein and then to the inferior vena cava allowing placental blood to bypass the liver
Fetal blood supplyIn the fetus the liver develops throughout
normal gestation and does not perform the normal filtration of the infant liver The liver does not perform digestive processes because the fetus does not consume meals directly but receives nourishment from the mother via the placenta The fetal liver releases some blood stem cells that migrate to the fetal thymus so initially the lymphocytes called T-cells are created from fetal liver stem cells Once the fetus is delivered the formation of blood stem cells in infants shifts to the red bone marrow
The liver and biliarysystem develop from the hepatic diverticulum
bullThe distal end of the hepatic divertivculum proliferates rapidly in the septum transversum to form the hepatocytes and intra-hepatic biliary system bullThe proximal part in the ventral mesogastrium does not proliferate rapidly becomes relatively narrow and forms the extrahepatic biliary system A secondary outgrowth from it forms the gall bladder and cystic duct during the 4thweek (day 24)bullThe vitelline and umbilical veins disrupted by growth of hepatic cells in the septum transversum form the liver sinusoids bullThe septum transversum mesoderm surrounding the hepatic cords forms the Kuppfer cells and haemopoietic cells
Developemental stagesAfter birth the umbilical vein and ductus
venosus are completely obliterated in two to five days the former becomes the ligamentum teres and the latter becomes the ligamentum venosum In the disease state of cirrhosis and portal hypertension the umbilical vein can open up again
During childhood-At birth the liver comprises roughly 4 of body weight and is at average 120g Over the course of development it will increase to 14ndash16 kg but will only take up 25ndash35 of body weight
Cardiac mesoderm is necessaryfor liver formation1048667In mid 1960rsquos Le Douarin developed amodel using cultured fragments of tissuefrom chick embryos1048667 Piece of primitive gut (endoderm) cannotdevelop into liver by itself1048667 Requires interaction with cardiac mesoderm toproduce glycogen storing hepatocytes1048667 A physical barrier between the two
The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-
THE LIVER
Early liver morphogenesis1048667Liver is derived from endoderm1048667It forms from a diverticulum (bud) whichbranches out from the primitive gut1048667The pancreas develops dorsally while the liverbud develops ventrally1048667The liver metabolises nutrients absorbed from thegut Therefore first organ to receive intake1048667It removes toxic compounds which are absorbedby modifying them so they are soluble
The gallbladder bile ducts and liver begin to develop during the 4th week of embryogenesis as a ventral bud from the most caudal aspect of the foregut (the future duodenum) This bud is called the hepatic diverticulum and it grows between the
layers of the ventral mesentery (Fig 1) The hepatic diverticulum has two distinct components pars hepatica and pars cystica (1) The pars hepatica the most cranial component gives rise to the liver common hepatic duct and intrahepatic bile ducts The pars cystica the most caudal component gives rise to the cystic diverticulum The cystic diverticulum is the anlage of the gallbladder and the cystic duct The original hepatic diverticulum elongates to form the common bile duct These structures begin
as solid cords but by the 8th week of gestation a lumen has been established throughout the biliary tract
Liver development
Gross Anatomy The liver is divided) into
four lobes the right (the largest lobe) left quadrate and caudate lobes
Supplied with blood via the protal vein and hepatic artery
Blood carried away by the hepatic vein
It is connected to the diaphragm and abdomainal walls by five ligaments
Gall Bladder Muscular bag for the
storage concentration acidification and delivery of bile to small intestine
The liver is the only human organ that has the remarkable property of self-regeneration If a part of the liver is removed the remaining parts can grow back to its original size and shape
Fetal blood supplyIn the growing fetus a major source of
blood to the liver is the umbilical vein which supplies nutrients to the growing fetus The umbilical vein enters the abdomen at the umbilicus and passes upward along the free margin of the falciform ligament of the liver to the inferior surface of the liver There it joins with the left branch of the portal vein The ductus venosus carries blood from the left portal vein to the left hepatic vein and then to the inferior vena cava allowing placental blood to bypass the liver
Fetal blood supplyIn the fetus the liver develops throughout
normal gestation and does not perform the normal filtration of the infant liver The liver does not perform digestive processes because the fetus does not consume meals directly but receives nourishment from the mother via the placenta The fetal liver releases some blood stem cells that migrate to the fetal thymus so initially the lymphocytes called T-cells are created from fetal liver stem cells Once the fetus is delivered the formation of blood stem cells in infants shifts to the red bone marrow
The liver and biliarysystem develop from the hepatic diverticulum
bullThe distal end of the hepatic divertivculum proliferates rapidly in the septum transversum to form the hepatocytes and intra-hepatic biliary system bullThe proximal part in the ventral mesogastrium does not proliferate rapidly becomes relatively narrow and forms the extrahepatic biliary system A secondary outgrowth from it forms the gall bladder and cystic duct during the 4thweek (day 24)bullThe vitelline and umbilical veins disrupted by growth of hepatic cells in the septum transversum form the liver sinusoids bullThe septum transversum mesoderm surrounding the hepatic cords forms the Kuppfer cells and haemopoietic cells
Developemental stagesAfter birth the umbilical vein and ductus
venosus are completely obliterated in two to five days the former becomes the ligamentum teres and the latter becomes the ligamentum venosum In the disease state of cirrhosis and portal hypertension the umbilical vein can open up again
During childhood-At birth the liver comprises roughly 4 of body weight and is at average 120g Over the course of development it will increase to 14ndash16 kg but will only take up 25ndash35 of body weight
Cardiac mesoderm is necessaryfor liver formation1048667In mid 1960rsquos Le Douarin developed amodel using cultured fragments of tissuefrom chick embryos1048667 Piece of primitive gut (endoderm) cannotdevelop into liver by itself1048667 Requires interaction with cardiac mesoderm toproduce glycogen storing hepatocytes1048667 A physical barrier between the two
The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

Early liver morphogenesis1048667Liver is derived from endoderm1048667It forms from a diverticulum (bud) whichbranches out from the primitive gut1048667The pancreas develops dorsally while the liverbud develops ventrally1048667The liver metabolises nutrients absorbed from thegut Therefore first organ to receive intake1048667It removes toxic compounds which are absorbedby modifying them so they are soluble
The gallbladder bile ducts and liver begin to develop during the 4th week of embryogenesis as a ventral bud from the most caudal aspect of the foregut (the future duodenum) This bud is called the hepatic diverticulum and it grows between the
layers of the ventral mesentery (Fig 1) The hepatic diverticulum has two distinct components pars hepatica and pars cystica (1) The pars hepatica the most cranial component gives rise to the liver common hepatic duct and intrahepatic bile ducts The pars cystica the most caudal component gives rise to the cystic diverticulum The cystic diverticulum is the anlage of the gallbladder and the cystic duct The original hepatic diverticulum elongates to form the common bile duct These structures begin
as solid cords but by the 8th week of gestation a lumen has been established throughout the biliary tract
Liver development
Gross Anatomy The liver is divided) into
four lobes the right (the largest lobe) left quadrate and caudate lobes
Supplied with blood via the protal vein and hepatic artery
Blood carried away by the hepatic vein
It is connected to the diaphragm and abdomainal walls by five ligaments
Gall Bladder Muscular bag for the
storage concentration acidification and delivery of bile to small intestine
The liver is the only human organ that has the remarkable property of self-regeneration If a part of the liver is removed the remaining parts can grow back to its original size and shape
Fetal blood supplyIn the growing fetus a major source of
blood to the liver is the umbilical vein which supplies nutrients to the growing fetus The umbilical vein enters the abdomen at the umbilicus and passes upward along the free margin of the falciform ligament of the liver to the inferior surface of the liver There it joins with the left branch of the portal vein The ductus venosus carries blood from the left portal vein to the left hepatic vein and then to the inferior vena cava allowing placental blood to bypass the liver
Fetal blood supplyIn the fetus the liver develops throughout
normal gestation and does not perform the normal filtration of the infant liver The liver does not perform digestive processes because the fetus does not consume meals directly but receives nourishment from the mother via the placenta The fetal liver releases some blood stem cells that migrate to the fetal thymus so initially the lymphocytes called T-cells are created from fetal liver stem cells Once the fetus is delivered the formation of blood stem cells in infants shifts to the red bone marrow
The liver and biliarysystem develop from the hepatic diverticulum
bullThe distal end of the hepatic divertivculum proliferates rapidly in the septum transversum to form the hepatocytes and intra-hepatic biliary system bullThe proximal part in the ventral mesogastrium does not proliferate rapidly becomes relatively narrow and forms the extrahepatic biliary system A secondary outgrowth from it forms the gall bladder and cystic duct during the 4thweek (day 24)bullThe vitelline and umbilical veins disrupted by growth of hepatic cells in the septum transversum form the liver sinusoids bullThe septum transversum mesoderm surrounding the hepatic cords forms the Kuppfer cells and haemopoietic cells
Developemental stagesAfter birth the umbilical vein and ductus
venosus are completely obliterated in two to five days the former becomes the ligamentum teres and the latter becomes the ligamentum venosum In the disease state of cirrhosis and portal hypertension the umbilical vein can open up again
During childhood-At birth the liver comprises roughly 4 of body weight and is at average 120g Over the course of development it will increase to 14ndash16 kg but will only take up 25ndash35 of body weight
Cardiac mesoderm is necessaryfor liver formation1048667In mid 1960rsquos Le Douarin developed amodel using cultured fragments of tissuefrom chick embryos1048667 Piece of primitive gut (endoderm) cannotdevelop into liver by itself1048667 Requires interaction with cardiac mesoderm toproduce glycogen storing hepatocytes1048667 A physical barrier between the two
The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

The gallbladder bile ducts and liver begin to develop during the 4th week of embryogenesis as a ventral bud from the most caudal aspect of the foregut (the future duodenum) This bud is called the hepatic diverticulum and it grows between the
layers of the ventral mesentery (Fig 1) The hepatic diverticulum has two distinct components pars hepatica and pars cystica (1) The pars hepatica the most cranial component gives rise to the liver common hepatic duct and intrahepatic bile ducts The pars cystica the most caudal component gives rise to the cystic diverticulum The cystic diverticulum is the anlage of the gallbladder and the cystic duct The original hepatic diverticulum elongates to form the common bile duct These structures begin
as solid cords but by the 8th week of gestation a lumen has been established throughout the biliary tract
Liver development
Gross Anatomy The liver is divided) into
four lobes the right (the largest lobe) left quadrate and caudate lobes
Supplied with blood via the protal vein and hepatic artery
Blood carried away by the hepatic vein
It is connected to the diaphragm and abdomainal walls by five ligaments
Gall Bladder Muscular bag for the
storage concentration acidification and delivery of bile to small intestine
The liver is the only human organ that has the remarkable property of self-regeneration If a part of the liver is removed the remaining parts can grow back to its original size and shape
Fetal blood supplyIn the growing fetus a major source of
blood to the liver is the umbilical vein which supplies nutrients to the growing fetus The umbilical vein enters the abdomen at the umbilicus and passes upward along the free margin of the falciform ligament of the liver to the inferior surface of the liver There it joins with the left branch of the portal vein The ductus venosus carries blood from the left portal vein to the left hepatic vein and then to the inferior vena cava allowing placental blood to bypass the liver
Fetal blood supplyIn the fetus the liver develops throughout
normal gestation and does not perform the normal filtration of the infant liver The liver does not perform digestive processes because the fetus does not consume meals directly but receives nourishment from the mother via the placenta The fetal liver releases some blood stem cells that migrate to the fetal thymus so initially the lymphocytes called T-cells are created from fetal liver stem cells Once the fetus is delivered the formation of blood stem cells in infants shifts to the red bone marrow
The liver and biliarysystem develop from the hepatic diverticulum
bullThe distal end of the hepatic divertivculum proliferates rapidly in the septum transversum to form the hepatocytes and intra-hepatic biliary system bullThe proximal part in the ventral mesogastrium does not proliferate rapidly becomes relatively narrow and forms the extrahepatic biliary system A secondary outgrowth from it forms the gall bladder and cystic duct during the 4thweek (day 24)bullThe vitelline and umbilical veins disrupted by growth of hepatic cells in the septum transversum form the liver sinusoids bullThe septum transversum mesoderm surrounding the hepatic cords forms the Kuppfer cells and haemopoietic cells
Developemental stagesAfter birth the umbilical vein and ductus
venosus are completely obliterated in two to five days the former becomes the ligamentum teres and the latter becomes the ligamentum venosum In the disease state of cirrhosis and portal hypertension the umbilical vein can open up again
During childhood-At birth the liver comprises roughly 4 of body weight and is at average 120g Over the course of development it will increase to 14ndash16 kg but will only take up 25ndash35 of body weight
Cardiac mesoderm is necessaryfor liver formation1048667In mid 1960rsquos Le Douarin developed amodel using cultured fragments of tissuefrom chick embryos1048667 Piece of primitive gut (endoderm) cannotdevelop into liver by itself1048667 Requires interaction with cardiac mesoderm toproduce glycogen storing hepatocytes1048667 A physical barrier between the two
The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

Gross Anatomy The liver is divided) into
four lobes the right (the largest lobe) left quadrate and caudate lobes
Supplied with blood via the protal vein and hepatic artery
Blood carried away by the hepatic vein
It is connected to the diaphragm and abdomainal walls by five ligaments
Gall Bladder Muscular bag for the
storage concentration acidification and delivery of bile to small intestine
The liver is the only human organ that has the remarkable property of self-regeneration If a part of the liver is removed the remaining parts can grow back to its original size and shape
Fetal blood supplyIn the growing fetus a major source of
blood to the liver is the umbilical vein which supplies nutrients to the growing fetus The umbilical vein enters the abdomen at the umbilicus and passes upward along the free margin of the falciform ligament of the liver to the inferior surface of the liver There it joins with the left branch of the portal vein The ductus venosus carries blood from the left portal vein to the left hepatic vein and then to the inferior vena cava allowing placental blood to bypass the liver
Fetal blood supplyIn the fetus the liver develops throughout
normal gestation and does not perform the normal filtration of the infant liver The liver does not perform digestive processes because the fetus does not consume meals directly but receives nourishment from the mother via the placenta The fetal liver releases some blood stem cells that migrate to the fetal thymus so initially the lymphocytes called T-cells are created from fetal liver stem cells Once the fetus is delivered the formation of blood stem cells in infants shifts to the red bone marrow
The liver and biliarysystem develop from the hepatic diverticulum
bullThe distal end of the hepatic divertivculum proliferates rapidly in the septum transversum to form the hepatocytes and intra-hepatic biliary system bullThe proximal part in the ventral mesogastrium does not proliferate rapidly becomes relatively narrow and forms the extrahepatic biliary system A secondary outgrowth from it forms the gall bladder and cystic duct during the 4thweek (day 24)bullThe vitelline and umbilical veins disrupted by growth of hepatic cells in the septum transversum form the liver sinusoids bullThe septum transversum mesoderm surrounding the hepatic cords forms the Kuppfer cells and haemopoietic cells
Developemental stagesAfter birth the umbilical vein and ductus
venosus are completely obliterated in two to five days the former becomes the ligamentum teres and the latter becomes the ligamentum venosum In the disease state of cirrhosis and portal hypertension the umbilical vein can open up again
During childhood-At birth the liver comprises roughly 4 of body weight and is at average 120g Over the course of development it will increase to 14ndash16 kg but will only take up 25ndash35 of body weight
Cardiac mesoderm is necessaryfor liver formation1048667In mid 1960rsquos Le Douarin developed amodel using cultured fragments of tissuefrom chick embryos1048667 Piece of primitive gut (endoderm) cannotdevelop into liver by itself1048667 Requires interaction with cardiac mesoderm toproduce glycogen storing hepatocytes1048667 A physical barrier between the two
The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

Fetal blood supplyIn the growing fetus a major source of
blood to the liver is the umbilical vein which supplies nutrients to the growing fetus The umbilical vein enters the abdomen at the umbilicus and passes upward along the free margin of the falciform ligament of the liver to the inferior surface of the liver There it joins with the left branch of the portal vein The ductus venosus carries blood from the left portal vein to the left hepatic vein and then to the inferior vena cava allowing placental blood to bypass the liver
Fetal blood supplyIn the fetus the liver develops throughout
normal gestation and does not perform the normal filtration of the infant liver The liver does not perform digestive processes because the fetus does not consume meals directly but receives nourishment from the mother via the placenta The fetal liver releases some blood stem cells that migrate to the fetal thymus so initially the lymphocytes called T-cells are created from fetal liver stem cells Once the fetus is delivered the formation of blood stem cells in infants shifts to the red bone marrow
The liver and biliarysystem develop from the hepatic diverticulum
bullThe distal end of the hepatic divertivculum proliferates rapidly in the septum transversum to form the hepatocytes and intra-hepatic biliary system bullThe proximal part in the ventral mesogastrium does not proliferate rapidly becomes relatively narrow and forms the extrahepatic biliary system A secondary outgrowth from it forms the gall bladder and cystic duct during the 4thweek (day 24)bullThe vitelline and umbilical veins disrupted by growth of hepatic cells in the septum transversum form the liver sinusoids bullThe septum transversum mesoderm surrounding the hepatic cords forms the Kuppfer cells and haemopoietic cells
Developemental stagesAfter birth the umbilical vein and ductus
venosus are completely obliterated in two to five days the former becomes the ligamentum teres and the latter becomes the ligamentum venosum In the disease state of cirrhosis and portal hypertension the umbilical vein can open up again
During childhood-At birth the liver comprises roughly 4 of body weight and is at average 120g Over the course of development it will increase to 14ndash16 kg but will only take up 25ndash35 of body weight
Cardiac mesoderm is necessaryfor liver formation1048667In mid 1960rsquos Le Douarin developed amodel using cultured fragments of tissuefrom chick embryos1048667 Piece of primitive gut (endoderm) cannotdevelop into liver by itself1048667 Requires interaction with cardiac mesoderm toproduce glycogen storing hepatocytes1048667 A physical barrier between the two
The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

Fetal blood supplyIn the fetus the liver develops throughout
normal gestation and does not perform the normal filtration of the infant liver The liver does not perform digestive processes because the fetus does not consume meals directly but receives nourishment from the mother via the placenta The fetal liver releases some blood stem cells that migrate to the fetal thymus so initially the lymphocytes called T-cells are created from fetal liver stem cells Once the fetus is delivered the formation of blood stem cells in infants shifts to the red bone marrow
The liver and biliarysystem develop from the hepatic diverticulum
bullThe distal end of the hepatic divertivculum proliferates rapidly in the septum transversum to form the hepatocytes and intra-hepatic biliary system bullThe proximal part in the ventral mesogastrium does not proliferate rapidly becomes relatively narrow and forms the extrahepatic biliary system A secondary outgrowth from it forms the gall bladder and cystic duct during the 4thweek (day 24)bullThe vitelline and umbilical veins disrupted by growth of hepatic cells in the septum transversum form the liver sinusoids bullThe septum transversum mesoderm surrounding the hepatic cords forms the Kuppfer cells and haemopoietic cells
Developemental stagesAfter birth the umbilical vein and ductus
venosus are completely obliterated in two to five days the former becomes the ligamentum teres and the latter becomes the ligamentum venosum In the disease state of cirrhosis and portal hypertension the umbilical vein can open up again
During childhood-At birth the liver comprises roughly 4 of body weight and is at average 120g Over the course of development it will increase to 14ndash16 kg but will only take up 25ndash35 of body weight
Cardiac mesoderm is necessaryfor liver formation1048667In mid 1960rsquos Le Douarin developed amodel using cultured fragments of tissuefrom chick embryos1048667 Piece of primitive gut (endoderm) cannotdevelop into liver by itself1048667 Requires interaction with cardiac mesoderm toproduce glycogen storing hepatocytes1048667 A physical barrier between the two
The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

The liver and biliarysystem develop from the hepatic diverticulum
bullThe distal end of the hepatic divertivculum proliferates rapidly in the septum transversum to form the hepatocytes and intra-hepatic biliary system bullThe proximal part in the ventral mesogastrium does not proliferate rapidly becomes relatively narrow and forms the extrahepatic biliary system A secondary outgrowth from it forms the gall bladder and cystic duct during the 4thweek (day 24)bullThe vitelline and umbilical veins disrupted by growth of hepatic cells in the septum transversum form the liver sinusoids bullThe septum transversum mesoderm surrounding the hepatic cords forms the Kuppfer cells and haemopoietic cells
Developemental stagesAfter birth the umbilical vein and ductus
venosus are completely obliterated in two to five days the former becomes the ligamentum teres and the latter becomes the ligamentum venosum In the disease state of cirrhosis and portal hypertension the umbilical vein can open up again
During childhood-At birth the liver comprises roughly 4 of body weight and is at average 120g Over the course of development it will increase to 14ndash16 kg but will only take up 25ndash35 of body weight
Cardiac mesoderm is necessaryfor liver formation1048667In mid 1960rsquos Le Douarin developed amodel using cultured fragments of tissuefrom chick embryos1048667 Piece of primitive gut (endoderm) cannotdevelop into liver by itself1048667 Requires interaction with cardiac mesoderm toproduce glycogen storing hepatocytes1048667 A physical barrier between the two
The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

Developemental stagesAfter birth the umbilical vein and ductus
venosus are completely obliterated in two to five days the former becomes the ligamentum teres and the latter becomes the ligamentum venosum In the disease state of cirrhosis and portal hypertension the umbilical vein can open up again
During childhood-At birth the liver comprises roughly 4 of body weight and is at average 120g Over the course of development it will increase to 14ndash16 kg but will only take up 25ndash35 of body weight
Cardiac mesoderm is necessaryfor liver formation1048667In mid 1960rsquos Le Douarin developed amodel using cultured fragments of tissuefrom chick embryos1048667 Piece of primitive gut (endoderm) cannotdevelop into liver by itself1048667 Requires interaction with cardiac mesoderm toproduce glycogen storing hepatocytes1048667 A physical barrier between the two
The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

Cardiac mesoderm is necessaryfor liver formation1048667In mid 1960rsquos Le Douarin developed amodel using cultured fragments of tissuefrom chick embryos1048667 Piece of primitive gut (endoderm) cannotdevelop into liver by itself1048667 Requires interaction with cardiac mesoderm toproduce glycogen storing hepatocytes1048667 A physical barrier between the two
The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

The liver and biliarysystem develop from the hepatic diverticulumbullThe distal end proliferates rapidly in the septum transversumto form the hepatocytes and intra-hepatic biliarysystembullThe proximal part in the ventral mesogastriumproliferate slowly becomes relatively narrow and forms the extrahepatic biliarysystem bullA secondary outgrowth from it forms the gall bladderand cysticductduring the 4thweek (day 24)
Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

Functions Metabolic SynthesisBreakdownOther functions ndash storage of vitamin ADB12FhellipExcretion of waste products from bloodstream
into bileVascular ndash storage of blood
SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

SynthesisProtein metabolism Synthesis of amino acidsCarbohydrate metabolism GluconeogenesisGlycogenolysisGlycogenesisLipid metabolismCholesterol synthesisLipogenesis Production of coagulation factors I II V VII IX X
and XI and protein C protein S and antithrombinMain site of red blood cell productionProduces insulin-like growth factor 1 (IGF-1) a
polypeptide protein ndash anabolic effectsProduction of trombopoetin
BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

BreakdownBreaks down insulin and other hormonesBreaks down hemoglobinBreaks down or modifies toxic substances
(methylation) rarr sometimes results in toxication
Converts ammonia to urea
Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

Other functionsProduces albumin the major osmolar
component of blood serumSynthesizes angiotensinogen the hormone
responsible for raising blood pressure when activated by renin (enzyme released when the kidney senses low blood pressure)
1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

1
234567
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderOmphalomesenteric veinOmphalaomesenteric ductUmbilical vein
1
2345
Capillary network of theomphalomesenteric veinLiver budIntestinal tube (duodenum)Gall bladderDorsal pancreas anlage
Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

Summary1048667 Liver develops from ventral endoderm1048667 Initially hepatoblasts with limited liver function aregenerated (this requires GATA and HNF3)1048667 This process depends on interaction between endodermand cardiac mesoderm as this produces inducing factorssuch as Hex1048667 Later hepatoblasts differentiate into hepatocytes Thisrequires further interaction with the septum transversum(which provides Bmp4)1048667 In the perinatal stages more functions are acquired byhepatocytes and this is driven by hormones which initiatetranscription of many liver specific genes
Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

Some questions1In child bone marrow is not developed then
where is is formed what do you mean by De novo in childs liver
diseaseWhat is difference between
ldquocentrilobularrdquo and ldquoperiportalrdquo
спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-

спасибо за ваше терпение
- Slide 1
- Development of the liver
- THE LIVER
- Slide 4
- Slide 5
- Gross Anatomy
- Fetal blood supply
- Slide 8
- Fetal blood supply (2)
- Slide 10
- Developemental stages
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Functions
- Synthesis
- Breakdown
- Other functions
- Slide 20
- Slide 21
- Some questions
- Slide 23
-